Radiofrequency ablation using the ThermoCool SmartTouch Catheter guided by ablation index versus antiarrhythmic drugs in atrial fibrillation treatment in China: a cost-consequence analysis
Abstract
Aim: To evaluate the costs and consequences of two front-line atrial fibrillation (AF) treatments from Chinese healthcare system perspective: radiofrequency catheter ablation (RFCA) using ThermoCool SmartTouch Catheter guided by Ablation Index (STAI), in comparison to antiarrhythmic drugs (AADs). Patients & methods: We simulated clinical and economic consequences for AF patients initially receiving STAI or AADs using a short-term decision tree model leading to a 10-year long-term Markov model. The model projected both clinical consequences and costs associated with, among others, AF, heart failure (HF), strokes, and deaths due to AF or AF related complications. Data informing the models included combination of a local real-world study and published clinical studies. Results: STAI was advantageous versus AADs on all 4 main clinical outcomes evaluated; AF: 25.83% lower (12.84% vs 38.67%), HF: 2.22% lower (1.33% vs 3.55%), stroke or post stroke: 1.82% lower (10.00% vs 11.82%) and deaths due to AF or AF related complications: 0.64% lower (4.11% vs 4.75%). The average total cost per patient in STAI group was ¥16,682 lower (¥123,124 vs ¥139,806). The one-way sensitivity analysis indicated that the difference in total cost was most sensitive to annual AF recurrence probability in AADs-treated patients. Probabilistic sensitivity analysis indicated a 98.5% probability that RFCA treatment would result in cost savings by the end of the 10th year. Conclusion: Radiofrequency catheter ablation using SmartTouch catheter guided by Ablation Index was superior to AADs as the first-line AF treatment in Chinese setting with better clinical outcomes and at lower costs over a 10-year time horizon.
Plain language summary
What is this article about?
Prior research suggests that radiofrequency catheter ablation (RFCA) is generally considered cost-effective compared with antiarrhythmic drugs (AADs) for atrial fibrillation (AF) treatment in China. However, these studies did not account for situations where patients require repeat ablations or switch from one treatment to another. Our study examines the health outcomes and costs of two front-line AF treatments from the perspective of the Chinese healthcare system: RFCA using ThermoCool SmartTouch Catheter guided by Ablation Index (STAI), in comparison to AADs.
What were the results?
Compared with AADs, RFCA using STAI improves clinical outcomes while reducing medical costs over a span of ten years.
What do the results mean?
These findings indicate that RFCA using STAI is a preferred option for first-line AF treatment in the Chinese healthcare context compared with AADs. Our analysis takes into account the possibility of patients needing repeated RFCA procedures if AF reoccurs, or switching from AADs to RFCA if the initial AAD treatment is unsuccessful.
Atrial fibrillation (AF) is the most common arrhythmia encountered in clinical practice, which is associated with an increased risk of stroke, heart failure and premature death [1]. Recently, a large community-based epidemiological study involving 47,841 adults aged over 45 years, utilizing both self-reporting and electroencephalogram (testing, found that AF affected about 1.8% of the study population, equating to approximately 7.9 million people in China [2]. This research also showed that prevalence of AF was strongly associated with age among both men and women: AF prevalence increased from 0.8% in men and 0.6% in women within the 45–54 year age group to 5.4% and 4.9% in those aged 75 years and above, respectively. Clinically, two most commonly diagnosed forms of AF are paroxysmal AF (episodes that can terminate spontaneously) and persistent AF (episodes that continue for more than 7 days and do not self-terminate) [3]. Antiarrhythmic drugs (AADs) have traditionally been the mainstay first-line treatment of AF. Over the past decade, attention has shifted from AADs toward radiofrequency catheter ablation (RFCA) owing to a growing body of evidence that AF ablation is a safe and more effective treatment option for restoring and maintaining normal sinus rhythm (NSR) and preventing future AF recurrences [4]. Despite being a minimally invasive procedure, RFCA carries a risk of procedure-related complications and it is, at least initially, substantially more expensive than pharmacotherapy. Unlike health economic studies for prescription drugs, economic evaluation of medical devices tends to be more dynamic and often has a shorter ‘shelf life’ [5]. This is partly because medical devices frequently undergo incremental innovations, some of which may result in significant improvement in efficacy and safety [6]. For example, contact-force catheters (ThermoCool SmartTouch catheter [ST catheter]; Biosense Webster Inc., CA, USA) guided by Ablation Index (AI; Biosense Webster Inc.) render more precise control over energy delivery and have been shown to improve clinical outcomes for AF patients compared with earlier generations of RFCA [7]. Currently, RFCA using AI-guided ST catheter (STAI) has become the device of choice for AF treatment in China.
To date, no economic evaluation of STAI for AF treatment has been conducted using real-world evidence in the context of Chinese clinical practice. In order to provide evidence for clinical and reimbursement decision-making from the perspective of the Chinese healthcare system, we evaluated long-term clinical and economic consequences associated with STAI (STAI group) versus AAD therapy (AADs group) as first-line treatments for Chinese AF patients. This evaluation was based on a real-world study at a tertiary hospital in China, as well as other studies conducted in the Chinese healthcare setting.
Methods
Study design of the real-world study & data collection
To accurately capture real-world evidence in the Chinese healthcare setting for both clinical outcomes and costs, we conducted a single center, prospective observational study at a tertiary care hospital in China. This study enrolled patients who were newly diagnosed with paroxysmal or persistent AF and who were eligible to receive RFCA using AI-guided ST catheter or AAD therapy.
In congruence with the most recent expert consensus statement on catheter and surgical ablation of atrial fibrillation [8], we considered the first three months post-ablation as a blanking period; episodic atrial fibrillation/atrial tachycardia/atrial flutter (AF/AT/AFL) occurring during the blanking period were not counted as AF recurrence. From 4 to 12 months after ablation, AF recurrence was defined as any episodes of AF/AT/AFL > 30 seconds recorded by electrocardiogram, thermal texture maps (TTM), 24-hour Holter monitoring or telemetry. Presence of AF symptoms was not required for the diagnosis of arrhythmia recurrence. Patients receiving AADs were managed at the discretion of treating physicians and clinical outcomes were measured in the same manner as ablation-treated patients, i.e., AAD treatment failure was defined as any episodes of AF/AT/AFL > 30 seconds recorded by electrocardiogram, TTM, 24-hour Holter monitoring or telemetry post the blanking period [1]. All AF patients received anti-coagulant treatment (warfarin or novel oral anticoagulants for RFCA-treated patients and novel oral anti-coagulants for patients receiving AADs).
One-year clinical outcomes and costs were collected in this real-world study, which informed the model parameters. Clinical outcomes included rates of AF recurrence, AAD treatment failure, and complications. As our study is designed from the perspective of the Chinese healthcare system, only direct medical costs were collected, which included hospitalization, outpatient follow-up visits, inpatient and outpatient procedures, lab tests and medication.
Model overview
We simulated clinical and economic consequences for AF patients initially treated with RFCA using AI-guided ST catheter or AADs using a short-term decision tree model leading to a 10-year long-term health state transition Markov model, which is consistent with a prior published study conducted in Chinese settings [9]. Two first-line treatment strategies were evaluated: STAI and AAD therapy. The analysis was performed from the perspective of the Chinese healthcare system. The model was informed by combined data from the local real-world study and previously published clinical studies.
