Clinical characteristics and treatment outcomes in multiple sclerosis patients treated with anti-CD20s who switched to fumarates: a retrospective analysis of a US healthcare claims database
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Anti-CD20 monoclonal antibodies and fumarates are common multiple sclerosis (MS) disease-modifying therapies (DMTs). Data on switching from anti-CD20s to other DMTs are limited. This retrospective, observational study of the US Komodo Health Sentinel claims database aimed to evaluate a de-escalation strategy in a real-world cohort, comparing clinical characteristics, relapses, healthcare encounters (HCEs) and healthcare costs (HCCs) between patients aged ≥18 years with stable MS who switched from anti-CD20s to fumarates (‘Switchers’) versus patients who stayed on anti-CD20s (‘Stayers’). Materials & methods: Patients with MS (diagnosed 1 January 2015–31 August 2022) were propensity score matched 5:1 (Stayers:Switchers) and followed from index to end of study; end of insurance eligibility; >45-day gap in index DMT; or DMT switch. Primary outcomes were clinical characteristics and claims-based annualized relapse rate (ARR). Rates of HCEs and HCCs were estimated. Results: Baseline characteristics were well balanced between cohorts (Stayers, n = 540; Switchers, n = 108). Mean (SD) duration of post-index follow-up was 341.4 (250.0) days for both cohorts. Mean (SD) ARR was 0.08 (0.41; Stayers) versus 0.14 (0.5; Switchers; p = 0.3). Twenty-one Stayers (3.9%) and 1 Switcher (0.9%) were hospitalized for infections, with mean stays of 9.9 and 1 day, respectively. Mean annualized all-cause HCEs were similar between cohorts; annualized inpatient infection-related HCEs were higher for Stayers versus Switchers (mean difference: -0.05; p = 0.005). Annualized all-cause HCCs were similar between cohorts; Switchers had lower annualized infection-related HCCs overall (mean difference: -$2412; p = 0.002) and in the inpatient setting (mean difference: -$2325; p = 0.002). Conclusion: After 1 year, no significant differences in ARR emerged between cohorts. Switchers experienced lower inpatient infection-related HCEs, shorter inpatient infection-related hospital stays and lower overall infection-related HCCs.
Plain language summary – a study looking at people living with multiple sclerosis who switched from treatment with anti-CD20s to fumarates
What is this article about?
•
There are many medications available to treat multiple sclerosis (MS) but each differs in how they work, how well they work and associated risks.
•
Common medications to treat MS include anti-CD20 monoclonal antibodies and fumarates.
•
The aim of this study was to understand the differences in relapses, healthcare visits and healthcare costs in people with stable MS who switched from anti-CD20 to fumarates compared with a matched group of people who stayed on anti-CD20.
What were the results?
•
The people in both groups (those who stayed on treatment and those who switched treatment) had similar age, race, insurance type, disease severity and length of time taking anti-CD20 medication. No significant differences in relapse rate were observed between the two groups. Overall healthcare claims and healthcare costs were similar between both groups.
•
Patients who switched treatment had lower healthcare claims and healthcare costs related to infections. Costs and healthcare claims related to infections were similar in the emergency room and outpatient setting.
What do the results mean?
•
After 1 year, people living with MS who switched treatments from anti-CD20 to fumarates had similar treatment efficacy compared with people who stayed on anti-CD20, but they had fewer infections requiring visits to a healthcare provider or hospital.
Although there are no curative therapies for multiple sclerosis (MS), the treatment options have expanded considerably over the past three decades; including generics, there are currently over 20 disease-modifying therapies (DMTs) available that can alter the course of the disease by reducing disease activity and accumulation of disability [1–4]. These medications differ in their routes of administration, mechanisms of action and efficacy and safety profiles [1,3,4]. Given that MS is a chronic disease requiring long-term treatment, switching between the many available DMTs, often for tolerability, safety or lack of efficacy, is a common clinical strategy to optimize individual patient outcomes [2,5,6].
Optimizing treatment of MS is important not only because of the impact on the lives of patients and their caregivers, but also because of the significant healthcare costs and subsequent economic impact. With the expanding options available for treatment and the advent of multiple high-efficacy therapies, goals of treatment have shifted to achieving no evidence of disease activity, monitoring for progression independent of relapses and mitigating risks of DMTs in the long term [7–9].
There is heterogeneity in treatment strategies used in clinical practice [2,10,11]. Two approaches typically used in the treatment of patients with newly diagnosed relapsing-remitting MS are an escalating approach and an early intensive treatment approach [11]. An escalating approach to DMT use is a common method, with the initiation of mildly efficacious agents (e.g., interferon-beta, glatiramer acetate or teriflunomide) or moderately efficacious agents (e.g., dimethyl fumarate [DMF], diroximel fumarate [DRF] or sphingosine-1-phosphate receptor modulators), and then escalating to highly efficacious agents (e.g., natalizumab, anti-CD20s or alemtuzumab) if there is breakthrough disease activity. Alternatively, in an early intensive treatment approach, there is emerging evidence to support the benefits of initiation of highly efficacious agents in some patients early in their disease course [10]. Currently in the US, the most commonly used classes of DMT include anti-CD20 monoclonal antibodies (mAbs) and fumarates [12].
While earlier intervention with high-efficacy therapies may improve long-term clinical outcomes [10], safety concerns such as the risk of infection may motivate switching. De-escalating treatment by switching to a moderate-efficacy agent, after disease activity has stabilized, may mitigate safety or tolerability concerns. The importance of minimizing the risk of infection in patients with MS is a particular concern during a pandemic such as that of COVID-19 [13–16]. However, there are limited data on patients who have switched from anti-CD20 mAbs due to efficacy or nonefficacy reasons.
The purpose of this study was to evaluate the effectiveness, safety and healthcare burden of fumarates after switching from anti-CD20 mAbs for nonefficacy reasons in stable patients, and comparing those outcomes versus a matched cohort of patients who stayed on anti-CD20 mAbs.
Materials & methods
Study design & patients
This was a retrospective, observational study of the Komodo Health Sentinel database to evaluate changes in outcomes of patients with MS who switched from anti-CD20 mAbs to fumarates. The Komodo Health Sentinel database is a real-world dataset that integrates disparate sources of patient-level data to map longitudinal patient journeys. Komodo pulls de-identified, patient-level claims data from clearing house, payer (≥150 payers) and provider data sources to follow patients as they move through the healthcare system. Komodo’s dataset allows researchers to conduct a robust claims-based analysis with a large sample size and long follow-up periods.
The earliest date of the first fumarates claim following the switch from an anti-CD20 mAb was defined as the index date for those patients who switched. Patients were eligible for inclusion in this analysis if they were aged ≥18 years at index with at least one diagnosis of MS (based on the International Classification of Diseases, Ninth and Tenth Revision [ICD-9, ICD-10] diagnosis codes) during the study period (1 January 2015 to 31 August 2022) and switched from anti-CD20 mAbs (ocrelizumab, ofatumumab or rituximab) to a fumarate (DMF or DRF) between 1 January 2017 and 31 May 2022. A gap of ≤450 days between the administration date of the last anti-CD20 claim and index fumarate was allowed (calculated as infusion date + 180 days supply + 270 days, for a maximum gap of 450 days). Patients must have had no relapses in the last year on anti-CD20 mAb therapy or during the period between anti-CD20 and fumarate initiation and must have had ≥3 months of exposure to fumarate post-index (Figure 1).
