Evaluation of hypercholesterolemia management in at-risk patients by cardiologists in France: a case vignette-based study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This online interactive survey investigated lipid-lowering approaches of French cardiologists in high- and very high-cardiovascular risk patients with hypercholesterolemia. Materials & methods: Physicians assessed three hypothetical patients at three clinic visits, and selected the patients’ cardiovascular risk category, target low-density lipoprotein cholesterol (LDL-C) and treatment. Results: A total of 162 physicians completed 480 risk assessments; 58% of assessments correctly categorized the hypothetical patients. Most physicians chose the correct LDL-C target for one of the very high-risk patients, but higher-than-recommended targets were selected for the other very high-risk patient and the high-risk patient. Statins were the most commonly chosen treatment. Conclusion: French cardiologists often underestimate cardiovascular risk in patients with hypercholesterolemia, select a higher-than-recommended LDL-C target and prescribe less intensive treatment than that recommended by guidelines.
Tweetable abstract
Based on case vignette analysis, French cardiologists underestimate cardiovascular risk in patients with hypercholesterolemia, resulting in suboptimal treatment #hypercholesterolemia #LDL-C target #lipid-lowering therapy
Graphical abstract
Plain language summary
What is this article about?
Cardiovascular disease is the main cause of death in Europe. High blood cholesterol (or hypercholesterolemia) is one of the major risk factors for cardiovascular disease, but it can be controlled by proper treatment. Studies have shown that patients in France with hypercholesterolemia generally receive suboptimal treatment.
What were the results?
We surveyed 162 French cardiologists to understand their approach to lowering of low-density lipoprotein cholesterol (LDL-C) levels. Using an online interactive survey, the physicians communicated with three virtual patients presenting hypothetical clinical scenarios. We found that many of the French cardiologists incorrectly judged the cardiovascular risk in patients with hypercholesterolemia, lacked knowledge about the correct LDL-C targets, and prescribed less intensive treatment than that recommended by guidelines.
What do the results of the study mean?
In order to decrease the proportion of patients receiving suboptimal treatment, continued physician education in assessing cardiovascular risk and increasing familiarity with correct LDL-C targets are required.
Cardiovascular (CV) disease is the leading cause of death in Europe [1]. While the age-standardized rate of CV mortality is lower in France than in many other European countries [2], CV disease is still a significant cause of morbidity, incurring healthcare costs of at least €15 billion per year [3].
One of the major modifiable risk factors for CV disease is hypercholesterolemia [4]. The magnitude of the CV risk correlates with the cumulative time that low-density lipoprotein cholesterol (LDL-C) remains above guideline recommended target levels [5].
The nationwide Esteban study showed that, based on the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) 2019 guidelines [6], approximately 72% of French adults required specific care (e.g., lifestyle measures, lipid-lowering drugs) for hypercholesterolemia [7]. The ESC/EAS 2019 hypercholesterolemia guidelines recommend that the use of lipid-lowering therapy be guided by the patient's overall CV risk, with more stringent LDL-C targets (and therefore more intensive therapy) prescribed for those with higher CV risk [6]. Using these definitions, more than 96% of French patients in the high- or very high-risk categories should be receiving lipid-lowering therapy [7].
Data from the Esteban study [8] and studies in specific patient groups, including those with familial hypercholesterolemia [9–11], individuals with pre-existing CV disease [11,12] and people living with HIV/AIDS and diabetes [13], indicate that patients in France with hypercholesterolemia generally receive suboptimal treatment in terms of achieving LDL-C targets. There may be a number of reasons for these findings, including low physician awareness of goals and guidelines, therapeutic inertia or reluctance to prescribe lipid-lowering therapies to target LDL-C levels or poor patient adherence [14,15].
While analyses of prescribing patterns can evaluate the extent of suboptimal treatment, they provide little insight into individual physicians’ clinical decision making processes. Therefore, we designed an online interactive survey of hypercholesterolemia treatment decisions using hypothetical patient case vignettes. The aim of the study was to investigate the approaches to hypercholesterolemia management in high- and very high-CV risk patients by French cardiologists, examining patient CV risk categorization, the LDL-C targets chosen and the therapeutic strategies they would employ.
Materials & methods
The study was based on the presentation to physicians of fictitious, formatted and randomized clinical cases, simulating real-life conditions and associated with questionnaires on therapeutic decisions. The study was overseen by a Scientific Committee of eight French specialists (three endocrinologists, four cardiologists and one internal medicine specialist). The online survey of physician practices was conducted between April and September 2021, using three hypothetical case vignettes of patients with hypercholesterolemia who were at high or very high CV risk.
Survey participants consented to answer the questions at the time of recruitment by phone or email, and signed a document outlining their agreement and rights. As the study did not involve active therapeutic interventions in real patients, no ethical approval was needed; however, all research was conducted according to the principles of the Declaration of Helsinki.
Case vignette methodology
The Scientific Committee determined the following parameters of the patients included in the vignettes: sex (male or female); age (55–60 years or 61–66 years); history of Type 2 diabetes (yes or no); LDL-C level (markedly elevated or moderately elevated); and the presence of myalgia from visit 2 (yes or no). To develop the case vignettes, the Scientific Committee combined the randomly generated information with other plausible clinical information, including sociodemographic details (specific age, profession); clinical examination features/relevant medical history; laboratory test results; and concomitant medications taken by the patient at baseline. Thirty-two simulations of clinical cases were constituted from a random and coherent combination of these different parameters.
This methodology makes it possible to study the impact of clinical, biological or socio-demographic parameters (related to the patient) on the diagnostic and/or therapeutic management of the patients [16]. Because of its great effectiveness in evaluating the diagnostic and therapeutic practices of physicians and the follow-up of the corresponding recommendations, this methodology seems to be the most adapted to meet the objectives of this study.
The randomly defined case vignettes were applied to three clinical scenarios: Case 1 – a high-risk primary prevention patient with moderate chronic kidney disease (CKD); Case 2 – a secondary prevention patient with a recent acute coronary syndrome (ACS); and Case 3 – a secondary prevention patient with symptomatic peripheral arterial disease (PAD). In the survey, physicians received three cases (one from each clinical scenario), with the case characteristics randomly chosen from the 32 possible case vignettes (Supplementary Figure 1).
