COVID-19 clinical trials: who is likely to participate and why?
This article has been corrected.
VIEW CORRECTIONPublication: Journal of Comparative Effectiveness Research
Abstract
Aim: To identify factors associated with willingness to participate in a COVID-19 clinical trial and reasons for and against participating. Materials & methods: We surveyed Massachusetts (MA, USA) residents online using the Dynata survey platform and via phone using random digit dialing between October and November 2021. Respondents were asked to imagine they were hospitalized with COVID-19 and invited to participate in a treatment trial. We assessed willingness to participate by asking, “Which way are you leaning” and why. We used multivariate logistic regression to model factors associated with leaning toward participation. Open-ended responses were analyzed using conventional content analysis. Results: Of 1071 respondents, 65.6% leaned toward participating. Multivariable analyses revealed college-education (OR: 1.59; 95% CI: 1.11, 2.27), trust in the healthcare system (OR: 1.32; 95% CI: 1.10, 1.58) and relying on doctors (OR: 1.77; 95% CI: 1.45, 2.17) and family or friends (OR: 1.31; 95% CI: 1.11, 1.54) to make health decisions were significantly associated with leaning toward participating. Respondents with lower health literacy (OR: 0.57; 95% CI: 0.36, 0.91) and who identify as Black (OR: 0.40; 95% CI: 0.24, 0.68), Hispanic (OR: 0.61; 95% CI: 0.38, 0.98), or republican (OR: 0.61; 95% CI: 0.38, 0.97) were significantly less likely to lean toward participating. Common reasons for participating included helping others, benefitting oneself and deeming the study low risk. Common reasons for leaning against were deeming the study high risk, disliking experimental treatments and not wanting to be a guinea pig. Conclusion: Our finding that vulnerable individuals and those with lower levels of trust in the healthcare system are less likely to be receptive to participating in a COVID-19 clinical trial highlights that work is needed to achieve a healthcare system that provides confidence to historically disadvantaged groups that their participation in research will benefit their community.
Shareable abstract
A survey among Massachusetts residents identifies factors associated with participating in COVID-19 clinical trials and the need to build trust among historically disadvantaged groups in research.
Plain language summary
What is this article about?
This article describes a survey in which respondents were asked to imagine they were hospitalized with COVID-19 and invited to participate in a study of a COVID-19 treatment. They were asked whether they would participate and why.
What were the results?
Of the 1071 respondents, 65.6% leaned toward participating. Respondents with a college education, greater trust in the healthcare system and who rely on others to make healthcare decisions were more likely to participate. Respondents who identified as Black, Hispanic or republican and those who needed help reading medical materials were less likely to participate. Reasons for participating included helping others, benefitting oneself and deeming the study low risk. Reasons for not participating were deeming the study high risk, disliking experimental treatments and not wanting to be a guinea pig.
What do the results mean?
Historically disadvantaged groups were less likely to participate in a possible clinical trial. Work is needed to create a healthcare system that provides confidence to historically disadvantaged groups that if they take part in research, it will benefit their community.
Appropriate representation of women, older adults and members of racial and ethnic minority groups in medical research is essential to enhance the generalizability of research findings and reduce health disparities. Achieving representative enrollment in research studies has been a national priority since the passage of the National Institutes of Health (NIH) Revitalization Act of 1993 [1]. More recently, the FDA has taken steps to promote diversity in industry-sponsored clinical trials, including the publication of an action plan in 2014 [2] and updated draft guidance released in 2022 [3]. Despite these initiatives, underrepresentation of older adults and members of racial and ethnic minority groups persist across a broad range of conditions and interventions including oncology [4,5], cardiovascular disease [6,7], dementia [8], vaccine clinical trials [9] and COVID-19 clinical trials [10].
Barriers to participating in research among minority populations have been well documented and include mistrust related to ongoing discrimination and the legacy of historical mistreatment epitomized by the Tuskegee Study [11], less access to research studies, logistical barriers, the restrictive nature of clinical trial eligibility criteria [12] and lack of researcher understanding of cultural differences [13,14]. Studies have been conflicting as to whether differences in participation relate merely to inequitable access to clinical trials [15] or to differences in attitudes toward research among different groups [16,17].
Marked racial and ethnic disparities in the COVID-19 pandemic have been documented with higher rates of infection, hospitalization and death among members of racial and ethnic minority groups [18–21]. Emerging evidence of racial and ethnic disparities in use of COVID-19 treatments compounds these disparities [22,23]. In the context of these ongoing disparities, public attitudes toward participating in COVID-19 clinical trials and differences according to race/ethnicity are important to understand to ensure equitable representation in future COVID-19 clinical trials and thereby reduce disparities.
The goals of this study were to assess the likelihood of participating in a hypothetical COVID-19 treatment clinical trial, examine factors associated with willingness to participate and to understand reasons for being willing or not willing to participate among a diverse population.
Methods
Survey development & content
The survey was developed by the authors. It was pre-tested for clarity and flow with a convenience sample (n = 20), with minor revisions of item wording and response options based on input from this sample. The survey consisted of multiple sections and included items assessing COVID-19 vaccination intent, a vignette describing a hypothetical COVID-19 treatment clinical trial and questions related to that trial, items assessing attitudes related to making health related decisions, experiences with healthcare and demographic characteristics. The full set of items included in the present study are summarized below with details provided in Appendix 1.
This survey included an experimental component that tested the impact of a priming question intended to shape how participation is framed (helping others vs getting cutting edge treatment) and a 2 × 2 test of different physician messages (acknowledging reasons not to trust the medical system vs acknowledging the difficulty of participating in a clinical study and emphasizing getting a cutting-edge treatment vs helping others). Further details of the priming question and physician messages are provided in Appendix 2.