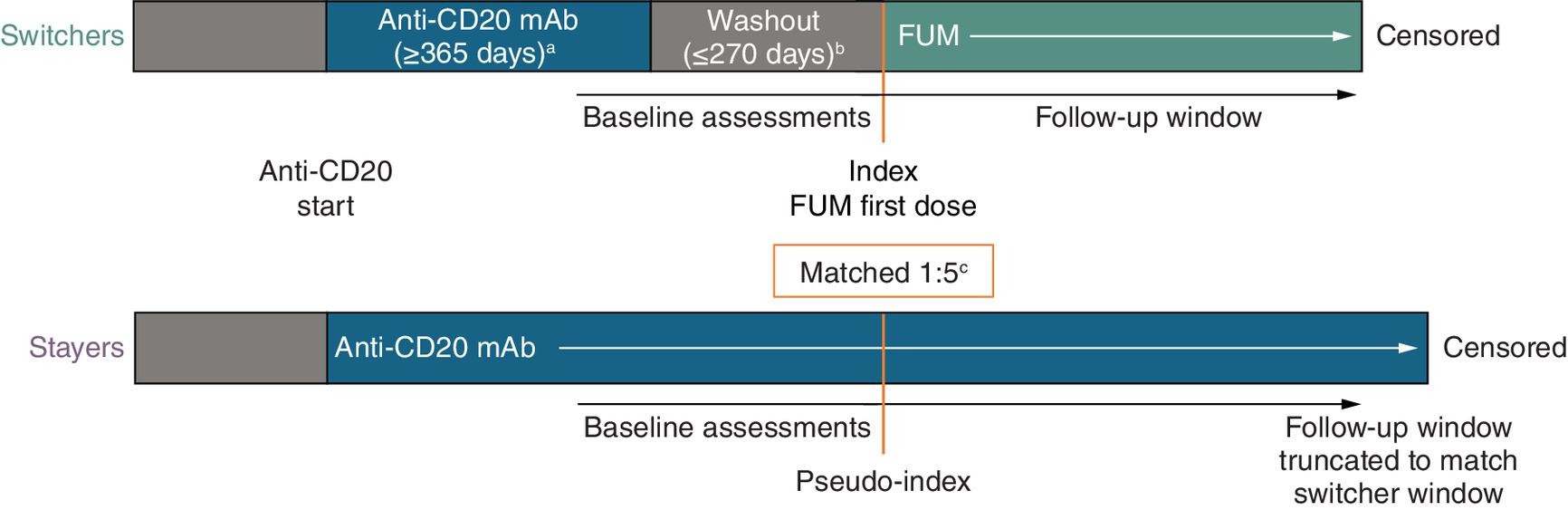
Figure 1. Study design.
aRequired ≥12 months on treatment with anti-CD20 mAb, without relapse during the treatment period and washout.
bWashout period is the duration between the end of anti-CD20 mAb exposure days’ supply and the first claim for a FUM.
cFor each Switcher, the best-matched five controls were selected: (1) from a pool of controls with anti-CD20 mAb exposure within 0–90 days of Switcher anti-CD20 mAb + FUM exposure; and (2) on propensity score matching plus baseline assessments evaluated at the time of switch/pseudo-index date. Pseudo-index date was derived for Stayers based on the index date for their matched pair in the Switchers group.
FUM: Fumarate; mAb: Monoclonal antibody.
Patients were propensity score matched at a ratio of 5:1 for those who stayed on anti-CD20 therapy (‘Stayers’) versus those who switched to a fumarate (‘Switchers’). Stayers were defined as all patients who had ≥1 year of exposure to anti-CD20 therapy and who did not have any relapse discernible via claims data during that first year of anti-CD20 exposure, and ≥1 year of continuous medical and pharmacy enrollment prior to anti-CD20 exposure. Patients who qualified for the fumarate Switchers group were excluded from the Stayers group. The index date for Stayers was derived based on the index date for their matched pair in the Switchers group (‘pseudo-index’). Baseline confounders included in the propensity score model were measured during the 12 months prior to index/pseudo-index date. Exact marginal distributions were specified for relapses, anti-CD20, sex and one or more infection encounters in the matching process. Infections were evaluated based on ICD-10 diagnosis codes recorded in the database. Age, MS Severity Score [17], Charlson Comorbidity Index, number of all-cause encounters, cost of all-cause encounters, number of infection encounters, costs of infection encounters, pre-anti-CD20 relapses and pre-anti-CD20 DMT type were included as variables in the propensity score model. Balance between baseline confounders was determined based on a standardized mean difference of <0.1. Patients were followed from index date to first occurrence of: end of study, end of insurance eligibility, gap in index DMT >45 days or switch from index DMT to another DMT.
Outcomes
The primary objectives were to describe clinical characteristics in the real-world setting and quantify annualized relapse rate (ARR), in patients with stable MS who switched from anti-CD20 mAbs to fumarates and in the matched cohort of patients who stayed on anti-CD20 mAb therapy. Relapse was defined as an MS-related inpatient claim with a primary diagnosis of MS, or an outpatient MS-related diagnosis and prescription claim for an intravenous steroid, adrenocorticotropic hormone, total plasma exchange or a high-dose oral corticosteroid ≤7 days after the outpatient visit. Mild relapses that did not prompt a patient to interact with the healthcare system are not captured in claims data. Subsequent relapses were counted, provided they occurred at least 30 days after the previous relapse event.
Secondary objectives included comparisons between matched cohorts of Switchers and Stayers of all-cause and infection-related post-index healthcare encounters (HCEs) and all-cause and infection-related post-index healthcare costs (HCCs). Healthcare claims were stratified by inpatient, outpatient, emergency room (ER) or other locations. Within each stratum, claims were windowed into 30-day intervals. The number of intervals where a patient experienced a claim was counted to derive the number of HCEs. HCCs were calculated as the summation of standardized costs associated with each claim (presented in 2022 USD) and did not include the costs of MS DMTs. HCEs and HCCs were annualized by dividing by the number of days followed then multiplying by 365.
Statistical analyses
Summary statistics were provided for baseline patient characteristics and demographics. For relapses and HCEs, the frequency and proportion of patients experiencing one or more event and mean annualized rate were presented. The mean annualized HCCs were also presented. Comparisons between Switchers and Stayers were calculated via generalized estimating equations accounting for matched-pair correlation. Odds ratios were estimated for binary variables and mean differences reported for continuous variables. HCEs and HCCs were reported overall (any location) and also by location. Statistical comparisons were made for the Switchers cohort (reference group) versus the Stayers cohort. Odds ratios <1 and mean differences <0 favor the Switchers cohort.
Compliance with ethics guidelines
This retrospective analysis was based on data collected as part of the Komodo Health Sentinel database, and therefore did not involve any new studies of human or animal subjects.
