Patient characteristics, burden of disease, healthcare resource utilization and costs in acute myeloid leukemia – a retrospective observational study with German claims data
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess patient characteristics, burden of disease, healthcare resource utilization and costs of acute myeloid leukemia (AML) by treatment intensity in German claims data. Materials & methods: In this retrospective cohort study using claims data from the German sickness fund AOK PLUS, we identified incident AML patients between 2012 and 2022. Incident AML patients were stratified into groups receiving intensive chemotherapy (IC) or nonintensive therapy (NIC). We then conducted descriptive analyses of patient characteristics, disease burden, including blood and platelet transfusions, healthcare resource utilization and costs. Results: We identified 1533 incident AML patients who received treatment (male: 53%; mean age: 67.7 years; median Charlson comorbidity index [CCI]: 5.0), corresponding to an incidence rate of 4.4/100,000. A total of 688 patients (44.9%) were categorized as IC, 845 patients (55.1%) as NIC. Notably, 860 additional patients (male: 48%; 78.0 years; median CCI: 5.0) had no relevant treatment code. NIC patients were older than IC patients (78.0 vs 61.0 years) and had a higher comorbidity burden (median CCI: 6.0 vs 4.0). NIC patients were hospitalized to a lesser extent (81.3% vs 87.9%), had shorter lengths of stay (64.0 vs 103.1 days/patient-year [PY]) and lower hospitalization costs/PY (56,063€/PY vs 110,186€/PY) compared with IC patients. Anemia and thrombocytopenia (NIC: 40.5 and 39.5%, IC: 76.9 and 42.6%) as well as blood and platelet transfusions were common, especially among IC patients (NIC: 93.0 and 74.3%, IC: 99.4 and 98.5%). Conclusion: Compared with IC patients, NIC patients were older, had a higher comorbidity burden and fewer hospitalizations. Combined with the high number of older patients not receiving AML treatment, this points to a lack of adequate treatment options for this patient population. The high rates of blood and platelet transfusions, particularly among IC patients, underscore the high disease burden and emphasize the need for better-tolerated therapies.
Plain language summary: Patients characteristics, burden of disease, healthcare use & costs in acute myeloid leukemia – a study with previously collected German Claims Data
What is this article about?
Acute myeloid leukemia (AML) is a type of cancer and the most frequent form of acute leukemia in adults. Treatments for AML include intensive chemotherapy and stem cell transplants, which help many patients go into remission, but relapses are common and the overall outlook remains poor. Only 14–32% of patients survive for 5 years after diagnosis.
Our study looked at the real-world impact of AML on patients in Germany, focusing on those who received intensive chemotherapy (IC) and those who did not (NIC). We used data from a German health insurance fund covering 3.5 million people from 2010 to 2022. We identified 1533 new AML patients who received treatment and divided them into IC and NIC groups based on their medication within 45 days after diagnosis. We excluded patients who did not receive treatment within that time period.
What were the results?
Most AML patients were at least once in the hospital. NIC patients were older and had more other health issues (‘comorbidities’) compared with IC patients. NIC patients spent less time in the hospital compared with IC patients. Hospital costs were almost half for NIC patients compared with IC patients. Blood transfusions were very common, especially among IC patients. In both groups, more than 90% of patients in received blood transfusions. Platelet transfusions were also frequent, with almost all IC patients and most NIC patients receiving them.
What do the results mean?
Our findings show that older AML patients often do not appear to get adequate treatment and have a high burden of disease. The high numbers of blood transfusions also indicate a high disease burden and highlight the need for better treatment options that are easier to tolerate.
Accounting for approximately 1% of all new cancer diagnoses, acute myeloid leukemia (AML) is the most common acute leukemia in adult patients, with previous studies reporting a median age of 63–71 years at incident diagnosis [1–4]. AML is a cancer beginning in cells in the bone marrow before commonly moving into the blood and other parts of the body. Characterized by a rapid growth, untreated AML patients typically die within months after diagnosis [3,5]. Treatment options for AML include either nonintensive therapies (NIC), such as hypomethylating agents, low dose chemotherapy or novel targeted therapies or intensive chemotherapy (IC), such as high dose cytarabine and an anthracycline, optionally with targeted inhibitors. Stem cell transplantation is also a potential option for patients eligible for IC. While remission rates are around 80% in IC patients, they remain low in NIC patients (37%) [6,7]. While IC-based treatment is the goal, around half of patients are not eligible to such intensive treatment due to age, comorbidities or other limiting factors such as patients’ overall health status or frailty. Real-world evidence (RWE) on disease epidemiology, patient characteristics, clinical outcomes and healthcare resource utilization (HCRU) and costs can provide crucial information to support and complement clinical research on treatments to lower the burden of disease and address unmet patient needs. Since RWE on AML patients and treatment is scarce, especially from Europe, this study aims at providing RWE on patient characteristics, disease burden, HCRU and costs in AML based on German claims data.
