Phone contacts and treatment discontinuation predict survival cancer patients in a subsidized drug access program
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Survival of patients with Hodgkin’s lymphoma is lower in in low- and middle-income countries, but factors leading to these outcomes are poorly understood. The objective of this study was to identify predictive factors associated with overall survival among cancer patients undergoing therapy in seven low- and middle-income countries. Materials & methods: A multicenter cohort was conducted in Egypt, Malaysia, Mexico, Peru, Philippines, Thailand and Ukraine. Results. A total of 460 patients were included. Phone-based support during patient follow-up and number of patients seen by the physician provided a positive impact, while the number of adverse events remains a predictor of death and physician decision to stop treatment. Conclusion: Furthers research on the potential benefit of phone-based programs to support patients with chronic diseases treatments should be explored in less developed countries.
Tweetable abstract
Study shows that phone-based support during patient follow-up and number of patients seen by the physician provided a positive impact on survival among cancer patients.
Plain language summary
What is this article about?
The high cost of cancer medication and a shortage of doctors who specialize in cancer care makes it hard for many patients in low- and middle-income countries to get cancer treatment. To find out what other factors play a role in cancer patient survival, this study looked at cancer patients who received medication at no or at low cost depending on what they could afford. It also looked at what factors play a role in the decision by the physicians treating these patients to recommend that the patient stop taking the cancer medicine.
What were the results?
We found that patients who were contacted by telephone during their treatment to find out how they were doing, if they were taking their medication, if they were experiencing side effects, etc., were more likely to be alive at the end of the study. We also found that doctors who see more cancer patients were less likely to recommend that patients stop taking their cancer medication.
What do the results of the study mean?
These results mean that reaching out to patients by phone to help them stay on their cancer medication and make sure they have support in managing side effects or scheduling appointments can help them live longer. Based on this finding, it may be helpful to include this kind of phone contact as part of routine cancer treatment. These results also show that physicians who have more experience treating cancer patients are more likely to recommend that their patients stay on their medication, which can also help improve survival. This suggests that helping more physicians gain experience with newer cancer medications could help their patients live longer.
Hodgkin’s lymphoma (HL) is a rare B cell lymphoma. In 2018, there were nearly 80,000 new HL cases and about 26,000 HL deaths worldwide [1], but HL incidence varies with age, gender and country [2]. An analysis of the Global Burden of Disease study found that less-developed regions had a lower incidence, but a higher mortality of HL compared with developed regions [3]. A Quality of Care Index (QCI) has recently been developed and used to evaluate the quality of care for hematologic malignancies among different populations [4]. A QCI evaluation of HL found an overall age-standardized QCI score of 76.3 (0–100 scale), but this varied from as high as 99.8 in developed countries (Australia, Iceland and Finland) to as low as 9.6–10.2 in less-developed countries (Eritrea, Somalia and Burundi) [4]. This study also found that areas with low socio–demographic index scores had QCI scores that were below global average scores.
While these studies make clear that quality of care and survival of patients with HL is lower in countries with less-developed economies, the factors that lead to these outcomes remain unclear. A recent evaluation of factors impacting global access to cancer therapy found that lack of approval of novel therapies, patient financial capacity to access specialized care, lack of universal healthcare coverage and limited oncology support services (laboratory, imaging, surgery and radiotherapy) negatively impacted patient access to cancer medicines [5].
Brentuximab vedotin (BV) is a CD30-directed antibody–drug conjugate indicated for the treatment of adults with several types of HL. Clinical trial and routine data demonstrate that BV prolongs progression-free survival, with a 43% reduction in the risk of disease progression or death [6]. Five-year data from a clinical trial found a statistically significant improvement in overall progression-free survival favoring the BV+AVD arm (82.2 vs 75.3%, [p = 0.002]) [7]. Although the recommended BV dosage varies based on disease indication, administration every 3 weeks is a common dosing schedule. Treatment usually continues for a maximum of 12 or 16 cycles, but may be stopped after fewer cycles in the event of unacceptable toxicity and/or the occurrence of adverse events (AEs).
The impact of physician behavior on outcomes for patients treated with BV in low- and middle-income countries (LMICs) is not well understood. Physician experience has been shown to impact survival in patients with lymphoma and physician experience using BV in the treatment of HL may be limited in LMICs in which BV is not typically used in clinical practice [8,9]. Additionally, the ability for physicians and patients in these countries to manage the side effects associated with BV is also not well understood. Treatment-related side effects and complications, including BV induced neurotoxicity, which is the most common non hematologic complication of BV therapy [10], may negatively impact quality of life and may cause stress for patients and physicians that may alter the quality of care.
A variety of factors associated with mortality and physician decision to stop treatment have been identified. One clear factor is that, without donor support, the cost of cancer medications for patients in LMICs can be a substantial barrier to access [11–13]. Strategies for addressing affordability, including reducing co-pays, increasing pricing transparency and establishing market entry agreements that increase access to new cancer drugs by balancing the cost of uncertainty in pricing between the holder of the market authorization and healthcare payers [5,14]. However, these strategies require structural changes to how healthcare is delivered and funded and their development and implementation will take significant time and coordination among multiple governmental and non governmental players.