Results
Patients
This analysis included 108 patients who were stable on anti-CD20 mAb therapy and then switched to fumarates (Switchers), matched to 540 patients who remained on anti-CD20 mAb therapy (Stayers) (Figure 2). Baseline demographics, insurance plan type and disease characteristics were well balanced after matching. Mean (SD) MS severity score was 5.53 (2.93) for Stayers and 5.46 (2.80) for Switchers (standardized mean difference: 0.022) (Table 1). Mean (SD) Charlson Comorbidity Index was 0.53 (1.17) for the Stayer group and 0.46 (0.85) for the Switcher group (standardized mean difference: 0.062). In the Stayers cohort, a higher proportion of patients were DMT-naive prior to initiation of anti-CD20 mAb therapy, compared with the Switchers cohort; the proportion of patients with a relapse in the 1 year prior to anti-CD20 mAb treatment was similar in both cohorts. Mean (SD) age among this patient group was 48.5 (12.1) years for Switchers and 49.8 (15.1) years for Stayers.
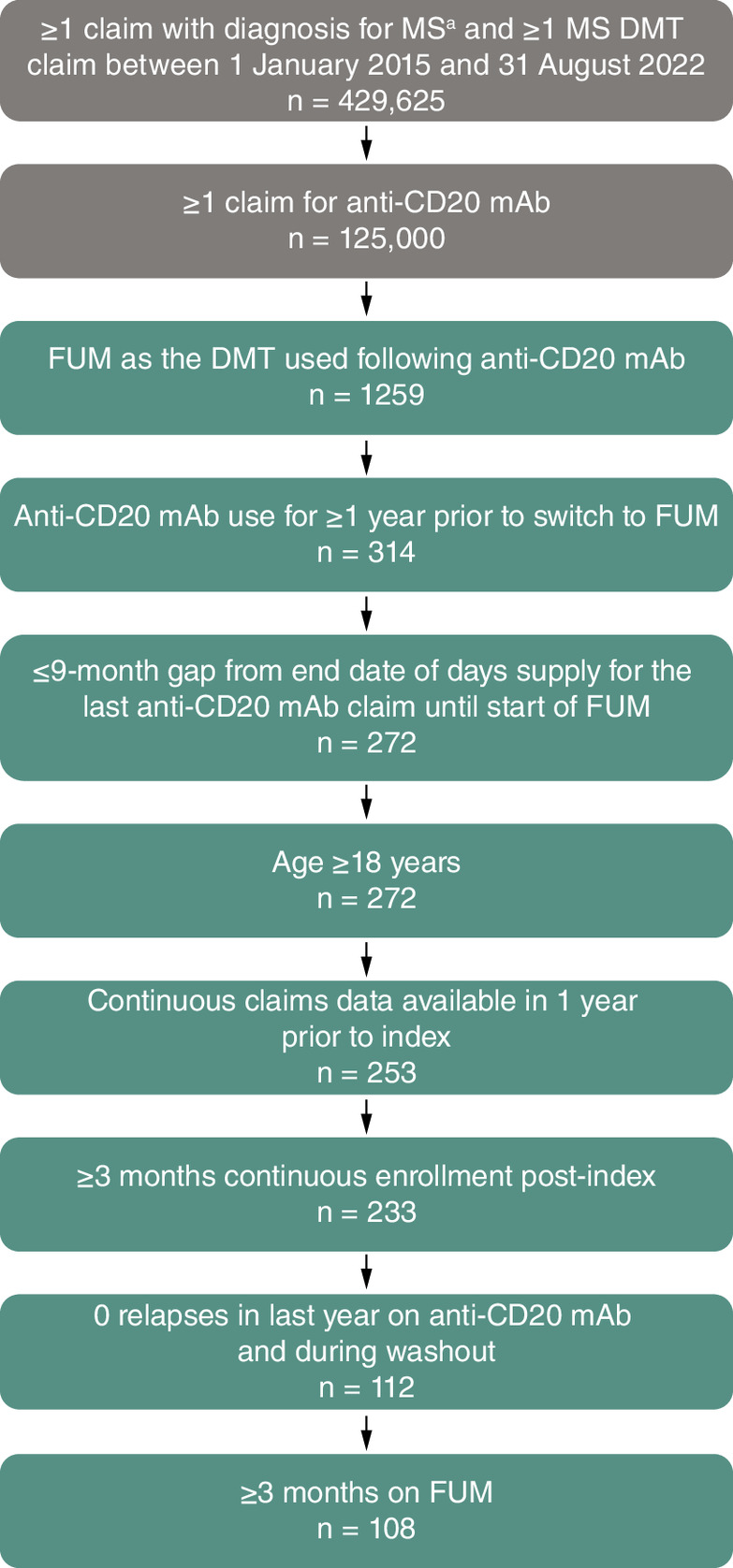
Figure 2. Study sample for Switchers and Stayers cohorts.
aICD-9-CM diagnosis code 340 or ICD-10 code G35.
DMT: Disease-modifying therapy; ICD-9-CM: International Classification of Diseases, Ninth Revision, Clinical Modification; FUM: Fumarate; mAb: Monoclonal antibody; MS: Multiple sclerosis.
| Demographics/characteristics | Anti-CD20 mAb Stayers (n = 540) | Anti-CD20 mAb to FUM Switchers (n = 108) | SMD |
|---|---|---|---|
| Age,† years, mean (SD) | 49.5 (14.0) | 49.4 (11.7) | 0.009 |
| Female,‡ n (%) | 380 (70.4) | 76 (70.4) | <0.001 |
| Race/ethnicity, n (%) | n = 386 | n = 83 | 0.208 |
| White | 277 (71.8) | 64 (77.1) | |
| Black | 59 (15.3) | 13 (15.7) | |
| Hispanic | 24 (6.2) | 3 (3.6) | |
| Asian or Pacific Islander | 7 (1.8) | 1 (1.2) | |
| Other | 19 (4.9) | 2 (2.4) | |
| MS Severity Score†,§, mean (SD) | 5.53 (2.93) | 5.46 (2.80) | 0.022 |
| Anti-CD20 mAb‡, n (%) | <0.001 | ||
| Rituximab | 30 (5.6) | 6 (5.6) | |
| Ocrelizumab | 505 (93.5) | 101 (93.5) | |
| Rituximab then ocrelizumab | 5 (1) | 1 (1) | |
| Ofatumumab | 0 (0) | 0 (0) | |
| Initial FUM used after anti-CD20, n (%) | N/A | ||
| Dimethyl fumarate | N/A | 69 (63.9) | |
| Diroximel fumarate | N/A | 39 (36.1) | |
| Duration of anti-CD20 exposure prior to index date (switch date), days, mean (SD) | N/A | 730.1 (317.2) | N/A |
| Duration of anti-CD20 exposure prior to pseudo-index date, days, mean (SD) | 730.1 (316.0) | N/A | N/A |
| Duration from last anti-CD20 exposure to index date (switch date), days, mean (SD) | N/A | 123.7 (104.6) | N/A |
| Baseline HCEs prior to index/pseudo-index date | |||
| All-cause HCEs†, mean (SD) | 7.98 (4.10) | 8.20 (3.88) | 0.057 |
| Cost of all-cause HCEs†, USD, mean (SD) | 11,516 (30,593) | 12,278 (20,957) | 0.029 |
| Infection-related HCEs‡, n (%) | 275 (50.9) | 55 (50.9) | <0.001 |
| Infection-related HCEs†, mean (SD) | 1.46 (2.39) | 1.56 (2.48) | 0.04 |
| Cost of infection-related HCEs†, USD, mean (SD) | 3037 (19,271) | 2611 (8969) | 0.028 |
| Comorbidities (≥3.0% in either cohort), n (%) | |||
| Chronic pulmonary disease | 54 (10.0) | 12 (11.1) | 0.036 |
| Paraplegia and hemiplegia | 34 (6.3) | 7 (6.5) | 0.008 |
| Diabetes without complications | 33 (6.1) | 6 (5.6) | 0.024 |
| Peripheral vascular disease | 29 (5.4) | 6 (5.6) | 0.008 |
| Cerebrovascular disease | 22 (4.1) | 3 (2.8) | 0.071 |
| Diabetes with complications | 17 (3.1) | 4 (3.7) | 0.031 |
| Mild liver disease | 18 (3.3) | 4 (3.7) | 0.02 |
| Rheumatic disease | 15 (2.8) | 5 (4.6) | 0.098 |
| Charlson Comorbidity Index†, mean (SD) | 0.53 (1.17) | 0.46 (0.85) | 0.062 |
| Any relapse 1 year prior to anti-CD20 mAb†, n (%) | n = 533 80 (15.0) | n = 99 15 (15.2) | 0.004 |
| Pre-anti-CD20 mAb DMT type†, n/N (%) | n = 533 | n = 99 | 0.276 |
| Injectable | 109 (20.5) | 23 (23.2) | |
| IV | 65 (12.2) | 9 (9.1) | |
| Oral | 205 (38.5) | 48 (48.5) | |
| None | 154 (28.9) | 19 (19.2) |
†
Variable included as a covariate in the PSM modeling process.