Online survey
An online survey was developed in the form of an interactive game. The three clinical cases were presented to the physicians in the form of chatbots, allowing the physician to communicate with the virtual patient through a conversational interface. Physicians completed questionnaires on their proposed management of each case at three visits. Visit 1 was the initial consultation (Cases 1 and 3) or the first follow-up visit after hospitalization for ACS (Case 2). Visits 2 and 3 were the first and second follow-up visits, at which target LDL-C level may or may not have been attained. The Scientific Committee chose treatment strategies based on the ESC guidelines for each scenario at each visit.
During visit 1, the physicians were asked to define the CV risk category of all three patients as low, medium, high or very high, although all three case vignettes were in the high-risk (Case 1: primary prevention with moderate CKD) or very high-risk category (Case 2: recent ACS and Case 3: symptomatic PAD) according the EAS/ESC guidelines [6]. The physicians were then asked to assign the patient an appropriate LDL-C target: <1.4 mmol/l (<0.55 g/l), <1.8 mmol/l (<0.7 g/l), <2.6 mmol/l (<1.0 g/l), <3.0 mmol/l (<1.15 g/l) or <3.4 mmol/l (<1.3 g/l), based on their risk assessment. Physicians were asked to reassess CV risk category and LDL-C target again at visit 2 only for Case 1 (primary prevention with moderate CKD), considering the result of the coronary artery calcification (CAC) score assessment.
At each point during the patient’s hypothetical management, physicians were asked to select the answers they considered to be the most appropriate and which allowed the best management of the patient. Multiple options could be chosen from the following proposed treatments: lifestyle/dietary measures; a statin; cholestyramine; a fibrate; ezetimibe; and/or a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor. Irrespective of the treatment chosen by the physician at visits 1 and 2, the scenario presented to them at the beginning of visits 2 and 3, respectively, included the fixed treatment chosen by the Scientific Committee (Supplementary Figures 1A–C).
The physicians’ responses were recorded directly on a remote server. The estimated duration of the game was 25 min on average for physicians to complete all three scenarios. In addition to the case vignettes, physicians completed a short survey about their own socio-demographics (age, sex and place of practice).
Physician participants
Physicians were eligible to participate if they were registered specialist cardiologists in private practice or mixed private/public practice in France (no limits by age or number of years in practice). Overall, 400 eligible physicians were invited to participate, with geographical distribution of participants matching the geographical distribution of cardiologists throughout France. This was achieved by developing a regional quota based on the geographical distribution of the 7100 cardiologists in France. First, a sample of 300 physicians was randomly drawn from the list of 7100 cardiologists, classified by region and compared with a list of 1850 cardiologists in private or mixed practice. Eligible cardiologists from this sample were invited to participate. Once the regional quota was filled, no further physicians from that region were invited. If additional participants were required, then more physicians were selected randomly from the remaining physicians on the list of 1850 in private/mixed practice, and invitations were sent to these physicians until the regional quotas were filled.
Physicians were each sent a link, with an identifier and a password, to the online questionnaire. The initial home page provided information on the modalities and general objective of the study. Case vignettes were presented in the same sequence (Case 1, followed by Cases 2 and 3) for each physician. Once the data for a given case vignette were entered and validated, the response fields were automatically frozen and the physician was not able to modify their answers on the previously validated case vignettes. Each physician could only complete the survey once. An honorarium (equivalent to the cost of a cardiologist consultation in France) was paid to each physician who completed the online survey.
Statistical analysis
Based on feasibility constraints, we assumed that, of 400 physicians invited to participate, a maximum of 250 physicians would complete the survey, providing a maximum of 750 case vignettes for analysis.
Since this was essentially an observational study, all analyses were considered descriptive and the results were reported as the frequency and percentage of each modality. No imputation was made for missing data.
In the case vignettes, the Fisher exact test was used to identify the relationship between LDL-C target and CV risk.
Results
Participants
Of the 400 physicians invited to participate, 162 participated in the clinical case assessments, with all 162 participating physicians completing Case 1, 160 completing Case 2 and 158 completing Case 3. Of the 158 physicians with sociodemographic data available, most participants (n = 114/158; 72%) were male, 61 (39%) were aged 25–50 years, 48 (30%) were aged 51–60 years and 49 (31%) were aged ≥61 years (Supplementary Table 1).
Risk stratification & LDL-C targets
Of the 480 risk assessments across the three case vignettes, eight were assigned to a low-risk category, 105 to moderate-risk, 160 to high-risk and 207 to a very high-risk category (Table 1). Overall, 276/480 risk assessments (58%) assigned the hypothetical patients to the correct risk category according to ESC/EAS hypercholesterolemia guidelines [6].
| Participant assessment, n (%) | Case 1: primary prevention with moderate CKD | Case 2: secondary prevention post-ACS | Case 3: secondary prevention with symptomatic PAD |
|---|---|---|---|
| Cardiovascular risk | (n = 162) | (n = 160) | (n = 158) |
| Low | 6 (3.7) | 0 | 2 (1.3) |
| Moderate | 74 (45.7) | 1 (0.6) | 30 (19.0) |
| High | 76 (46.9) | 27 (16.9) | 57 (36.1) |
| Very high | 6 (3.7) | 132 (82.5) | 69 (43.7) |
| Risk category according to ESC/EAS 2019 recommendations | High | Very high | Very high |
| Risk underestimated | 80 (49.4) | 28 (17.5) | 89 (56.3) |
| Target LDL-C level | (n = 162) | (n = 160) | (n = 158) |
| <1.4 mmol/l (<0.55 g/l) | 5 (3.1) | 134 (83.8) | 46 (29.1) |
| <1.8 mmol/l (<0.7 g/l) | 37 (22.8) | 25 (15.6) | 58 (36.7) |
| <2.6 mmol/l (<1.0 g/l) | 61 (37.7) | 1 (0.6) | 34 (21.5) |
| <3.0 mmol/l (<1.15 g/l) | 27 (16.7) | 0 | 4 (2.5) |
| <3.4 mmol/l (<1.3 g/l) | 32 (19.8) | 0 | 16 (10.1) |
| Target LDL-C level according to ESC/EAS 2019 recommendations | <1.8 mmol/l (<0.7 g/l) | <1.4 mmol/l (<0.55 g/l) | <1.4 mmol/l (<0.55 g/l) |
| Target overestimated | 120 (74.1) | 26 (16.3) | 112 (70.9) |
Values in bold indicate the correct category/target for each case vignette.
ACS: Acute coronary syndrome; CKD: Chronic kidney disease; EAS: European Atherosclerosis Society; ESC: European Society of Cardiology; LDL-C: Low-density lipoprotein cholesterol; PAD: Peripheral arterial disease.