Hypothetical research study
The following scenario was presented via an audio-recording to avoid the potential reading burden. Participants who indicated they could not hear the scenario clearly were presented with the description in text.
Imagine you are hospitalized with COVID-19. You have been in the hospital for 5 days and you are getting sicker. You have a high fever. You need tubes in your nose to get enough oxygen.
Today, a new doctor tells you about a research study of a medicine that might work for COVID-19. The doctor explains that many patients take this medicine for other problems. Doctors do not know if it will work for COVID-19. Some small studies suggest it might help. However, there is a risk the medicine may cause complications. For example, you could get a urinary tract infection. After answering your questions, the doctor says…[respondents randomly assigned to receive one of four different messages, Appendix 2].
Respondents were then asked, “Based on the information you have so far, which way are you leaning right now?” Four response options were provided: “STRONGLY leaning AGAINST taking part in the study.”; “SOMEWHAT leaning AGAINST taking part in the study.”; “SOMEWHAT leaning toward taking part in the study.”; “STRONGLY leaning toward taking part in the study.” This was followed by an open-ended item: “Why are you leaning that way?”.
Next, respondents answered questions from a bank that asked them to consider, “To what extent, if any, would the following affect your willingness to take part in the study?”, followed by a list of conditions (If my doctor recommended that I take part; if my friends or family members thought I should take part; if over 500 people had already taken part; if thousands of people are already taking this medicine for other problems; if the medicine was not FDA approved; if the study was being done by the National Institutes of Health (NIH); if the study was being done by a drug company), with response options for each condition including “LESS willing to take part”, “NO DIFFERENCE” and “MORE willing to take part”.
Survey administration
We partnered with MassINC Polling Group to administer the survey to a sample of adult English or Spanish speaking Massachusetts (MA, USA) residents. MassINC fielded the online survey via the Dynata survey platform. Online participants received ∼$5 for their participation; the online survey took approximately 11 minutes to complete and was offered in English and Spanish. MassINC also partnered with Metro Research to administer the survey via phone; phone participants were solicited using random digit dialing and no incentive was provided. We oversampled Black and Latino residents with the goal of recruiting at least 250 Black respondents and 250 Latino respondents. The survey was conducted from 28 October to 17 November 2021.
Analyses
We calculated frequencies to describe respondent characteristics. We dichotomized responses to the question about likelihood of participating in the hypothetical research study, grouping the two “leaning toward” responses (strongly and somewhat toward) and the two “leaning against” responses (strongly and somewhat against). We eliminated (n = 63) discordant responses where the rating (leaning toward or against) was clearly inconsistent with the short answer response, as we judged such responses to indicate poor data quality. We used chi-square statistics and t-tests to examine the associations between respondent characteristics, experiences and attitudes and intent to participate in the hypothetical research study. We then used a multivariate logistic regression model to obtain odds ratios (ORs) and 95% confidence intervals (CIs) adjusted for other variables. To select a parsimonious model of factors associated with “leaning toward” participation in the hypothetical study, we used a backward stepwise approach starting with standard demographic variables (race/ethnicity, age, gender and education) and survey mode (online or phone) which were forced into the model and all variables that had an associated p value of less than 0.020 in the bivariate analyses. After obtaining a final model, we added each variable that had been dropped initially to examine whether its inclusion/exclusion improved model fit. Details of the analyses of the experimental manipulation are provided in Appendix 2. For the items assessing conditions that might make respondents more, or less willing to participate, we calculated the net impact of each condition on intent to participate as the difference between the percentage of respondents who said they would be more willing to participate and the percentage who indicated they would be less willing to participate. Analyses were performed with SAS version 9.4 (SAS Institute Inc., NC, USA) and SPSS version 28.0.1.0 (IBM SPSS Statistics, Armonk, NY, USA).
We analyzed responses to the open-ended item “Why are you leaning that way?” using conventional content analysis [24]. One author (KM) reviewed the responses and generated an initial set of codes. Two authors (KF, ME) reviewed the initial codes and suggested modifications. Responses were then coded using the refined code list. More than 20% of the responses were reviewed by at least 2 authors to ensure consistency. Questions about codes identified during coding were discussed and resolved by at least 2 authors.
The study was reviewed and approved by the UMass Chan Medical School and Boston Medical Center Institutional Review Boards. Informed consent was provided by all participants.
Results
After excluding respondents whose responses to the open-ended and close-ended items were discordant (n = 63), 1071 individuals provided a response to the “which way are you leaning” question and constitute the analytic sample. Of these, 566 (53%) were women, 530 (49.5%) identified as White, 248 (23.2%) as Hispanic and 219 (20.5%) as Black. Most participants (n = 759; 70.9%) completed the survey online. Additional sociodemographic characteristics, health system attitudes and experiences and factors respondents might depend on when making decisions about their health are shown in Table 1. In response to the question “which way are you leaning?”, 703 (65.6%) respondents indicated they were leaning toward participating in the COVID-19 treatment clinical trial, while 368 (34.4%) were leaning against. The priming question and varied physician messages had no impact on respondent willingness to participate (Appendix 2).