The impact of other strategies, including patient targeted communication during treatment that could be more easily and rapidly deployed to improve outcomes for patients with cancer in LMICs have not been well studied. One recent study found that patient-initiated emails are associated with a survival benefit among patients with cancer undergoing chemotherapy [15], while another found that telephone follow-up of patients with cancer had a positive impact on clinical, psychological and quality of life dimensions [16]. A recent review also found that the use of telehealth interventions focusing on early identification of treatment-related symptoms in adults with hematologic malignancies positively impacted patient health, including an overall decline in chemotherapy delays, decreased rates of dose reductions and improved communication that supported real-time management of acute and chronic treatment-related side effects [17]. However, the primary studies and many of the studies evaluated in the review were conducted in countries with well developed economies and their relevance to the experience of patients in LMICs is under investigated.
Importantly, the COVID-19 pandemic has fostered a shift toward the increased use of a variety of telehealth-based methods for patient-provider communication. As this trend will likely persist as COVID-19 continues to circulate, understanding how these methods can be utilized in the context of cancer care may provide insights that can improve the treatment experience and longer-term outcomes for patients with cancer.
The aim of this study was to identify predictive factors associated with overall survival and physician decision to discontinue the BV treatment, especially the potential effect of communication interventions, among cancer patients undergoing therapy in seven LMICs.
Materials & methods
Study setting & design
In 2018, a BV Access Program was implemented in seven LMICs (Egypt, Malaysia, Mexico, Peru, Philippines, Thailand and Ukraine), by Axios International. The BV Program utilizes the validated Patient Financial Eligibility Tool (PFET) to determine patients ability to pay for treatment and, based on the results of individual PFET assessments, program participants paid for a predetermined number of BV treatment cycles and received the remaining treatment cycles for free [18]. Consequently, the access program reduces financial and other barriers to accessing BV therapy and enables evaluation of other patient and physician factors that impact the end points of physician’s decision to discontinue treatment early and patient mortality. The program uses a personalized approach adapted to the needs of patients with CD30+ hematologic malignancies who are treated with BV.
In addition to reducing patients’ financial burden, the BV Access Program also included patient support and follow-up through phone- and email-based patient contact. This support included delivering information and documentation to the patients at the start of the program, described modalities of care, organization of treatment and follow-up, organizing physician and hospital appointments, prevention and detection of side effects and coordinating complementary therapies and clinical examinations. The vast majority of patients received contact by both phone and email; 3.7% of patients did not receive contact by email, and there was no significant difference in the proportion of patients who did not receive email contact by country (data not shown).
As part of its evaluation of the BV Access Program, Axios International conducted an anonymized retrospective analysis of patients enrolled in the program in 2019–2020 in the seven LMICs where the program was implemented: Egypt, Malaysia, Mexico, Peru, Philippines, Thailand and Ukraine. Patients enrolled in the program were newly treated with BV. The manufacturer of this product had no role in the study conception and design, analyses or drafting of the manuscript.
Study population
Patients at least 18 years of age who had a physician confirmed prescription for BV and accepted the inclusion criteria for the BV Access Program implemented by Axios International were eligible for program participation. Patients participating in the program received medication and healthcare at multiple public and private hospitals in different cities throughout the seven countries included in this study.
Data collection
An Axios Program manager collected patient data at the time of entry into the BV Access Program and throughout patient treatment and follow-up of patient. All information from patient files was extracted anonymously from medical program reports, no information was collected directly from patients.
Collected data were evaluated in the context of three primary end point outcomes: treatment completed (i.e., patient completed all scheduled injections), treatment stopped by physician (i.e., due to major AEs, lack of clinical response or therapeutic escape/disease progression) or patient death.
Data collected in program reports were sex, age, hospital status where the patient was treated (public vs private) and number and type (phone, email and both) of program manager–patient contacts throughout the entire follow-up. Treatment-related AEs were also collected, and AEs and primary outcome were confirmed by the physician. The number of patients followed by the physician was also collected.
Statistical analyses
Descriptive statistics were computed for the characteristics of patients included in the program and are calculated as mean and standard deviation (SD), median (M) and interquartile range for quantitative variables, and as percentage for qualitative variables. Chi-square test was used for qualitative data comparisons and Student t-test was used for quantitative comparisons.
The Kaplan–Meier method was used to obtain the probabilities of overall survival as well as treatment stopped by physician decision. Kaplan–Meir curves were plotted for the patients included in the seven countries in aggregate and analyzed per country. Statistical differences among the countries were tested using stratified log-rank tests.
Two multivariate Cox proportional-hazard models were fitted to identify predictive factors of survival and treatment stopped by physician, and the models were stratified by country. All variables tested in univariate analysis were included in the Cox models. Hazard-ratios (HR) and 95% CI were calculated for each variable. For all analyses, a significance level for ≤0.05 was used. Statistical analyses were performed using Excel Stat (Addinsoft).
Results
Patient demographics
Baseline characteristics for the 460 patients included in the study are summarized in Table 1. The majority of patients (73.1%) received care at a public hospital and at least one AE was reported in 276 patients (60.0%). The mean number of patients followed by each physician in the study was 5.6 (SD = 7.8) and overall mean treatment duration was 9.3 months (SD = 4.8). Patient outcomes and mean treatment duration by outcome category are also shown in Table 1.
