Cost–effectiveness of lung cancer screening with volume computed tomography in Portugal
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Lung cancer is the most common cause of cancer death in Portugal. The Dutch–Belgian lung cancer screening (LCS) study (NELSON), the biggest European LCS study, showed a lung cancer mortality reduction in a high-risk population when being screened. In this study, the cost–effectiveness of LCS, based on the NELSON study protocol and outcomes, was evaluated compared with no screening in Portugal. Methods: The present study modified an established decision tree by incorporating a state-transition Markov model to evaluate the health-related advantages and economic implications of low-dose computed tomography (LDCT) LCS from the healthcare standpoint in Portugal. The analysis compared screening versus no screening for a high-risk population aged 50–75 with a smoking history. Various metrics, including clinical outcomes, costs, quality-adjusted life years (QALYs), life-years (LYs) and the incremental cost–effectiveness ratio (ICER), were calculated to measure the impact of LDCT LCS. Furthermore, scenario and sensitivity analyses were executed to assess the robustness of the obtained results. Results: Annual LCS with volume-based LDCT resulted in €558 million additional costs and 86,678 additional QALYs resulting in an ICER of €6440 per QALY for one screening group and a lifetime horizon. In total, 13,217 premature lung cancer deaths could be averted, leading to 1.41 additional QALYs gained per individual diagnosed with lung cancer. Results are robust based on the sensitivity analyses. Conclusion: This study showed that annual LDCT LCS for a high-risk population could be cost-effective in Portugal based on a willingness to pay a threshold of one-time the GDP (€19,290 per QALY gained).
Plain language summary
What is this article about?
Various lung cancer screening (LCS) studies have been performed or are currently being performed worldwide. The two biggest LCS studies so far demonstrated that LCS in a high-risk group was able to lower the lung cancer mortality rate. In Portugal, no LCS study or pilot program has started yet. Therefore, this cost–effectiveness analysis could help with the implementation of an LCS pilot in Portugal. The outcomes of this study focus on the economic and clinical aspects of an annual LCS program in Portugal compared with the current situation with no screening program.
What were the results?
LCS, based on the NELSON study protocol and outcomes, improves the clinical outcomes of lung cancer patients while the extra costs are acceptable making it a cost-effective intervention compared with no screening. The incremental cost–effectiveness ratio (ICER) was €6440 per QALY gained at a willingness to pay threshold of one-time the GDP (€19,290).
What do the results mean?
These findings indicate that LCS in Portugal could potentially be a preferred option for diagnosing lung cancer patients compared with the current clinical pathway. The results provide decision-makers with information to consider launching an LCS pilot study to develop the most optimal LCS program in Portugal.
Globally, lung cancer imposes a major disease burden as it is the second most diagnosed cancer and the leading cause of cancer death in 2022, with 2.5 million new lung cancer cases and 1.8 million deaths, representing 18.7% of all cancer deaths [1]. In Portugal, lung cancer is the fourth most diagnosed cancer type and the main cause of cancer death in men and women combined in 2022 [1]. The economic impact attributed to non-small-cell lung cancer (NSCLC) is of considerable magnitude, amounting to €143 million in 2012. This represents approximately 0.09% of the Portuguese Gross Domestic Product (GDP) and 0.92% of the total healthcare expenditures in Portugal during the same year [2]. In recent years, the lung cancer treatment pathway for mainly late-stage lung cancer patients has changed with the introduction of immunotherapies and targeted therapies. These innovative medicines enhance both quality of life and survival rates of cancer patients however, they also contribute to rising healthcare costs [3].
Lung cancer is diagnosed in more than 75% of the cases in an advanced stage due to the late clinical appearance of symptoms [4,5]. Additionally, the late detection of lung cancer explains the high mortality rate for lung cancer patients [6]. In the last decades, minor improvement in lung cancer survival was established compared with other cancer types, such as breast cancer. However, early lung cancer detection would lower the mortality rates as the survival rates for early detected lung cancers are higher [7]. The five-year survival rate for stage I and II Portuguese patients lies between 36.9 and 59.8% and between 2.0 and 11.9% for stage III and IV patients [8].
The main risk factor for developing lung cancer is tobacco smoking, with 80% of the cases being attributed to smoking [9]. Multiple trials demonstrated that screening high-risk lung cancer patients based on their smoking history was able to detect lung cancer in an early stage and was able to reduce the mortality rate. The two biggest lung cancer screening (LCS) trials that were performed were the National Lung Cancer Screening Trial (NLST) and the Dutch–Belgian LCS trial (NELSON) [10,11]. The NLST demonstrated that baseline screening with low-dose computed tomography (LDCT) for high-risk individuals was able to detect 58.3% of the cancer cases in stage I and 15.4% in stage IV. Additionally, a mortality reduction of 20% was achieved with LDCT screening compared with x-ray-based screening after a 6.5-year follow-up [11]. Similar results were found in the NELSON trial for early-stage detection as 64.9% of the lung cancer cases were detected in stage I and 6.8% of the cases in stage IV. Moreover, a mortality reduction of 24 and 33% were observed for men and females, respectively, after a 10-year follow-up [10]. The biggest difference in the results was the number of false-positive cases which were 1.2 and 23% for the NELSON and NLST studies, respectively [10,11]. The higher false-positive rate in the NLST was due to a different stratification approach (classifying nodules into positive, negative and indeterminates). Additionally, in the NLST a diameter nodule measurement approach was chosen compared with a volumetric doubling time approach in the NELSON study [11].
Recently, many LCS projects in Europe are starting either as individual pilots, as research programs (e.g., 4-ITLR in The Netherlands, Spain, France, Germany and Italy), or as national programs (Croatia, Poland, UK) [12,13]. In December 2022, the Portuguese Minister of Health announced that there will be an extension of the cancer screening program to lung, prostate and stomach cancer, which will start in 2023 with pilot projects following the EU cancer beating plan [14,15].
So far, the cost–effectiveness of LCS in Portugal has not been investigated yet. This study aims to inform policymakers by assessing the costs and health impact together with the cost–effectiveness and clinical effects of implementing LDCT LCS according to the NELSON protocol (volume-based) in Portugal. For this study, we adapted the existing model for the UK, which investigated the cost–effectiveness of LCS with volume-based LDCT with no screening [16].
Methods
This study used the established CEA model designed to assess the cost–effectiveness of LCS in the UK [16]. The UK model, which integrates a decision tree and a Markov model, is well-validated and robust for lung cancer screening assessment, making it suitable for our study. Furthermore, our study utilized this established framework to assess local variables in Portugal, enabling reliable conclusions while facilitating comparisons with UK and European studies [16,17]. Detailed descriptions regarding the model structure and assumptions have been previously provided in the study [16]. Hence, the structure is briefly discussed in this study. The methodological adjustments to the model as well as the variations in input parameters from the Portuguese model will be discussed.
In the CEA, the total costs, life years (LYs) and quality-adjusted life years (QALYs) were evaluated to determine the incremental cost–effectiveness ratio (ICER) which was calculated by dividing the incremental costs by the incremental QALYs. The net monetary benefit (NMB) was calculated to determine the cost–effectiveness of LCS at the specified WTP threshold. The NMB was obtained by multiplying the WTP threshold by the incremental QALYs and then subtracting the incremental costs. The costs were segmented into recruitment, screening, diagnostic and treatment costs. There is no generally recommended willingness-to-pay (WTP) threshold for screening interventions in Portugal. The WTP represents the maximum amount a decision-maker is willing to spend to gain additional QALYs. As there is no official WTP threshold in Portugal, a WTP of one-time the GDP per capita for the base-case analysis was chosen, which is in line with the recommendations of the World Health Organization recommending a WTP of one to three-times the GDP per capita [18]. The 2022 GDP per capita in Portugal was €19,290 and therefore taken as the WTP [19]. The cost–effectiveness of LCS with the volume-based low-dose CT was assessed using the Portuguese guidelines for health technology assessments [20]. Therefore, the study took the payer perspective and a 4% discount rate was used for both the health effects and costs [20]. The costs were inflated to the year 2022 and expressed in euros [20,21].
Model structure
A decision tree was built to simulate the screening and diagnostic pathway for lung cancer patients in a screening scenario and a no screening scenario (current clinical pathway). For the screening arm, eligible individuals either participated in the screening program or did not participate. Participants receiving a negative screening result were subjected to an annual screening strategy that included 17 screening rounds corresponding to the mean age of NELSON study participants (58 years) and with a maximum age criterion of 74 years. Individuals in the no screening arm and individuals not participating in the screening program were diagnosed via clinical care. Additionally, in the no screening arm, a branch of missed individuals was included and assumed to be asymptomatic patients in the pre-clinical disease stage. To simulate long-term survival and costs, all lung cancer patients entered a state-transition Markov model. Patients could transition from a pre-progression state to either a post-progression state or a death state (lung cancer death or background mortality) in the Markov trace. The cycle length of three months was chosen as it reflects the typical course of treatment for individuals with lung cancer [22].