| Characteristic | Leaning toward (n = 703) | Leaning against (n = 368) | p-value |
|---|---|---|---|
| Demographics | |||
| Survey language | 0.18 | ||
| English | 677 (96.3) | 348 (94.6) | |
| Spanish | 26 (3.7) | 20 (5.4) | |
| Age range, years | 0.82 | ||
| 18–29 | 128 (18.2) | 68 (18.5) | |
| 30–44 | 186 (26.5) | 100 (27.3) | |
| 45–59 | 196 (27.9) | 108 (29.4) | |
| 60+ | 193 (27.5) | 91 (24.8) | |
| Gender | 0.56 | ||
| Man | 323 (46.1) | 178 (48.4) | |
| Woman | 377 (53.8) | 189 (51.4) | |
| Non-binary | 1 (0.14) | 1 (0.27) | |
| Race/ethnicity | <0.001 | ||
| White, non-Hispanic | 401 (57.0) | 129 (35.1) | |
| Asian | 30 (4.3) | 15 (4.1) | |
| Black | 114 (16.2) | 105 (28.5) | |
| Hispanic | 139 (19.8) | 109 (29.6) | |
| Other | 19 (2.7) | 10 (2.7) | |
| Education | <0.001 | ||
| High school or less | 154 (22.0) | 119 (32.3) | |
| Some college | 210 (30.0) | 125 (34.0) | |
| College or more | 336 (48.0) | 124 (33.7) | |
| How often do you have someone help you read medical materials? | 0.39 | ||
| Never | 376 (53.8) | 192 (52.3) | |
| Occasionally / sometimes | 239 (34.2) | 120 (32.7) | |
| Often / always | 84 (12.0) | 55 (15.0) | |
| Political affiliation | <0.001 | ||
| Democrat | 263 (37.4) | 106 (28.8) | |
| Independent | 257 (36.6) | 118 (32.1) | |
| Republican | 98 (13.9) | 55 (15.0) | |
| Other/no affiliation | 85 (12.1) | 89 (24.2) | |
| How often in the past 12 months would you say you were worried or stressed about having enough money to pay for basic living expenses? | 0.57 | ||
| Never | 199 (28.4) | 89 (24.4) | |
| Rarely | 155 (22.1) | 87 (23.8) | |
| Sometimes | 231 (33.0) | 125 (34.3) | |
| Frequently | 116 (16.6) | 64 (17.5) | |
| In general, how would you rate your overall health? | <0.001 | ||
| Poor | 6 (0.86) | 15 (4.1) | |
| Fair | 94 (13.5) | 44 (12.0) | |
| Good | 241 (34.5) | 115 (31.4) | |
| Very good | 276 (39.5) | 129 (35.3) | |
| Excellent | 82 (11.7) | 63 (17.2) | |
| In general, how would you rate your overall mental or emotional health? | 0.74 | ||
| Poor | 29 (4.1) | 15 (4.1) | |
| Fair | 116 (16.6) | 58 (15.8) | |
| Good | 203 (29.0) | 101 (27.5) | |
| Very good | 230 (32.9) | 117 (31.8) | |
| Excellent | 122 (17.4) | 77 (20.9) | |
| Health system attitudes and experiences | |||
| How much do you trust the healthcare system to do what's right for you? | <0.001 | ||
| Do not trust at all | 20 (2.8) | 32 (8.7) | |
| Trust a little | 166 (23.6) | 106 (28.8) | |
| Trust somewhat | 315 (44.8) | 150 (40.8) | |
| Trust a great deal | 202 (28.7) | 80 (21.7) | |
| Doctors, nurses and others in the healthcare system usually treat me with respect. | <0.001 | ||
| Strongly disagree | 13 (1.9) | 11 (3.0) | |
| Somewhat disagree | 26 (3.7) | 37 (10.1) | |
| Somewhat agree | 294 (41.9) | 147 (40.0) | |
| Strongly agree | 368 (52.5) | 173 (47.0) | |
| If you needed healthcare tomorrow, how confident are you that you could get it? | 0.12 | ||
| Not at all confident | 23 (3.3) | 17 (4.6) | |
| A little confident | 62 (8.9) | 45 (12.3) | |
| Somewhat confident | 201 (28.8) | 112 (30.5) | |
| Very confident | 412 (59.0) | 193 (52.6) | |
| Factors respondents might “depend on in making decisions about health”† | |||
| I depend on my doctor's advice, mean (SD) | 3.39 (0.67) | 2.98 (0.90) | <0.001 |
| I depend on numbers and statistics, mean (SD) | 3.00 (0.79) | 2.70 (1.01) | <0.001 |
| I depend on my intuition or gut feelings, mean (SD) | 2.91 (0.84) | 2.95 (0.91) | 0.51 |
| I depend on what I see happening with my friends and family, mean (SD) | 2.67 (0.81) | 2.46 (0.95) | <0.001 |
| I depend on advice from certain friends and/or family members, mean (SD) | 2.60 (0.86) | 2.24 (0.93) | <0.001 |
| I depend on my faith or religion, mean (SD) | 2.02 (1.03) | 2.14 (1.10) | 0.09 |
| I depend on the news or social media, mean (SD) | 2.01 (0.91) | 1.83 (0.87) | 0.001 |
Because of missing values, the number of observations in each characteristic category may not add up to the column's total.
†
Response options were assigned values as follows: strongly disagree = 1; somewhat disagree = 2; somewhat agree = 3; strongly agree = 4.
On bivariate analysis (Table 1), sociodemographic factors that were significantly associated with leaning toward participating included White race, college education or more, democrat or independent political affiliation and being in good or very good health. Having greater trust in the healthcare system and being treated with respect by doctors and nurses were associated with leaning toward participating. In making decisions about their health, respondents who leaned toward participating were more likely to depend on advice from doctors or from certain friends and family, numbers and statistics, what they see happening with friends and family and the news or social media than respondents who leaned against participating. Respondents who leaned against participating tended to be more likely to depend on their faith or religion in making decisions about their health, although this did not achieve statistical significance.