A high proportion of physicians (132/160; 83%) correctly identified Case 2 (secondary prevention post-ACS) as being at very high risk, but the risk category was underestimated for Case 1 (primary prevention with moderate CKD) by 49% (80/162) of physicians and for Case 3 (symptomatic PAD) by 56% (89/158) (Table 1 & Figure 1).

Figure 1. Cardiovascular risk category assigned to each case at visit 1 (due to rounding, the sum total exceeds 100% for some cases).
The black box indicates the proportion of physicians who underestimated each case’s risk category.
ACS: Acute coronary syndrome; CKD: Chronic kidney disease; PAD: Peripheral arterial disease.
In Case 1 (primary prevention with moderate CKD), a CAC score was obtained between visits 1 and 2 and the patient had a score of 300 Agatston units. When asked to reassess the patient’s risk at visit 2, the cardiologists made only minor changes to the risk category, with a slight reduction in the number of physicians classifying the patient as moderate or high risk and an increase in the number classifying the patient as low or very high risk (Figure 2).
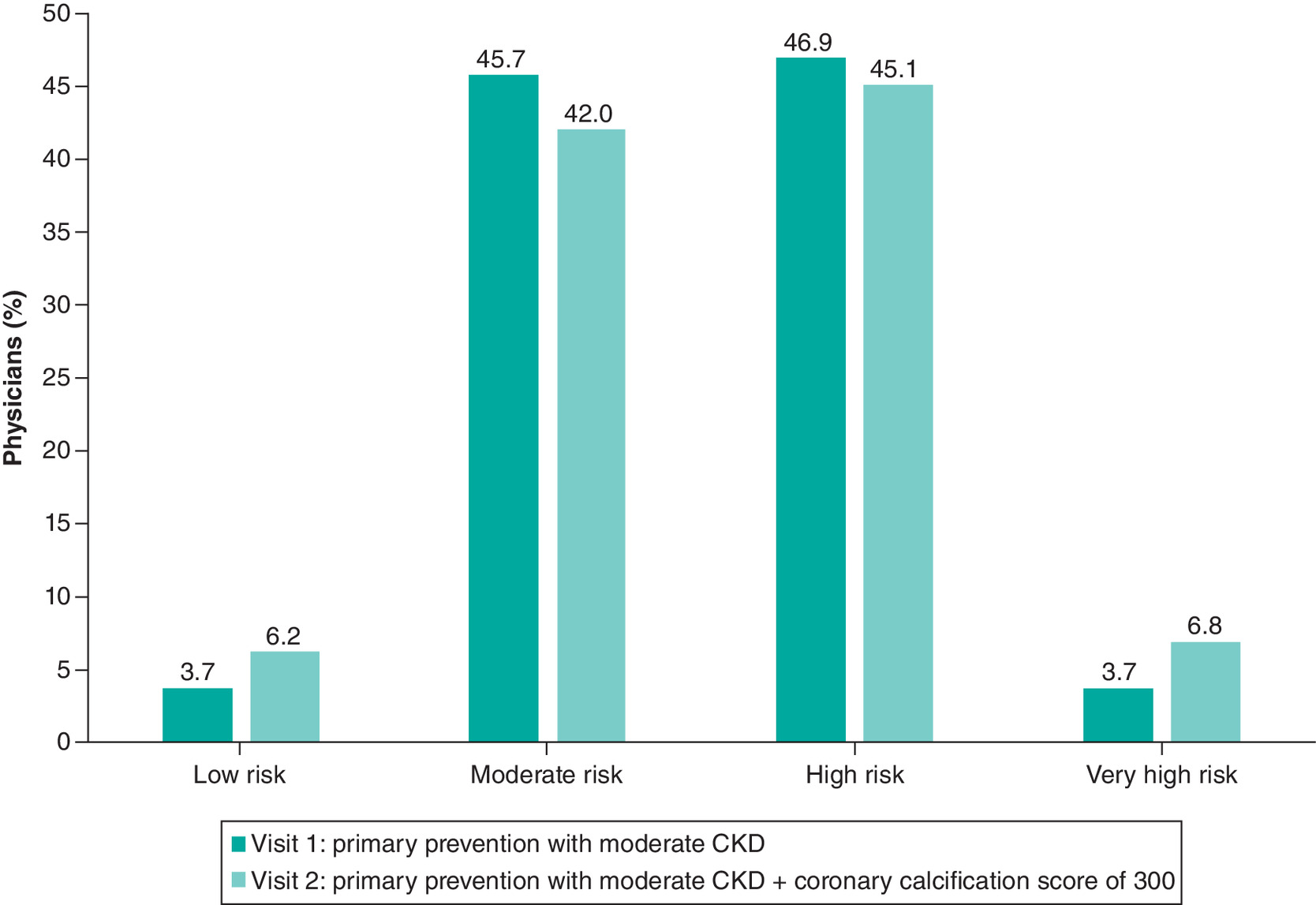
Figure 2. Cardiovascular risk category assigned to Case 1 (primary prevention with moderate chronic kidney disease) at visits 1 and 2.
CKD: chronic kidney disease.
A high proportion of participating cardiologists (134/160; 84%) defined the correct LDL-C target according to ESC/EAS recommendations for Case 2 (secondary prevention post-ACS), but a higher-than-recommended LDL-C target was set by 74% (120/162) for Case 1 (primary prevention with moderate CKD) and by 71% (112/158) for Case 3 (symptomatic PAD; Table 1).
There were differences between CV risk categories in the proportion of physicians who gave the correct LDL-C target (Table 2; p < 0.0001). Overall, 50% (4/8) of physicians who assigned the case to a low-risk category gave the correct LDL-C target (<3.0 mmol/l [<1.15 g/l]) for that category, 35% (37/105) who considered the case to be moderate-risk gave the correct LDL-C target (<2.6 mmol/l [<1.0 g/l]) for that category, 50% (80/160) who assigned the case to a high-risk category gave the correct LDL-C target (<1.8 mmol/l [<0.7 g/l]), but 83% (171/207) of physicians who assigned the case to the very high-risk category gave the correct LDL-C target (<1.4 mmol/l [<0.55 g/l]).
| CV risk category | LDL-C target | ||||
|---|---|---|---|---|---|
| <3.4 mmol/l (<1.3 g/l) | <3.0 mmol/l (<1.15 g/l) | <2.6 mmol/l (<1.0 g/l) | <1.8 mmol/l (<0.7 g/l) | <1.4 mmol/l (<0.55 g/l) | |
| Low risk | 50.0 | 50.0 | 0 | 0 | 0 |
| Moderate risk | 39.1 | 18.1 | 35.2 | 7.6 | 0 |
| High risk | 1.9 | 5.0 | 34.4 | 50.0 | 8.7 |
| Very high risk | 0 | 0 | 1.9 | 15.5 | 82.6 |
Values in bold italics indicate the correct target for the specific cardiovascular risk category.