Materials & methods
This retrospective noninterventional cohort study uses claims data from the German sickness fund AOK PLUS. The data covers reimbursement codes from 2010 to 2022 for 3.5 million persons in the federal states of Saxony and Thuringia in central eastern Germany, representing around 4% of the total German population. Besides basic patient characteristics, the data include information on in- and outpatient diagnoses and procedures, outpatient prescriptions and costs. Due to the noninterventional, retrospective study design using anonymized data not focusing on any particular pharmacologic intervention, and in accordance with local laws and policies, patients’ informed consent was not required for this study. We identified AML patients based on the presence of at least one discharge inpatient or confirmed outpatient diagnosis codes (ICD-10 GM C92.00) in two consecutive quarters by specialists (oncology or hematology) between 1 January 2012 and 31 December 2022. To ensure incidence, a previous insurance period of 24 months without any AML diagnosis code (ICD-10 GM C92.0) was required. The earliest AML diagnosis date served as index date. Patients were followed up either for 1 year after index date or until earlier death or loss to follow-up, whichever occurred first. Depending on the treatment received within 45 days of index date, we stratified patients into having received IC or NIC (see Supplementary Table 1 for a list of treatments and corresponding codes used for this categorization). Patients with codes for both treatment types (NIC and IC) during follow-up were classified as IC patients. We excluded patients without any relevant treatment (as listed in Supplementary Table 1) from further analyses. Table 1 shows the inclusion and exclusion criteria applied in this study.
| Inclusion criteria | • ≥1 discharge inpatient and/or confirmed outpatient diagnosis codes (ICD-10-GM code: C92.00) in 2 consecutive quarters by specialists (oncology or hematology) between 1 January 2012 and 31 December 2022 • ≥2 years of continuous insurance before the first AML diagnosis • Any predefined AML treatment during follow-up |
| Exclusion criteria | • Any AML diagnosis code (ICD-10 GM: C92.0) prior 1 January 2012 • <2 years of continuous insurance before the first AML diagnosis • No predefined AML treatment during follow-up |
AML: Acute myeloid leukemia.
Based on the number of identified patients, we estimated the incidence rate (IR). We determined baseline characteristics such as age, gender, and the Charlson comorbidity index (CCI) at index date. We also assessed HCRU with regards to outpatient general practitioners and specialist (hematologist or oncologist) visits, all-cause and AML-related hospitalizations including length of stay (LOS), blood and platelet transfusions, the use of supportive care (defined as the placement of central venous catheters, antibacterial or antifungal treatment), and days absent from work. For the cost analyses, we looked at costs for hospitalizations (all-cause and AML-related), outpatient visits, prescriptions, combined other costs (including medical aids, remedies and inpatient rehabilitation costs), indirect costs estimated from days absent from work (all-cause and AML-related) and total costs.
All variables were analyzed descriptively and for each, the absolute number of patients or days, proportions, mean and standard deviation or median and (interquartile) range were assessed. Epidemiological estimates were reported per 100,000 persons per year, while HCRU and costs were reported per patient-year.
Results
From 2012 to 2022, we identified 1533 incident AML patients (47.1% female) with any listed treatment, corresponding to an annual IR of 4.4/100,000. A further 860 patients (mean age 74.2 years) were identified based on diagnosis codes but had no relevant treatment codes and were thus excluded from further analysis (Figure 1). Based on treatment codes between index date and 45 days later, we identified 688 IC and 845 NIC patients (Table 2). IC patients were markedly younger than NIC patients (mean age 57.8 vs 75.7 years, Table 2) and their CCI was lower (median score 4 vs 6, Table 2).