Characteristics that were significantly associated with leaning toward participating on multivariable analyses (Table 2) included having a college education or more (OR: 1.59; 95% CI: 1.11, 2.27), depending on a doctor's advice (OR: 1.77; 95% CI: 1.45, 2.17) or advice from certain friends or family (OR: 1.31; 95% CI: 1.11, 1.54) to make decisions about one's health and having higher trust in the healthcare system (OR: 1.32; 95% CI: 1.10, 1.58). Respondents who identify as Black (OR: 0.40; 95% CI: 0.24, 0.68), Hispanic (0.61; 95% CI: 0.38, 0.98), of republican political affiliation (OR: 0.61; 95% CI: 0.38, 0.97) and with lower health literacy (OR: 0.57; 95% CI: 0.36, 0.91) were significantly less likely to lean toward participating.
| Characteristic | Adjusted† odds ratio (95% CI) |
|---|---|
| Age range, years | |
| 18–29 | REF |
| 30–44 | 0.97 (0.62, 1.52) |
| 45–59 | 0.83 (0.53, 1.32) |
| 60+ | 0.77 (0.48, 1.25) |
| Gender | |
| Man | REF |
| Woman | 1.05 (0.78, 1.41) |
| Non-binary | 0.19 (0.01, 3.28) |
| Race/ethnicity | |
| White, non-Hispanic | REF |
| Asian | 0.52 (0.25, 1.07) |
| Black | 0.40 (0.24, 0.68) |
| Hispanic | 0.61 (0.38, 0.98) |
| Other | 0.76 (0.32, 1.82) |
| Education | |
| High school or less | REF |
| Some college | 1.14 (0.79, 1.65) |
| College or more | 1.59 (1.11, 2.27) |
| How often do you have someone help you read medical materials? | |
| Never | REF |
| Occasionally / sometimes | 0.95 (0.69, 1.30) |
| Often / always | 0.57 (0.36, 0.91) |
| Depend on doctor's advice to make decisions about health. | 1.77 (1.45, 2.17) |
| Depend on advice from certain friends and/or family members to make decisions about health. | 1.31 (1.11, 1.54) |
| How much do you trust the healthcare system to do what's right for you? | 1.32 (1.10, 1.58) |
| Political affiliation | |
| Democrat | REF |
| Independent | 0.75 (0.53, 1.07) |
| Republican | 0.61 (0.38, 0.97) |
| Other / No affiliation | 0.50 (0.33, 0.77) |
†
Adjusted model includes Age, Race, Ethnicity, Gender, Education, Political affiliation, “Depend on doctor's advice”, “Depend on certain friends and family”, “Trust in the healthcare system”, “Have someone help read medical materials” and survey mode (online or phone).
REF: Indicates the referent category for each variable.
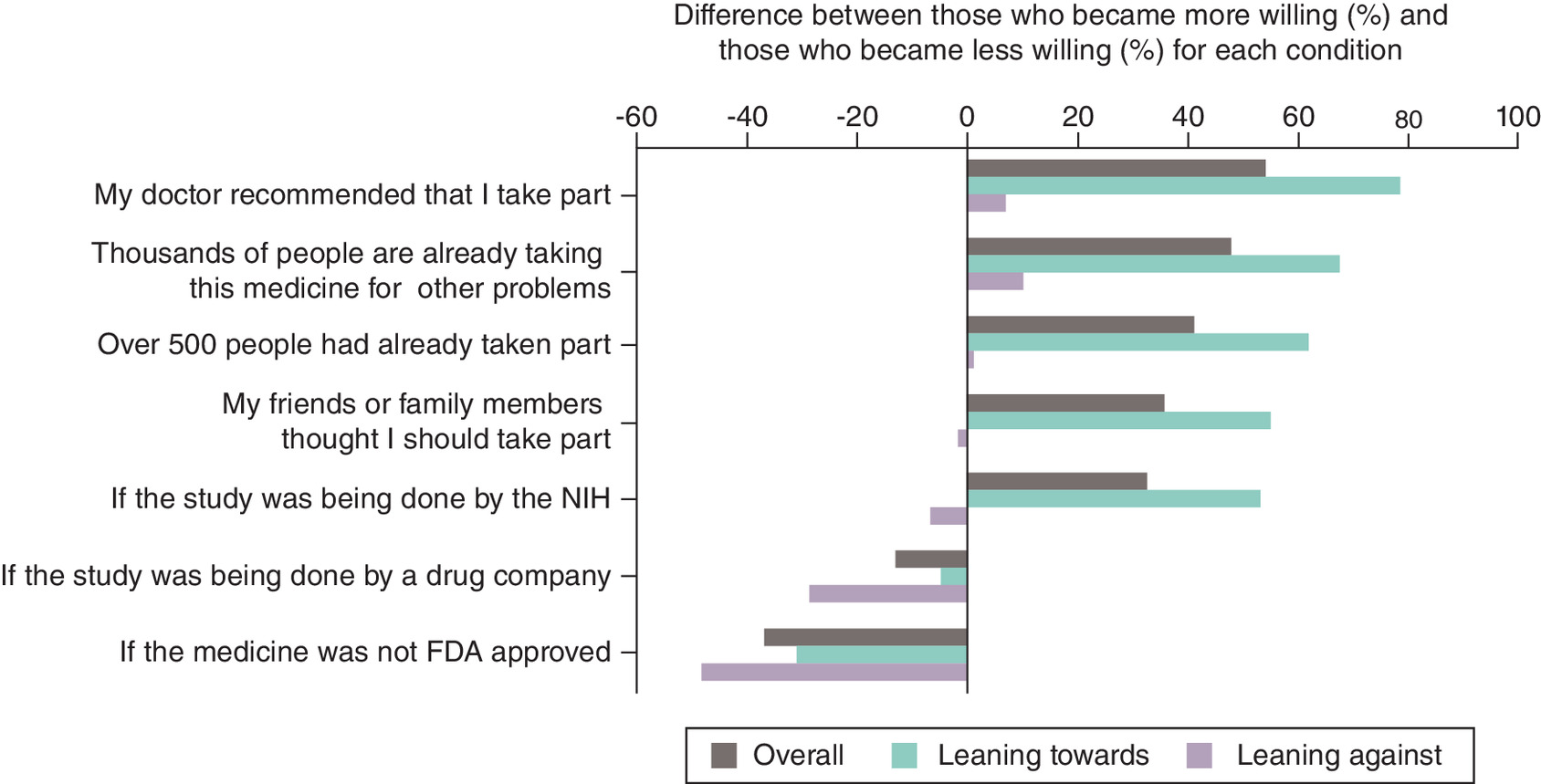
The net impact of conditions that might increase or decrease willingness to participate is displayed in Figure 1. A recommendation from one's doctor had the greatest net impact on willingness to participate with 65% of respondents becoming more willing and 11% becoming less willing, for a net impact of 54% more willing to participate, overall. The impact of a doctor recommendation was greatest among those already leaning toward participating, with a net impact of 78.4% in this group (difference between 81.4% who became more willing and 3% who became less willing), as compared with a net impact of 6.9% (difference between 33.3% who became more willing and 26.4% who became less willing) among those leaning against participating. A study involving a non-FDA approved medication had the greatest negative impact on willingness to participate with a net impact of 36.8% less willing to participate overall, compared with a net negative impact of 13% if a study is being conducted by a drug company. These findings were most apparent among respondents leaning against participating.
