Network meta-analysis of multiple doses of vonoprazan for the treatment of erosive esophagitis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: 20 mg of vonoprazan (VPZ20) is recommended in most countries to treat erosive esophagitis (EE). Whether other doses of vonoprazan, such as 5 mg (VPZ5), 10 mg (VPZ10), 20 mg (VPZ20), and 40 mg (VPZ40) are more effective is unknown. Materials & methods: Three databases were electronically searched to identify studies published before November 2021. Network meta-analysis was performed using STATA 14.0. Results: VPZ20 and VPZ40 were comparable to PPI, VPZ5 and VPZ10 in 4- and 8-week healing rates, and this was also detected in patients with refractory EE. All regimens resulted in similar treatment-emergent adverse events (TEAEs). However, VPZ40 ranked first for healing rate and TEAEs; however, VPZ20 ranked worst for TEAEs. Conclusion: Different doses of VPZ are comparable in efficacy and safety, but VPZ40 may be best in both effectiveness and safety.
Tweetable abstract
A new network meta-analysis reveals that 40 mg of #vonoprazan may be the best dosing strategy for treating #erosive esophagitis from the perspective of both effectiveness and safety.
Plain language summary
What is this article about?
Erosive esophagitis refers to esophageal mucosal erosions on endoscopy and heartburn symptoms, accounting for 10% of gastroesophageal reflux disease (GERD). A recent meta-analysis has evaluated the efficacy and safety of 20 mg of vonoprazan as a novel potassium-competitive acid blocker. However, other doses, including 5 mg, 10 mg and 40 mg, are also used in practice. Therefore, this study aimed to determine the optimal dosing strategy of vonoprazan in treating erosive esophagitis.
What were the results?
Different doses of vonoprazan had comparable efficacy and safety; however, 40 mg of vonoprazan may be the best option for treating erosive esophagitis from the perspective of both efficacy and safety.
What do the results of the study mean?
In order to achieve a satisfactory healing rate and lower treatment-emergent adverse events for the treatment of erosive esophagitis in practice, priority should be given to choosing 40 mg of vonoprazan.
Gastroesophageal reflux disease (GERD) is a common gastrointestinal disorder that results from the retrograde flow of stomach contents into the esophagus and is characterized by troublesome complications such as heartburn and acid regurgitation [1]. The prevalence of GERD has been increasing, and a recent meta-analysis of approximately 100 studies reported a global prevalence of 13.3%, 17.1% in Europe, 15.4% in North America and 10.0% in Asia [2]. GERD could be mainly classified into two subtypes based on endoscopic findings, including non-erosive reflux disease and erosive esophagitis [3]. Erosive esophagitis, defined as esophageal mucosal erosions on endoscopy and heartburn symptoms [4], accounts for 10% of GERD [5].
The effective treatment of erosive esophagitis mainly starts from: relieving symptoms, accelerating esophageal mucosal healing, and preventing complications [6]. Although several strategies have been proposed and tested in practice [7], drugs are currently the mainstay of GERD treatment [8]. Among the available therapeutic agents, proton pump inhibitors (PPIs) have been demonstrated to have excellent mucosal healing and symptom relief because it strongly inhibits gastric acid secretion. Currently, PPIs are considered the most common first-line treatment for erosive esophagitis [9,10]. Unfortunately, approximately 20–40% of patients with mucosal erosions do not achieve mucosal healing or satisfactory symptom relief [11,12].
Some new acid inhibitors have been proposed and tested after PPIs. As a novel potassium-competitive acid blocker, vonoprazan (VPZ) can strongly inhibit H+, and K+ ATPase competitively and reversibly [13,14]. Compared with earlier PPIs, VPZ may have stronger and more sustained acid suppression but less variation in time to onset of action [15]. Several studies [14,16] have investigated the efficacy and safety of VPZ 20 mg (VPZ20) in treating GERD. Meanwhile, a recent meta-analysis concluded that VPZ20 is non-inferior to PPIs, or even more effective than PPIs, in patients with severe erosive esophagitis, with a similar safety profile [17].
In addition to the standard dose of 20 mg, multiple doses of VPZ are used in clinical practice, including 5 mg, 10 mg and 40 mg [18,19]. To date, only one study has directly compared all doses of VPZ in an individual study [18]. Therefore, it does not provide clinicians with conclusive information on the optimal dose for patients with erosive esophagitis. Fortunately, network meta-analysis enhances the strength of evidence by combining all available evidence [20]. Therefore, we performed this network meta-analysis, which combined direct and indirect evidence from all eligible studies, to compare the efficacy and safety of multiple doses of VPZ.