| n (%) of patients or mean value (SD, IQR) | |
|---|---|
| Sex-ratio M:F | 1.02 |
| Mean age | 38.6 (12.9; 25.3–37.9) |
| Patients included by country (n) | |
| Egypt | 66 (14.3) |
| Mexico | 96 (20.9) |
| Malaysia | 65 (14.1) |
| Peru | 27 (5.9) |
| Philippines | 86 (18.7) |
| Thailand | 32 (7.0) |
| Ukraine | 88 (19.1) |
| Patient outcome | |
| Treatment completed | 223 (48.5) |
| Treatment stopped (by MD decision) | 122 (26.5) |
| Death | 115 (25.0) |
| Hospital status | |
| Public | 247 (73.1) |
| Private | 91 (26.9) |
| Mean treatment duration in patients with (in months) | |
| Treatment completed | 12.4 (2.7; 10.7–13.5) |
| Treatment stopped (by MD decision) | 7.7 (4.1; 4.2–10.4) |
| Death | 4.9 (4.3, 1.4–7.4) |
| Mean number of follow-up contacts per month by | |
| Phone | 2.1 (3.7; 0.3–2.1) |
| 1.8 (4.8; 0.09–1.7) | |
| Phone and email | 4.0 (7.6; 0.8–4.3) |
| Mean number of adverse events per month | 0.32 (0.73; 0.01–0.39) |
| At least one adverse event | 276 (60.0) |
| Mean number of patients followed by MD | 5.6 (7.8; 1.0–6.0) |
IQR: Interquartile range; MD: Medical doctor; SD: Standard deviation.
Of the 460 patients included in this analysis, 447 patients (97.1%) were treated for a HL (relapsed or refractory, CD30+, following autologous stem cell transplant), nine patients (2.0%) were treated for anaplastic large cell lymphoma and four patients (0.9%) were treated for T cell cutaneous lymphoma.
Patient outcomes
Patient characteristics (country, hospital status, mean number and type of follow-up contacts, AEs and mean number of patients followed by the physician) for each outcome category (completed treatment, treatment stopped by physician and patient death) are summarized in Table 2. Overall, 223 patients (48.5%) completed treatment, 122 (26.5%) stopped treatment due to physician decision and 115 (25.0%) died. The proportion of the 122 patients who stopped treatment and 115 who died based on the country in which they were treated is shown in Table 2. The proportion of who died as a total of patients treated in each country was: Egypt, 36.4%; Malaysia, 21.5%; Mexico, 14.6%; Peru, 25.9%; Philippines, 31.4%; Thailand, 18.7% and Ukraine, 26.1%. The proportion of patients from each country who stopped treatment due to physician decision was: Egypt, 30.3%; Malaysia, 21.5%; Mexico, 37.5%; Peru, 29.6%; Philippines, 14.0%; Thailand, 31.2% and Ukraine 25.0%.
| Patients with treatment completed (n = 223) | Patients who died (n = 115) | p-value† | Patients with treatment stopped by MD (n = 122) | p-value‡ | |
|---|---|---|---|---|---|
| Sex ratio M:F | 1.33 | 1.0 | 0.29 | 1.32 | 0.22 |
| Mean age (SD, IQR) | 31.8 (10.9; 22.5–33.7) | 37.1 (14.5; 27.8–36.7) | 0.001 | 34.5 (14.2; 25.7–37.8) | 0.001 |
| By country (%) | |||||
| Egypt | 9.9 | 20.9 | 16.4 | ||
| Malaysia | 16.7 | 12.2 | 11.5 | ||
| Mexico | 20.6 | 12.1 | 29.5 | ||
| Peru | 5.4 | 6.1 | 0.07 | 6.6 | 0.04 |
| Philippines | 21.1 | 23.5 | 9.8 | ||
| Thailand | 7.2 | 5.2 | 8.2 | ||
| Ukraine | 19.3 | 20.0 | 18.0 | ||
| Hospital status (%) | |||||
| Public | 74.0 | 71.3 | 0.60 | 79.7 | 0.28 |
| Private | 26.0 | 28.7 | 20.3 | ||
| Mean number of follow-up contacts per month (SD, IQR) | |||||
| Phone | 1.8 (5.8; 0.5–4.3) | 3.9 (5.8; 0.6–4.7) | 0.0001 | 3.1 (3.7; 0.7–4.5) | <10-4 |
| Mails | 0.9 (1.0; 0.1–1.7) | 4.0 (6.7; 0.6–4.5) | <10-4 | 2.6 (5.5; 0.3–3.1) | <10-4 |
| Phone and mails | 2.8 (2.4; 0.7–4.6) | 8.1 (11.6; 1.7–9.4) | <10-4 | 5.6 (7.5; 1.0–7.0) | <10-4 |
| Mean number of adverse events per month (SD, IQR) | 0.07 (0.15; 0–0.09) | 0.83 (1.2; 0.19–1.1) | <10-4 | 0.26 (0.33; 0–0.32) | <10-4 |
| At least one adverse event (%) | 42.2 | 89.6 | <10-4 | 72.8 | <10-4 |
| Mean number of patients followed by MD | 6.2 (8.0; 1.0–6.0) | 5.1 (7.2; 1.0–5.0) | 0.01 | 2.3 (1.6;1.0–3.0) | <10-4 |
†
p values for the comparisons between patients with treatment completed and patients who died.
‡
p values for the comparisons between patients with treatment completed and patients with treatment stopped by MD.
MD: Medical doctor.
The probability of survival by Kaplan–Meier analysis for all 460 patients and by country is plotted in Figure 1. Survival probability for all 460 patients was 75.0% at 6 months and 63.7% at 12 months (Figure 1A). When stratified by country, survival probability at 12 months ranged from 44.5% (Egypt) to 78.3% (Mexico) (p = 0.09) (Figure 1B).