‡
Variable exactly matched in the PSM modeling process.
§
MS severity score is derived from a previously published algorithm. The algorithm uses the binary presences of MS symptoms, DMT utilization, durable medical equipment utilization, MS-related hospitalizations and MS relapses as MS disease severity predictors. MS severity score ranges from 0 to 22; a score of 0–4 indicates low MS severity, 5–10 indicates moderate MS severity and ≥11 indicates high MS severity [18].
DMT: Disease-modifying therapy; FUM: Fumarate; HCE: Healthcare encounter; IQR: Interquartile range; IV: Intravenous; mAb: Monoclonal antibody; MS: Multiple sclerosis; N/A: Not applicable; PSM: Propensity score matching; SMD: Standardized mean difference; USD: US dollar.
The mean (SD; range) duration of anti-CD20 mAb exposure prior to switching to a fumarate was 730.1 (317.2; 361–1778) days, and the mean (SD; range) duration of anti-CD20 mAb exposure prior to pseudo-index in the Stayer group was 730.1 (316.0; 361–1778) days (Table 1). In the Switchers group, the mean (SD; range) duration from last dose of anti-CD20 mAb to fumarate initiation was 123.7 (104.6; 1–452) days (Table 1). The mean (SD; range) duration of fumarate exposure was 341.4 (250.0; 87–1240) days. Total post-index follow-up time in the Stayers group was matched exactly to the Switchers group. The mean duration of exposure for the anti-CD20 Stayer cohort was 1071.5 (365.1; 460–1929) days.
Relapses
There was no significant difference in ARR between the Switchers and Stayers cohorts during the follow-up period (Figure 3); mean (SD) ARR was 0.14 (0.5) for Switchers and 0.08 (0.41) for Stayers (p = 0.3). Of patients who switched from anti-CD20 mAb to a fumarate, 11/108 (10.2%) experienced a relapse during the follow-up period; 36/540 (6.7%) patients who stayed on anti-CD20 mAb therapy experienced a relapse (odds ratio: 1.62; p = 0.19). Mean (SD) time to first relapse post-index date was 189.7 (131.5) days for Switchers and 250.8 (187.8) days for Stayers. The Kaplan–Meier estimated proportions of patients relapse free at 6 months were 94.9% (95% confidence interval [CI]: 90.7%; 99.4%) in the Switcher group and 96.4% (95% CI: 94.7%; 98.1%) in the Stayer group (p = 0.20); at 12 months, the estimated proportions relapse free were 89.0% (95% CI: 82.2%; 96.3%) in the Switcher group and 91.9% (95% CI: 88.9%; 95.0%) in the Stayer group (p = 0.20). Of the 11 patients in the Switchers group who experienced a relapse, two patients experienced a relapse event within the first 3 months after switching and had 180 days and 412 days between their last dose of anti-CD20 and their first dose of fumarate. These two patients remained on fumarate treatment after the relapse occurred.
![Bar graph comparing the annualized relapse ratebetween Stayers (anti-CD20 monoclonal antibody [mAb] only) and Switchers (anti-CD20 mAb to fumarate).](/cms/10.57264/cer-2024-0071/asset/d72ac3f0-9c3c-4239-a460-c709d89fccd4/assets/images/large/figure3.jpg)
Figure 3. Annualized relapse rate.
Relapses were captured if they resulted in a patient having an outpatient visit with their multiple sclerosis clinician, an inpatient hospital stay, an emergency room visit, or intravenous steroid use. Mild relapses that did not prompt a patient to interact with the healthcare system were not captured in claims data.
ARR: Annualized relapse rate; CI: Confidence interval; FUM: Fumarate; mAb: Monoclonal antibody; SD: Standard deviation.
HCEs & HCCs
The annualized rate of all-cause HCEs and annualized all-cause HCCs were similar between patient cohorts. Mean (SD) annualized rate of all-cause HCEs was 8.08 (4.62) in the Switchers cohort and 7.67 (4.42) in the Stayers cohort (p = 0.29). Mean (SD) annualized all-cause HCCs were $20,634 ($37,679) for the Switchers and $20,147 ($70,199) for the Stayers (p = 0.89). Across ER, inpatient and outpatient settings, there were no significant differences in all-cause HCEs or all-cause HCCs between the cohorts.
Overall, the probability of experiencing ≥1 infection-related HCE was not significantly different between the Switchers and Stayers cohorts (odds ratio: 0.77; p = 0.2) (Figure 4). Annualized rates of infection-related HCEs overall (any location) were not significantly different between the two cohorts (mean [SD]: Switchers, 1.12 [2.25]; Stayers, 1.17 [2.15]; mean difference: -0.05; p = 0.79) (Figure 5). There were no significant differences in rates of infection-related HCEs between cohorts in the ER or outpatient settings. However, in the inpatient setting, Switchers demonstrated a lower annualized rate of infection-related HCEs (mean [SD]: Switchers, 0.01 [0.09]; Stayers, 0.06 [0.35]; mean difference: -0.05; p = 0.005).
![Forest plot showing the odds ratios forinfection-related healthcare encounters in Switchers (anti-CD20 monoclonal antibody [mAb] to fumarate) versus Stayers (anti-CD20 mAb only).](/cms/10.57264/cer-2024-0071/asset/86d61d98-c3c1-41ea-b43e-3b3887aa29ed/assets/images/large/figure4.jpg)
Figure 4. Probability of infection-related healthcare encounters for Switchers versus Stayers.