CV: Cardiovascular; LDL-C: Low-density lipoprotein cholesterol.
Treatments
Most physicians selected lifestyle changes for all three patients (Supplementary Table 2). Approximately 25% (41/162) of physicians selected lifestyle changes alone for Case 1 (primary prevention with moderate CKD) at visit 1, but none chose this option for Case 2 (secondary prevention post-ACS) and only 5% (8/158) chose lifestyle measures alone for Case 3 (symptomatic PAD).
Statins were the most commonly chosen type of pharmacotherapy at visit 1, as monotherapy or in combination with another drug or lifestyle changes, being selected by 74% (119/162) of physicians for Case 1 (primary prevention with moderate CKD), 98% (156/160) for Case 2 (secondary prevention post-ACS) and 89% (140/158) for Case 3 (symptomatic PAD). In all cases, statin therapy was commonly selected in combination with lifestyle changes at visit 1 (Figure 3).
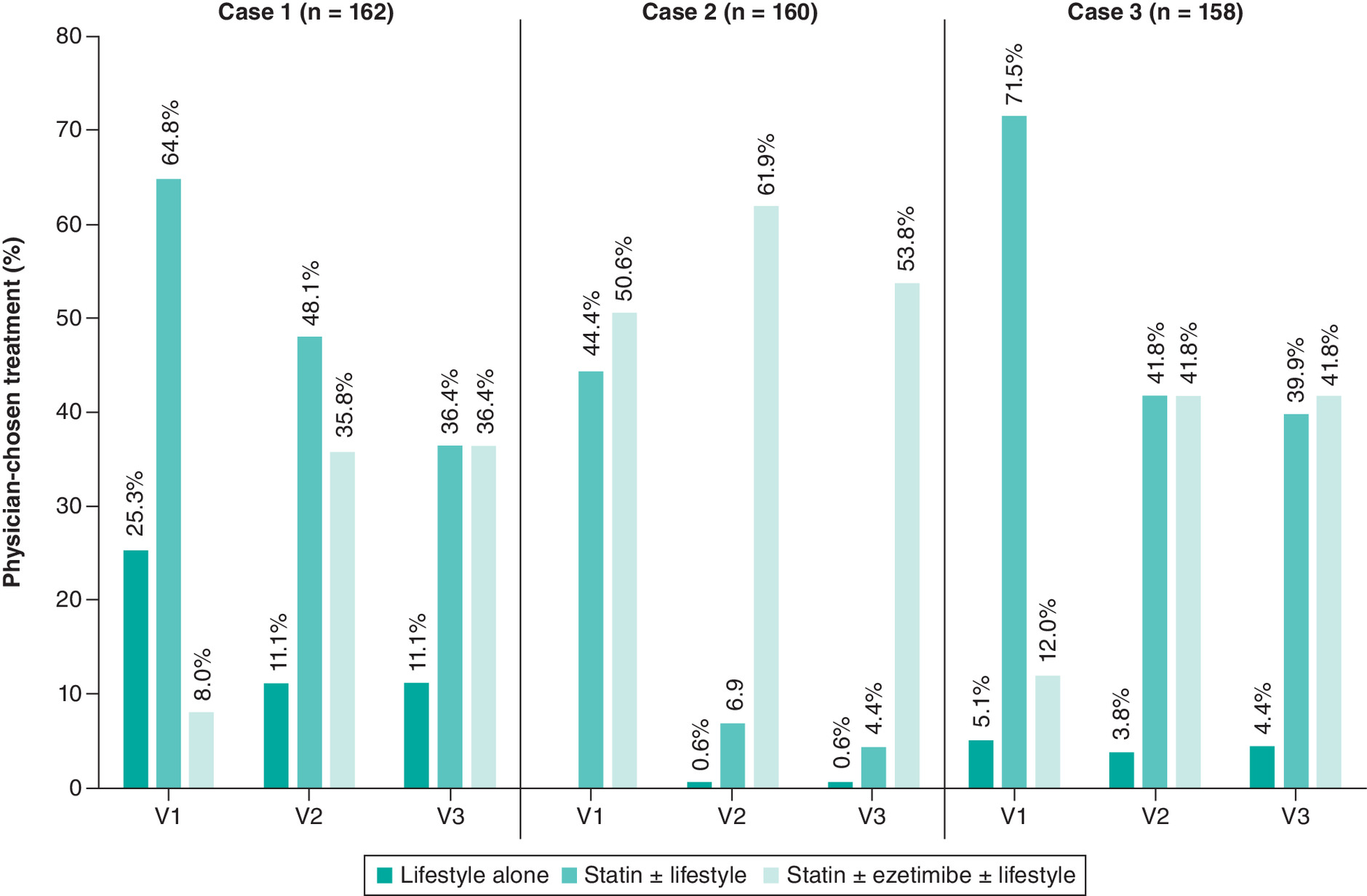
Figure 3. Use of statins ± ezetimibe ± lifestyle at each visit in Case 1 (primary prevention with moderate chronic kidney disease), Case 2 (secondary prevention post acute coronary syndrome) and Case 3 (secondary prevention with symptomatic peripheral arterial disease).
V: Visit.
Among statins, atorvastatin was the most commonly chosen statin at visit 1 in all three cases. None of the physicians selected cholestyramine for any patient at any visit. The most common combination chosen was a statin + ezetimibe, with or without concomitant lifestyle measures (Figure 3 & Supplementary Table 2). Among physicians who chose to prescribe statins, the proportion who selected high-intensity statins increased from 26% (31/119) at visit 1 to 42% (52/123) at visit 3 for Case 1 and from 51% (71/140) at visit 1 to 72% (99/137) at visit 3 for Case 3 (Supplementary Table 3). Most physicians selected high-intensity statins for Case 2 irrespective of visit, ranging from 79% (124/156) at visit 1 to 88% (105/120) at visit 3.