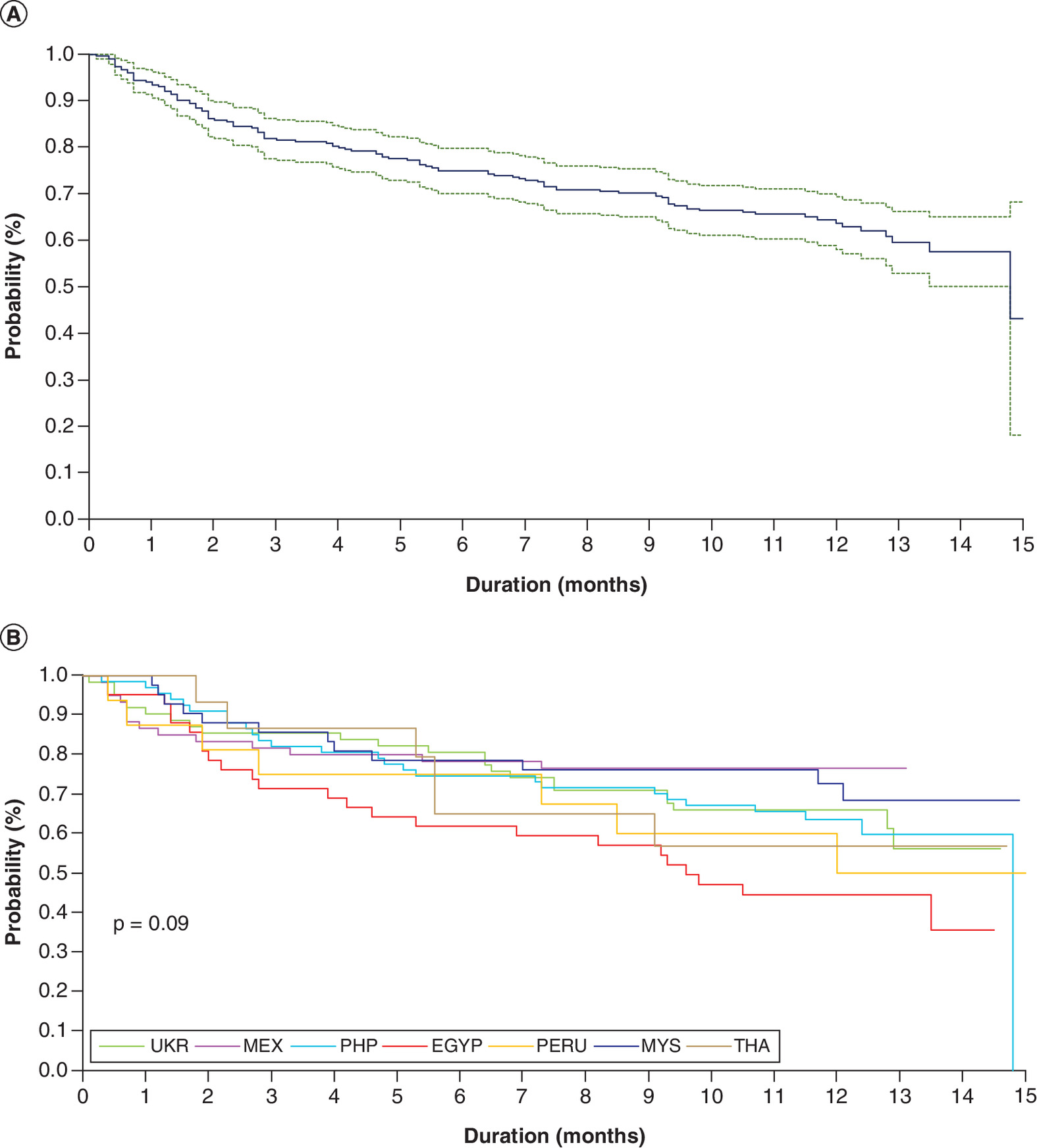
Figure 1. Kaplan–Meier analysis of survival among patient with Hodgkin's lymphoma in seven low- and middle-income countries 2019 (n = 460).
(A) Overall probability of survival in the seven countries. (B) Probability of survival by country.
EGYP: Egypt; MEX: Mexico; MYS: Malaysia; PHP: Phillipines; THA: Thailand; UKR: Ukraine.
The probability of the physician deciding to stop treatment for all 460 patients and by country is shown in Figure 2. The probability to continue the treatment was 86.4% at 6 months and 68.4% at 12 months (Figure 2A). When stratified by country, the probability at 12 months ranged from 49.9% (Mexico) to 81.3% (Thailand) (p = 0.003) (Figure 2B).