The schematic diagrams of the model are presented in Figure 1a and b. The short-term decision tree model was constructed based on the results of our real-world study in China, capturing both the primary clinical outcomes and costs over one-year time period. The long-term Markov model was built based on previously published long-term cost-utility study of RFCA versus cryoballoon ablation and AADs in Chinese AF patient population, simulating the clinical outcomes and costs over a time horizon of 10 years for a cohort of 10,000 adult patients [9]. The cycle length in the Markov model was one year with a half-year correction. The model simulated expected treatment outcomes and costs for each individual patient driven by transition probabilities of applicable health states over annual cycles. The results of all patients were then pooled and analyzed to estimate the average results per patient for each treatment strategy. To more accurately reflect clinical practice, the model took into consideration of possible repeat ablations in some patients who underwent RFCA but experienced AF recurrence later. In addition, among patients who failed AAD treatment may cross over to ablation treatment. An annualized discount rate for both costs and outcomes was set to 5% [10].
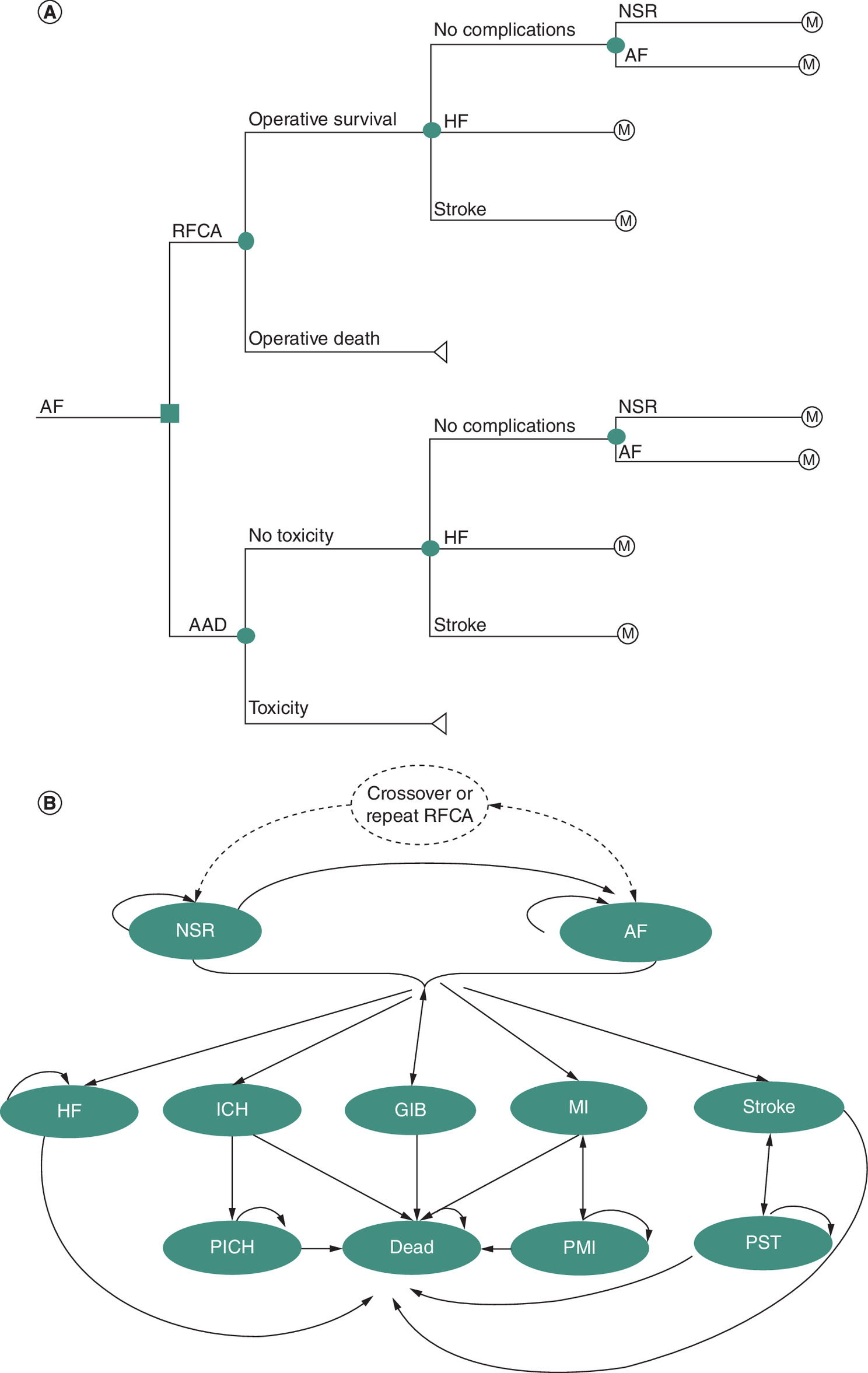
Figure 1. Diagrams of models.
(A) Short-term model. (B) Long-term model.
AAD: Antiarrhythmic drug; AF: Atrial fibrillation; GIB: Gastrointestinal bleeding; HF: Heart failure; ICH: Intracranial hemorrhage; MI: Myocardial infarction; NSR: Normal sinus rhythm; RFCA: Radiofrequency catheter ablation; PICH: Post-intracranial hemorrhage; PMI: Post myocardial infarction; PST: Post stoke.
Model structure
The starting point for the decision tree model was the initial choice of first-line treatment strategy: STAI or AADs therapy. Following the ablation procedure, excluding those who experienced procedure-related death, patients were assigned into one of the four health states as observed in our observational study: (1) NSR; (2) AF; (3) heart failure (HF); and (4) stroke. For patients on AADs therapy, they were either in the state of AAD toxicity or absent of AAD toxicity initially. The later state was further branched out into the same four health states as the STAI group. Based on the real-world study results, STAI-treated patients were defined as being in AF status if they had recurrent AF; AADs-treated patients were defined as being in AF status if they failed the AAD treatment; patients in both treatments were defined as being in NSR status if they were free of any arrhythmia.
The health state transition paths in the Markov model applied to both treatment options. The health states reflect the possible clinical events of AF patients in the long term, including: 1) NSR; 2) AF; 3) HF; 4) intracranial hemorrhage (ICH); 5) gastrointestinal bleeding (GIB); 6) myocardial infarction (MI); 7) stroke; 8) death; 9) post-ICH (PICH); 10) post-MI (PMI); 11) post-stroke (PST). The NSR, AF, HF, and stroke states in the decision tree model are articulated with corresponding states in the Markov model.
In each cycle of simulation, patients may remain in NSR or AF state or transition into one of the five health states: HF; ICH; GIB; MI; and stroke. Additionally, patients in NSR may transition to AF state. Patients surviving the first year of ICH, MI, or stroke would progress to their respective post-complication state (PICH, PMI or PST). Patients may stay in the state of HF, GIB, PICH, PMI or PST or transition into the terminal state of death. For patients in the state of PMI or PST, they may revert to the state of MI or stroke if the complication recurred. Patients in NSR state may transition into AF state as a result of AF recurrence after ablation or failure of AAD treatment, and patients in AF state may transition into NSR state if they experience repeat ablations or crossover. We assumed that no patients discontinue treatment prematurely [10].
Model input
Parameters for short-term decision tree model
Parameters for clinical outcomes and costs for short-term decision tree model were informed with the findings of our real-world study. The observational study enrolled a total of 202 patients and 131 had paroxysmal AF and 71 had persistent AF. Of the study population, 149 underwent ablation using AI-guided ST catheter, which provides real-time contact force data in combination with the Carto 3-dimensional electroanatomic mapping system and 53 were treated with AADs. By the end of 1-year follow-up, no procedure-related death and no AAD toxicity were observed, and freedom of any arrhythmia was significant greater for STAI versus AADs therapy (87.60% vs 63.40%). A total of 4 cases of ischemic strokes occurred (2 in each group) and one case of heart failure observed in AADs group.