Treatment choice was influenced by the risk category applied in each case at visit 1. Regardless of the CV risk level, statins were the most commonly prescribed treatment; for low-risk, moderate-risk, high-risk and very high-risk cases, 25% (2/8), 53% (56/105), 96% (154/160) and 98% (203/207) of physicians, respectively, chose statins. Similarly, ezetimibe was not selected for any low-risk cases, but was chosen by 6% (6/105), 18% (28/160) and 44% (90/207) of physicians for moderate-, high- and very high-risk cases, respectively.
In Case 1 (primary prevention with moderate CKD), LDL-C levels remained uncontrolled at visit 2, and the patient had a CAC score of 300 Agatston units. Overall, 16% (26/162) of physicians chose to leave the treatment unchanged at visit 2 for Case 1 (after CAC score was available), but 84% (136/162) revised the treatment. However, at visit 3, although LDL-C levels still remained uncontrolled, 61% (99/162) of physicians chose to leave treatment unchanged for Case 1 (primary prevention with moderate CKD) and only 39% (63/162) changed the treatment.
Physicians were more likely to change the prescription for Case 2 (secondary prevention post-ACS) when LDL-C targets were not met: 96% (154/160) opted to change the treatment at visit 2 and 80% (128/160) chose to change treatment at visit 3. For this case, the presence of myalgia reduced the proportion of physicians who chose a statin (from 78% [65/83] without myalgia to 73% [56/77] with myalgia) or ezetimibe (from 86% [71/83] without myalgia to 70% [54/77] with myalgia) and increased the proportion of physicians who selected a PCSK9 inhibitor (from 17% [14/83] without myalgia to 25% [19/77] with myalgia).
For Case 3 (symptomatic PAD), 82% (129/158) of physicians changed the treatment at visit 2. Although all the patients achieved their LDL-C targets at visit 3, treatment was changed by 10% (15/158) of physicians.
Among all case vignettes, the most common treatment change at visits 2 and 3 was the addition of a new agent, usually ezetimibe (Figure 3 & Supplementary Table 2). The most common reason the physicians gave for their choice of treatment at visit 3 was the patient’s CV risk (52% [248/480] of all physicians across all cases); the second most common reason was the difference between the actual LDL-C level and the target level (in 25% [119/480] of physicians across all three cases; Supplementary Figure 2).
Discussion
Our case-vignette-based study in 162 French cardiologists working completely or partially in private practice indicates some lack of knowledge about CV risk stratification, LDL-C targets and treatment recommendations according to the current (2019) ESC/EAS hypercholesterolemia guidelines [6].
For the hypothetical primary prevention patient with moderate CKD or the one with symptomatic PAD, more than half of the physicians assigned the cases to the wrong CV risk category and CV risk for these cases was underestimated by 49 and 56% of physicians, respectively. Moreover, at least half of the cardiologists were unable to choose the recommended LDL-C target level for cases they considered to be at low, moderate or high risk, although approximately 83% of physicians chose the correct LDL-C target for the cases at very high CV risk. As a result, a higher-than-recommended target LDL-C level was set by 74% of physicians for the primary prevention case with moderate CKD (Case 1) and by 71% for the symptomatic PAD case (Case 3). Physicians were most likely to correctly identify Case 2 (the secondary prevention post-ACS patients) as being at very high risk (by 83% of physicians) and as needing the most stringent target LDL-C level (by 84%); nevertheless, 18% of physicians still underestimated the CV risk and 16% overestimated the target LDL-C level in this case.
Our research is not the first to find that physicians tend to underestimate CV risk [17,18], although most studies have been conducted in primary care rather than specialist cardiology practice, did not use simulated virtual patient cases and were published >5 years ago. Further, data from studies conducted in countries other than France may not be directly comparable with our findings; however, such studies do provide an opportunity to assess international differences and similarities in clinical practice. Liew and colleagues investigated CV risk assessment by primary care physicians in Malaysia and found that the risk was underestimated in 60% of high-risk patients [18]. Patient factors associated with the underestimation of CV risk were female sex, younger age, non smoking status and absence of hypertension and diabetes [18], some of which were also present in the case vignettes in our survey. In France, Bruckert and colleagues found that primary care physicians tended to underestimate the risk of patients at high CV risk and overestimate the risk for patients with a medium risk [17].
One possible explanation for the finding that physicians underestimate CV risk is the underuse or mistrust in the accuracy of validated risk assessment tools [19]. Research conducted in the 2000s found that 62% of European physicians (including cardiologists) were more likely to base their CV risk assessments on subjective judgement than on formal risk calculators, and that the proportion choosing subjective assessment was highest (88%) in France [20]. Nevertheless, the case vignettes in our study did not require use of a risk assessment tool, since they all had documented atherosclerotic CV disease or CKD and could therefore be assigned to a high- or very high-risk category without the use of a risk assessment model according to ESC/EAS hypercholesterolemia guidelines [6]. It is likely that the cardiologists in our survey underestimated the importance of moderate CKD in the primary prevention case vignette and symptomatic PAD in Case 3 when assigning the risk level for these patients.
Related to the underestimation of CV risk by cardiologists in our study was the selection of incorrect LDL-C targets in 55% of the cases. The selection of the correct LDL-C target was highest in Case 2 (secondary prevention post-ACS), and closely mirrored the correct selection of CV risk category in this patient. However, knowledge of correct LDL-C targets was low in the other cases (23% in Case 1: primary prevention with moderate CKD and 29% in Case 3: symptomatic PAD), and most physicians assigned these patients a higher-than-recommended target LDL-C level. Moreover, as shown in Table 2, irrespective of whether the CV risk category was correct or not, the choice of LDL-C target did not align with the assigned risk categories in at least 50% of cases considered to be at low, medium or high risk. This suggests a lack of knowledge about LDL-C target levels by French cardiologists for patients other than those with a recent ACS.
Another finding in our study was the lack of effect of the CAC score on the cardiologists’ assessment of CV risk assessment in Case 1 (primary prevention with moderate CKD). The ESC/EAS hypercholesterolemia guidelines note that the presence of a CAC score >100 Agatston units modifies the CV risk in asymptomatic patients at low or moderate risk, and may result in them being reclassified to a higher risk bracket [6]. However, in our survey, the presence of a CAC score of 300 Agatston units in this case made little difference to their original risk categorization.