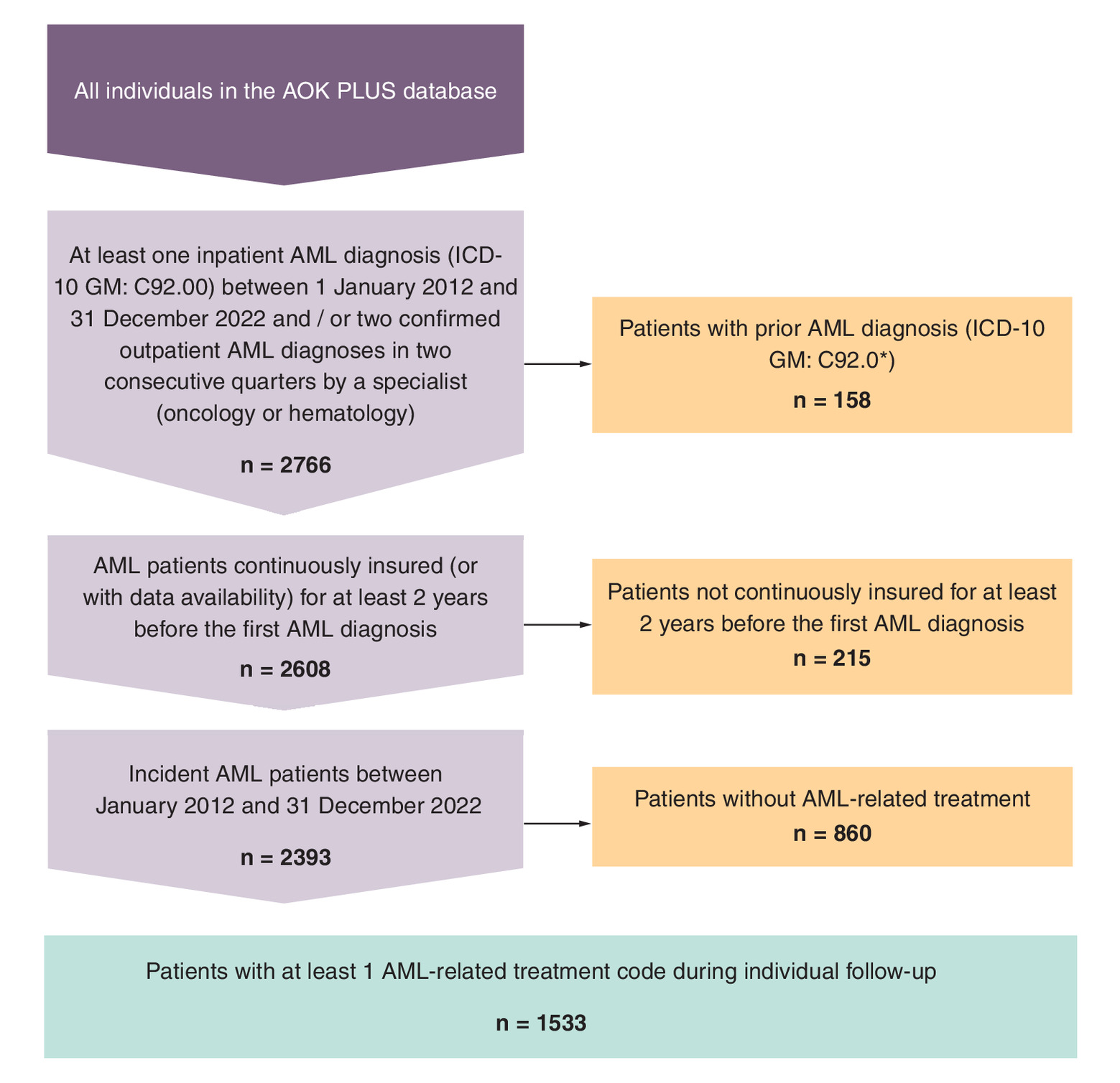
Figure 1. Attrition chart of the study population.