Qualitative analyses (Table 3) revealed that the most common reason (n = 276; 48.1%) for leaning toward participating was to help others (“I like to help others”). Some respondents framed this in terms of wanting to contribute to society (“I think it would benefit society”), while others referred to the value of what would be learned (“The information would be beneficial”) and still others referred to a desire to contribute to ending the COVID-19 pandemic (“I would like to help with what I have to fight COVID-19”). Some of these respondents expressed a sense of duty to participate (“I think it is the right thing to do”) and others commented on the importance of research (“Research is vital”). Nearly half (n = 230; 40.1%) of the respondents leaning toward participating viewed participation as being potentially beneficial to themselves (“So I could get better”). Some responses in this category suggested the possibility of therapeutic misconception (“I don't think the doctor would suggest it if there was a possibility that it did not help”). Many respondents (n = 212; 36.9%) leaning toward participating appeared to weigh the risks and benefits of participation and judge the risks of the study to be low, while the risks of illness were viewed as high (“It seems like an educated risk. A side effect of a UTI is better than not being able to breathe”). Some took the fact that the study drug was already approved for treatment of other conditions as an indication of its safety (“If the medicine is taken by other patients, then I assume it is safe for me to take”). A small number (n = 22; 3.8%) explicitly acknowledged willingness to accept the risk inherent in participating in research (“Because like everything else in life, you take a chance and see what happens”).
| Theme | n (%) |
|---|---|
| Leaning toward participating | n = 574 |
| Participation might help others | 276 (48.1) |
| Participation would potentially benefit self | 230 (40.1) |
| Judge risks of participating to be low and/or risks of disease to be high | 212† (36.9) |
| Trust in doctor, healthcare system, or science | 23 (4.0) |
| Recognize inherent risk in participating and willing to accept it | 22 (3.8) |
| Would want more information before participating | 36 (6.3) |
| Expressed fear or worry about the potential side effects, but still leaning toward participating | 8 (1.4) |
| Leaning against participating | n = 230 |
|---|---|
| Weighed risks and judge risks of study to be high, focus on risk | 90‡ (39.1) |
| Don't like untested experimental treatments, often related to inherent uncertainty | 57§ (24.8) |
| Don't want to be a guinea pig | 40 (17.4) |
| Reference to lack of trust in the doctor, healthcare system, and/or science | 26 (11.3) |
| Don't think participation will benefit self | 15 (6.5) |
| Not enough information | 35 (15.2) |
| Fear or worry about the potential side effects deterred from participating | 8 (3.5) |
Percentages add up to more than 100 because multiple codes may be applied to each response.
†
Does not include n = 1 “leaning against” respondent whose response referenced this theme.
‡
Does not include n = 6 “leaning toward” respondents whose response referenced this theme.
§
Does not include n = 2 “leaning toward” respondents whose response referenced this theme.
Among respondents leaning against participating, the most common reason was a focus on the risks (“There's risk involved in the study”). In some cases, this related to underlying conditions that might increase the risk further (“I am leaning this way because I am immunocompromised, and I fear unknown complications”). Approximately one-quarter (n = 57; 24.8%) indicated discomfort with experimental treatments, including due to the inherent uncertainty (“I don't want to take chances on the unknown”). Additional reasons for leaning against participating included not wanting to be a guinea pig (“I am not a lab rat, nor do I intend to be”) (n = 40; 17.4%); not trusting doctors, the healthcare system, or science (“Sometimes the medication and the research, they are not trustworthy”) (n = 26; 11.3%); and not thinking participation would be beneficial for themselves (“I am not convinced that the new drug will improve my condition”) (n = 15; 6.5%). Respondents leaning against participating were more likely to want more information (n = 35; 15.2%) than those leaning toward participating (n = 36; 6.3%). A small number of respondents in both groups referred to being nervous or worried about participating; this was more common among those leaning against participating (n = 8; 3.5% vs n = 8; 1.4%).