ER: Emergency room.
![Bar charts comparing the annualized mean rate ofinfection-related healthcare encounters between Stayers (anti-CD20 monoclonal antibody [mAb] only) and Switchers (anti-CD20 mAb to fumarate) overall, and across different settings: outpatient, inpatient and emergency room.](/cms/10.57264/cer-2024-0071/asset/d5dfc47c-34a2-48fd-ab5d-bdbe059ce202/assets/images/large/figure5.jpg)
Figure 5. Annualized rate of infection-related healthcare encounters.
ER: Emergency room; HCE: Healthcare encounter.
Annualized infection-related HCCs overall were lower in the Switchers cohort than in the Stayers cohort (mean [SD]: Switchers, $543 [$1932]; Stayers, $2954 [$18,063]; mean difference: -$2412; p = 0.002) (Figure 6). In the inpatient setting, annualized infection-related HCCs were significantly lower in the Switchers cohort than in the Stayers cohort (mean [SD]: Switchers, $70 [$729]; Stayers, $2396 [$17,628]; mean difference: -$2325; p = 0.002). No significant differences in annualized infection-related HCCs were observed between the cohorts in the ER or outpatient settings.
![Bar charts comparing the annualized mean cost (in USD)of infection-related healthcare encounters between Stayers (anti-CD20 monoclonal antibody [mAb] only) and Switchers (anti-CD20 mAb to fumarate) overall, and across different settings: outpatient, inpatient and emergency room.](/cms/10.57264/cer-2024-0071/asset/fdd88415-bf6e-4919-ad28-f354038d8e8a/assets/images/large/figure6.jpg)
Figure 6. Annualized cost of infection-related healthcare encounters.
Costs of healthcare encounters did not include the cost of multiple sclerosis disease-modifying therapies.
ER: Emergency room; USD: US Dollar.
There was one (0.9%) patient hospitalized (inpatient) for infections in the Switchers cohort, and 21 (3.9%) in the Stayers cohort (Table 2). For the Switcher patient with the infection-related inpatient hospitalization, infection types (percentage of overall Switcher cohort) included urinary tract infection (0.9%), sepsis (0.9%) and Escherichia coli (0.9%); washout period was 108 days between last dose of anti-CD20 mAb and first dose of fumarate. For Stayers, the most common infection types (n; % of overall Stayer cohort) included COVID-19 (n = 13; 2.4%), sepsis (n = 7; 1.3%) and pneumonia (n = 4; 0.7%). From date of switch to fumarate (index) or pseudo-index date, mean (SD) time to inpatient hospitalization for infection was 50.0 (0.0) days for the Switcher patient (n = 1) and 268.6 (210.3) days for Stayers (n = 21). Mean (SD) duration of inpatient hospitalization stay for infection was 1.0 (0.0) day in the Switchers cohort and 9.9 (10.9) days in the Stayers cohort.
| Infection-related hospitalization | Anti-CD20 mAb Stayers | Anti-CD20 mAb to FUM Switchers |
|---|---|---|
| Patients with infection-related hospitalization, n (%)‡ | 21/540 (3.9) | 1/108 (0.9) |
| Infection type, n (% of overall population)§ | ||
| COVID-19 | 13 (2.4) | 0 |
| Sepsis | 7 (1.3) | 1 (0.9) |
| Pneumonia | 4 (0.7) | 0 |
| Intestinal infection | 3 (0.6) | 0 |
| Cellulitis of lower limb | 2 (0.4) | 0 |
| Urinary tract infection | 1 (0.2) | 1 (0.9) |
| Escherichia coli | 1 (0.2) | 1 (0.9) |
†
ICD-10 codes from infection first-position diagnosis codes for emergency room/inpatient hospitalizations.
‡
A hospitalization could have multiple infection claims for different infection types. For each infection type, individual patients were counted once; one patient was hospitalized twice in the Stayer group.
§
No other infection-related inpatient hospitalizations for the Switchers. For the Stayers, additional infections resulting in hospitalization included: streptococcus 1 (0.2), sequelae of other specified infectious and parasitic diseases 1 (0.2), chronic obstructive pulmonary disease with (acute) lower respiratory infection 1 (0.2) and peritonitis 1 (0.2).
FUM: Fumarate; ICD-10: International Classification of Diseases, Tenth Revision; mAb: Monoclonal antibody.
Discussion
This retrospective analysis of the Komodo Health Sentinel database assessed relapses and annualized HCEs (including infections) and HCCs in 108 clinically stable patients with MS who switched from anti-CD20 mAbs to a fumarate (Switchers) and a matched cohort of 540 patients who stayed on anti-CD20 mAbs (Stayers). After an average of approximately 1 year of post-index follow-up, there was no significant difference in relapse rates between Switcher and Stayer cohorts. This finding is consistent with previous studies of patients switching from anti-CD20 mAbs to fumarates [19,20]. In 25 patients with stable relapsing-remitting MS who switched from ocrelizumab to DRF, no relapses occurred over 1 year of follow-up [19]. A retrospective chart review of ten patients with MS who switched from rituximab or ocrelizumab to DMF reported that eight patients remained free from relapses and MRI activity with follow-up of ≤24 months; relapses occurred in one patient who discontinued DMF, and MRI activity was reported in one patient [20]. In both of these studies, the median duration between discontinuation of anti-CD20s to initiation of fumarate therapy was approximately 7 months [19,20].
In this study, two patients in the Switchers group experienced a relapse within 3 months following switch from anti-CD20 mAbs to fumarates. Several possible explanations could be explored, including return of disease activity with long duration from prior therapy dose, higher disease activity in patient selected for switch, or potential early relapse prior to onset of efficacy for fumarate switch. The latter might only be applicable as a potential explanation for very early relapse post switch, as onset of efficacy for DMF has been shown as early as 10 weeks and onset of efficacy for DRF within 7 weeks [21,22]. The two patients who experienced a relapse within 3 months following switch had durations of 180 days and 412 days between their last dose of anti-CD20 mAb and their first dose of fumarate. It is not possible to determine whether the duration between treatments had any effect on the occurrence of relapses, given the small numbers involved and limitations inherent to claims data whereby patient-level details are limited.
Annualized rates of infection-related HCEs were significantly lower in the Switchers cohort than in the Stayers cohort in the inpatient setting. No significant differences were observed between cohorts in overall rates of infection-related HCEs, or in rates of infection-related HCEs in the outpatient and ER settings. Annualized costs of HCEs were lower among Switchers compared with Stayers; this was mostly driven by the much lower annual costs of infection-related inpatient HCEs observed in the Switchers cohort. Duration of inpatient hospitalization stay for infection was significantly different between the groups, with a mean of 1.0 day for Switchers and 9.9 days for Stayers. Together, these data suggest that the reduced rate of infection-related inpatient HCEs in patients who switched from anti-CD20 mAbs to fumarates has a significant downstream effect in terms of costs of infection-related HCEs overall. Notably, in the Stayers group there were 13 (2.4%) patients hospitalized due to COVID-19 and seven (1.3%) patients hospitalized due to sepsis, while in the Switchers group there were zero hospitalizations due to COVID-19 and one (0.9%) due to sepsis. Infections requiring hospitalization are considered to be serious adverse events [23]. These results are also consistent with a prior study comparing infection-related healthcare resource utilization and HCCs between DMF and ocrelizumab, where the largest differences were observed in the inpatient-related infections [24].