AML: Acute myeloid leukemia.
| Any treatment | Intensive chemotherapy | Nonintensive chemotherapy | |
|---|---|---|---|
| Total, n (%) | 1,533 (100.0%) | 688 (44.9%) | 845 (55.1%) |
| Gender, n (%) | |||
| Female | 722 (47.1%) | 348 (50.6%) | 374 (44.3%) |
| Male | 811 (52.9%) | 340 (49.4%) | 471 (55.7%) |
| Age (in years) | |||
| Mean (SD) | 67.7 (16.8) | 57.8 (17.8) | 75.7 (10.4) |
| Median (range) | 72.0 (0.0–98.0) | 61.0 (0.0–92.0) | 78.0 (5.0–98.0) |
| IQR | 60.0–79.0 | 51.0–70.0 | 72.0–82.0 |
| Charlson comorbidity index, points | |||
| Mean (SD) | 5.4 (2.8) | 4.8 (2.8) | 5.9 (2.7) |
| Median (range) | 5.0 (2.0–17.0) | 4.0 (2.0–16.0) | 6.0 (2.0–17.0) |
IQR: Interquartile range; SD: Standard deviation.
HCRU is shown in Table 3. Across all subgroups, more than 81% of patients had at least one AML-related hospitalization with a frequency per patient-year ranging from 4.7 (IC patients) to 5.3 (NIC patients). The mean LOS for AML-related hospitalizations was 103.1 days in IC and 64 days in NIC patients. Compared with IC patients, NIC patients had more outpatient visits per patient-year for general practitioners and specialists alike (NIC: 15.6 and 26.2; IC: 11.6 and 12.0). Most IC and NIC patients received at least one blood transfusion during follow-up (99.4 vs 93.0%), with 76.2% of IC patients having a diagnosis code for drug-induced anemia compared with 39.5% in NIC patients. 98.5% of IC patients and 74.3% of NIC patients received platelet transfusions. 33.3% of IC patients and 26.2% of NIC patients had a drug-induced thrombocytopenia. Supportive care was received by 99.0% (IC) and 81.5% (NIC) of patients. The proportion of patients with AML-related work absences was markedly higher in IC than NIC patients (40.0 vs 4.5%).
| Any treatment | Intensive chemotherapy | Nonintensive chemotherapy | |
|---|---|---|---|
| Total, n | 1533 | 688 | 845 |
| AML-related inpatient hospitalizations | |||
| Patients, n (%) | 1292 (84.3) | 605 (87.9) | 687 (81.3) |
| Frequency per patient-year | 5 | 4.7 | 5.3 |
| AML-related hospital LOS | |||
| Mean | 85.8 | 103.1 | 64 |
| All-cause GP visits | |||
| Frequency per patient-year | 13.4 | 11.6 | 15.6 |
| All-cause outpatient specialist visits | |||
| Frequency per patient-year | 18.3 | 12 | 26.2 |
| Blood transfusions | |||
| Patients, n (%) | 1470 (95.9) | 684 (99.4) | 786 (93.0) |
| Frequency per patient-year | 9.4 | 6.8 | 12.8 |
| Blood transfusions related to a drug-induced anemia diagnosis | |||
| Patients, n (%) | 858 (56.0) | 524 (76.2) | 334 (39.5) |
| Frequency per patient-year | 2.1 | 2.5 | 1.7 |
| Platelet transfusions | |||
| Patients, n (%) | 1,306 (85.2) | 678 (98.5) | 628 (74.3) |
| Frequency per patient-year | 4.4 | 4.6 | 4 |
| Platelet transfusions related to a drug-induced thrombocytopenia diagnosis | |||
| Patients, n (%) | 450 (29.4) | 229 (33.3) | 221 (26.2) |
| Frequency per patient-year | 1.1 | 1.1 | 1.1 |
| Supportive care | |||
| Patients, n (%) | 1370 (89.4) | 681 (99.0) | 689 (81.5) |
| Frequency per patient-year | 12.4 | 12.9 | 11.9 |
| AML-related days absent from work (days per patient-year) | |||
| Patients, n (%) | 313 (20.4) | 275 (40.0) | 38 (4.5) |
| Frequency per patient-year | 87.3 | 140.4 | 20.1 |
AML: Acute myeloid leukemia; GP: General practitioner; LOS: Length of stay.