Discussion
Our findings provide critical insights into who is inclined toward and against participating in a hypothetical COVID-19 treatment clinical trial and why. Consistent with other studies that have found disparities in research participation [9,10,17], we demonstrate that more vulnerable individuals- those who belong to a racial or ethnic minority group, with lower educational attainment and lower health literacy- and those with lower levels of trust in the healthcare system are less likely to be receptive to participating in a COVID-19 clinical trial than more advantaged and more trusting individuals. Among those leaning toward participating, the most common reason was to help others, highlighting the inherently prosocial nature of taking part in a clinical trial. It is well established that prosocial behaviors are more common among those perceived to be in one's “in-group” [25–27] and this is enhanced by greater trust [28], while social exclusion decreases the likelihood of prosocial behavior [29]. Viewed through this lens, it is not surprising that members of racial and ethnic minority groups who have experienced discrimination and disparities in the healthcare system and those with lower levels of trust in the healthcare system would be less inclined to participate in a clinical trial of uncertain benefit to themselves and their community. Thus, it may be helpful to consider that diverse research participation may be a metric of an equitable and trustworthy healthcare system as much or more than it may be a mechanism for achieving an equitable and trustworthy healthcare system.
Our findings underscore how much work is needed to achieve a healthcare system in the US that provides confidence to all members of society that their participation in research will yield benefits to their community. Long-term, the most meaningful way of achieving this is through elimination of disparities in health and healthcare. In the short-term, emphasizing how research efforts may be of direct benefit to specific communities, sharing research findings with the community [30], engaging members of marginalized communities in developing research priorities and increasing the numbers of research professionals who are members of communities under-represented in research are likely to be effective strategies, consistent with principles of community-engaged participatory research [31,32]. More work is needed to determine how to bring these principles of community engagement to clinical trials that enroll participants across many sites across the country and are often conducted by pharmaceutical companies. Policies to require community advisory boards for clinical trials at the study or site level, similar to data safety monitoring boards, are likely to be of value if executed thoughtfully [33].
Viewing participation as of potential benefit to oneself was the second most common reason for leaning toward participating in our study. Although we did not directly measure therapeutic misconception, any expectation of direct therapeutic benefit from a clinical trial could be viewed as evidence of therapeutic misconception, or lack of understanding the distinction between clinical care and research [34]. That this was cited as a reason for participating by 4 in 10 of those leaning toward participating highlights the need to guard against therapeutic misconception when recruiting participants to clinical trials. This finding is consistent with a prior study which found therapeutic misconception to some degree in 62% of 44 clinical trials [35]. Strategies are needed to decrease therapeutic misconception and increase participant understanding of research participation. One promising study premised on the fact that researchers and patients have fundamentally misaligned primary cognitive frames showed that scientific reframing via a brief educational intervention significantly reduced therapeutic misconception scores without negatively influencing willingness to participate in research [36]. Concerted efforts are needed to systematically incorporate and build on this approach as enrolling participants in clinical trials who expect personal benefit from participation is not only unethical, but is likely to increase mistrust of medical research, making it more difficult to enroll diverse participants.
Our study indicates that whether one leans toward or against participating may also reflect individual differences in how one views the balance of potential risks, benefits and acceptance of uncertainty. These factors are likely hard to change and may therefore not be a reasonable target for encouraging increased participation in research. In fact, in examining factors that might reasonably be expected to make one more willing to participate (doctor recommended it, thousands already taking the medication, family and friends thought you should), we found these were most influential among those already leaning toward participating. Conversely, factors that might reasonably be expected to make one less willing to participate (medication not FDA-approved, study being done by a drug company) were more influential among those already leaning against participating. These findings are consistent with confirmation bias [37] and suggest that someone already inclined not to participate because they are concerned about risk may subconsciously ignore, misinterpret, or reject information demonstrating overall safety. Therefore, efforts to convince them of safety are unlikely to be of value.
Our study has several strengths, including the large sample size and oversampling of Black and Hispanic participants. At the same time, the findings of our study should be viewed considering several limitations. We used a vignette-based study design to assess likelihood of participating in a COVID-19 clinical trial. It is possible that owing to the hypothetical nature of this vignette, participants responses on the survey may not have paralleled their response in real life. In addition, we provided limited information about the potential trial to participants. Different or additional information might have affected participants' responses. For example, vulnerable populations and particularly those with lower education and/or health literacy may require more details when evaluating whether to participate in a research study so this may have artifactually reduced the intended participation of these respondents. The benefits of this study design are that it allowed us to explore reasons for intent to participate or not, and to examine which factors would have made participants more or less willing to participate. Our study does not provide information on whether these factors would differ for a trial testing a treatment for a medical condition other than COVID-19 or for a chronic versus an acute condition. Because our sample was restricted to Massachusetts (MA, USA) residents, the results may not be generalizable to the US population and we were unable to assess for differences in likelihood to participate and reasons by geographic location. Lastly, the recruitment approach does not allow us to determine a response rate.
Conclusion
We found that more vulnerable individuals (racial/ethnic minorities, those with lower educational attainment and lower health literacy) and those with less trust in the healthcare system are less likely to participate in a COVID-19 clinical trial. This finding combined with evidence highlighting the challenge of therapeutic misconception raises questions about unintended risks associated with efforts focused solely on increasing diversity in research. Although ensuring diverse participation in clinical trials has been promoted as a means of increasing equity in healthcare, and may in fact contribute to achieving this goal, it is also important to consider that this is asking more vulnerable individuals in society to take on risk that may not benefit them directly. First and foremost, this indicates the importance of incorporating strategies in the informed consent process to reduce the possibility of therapeutic misconception and ensure that participants are truly fully informed. Second, it highlights the need to ensure that the benefits of the knowledge gained through research accrue to the population(s) affected by the disease equitably. This is most likely to be achieved through community-engaged participatory research in which community members are engaged in all stages of research.