Anti-CD20 mAbs are associated with an increased risk of infections, due to the depletion of B-cells fundamental to their therapeutic mechanism of action, and in some cases, hypogammaglobulinemia. This includes greater risks of severe COVID-19, and hospitalizations and intensive care unit admissions due to COVID-19, when compared with other DMTs including DMF [10,25,26]. Therefore, the lower rate of infection-related HCEs observed for the Switcher cohort in the inpatient setting may indicate reconstitution of B-cells following the switch from anti-CD20 mAb to fumarate, and a subsequent restoration of the immune response to infection. This may account for the shorter inpatient stays and lower HCCs observed in the Switcher cohort compared with the Stayer cohort. Surveillance for infection should be implemented for patients switching from anti-CD20 mAbs to another DMT, and B-cell repletion monitored, to ensure early intervention if infection is suspected during the early months on the new DMT. Although this analysis did not allow for assessment of B-cells, a prior study demonstrated B-cell reconstitution over a duration of 1 year after switching from anti-CD20 mAb to DRF [19].
An interesting real-world observation in the data presented here is that anti-CD20 mAb use was seen in naive patients (28.9% of Stayers; 19.2% of Switchers); mean ages were comparable between these two groups (49.8 and 48.5 years, respectively). There is an assumption often made that anti-CD20 mAbs are reserved for moderate/severe patients or later in disease course. This data shows evidence of early adoption. Early use of anti-CD20 mAbs may indicate an approach of early initiation of high-efficacy therapy, with potential rationale for younger patients or newly diagnosed patients with moderate/severe disease, in order to mitigate age-associated risks of infection (immunosenescence), and impaired vaccine response in older patients [27]. In patients who cannot tolerate anti-CD20 mAbs or are at high risk for infections with prolonged use, it may be beneficial to switch to a medication with an improved long-term safety profile.
The DISCO-MS study, a multicenter, randomized, controlled, noninferiority trial examining discontinuation of DMT in patients aged 55 years or older with stable MS, was unable to conclude whether DMT cessation was noninferior to continuation of DMT [28]. The negative outcome of the DISCO-MS study highlights the need for additional research on treatment strategies when a transition from a high-efficacy DMT is warranted. While de-escalation might be especially useful in patients experiencing immunosenescence, it may also be useful for stable patients of any age if there are safety concerns related to long-term immune suppression, such as the risk of infections or reduced response to vaccination.
Limitations of the current study include those inherent to analyses of claims data – for example, the absence of randomization, possible coding errors, the inability to verify reported diagnoses, and challenges associated with evaluating MS disease severity and disability level. Even though MS Severity Score uses disability and disease duration to rate disease severity [17], we acknowledge that clinical disability level in claims-based data is limited and calls for caution in interpretation of results. Claims databases do not allow for analysis of MRI outcomes, so it is not possible to determine whether differences could have been observed in MRI activity in this population. However, a single-center retrospective study [29] evaluated patients with MS who had been stable on ocrelizumab and who subsequently switched to diroximel fumarate due to concerns related to B-cell depletion during the COVID-19 pandemic; in that study, MRI outcomes remained stable 1-year after switching from ocrelizumab to diroximel fumarate. Although propensity score methods can be used to balance groups for comparative analyses, there may be biases that the available covariates do not address; in addition, while balance was achieved on most covariates in this analysis, some differences were still present, with the Stayers cohort having a higher proportion of patients who were naive to prior DMTs before initiating an anti-CD20 mAb DMT. While race/ethnicity was not a variable in the propensity score match, the patient distribution was relatively similar for the two cohorts, although there was a higher percentage of Hispanic patients in the Stayer group compared with the Switcher group (6.2 vs 3.6%, respectively). Another challenge with claims data is that it cannot inform on reasons why a stable patient has made a switch in DMT; therefore, although we are confident that we have captured patients who switched due to nonefficacy reasons by ensuring that patients were stable with no relapses during anti-CD20 mAb treatment, we do not know the specific nonefficacy reason for switching (e.g., tolerability, safety, insurance coverage, route of administration challenges, concern for vaccine response, age, transportation issues, or another reason).
Due to B-cell depletion persisting after discontinuation of anti-CD20 mAbs, treatment with anti-CD20 mAbs could potentially have a carry-over effect in patients who switch from anti-CD20 mAbs to another therapy [30–33]. Recent studies suggest that this carry-over effect may persist after B-cell repopulation in the peripheral blood, as evidenced by low relapse rates in patients who discontinued anti-CD20 mAb DMTs [32,33]. In our study, the average washout duration was approximately 4 months, with average duration on fumarates of approximately 11 months, combining to an average overall follow-up post anti-CD20 mAb treatment of over 1 year. It is possible that the low relapse rate observed in the Switchers cohort was less likely to be driven by a carryover effect of anti-CD20 mAbs on B-cells, however, the potential contribution of a carryover effect cannot be ruled out. Studies with longer follow-up time would be useful to confirm these findings.
This analysis also did not include data for neurological examinations or radiological outcomes either pre- or post-switch; however, small retrospective studies have indicated stability in radiological outcomes, cognitive assessments and patient-reported outcomes in patients with MS who switched from anti-CD20 mAbs to fumarates [19,20]. Relapses were captured if they resulted in a patient having an outpatient visit, an inpatient hospital stay, or an ER visit; however, relapses that did not prompt a patient to interact with the healthcare system would not be captured in the claims data. A limitation regarding the relapse data could be misclassification bias whereby relapses during treatment with a high-efficacy therapy may be classified differently than with a moderate-efficacy therapy [34]. It is possible that a patient presenting with neurological symptoms may prompt a clinician to label those symptoms as a relapse when a patient is not on a high-efficacy therapy, while those same symptoms may be more likely to be considered as a pseudo-relapse when a patient is on a high-efficacy therapy.
Despite these limitations, analysis of claims data is a valuable tool that has been applied previously to assess DMT treatment patterns, relapses, healthcare resource utilization and costs in the real-world clinical care of patients with MS [35–37]. Our analysis is the first claims-based study evaluating stable patients who transition from anti-CD20 mAb therapy to a fumarate and the first study conducted to date that compares outcomes between an anti-CD20 mAb to fumarate switch group versus a matched group that stayed on anti-CD20 mAb therapy. In the absence of randomized trial data, this study provides evidence to support that switching from anti-CD20 mAbs to fumarates in patients who have been clinically stable can provide benefits associated with fewer infection-related inpatient HCEs and lower infection-related HCCs, while maintaining effectiveness in terms of relapse rate.
Summary points
•
Anti-CD20 monoclonal antibodies (mAbs) and fumarates are commonly used disease-modifying therapies (DMTs) for multiple sclerosis (MS). Switching between DMTs is a common clinical strategy for optimizing individual patient outcomes.
•
Earlier intervention with high-efficacy therapies may improve long-term clinical outcomes, but switching may be considered due to safety concerns such as the risk of infection.