Model inputs
The model inputs are described below, and all parameters used in the base-case analysis of the CEA are presented in Table 1. Local data was used when available to correctly depict the Portuguese situation. International data and other European sources were used when local data was not available.
| Parameter | Base-case value | PSA distribution | Ref. | |
|---|---|---|---|---|
| Discount rate for costs | 4% | Fixed | [20] | |
| Discount rate for health outcomes | 4% | Fixed | [20] | |
| Time horizon | Lifetime (42 years) | Fixed | ||
| Screening outcomes | ||||
| NELSON round 1 | ||||
| Regular scan | Negative | 79.21% | Dirichlet | [23] |
| Indeterminate | 19.20% | Dirichlet | [23] | |
| Positive | 1.59% | Dirichlet | [23] | |
| Indeterminate scan | Negative | 94.57% | Dirichlet | [23] |
| Positive | 5.43% | Dirichlet | [23] | |
| True negative | 99.93% | Dirichlet | [23] | |
| False negative | 0.07% | Dirichlet | [23] | |
| True positive | 38.67% | Dirichlet | [23] | |
| False positive | 61.33% | Dirichlet | [23] | |
| Stage distribution | ||||
| Stage I | 64.86% | Dirichlet | [24] | |
| Stage II | 9.46% | Dirichlet | [24] | |
| Stage III | 18.92% | Dirichlet | [24] | |
| Stage IV | 6.76% | Dirichlet | [24] | |
| NELSON round 2 | ||||
| Regular scan | Negative | 92.17% | Dirichlet | [23] |
| Indeterminate | 6.58% | Dirichlet | [23] | |
| Positive | 1.25% | Dirichlet | [23] | |
| Indeterminate scan | Negative | 91.23% | Dirichlet | [23] |
| Positive | 8.77% | Dirichlet | [23] | |
| True negative | 99.73% | Dirichlet | [23] | |
| False negative | 0.27% | Dirichlet | [23] | |
| True positive† | 44.35% | Dirichlet | [23] | |
| False positive† | 55.65% | Dirichlet | [23] | |
| Stage distribution | ||||
| Stage I | 75.86% | Dirichlet | [24] | |
| Stage II | 6.90% | Dirichlet | [24] | |
| Stage III | 13.79% | Dirichlet | [24] | |
| Stage IV | 3.45% | Dirichlet | [24] | |
| Mean age NELSON study | 58.00 | Fixed | [23] | |
| Screening uptake rate | 60% | Beta | [25] | |
| Epidemiology and demography | ||||
| Stage distribution (no screening) | ||||
| Stage I | 13.2% | Dirichlet | [26] | |
| Stage II | 4.8% | Dirichlet | [26] | |
| Stage III | 23.6% | Dirichlet | [26] | |
| Stage IV | 58.4% | Dirichlet | [26] | |
| Total population | 10,196,707 | Fixed | [27] | |
| Population aged 50–74 years | 32.5% | Beta | [28] | |
| Lung cancer incidence aged 50–74 years | 0.46% | Beta | [29] | |
| Smoking rate | 17.2% | Beta | [30] | |
| Costs | ||||
| Screening costs | ||||
| CT-scan | € 74.7 | Gamma | [31] | |
| Diagnostic costs per person | ||||
| Screening | € 654.7 | Gamma | [31,32] | |
| No screening | € 327.0 | Gamma | [31,32] | |
| Treatment costs | ||||
| First year – per cycle | ||||
| Stage I | € 2491 | Gamma | [33] | |
| Stage II | € 3837 | Gamma | [33] | |
| Stage III | € 3452 | Gamma | [33] | |
| Stage IV | € 4567 | Gamma | [33] | |
| Second year – per cycle | ||||
| Stage I | € 733 | Gamma | [33] | |
| Stage II | € 2439 | Gamma | [33] | |
| Stage III | € 3359 | Gamma | [33] | |
| Stage IV | € 8362 | Gamma | [33] | |
| Average end-of-life costs per patient | € 6824 | Gamma | [34–37] | |
| Utilities | ||||
| Pre-progression state | ||||
| Stage I | 0.78 | Beta | [38] | |
| Stage II | 0.78 | Beta | [38] | |
| Stage III | 0.69 | Beta | [38] | |
| Stage IV | 0.69 | Beta | [38] | |
| Post-progression state | ||||
| Stage I | 0.69 | Beta | [38] | |
| Stage II | 0.69 | Beta | [38] | |
| Stage III | 0.69 | Beta | [38] | |
| Stage IV | 0.69 | Beta | [38] | |
| Lung cancer free participants | ||||
| Age-dependent utility values | ||||
| 50–69 | 0.868 | Beta | [39] | |
| 70+ | 0.790 | Beta | [39] | |
| Survival | ||||
| Overall survival (5-year survival rate) | ||||
| Stage I | 54.83% | NA | [40,41] | |
| Stage II | 24.86 | NA | [40,41] | |
| Stage III | 14.70% | NA | [40–42] | |
| Stage IV | 3.77% | NA | [40,42] | |
| Disease/progression-free survival (1-year disease/progression-free survival rate) | ||||
| Stage I | 87.80% | NA | [43] | |
| Stage II | 75.79% | NA | [44] | |
| Stage III | 48.92% | NA | [45] | |
| Stage IV | 37.60% | NA | [46–48] | |
| Background mortality | ||||
| Life expectancy by age | General population | Beta | [49] | |
†
True positive refers to the proportion of true positive scans among the total of positive results, while false positive refers to the proportion of false-positive scans among the total of positive results, the sum of them equals to 100.
NA: Not applicable; PSA: Probabilistic sensitivity analysis.
Eligible population
High-risk lung cancer individuals were identified based on the NELSON study age criteria (50–74 years) and smoking rate. The eligible Portuguese population based on only the age criteria was 3,313,821 [27,28]. The percentage of daily smokers in Portugal was 17.2% [30], resulting in an eligible population of 570,143 individuals. The final population cohort was determined by considering a screening uptake rate of 60% similar to the breast cancer screening uptake in Portugal [25]. Thus, the total number of screening participants was 342,086.
Epidemiological & screening inputs
To populate the screening arm for the LCS participants the NELSON screening outcomes were used [16,24.23]. The lung cancer incidence in the age category 50–74 [29], and the stage distribution at the time of diagnosis were used to populate the no screening arm and the branch of the non-participants in the screening arm to calculate the number of diagnosed lung cancer individuals. The stage distribution was obtained from a study retrieving data from all population-based cancer registries in Portugal [26].
Survival
Disease-free survival (DFS) rates and progression-free survival (PFS) rates were used to determine the transition probabilities for lung cancer patients going from the pre-progression to the post-progression health state in the Markov trace. DFS and PFS curves were extrapolated based on international clinical trials since such curves were not available for Portuguese lung cancer patients [43–48]. The overall survival (OS) of NSCLC and SCLC patients per stage was provided by retrospective analysis studies [40–42] and was utilized to guide the model's transition from the pre-and post-progression to death state. All analyses utilized the database held by the Portuguese Oncology Institute of Porto, Portugal's largest cancer hospital [50]. Firstly, the database was used to describe treatment patterns and OS among Portuguese SCLC patients, between January 2012 and June 2017, with follow-up to December 2017 [40]. A total of 227 patients were diagnosed with SCLC and were further stratified into subgroups with limited disease (LD) or extensive disease (ED) (37 LD; 190 ED) [40]. Additionally, the stage distribution for early-stage NSCLC was also derived from the same database. For the analysis, 495 patients were included who were diagnosed during the period 2012–2016, with a follow-up until June 2017 [41]. For advanced NSCLC, the study identified 1008 patients with advanced disease, between 2012 and 2016 [42]. The distribution of NSCLCs and SCLCs was taken into consideration when calculating the survival with 85% of the cancers being classified as NSCLC and 15% as SCLC [51]. The model accounted for all-cause mortality using background mortality, which was based on Portuguese national life tables for the years 2019–2021, this lifetable does not take into account the increased mortality due to COVID-19 [49].
All survival data was extrapolated for a lifetime horizon according to the NICE guidelines and Guyot methodology [52,53]. The parametric distributions and their corresponding parameters are listed in the supplementary files (Supplementary Table 1).
Costs
In Portugal, the NHS perspective is the recommended method for evaluating health technology, with only direct costs included in the analysis [20]. The direct costs included recruitment, screening, diagnosis and treatment expenditures.
The recruitment strategy followed the Yorkshire Lung Cancer Screening Trial (YLST) which according to local experts would be the most likely scenario for Portugal to follow [54]. The recruitment strategy included sending invitation letters and a telephone triage call to check whether the individuals would match the eligibility criteria, and the costs were obtained from the Portuguese cervical cancer screening program [55]. Details for recruitment costs are presented in Supplementary Table 2. The screening costs were determined by the cost of a CT, which was obtained by the Portuguese NHS tariffs 2018 published by the Central Administration of the Health System (ACSS) [31].