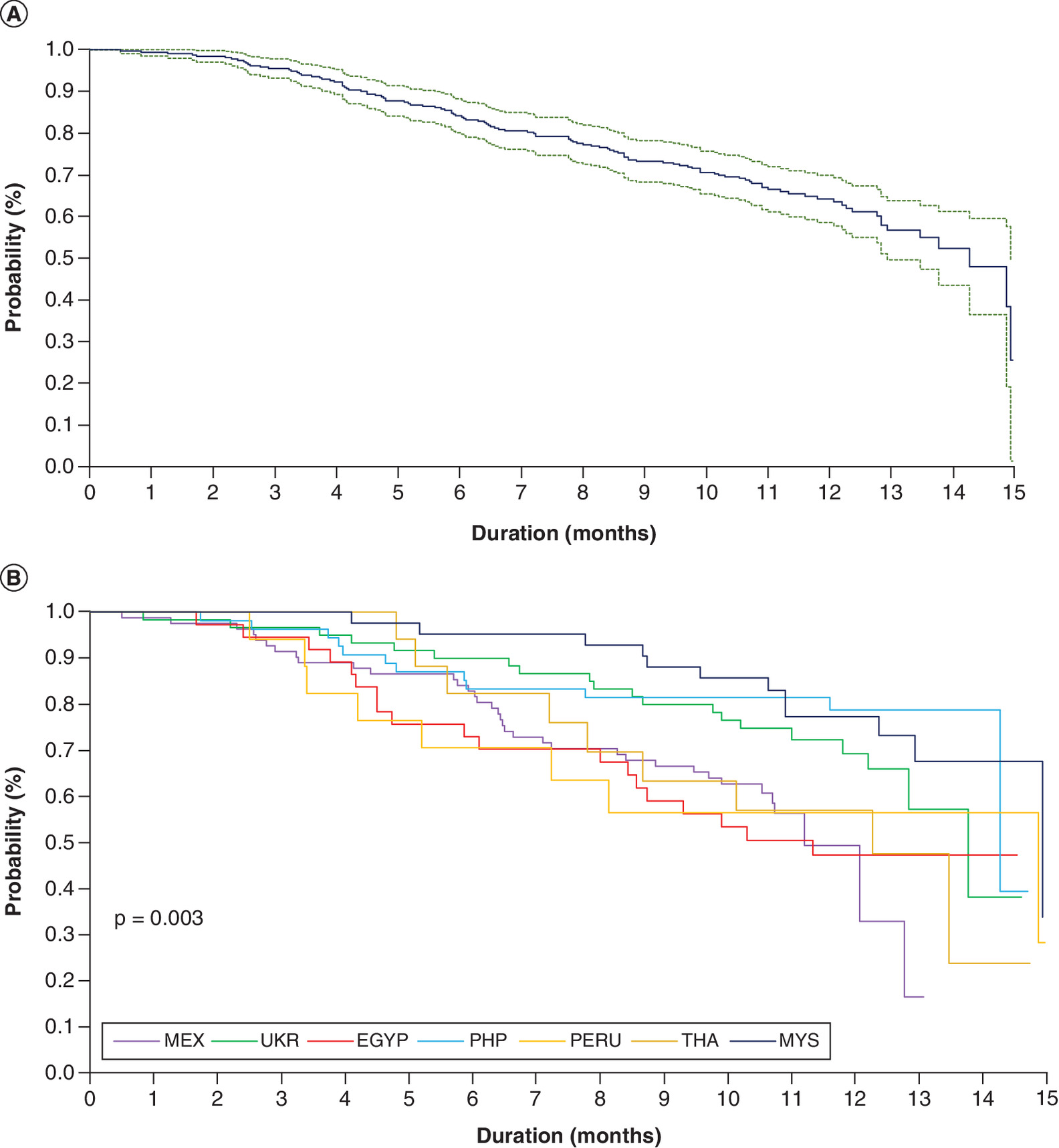
Figure 2. Kaplan–Meier analysis of treatment stopped by medical doctor among patient with Hodgkin’s lymphoma in seven low- and middle-income countries 2019 (n = 460).
(A) Overall probability of treatment stopped in the seven countries. (B) Probability of survival by country.
EGYP: Egypt; MEX: Mexico; MYS: Malaysia; PHP: Phillipines; THA: Thailand; UKR: Ukraine.
Independent predictive factors
Multivariate Cox proportional models were fitted to identify predictive factors associated with mortality (Model 1) and with physician decision to stop treatment (Model 2), and the results are summarized in Table 3. Mortality was significantly associated with number of AEs (HR: 16.43; 95% CI: 9.16–26.71; p < 10-4), number of contacts by email and phone (respectively, HR: 1.48; 95% CI: 1.35–1.63; p < 104; HR: 0.89, 95% CI: 0.40–0.95; p = 0.009) and number of patients followed by the physician (HR: 0.88; 95% CI: 0.67–0.98; p = 0.001). Physician decision to stop the treatment was associated with number of AEs (HR: 3.82, 95% CI: 1.95–6.48; p < 10-4), number of email and phone contacts (respectively, HR: 1.35; 95% CI: 1.20–1.53; p < 10-4; HR: 1.26; 95% CI: 1.16–1.34; p < 10-4) and mean number of patients followed by physician (HR: 0.94; 95% CI: 0.87–0.97; p = 0.02).
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-value | HR | 95% CI | p-value | |
| Age | 1.02 | 1.01–1.04 | 0.02 | 1.02 | 1.01–1.04 | 0.009 |
| Sex | ||||||
| Male | 1.0 | – | – | 1.0 | – | – |
| Female | 0.79 | 0.50–1.26 | 0.32 | 0.76 | 0.50–1.14 | 0.18 |
| Hospital status | ||||||
| Public | 1.0 | – | – | 1.0 | – | – |
| Private | 1.43 | 0.73–2.82 | 0.30 | 0.63 | 0.31–0.94 | 0.03 |
| Contacts per month by phone (n) | 0.89 | 0.49–0.95 | 0.009 | 1.26 | 1.16–1.34 | <10-4 |
| Contacts per month by mail (n) | 1.48 | 1.35–1.63 | <10-4 | 1.35 | 1.20–1.53 | <10-4 |
| Adverse events per month (n) | 16.43 | 9.16–26.71 | <10-4 | 3.82 | 1.95–6.48 | <10-4 |
| Patients followed by MD (n) | 0.88 | 0.67–0.98 | 0.001 | 0.94 | 0.87–0.97 | 0.02 |
†
Stratified on the countries.
MD: Medical doctor.