Table 4 shows costs per patient-year by patient subgroups. Patient subgroups differed with regard to the absolute amount of total costs per patient-year (IC: €202,233; NIC: €132,126) as well as the distribution of costs. In IC patients, highest costs occurred due to AML-related hospitalizations (54.5%), AML-related work absences (13.1%) and outpatient prescriptions (10.3%). In NIC patients, AML-related hospitalizations, prescriptions and AML-related work absences accounted for 42.4%, 30.7% and 2.8% of total costs, respectively.
| Costs in EUR per PY (% of total costs) | Any treatment | Intensive chemotherapy | Nonintensive chemotherapy |
|---|---|---|---|
| All-cause inpatient hospitalizations | 122,532 (71.5) | 152,207 (75.3) | 84,939 (64.3) |
| AML-related inpatient hospitalizations | 86,310 (50.4) | 110,186 (54.5) | 56,063 (42.4) |
| All-cause outpatient visits | 846(0.5) | 866 (0.4) | 821 (0.6) |
| Outpatient prescriptions | 29,605 (17.3) | 20,920 (10.3) | 40,607 (30.7) |
| Other costs (including medical aids, remedies, inpatient rehabilitation) | 1887 (1.1) | 1527 (0.8) | 1848 (1.4) |
| Indirect costs of all-cause days absent from work | 16,654 (9.7) | 26,713 (13.2) | 3910 (3.0) |
| Indirect costs of AML-related days absent from work | 16,436 (9.6) | 26,449 (13.1) | 3750 (2.8) |
| Total all-cause costs | 171,305 (100.0) | 202,233 (100.0) | 132,126 (100.0) |
AML: Acute myeloid leukemia.
Discussion
This retrospective real-world data study based on German claims data explored patient characteristics, burden of disease, HCRU and costs of AML patients stratified by treatment groups. While this study was based on data from 3.5 million people insured with one statutory health insurance (SHI) provider, the data are considered representative of the German population. Almost 90% of the German population are insured with a SHI, and German healthcare services and costs are widely determined by nationwide regulations [8–10]. Additionally, insurance is irrespective of employment status and is also granted to pensioners, students and children [10]. Incident rates found in this study were comparable to other real-world data studies, reporting IRs from 4.2 to 9.0/100,000 in different healthcare settings and databases [2,11].
A descriptive comparison of AML patients with IC and NIC treatment showed differences in baseline characteristics, HCRU and costs. NIC patients made up more than half of the patient population in our study. Together with previous European real-world studies reporting 28.6–62.0% of patients receiving IC [11–13], this shows that – despite being associated with poorer remission rates [6,7] – a considerable proportion of patients received NIC instead of IC.
We also found a large proportion of patients with an AML diagnosis who did not receive any predefined AML treatment, corroborating findings from other European and world-wide real-world data studies [12,14–20]. Compared with two studies from the US, in which Meyers et al. [19] and Katz et al. [20] report 57.1% and 58.2% of patients treated with supportive care only, the percentage of patients receiving no predefined AML treatment in this study is smaller (35.9%). However, focusing on patients qualifying for Medicare via their older age, the patient population analyzed by Meyers et al. was distinctively older than in the present study [19]. Another important factor possibly explaining the observed difference is the observation period which ranged from 1997 to 2007 [19] and 2000 to 2003 [20], respectively, compared with 2012 to 2022 in our study. The study period playing an important role in the proportion of patients without treatment is underlined by the findings from Hagiwara et al. [21]. They found that 32.2% of patients diagnosed between 2007 and 2016 did not receive AML treatment [21]. Patients without cancer treatment were often older or had a higher burden of comorbidities compared with treated patients [12,14–21]. Combined with the older age of NIC compared with IC patients, this underlines the need of adequate treatment for patients of older age and/or high comorbidity burden. Note that the participation in clinical trials or a short follow-up ending before treatment initiation might have further increased the number of patients without claims for treatment [22].
We observed a high share of patients having received blood or platelet transfusions. Although we did not find diagnosis codes for drug-induced anemia or thrombocytopenia in all of these patients, it is very likely that, even in the absence of these diagnosis codes (diagnoses may not always have been coded), patients with transfusions suffered either from anemia or thrombocytopenia highlighting the burden of disease. Previous studies report proportions of blood or platelet transfusions among AML patients from 10.8 to 91.5%, depending on treatment subgroup and phase, but generally do not differentiate by the underlying reason for transfusion.
The rather long LOS found in our study is supported by reported numbers from other studies [12,18,23] and emphasizes the high burden of disease and treatment, especially in IC patients. This is further supported by the high proportion of IC patients with supportive care. Assuming that IC patients received transfusions more often in the inpatient sector, the higher share of IC patients receiving a transfusion might partly explain the longer LOS found in these patients.