The diagnostic costs were obtained by the NHS and were applied to screening participants who had a positive or false-positive CT scan result and those who had symptoms suggestive of lung cancer (diagnosed outside a screening program). The NELSON trial served as the foundation for the diagnostic pathway and utilization numbers for each diagnostic procedure, while the Portuguese NHS tariffs 2018 provided the costs for the diagnostic services [23,31,32]. The weighted diagnosis for each individual was determined using the costs and utilization numbers for each procedure (Supplementary Table 3). Extra diagnostic costs were applied to individuals in the no-screening arm as they did not participate in the screening. The costs for this group encompass the diagnostic process from the time they first experience symptoms until they receive the first hospital consultation. The extra cost is defined as the consultation fee from the physician [32].
The treatment costs per stage were calculated based on the treatment pathway and utilization values from the FAROL study [33]. Specifically, the treatment pathway included pharmacological treatment, radiotherapy, surgery, hospitalization and medical appointments, excluding the cost of diagnostic tests. In their analysis, the expenditures were determined for 358 individuals diagnosed with lung cancer between July 2016 and June 2017 with a two-year follow-up period. For the new post-progression patients three monthly first-year costs were one-time applied after year 3. Thus, stage I and II new post-progression patients received one-time the stage III treatment costs and stage III and IV new post-progression patients received one-time the stage IV treatment costs. Additionally, follow-up costs were applied to both pre- and post-progression patients from year 3 onwards. The follow-up costs considered the costs of a CT scan and a physical examination and were based on the ESMO guidelines (Supplementary Table 5) [56].
The end-of-life (EoL) costs were retrieved from a study using data from a Portuguese Comprehensive Cancer Centre and were in the model applied to lung cancer patients who died in the hospital [34]. The EoL cost was the mean number of patients receiving systemic therapy or best supportive care in their last 3 months of life [34]. The EoL costs for individuals who died at home or in another healthcare institution were calculated based on the home care and palliative care costs presented by the Portuguese NHS tariffs (Supplementary Table 5) [35,36].
Utilities
Lung cancer-specific utility values from a systematic literature review and meta-analysis were used, which included data from several European countries, North American countries, Australia and Thailand, as no equivalent data for Portuguese patients was available in literature [38]. The utility values for stage I, II, III and IV lung cancer patients were 0.78, 0.78, 0.69 and 0.69, respectively. For individuals, not having lung cancer diagnosed (including the missed individuals), age-dependent general population utility values were applied [39]. This study provides Portuguese population health-related quality of life data measured by the EQ-5D-5L that can be used as population norms. These norms can be used to advise Portuguese policymakers, care providers and academics on topics concerning healthcare policy and planning, as well as the quantification of treatment effects on health status [39].
Sensitivity analyses
To identify the key drivers of the ICER a one-way sensitivity analysis (OSA) was conducted by varying the deterministic parameter values by 20%. A probabilistic sensitivity analysis (PSA) was conducted by performing a Monte Carlo simulation using 1000 iterations and presented in a cost–effectiveness scatterplot to analyze the robustness of the CEA.
Scenario analysis
Multiple scenarios were investigated to detect the impact on the costs, QALYs and ICER. Firstly, the difference between public and private healthcare sector costs was considered. Therefore, a questionnaire was completed by two experts from different private healthcare centers to compare their private healthcare prices with the public prices presented in the Portuguese NHS tariffs. One scenario focused on increased screening costs based on the CT scan costs in the private healthcare sector. A second scenario focused on increased diagnostic costs based on private healthcare prices. Additionally, one scenario focused on applying the OS rates published by the International Association for the Study of Lung Cancer (IASLC) to determine the effect of better survival outcomes on the ICER. This IASLC study included survival data of 17,477 patients from 16 countries around the globe [37]. In Portugal, the current lung cancer incidence rate is more than two-times lower than in The Netherlands. Therefore, a fourth screening scenario was performed where the lung cancer incidence rate in the screening population was lowered in the same ratio as the current lung cancer incidence by lowering the number of positive scans to investigate the impact of the missed individuals on the outcomes. Additional information regarding the parameters used in the scenario analysis are presented in Supplementary Table 6.
Results
Base-case outcomes
In total, it is estimated that 570,143 individuals would be eligible for screening per screening round, based on the NELSON screening protocol, in Portugal. Assuming that 60% of the eligible population (342,086 individuals) will participate in the annual LCS program, the implementation of screening in contrast to a no-screening scenario is projected to generate an incremental cost of €558.2 million when assessed over a lifetime horizon (Table 2). The main drivers for the extra costs are the screening costs (€303 million) with a CT scan of €74.7 per screening participant and the treatment costs (€216.2 million) mainly due to the total extra stage I costs. The recruitment and screening costs of a screening program will represent, within the current assumptions an annual cost of €18 million.
| Clinical and health outcomes† | Screening | No screening | Incremental |
|---|---|---|---|
| Lung cancer diagnoses | |||
| Total | 61,392 (100%) | 38,659 (63%) | 22,732 (59%) |
| Stage I | 33,370 (54%) | 5102 (8%) | 28,268 |
| Stage II | 3888 (6%) | 1844 (3%) | 2044 |
| Stage III | 10,655 (17%) | 9129 (15%) | 1527 |
| Stage IV | 13,478 (22%) | 22,584 (37%) | -9106 |
| Missed individuals‡ | NA | 22,732 | -22,732 |
| Stage III and IV averted | 7579 | ||
| Lung cancer deaths | |||
| Total | 41,969 | 55,186 | -13,217 |
| Stage I | 15,846 | 2422 | 13,424 |
| Stage II | 2856 | 1,354 | 1502 |
| Stage III | 10,039 | 8595 | 1443 |
| Stage IV | 13,228 | 22,164 | -8936 |
| Missed individuals‡ | NA | 20,650 | -20,650 |
| Life years | |||
| Total | 8,253,694 | 8,140,471 | 113,222 |
| Stage I | 196,016 | 29,834 | 166,182 |
| Stage II | 13,189 | 6144 | 7045 |
| Stage III | 18,185 | 15,441 | 2745 |
| Stage IV | 10,904 | 18,256 | -7352 |
| Missed individuals‡ | NA | 55,397 | -55,397 |
| Lung cancer free participants§ | 8,015,399 | 8,015,399 | 0 |
| Quality-adjusted life years | |||
| Total | 6,909,134 | 6,822,456 | 86,678 |
| Stage I | 154,252 | 23,474 | 130,779 |
| Stage II | 10,440 | 4860 | 5580 |
| Stage III | 12,548 | 10,654 | 1894 |
| Stage IV | 7524 | 12,597 | -5073 |
| Missed individuals‡ | NA | 46,502 | -46,502 |
| Lung cancer free participants§ | 6,724,370 | 6,724,370 | 0 |
| Costs† | |||
| Total | 1,249,467,228 | 691,288,624 | 558,178,604 |
| Recruitment costs | 1,612,567 | NA | 1,612,567 |
| Screening costs | 302,984,791 | NA | 302,984,791 |
| Diagnostic costs | 57,506,773 | 20,102,212 | 37,404,560 |
| Treatment costs | 887,363,097 | 671,186,412 | 216,176,686 |
| Stage I | 379,825,493 | 57,906,307 | 321,919,187 |
| Stage II | 70,767,662 | 33,171,575 | 37,596,086 |
| Stage III | 183,385,894 | 155,864,761 | 27,521,133 |
| Stage IV | 253,384,048 | 424,243,769 | -170,859,721 |
| Health economic outcomes | |||
| Incremental cost–effectiveness ratio (costs per QALY) | € 6440 | ||
| NMB | € 1,113,834,089 | ||
†
The clinical and health outcomes and costs presented in the table are the total costs over a lifetime horizon for the screening and no screening group.
‡
Missed individuals were part of the no-screening arm and assumed to be asymptomatic patients in the pre-clinical disease stage.
§
Lung cancer free participants refer to people who either do not have lung cancer. or have not been identified with lung cancer.
NA: Not applicable; NMB: Net monetary benefit.
A total of 113,222 life-years and 86,678 QALYs would be gained by this LCS program over a lifetime horizon. Per eligible individual screening resulted in €979 additional costs, 0.15 additional QALYs, and 0.20 additional life years saved. For lung cancer patients diagnosed in the screening arm, 1.41 QALYs were gained per individual. The ICER was estimated to be €6440 per QALY gained or €4930 per life-year saved. The net monetary benefit was €1,113,834,089, based on a WTP threshold of €19,290 per QALY gained.
In the LCS arm, 60% of the cancers (37,258 individuals) were detected in stages I and II compared with 18% (6947) in the no screening arm. As a result of the increased detection of early-stage lung cancer, which is known to be correlated with higher rates of survival, a total of 13,217 lung cancer-related deaths could potentially be prevented in one cohort.
Sensitivity & scenario outcomes
A one-way sensitivity analysis was performed to determine the most influential parameters. These were the screening costs, utility values for progression-free stage I patients, year 1 treatment costs for stage I patients, and the discount rates for both health effects and costs. All ICERs were in the range of €5677 to €7379 indicating that all outcomes were still below the WTP threshold (Figure 1).