From this real-world study, the total direct cost per patient of STAI and AADs therapy in 1 year was ¥79,564 and ¥4428, respectively. The cost of emergency room or urgent care visits were not included in our model due to lack of data. Base-case parameters for the decision tree model are listed in Table 1.
| Parameter | Value | Distribution | Data source |
|---|---|---|---|
| The proportion of STAI operative survival | 1.0000 | Uniform | RWS |
| The proportion of AAD toxicity | 0.0000 | Uniform | RWS |
| The proportion of stroke among STAI patients at the first year | 0.0130 | Beta | RWS |
| The proportion of stroke among AADs patients at the first year | 0.0380 | Beta | RWS |
| The proportion of HF among STAI patients at the first year | 0.0000 | Uniform | RWS |
| The proportion of HF among AADs patients at the first year | 0.0190 | Beta | RWS |
| The proportion of AF among STAI patients at the first year | 0.1224 | Beta | RWS |
| The proportion of AF among AADs patients at the first year | 0.3451 | Beta | RWS |
| Total direct medical cost per patient of STAI | ¥79,572 | Lognormal | RWS |
| Total direct medical cost per patient of AADs therapy | ¥4428 | Lognormal | RWS |
*RWS: Parameters for long-term Markov model were informed with the findings of our real-world study.
AAD: Antiarrhythmic drug; AF: Atrial fibrillation; HF: Heart failure; RWS: Real-world study; STAI: ThermoCool SmartTouch Catheter guided by Ablation Index.
Parameters for long-term Markov model
Base-case parameters for clinical outcomes and costs informing the long-term Markov model were extracted from the literature and listed in Table 2. At the first year of simulation, the proportions of patients in the states of NSR, AF, stroke and HF were identical to the corresponding states of the short-term model. The construction of patient cohort was based on a retrospective 12-month follow-up study in usual care setting in China with starting age of 60 years old and 60% being males as outlined in our previous publication [9]. The annual risk of ischemic stroke in patients on anticoagulant therapy while in AF state was estimated based on the clinical risk stratification using CHA2DS2-VASc score as reported in a clinical trial and hazard ratio (HR = 1.87) in patients with AF on anticoagulant therapy compared with patients in NSR [11,12]. Owing to the aging population, we took into consideration of both background natural cause of death and risk of death attributable to AF or AF related complications. The age- and gender-specific risk of other-cause mortality in the general population was obtained from the 6th China national census data and the mortality risk of AF or AF related complications was derived from the literature [13]. For probabilities of repeat ablation and crossover, additional confirmation was sought from a panel of Chinese clinical experts. We assumed that clinical effectiveness for repeat ablation and crossover was invariant from our real-world study.
| Parameter | Value | Distribution | Data source | Ref. |
|---|---|---|---|---|
| Health outcomes | ||||
| Hazard ratio of stroke in AF state vs NSR state | 1.8700 | Lognormal | Literature | [12] |
| Annual long-term (>1 year) probability of AAD treatment failure | 0.4400 | Beta | Literature | [14] |
| Annual long-term (>1 year) probability of AF recurrence for STAI-treated patients | 0.0528 | Beta | Literature | [15] |
| Annual long-term (>1 year) probability of AAD toxicity | 0.1680 | Beta | Literature | [16] |
| Hazard ratio of HF in AF state vs NSR state | 6.0100 | Lognormal | Literature | [17] |
| Annual probability of HF in NSR state | 0.0013 | Beta | Literature | [18] |
| Hazard ratio of death in HF state vs NSR state | 2.4900 | Lognormal | Literature | [19] |
| Annual probability of ICH for NOACs users | 0.0026 | Beta | Literature | [20] |
| Annual probability of ICH in NSR state | 0.0080 | Beta | Literature | [21] |
| Hazard ratio of death in ICH state vs NSR state | 7.4000 | Lognormal | Literature | [9] |
| Hazard ratio of death in PICH state vs NSR state | 2.1300 | Lognormal | Literature | [22] |
| Annual probability of GIB for NOACs users | 0.0129 | Beta | Literature | [23] |
| Annual probability of GIB in NSR state | 0.0058 | Beta | Literature | [24] |
| Hazard ratio of death in GIB state vs NSR state | 3.5000 | Lognormal | Literature | [9] |
| Hazard ratio of death in Stroke state vs NSR state | 7.4000 | Lognormal | Literature | [9] |
| Hazard ratio of death in PST state vs NSR state | 2.3000 | Lognormal | Literature | [9] |
| Annual probability of MI in NSR state | 0.0017 | Beta | Literature | [9] |
| Hazard ratio of death in MI state vs NSR state | 5.8400 | Lognormal | Literature | [9] |
| Hazard ratio of death in PMI state vs NSR state | 2.2100 | Lognormal | Literature | [9] |
| Annual transition probability of from PMI state to MI state | 0.0546 | Beta | Literature | [9] |
| Hazard ratio of MI in AF state vs NSR state | 1.5400 | Lognormal | Literature | [9] |
| Annual probability of repeat ablation in AF state | 0.3019 | Beta | Literature and verified by KOLs | [25] |
| Annual probability of crossover in AF state | 0.3564 | Beta | Literature and verified by KOLs | [26] |
| Annual probability of AF recurrence after repeat ablation or crossover | 0.1240 | Beta | RWS | / |
| Costs | ||||
|---|---|---|---|---|
| Annual long-term (>1 year) cost of AADs therapy | ¥3000 | Lognormal | Literature | [27] |
| Annual long-term (>1 year) cost of NOACs therapy | ¥8188 | Lognormal | Literature | [27] |
| Annual management cost of AAD toxicity | ¥551 | Lognormal | Literature | [27] |
| Total direct medical cost in HF state | ¥15,763 | Lognormal | Literature | [28] |
| Total direct medical cost in ICH state | ¥44,627 | Lognormal | Literature | [9,29] |
| Annual management cost in PICH state | ¥2913 | Lognormal | Literature | [27] |
| Total direct medical cost in GIB state | ¥13,276 | Lognormal | Literature | [27,30] |
| Total direct medical cost in MI state | ¥50,900 | Lognormal | Literature | [9,31] |
| Annual management cost in PMI state | ¥1125 | Lognormal | Literature | [9] |
| Total direct medical cost in Stroke state | ¥26,613 | Lognormal | Literature | [32] |
| Annual management cost in PST state | ¥3912 | Lognormal | Literature | [27] |
| Total direct medical cost of crossover or repeat ablation | ¥79,564 | Lognormal | RWS | / |
| Annual cost in NSR state | ¥0 | / | / | / |
| Annual cost in Death state | ¥0 | / | / | / |
†
KOL indicates Key Opinion Leaders.
*RWS: Parameters for Markov model were informed with the findings of our real-world study.
AAD: Antiarrhythmic drug; AF: Atrial fibrillation: HF: Heart failure; ICH: Intracranial hemorrhage; GIB: Gastrointestinal bleeding; MI: Myocardial infarction; NSR: Normal sinus rhythm; NOAC: New oral anticoagulant; RWS: Real-world study; STAI: ThermoCool SmartTouch Catheter guided by Ablation Index; PICH: Post-intracranial hemorrhage; PMI: Post myocardial infarction; PST: Post stoke.
Treatment and associated cost related to various health states extracted from literature were obtained from studies conducted in Chinese clinical settings. All patients in the state of AF received new oral anticoagulants (NOACs: rivaroxban and dabigtran) and the cost included both drugs and routine clinical monitoring. For patients who experienced repeat ablations or crossovers, we assumed that they incurred the same annual cost as obtained in the real-world study.