The absence of CAC (score 0 Agatston units) is a statistically significant negative predictor of CV events, associated with a low 10 year risk of CV events in patients who would otherwise be classified as at moderate risk [21]. However, when calcification is present, there is no defined threshold of CAC score that predicts CV risk, because the relationship between CAC score and risk must be interpreted according to the expected values for the patient’s age, race and sex [22]. A large-scale analysis of real-world patients found that, when primary prevention patients have any level of CAC (score >0 Agatston units), the benefit they derive from statin therapy is equivalent to the benefit achieved by secondary prevention patients [23]. Moreover, the more severe the CAC, the greater the likely benefit from statin therapy [23].
The 2019 ESC/EAS guidelines on dyslipidemia management suggest a CAC score of >100 Agatston units to modify risk [6]. However, the 2021 ESC/EAS guidelines on the primary prevention of CV disease do not specify a threshold, but recommend interpreting the CAC score based on the patient's age and sex [24]. Using the reference CAC score values from the multi-ethnic study of atherosclerosis [22], a CAC score of 300 Agatston units in Case 1 in our study would be higher than the 90th percentile in a woman aged ≥65 years or a man aged ≥55 years. While it may be tempting to speculate that the cardiologists in our study did not modify the CV risk category in Case 1 based on the CAC score because they were following the 2021 EAS recommendations on primary prevention, it is unlikely based on the timing of that publication (September 2021) compared with the conduct of our study (April–September 2021).
The underestimation of risk by cardiologists may lead to under treatment, and this was also apparent in our study (Figure 3). In fact, in all three case vignettes, high-intensity statin therapy should be prescribed according to the practical guidance on lipid-lowering therapy from the EAS [25]. While high-intensity statins were the most commonly prescribed lipid-lowering therapy by the cardiologists participating in our survey, few physicians increased treatment intensity at visits 2 and 3. In addition, few physicians would implement PCSK9 inhibitor therapy, which is likely explained by the approved indications (only for secondary prevention after LDL-C levels remain uncontrolled after maximally tolerated statin therapy ± other lipid-lowering agents) and reimbursement restrictions placed on the use of these agents in France.
Unfortunately, the under treatment of hypercholesterolemia in Europe (generally) and France (specifically) has been demonstrated in multiple previous studies [8,10–12,26–30]. The Europe-wide DA VINCI study of primary or secondary prevention patients being treated in primary care or by a cardiologist found that only 33% of patients achieved the 2019 guideline recommended LDL-C targets [29]. Moreover, only 18% of patients in the very high-risk category achieved the 2019 LDL-C targets in the DA VINCI study; only 11% reached this target on statin monotherapy and 21% achieved the target on the combination of a statin with ezetimibe or PCSK9 inhibitor [29]. This is concerning because data show that therapeutic inertia in the management of hypercholesterolemia is associated with an increased risk of CV events [26].
Our data indicate that French cardiologists were more likely to initiate intensive therapy and escalate therapy for post-ACS patients than for primary prevention patients with moderate CKD or those with symptomatic PAD. In this respect, our data are consistent with the DAUSSET study on the real-world treatment practices of French cardiologists in very high-risk secondary prevention patients [27]. In that study, 98% of the secondary prevention post-ACS patients were prescribed lipid-lowering therapy, and 81% had treatment intensified during follow-up, usually because the LDL-C target had not been met [27]. It should be noted that the target LDL-C level was <1.8 mmol/l (<0.7 g/l) in most patients in the DAUSSET study [27]. Mert and colleagues reported similar undertreatment of hypercholesterolemia by Turkish cardiologists, specifically in patients with diabetes, with underuse of statins and suboptimal statin dosages being the most commonly cited reason for not achieving LDL-C targets [28].
Similarly, our study showed a low rate of treatment modification in response to the development of myalgia during statin therapy. Physicians may consider myalgia to be unrelated to statin therapy, based on the high incidence of background muscle pain in the general population, or to be a ‘nocebo’ effect arising from the patient’s expectations of muscle symptoms [31]. Placebo-controlled studies suggest that myalgia may be unrelated to statin therapy in approximately 50% of patients who develop it [32]. According to a recent large-scale analysis, fewer than 10% of patients on statins are unable to tolerate these agents at the dosage required to reduce CV risk, although certain factors (e.g., female sex, age ≥65 years and comorbidities, such as diabetes and chronic renal disease) increase the risk [33]. Our data suggest that the French cardiologists in our survey are choosing to monitor patients with myalgia during statin therapy rather than immediately modifying the regimen.
Our study has strengths and limitations. First, we did not achieve the planned enrolment of 250 physicians, in part due to the SARS-CoV-2 pandemic and associated lockdowns in France; however, we believe that the descriptive data provided by the 162 participating physicians still accurately demonstrates the underestimation of CV risk among cardiologists in France. Second, our study used theoretical patient case vignettes, which may be seen as a limitation, since we did not assess actual prescribing patterns. However, the use of theoretical case vignettes is also a strength because this method has proven validity [16], controls for patient variability and provides a more reliable method of assessing practice patterns compared with chart abstraction [34]. Moreover, we carefully designed our study to limit bias by randomizing patient characteristics within each case. We also limited the number of case vignettes to three in order to retain physician attention (and therefore response reliability) [35]. However, the online survey we used to assess physicians’ responses to the case vignettes was not formally validated. Finally, we did not gather information on the experience of the participating physicians (i.e., number of years in practice). Nevertheless, some correlation is expected between physician age, which was evenly distributed among the participating physicians (~33% in each of the three main age groups) and the number of years in practice, although we accept that this could be biased by the quality of initial and ongoing training and not necessarily linked to age.
Conclusion
Our survey of cardiologists in France indicates that many underestimate the CV risk faced by patients with hypercholesterolemia and additional risk factors. As a result, a high proportion of French cardiologists also set a higher-than-recommend target LDL-C level and prescribe less intensive lipid-lowering treatment than many patients need.
•
Patients in France with hypercholesterolemia generally receive suboptimal treatment in terms of achieving low-density lipoprotein cholesterol (LDL-C) targets and this could be due to physicians having low awareness of treatment goals and guidelines, therapeutic inertia or reluctance to prescribe lipid-lowering therapies to target LDL-C levels or poor patient adherence.
•
An online interactive survey of 162 cardiologists from various regions of France used hypothetical patient case vignettes to assess individual physicians’ approaches to hypercholesterolemia management in patients with high- and very high-cardiovascular (CV) risk.