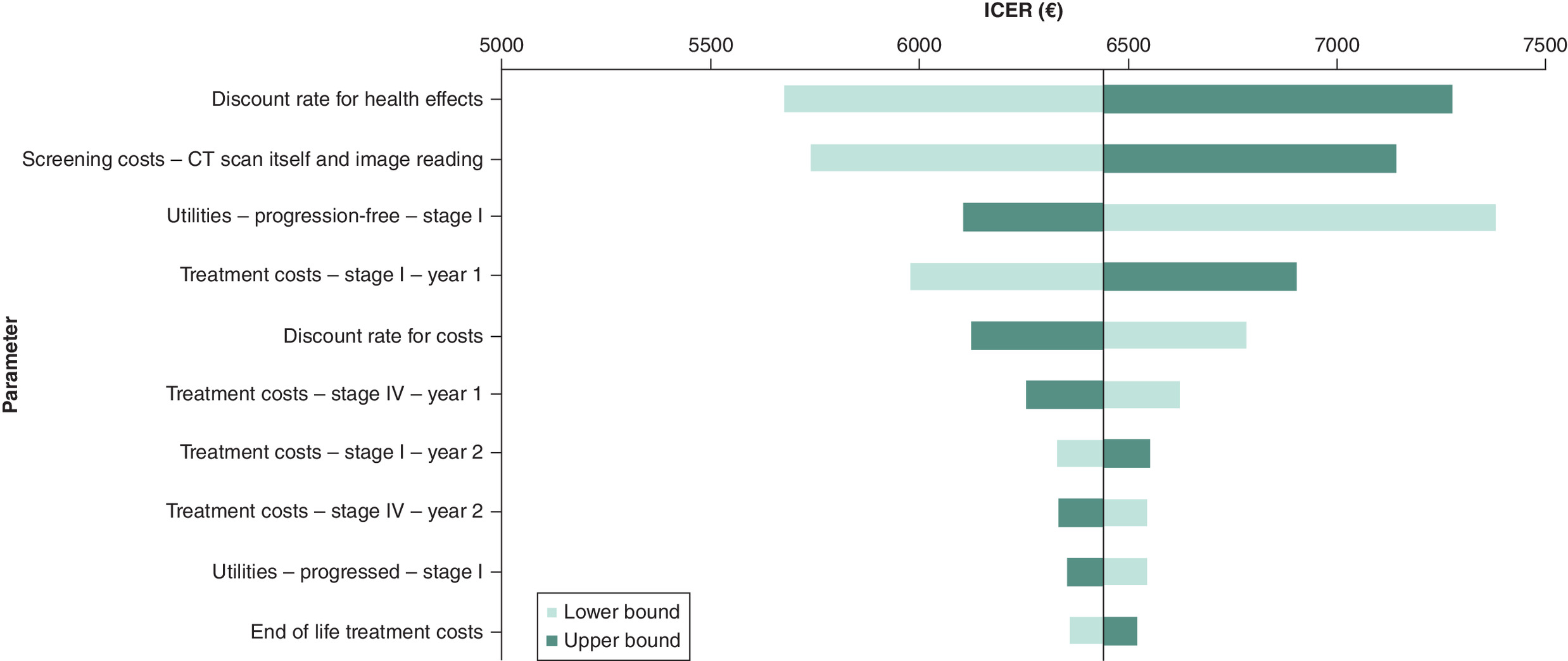
Figure 1. Tornado diagram for the one-way sensitivity analysis for lung cancer screening.
All incremental cost–effectiveness ratios (ICERs) are under the assumed willingness-to-pay threshold of €19,290 per quality-adjusted life year gained. The lower bound refers to a 20% decrease and the upper bound to a 20% increase in the base case parameter value.
The cost–effectiveness acceptability curve summarizes the uncertainty in the ICER and reflects the proportion of results that are considered cost-effective relative to the WTP threshold (Figure 2). The PSA demonstrated that based on 1000 iterations the probabilistic ICERs ranged between €4341 and €17,334 with a probabilistic ICER of €6446. Assuming a WTP threshold of €19,290 the probability of LCS screening to be cost-effective in Portugal was 100%.
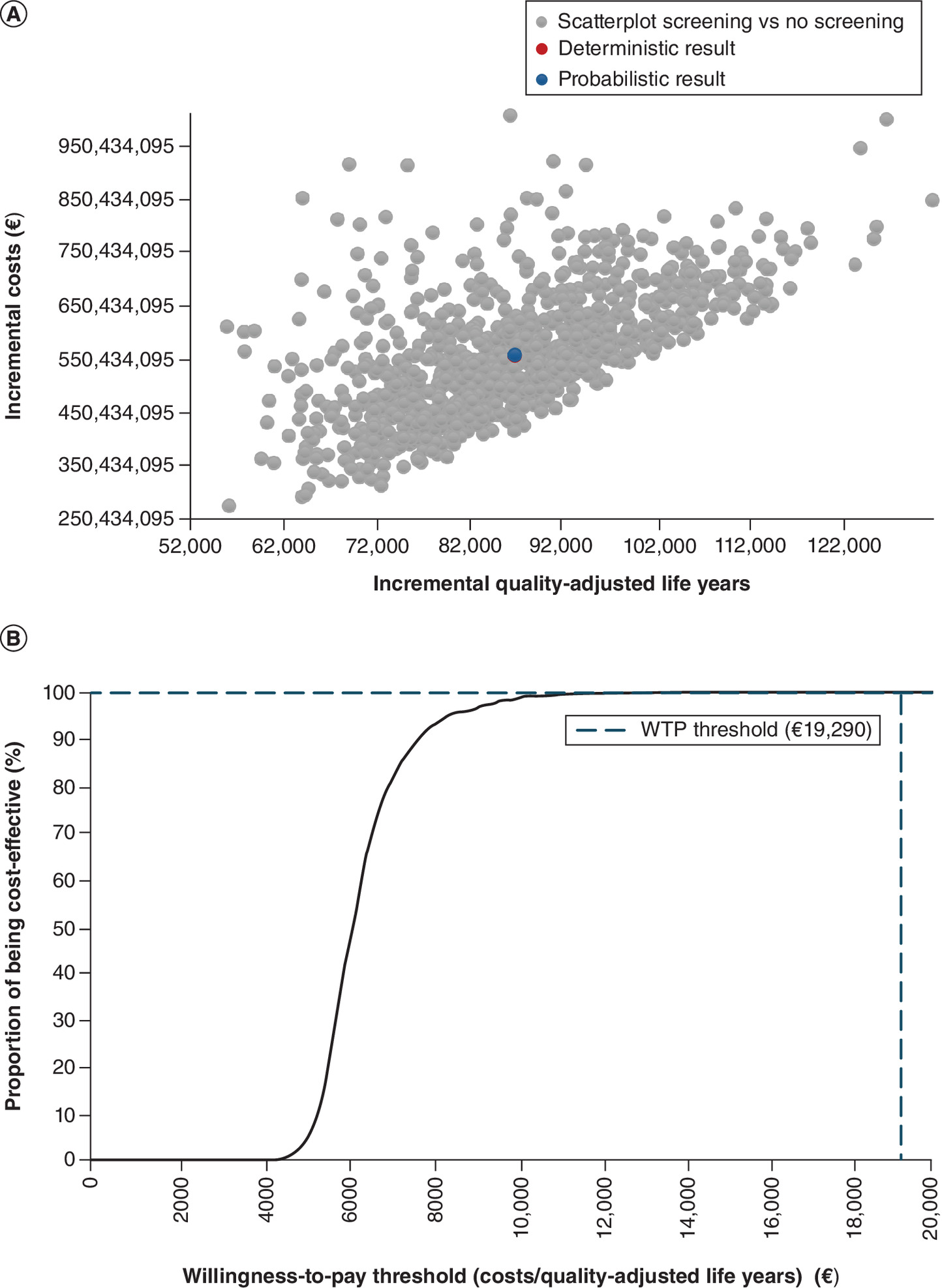
Figure 2. Probabilistic sensitivity analysis.
(A) Incremental cost–effectiveness scatterplot. The deterministic and probabilistic incremental cost–effectiveness ratio (ICER) overlap. The deterministic ICER is €6440 (incremental costs €558,178,604; incremental quality-adjusted life years (QALYs) 86,678). The probabilistic ICER is €6446 (incremental costs €558,833,040; incremental QALYs 86,695).; (B) cost–effectiveness acceptability curve.