Discussion
This longitudinal study found that the number of AEs was the greatest risk factor for death and for physician decision to stop treatment. More interestingly, this study also found that patient support provided by phone, but not email contacts, had a protective effect on survival and that the number of patients followed by the physician had a positive impact on both survival and remaining on BV therapy.
The finding that phone-based patient support provided a protective effect on survival adds to a growing body of evidence demonstrating the benefits of phone-based support programs. A study comparing the impact of community nurse phone-based health mentoring versus general practice care and non interventional brief telephone calls (UC) on 1207 patients with chronic obstructive pulmonary disease (COPD) across 31 general practitioners in Tasmania found that health mentoring increased self-management capacity and knowledge compared with UC [19]. The Tasmania study also found that telephone-based counselling resulted in greater changes in lifestyle modification compared with email counselling. Evaluation of a telephone-based chronic disease management program using claims data from participants in employer self-insured health plans in the USA found that participation in the program was associated with average annual savings of $1,157.91 in healthcare expenditures per member enrolled, and that savings increased with the length of participation in the program [20]. A systematic review including 30 studies and describing the results of telephone-based coaching services in patients with chronic diseases found such programs could improve health behavior, self-efficacy and health status [21]. Notably, this study also found that these improvements were especially true in vulnerable populations who had difficulty accessing health services. These studies and our findings regarding the positive effect of telephone-based support suggest that this mode of interacting with patients has the potential to improve multiple aspects of care for patients with chronic diseases. Patients receiving a BV regimen may have similarities to patients undergoing treatment for non oncologic chronic diseases. As cancer therapy evolves to include long-term maintenance regimens that allow cancer to be managed as a chronic disease, phone-based support may have a growing role to play in improving patients disease self-management abilities and health outcomes.
Our study found that phone-based patient support provided during treatment significantly reduced mortality by 11%. Focus groups and interviews with lymphoma survivors found that these patients desired additional support once their treatment had successfully been completed [22]. Key concerns identified include better access to information that could be shared with general practitioners, receiving a list of services and information regarding treatment expectations, feelings of loss related to treatment side effects, fear of recurrence, support in transitioning back to pretreatment activities and relationships, a desire for patient-centric post-treatment care and ongoing social services to address unmet psychosocial and practical needs [22]. Our findings suggest that providing continued phone-based support to patients in the treatment access program once they have completed treatment could provide benefits. Additional studies exploring post-treatment support would be warranted to determine how different modes of support might improve treatment outcomes.
Another interesting aspect to consider is the potential impact of patient support provided through the BV Access Program on patients ability to self-management AEs and other aspects of their treatment. We have previously shown that patient's understanding of disease, their involvement in treatment decisions, age, time spent with physician and fear of how patients were perceived by others were the most predictive factors associated with a high ability to self-manage a chronic disease, and that socio-cultural factors have an indirect impact on disease self-management [23]. In our current study, AEs were the biggest predictor of death or physician decision to stop treatment. Although our study did not evaluate which aspects of phone-based support might account for the protective effect of this support on survival, support for managing complications and AEs is one of its components. Several reviews have found evidence that self-management strategies can improve knowledge, symptom management, self-management behaviors, pain, disability, fatigue, depression and health distress [24,25]. Another assessment supports the need for self-management strategies to be tailored to the needs of each patient [26]. The phone-based support component of the treatment access program also provides a forum in which patients can share their specific needs and concerns, and could potentially reduce patients’ treatment burden by limiting out-of-pocket travel expenses, loss of income and co-pays associated with in-person visits with a care provider. Further evaluation of the effect of this support on AEs would provide additional insight into the mechanism by which phone contact could elicit a positive effect.
The interaction of AEs with number of patients seen by the physician may also warrant further explanation. In our current study, increased number of patients seen by the physician had a positive effect on risk of death as well as physician decision to stop treatment. This finding contrasts with a previous cohort study evaluating medication adherence among patients in Egypt with COPD, which found no association between number of patients attended by the physician and the probability of the physician deciding to discontinue COPD therapy [27]. In contrast to long-standing COPD therapy, BV was initially approved in 2011. Consequently, physicians have had less time to gain substantial experience in managing patients treated with BV, including managing AEs. Physicians in our current study who see more patients could potentially have more experience with HL, which could impact their willingness to continue patients on therapy when AEs or complications arise. A study in patients with B-cell non-Hodgkin’s lymphoma found that lower oncologist experience with rituximab was associated with an increased risk of rituximab discontinuation [8]. Other studies have also found that physician experience with HIV/AIDS or tuberculosis had a positive effect on survival [28,29]. Survival outcomes in patients with lymphoma treated by rural community-based providers had a higher risk of death than those treated by university-based providers [25], the latter of which would be expected to have more experience and be more familiar with the latest treatment advances. Further studies are needed to understand the mechanism of these findings more fully, and to leverage this understanding for improved patient outcomes.
In addition to experience, other physician related factors may also contribute to physician decision to continue or discontinue cancer therapy. For example, physicians whose patients experience AEs reported stress, anxiety, sleep disturbance and lower professional confidence [27]. The impact of these stressors on physicians could potentially play a role in their decision to discontinue treatment in patients with a greater number of AEs, as observed in the current study. Additionally, physicians treating patients with melanoma or lung cancer have reported a preference for prescribing cancer therapies that offer less variability in survival outcome, even if those therapies provide a reduced likelihood of ‘tail-of-the-curve’ overall survival [30]. Here again, this preference could potentially impact physician decision to discontinue treatment, especially in patients with a greater number of AEs who may require more variable management. Understanding the factors that lead physicians to discontinue cancer therapy will also be important for improving patient outcomes and their quality of life.