Methods
The present network meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension statement for reporting network meta-analysis [21]. Ethics approval and informed consent did not apply, as the statistical analysis was performed based on the published data.
Literature retrieval
A comprehensive literature retrieval was performed by two independent reviewers (Jie He and Yuanyuan Gao) in PubMed, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) to identify relevant randomized controlled trials (RCTs) from their inception until December 2021. The following terms and analogs were used to construct a basic search query following the PICOS principle: “erosive esophagitis” and “vonoprazan”. The detailed search strategies of three target English databases are shown in Supplementary Table 1. In addition, the reference lists of eligible studies and previous meta-analyses were screened as well. Disagreements were resolved by discussions between two reviewers (Jie He and Yuanyuan Gao) until a consensus was reached.
Selection criteria
Inclusion criteria for the present network meta-analysis included: (a) prospective RCTs; (b) patients with confirmed erosive esophagitis and aged ≥16 years; (c) PPIs administered at conventional doses as the control strategy; (d) VPZ was administered as the study strategy; and (e) 4- and 8-week endoscopic healing rates and treatment-emergent adverse events (TEAEs) were reported and data were applicable for statistical analysis. In addition, conference abstracts with sufficient data were also eligible for inclusion. Ineligible studies were excluded based on the following criteria: (a) duplicate reports that had insufficient data and relatively poor quality; (b) lack of data to conduct a network meta-analysis; (c) studies that did not report data for 4 or 8 weeks; and (d) animal studies, review papers, and observational studies.
Study selection
Two independent reviewers (Jie He and Yuanyuan Gao) selected eligible studies based on the following three-step selection criteria. First, duplicate studies were removed using the literature management software, namely EndNote (version X9, Clarivate Analytics). Second, irrelevant studies were excluded after screening the study title and abstract. Third, ineligible studies were further excluded by screening the full texts of the remaining studies. Disagreements were resolved by discussions between two reviewers (Jie He and Yuanyuan Gao) until a consensus was reached.
Data extraction
Two independent reviewers (Jie He and Yuanyuan Gao) extracted the following data from included studies: the name of the first author, country of study, year of publication, study design, condition of disease, comparison details, sample size (including the percentage of male patients), the number of patients with different severity grades which were defined according to Los Angeles (LA) classification system, age distribution, duration of treatment, and outcome details. If needed, missing data were added by emailing the corresponding author.
Outcome measures
We defined the 4-week endoscopic healing rate as a primary outcome, and 8-week endoscopic healing rate, the 4- and 8-week healing rate in patients with LA grades of C and D, and the incidence of TEAEs as secondary outcomes. Mucosal healing of erosive esophagitis was assessed endoscopically as “no mucosal breaks”, and endoscopic healing rate was defined as the percentage of patients with endoscopically confirmed mucosal healing. TEAEs were defined as undesirable medical symptoms or conditions that occurred throughout treatment.
Geometry of the evidence network
Network graphs were generated to show the evidence of the 4- and 8-week endoscopic healing rates and the TEAEs rate. Each node represented a treatment strategy in a single graph, and a solid line between two nodes indicated that two treatment strategies were directly compared in original studies. In general, the size of the nodes represented the cumulative sample size, and the thickness of the solid line represented the number of reports that directly compared one strategy to another [22].
Risk of bias assessment
Two independent reviewers (Jie He and Yuanyuan Gao) assessed the methodological quality of the included studies using the Cochrane risk of bias assessment tool (RoB) [23]. Seven items were involved, each item rated as “low”, “high”, or “unclear” risk of bias. The overall level of methodological quality was rated as “high” if seven items were judged to be at “low” risk of bias, as “low” if at least one of seven items was judged to be at “high” risk of bias, or as “moderate” if at least one judged to be at “unclear” risk of bias but none was judged to be at “high” risk of bias. Disagreements were resolved by discussions between two reviewers (Jie He and Yuanyuan Gao) until a consensus was reached.