•
A de-escalating treatment approach involves switching from a high-efficacy DMT, such as an anti-CD20 mAb, to a moderate- or low-efficacy agent; however, data on switching from anti-CD20 mAbs to other DMTs are limited.
•
This retrospective, observational study of the Komodo Health Sentinel database assessed relapses, healthcare encounters (HCEs) and healthcare costs (HCCs) in a cohort of patients with stable MS who switched from anti-CD20 mAbs to fumarates compared with a matched cohort of patients who stayed on anti-CD20 mAbs.
•
The analysis included 108 ‘Switchers’ matched to 540 ‘Stayers’; baseline demographics and disease characteristics were well balanced after matching.
•
No significant difference was observed in annualized relapse rate between ‘Switchers’ and ‘Stayers’, and rates of HCEs and HCCs were similar between cohorts.
•
However, Switchers had lower rates of infection-related HCEs in the inpatient setting, and lower infection-related HCCs both overall and in the inpatient setting.
•
This study provides evidence that switching from anti-CD20 mAbs to fumarates, in patients who have been clinically stable, can provide benefits associated with fewer infection-related inpatient HCEs and lower infection-related HCCs, while maintaining effectiveness in terms of relapse rate.
Author contributions
All authors contributed to the investigation, critically reviewed, edited each draft of the manuscript and approved the final version for publication. Formal analysis was conducted by N Belviso, Yu Zhang, JB Lewin and SM England. JB Lewin and SM England were responsible for conceptualization and the methodology.
Acknowledgments
Some of these data were reported previously as a poster at the Consortium of Multiple Sclerosis Centers (CMSC) 2023 Annual Meeting, 31 May–4 June 2023 (CO, USA).
Financial disclosure
Biogen (MA, USA) sponsored this study and provided funding for medical writing and editorial support in the development of this paper. The authors had full editorial control of the paper and provided their final approval of all content. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
ABB Zacharia: consulting fees from Biogen, EMD Serono, Greenwich Biosciences and TG Therapeutics. JJ Feng: consulting fees from Bristol Myers Squibb, Horizon, Novartis and TG Therapeutics. BP Moss: contracted research for Genentech and Novartis; consulting fees from Biogen; and stock/stock options in Pfizer. N Belviso, JP Mendoza, JB Lewin and SM England: full-time employees of and hold stock/stock options in Biogen. Y Zhang and F Branco: full-time employees of and held stock/stock options in Biogen when this work was conducted. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by D Pertab, Excel Scientific Solutions (Glasgow, UK) and editorial support was provided by C Farrell, Excel Scientific Solutions (CT, USA); funding was provided by Biogen (MA, USA).
Ethical conduct of research
This retrospective analysis was based on data collected from the Komodo Health Sentinel database, and therefore did not involve any new studies of human or animal subjects.
Data sharing statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Open access
This work is licensed under the Attribution-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.pdf)
- Download
- 1.41 MB
References
Papers of special note have been highlighted as: • of interest
1.
Multiple Sclerosis Coalition. The use of disease-modifying therapies in multiple sclerosis: principles and current evidence. (2019). https://ms-coalition.org/wp-content/uploads/2019/06/MSC_DMTPaper_062019.pdf
2.
Grand'Maison F, Yeung M, Morrow SA et al. Sequencing of high-efficacy disease-modifying therapies in multiple sclerosis: perspectives and approaches. Neural. Regen. Res. 13(11), 1871–1874 (2018).
• Review discussing existing disease-modifying therapies (DMTs) and the different clinical approaches for treating patients with multiple sclerosis (MS), including considerations for the selection and sequencing of DMTs.
3.
Fox RJ, Mehta R, Pham T et al. Real-world disease-modifying therapy pathways from administrative claims data in patients with multiple sclerosis. BMC Neurol. 22(1), 211 (2022).
• Claims-based analysis of DMT treatment pathways for patients with newly diagnosed MS in the US, which reported that approximately 70% of patients switched or discontinued DMT during a follow-up period of 2–10.5 years.
4.
Burton JM, Freedman MS. The shifting landscape of disease-modifying therapies for relapsing multiple sclerosis. J. Neuroophthalmol. 38(2), 210–216 (2018).
5.
Mäurer M, Tiel-Wilck K, Oehm E et al. Reasons to switch: a noninterventional study evaluating immunotherapy switches in a large german multicentre cohort of patients with relapsing-remitting multiple sclerosis. Ther. Adv. Neurol. Disord. 12, 1756286419892077 (2019).
• A noninterventional study to investigate reasons for switching DMT in 595 patients with relapsing-remitting MS in Germany; most commonly cited reasons were failure of current therapy, patient wish and adverse events.
6.
Sipilä JOT. Treatment courses of patients newly diagnosed with multiple sclerosis in 2012–2018. J. Clin. Med. 12(2), 595 (2023).
7.
Smith AL, Cohen JA, Hua LH. Therapeutic targets for multiple sclerosis: current treatment goals and future directions. Neurotherapeutics 14(4), 952–960 (2017).
8.
Pandit L. No evidence of disease activity (NEDA) in multiple sclerosis – shifting the goal posts. Ann. Indian Acad. Neurol. 22(3), 261–263 (2019).
9.
Sharrad D, Chugh P, Slee M, Bacchi S. Defining progression independent of relapse activity (PIRA) in adult patients with relapsing multiple sclerosis: a systematic review. Mult. Scler. Relat. Disord. 78, 104899 (2023).
10.
Freeman L, Longbrake EE, Coyle PK, Hendin B, Vollmer T. High-efficacy therapies for treatment-naïve individuals with relapsing-remitting multiple sclerosis. CNS Drugs 36(12), 1285–1299 (2022).
11.
Prosperini L, Mancinelli CR, Solaro CM et al. Induction versus escalation in multiple sclerosis: a 10-year real world study. Neurotherapeutics 17(3), 994–1004 (2020).
• This retrospective study of registry data used propensity score matching to compare long-term outcomes for patients with active MS who followed an escalation-based treatment strategy versus those who followed an induction-based strategy. Disability outcomes were favorable for induction versus escalation, but the induction approach was associated with a worse safety profile.
12.
Henderson M, Horton DB, Bhise V et al. Initiation patterns of disease-modifying therapies for multiple sclerosis among us adults and children, 2001 through 2020. JAMA Neurol. 80(8), 860–867 (2023).
13.
Thebault S, Gandelman S, Lane C et al. Severe neuroinvasive west nile virus in association with anti-cd20 monotherapy for multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 10(5), e200154 (2023).
14.
Sormani MP, Schiavetti I, Carmisciano L et al. Covid-19 severity in multiple sclerosis: putting data into context. Neurol. Neuroimmunol. Neuroinflamm. 9(1), e1105 (2022).
15.
Schiavetti I, Ponzano M, Signori A et al. Severe outcomes of Covid-19 among patients with multiple sclerosis under anti-cd-20 therapies: a systematic review and meta-analysis. Mult. Scler. Relat. Disord. 57, 103358 (2022).
16.
Salter A, Fox RJ, Newsome SD et al. Outcomes and risk factors associated with sars-cov-2 infection in a north american registry of patients with multiple sclerosis. JAMA Neurol. 78(6), 699–708 (2021).