This study has strengths, including its longitudinal design, lack of missing data, inclusion of patients in seven LMICs worldwide, robust outcomes measures (death and treatment stopped), and no patient attrition during follow-up. First, limitations of this study include the lack of clinical data related to disease severity, stage of cancer and comorbidities that could have impacted treatment outcomes as well as survival. However, the binary categorization of outcomes (treatment stopped or death) would be expected to reduce the risk of information bias. Second, due to small sample size as well as statistical lack of power, a country-by-country comparison could not be conducted. Thirdly, a total of 3.7% of patients not contact by email. While this could create a potential selection bias, the number of patients without email contact remained very low and did not vary significantly among countries. Despite these limitations, this study provides important insights into factors that impact survival, and physician decision to stop treatment for lymphoma patients. The results of this study provide a foundation for future investigation into factors that may improve outcomes for these patients in LMICs.
Conclusion
A drug access program that addresses patients’ financial needs and provides patient support during cancer therapy can improve the likelihood of survival. Phone-based support and the number of patients seen by the physician provided the greatest positive effect, while the number of AEs remains a critical predictor of death and physician decision to stop treatment. Further studies of mechanisms by which these factors impact patient outcomes should help to identify specific items that can be enhanced or avoided to further improve outcomes for lymphoma patients undergoing therapy.
Findings from this study may also be useful in developing additional access programs for other cancer as well chronic diseases therapies in LMICs. This is important because increasing access to and the effectiveness of cancer care in LMIC's is of increasing priority, as evidenced by the recent inclusion of cancer medications on the WHO’s Essential Medicines List [31]. A recent study of an electronic patient symptom management program conducted during the COVID-19 pandemic demonstrated that the program was feasible and that the self-management instructions and provider phone calls that the program provided resolved or decreased the severity of cancer-related symptoms [32]. In light of the ongoing COVID-19 pandemic, which poses a greater risk of mortality and severe COVID-19 disease as well as long COVID syndrome to patients with cancer due age, comorbidities and immunosuppression related to cancer and cancer therapy the potential benefit of phone-based programs to support these patients should be explored in the near term.
•
While a large panel of factors associated with mortality and physician decision to stop treatment have been identified, the impact of patient targeted communication during treatment on outcomes for patients with cancer in low- and middle-income countries has not been well investigated.
•
The objective of this study was to identify predictive factors associated with overall survival and physician decision to discontinue the treatment of Hodgkin’s lymphoma, especially the potential effect of communication interventions, among cancer patients undergoing therapy in seven low- and middle-income countries.
•
This longitudinal study found that the number of adverse events was the greatest risk factor for death and for physician decision to stop treatment. This study found that patient support provided by phone, but not email contacts, had a protective effect on survival and that the number of patients followed by the physician presented also a positive impact on both survival and remaining on treatment.
•
Findings from this study may also be useful in developing additional access programs for other cancer as well chronic diseases therapies in low- and middle-income countries.
Author contributions
Conceived and designed the experiments: J Ladner, F Madi, R Jayasundera and J Saba. Performed the experiments: F Madi, R Jayasundera and J Saba. Analyzed the data: J Ladner, J Saba and E Audureau. Contributed reagents/materials/analysis tools: J Ladner, F Madi, R Jayasundera, J Saba and E Audureau. Wrote the paper: J Ladner, F Madi, R Jayasundera, J Saba and E Audureau. All authors had intellectual input into the concepts explored, critically reviewed each draft of the full manuscript and approved the final version.
Acknowledgments
The authors would like to thank all physicians and patients who participated in the study. Special thanks to S Seiler for editing and revision of the manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Medical writing support was received for the creation of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. Patients provided written informed consent to enroll in the BV Access Program.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 68, 394–424 (2018).
2.
Shin-ichi N. Epidemiology and pathologic features of Hodgkin lymphoma. Int. J. Hematol. 83(5), 391–397 (2006).
3.
Zhou L, Deng Y, Li N et al. Global, regional, and national burden of Hodgkin lymphoma from 1990 to 2017: estimates from the 2017 Global Burden of Disease study. J. Hem. Onc. 12, 107 (2019).
4.
Keykhaei M, Masinaei M, Mohadmmadi E et al. A global, regional, and national survey on burden and Quality of Care Index (QCI) of hematologic malignancies; global burden of disease systematic analysis 1990-2017. Exp. Hematol. Oncol. 10, 11 (2021).
5.
Cortes J, Perez-Garcia JM, Llombart-Cussac A et al. Enhancing global access to cancer medicines. CA Cancer J. Clin. 70, 105–124 (2020).
6.
Scott JS. Brentuximab vedotin: a review in CD30-positive Hodgkin lymphoma. Drugs 77, 435–445 (2017).
7.
Strauss DJ, Dlugosz-Danecka M, Connoer JM et al. Brentuximab vedotin with chemotherapy for patients with previously untreated stage III/IV classical Hodgkin lymphoma: 5-year updated of the ECHELON-1 study. Blood 136(Suppl. 1), 26–28 (2020).
8.
Huntington SF, Hoag JR, Wang R et al. Physician experience and risk of rituximab discontinuation in older adults with non-Hodgkin's lymphoma. J. Natl Compr. Canc. Netw. 17(10), 1194–1202 (2019).
9.
Loberiza FR, Cannon AJ, Weisenburger DD et al. Survival disparities in patients with lymphoma according to place of residence and treatment provider: a population-based study. J. Clin. Oncol. 27, 5376–5382 (2009).