Statistical analysis
In this network meta-analysis, all outcomes were dichotomous variables, so an odds ratio (OR) with a 95% credible interval (CrI) was used to express the magnitude of the pooled results. We assessed the transitivity across studies by reviewing the most clinical and methodological characteristics [24,25]. Second, global and local consistency tests were performed using the design-by-treatment interaction method (Wald test) [26] and the node-splitting method [27], respectively. Third, we evaluated the loop inconsistency by calculating the value of the τ2 statistic, which was also estimated using the node-splitting method [28,29]. However, we performed a random-effects network meta-analysis to determine the relative efficacy of different treatment strategies regardless of the level of statistical heterogeneity [30]. In addition, subgroup analysis was performed to investigate the role of various doses in patients diagnosed with severe erosive esophagitis (defined as C and D based on the LA classification system). Sensitivity analysis was also performed to examine the robustness of the primary outcome by excluding studies that included patients with refractory erosive esophagitis. Fourth, ranking probabilities were estimated to determine the relative ranking of targeted treatment strategies. The surface under the cumulative ranking (SUCRA) was also calculated for each strategy [31]. Finally, adjusted funnel plots were made to examine the risk of publication bias by visually inspecting the symmetry criterion. We generated comparison-adjusted funnel plots for the individual outcome for publication bias, with a symmetric plot