Summary points
•
Marked racial and ethnic disparities in both outcomes and treatments for COVID-19 have been documented.
•
Understanding public attitudes toward participating in COVID-19 clinical trials and differences according to race/ethnicity are important to ensure equitable representation in future COVID-19 clinical trials.
•
This survey was administered to a sample of adult English or Spanish speaking Massachusetts (MA, USA) residents between October and November 2021.
•
Respondents were asked to imagine they were hospitalized with COVID-19 and invited to participate in a hypothetical COVID-19 clinical treatment trial, followed by the questions: “Based on the information you have so far, which way are you leaning right now”, and why.
•
Factors associated with being more likely to participate included having a college education or more, depending on a doctor's advice or advice from certain family or friends to make health decisions and having higher trust in the healthcare system.
•
Identifying as Black, Hispanic, or republican and having lower health literacy were associated with being less likely to lean toward participating.
•
More vulnerable individuals and those with less trust in the healthcare system are less likely to be receptive to participating in a COVID-19 clinical trial than more advantaged and trusting individuals.
•
Work is needed to achieve a healthcare system that provides confidence to historically disadvantaged groups that participation in research will yield benefits to their communities.
Author contributions
KA Fisher, BP Linas and KM Mazor were responsible for study conception and design. KA Fisher, KM Mazor and N Nguyen were responsible for acquisition of data. KA Fisher, MM Epstein, H Fouayzi and S Crawford supervised and conducted the data analysis and interpretation of data. KA Fisher drafted the manuscript, and all other authors revised it critically for intellectual content.
Financial disclosure
This research was, in part, funded by the National Institutes of Health (NIH) Agreement OT2HL158287. The views and conclusions contained in this document are those of the authors and should not be interpreted as representing the official policies, either expressed or implied, of the NIH. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained institutional review board approval from the UMass Chan Medical School and Boston University Medical Center Institutional Review Boards for the research described. In addition, they have obtained verbal or written informed consent from the individuals who responded to this survey via phone or online, respectively.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest
1.
NIH Revitalization Act, Subtitle B, Part 1, Sec 131–133, June 10, 1993. https://orwh.od.nih.gov/sites/orwh/files/docs/NIH-Revitalization-Act-1993.pdf (2023).
2.
Food and Drug Administration. FDA action plan to enhance the collection and availability of demographic subgroup data. In: Dept of Health and Human Services, ed2014. https://www.fda.gov/media/89307/download
3.
Food and Drug Administration. Diversity plans to improve enrollment of participants from underrepresented racial and ethnic populations in clinical trials; Draft guidance for industry; Availability. In: Dept of Health and Human Services, ed2022. Docket number FDA-2021-D-0789. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/diversity-plans-improve-enrollment-participants-underrepresented-racial-and-ethnic-populations
4.
Aldrighetti CM, Niemierko A, Van Allen E, Willers H, Kamran SC. Racial and ethnic disparities among participants in precision oncology clinical studies. JAMA Netw. Open 4(11), e2133205 (2021).
5.
Loree JM, Anand S, Dasari A et al. Disparity of race reporting and representation in clinical trials leading to cancer drug approvals from 2008 to 2018. JAMA Oncol. 5(10), e191870 (2019).
6.
Tahhan AS, Vaduganathan M, Greene SJ et al. Enrollment of older patients, women, and racial and ethnic minorities in contemporary heart failure clinical trials: a systematic review. JAMA Cardiol. 3(10), 1011–1019 (2018).
7.
Vilcant V, Ceron C, Verma G, Zeltser R, Makaryus AN. Inclusion of under-represented racial and ethnic groups in cardiovascular clinical trials. Heart Lung Circ. 31(9), 1263–1268 (2022).
8.
Canevelli M, Bruno G, Grande G et al. Race reporting and disparities in clinical trials on Alzheimer's disease: a systematic review. Neurosci. Biobehav. Rev. 101, 122–128 (2019).
9.
Flores LE, Frontera WR, Andrasik MP et al. Assessment of the inclusion of racial/ethnic minority, female, and older individuals in vaccine clinical trials. JAMA Netw. Open 4(2), e2037640 (2021).
10.
Xiao H, Vaidya R, Liu F, Chang X, Xia X, Unger JM. Sex, racial, and ethnic representation in COVID-19 clinical trials: a systematic review and meta-analysis. JAMA Intern. Med. 183(1), 50–60 (2023).
• This systematic review and meta-analysis found that female, Asian, Black and Hispanic or Latino participants were under-represented in COVID-19 clinical trials, highlighting a system-wide difference in representation for these demographic groups.
11.
Scharff DP, Mathews KJ, Jackson P, Hoffsuemmer J, Martin E, Edwards D. More than Tuskegee: understanding mistrust about research participation. J. Health Care Poor Underserved 21(3), 879–897 (2010).
12.
Adams-Campbell LL, Ahaghotu C, Gaskins M et al. Enrollment of African Americans onto clinical treatment trials: study design barriers. J. Clin. Oncol. 22(4), 730–734 (2004).
13.
Bonevski B, Randell M, Paul C et al. Reaching the hard-to-reach: a systematic review of strategies for improving health and medical research with socially disadvantaged groups. BMC Med. Res. Methodol. 14, 42 (2014).
14.
George S, Duran N, Norris K. A systematic review of barriers and facilitators to minority research participation among African Americans, Latinos, Asian Americans, and Pacific Islanders. Am. J. Public Health 104(2), e16–31 (2014).
15.
Unger JM, Hershman DL, Till C et al. “When offered to participate”: a systematic review and meta-analysis of patient agreement to participate in cancer clinical trials. J. Natl Cancer Inst. 113(3), 244–257 (2021).