Sensitivity analyses
We conducted both one-way and probabilistic sensitivity analyses (OWSA and PSA) to assess which variables had most influence on model output and robustness of the simulation. For first OWSA, where data available, parameters were varied across the range of their 95% confidence intervals (CIs); otherwise, we assumed that the standard deviation was 10% of the base case values and then calculated the 95% CI based on their assumed distributions. As the time horizon in the long-term model was fairly arbitrary, in the second OWSA, we repeated the base-case simulations with different time horizons varying from 5 years to 15 years.
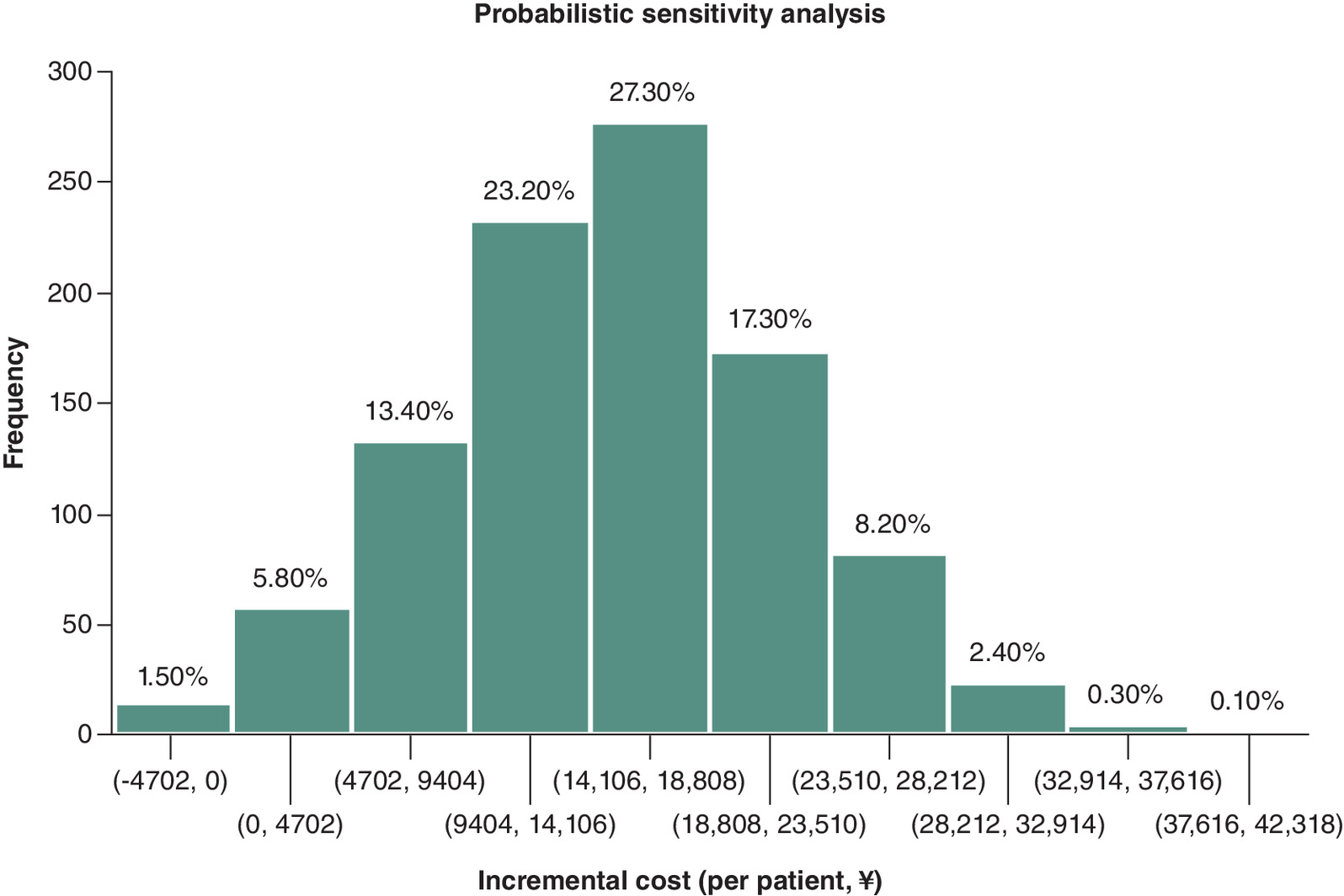
For PSA, we conducted the Monte Carlo simulations with 1000 iterations, each time randomly sampling from the distribution for all parameters simultaneously. We assumed lognormal distribution for the cost parameters and beta distribution for variables expressed in percentage.
Scenario analysis
To conform to most health economic models published in this area, we omitted repeat ablations and crossovers in this scenario analysis. In this scenario, all health and cost consequences in the model were directly associated with the initial therapy modalities.
Results
Base case analysis
Findings of this cost consequence analysis are shown in Table 3. The model projected, compared with AADs group, STAI group was advantageous on all 4 main clinical outcomes evaluated. By end of 10th year, it was estimated that AF was 25.83% lower in STAI group versus AADs group (12.84% vs 38.67%). Similarly, in STAI group, HF was 2.22% lower (1.33% vs 3.55%), stroke or post stroke was 1.82% lower (10.00% vs 11.82%) and death due to AF and AF related complications was 0.64% lower (4.11% vs 4.75%) compared with AADs group.
| Consequences (at the 10th year) | STAI Group | AADs Group | Difference |
|---|---|---|---|
| Clinical outcomes (prevalence) | |||
| AF | 12.84% | 38.67% | 25.83% |
| HF | 1.33% | 3.55% | 2.22% |
| Stroke and PST | 10.00% | 11.82% | 1.82% |
| Death due to AF or AF related complications | 4.11% | 4.75% | 0.64% |
| Costs | |||
|---|---|---|---|
| Total Cost | ¥123,124 | ¥139,806 | ¥16,682 |
| Cost due to AF | ¥115,551 | ¥129,410 | ¥13,859 |
| Cost due to HF | ¥678 | ¥3099 | ¥2421 |
| Cost due to Stroke and PST | ¥3915 | ¥5302 | ¥1387 |
AAD: Antiarrhythmic drug; AF: Atrial fibrillation; HF: Heart failure; PST: Post stoke; STAI: ThermoCool SmartTouch Catheter guided by Ablation Index.
On the cost front, the Markov model projected that STAI group incurred lower overall medical costs compared with AADs group in the long term; the average total cost per patient in STAI group was estimated to be ¥16,682 lower than that of AADs group (¥123,124 vs ¥139,806). The cost breakdown showed that the total cost savings in the STAI group came primarily from the lower risk of AF episodes – the STAI group saved ¥13,859/patient associated with AF status compared with the AADs group.
Sensitivity analysis
OWSA
Results of the first OWSA are illustrated in the tornado diagram (Figure 2). The difference in total cost per patient between the two groups was most sensitive to long-term (>1 year) annual probability of AAD treatment failure and annual cost of NOACs therapy. In addition, the incremental cost was also sensitive to the total direct medical cost of STAI, discount rate, and annual probability of crossover.