indicating no publication bias [32]. Statistical analysis was performed using STATA 14.0 (StataCorp LP, College Station, Texas, USA) with the “network” command [33]. Furthermore, all results were presented graphically using the graphical tools developed by Chaimani et al. [34].
Results
Literature selection
A total of 134 studies were identified from the literature retrieval, including 129 studies from electronic databases and five studies from previous meta-analyses. First, 49 duplicate studies and 12 registered study protocols were removed. Then, based on the title and abstract, 56 irrelevant studies were excluded from the initial eligibility assessment. Finally, nine studies [6,18,19,35–40] were included in this network meta-analysis after excluding seven ineligible studies due to ineligible topics (n = 4), insufficient data (n = 2), and duplicate study (n = 1). The PRISMA flow diagram of study retrieval and selection is shown in Figure 1. Six treatment strategies, including VPZ 5 mg (VPZ5), VPZ 10 mg (VPZ10), VPZ 20 mg (VPZ20), VPZ 40 mg (VPZ40), LPZ 30 mg (LPZ30), and EPZ 20 mg (EPZ20) were identified. According to a previous network meta-analysis [41], LPZ30 was comparable to EPZ20 in 4- and 8-week endoscopic healing rates, so the combination of the two strategies was considered as a standard control group, named the PPI group. Network plots of 4- and 8-week endoscopic healing rates and the incidence of TEAEs are shown in Figure 2.
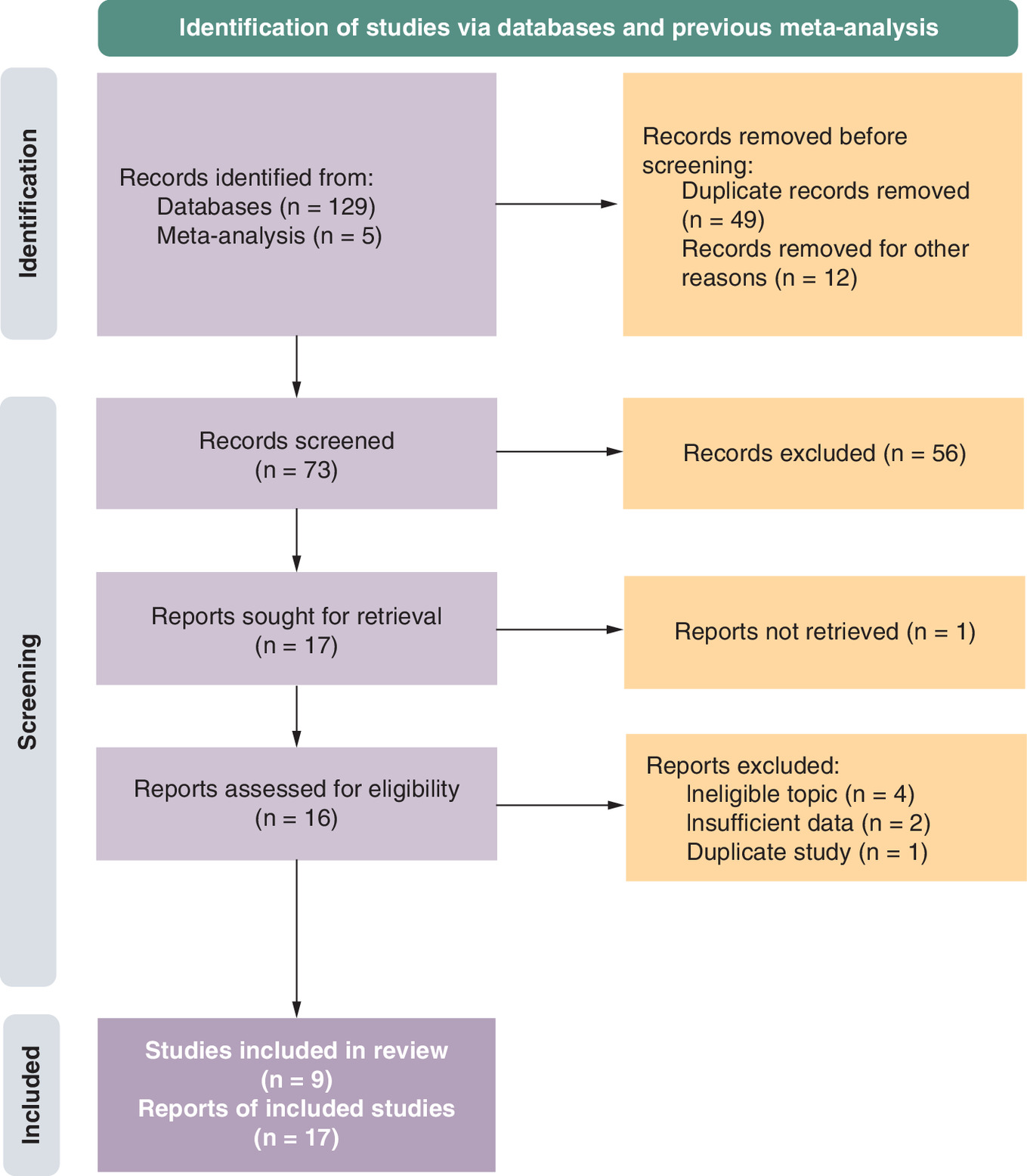
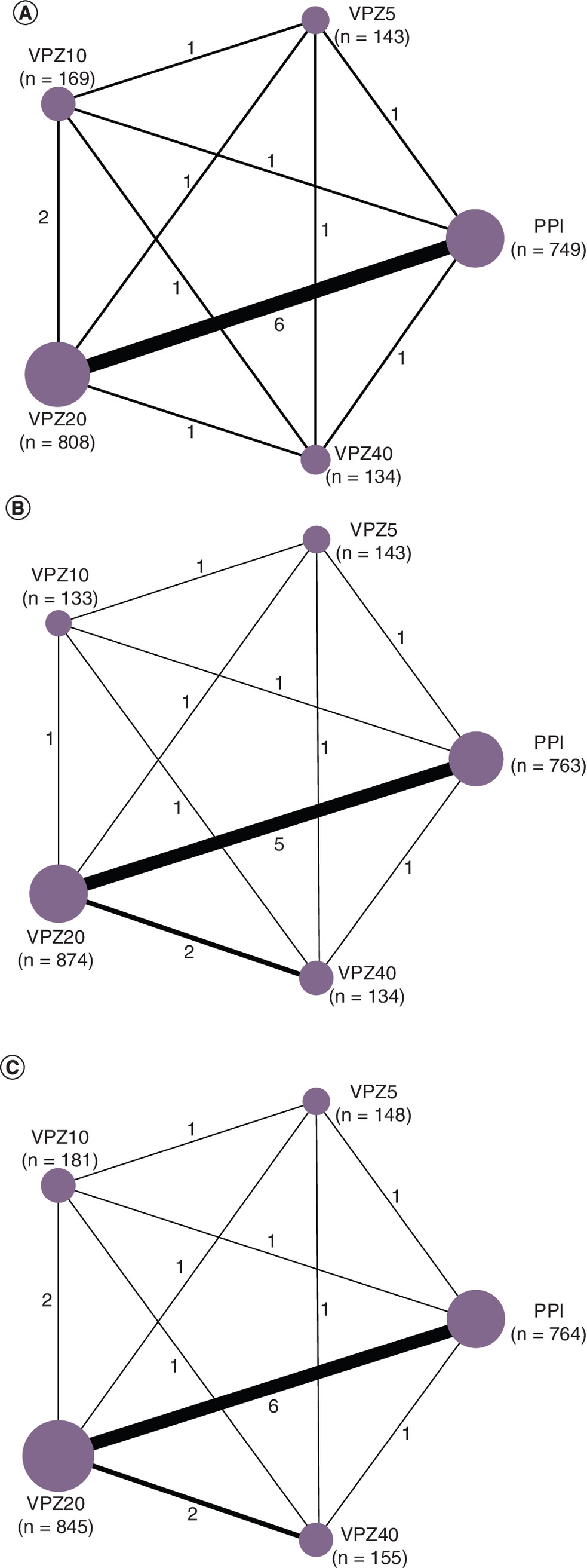
Figure 2. Network plots of the endoscopic healing rates at (A & B) 4 and 8 weeks and (C) treatment-emergent adverse events.