The NIC patients in our population were markedly older compared with IC patients and had a higher comorbidity burden. This finding is supported by previous studies and corresponds to recommendations of medical guidelines [11,12,22–24]. Several estimates, such as the lower hospitalization frequency, the higher number of outpatient visits and almost doubled outpatient prescription costs, all compared with IC patients, indicate a higher importance of the outpatient sector in the treatment of NIC patients. While this overall finding is consistent with findings from the US [25], no previous study looked directly at prescription costs. Despite prescription costs being higher in NIC patients in our study, total direct and indirect costs were higher for IC patients. These higher total costs were mainly driven by AML-related hospitalization costs and costs emerging from AML-related work absences. Hospitalizations as the biggest cost factor were also observed in other studies [18,19,23,26] as well were higher hospitalization costs for patients receiving more intense treatment. Higher costs for work-absences in IC patients are likely due to their younger age and, consequently, a higher proportion of patients within working age compared with NIC patients.
This study has several limitations. First, our study uses secondary, administrative data that is not collected for research purposes nor the specific objectives of this study. Thus, data do not include important clinical variables, such as tumor stage or genetic subtype of the tumor as well as laboratory values in general. Missing information due to coding errors might also occur. However, since the data is collected for reimbursement processes and eventually quality-checked by the payers, the coding of SHI-based databases is generally considered to be of high quality and they are commonly used for epidemiology and HCRU studies in the German population. Missing data due to out-of-pocket transactions are generally not considered to bias the information available in German claims data, as those transactions are limited to small copayments (not more than 10 EUR) and over-the-counter drugs. The SHI providing the data for this study covers mainly patients in the central eastern parts of Germany, bearing the risk of selection bias. However, as discussed above, given the uniform nationwide healthcare regulations, as well as data entry requirements and access to healthcare resources, the results found in this study are not expected to significantly differ from those of other patients in Germany. The purely descriptive study design limits statistical comparisons between the patient groups. However, baseline heterogeneity in patient groups could be adjusted for using methods such as propensity score balancing, allowing for a more valid comparative analysis. The a priori definition of relevant treatments bears the risk of missing off-label treatments or procedures. This was addressed by consulting the contemporaneous medical guidelines instead of relying only on regulatory-approved indications.
Future research either employing more advanced statistical methods to control for the heterogeneity of patient groups or using more detailed information on disease severity, mutation subtype or cytogenic risk could enhance the conclusions drawn from the results of this study. The observed burden of disease, especially in IC patients, the differential use of healthcare sectors across the patient groups, and the substantial proportion of patients who remained untreated provide valuable insights and can inform future research. For example, future studies could explore the underlying factors driving treatment decisions, and assessing how these influence clinical outcomes and HCRU. The large proportion of patients without treatment highlights a potentially underserved population, and underlines the need of further investigation. Further studies using more recent data and focusing on newer treatment options that have become available in recent years could help to better understand the evolving treatment landscape of AML and its implications for HCRU.
Conclusion
In this retrospective claims data study investigating patient characteristics, disease burden, HCRU and costs of patients with AML, we found that NIC patients were markedly older, had a higher comorbidity burden, and were less often hospitalized compared with IC patients. Additionally, a high number of older patients did not receive any study-relevant AML treatment, indicating a lack of adequate treatment options in this patient population. Across all treatment subgroups, but especially in IC patients, we observed high rates of blood and platelet transfusions as well as supportive care utilization, indicating a high burden of disease and further emphasizing the need for better-tolerated therapies. While overall costs were higher in IC patients, mainly driven by hospitalization costs and indirect costs from work absences, prescription costs were almost doubled in NIC patients, highlighting the importance of the outpatient sector in the treatment of these patients.
Summary points
•
Acute myeloid leukemia (AML) is the most frequent acute leukemia in adults.
•
While patients who are not treated die within months after diagnosis, remissions rates range from ∼40% in patients treated with nonintensive therapy (NIC) to 80% in patients treated with intensive therapy (IC).
•
This retrospective observational cohort study used 2010–2022 claims data from a German sickness fund.
•
We identified 1533 incident AML patients of which 45% received IC and 55% received NIC.