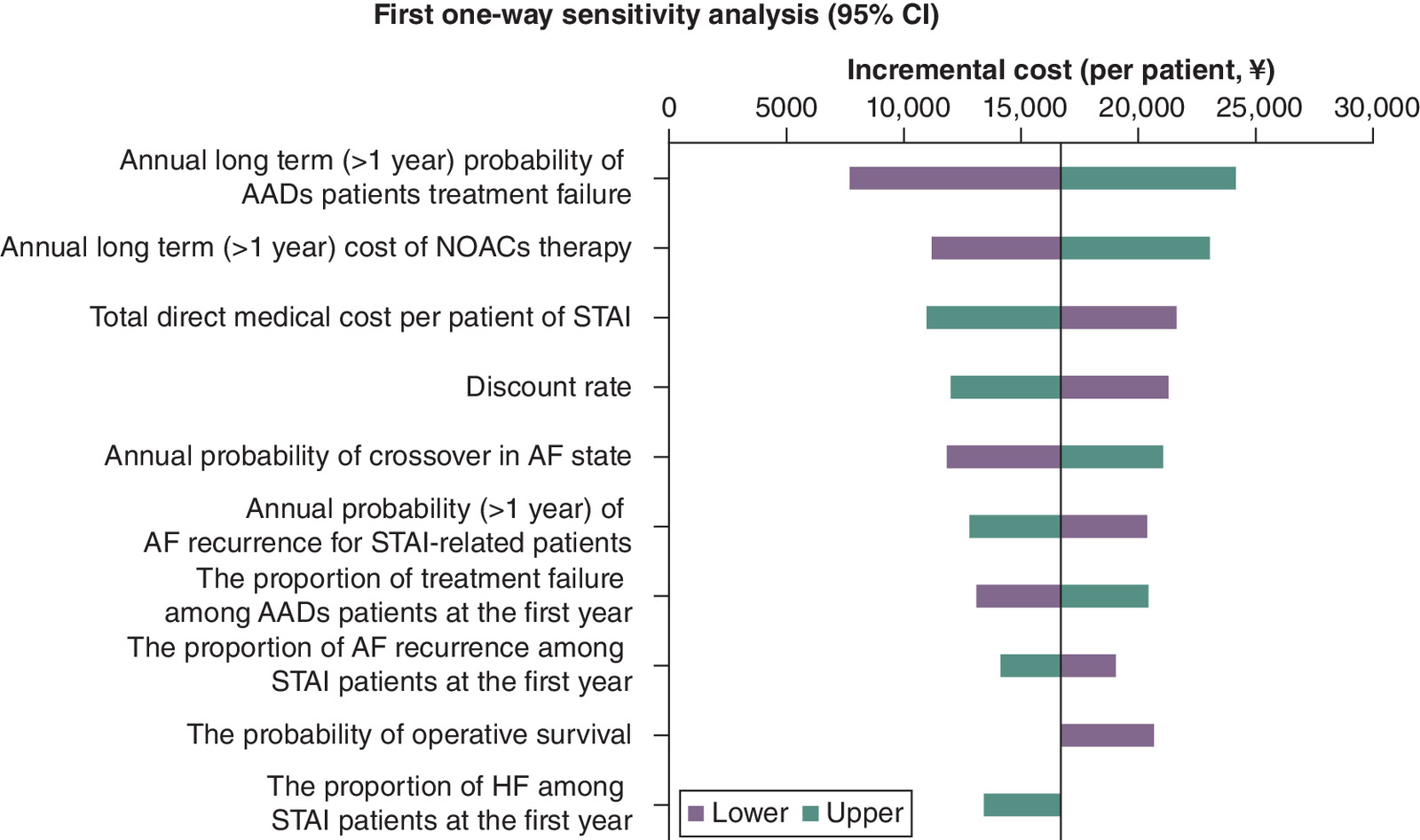
Figure 2. First one-way sensitivity analysis – incremental cost (per patient) between STAI and antiarrhythmic drug groups.
Only variations with impact on the base case result are shown in the chart.
*Each parameter varied across the range of their 95% confidence intervals (CIs); if the 95% CI of the parameter was not available, we assumed that the standard deviation was 10% of the base case values and then calculated the 95% CI based on their assumed distributions.
AADs: Antiarrhythmic drugs; AF: Atrial fibrillation; HF: Heart failure; NOACs: New oral anticoagulants; STAI: ThermoCool SmartTouch Catheter guided by Ablation Index.
The second OWSA on varying time horizons (5–15 years) indicated that AAD treatment had cost advantage up to 7 years post treatment but the cost advantage reversed in favor of RFCA with the increased time horizon of 8 years or longer. The cost savings associated with RFCA was continuously enlarged with a longer time horizon (Figure 3).
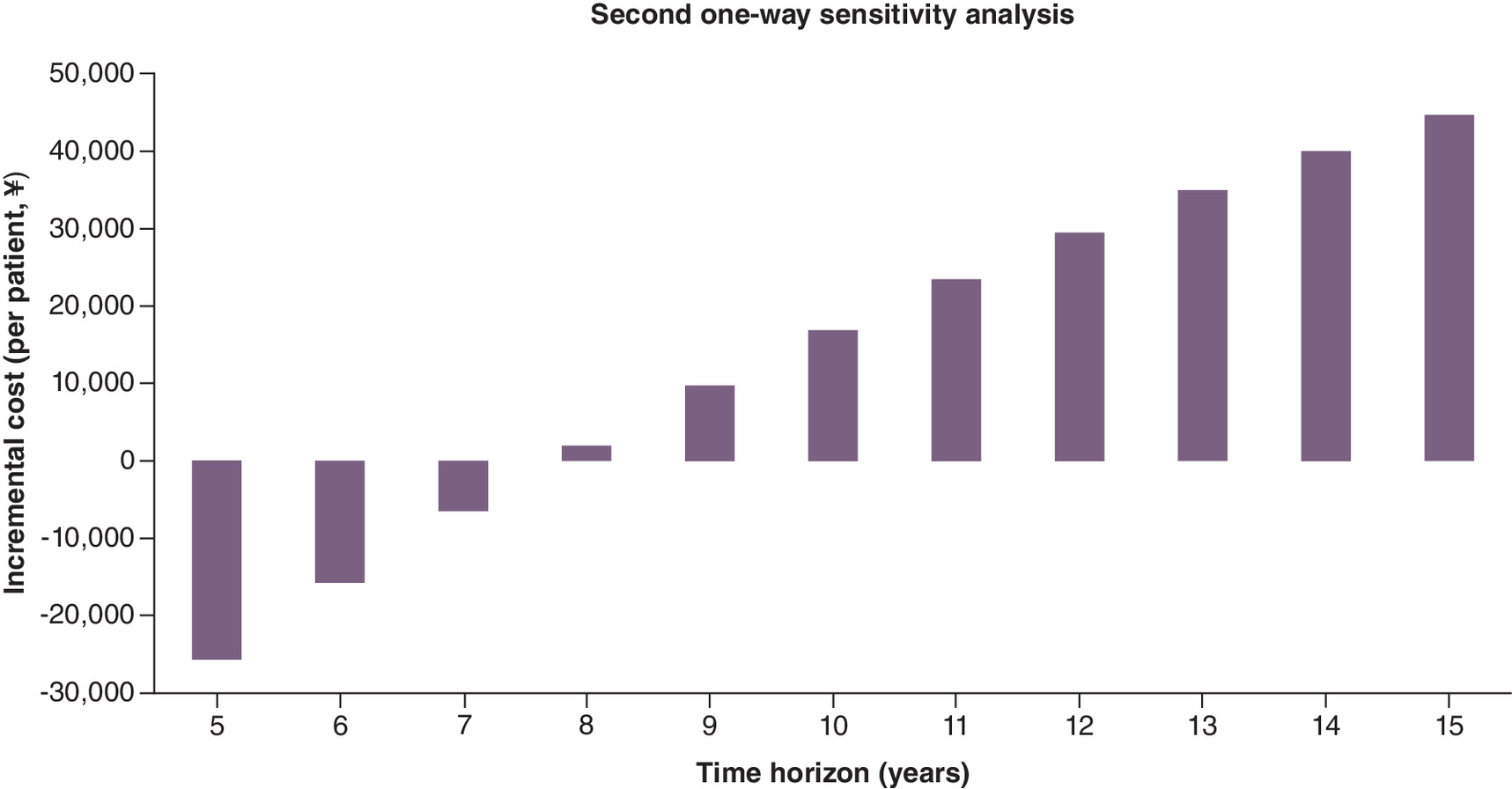
Figure 3. Second one-way sensitivity analysis – incremental costs (per patient) between STAI and antiarrhythmic drug groups (varying time horizon).