•
Randomly defined case vignettes applied to three clinical scenarios were as follows: Case 1 – a high-risk primary prevention patient with moderate chronic kidney disease (CKD); Case 2 – a secondary prevention patient with a recent acute coronary syndrome (ACS); and Case 3 – a secondary prevention patient with symptomatic peripheral arterial disease (PAD).
•
Although the secondary prevention patient with recent ACS (Case 2) was correctly identified as being at very high risk by 83% of physicians, more than half of the physicians assigned the high-risk primary prevention patient with moderate CKD (Case 1) and the very high-risk secondary prevention patient with symptomatic PAD (Case 3) to the wrong CV risk category, with 49 and 56% of physicians, respectively, underestimating the CV risk.
•
A coronary artery calcification score of 300 Agatston units in our survey did not significantly change the original categorization of low- or moderate-risk patients, although European Society of Cardiology/European Atherosclerosis Society guidelines suggest reclassification of risk in cases where the coronary artery calcification score is >100 Agatston units.
•
At least half of the cardiologists did not choose the recommended LDL-C target level for cases they considered to be at low, moderate or high risk, with a higher-than-recommended LDL-C target set for the high-risk primary prevention patient with moderate CKD (Case 1) and the very high-risk secondary prevention patient with symptomatic PAD (Case 3).
•
The most common choice of pharmacotherapy included statins as monotherapy or in combination with ezetimibe, with or without concomitant lifestyle changes.
•
Our data indicate that French cardiologists were more likely to initiate intensive therapy and escalate therapy for post-ACS patients than for primary prevention patients with moderate CKD or those with symptomatic PAD, and would choose to monitor patients with myalgia during statin therapy rather than immediately modify the regimen.
Author contributions
J Ferrières, E Bruckert, M Farnier, M Krempf, J-J Mourad and F Schiele: designed the research study, reviewed the protocol and the case-vignettes, analyzed and interpreted the results, reviewed the manuscript. B Roux: wrote the protocol, designed the case-vignettes, implemented the serious game methodology, ensured data management and statistical analysis, reviewed the manuscript.
Acknowledgments
This study was conducted by FAST4. The authors would like to thank C Rees of Springer Healthcare Communications, who wrote the outline and first draft of the manuscript.
Financial & competing interests disclosure
This work was supported by Servier. J Ferrières has received personal fees from Amgen, Sanofi and Servier. E Bruckert has received honoraria from Amgen, Genfit, MSD, Sanofi, Regeneron, Danone, Aegerion Pharmaceuticals, Lilly, Ionis Pharmaceuticals, Silence Therapeutics, Akcea Therapeutics, Novartis, Amarin Corporation, Servier and Mylan/Viatris. M Farnier has received consulting fees and/or honoraria from Abbott, Amarin, Amgen, AstraZeneca, Austell, Kowa, Merck and Co., Organon, Recordati, Sanofi/Regeneron, Servier, SMB and Viatris. M Krempf has received consulting fees and/or honoraria from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Servier and Sanofi. J-J Mourad has received fees for consultancy from Servier, Viatris, Pfizer and Isis Medical. B Roux is the director of FAST4, Clinical Research Organization. F Schiele reports personal fees from Amgen, Astra Zeneca, Bayer, Pfizer, Recordati, Mylan, Novo Nordisk, Novartis and Sanofi, outside the submitted work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing assistance was provided by Catherine Rees of Springer Healthcare Communications, who wrote the outline and first draft of the manuscript. This medical writing assistance was funded by Servier.
Ethical conduct of research
The authors state that they have followed the principles outlined in the Declaration of Helsinki for all human experimental investigations. In addition, they have obtained verbal and written informed consent from the participants for the inclusion of their data within this work.
Data sharing statement
Data generated during this study are available from the corresponding author upon reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 403.05 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Townsend N, Nichols M, Scarborough P, Rayner M. Cardiovascular disease in Europe–epidemiological update 2015. Eur. Heart J. 36(40), 2696–2705 (2015).
2.
Timmis A, Townsend N, Gale CP et al. European Society of Cardiology: cardiovascular disease statistics 2019. Eur. Heart J. 41(1), 12–85 (2020).
3.
Tuppin P, Rivière S, Rigault A et al. Prevalence and economic burden of cardiovascular diseases in France in 2013 according to the national health insurance scheme database. Arch. Cardiovasc. Dis. 109(6–7), 399–411 (2016).
4.
Ference BA, Ginsberg HN, Graham I et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society consensus panel. Eur. Heart J. 38(32), 2459–2472 (2017).
• Consensus statement from the European Atherosclerosis Society (EAS) summarizing the genetic and clinical evidence supporting a causal relationship between low-density lipoproteins and atherosclerotic cardiovascular disease.
5.
Domanski MJ, Tian X, Wu CO et al. Time course of LDL cholesterol exposure and cardiovascular disease event risk. J. Am. Coll. Cardiol. 76(13), 1507–1516 (2020).
6.
Mach F, Baigent C, Catapano AL et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur. Heart J. 41(1), 111–188 (2020).
•• These European Society of Cardiology (ESC) and EAS guidelines propose novel low-density lipoprotein cholesterol goals and provide advice on cardiovascular risk stratification and patient management.
7.
Olie V, Grave C, Gabet A. Impact of lowering low-density lipoprotein cholesterol thresholds on the proportion of adults requiring an intervention: application of the 2019 ESC/EAS guidelines for the management of dyslipidaemia to the French population. Arch. Cardiovasc. Dis. 115(2), 106–108 (2022).
8.
Blacher J, Gabet A, Vallee A et al. Prevalence and management of hypercholesterolemia in France, the Esteban observational study. Medicine (Baltimore) 99(50), e23445 (2020).
9.
Beliard S, Boccara F, Cariou B et al. High burden of recurrent cardiovascular events in heterozygous familial hypercholesterolemia: the French Familial Hypercholesterolemia Registry. Atherosclerosis 277, 334–340 (2018).
10.
Berard E, Bongard V, Haas B et al. Prevalence and treatment of familial hypercholesterolemia in France. Can. J. Cardiol. 35(6), 744–752 (2019).
11.
Ferrieres J, Banks V, Pillas D et al. Screening and treatment of familial hypercholesterolemia in a French sample of ambulatory care patients: a retrospective longitudinal cohort study. PLoS ONE 16(8), e0255345 (2021).
12.
Ferrieres J, Rouyer MV, Lautsch D et al. Suboptimal achievement of low-density lipoprotein cholesterol targets in French patients with coronary heart disease. Contemporary data from the DYSIS II ACS/CHD study. Arch. Cardiovasc. Dis. 110(3), 167–178 (2017).