•
NIC patients were older and had more comorbidities compared with IC patients, potentially showing a need for effective treatment options in these patient populations.
•
Blood and platelet transfusions were very common across all patients but even more prominent in IC patients, indicating a high burden of treatment and emphasizing the need for well tolerable treatment options.
Author contributions
K Greth, M Lehne, M Ghiani, M Gokhale and A Russell were responsible for study design; M Gokhale, A Russell, S Purcell and S Kaulfuss were responsible for study conception; A Mevius was responsible for acquisition of data; K Greth and M Lehne were responsible for data analysis, and drafting and revision of the manuscript; M Gokhale, A Mevius, A Russell, S Purcell, S Kaulfuss and M Ghiani critically reviewed the manuscript; all authors provided final approval of the version submitted and agreed to be accountable for all aspects of the work.
Financial disclosure
The development of this publication including the underlying study was supported financially by Pfizer Inc. including the work of Cytel Inc.
Competing interests disclosure
K Greth, M Lehne and M Ghiani are employees of Cytel Inc., a research consultancy receiving funding from various pharmaceutical companies. A Mevius is employee of IPAM e.V., a scientific institute receiving financial compensation for its studies. S Purcell, S Kaulfuss, M Gokhale and A Russell are employees of Pfizer Inc. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Due to the non interventional, retrospective study design using anonymized data not focusing on any particular pharmacologic intervention, and in accordance with local laws and policies, patients' informed consent was not required for this study. The study was approved by the responsible authority, the data owner AOK PLUS.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 33.70 KB
References
Papers of special note have been highlighted as: • of interest
1.
De Kouchkovsky I, Abdul-Hay M. Acute myeloid leukemia: a comprehensive review and 2016 update. Blood Cancer J. 6(7), e441 (2016).
2.
SEER Cancer Stat Facts: Acute Myeloid Leukemia. National Cancer Institute, MD, USA, Available from: https://seer.cancer.gov/statfacts/html/amyl.html
3.
Dharmani C, Wang E, Tu N et al. Elderly patients with acute myeloid leukemia who only receive supportive care in the Surveillance, Epidemiology and End Results-Medicare database: demographics, treatment patterns and outcomes. Future Oncol. (London, England) 19(24), 1677–1693 (2023).
4.
Estey EH. Acute myeloid leukemia: 2019 update on risk-stratification and management. Am. J. Hematol. 93(10), 1267–1291 (2018).
• A thorough discussion of treatment options for acute myeloid leukemia (AML).
5.
The American Cancer Society medical and editorial content team. What is acute myeloid leukemia (AML)? (2018). (updated 21 August 2018). Available from: https://www.cancer.org/cancer/types/acute-myeloid-leukemia/about/what-is-aml.html
6.
Castaigne S, Pautas C, Terré C et al. Effect of gemtuzumab ozogamicin on survival of adult patients with de-novo acute myeloid leukaemia (ALFA-0701): a randomised, open-label, Phase III study. Lancet 379(9825), 1508–1516 (2012).
7.
DiNardo CD, Jonas BA, Pullarkat V et al. Azacitidine and venetoclax in previously untreated acute myeloid leukemia. N. Engl. J. Med. 383(7), 617–629 (2020).
8.
GKV Spitzenverband. Krankenversicherung. (2025).
9.
Bundesministerium für Gesundheit. Aufgaben und organisation der gesetzlichen Krankenversicherung. (2025). (updated 10 June). Available from: https://www.bundesgesundheitsministerium.de/themen/krankenversicherung/grundprinzipien/aufgaben-und-organisation-der-gkv.html
10.
Bundesministerium für Gesundheit. Daten des Gesundheitswesens 2022. (2022).
11.
Calabria S, Ronconi G, Dondi L et al. Acute myeloid leukemia: incidence, transplantation and survival through Italian administrative healthcare data. Tumori 109(5), 496–503 (2023).
• This real-world study shows a comprehensive overview of AML treatment in Italy, helping to improve treatment strategies especially in older AML patients.
12.
Sutter T, Schittenhelm M, Volken T, Lehmann T. Treatment regimens in patients over 64 years with acute myeloid leukaemia: a retrospective single-institution, multi-site analysis. Hematology 28(1), 2206694 (2023).
13.