Only variations with impact on the base case result are shown in the chart.
The result of PSA (Figure 4) showed that by the end of 10th year, there was a probability of 98.5% that treatment with STAI could result in cost savings, indicating that our results are robust.
Scenario analyses
In the scenario analysis, similar to most prior health economic research in this area, we assumed that no crossover or repeat ablation was allowed. As a result, more prominent clinical advantages were projected for STAI group. By the 10th year, compared with AADs group, patients in STAI group had an estimated 35.76% lower AF (33.89% vs 69.65%), 5.83% lower strokes (13.21% vs 19.04%), 3.97% lower HF (2.21% vs 6.18%), and 1.93% lower deaths attributable to AF or AF related complications (4.67% vs 6.60%).
Discussion
Results from our analysis indicated that, despite a higher upfront cost, first-line treatment for paroxysmal or persistent AF using ablation with STAI, when compared with drug therapy, could result in better clinical outcomes at lower costs over a 10-year horizon.
Our model projected that STAI treatment was associated with estimated reductions of 25.83% in AF recurrence, 2.23% in HF incidence, 1.82% in stroke incidence, and 0.64% in mortality due to AF or AF related complications. In addition, the STAI group accrued total cost savings of ¥16,682/patient over ten years, compared with the AADs group, mainly due to savings in treatment costs from lower incidence of AF episodes in the STAI group. Analyses with varying time horizons showed that total costs were lower with drug therapy in the earlier years of treatment, but the cost advantage reversed in favor of RFCA once the time horizon was extended to eight years or longer.
To our knowledge, this study is the first health economic evaluation using a cost-consequence approach to compare two common strategies for first-line treatment of AF, i.e., STAI and AAD therapy. Chinese healthcare system is characterized by a predominantly public healthcare market on both the provider and payer side. Our research is conducted from the perspective of the healthcare system; as such, our results could provide rationale for payers to make informed choice in their consideration of insurance coverage. In addition, by employing a cost-consequence framework, our study allows for considering various costs and health outcomes according to local contexts and priorities. This approach provides intuitive and valuable insights to various decision makers, including payers who are responsible for reimbursement decisions, as well as hospital administrators and clinicians who are engaged in procurement and AF treatment process. However, it should be acknowledged that our real-world data was based on a single-center study, which may not be representative of standard of care and costs in hospitals of other regions.
Results from our study are qualitatively consistent with previously published model-based economic evaluations. Two health economic studies compared the cost–effectiveness of RFCA with drug therapy from the perspective of third-party healthcare payers in China. Du et al. structured a 12-month short-term decision tree model leading to a Markov model that simulated long-term treatment outcomes and costs [27]. Similar to our study, the short-term model was populated with data from a prospective observational study, in which ST catheters were used but they were not guided with AI. Nevertheless, their study showed that the incremental cost–effectiveness ratio (ICER) of RFCA versus AADs was ¥66,764, ¥36,280, and ¥29,359 per QALY at time horizons of 8, 15, and 20 years, respectively. The authors concluded that ablation treatment was cost-effective over the long-term. Hu et al. applied discrete event simulation to evaluate the lifetime cost–effectiveness of first-line treatment using STAI, second-generation of cryoballoon ablation (CB2), or AADs [33]. The main clinical parameters populating this model were derived from a meta-analysis of global clinical trials. The model projected ICERs of $5927 per QALY for STAI versus AADs and $12,167 per QALY for CB2 versus AADs, with both ablation technologies being considered cost-effective relative to AADs. The major difference between our study and the prior economic assessments of AF ablation is the explicit incorporation of possible repeat ablations and crossover treatment. When considering these factors in real clinical practice, our research indicates that, compared with AADs, STAI as first-line AF treatment is the dominant strategy in the long term.
There are a number of cost–effectiveness evaluations of RFCA versus AADs in several other countries, including Canada, UK, US, and Sweden [34–41]. Despite variations in modeling approaches, assumptions, patient populations, standards of care, cost of ablation procedures relative to other medical services, and willingness-to-pay thresholds, among other factors, these studies agree that RFCA is a cost-effective alternative to AAD therapy. In addition, the base-case results of the Swedish study indicated that RFCA could reduce costs and improve patient outcomes as measured by QALYs. Unlike AAD treatment, the cost for RFCA is front-loaded. As expected, studies which examined the impact of different time horizons found that longer time horizons consistently yielded more favorable ICERs.
Several design features in our study are worth mentioning. First, the bulk of prior health economic evaluations of RFCA versus drug therapy focused on AF patients who were refractory to at least one AAD, i.e., these studies assessed RFCA as a second-line treatment, largely reflecting the then prevailing clinical guidelines and available clinical trial evidence [42,43]. It is worth noting that the latest guidelines by the European Society of Cardiology suggest that catheter ablation can be used for patients with proximal AF without the prerequisite AAD treatment failure [44,45].
Second, our model included both direct medical costs and one-year clinical outcomes of STAI and AAD therapy in real-world clinical practice in China, while previous economic evaluations set in China were based on data of early-generation ablation technologies or global clinical practice. The results of our real-world study suggested that, STAI was associated with higher arrhythmia-free survival at one year, which is consistent with findings from several previous studies. Therefore, this real-world study confirms enhanced clinical effectiveness of STAI in clinical practice in China. In addition, this study is the first in China to account for treatment crossovers and repeat ablations as part of the base-case scenario. In scenarios where these practices were omitted, the model projected better clinical outcomes for STAI treatment than the base-case scenario. Although both treatment crossovers and repeat ablations are frequent in clinical practice, most prior health economic research did not account for these practices and examine their impact on cost–effectiveness. We believe that this study can better support policy decision-making by reflecting routine clinical practice more comprehensively.
Our study has several limitations. First, the results from the real-world study that informed the short-term model were based on a single center study with a relatively small sample size. As a result, we did not observe any procedure-related complications, deaths, or severe AAD-related drug toxicity events. However, we incorporated the risk of AAD-related toxicity in the long-term model, as effective drug therapy requires taking medications for a prolonged period. These results from a single center may not be representative of current practice in other regions of China. Secondly, the incidence of arrhythmia recurrence may have been underestimated, particularly for patients with sporadic arrhythmia episodes, as routine follow-up visits were impacted by the coronavirus epidemic. In addition, the cost outcome in our study was sensitive to the probability of treatment crossover, which likely varies considerably across countries. Owing to the lack of real-world data in this regard in China, we relied on statistics reported from global studies, which were validated by local clinical experts. Finally, our study did not consider patient quality of life as a clinical outcome. Multiple studies have shown that ablation treatment greatly improves patients' quality of life. Incorporating health utility measures could potentially lead to even more favorable results for STAI relative to AAD treatment [46–49].
Conclusion
Radiofrequency catheter ablation using SmartTouch catheter guided by Ablation Index was superior to antiarrhythmic drugs as the first-line AF treatment in Chinese setting with better clinical outcomes and at lower costs over a 10-year time horizon.
Summary points
•
This study simulated clinical and economic consequences for atrial fibrillation (AF) patients initially receiving ThermoCool SmartTouch Catheter guided by Ablation Index (STAI) or antiarrhythmic drugs (AADs) using a short-term decision tree model leading to a 10-year long-term Markov model from Chinese healthcare system perspective.