13.
Kousignian I, Sautereau A, Vigouroux C et al. Diagnosis, risk factors and management of diabetes mellitus in HIV-infected persons in France: a real-life setting study. PLoS ONE 16(5), e0250676 (2021).
14.
Allen JD, Curtiss FR, Fairman KA. Nonadherence, clinical inertia, or therapeutic inertia? J. Manag. Care Pharm. 15(8), 690–695 (2009).
15.
Rizos CV, Barkas F, Elisaf MS. Reaching low density lipoprotein cholesterol targets. Curr. Med. Res. Opin. 30(10), 1967–1969 (2014).
16.
Peabody JW, Luck J, Glassman P et al. Measuring the quality of physician practice by using clinical vignettes: a prospective validation study. Ann. Intern. Med. 141(10), 771–780 (2004).
17.
Bruckert E, Bonnelye G, Thomas-Delecourt F, André L, Delaage PH. Assessment of cardiovascular risk in primary care patients in France. Arch. Cardiovasc. Dis. 104(6–7), 381–387 (2011).
18.
Liew SM, Lee WK, Khoo EM et al. Can doctors and patients correctly estimate cardiovascular risk? A cross-sectional study in primary care. BMJ Open 8(2), e017711 (2018).
19.
Hobbs FD, Jukema JW, Da Silva PM, Mccormack T, Catapano AL. Barriers to cardiovascular disease risk scoring and primary prevention in Europe. QJM 103(10), 727–739 (2010).
20.
Graham IM, Stewart M, Hertog MG. Cardiovascular Round Table Task Force. Factors impeding the implementation of cardiovascular prevention guidelines: findings from a survey conducted by the European Society of Cardiology. Eur. J. Cardiovasc. Prev. Rehabil. 13(5), 839–845 (2006).
21.
Nasir K, Bittencourt MS, Blaha MJ et al. Implications of coronary artery calcium testing among statin candidates according to American College of Cardiology/American Heart Association cholesterol management guidelines: MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Coll. Cardiol. 66(15), 1657–1668 (2015).
22.
Mcclelland RL, Chung H, Detrano R, Post W, Kronmal RA. Distribution of coronary artery calcium by race, gender, and age: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation 113(1), 30–37 (2006).
23.
Mitchell JD, Fergestrom N, Gage BF et al. Impact of statins on cardiovascular outcomes following coronary artery calcium scoring. J. Am. Coll. Cardiol. 72(25), 3233–3242 (2018).
24.
Visseren FLJ, Mach F, Smulders YM et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 42(34), 3227–3337 (2021).
•• Guidelines from the ESC proposing novel approaches to tailored treatment intensification and summarizing recent evidence on the efficacy of antithrombotic treatment regimens in atherosclerotic cardiovascular disease.
25.
Averna M, Banach M, Bruckert E et al. Practical guidance for combination lipid-modifying therapy in high- and very-high-risk patients: a statement from a European Atherosclerosis Society task force. Atherosclerosis 325, 99–109 (2021).
•• This guideline provides evidence based practical advice for the use of combination lipid-modifying therapy to treat elevated low-density lipoprotein cholesterol/or triglycerides in high-risk and very-high-risk patients to prevent atherosclerotic cardiovascular disease events.
26.
Diaz Rodriguez A, Murga N, Camafort-Babkowski M et al. Therapeutic inertia in hypercholesterolaemia is associated with ischaemic events in primary care patients. a case-control study. Int. J. Clin. Pract. 68(8), 1001–1009 (2014).
27.
Ferrieres J, Roubille F, Farnier M et al. Control of low-density lipoprotein cholesterol in secondary prevention of coronary artery disease in real-life practice: the DAUSSET study in French cardiologists. J. Clin. Med. 10(24), 5938 (2021).
• A national, multicenter, non interventional study describing real-life clinical practices for low-density lipoprotein cholesterol control as secondary prevention of coronary heart disease.
28.
Mert KU, Basaran O, Mert GO et al. Management of LDL-cholesterol levels in patients with diabetes mellitus in cardiology practice: real-life evidence of under-treatment from the EPHESUS registry. Eur. J. Clin. Invest. 51(7), e13528 (2021).
29.
Ray KK, Molemans B, Schoonen WM et al. EU-wide cross-sectional observational study of lipid-modifying therapy use in secondary and primary care: the DA VINCI study. Eur. J. Prev. Cardiol. 28(11), 1279–1289 (2021).
30.
Ferrieres J, Gorcyca K, Iorga SR, Ansell D, Steen DL. Lipid-lowering therapy and goal achievement in high-risk patients from French general practice. Clin. Ther. 40(9), 1484–1495 e1422 (2018).
• This retrospective database study summarizes the patterns of lipid-lowering therapy use and its role in achieving guideline-identified lipid goals in a French general practice cohort with atherosclerotic cardiovascular disease/or diabetes mellitus.
31.
Mammen AL. Statin-associated myalgias and muscle injury-recognizing and managing both while still lowering the low-density lipoprotein. Med. Clin. North Am. 105(2), 263–272 (2021).
32.
Parker BA, Capizzi JA, Grimaldi AS et al. Effect of statins on skeletal muscle function. Circulation 127(1), 96–103 (2013).
33.
Bytyçi I, Penson PE, Mikhailidis DP et al. Prevalence of statin intolerance: a Meta-Analysis. Eur. Heart J. 43(34), 3213–3223 (2022).
34.
Peabody JW, Luck J, Glassman P, Dresselhaus TR, Lee M. Comparison of vignettes, standardized patients, and chart abstraction: a prospective validation study of 3 methods for measuring quality. JAMA 283(13), 1715–1722 (2000).
•• A prospective validation study assessing the suitability of clinical vignettes as a means for measuring physician competence and quality of practice.
35.
Bachmann LM, Muhleisen A, Bock A, Ter Riet G, Held U, Kessels AG. Vignette studies of medical choice and judgement to study caregivers' medical decision behaviour: systematic review. BMC Med. Res. Methodol. 8, 50 (2008).
Information & Authors
Information
Published In
Copyright
© 2023 Jean Ferrières. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 17 October 2022
Accepted: 6 February 2023
Published online: 8 March 2023
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Evaluation of hypercholesterolemia management in at-risk patients by cardiologists in France: a case vignette-based study. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2022-0181
Export citation
Select the citation format you wish to export for this article or chapter.