Juliusson G, Antunovic P, Derolf A et al. Age and acute myeloid leukemia: real world data on decision to treat and outcomes from the Swedish Acute Leukemia Registry. Blood 113(18), 4179–4187 (2009).
14.
Dharmani C, Wang E, Tu N, Salas M, Kamel YM. Characteristics and outcomes of elderly patients with acute myeloid leukemia who receive no treatment in the Surveillance, Epidemiology and End Results-Medicare database. Future Oncol. (London, England) 19(2), 159–171 (2023).
15.
Bang SM, Kang KW, Song IC et al. Real-world treatment patterns and clinical outcomes in korean patients with AML ineligible for first-line intensive chemotherapy: a subanalysis of the current study, a non-interventional, retrospective chart review. J. Korean Med. Sci. 38(44), e345 (2023).
• The poor clinical outcomes in Korean AML patients without IC treatment show the high unmet need for novel agents.
16.
Hubscher E, Sikirica S, Bell T et al. Patterns of undertreatment among patients with acute myeloid leukemia (AML): considerations for patients eligible for non-intensive chemotherapy (NIC). J. Cancer Res. Clin. Oncol. 147(11), 3359–3368 (2021).
17.
Miyamoto T, Sanford D, Tomuleasa C et al. Real-world treatment patterns and clinical outcomes in patients with AML unfit for first-line intensive chemotherapy. Leukemia Lymphoma 63(4), 928–938 (2022).
18.
Bell JA, Galaznik A, Farrelly E et al. Economic burden of elderly patients with acute myeloid leukemia treated in routine clinical care in the United States. Leukemia Res. 71, 27–33 (2018).
19.
Meyers J, Yu Y, Kaye JA, Davis KL. Medicare fee-for-service enrollees with primary acute myeloid leukemia: an analysis of treatment patterns, survival, and healthcare resource utilization and costs. Appl. Health Econ. Health Policy 11(3), 275–286 (2013).
20.
Katz LM, Howell JB, Doyle JJ et al. Outcomes and charges of elderly patients with acute myeloid leukemia. Am. J. Hematol. 81(11), 850–857 (2006).
21.
Hagiwara M, Sharma A, Chung KC, Delea TE. Healthcare resource utilization and costs in patients with newly diagnosed acute myeloid leukemia. J. Med. Econ. 21(11), 1119–1130 (2018).
22.
Röllig C, Ayuk FA, Braess J et al. Akute myeloische leukämie (AML). (2022).
23.
Brunner AM, Huggar D, Copher R et al. Economic burden during remission and after relapse among older patients with newly diagnosed acute myeloid leukemia without hematopoietic stem cell transplant: a retrospective study using the SEER-Medicare database. Leukemia Res. 132, 107353 (2023).
• Based on SEER data, this study shows that effective treatments initiating remission in AML patients may substantially reduce the economic burden of the disease.
24.
Heuser M, Ofran Y, Boissel N et al. Acute myeloid leukaemia in adult patients: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 31(6), 697–712 (2020).
25.
Gershon A, Ma E, Xu T et al. Early real-world first-line treatment with venetoclax plus HMAs versus HMA monotherapy among patients with AML in a predominately US community setting. Clin. Lymphoma Myeloma Leuk. 23(5), e222–e231 (2023).
26.
Pandya BJ, Chen CC, Medeiros BC et al. Economic and clinical burden of acute myeloid leukemia episodes of care in the United States: a retrospective analysis of a commercial payer database. J. Manag. Care Spec. Pharm. 26(7), 849–859 (2020).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 21 October 2024
Accepted: 23 October 2025
Published online: 28 November 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Patient characteristics, burden of disease, healthcare resource utilization and costs in acute myeloid leukemia – a retrospective observational study with German claims data. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0196
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mary M. Mikhail, Hanan B. Ahmed, Mahmoud El-Shahat, Hossam E. Emam, Thiophene- and pyrrole-derived heterocyclic carbon quantum dots for biomedical applications, Journal of Molecular Structure, 10.1016/j.molstruc.2026.146745, 1374, (146745), (2026).
- Amer M. Zeidan, Ruizhi Zhao, Dina Christensen, Janan Amin, Thomas W. LeBlanc, The burden of acute myeloid leukemia: an integrated review of clinical, economic, and patient-centered evidence, Expert Review of Anticancer Therapy, 10.1080/14737140.2026.2705531, (2026).