17.
Roxburgh RH, Seaman SR, Masterman T et al. Multiple sclerosis severity score: using disability and disease duration to rate disease severity. Neurology 64(7), 1144–1151 (2005).
18.
Toliver JC, Barner JC, Lawson KA, Rascati KL. Use of a claims-based algorithm to estimate disease severity in the multiple sclerosis medicare population. Mult. Scler. Relat. Disord. 49, 102741 (2021).
19.
Kaczmarek O, Sethi A, Teng E et al. Disease modifying therapy choice in people with multiple sclerosis in the era of Covid: characterizing outcomes in patients who switched from anti-cd20 therapies to diroximel fumarate. Poster p129 presented at the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS) Forum 2022, FL, USA, 24–26 February 2022.
20.
Vollmer B, Riddle E, Mendoza J, Alvarez E. Retrospective evaluation of de-escalation from anti-cd20 therapies to fumarates as a treatment approach. Poster p3.003 presented at the 74th Annual Meeting of the American Academy of Neurology (AAN), WA, USA, 2–7 April 2022.
21.
Kappos L, Giovannoni G, Gold R et al. Time course of clinical and neuroradiological effects of delayed-release dimethyl fumarate in multiple sclerosis. Eur. J. Neurol. 22(4), 664–671 (2015).
22.
Singer BA, Shafer SJ, Arnold DL et al. Diroximel fumarate and dimethyl fumarate demonstrate early radiological efficacy in relapsing-remitting multiple sclerosis (2190). Neurology 96(Suppl. 15), 2190 (2021).
23.
US Food & Drug Administration. What is a serious adverse event? 18 May 2023. https://www.fda.gov/safety/reporting-serious-problems-fda/what-serious-adverse-event
24.
Nicholas JA, Gudesblatt M, Garabedian M et al. Dimethyl fumarate is associated with lower rates of infection and lower infection-related healthcare costs when compared with ocrelizumab. Mult. Scler. Relat. Disord. 63, 103921 (2022).
• Insurance-based PS-matching analysis that indicated lower annualized infection rates and lower annualized infection-related healthcare costs in patients with MS who received treatment with dimethyl fumarate compared with those who received ocrelizumab.
25.
Simpson-Yap S, De Brouwer E, Kalincik T et al. Associations of disease-modifying therapies with Covid-19 severity in multiple sclerosis. Neurology 97(19), e1870–e1885 (2021).
26.
Sormani MP, De Rossi N, Schiavetti I et al. Disease-modifying therapies and coronavirus disease 2019 severity in multiple sclerosis. Ann. Neurol. 89(4), 780–789 (2021).
27.
Lycke J, Svenningsson A. Long-term treatment with anti-cd20 monoclonal antibodies is untenable because of risk: commentary. Mult. Scler. 28(8), 1177–1178 (2022).
28.
Corboy JR, Fox RJ, Kister I et al. Risk of new disease activity in patients with multiple sclerosis who continue or discontinue disease-modifying therapies (discoms): a multicentre, randomised, single-blind, Phase IV, non-inferiority trial. Lancet Neurol. 22(7), 568–577 (2023).
29.
Gudesblatt M, Bumstead B, Buhse M et al. De-escalation of disease-modifying therapy for people with multiple sclerosis due to safety considerations: characterizing 1-year outcomes in 25 people who switched from ocrelizumab to diroximel fumarate. Adv Ther. 41(8), 3059–3075 (2024).
30.
Moser T, O'Sullivan C, Otto F et al. Long-term immunological consequences of anti-cd20 therapies on humoral responses to Covid-19 vaccines in multiple sclerosis: an observational study. Ther. Adv. Neurol. Disord. 15, 17562864221092092 (2022).
31.
Boremalm M, Sundstrom P, Salzer J. Discontinuation and dose reduction of rituximab in relapsing-remitting multiple sclerosis. J. Neurol. 268(6), 2161–2168 (2021).
32.
Kappos L, Traboulsee A, Li DKB et al. Ocrelizumab exposure in relapsing-remitting multiple sclerosis: 10-year analysis of the Phase II randomized clinical trial and its extension. J. Neurol. 271(2), 642–657 (2024).
33.
Starvaggi Cucuzza C, Longinetti E, Ruffin N et al. Sustained low relapse rate with highly variable b-cell repopulation dynamics with extended rituximab dosing intervals in multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 10(1), e200056 (2023).
34.
Pham A, Cummings M, Lindeman C, Drummond N, Williamson T. Recognizing misclassification bias in research and medical practice. Fam. Pract. 36(6), 804–807 (2019).
35.
Bergvall N, Makin C, Lahoz R et al. Comparative effectiveness of fingolimod versus interferons or glatiramer acetate for relapse rates in multiple sclerosis: a retrospective US claims database analysis. Curr. Med. Res. Opin. 29(12), 1647–1656 (2013).
36.
Freeman L, Kee A, Tian M, Mehta R. Retrospective claims analysis of treatment patterns, relapse, utilization, and cost among patients with multiple sclerosis initiating second-line disease-modifying therapy. Drugs Real World Outcomes 8(4), 497–508 (2021).
• Retrospective claims analysis of treatment patterns, relapses, healthcare resource utilization and healthcare costs among patients with MS initiating second-line DMT. Patients who switched to oral DMTs had higher persistence and adherence compared with those who switched to injectable DMTs.
37.
Araujo L, Kyatham S, Bzdek KG, Higuchi K, Greene N. Health economic outcomes of switching to alemtuzumab from other disease-modifying therapies in people with multiple sclerosis in the USA. J. Comp. Eff. Res. 12(1), e220127 (2023).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 30 April 2024
Accepted: 13 January 2025
Published online: 12 February 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Clinical characteristics and treatment outcomes in multiple sclerosis patients treated with anti-CD20s who switched to fumarates: a retrospective analysis of a US healthcare claims database. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0071
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Daniel Bandari, Devon Conway, Liang Dong, Nicholas Hong, Minxing Li, Anne Littlewood, Mike Roy, Sam Ulin, Chencan Zou, Babak Amerian-Williams, Nicholas Belviso, James B. Lewin, Jason P. Mendoza, Mirla Avila, Comparative Effectiveness of Diroximel Fumarate vs. Dimethyl Fumarate in Persons with Multiple Sclerosis: A US Claims Analysis of Relapse Outcomes, Advances in Therapy, 10.1007/s12325-026-03608-1, 43, 7, (3031-3042), (2026).
- Ahmed Z. Obeidat, Michelle Betz, Rebecca Straus Farber, Erica Goff, Mark Gudesblatt, Le H. Hua, Yang Mao-Draayer, Derrick Robertson, Jonathan D. Santoro, Tony Wang, Daniel Gomes, Ivan Bozin, Jason P. Mendoza, Boyang Bian, James B. Lewin, Nicholas Belviso, Sai L. Shankar, Comparative Effectiveness and Risk of Severe Infection in Adult Patients With MS Treated With Diroximel Fumarate Versus Anti-CD20 Monoclonal Antibodies: A Real-World Claims Analysis, Advances in Therapy, 10.1007/s12325-025-03480-5, (2026).