•
Our model reflected routine clinical practice by taking into consideration of possible repeat ablations in some patients who underwent radiofrequency catheter ablation (RFCA) but experienced AF recurrence later. In addition, among patients who failed AAD treatment may cross over to ablation treatment.
•
The model was built on the Chinese real-word study and one-year clinical outcome and costs were collected in this real-world study, which informed the model parameters.
•
The real-world study was a single center, prospective, observational study at a tertiary care hospital in China in patients newly diagnosed with paroxysmal or persistent AF and who were eligible to receive RFCA using AI-guided ST catheter or AADs therapy.
•
From this real-world study, the total direct cost per patient of STAI and AADs therapy in 1 year was ¥79,564 and ¥4,428, respectively.
•
From this real-world study, by the end of 1-year follow-up, no procedure-related death and no AAD toxicity were observed, and freedom of any arrhythmia was significant greater for STAI versus AADs therapy (87.60% vs 63.40%). A total of 4 cases of ischemic strokes occurred (2 in each group) and one case of heart failure observed in AADs group.
•
By end of 10th year, it was estimated that AF was 25.83% lower in STAI group versus AADs group (12.84% vs 38.67%). Similarly, heart failure (HF) was 2.22% lower (1.33% vs 3.55%), stroke or post stroke was 1.82% lower (10.00% vs 11.82%) and death due to AF and AF related complications was 0.64% lower (4.11% vs 4.75%) compared with AADs group.
•
The average total cost per patient in STAI group was estimated to be ¥16,682 lower than that of AADs group (¥123,124 vs ¥139,806). The cost breakdown showed that the total cost savings in the STAI group came primarily from the lower risk of AF episodes.
•
The incremental cost was most sensitive to long-term (>1 year) annual probability of AAD treatment failure and annual cost of NOACs therapy.
•
Varying time horizons (5–15 years) indicated that AAD treatment had cost advantage up to 7 years post treatment but the cost advantage reversed in favor of RFCA with the increased time horizon of 8 years or longer. The cost savings associated with RFCA was continuously enlarged with a longer time horizon.
•
The study findings were limited by, among others, model input from a local real-world study which was based on a single center study and had a relatively small sample size.
Author contributions
L Zheng, B Zhang, C Zuo and J Xuan contributed to the study conception and design; L Zheng, B Zhang, J Han, D Zhou, J Jiang, A Zu, J Zhong, Y He, X Sun, L Chen and Y Lu were responsible for acquisition of data; L Zheng, B Zhang, X Lu and C Zuo were responsible for data analysis; C Zuo was responsible for drafting the manuscript; L Zheng and B Zhang and J Xuan were responsible for revision of the manuscript.
Financial disclosure
This work was supported by Johnson & Johnson Medical (China) Co. Ltd. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interest disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
Manuscript writing and editorial assistance was provided by X Henry Hu of Summit Health Outcomes, Summit, NJ, USA.
Ethical conduct of research
The author state that approval was obtained from the Clinical Ethics Committee of First Affiliated Hospital, Zhejiang University School of Medicine. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. The data will not be made publicly available.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Calkins H, Hindricks G, Cappato R et al. HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace 20(1), e1–e160 (2018).
•• Expert consensus statement on catheter and surgical ablation of atrial fibrillation with supporting clinical evidence.
2.
Du X, Guo L, Xia S et al. Atrial fibrillation prevalence, awareness and management in a nationwide survey of adults in China. Heart 107(7), 535–541 (2021).
3.
January CT, Wann LS, Alpert JS et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 64(21), e1–e76 (2014).
4.
National Institute for Health and Care Excellence Clinical Guidelines. Atrial Fibrillation: Management. National Institute for Health and Care Excellence, UK (2014).
5.
Kirisits A, Redekop WK. The economic evaluation of medical devices. App. Health Econ. Health Pol. 11(1), 15–26 (2013).
6.
Drummond M, Griffin A, Tarricone R. Economic evaluation for devices and drugs–same or different? Value Health 12(4), 402–404 (2009).
7.
Gupta D, Potter T, Disher T et al. Comparative effectiveness of catheter ablation devices in the treatment of atrial fibrillation: a network meta-analysis. J. Comp. Eff. Res. 9(2), 115–126 (2020).
8.
Calkins H, Hindricks G, Cappato R et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 14(10), e275–e444 (2017).
9.
Sun XR, He SN, Lin ZY et al. Radiofrequency catheter ablation versus cryoballoon ablation in the treatment of paroxysmal atrial fibrillation: a cost–effectiveness analysis in China. Clin. Ther. 41(1), 78–91 (2019).
• This study is a cost–effectiveness analysis study of radiofrequency catheter ablation (RFCA) vs cryoballoon ablation and antiarrhythmic drugs (AADs) in Chinese AF patient population, simulating the clinical outcomes and costs over a time horizon of 10 years for a cohort of 10,000 adult patients, with supporting clinical pathway and the model structure evidence.
10.
China Guidelines for Pharmacoeconomic Evaluations Working Group. China guidelines for pharmacoeconomic evaluations [content in Chinese]. China Center for Health Economic Research, (2011).
•• These guidelines provide methodological guidance for pharmacoeconomic evaluations in China, including recommendation on study perspectives, time horizon, data sources and thresholds for decision making, etc.
11.
Cardoso R, Mendirichaga R, Fernandes G et al. Cryoballoon versus radiofrequency catheter ablation in atrial fibrillation: a meta-analysis. Cardiovasc. Electrophysiol. 27, 1151–1159 (2016).
12.
Journal of Cardiovascular and Pulmonary Diseases Working Group. Annual Report on Cardiovascular Health and Diseases in China [content in Chinese]. J. Cardiovasc. Pulmonary Dis., (2019).
13.
Stats.gov. Sixth Census. http://www.stats.gov.cn/ztjc/zdtjgz/zgrkpc/dlcrkpc/ (2022).
•• The age- and gender- specific risk of other-cause mortality in the general Chinese population.
14.
Fang Y, Wenbo H, Chao Z et al. Radiofrequency ablation versus antiarrhythmic drug therapy for atrial fibrillation: meta-analysis of safety and efficacy. J. Cardiovasc. Pharmacol. 73, 241–247 (2019).
15.
Tilz RR, Heeger CH, Wick A et al. Ten-year clinical outcome after circumferential pulmonary vein isolation utilizing the Hamburg approach in patients with symptomatic drug-refractory paroxysmal atrial fibrillation. Circ. Arrhythm Electrophysiol. 11, e005250 (2018).
16.
Pappone C, Rosanio S, Augello G et al. Mortality, morbidity, and quality of life after circumferential pulmonary vein ablation for atrial fibrillation: outcomes from a controlled nonrandomized long-term study. J. Am. Coll. Cardiol. 42(2), 185–197 (2003).
17.
Vermond RA, Geelhoed B, Verweij N et al. Incidence of atrial fibrillation and relationship with cardiovascular events, heart failure, and mortality: a community-based study from the Netherlands. J. Am. Coll. Cardiol. 66(9), 1000–1007 (2015).
18.
Hao G, Wang X, Chen Z et al. Prevalence of heart failure and left ventricular dysfunction in China: the China hypertension survey, 2012–2015. Eur. J. Heart Fail 21(11), 1329–1337 (2019).
19.
Ahmed A, Allman RM, Fonarow GC et al. Incident heart failure hospitalization and subsequent mortality in chronic heart failure: a propensity-matched study. J. Card. Fail. 14(3), 211–218 (2008).
20.