10.
Velasco R, Domingo-Domenech E, Sured A. Brentuximab-induced peripheral neurotoxicity: a multidisciplinary approach to manage an emerging challenge in Hodgkin lymphoma therapy. Cancers 13, 6125 (2021).
11.
Atieno OM, Opanga S, Martin A, Kurdi A, Godman B. Pilot study assessing the direct medical cost of treating patients with cancer in Kenya; findings and implications for the future. J. Med. Econ. 21(9), 878–887 (2018).
12.
Al-Ziftawi NH, Shafie AA, Ibrahim MIM. Cost-effectiveness analyses of breast cancer medications use in developing countries: a systematic review. Expert Rev. Pharmacoecon. Outcomes Res. 21(4), 655–666 (2021).
13.
Gershon N, Berchenko Y, Hall PS, Goldstein DA. Cost effectiveness and affordability of trastuzumab in sub-Saharan Africa for early stage HER2-positive breast cancer. Cost Eff. Resour. Alloc. 17, 5 (2019).
14.
Godman B, Hill A, Simoens S et al. Potential approaches for the pricing of cancer medicines across Europe to enhance the sustainability of healthcare systems and the implications. Expert Rev. Pharmacoecon. Outcomes Res. 21(4), 527–540 (2021).
15.
Coquet J, Blayney DW, Brooks JD, Hernandez-Boussard T. Association between patient-initiated emails and overall 2-year survival in cancer patients undergoing chemotherapy: evidence from the real-world setting. Cancer Med. 9, 8552–8561 (2020).
• Of interest.
16.
Rochette C, Michallet AS, Malartre-Sapienza S, Rodier S. Telephone follow-up of oncology patients: the contribution of the nurse specialist for a Service-Dominant Logic in hospital. BMC Health Services Res. 21, 580 (2021).
• Of interest.
17.
Yajima C, Bowe C, Barber D, Dains J. Telehealth interventions for supportive management and early recognition of treatment-related symptoms in patients with hematologic malignancies. J. Adv. Pract. Oncol. 12(8), 835–849 (2021).
• Of interest.
18.
Saba J, Audureau E, Bize M, Koloshuk B, Ladner J. Development and validation of a multilateral index to determine economic status in developing countries: the Patient Financial Eligibility Tool (PFET). Popul. Health Manag. 16(2), 82–89 (2013).
19.
Walters J, Cameron-Tucker H, Wills K et al. Effects of telephone community-recruited chronic obstructive pulmonary disease on self-management capacity, quality of life and psychological morbidity: a randomised controlled trial. BMJ Open 3, e003097 (2013).
• Of interest.
20.
Avery G, Cook D, Talens S. The impact of a telephone-based chronic disease management program on medical expenditures. Popul. Health Manag. 19(3), 156–162 (2016).
21.
Dennis SM, Harris M, Lloyd J et al. Do people with existing chronic conditions benefit from telephone coaching? A rapid review. Aust. Health Rev. 37(3), 381–388 (2013).
• Of interest.
22.
Monterosso L, Taylor K, Platt V et al. A qualitative study of the post-treatment experiences and support needs of survivors of lymphoma. Eur. J. Oncol. Nurs. 28, 62–68 (2017).
23.
Ladner J, Alshurafa S, Madi F et al. Factors impacting self-management ability in patients with chronic diseases in the United Arab Emirates, 2019. J. Comp. Eff. Res. 11(3), 179–192 (2022).
• Of interest.
24.
Franek J. Self-management support interventions for persons with chronic disease: an evidence-based analysis. Ont. Health Technol. Assess. Ser. 13(9), 1–60 (2013).
25.
Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ. Counsel. 48, 177–187 (2002).
• Of interest.
26.
Trappenburg J, Jaarsma T, van Os-Medendorp H, Kort H, Hoes A, Schuurmans M. Self-management: one size does not fit all. Patient Educ. Counsel. 92, 134–137 (2013).
27.
Ladner J, El Badrawy M, Nofal A, Saba J, Audureau E. A cohort study of medication adherence among patients with chronic obstructive pulmonary disease in Egypt. NPJ Prim. Care Respir. Med. 30, 31 (2020).
28.
Kitahata MM, Koepsell TD, Deyo RA, Maxewell CL, Dodge WT, Wagner EH. Physicians' experience with the acquired immunodeficiency syndrome as a factor in patients' survival. N. Engl. J. Med. 334, 701–706 (1996).
29.
Kamran K, Campbell A, Wallington T, Gardam M. The impact of physician training and experience on the survival of patients with active tuberculosis. Can. Med. Assoc. J. 175(7), 749–753 (2006).
30.
Shafrin J, Schwart TT, Okoro T, Romley JA. Patient versus physician evaluation of durable survival gains: implications for value framework assessments. Value Health 20, 217–223 (2017).
31.
World Health Organization Model List of Essential Medicines – 22nd List, 2021. World Health Organization, Switzerland (2021). https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2021.02
32.
Wujcik D, Dudley WN, Dudley M, Gupta V, Brant J. Electronic patient symptom management program to support patients receiving cancer treatment at home during the COVID-19 pandemic. Value Health 25(6), 931–936 (2022).
• Of interest.
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 December 2022
Accepted: 22 May 2023
Published online: 6 June 2023
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Phone contacts and treatment discontinuation predict survival cancer patients in a subsidized drug access program. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2022-0210
Export citation
Select the citation format you wish to export for this article or chapter.