The size of each node is corresponding to the number of patients, and the thickness of each solid line between two nodes is corresponding to the number of direct comparisons.
PPI: Proton pump inhibitors; VPZ5: Vonoprazan 5 mg; VPZ10: Vonoprazan 10 mg; VPZ20: Vonoprazan 20 mg; VPZ40: Vonoprazan 40 mg; TEAEs: Treatment-emergent adverse events.
Study characteristics
All eligible studies were conducted in China (n = 3) [35,36,40] and Japan (n = 6) [6,18,19,37–39]. Most studies [6,18,19,35,38–40] recruited patients from multiple centers and two studies [36,37] recruited patients from a single center. Two studies [19,36] explicitly reported recruiting patients with refractory erosive esophagitis. Eight studies [6,19,35–40] were designed with two arms, but one was designed with multiple arms [18]. The mean age of the 2305 patients included in our network meta-analysis was 57.49 years, and the percentage of male patients was 63.98%. Additional baseline characteristics of the included studies are shown in Table 1.
| Study, year | Origin | Design | Condition | Comparison | Sample size | Male patients | Age, years | Patients with grade A/B (n) | Patients with grade C/D (n) | Treatment period |
|---|---|---|---|---|---|---|---|---|---|---|
| Ashida, et al., 2015 | Japan | Multi-center | EE | VPZ5 | 148 | 110 | 57.9 ± 12.9 | 88 | 55 | 8 weeks |
| VPZ10 | 145 | 113 | 57.3 ± 13.0 | 89 | 44 | |||||
| VPZ20 | 154 | 115 | 58.3 ± 13.8 | 94 | 50 | |||||
| VPZ40 | 146 | 114 | 57.6 ± 12.8 | 84 | 51 | |||||
| LPZ30 | 140 | 99 | 55.8 ± 13.9 | 86 | 47 | |||||
| Ashida, et al., 2016 | Japan | Multi-center | EE | VPZ20 | 207 | 137 | 58.3 ± 13.8 | 132 | 75 | 8 weeks |
| LPZ30 | 202 | 154 | 57.4 ± 13.2 | 129 | 73 | |||||
| Chen, et al., 2018 | China | Multi-center | EE | VPZ20 | 142 | 105 | 51.8 ± 13.7 | 89 | 54 | 8 weeks |
| LPZ30 | 133 | 110 | 51.5 ± 12.5 | 85 | 46 | |||||
| Xiao, et al., 2020 | China | Multi-center | EE | VPZ20 | 244 | 176 | 54.1 ± 13.2 | 168 | 76 | 8 weeks |
| LPZ30 | 237 | 179 | 53.8 ± 12.5 | 167 | 68 | |||||
| Okanobu, et al., 2021 | Japan | Single-center | EE | VPZ10 | 36 | 24 | 62 (38–83) | 29 | 7 | 4 weeks |
| VPZ20 | 37 | 26 | 69 (35–85) | 28 | 9 | |||||
| Iwakiri, et al., 2017 | Japan | Multi-center | Refractory EE | VPZ20 | 9 | 5 | 73.8 ± 7.5 | 2 | 3 | 8 weeks |
| VPZ40 | 10 | 3 | 71.2 ± 10.5 | 6 | 2 | |||||
| Huang, et al., 2021 | China | Single-center | Refractory EE | VPZ20 | 30 | 14 | 44.3 ± 16.4 | 10 | 20 | 4 weeks |
| EPZ20 | 30 | 17 | 45.5 ± 17.3 | 12 | 18 | |||||
| Uemura, et al., 2019 | Japan | Multi-center | EE | VPZ20 | 139 | n.a. | n.a. | n.a. | n.a. | 8 weeks |
| LPZ30 | 69 | n.a. | n.a. | n.a. | n.a. | |||||
| Sakurai, et al., 2019 | Japan | Multi-center | EE | VPZ20 | 22 | 6 | 58.0 ± 13.8 | 10 | 3 | 4 weeks |
| EPZ20 | 25 | 10 | 54.7 ± 13.2 | 9 | 3 |
EE: Erosive esophagitis; EPZ: Esomeprazole; LPZ: Lansoprazole; n.a.: Not applicable; VPZ: Vonoprazan.