Pan LH, Zhao SS. Re-recognition of Oral Anticoagulant-associated Hemorrhage. Prac. J. Cardia Cerebral Pneumal. Vasc. Dis. 30(02), 1–6 (2022).
21.
Tian Y, Ma CH, Zhao MM, Chen GX. Effect of anticoagulant therapy on ischemic stroke in early AF patients on hemodialysis. Chin. J. Geriatr. Heart Brain 18(04), 388–390 (2016).
22.
Banerjee G, Ambler G, Wilson D et al. Baseline factors associated with early and late death in intracerebral haemorrhage survivors. Eur. J. Neurol. 7(7), 1257–1263 (2020).
23.
Steinberg BA, Simon DN, Thomas L et al. Management of major bleeding in patients with atrial fibrillation treated with non-vitamin K antagonist oral anticoagulants compared with warfarin in clinical practice (from Phase II of the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation [ORBIT-AF II]). Am. J. Cardiol. 119(10), 1590–1595 (2017).
24.
Blackhouse G, Assasi N, Xie F et al. cost–effectiveness of catheter ablation for rhythm control of atrial fibrillation. Int. J. Vasc. Med. 2013, 262809 (2013).
25.
Andrade JG, Champagne J, Dubuc M et al. Cryoballoon or radiofrequency ablation for atrial fibrillation assessed by continuous monitoring: a randomized clinical trial. Circulation 140(22), 1779–1788 (2019).
• This study compared the efficacy of cryoballoon with radiofrequency ablation reporting the percentage of expiring repeat ablation patients with radiofrequency ablation.
26.
Andrade JG, Wells GA, Deyell MW et al; EARLY-AF Investigators. Cryoablation or drug therapy for initial treatment of atrial fibrillation. N. Engl. J. Med. 384(4), 305–315 (2021).
• This study compared the efficacy of cryoballoon with drug therapy reporting the percentage of crossover to ablation patients.
27.
Du X, He X, Jia Y et al. A long-term cost–effectiveness analysis comparing radiofrequency catheter ablation with antiarrhythmic drugs in treatment of Chinese patients with atrial fibrillation. Am. J. Cardiovasc. Drugs 19, 569–577 (2019).
28.
Huang J, Yin H, Zhang M, Ni Q, Xuan J. Understanding the economic burden of heart failure in China: impact on disease management and resource utilization. J. Med. Econ. 20(5), 549–553 (2017).
29.
Xuan J, Cheng P, Hu Z. Comparative analysis on hospitalization expenses for cerebral hemorrhage in different medical insurances. Modern Hosp. Manag. 13(04), 66–68 (2015).
30.
Jing F, Guo J, He J et al. Analysis of the hospitalization cost of 93 aged patients with acute upper gastrointestinal bleeding. MMJC 12(6), 3 (2010).
31.
Huang G, Zhang Y, Zheng G et al. Influencing factors of hospitalization expenses in patients with acute myocardial infarction. Chinese J. Health Stat. 38(1), 4 (2021).
32.
Meng X, Wang A, Wang R, Wu S, Han Y. Direct cost and indirect cost of ischemic stroke in China. Value Health, https://www.ispor.org/docs/default-source/euro2022/poster-stroke-burden1020clean-pdf.pdf?sfvrsn=a690d101_0 (2022).
33.
Hu M, Han Y, Zhao W, Chen W. Long-term cost–effectiveness comparison of catheter ablation and antiarrhythmic drugs in atrial fibrillation treatment using discrete event simulation. Value Health 25(6), 975–983 (2022).
34.
Khaykin Y, Mallow PJ, Rizzo JA et al. cost–effectiveness of catheter ablation versus antiarrhythmic drug therapy for the treatment of atrial fibrillation: a Canadian perspective. J. Health Econ. Outcomes Res. 3, 1–12 (2016).
35.
Blackhouse G, Assasi N, Xie F et al. cost–effectiveness of catheter ablation for rhythm control of atrial fibrillation. Int. J. Vasc. Med. 2013, 262809 (2013).
36.
Leung LWM, Imhoff RJ, Marshall HJ et al. cost–effectiveness of catheter ablation versus medical therapy for the treatment of atrial fibrillation in the United Kingdom. J. Cardiovasc. Electrophysiol. 33(2), 164–175 (2022).
37.
NICE. Guideline atrial fibrillation: diagnosis and management, final. https://www.nice.org.uk/guidance/ng196 (2022).
38.
Chan PS, Vijan S, Morady F, Oral H. cost–effectiveness of radiofrequency catheter ablation for atrial fibrillation. J. Am. Coll. Cardiol. 47(2), 2513–2520 (2006).
39.
Reynolds MR, Zimetbaum P, Josephson ME, Ellis E, Danilov T, Cohen DJ. cost–effectiveness of radiofrequency catheter ablation compared with antiarrhythmic drug therapy for paroxysmal atrial fibrillation. Circ. Arrhythm Electrophysiol. 2(4), 362–369 (2009).
40.
Chew DS, Li Y, Cowper PA et al. cost–effectiveness of catheter ablation versus antiarrhythmic drug therapy in atrial fibrillation: the CABANA randomized clinical trial. Circulation 146, 535–547 (2022).
41.
Eckard N, Davidson T, Walfridsson H, Levin LÅ. cost–effectiveness of catheter ablation treatment for patients with symptomatic atrial fibrillation. J. Atr. Fibrillation 2(2), 195 (2009).
42.
Skanes AC, Healey JS, Cairns JA et al; Canadian Cardiovascular Society Atrial Fibrillation Guidelines Committee. Focused 2012 update of the Canadian Cardiovascular Society atrial fibrillation guidelines: recommendations for stroke prevention and rate/rhythm control. Can. J. Cardiol. 28(2), 125–136 (2012).
43.
Calkins H, Brugada J, Packer DL et al. Heart Rhythm Society; European Heart Rhythm Association; European Cardiac Arrhythmia Society; American College of Cardiology; American Heart Association; Society of Thoracic Surgeons. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Arrhythmia Society (ECAS); in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and the Society of Thoracic Surgeons (STS). Endorsed and approved by the governing bodies of the American College of Cardiology, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, and the Heart Rhythm Society. Europace 9(6), 335–379 (2007).
44.
Chinese Society of Pacing and Electrophysiology, Chinese Society of Arrhythmias, Atrial Fibrillation Center Union of China. Current knowledge and management of atrial fibrillation: consensus of Chinese experts 2021. Chin. J. Cardiac Arrhyth. 26, 15–88 (2022).
45.
Hindricks G, Potpara T, Dagres N et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 42(5), 373–498 (2021).
46.
Wilber DJ, Pappone C, Neuzil P et al. ThermoCool AF Trial Investigators. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA 303(4), 333–340 (2010).
47.
Wazni OM, Marrouche NF, Martin DO et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. JAMA 293, 2634–2640 (2005).
48.
Zheng ZH, Fan J, Ji C et al. Long-term outcomes and improvements in quality of life in patients with atrial fibrillation treated with catheter ablation vs. antiarrhythmic drugs. Am. J. Cardiovasc. Drugs 21(3), 299–320 (2021).
49.
Chew DS, Li Y, Cowper PA et al. cost–effectiveness of catheter ablation versus antiarrhythmic drug therapy in atrial fibrillation: the CABANA randomized clinical trial. Circulation 146(7), 535–547 (2022).
Information & Authors
Information
Published In
Copyright
© 2024 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 16 March 2023
Accepted: 27 November 2023
Published online: 11 January 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Radiofrequency ablation using the ThermoCool SmartTouch Catheter guided by ablation index versus antiarrhythmic drugs in atrial fibrillation treatment in China: a cost-consequence analysis. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0035
Export citation
Select the citation format you wish to export for this article or chapter.