One of the scenarios focused on the difference between the public and private healthcare sector prices as it was observed that the CT scan costs were 1.5 to three-times higher in the public sector than the private sector. Increasing the CT scan costs by 0.5 and 4 results in an ICER of €8187 and €16,926 per QALY, respectively. This shows that increasing the CT scan costs from €74.70 to €298.80 still results in an ICER below the WTP threshold. Increasing the total diagnostic by two or ten-times resulted in ICERs of €6876 and €10,368, respectively, making screening still cost-effective in Portugal. An overview of performed scenarios is demonstrated in Table 3 and showed that for all scenarios LCS remained a cost-effective option compared with no screening.
| Scenario name | Screening | No screening | Incremental costs | Incremental QALYs | ICER | ||
|---|---|---|---|---|---|---|---|
| Total costs | Total QALYs | Total costs | Total QALYs | ||||
| Base-case analysis | € 1,249,467,228 | 6,909,134 | € 691,288,624 | 6,822,456 | € 558,178,604 | 86,678 | € 6440 |
| CT-scan cost 50% increase, €112 | € 1,400,959,624 | 6,909,134 | € 691,288,624 | 6,822,456 | € 709,671000 | 86,678 | € 8187 |
| CT-scan cost 100% increase, €149 | € 1,552,452,020 | 6,909,134 | € 691,288,624 | 6,822,456 | € 861,163,396 | 86,678 | € 9935 |
| CT-scan cost 150% increase, €187 | € 1,703,944,415 | 6,909,134 | € 691,288,624 | 6,822,456 | € 1,012,655,791 | 86,678 | € 11,683 |
| CT-scan cost 200% increase, €224 | € 1,855,436,811 | 6,909,134 | € 691,288,624 | 6,822,456 | € 1,164,148,187 | 86,678 | € 13,431 |
| Private diagnostic costs for both arms – two-times as high compared with the base-case value | € 1,306,494,497 | 6,909,134 | € 710,481,960 | 6,822,456 | € 596,012,537 | 86,678 | € 6876 |
| Private diagnostic costs for both arms – five-times as high compared with the base-case value | € 1,477,576,302 | 6,909,134 | € 768,061,969 | 6,822,456 | € 709,514,334 | 86,678 | € 8186 |
| Private diagnostic costs for both arms – ten-times as high compared with the base-case value | € 1,762,712,645 | 6,909,134 | € 864,028,649 | 6,822,456 | € 898,683,995 | 86,678 | € 10,368 |
| Global TNM 8th edition – overall survival | € 1,357,406,790 | 6,961,124 | € 803,120,593 | 6,878,646 | € 554,286,197 | 82,479 | € 6720 |
| Increased lung cancer incidence in the no screening arm (0.92%) | € 1,514,242,639 | 6,810,715 | € 1,365,653,545 | 6,709,609 | € 148,589,094 | 101,106 | € 1470 |
| Overall survival for missed individuals follows stage I patients | € 1,249,467,228 | 6,909,134 | € 691,288,624 | 6,865,300 | € 558,178,604 | 43,834 | € 12,734 |
| Overall survival for missed individuals follows stage III patients | € 1,249,467,228 | 6,909,134 | € 691,288,624 | 6,808,705 | € 558,178,604 | 100,429 | € 5558 |
| Overall survival for missed individuals follows stage IV patients | € 1,249,467,228 | 6,909,134 | € 691,288,624 | 6,791,719 | € 558,178,604 | 117,415 | € 4754 |
| Screening uptake rate, 25% | € 932,363,217 | 6,936,318 | € 698,848,134 | 6,900,202 | € 233,515,083 | 36,116 | € 6466 |
| Screening uptake rate, 75% | € 1,385,368,948 | 6,897,483 | € 688,048,834 | 6,789,136 | € 697,320,114 | 108,347 | € 6436 |
| Societal perspective | € 1,422,464,717 | 6,909,134 | € 839,033,607 | 6,822,456 | € 583,431,110 | 86,678 | € 6731 |
| Include screening-associated disutility | € 1,249,467,228 | 6,902,458 | € 691,288,624 | 6,822,456 | € 558,178,604 | 80,002 | € 6977 |
| Decrease discount rate (costs: 2%,health outcomes: 2%) | € 1,434,455,650 | 8,481,336 | € 796,751,313 | 8,361,533 | € 637,704,337 | 119,803 | € 5323 |
| Increase discount rate (costs: 8%,health outcomes: 8%) | € 980,168,086 | 4,960,938 | € 537,975,188 | 4,911,861 | € 442,192,898 | 49,077 | € 9010 |
| Time horizon, 5 year | € 482,464,776 | 2,216,129 | € 255,084,063 | 2,211,722 | € 227,380,713 | 4406 | € 51,603 |
| Time horizon, 10 year | € 862,226,902 | 3,901,319 | € 469,594,096 | 3,882,941 | € 392,632,807 | 18,378 | € 21,364 |
| Time horizon, 15 year | € 1,142,769,416 | 5,091,399 | € 628,740,232 | 5,053,121 | € 514,029,184 | 38,278 | € 13,429 |
| Screening rounds (n), 3 | € 335,352,447 | 7,170,355 | € 176,873,389 | 7,143,575 | € 158,479,058 | 26,780 | € 5918 |
| Screening rounds (n), 5 | € 518,051,917 | 7,110,158 | € 279,386,663 | 7,069,221 | € 238,665,254 | 40,937 | € 5830 |
| Screening rounds (n), 10 | € 891,001,904 | 7,001,568 | € 489,103,501 | 6,934,953 | € 401,898,403 | 66,615 | € 6033 |
| Screening rounds (n), 15 | € 1,163,969,916 | 6,930,353 | € 643,020,376 | 6,847,887 | € 520,949,540 | 82,466 | € 6317 |
ICER: Incremental cost–effectiveness ratio; QALYs: quality-adjusted life years.
Discussion
Improved clinical outcomes were observed in the analysis with the majority of the lung cancer cases diagnosed in an early stage resulting in 13,217 lung cancer deaths prevented. Moreover, LCS showed to be cost-effective (€6440 per QALY) compared with no screening in Portugal following a WTP threshold of €19,290 per QALY(one-time the GDP per capita). The sensitivity analysis showed that the average probabilistic ICER was €6446 per QALY out of the 1000 iterations, indicating that the results were robust.
This is the first study that assessed the cost–effectiveness of LCS in Portugal, and its conclusion is in line with the ICERs of LCS in different countries, demonstrating that LCS is cost-effective [57–61]. The incremental QALYs gained in the screening population was 86,678 and the additional QALYs gained per lung cancer patient was 1.41. This increase in QALYs was mainly attributed to the stage shift from late to early-stage lung cancer detection, as the 5-year survival rate for stage I lung cancer patients is higher (55%) compared with that for stage IV (3.8%) patients in Portugal [41,42].
The OSA concurrently revealed that the CT scan costs also exert a notable influence on the ICER. The unit cost of a CT scan was € 74.70 in the model, derived from the Portuguese NHS tariffs [31]. However, the healthcare system in Portugal is fragmented with both public and private healthcare providers. Therefore, the unit cost of a CT scan might be higher in practice – it is estimated to be 1.5 to three-times higher in a private healthcare center compared with the publicly used NHS tariff, based on expert opinions. Hence, scenario analyses were conducted to investigate the precise influence of CT scan expenses, and the findings indicated that the ICER would experience a substantial rise to €9935 per QALY, which was notably greater than the base-case ICER of €6440 per QALY, when the CT scan costs were doubled (€149.40). In addition to the CT scan costs, diagnostic costs and treatment costs for lung cancer patients could also increase if LCS was offered through private healthcare providers. Therefore, a concerted endeavor should be directed toward cost containment, with the aim of ensuring the sustainability and broad accessibility of LCS for individuals in need thereof.
Scenario analyses demonstrated that while the cost–effectiveness of LCS remains independent of the uptake rate, variations in clinical outcomes are evident. Specifically, the additional QALYs gained per individual through screening diverged, amounting to 0.74 and 1.60 at uptake rates of 25% and 75%, respectively. Similarly, a lung cancer mortality reduction of 11.3% was achieved at a 25% uptake rate, and it escalated to 24.7% at an uptake rate of 75%. Therefore, it is crucial to achieve an optimal uptake rate to fully realize the benefits of LCS, and an effective recruitment strategy is pivotal in ensuring widespread and meaningful participation in screening programs, drawing lessons from the cervical cancer screening trial in Portugal [62]. A Portuguese study revealed that employing a stepwise approach, which incorporated automated text messages or phone calls followed by manual phone calls and face-to-face interviews, yielded the highest uptake rate. This surpassed the participation rates observed among individuals invited solely via written letters [62].
Another scenario explored the generalizability of NELSON study outcomes in Portuguese population. It was estimated in our model that the lung cancer incidence was 0.46% for high-risk individuals in Portugal, while the counterpart calculated in The Netherlands, where the NELSON study was performed, was 0.86% - approximately two-times higher [29]. Therefore, a scenario analysis was undertaken to explore the impact of a higher lung cancer incidence on the ICER. When lung cancer incidence in the no screening arm was twofold (0.92%), there would be a significant reduction in ICER to €1470 per QALY. This may largely explained by the significant reduction in the incremental costs, given the lung cancer diagnoses in the no screening arm would compensate for the missed individuals, incurring higher treatment costs in the no screening arm. This scenario is supported by a nationwide survey of Portuguese physicians asserting an approximate twofold elevation in the annual lung cancer incidence, indicating a potential case of underreporting the prevalence of the disease in Portugal [63]. The analysis suggested that LCS would be potentially even more cost-effective when the disease burden was heavier for lung cancer.