Risk of bias of eligible studies
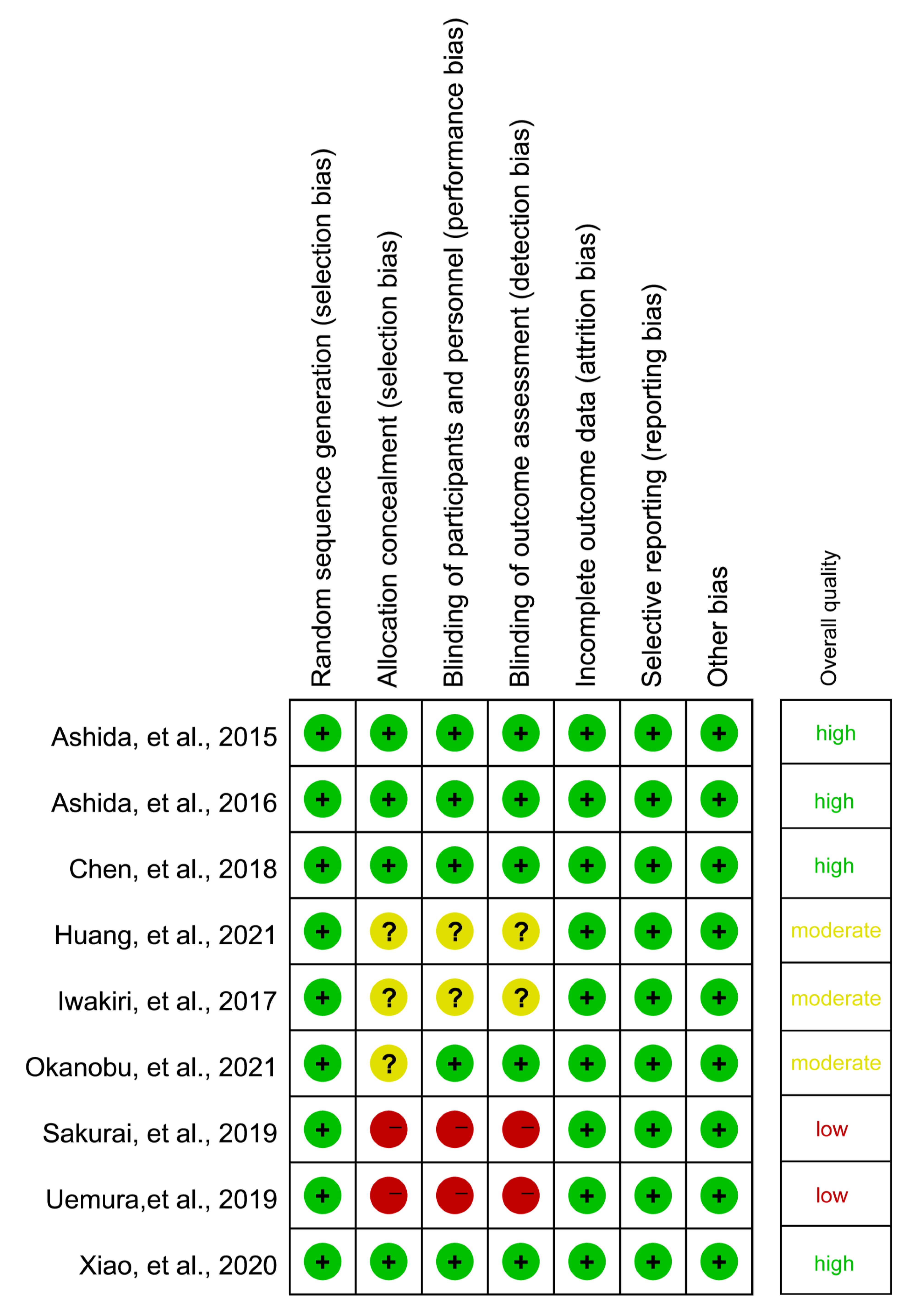
Details of the risk of bias assessment are shown in Supplementary Figure 1. All studies [6,18,19,35–40] reported methods to generate random sequences, but only four studies [6,18,35,40] used appropriate methods to perform allocation concealment. Two studies [38,39] were judged to be high risk in allocation concealment, and blinding of participants, personnel, and outcome assessors due to the open-label study design. All studies were judged to be low risk for the remaining three items. Overall, in terms of the overall methodological quality, two studies were rated as “low” level, three studies as “moderate” level, and four studies as “high” level.