16.
Milani SA, Swain M, Otufowora A, Cottler LB, Striley CW. Willingness to participate in health research among community-dwelling middle-aged and older adults: does race/ethnicity matter? J. Racial Ethn. Health Disparities 8(3), 773–782 (2021).
17.
Williams CP, Senft Everson N, Shelburne N, Norton WE. Demographic and health behavior factors associated with clinical trial invitation and participation in the United States. JAMA Netw. Open 4(9), e2127792 (2021).
18.
Gold JAW, Rossen LM, Ahmad FB et al. Race, ethnicity, and age trends in persons who died from COVID-19 - United States, May-August 2020. MMWR Morb. Mortal. Wkly Rep. 69(42), 1517–1521 (2020).
19.
Karaca-Mandic P, Georgiou A, Sen S. Assessment of COVID-19 hospitalizations by race/ethnicity in 12 States. JAMA Intern. Med. 181(1), 131–134 (2021).
20.
Rossen LM, Branum AM, Ahmad FB, Sutton P, Anderson RN. Excess deaths associated with COVID-19, by age and race and ethnicity - United States, January 26-October 3, 2020. MMWR Morb. Mortal. Wkly Rep. 69(42), 1522–1527 (2020).
21.
Garg S, Kim L, Whitaker M et al. Hospilatization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019 - COVID-NET, 14 states, March 1–30, 2020. MMWR Morb. Mortal. Wkly Rep. 69(15), 458–464 (2020).
22.
Wiltz JL, Feehan AK, Molinari NM et al. Racial and ethnic disparities in receipt of medications for treatment of COVID-19 - United States, March 2020-August 2021. MMWR Morb. Mortal. Wkly Rep. 71(3), 96–102 (2022).
23.
Boehmer TK, Koumans EH, Skillen EL et al. Racial and ethnic disparities in outpatient treatment of COVID-19 - United States, January-July 2022. MMWR Morb. Mortal. Wkly Rep. 71(43), 1359–1365 (2022).
24.
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual. Health Res. 15(9), 1277–1288 (2005).
25.
Brewer MB. In-group bias in the minimal intergroup situation: a cognitive-motivation analysis. Psychol. Bull. 86(2), 307–324 (1979).
26.
Dovidio JF, Piliavin JA, Gaertner SL, Schroeder DA, Clark RD III. The arousal: cost-reward and the process of intervention: a review of the evidence. In: Prosocial Behavior. Clark MS (Ed.). 86–118 (1991).
27.
Levine M, Prosser A, Evans D, Reicher S. Identity and emergency intervention: how social group membership and inclusiveness of group boundaries shape helping behavior. Pers. Soc. Psychol. Bull. 31(4), 443–453 (2005).
28.
Cuadrado E, Tabernero C. Affective balance, team prosocial efficacy and team trust: a multilevel analysis of prosocial behavior in small groups. PLOS ONE 10(8), e0136874 (2015).
• Using a multilevel perspective, this paper examined the relationships between individual- and group-level variables and their impact on prosocial behavior toward team members.
29.
Twenge JM, Baumeister RF, DeWall CN, Ciarocco NJ, Bartels JM. Social exclusion decreases prosocial behavior. J. Pers. Soc. Psychol. 92(1), 56–66 (2007).
• In several experiments, the authors found that social exclusion caused a reduction in prosocial behavior, and that rejection temporarily impairs capacity for empathetic understanding of and cooperation with other people.
30.
Shalowitz DI, Miller FG. Communicating the results of clinical research to participants: attitudes, practices, and future directions. PLoS Med. 5(5), e91 (2008).
• Provides a review on the effects of communicating aggregate and individual research findings to participants, investigators and the broader research enterprise, as well as attitudes surrounding communication of results and disclosure practices.
31.
Cook WK. Integrating research and action: a systematic review of community-based participatory research to address health disparities in environmental and occupational health in the USA. J. Epidemiol. Community Health 62(8), 668–676 (2008).
32.
Rai T, Hinton L, McManus RJ, Pope C. What would it take to meaningfully attend to ethnicity and race in health research? Learning from a trial intervention development study. Sociol Health Illn. 44(S1), 57–72 (2022).
33.
Rai T, Hinton L, McManus RJ, Pope C. What would it take to meaningfully attend to ethnicity and race in health research? Learning from a trial intervention development study. Sociol Health Illn. 44(S1), 57–72 (2022).
34.
Appelbaum PS, Roth LH, Lidz CW, Benson P, Winslade W. False hopes and best data: consent to research and the therapeutic misconception. Hastings Cent. Rep. 17(2), 20–24 (1987).
35.
Appelbaum PS, Lidz CW, Grisso T. Therapeutic misconception in clinical research: frequency and risk factors. IRB 26(2), 1–8 (2004).
• Details the risks of therapeutic misconception (TM) among research participants, when and why it occurs, and ways that it can be avoided.
36.
Christopher PP, Appelbaum PS, Truong D, Albert K, Maranda L, Lidz C. Reducing therapeutic misconception: a randomized intervention trial in hypothetical clinical trials. PLOS ONE 12(9), e0184224 (2017).
• This trial tested the efficacy of an informed consent intervention based on scientific reframing compared to a traditional informed consent procedure in reducing TM among participants considering enrollment in hypothetical clinical trials.
37.
Plous S. The Psychology of Judgement and Decision-Making. (1st Edition). McGraw-Hill, NY, USA (1993).
Information & Authors
Information
Published In
Copyright
© 2024 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 29 November 2023
Accepted: 28 June 2024
Published online: 24 July 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
COVID-19 clinical trials: who is likely to participate and why?. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0181
Export citation
Select the citation format you wish to export for this article or chapter.