One of the strengths of our study is that the local overall survival (OS) data was used, and it was obtained from the Portuguese Oncology Institute of Porto [40–42]. An alternative is the OS data derived from a global source, the IASLC TNM 8th edition [37]. The scenario analysis indicated a similar ICER for both datasets although the OS global dataset showed higher survival rates for all 4 stages compared with the Portuguese data and mainly for the stages I to III. For instance, the 5-year OS rate for stage I exhibited a substantial 24% increment in the global dataset as compared with the Portuguese dataset, with figures of 79% versus 55%, respectively [37,42]. Consequently, this could lead to an overestimation of the incremental life-years gained, given more early-stage lung cancer patients would be detected with LCS. Hence, the incorporation of the local OS dataset better reflects the specific contextual nuances pertinent to the Portuguese settings. Furthermore, these OS inputs were congruent with the outcomes reported in another Portuguese study, which encompassed four cancer registries spanning the entirety of the nation [64]. Simultaneously, the aforementioned analysis also revealed that should there be additional enhancements in the OS for lung cancer patients in Portugal, LCS would result in additional life years gained for the diagnosed lung cancer patients. In addition, other scenarios were conducted to explore uncertainties in the data inputs and provided insights into the potential implementation of LCS.
Limitations of this model are similar to the original UK model, which revolves around the scarcity and robustness of the local data to populate the model [16]. For instance, the model utilized the utility values reported by systematic review, which investigated the health state utility values for lung cancer patients with 27 included studies from various European countries, due to the absence of Portuguese local data [38]. Health state utility values play a crucial role in health economics and outcomes research, as they quantify the preferences and quality of life associated with different health conditions. This limitation hinders our ability to assess the qualified-adjusted life years precisely for the local population. However, for the cancer-free screening participants, Portugal-specific population norms were used, and it was measured by the EQ-5D-5L questionnaire to reflect the quality of life for local population [39]. Additionally, the one-way sensitivity analysis showed that 20% variation in the utility value for stage I lung cancer patients resulted in ICERs ranging between €6107 to €7379 per QALY, indicating a marginal difference compared with the base-case ICER (€6440 per QALY). Moreover, the probabilistic sensitivity analysis conducted over 1000 iterations, yielded an average ICER of €6446. These findings collectively underscore the resilience and robustness of the base-case results. Nevertheless, addressing this data gap through further empirical investigations would improve the precision and accuracy of resource allocation decisions for LCS.
It is notable that Portugal has already instituted screening programs for breast and cervical cancer; however, no cost–effectiveness studies exist regarding these programs. Furthermore, a pilot program for colorectal cancer (CRC) screening was initiated in 2016 and subsequently extended to encompass a regional scope by 2018 [65]. Remarkably, the decisions on the screening strategies for CRC were underpinned by a cost–effectiveness study [66]. The study concluded that the CRC screening with the biennial fecal immunochemical test (FIT) resulted in an ICER of €2694 per QALY, while with the colonoscopy every 10 years, the ICER was €48,285 per QALY, both under the NHS tariff in Portugal. The unit price for a FIT was merely €3, and it was €397 for a colonoscopy, which was more comparable to the LDCT used for LCS in our study. Therefore, our results demonstrate that the annual LCS with the volume-based low-dose CT is more cost-effective than the CRC screening with a colonoscopy, with an ICER of €6440 per QALY.
According to the Portuguese Health Minister, Portugal's cancer screening program will expand to include lung cancer among others, beginning with pilot projects in 2023 [67]. This is in line with the recommendations of the European Union [15]. Our study provides timely evidence and insights to support the implementation of the LCS pilot programs and assures a nationwide Portuguese LCS program is likely to be cost-effective.
Conclusion
Our study demonstrates that annual LCS with volume-based low-dose CT for a high-risk asymptomatic population in Portugal is cost-effective, representing an efficient use of governmental resources and leads to improved outcomes for lung cancer patients.
Summary points
•
Lung cancer is mainly diagnosed in a late stage of the disease which is associated with a low 5-year survival rate, which is 2% in Portugal. Lung cancer screening (LCS) studies have demonstrated to detect lung cancer in an early stage, resulting in a mortality benefit for lung cancer patients.
•
This study investigated the clinical and economic consequences of an annual LCS program compared with no LCS program from a Portuguese healthcare system perspective and over a lifetime horizon.
•
A validated model developed to calculate the cost–effectiveness of LCS in the UK was adapted to reflect the Portuguese situation. The model consisted of a decision tree with an integrated Markov trace. The model reflected the natural history of lung cancer where patients started in the pre-progression state in either stage I, II, III or IV lung cancer, and could transit to the post-progression and/or death state over time.
•
The model was built on the Dutch–Belgian randomized lung cancer screening trial (NELSON), the biggest European LCS study. The study protocol and outcomes were used to inform the model and populate the decision tree.
•
The treatment costs and overall survival data were obtained from the Portuguese Oncology Institute of Porto, which is the largest oncological hospital in Portugal.
•
The analysis estimated a total of €558.2 million incremental costs when comparing LCS to no screening. Overall, per eligible individual annual LCS resulted in €979 additional cost per individual.
•
The incremental QALYs gained were 86,678 for the screening arm, indicating 0.15 additional QALYs gained per eligible individual or 1.41 QALYs gained per lung cancer patient. In total, 13,271 lung cancer deaths could be averted when implementing screening.
•
The main driver for the extra cost was the screening cost as all participants needed to undergo a low-dose CT scan. Doubling or quadrupling the CT scan cost to reflect the private healthcare sector resulted still in a cost-effective program with ICERs of €9935 and €16,926 per QALY gained.
•
Results of this study showed that an annual LCS compared with no screening would be cost-effective in Portugal with an ICER of €6440 per QALY gained.
Author contributions
H ten Berge, K Togka, X Pan and R Medeiros participated in the concept and design of the paper. H ten Berge, K Togka and M Borges conducted the data acquisition and analysis. H ten Berge, K Togka performed the modelling and drafted the manuscript. X Pan performed the technical validation, and M Borges and R Sousa reviewed the methodology. R Medeiros provided critical feedback and supervision throughout the research process. All authors participated in the data validation, data interpretation and critical revision of the paper. Final approval of the manuscript was given by all authors.
Acknowledgments
This project was developed by Aliança para o Cancro do Pulmão (Lung Cancer Alliance) gathering SPP-Sociedade Portuguesa de Pneumologia, GECP-Grupo de Estudos do Cancro do Pulmão, Pulmonale, LPCC- Liga Portuguesa Contra o Cancro, AstraZeneca, SPCCTV-Sociedade Portuguesa de Cirurgia Cardíaca, Torácica e Vascular and OM-Ordem dos Médicos.
Financial disclosure
This work was funded by AstraZeneca PLC. H ten Berge, K Togka and X Pan are employed by iDNA. S Figuieredo and R Sousa are employed by AstraZeneca. M Borges has received support for attending meetings or traveling from Roche Portugal outside the submitted work. DM Cabral received payment or honoraria for lectures, presentations or education events from Medtronic symposium outside the submitted work. A Araújo received payment or honoraria for lectures, presentations, education events or attending meetings from Janssen, IPSEN, BMS, MSD, Takeda, Sanofi and Daiichi Sankyo; has been advisory board member of BMS, MSD, Janssen, Pfizer, Eli Lilly Oncology and Takeda outside the submitted work. F Estevinho received payment or honoraria for lectures, presentations, education events or attending meetings Takeda, AstraZeneca, Sanofi, BMS, MSD, Roche, Pfizer, Boehringer Ingelheim, Janssen Cilag, Pierre Fabre, Novartis, Lilly and Servier Portugal; has been an advisory board member of Janssen-Cilag, BMS, MSD, Merck, Novartis, Boehringer Ingelheim, AstraZeneca, Pfizer outside the submitted work. FMP Martelo received payment or honoraria for lectures, presentations, education events, or attending meetings from Merck Sharp & Dohme, Roche and Medtronic; has been an advisory board member for AstraZeneca outside the submitted work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 192.41 KB
References
Papers of special note have been highlighted as: • of interest
1.
Ferlay J, Ervik M, Lam F et al. Global Cancer Observatory: Cancer Today (2024). https://gco.iarc.who.int/today
2.
Borges M, Gouveia M, Alarcão J et al. Cost and burden of non-small-cell lung cancer's in Portugal. Value Health 17(7), A626 (2014).
• Provides estimates of the substantial economic burden of non-small-cell lung cancer in Portugal.
3.
Costa L, Alexandre T, Mansinho A et al. Health outcomes and budget impact projection of anti-PD-(L)1s in cancer care in Portugal. Front. Public Health 11, 1133959 (2023).
4.
Duma N, Santana-Davila R, Molina JR. Non–small cell lung cancer: epidemiology, screening, diagnosis, and treatment. Mayo Clin. Proc. 94(8), 1623–1640 (2019).
5.
Shankar A, Dubey A, Saini D et al. Environmental and occupational determinants of lung cancer. Transl. Lung Cancer Res. 8(Suppl. 1), S31 (2019).
6.
de Alencar VTL, Formiga MN, de Lima VCC. Inherited lung cancer: a review. Ecancermedicalscience 14, 1008 (2020).
7.
Knight SB, Crosbie PA, Balata H, Chudziak J, Hussell T, Dive C. Progress and prospects of early detection in lung cancer. Open Biol. 7(9), 170070 (2017).
8.
Guerreiro T, Forjaz G, Antunes L et al. Lung cancer survival and sex-specific patterns in Portugal: a population-based analysis. Pulmonology 29(Suppl. 4), S70–S79 (2023).
9.
Walser T, Cui X, Yanagawa J et al. Smoking and lung cancer: the role of inflammation. Proc. Am. Thorac. Soc. 5(8), 811 (2008).
10.
de Koning HJ, van der Aalst CM, de Jong PA et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N. Engl. J. Med. 382(6), 503–513 (2020).
• The biggest European lung cancer study proves reduced lung cancer mortality with low-dose CT screening.
11.
National Lung Screening Trial Research Team, Aberle D, Adams A et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 365(5), 395–409 (2011).
12.
European Commission. 4-IN THE LUNG RUN: towards INdividually tailored INvitations, screening INtervals, and INtegrated co-morbidity reducing strategies in lung cancer screening. https://cordis.europa.eu/project/id/848294 (2022).
13.
NHS England. Evaluation of the Targeted Lung Health Check programme. https://www.england.nhs.uk/contact-us/privacy-notice/how-we-use-your-information/our-services/evaluation-of-the-targeted-lung-health-check-programme/ (2022).
14.
Economia Online. Screenings will be extended to lung, prostate and stomach cancer, says minister (2022). https://eco.sapo.pt/2022/12/09/rastreios-vao-ser-alargados-a-cancro-do-pulmao-prostata-e-estomago-diz-ministro/
15.
European Commission. Europe's Beating Cancer Plan (2021).
• This report written by the European Commission highlights the political commitment to early detection of (lung) cancer in Europe.
16.
Pan X, Dvortsin E, Baldwin DR et al. Cost-effectiveness of volume computed tomography in lung cancer screening: a cohort simulation based on Nelson study outcomes. J. Med. Econ. 27(1), 27–38 (2024).
• This study performed a cost–effectiveness analysis for lung cancer screening (LCS) in the UK, and this model was used to determine the cost–effectiveness of LCS in Portugal.
17.
ten Berge H, Ramaker D, Piazza G et al. Shall we screen lung cancer with volume computed tomography in Austria? A cost-effectiveness modelling study. Cancers (Basel) 16(15), 2623 (2024).
18.
Tan-Torres Edejer T Baltussen R, AdamT et al. Making choices in health: WHO guide to cost-effectiveness analysis. WHO, Switzerland (2003). https://iris.who.int/handle/10665/42699
19.
Eurostat. Real GDP per capita (2022). https://ec.europa.eu/eurostat/databrowser/view/sdg_08_10/default/table
20.
Perelman J, Soares M, Mateus C et al. Methodological Guidelines for Economic Evaluation Studies of Health Technologies. Infarmed– National Authority of Medicines and Health Products, Lisboa,Portugal (2019). https://www.infarmed.pt/web/infarmed-en/human-medicines
21.
Trading Economics. Portugal Inflation Rate (2022). https://tradingeconomics.com/portugal/inflation-cpi
22.
National Institute for Health and Care Excellence (NICE). NICE Guideline - Lung cancer: diagnosis and management. NICE, UK (2019). https://www.nice.org.uk/guidance/ng122
23.
Horeweg N, Van Der Aalst CM, Vliegenthart R et al. Volumetric computed tomography screening for lung cancer: three rounds of the NELSON trial. Eur. Respir. J. 42(6), 1659–1667 (2013).
24.
Yousaf-Khan U, Van Der Aalst C, De Jong PA et al. Final screening round of the NELSON lung cancer screening trial: the effect of a 2.5-year screening interval. Thorax 72(1), 48–56 (2017).
25.
Ministry of Health General Directorate of Health. National Strategy Against Cancer 2021–2030 (ESTRATÉGIA NACIONAL DE LUTA CONTRA O CANCRO) (2022). https://www.consultalex.gov.pt/ConsultaPublica_Detail.aspx?Consulta_Id=248 (Accessed: 18 June 2023)
26.
Guerreiro T, Antunes L, Bastos J et al. Lung cancer: a nationwide study to characterize sex differences, incidence, and spatial patterns in Portugal. In Vivo 34(5), 2711–2719 (2020).
27.
United Nations Department of Economics and Social Affairs. Population Division. World Population Prospects (2020). Online edition. https://population.un.org/wpp/Download/Standard/Population/
28.
PORDATA. Resident population, annual average: total and by age group (2020).https://www.pordata.pt/en/db/search+environment/new+search
29.
World Health Organization - International Agency for Research on Cancer. Estimated number of new cases in 2020, Portugal, both sexes, ages 50–74 (2020). https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=cancer&mode_population=continents&population=900&populations=620&key=asr&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=10&ages_group%5B%5D=14&group_cancer=1&
30.
Statistics Portugal. National Health Survey: less smoking, but increased risky alcohol consumption – 2019 (2020). https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_destaques&DESTAQUESdest_boui=414436388&DESTAQUESmodo=2
31.
National Health Service (Serviço nacional de saúde). Portaria n.o 254/2018, de 7 de setembro (2018). https://www.acss.min-saude.pt/2016/12/15/precos-do-sns-2/
32.
National Health Service (Serviço nacional de saúde). Portaria n.o 234/2015 (2015). https://www.acss.min-saude.pt/2016/12/15/precos-do-sns-2/
33.
Borges M, Sousa V, Oliveira A et al. A journey towards a value-based healthcare (VBHC) funding model for lung cancer: the FAROL (“lighthouse”) project. Presented at: EHMA 2022 Annual Conference. Brussels, Belgium (17 June 2022).
34.
Pereira IA, Gomes J, Redondo P, Antunes L, Borges M, Savva-Bordalo J. 1515P Aggressiveness and economic impact of advanced cancer treatment near the end of life. Ann. Oncol. 31, S935 (2020).
35.
National Health Service (Serviço nacional de saúde). Portaria n.o 207/2017, de 11 de juhlo. (2017). https://www.acss.min-saude.pt/2016/12/15/precos-do-sns-2/ (Accessed: 8 September 2023)
36.
National Health Service (Serviço nacional de saúde). Portaria n.o 176/2022, de 7 de juhlo (2022). https://www.acss.min-saude.pt/2016/12/15/precos-do-sns-2/
37.
Goldstraw P, Chansky K, Crowley J et al. The IASLC Lung Cancer Staging Project: proposals for revision of the TNM Stage groupings in the forthcoming (eighth) edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 11(1), 39–51 (2016).
38.
Blom EF, Haaf K ten, de Koning HJ. Systematic review and meta-analysis of community- and choice-based health state utility values for lung cancer. Pharmacoeconomics 38(11), 1187 (2020).
39.
Ferreira PL, Pereira LN, Antunes P, Ferreira LN. EQ-5D-5L Portuguese population norms. Eur. J. Health Econ. 24(9), 1411–1420 (2023).
40.
Soares M, Antunes L, Redondo P et al. Small cell lung cancer treatment and survival in Portugal: a retrospective analysis from the I-O Optimise initiative. Eur. J. Cancer Care (Engl.) 30(6), e13496 (2021).
41.
Soares M, Antunes L, Redondo P et al. Treatment and outcomes for early non-small-cell lung cancer: a retrospective analysis of a Portuguese hospital database. Lung Cancer Manag. 10(2), LMT46 (2021).
42.
Soares M, Antunes L, Redondo P et al. Real-world treatment patterns and survival outcomes for advanced non-small-cell lung cancer in the pre-immunotherapy era in Portugal: a retrospective analysis from the I-O Optimise initiative. BMC Pulm. Med. 20(1), 240 (2020).
43.
McPherson I, Bradley NA, Govindraj R, Kennedy ED, Kirk AJB, Asif M. The progression of non-small-cell lung cancer from diagnosis to surgery. Eur. J. Surg. Oncol. 46(10 Pt A), 1882–1887 (2020).
44.
Felip E, Altorki N, Zhou C et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB–IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet 398(10308), 1344–1357 (2021).
45.
Antonia SJ, Villegas A, Daniel D et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N. Engl. J. Med. 377(20), 1919–1929 (2017).
46.
Gandhi L, Rodríguez-Abreu D, Gadgeel S et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 378(22), 2078–2092 (2018).
47.
Soria J-C, Ohe Y, Vansteenkiste J et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N. Engl. J. Med. 378(2), 113–125 (2018).
48.
Horn L, Mansfield AS, Szczęsna A et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N. Engl. J. Med. 379(23), 2220–2229 (2018).
49.
Statistics Portugal. Web Portal (2022). https://sdmxessnet.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&indOcorrCod=0004158&contexto=bd&selTab=tab2
50.
National program for oncological disease (programa nacional para as doençasoncológicas). SNS resources in Oncology - Survey Report 2021 (Recursos do SNS em Oncologia - Relatorio de Inquerito 2021). Ministry of Health, General Directorate of Health, Portugal (2022). https://www.dgs.pt/portal-da-estatistica-da-saude/diretorio-de-informacao/diretorio-de-informacao/por-anos-dos-dados-1288901-pdf.aspx?v=%3d%3dDwAAAB%2bLCAAAAAAABAArySzItzVUy81MsTU1MDAFAHzFEfkPAAAA
51.
Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA. Non–small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clinic Proc. 83(5), 584 (2008).
52.
Guyot P, Ades AE, Beasley M, Lueza B, Pignon JP, Welton NJ. Extrapolation of survival curves from cancer trials using external information. Med. Decis. Making 37(4), 353–366 (2017).
53.
Latimer N. NICE DSU Technical Support Document 14: survival analysis for economic evaluations alongside clinical trials-extrapolation with patient-level data report by the Decision Support Unit. NICE, Sheffield, UK (2011). https://www.ncbi.nlm.nih.gov/books/NBK395885/pdf/Bookshelf_NBK395885.pdf
54.
Crosbie PA, Gabe R, Simmonds I et al. Yorkshire Lung Screening Trial (YLST): protocol for a randomised controlled trial to evaluate invitation to community-based low-dose CT screening for lung cancer versus usual care in a targeted population at risk. BMJ Open 10(9), e037075 (2020).
55.
Firmino-Machado J, Soeteman DI, Lunet N. Cost-effectiveness of a stepwise intervention to promote adherence to cervical cancer screening. Eur. J. Public Health 30(3), 401–410 (2020).
56.
Postmus PE, Kerr KM, Oudkerk M et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 28(Suppl. 4), iv1–iv21 (2017).
57.
Al Khayat MNMT, Eijsink JFH, Postma MJ, van de Garde EMW, van Hulst M. Cost-effectiveness of screening smokers and ex-smokers for lung cancer in The Netherlands in different age groups. Eur. J. Health Econ. 23(7), 1221–1227 (2022).
58.
Tomonaga Y, ten Haaf K, Frauenfelder T et al. Cost-effectiveness of low-dose CT screening for lung cancer in a European country with high prevalence of smoking – a modelling study. Lung Cancer 121, 61–69 (2018).
59.
Hofer F, Kauczor HU, Stargardt T. Cost-utility analysis of a potential lung cancer screening program for a high-risk population in Germany: a modelling approach. Lung Cancer 124, 189–198 (2018).
60.
Hinde S, Crilly T, Balata H et al. The cost-effectiveness of the Manchester ‘lung health checks’, a community-based lung cancer low-dose CT screening pilot. Lung Cancer 126, 119–124 (2018).
61.
Veronesi G, Navone N, Novellis P et al. Favorable incremental cost-effectiveness ratio for lung cancer screening in Italy. Lung Cancer 143(March), 73–79 (2020).
62.
Firmino-Machado J, Soeteman DI, Lunet N. Cost-effectiveness of a stepwise intervention to promote adherence to cervical cancer screening. Eur. J. Public Health 30(3), 543–552 (2020).
63.
Barata F, Fidalgo P, Figueiredo S, Tonin FS, Duarte-Ramos F. Limitations and perceived delays for diagnosis and staging of lung cancer in Portugal: a nationwide survey analysis. PLOS ONE 16(6), e0252529 (2021).
64.
Guerreiro T, Forjaz G, Antunes L et al. Lung cancer survival and sex-specific patterns in Portugal: a population-based analysis. Pulmonology 29(Suppl. 4), S70–S79 (2023).
• Demonstrated that the stage of diagnosis has the biggest impact on survival, emphasizing that early-stage diagnosis is critical in improving survival prospects.
65.
Monteiro H, Tavares F, Reis J et al. Colorectal screening program in northern Portugal: first findings. Acta Med. Port. 35(3), 164–169 (2022).
66.
Areia M, Fuccio L, Hassan C, Dekker E, Dias-Pereira A, Dinis-Ribeiro M. Cost-utility analysis of colonoscopy or fecal immunochemical test for population-based organised colorectal cancer screening. United European Gastroenterol. J. 7(1), 105–113 (2019).
• Provides information on the cost-utility of colorectal cancer screening in Portugal, a similar cancer screening program aiming to detect cancer in an early stage.
67.
Portugal Resident. New cancer screening pilot projects scheduled for 2023. https://www.portugalresident.com/new-cancer-screening-pilot-projects-scheduled-for-2023/ (2023).
Information & Authors
Information
Published In
Copyright
© 2024 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 July 2024
Accepted: 6 September 2024
Published online: 27 September 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of lung cancer screening with volume computed tomography in Portugal. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0102
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Nuo Chen, Siyuan Wang, Jing Bai, Fanny Franchini, Kaung Mon Winn, Jingyi Hu, Jian Wang, Gang Chen, Cost-Effectiveness and Budget Impact of Lung Cancer Screening: A Systematic Review, PharmacoEconomics, 10.1007/s40273-026-01639-8, (2026).
- Jaime L. Peters, Tristan Snowsill, Sophie Robinson, Edward Griffin, Christopher Hyde, Considering research waste in economic evaluations of low-dose computed tomography screening for lung cancer, International Journal of Technology Assessment in Health Care, 10.1017/S0266462326103687, 42, 1, (2026).
- Zijuan Fan, Manqi Zheng, Ziyun Guan, Hanting Liu, Pengyue Guo, Yang Zhu, Bo Zhang, Luyao Hu, Xianqi Zhao, Tiantian Fu, Mengting Liu, Xinran Jiang, Ningjun Ren, Chunli Zhang, Wenxi Wang, Chun Hao, Jinghua Li, Cost-effectiveness of lung cancer screening: insights from risk stratification, guidelines, and emerging technologies—a systematic review, npj Primary Care Respiratory Medicine, 10.1038/s41533-026-00482-w, (2026).
- Georgia Hardavella, Kyriaki Tavernaraki, Dimitrios Lioumpas, Efimia Boutsikou, Eleni Karetsi, Elli Keramida, Alexandros Letsos, Konstantinos Livanios, Ιra Michailidou, Stylianos Benakis, Aggeliki Pandi, Leonidas Papastavrou, Konstantinos Stefanidis, Eleftherios Zervas, Theoni Agapitou, Martha Andritsou, Stavros Anevlavis, Gerasimos Apollonatos, Kathi Apostolidou, Katerina Bakiri, Zafeiria Barmparessou, Elena Bellou, Danai Bisirtzoglou, Loukas Dagdilelis, Eleni Fili, Christophoros Foroulis, Stylianos Gaitanakis, Christina Gkriniouk, George Kapetanakis, Konstantinos Karagiannis, Ioannis Karampinis, Eleni Kokkotou, Alexandra Kote, Athanasios Kostoulas, Sofia Lambaki, Dimitrios Magouliotis, Maria Mani, Gerasimos Metaxas, Aggeliki Miziou, Katerina Mproupi, Styliani Mytilinaiou, Konstantinos Potaris, Konstantinos Samitas, Vasilios Skouras, Dionysis Spyratos, Andreas Stathoulopoulos, Myrsini Stasinopoulou, Lamprini Stournara, Emmanouil Theodorakis, Sokratis Tsagaropoulos, Stylianos Vittorakis, Charalampos Zisis, Panagiotis Zois, Ioannis Gkiozos, Structured narrative review on lung cancer screening: current evidence, clinical practice implications and implementation insights from a multidisciplinary task force and patient representatives, European Respiratory Review, 10.1183/16000617.0249-2024, 34, 178, (240249), (2025).
- Frederic W. Grannis, Cassandra’s tears: population lung cancer screening in Western Europe, Academia Oncology, 10.20935/AcadOnco7809, 2, 3, (2025).
- Tatiana Bezdenezhnykh, James O'Mahony, Benjamin Jacob, Deirdre Murray, Daniel Ryan, Jarushka Naidoo, Seamus Cotter, Alan Smith, Patrick Redmond, Protocol for the economic evaluation of LCS in Ireland: modelling costs, eligibility, and outcomes, HRB Open Research, 10.12688/hrbopenres.14126.2, 8, (55), (2025).
- Tatiana Bezdenezhnykh, James O'Mahony, Benjamin Jacob, Deirdre Murray, Daniel Ryan, Jarushka Naidoo, Seamus Cotter, Alan Smith, Patrick Redmond, Protocol for the economic evaluation of LCS in Ireland: modelling costs, eligibility, and outcomes, HRB Open Research, 10.12688/hrbopenres.14126.1, 8, (55), (2025).