Meta-analysis of the endoscopic healing rate
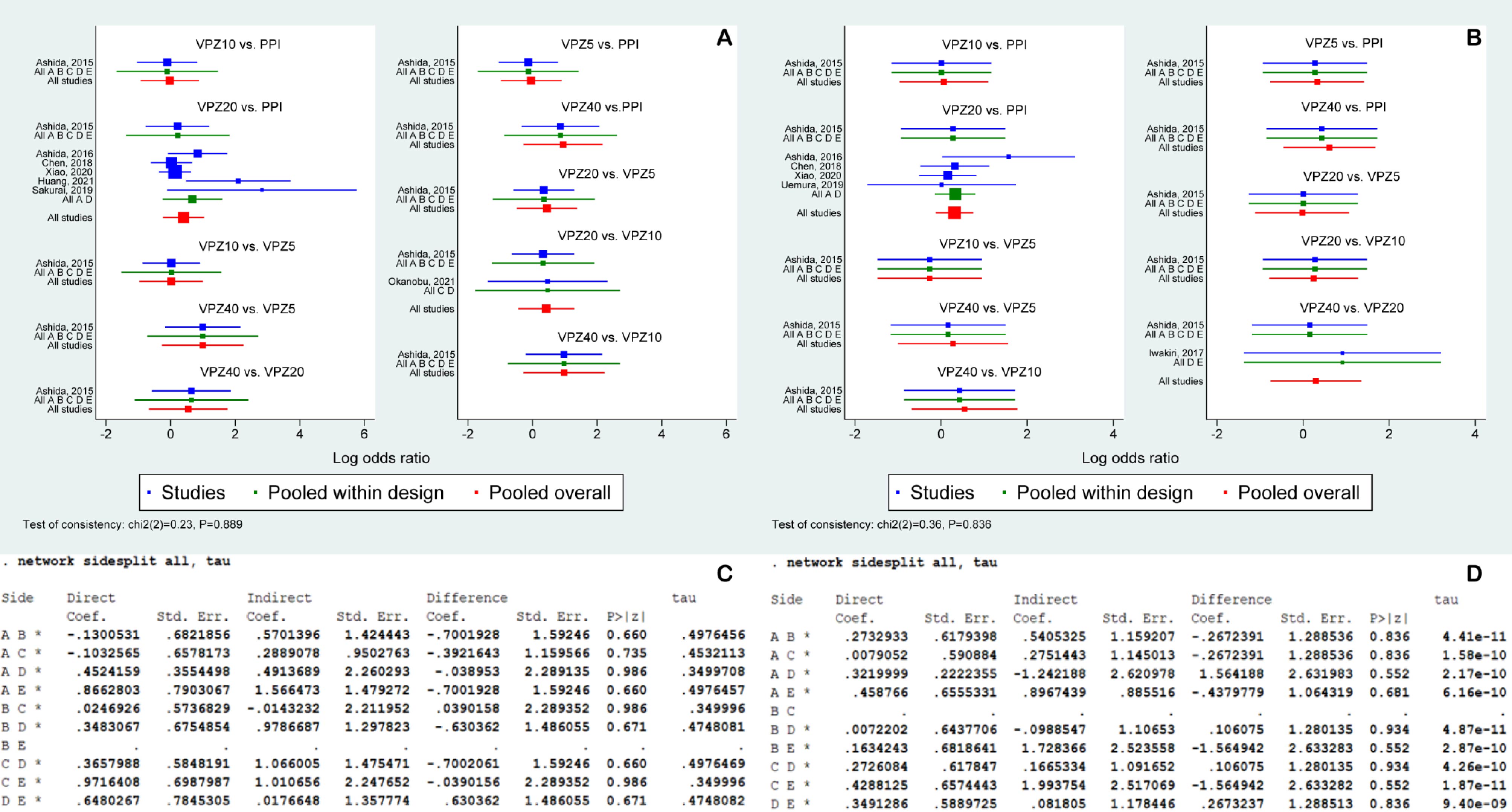
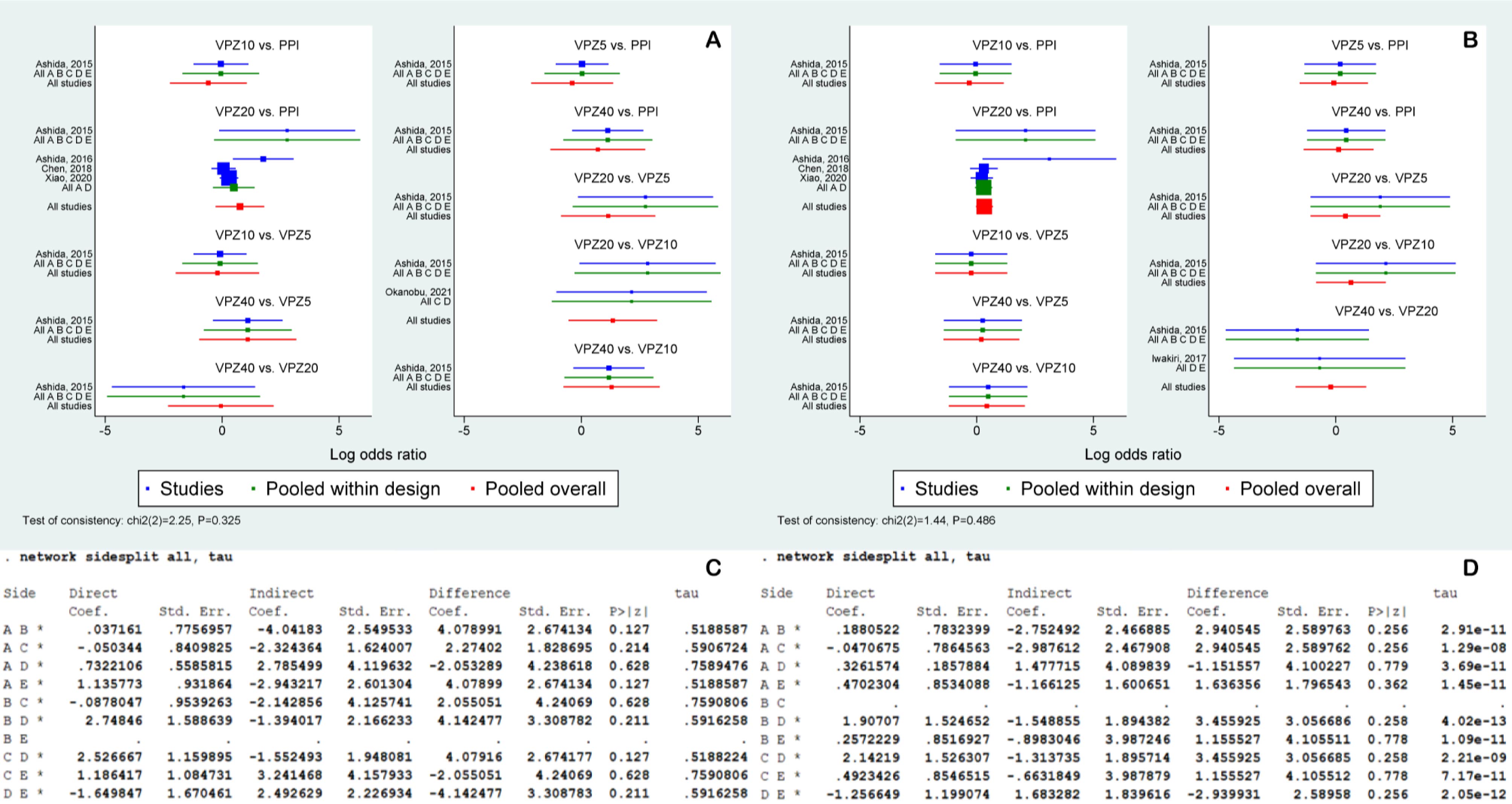
A total of seven [6,18,35–38,40] and six [6,18,19,35,39,40] studies reported endoscopic healing rates at 4 and 8 weeks, respectively. As shown in Supplementary Figure 2, no significant inconsistency was identified for outcomes at 4 and 8 weeks by the global inconsistency test (A and B) and the node-split test (C and D). Meanwhile, as shown in Supplementary Figure 3, the loop-specific inconsistency test did not detect inconsistency for all closed loops of the endoscopic healing rates at 4 (A) and 8 (B) weeks. Therefore, the consistency model was used to estimate the relative efficacy of different treatment strategies. As shown in Figure 3, the pooled results show that patients receiving VPZ20 or VPZ40 had comparable healing rates at 4 (A) and 8 (C) weeks to those receiving PPI, VPZ5, or VPZ10. However, SUCRA suggested that VPZ40 had the highest probability of being best in mucosal healing rate at 4 weeks (B) (93.0%), followed by VPZ20 (67.8%), PPI (33.5%), VPZ10 (28.5%), and VPZ5 (27.3%), and VPZ40 had the largest probability of being best in healing rate at 8 weeks (D) (75.9%), followed by VPZ20 (59.1%), VPZ5 (55.9%), VPZ10 (35.0%), and PPI (24.1%).
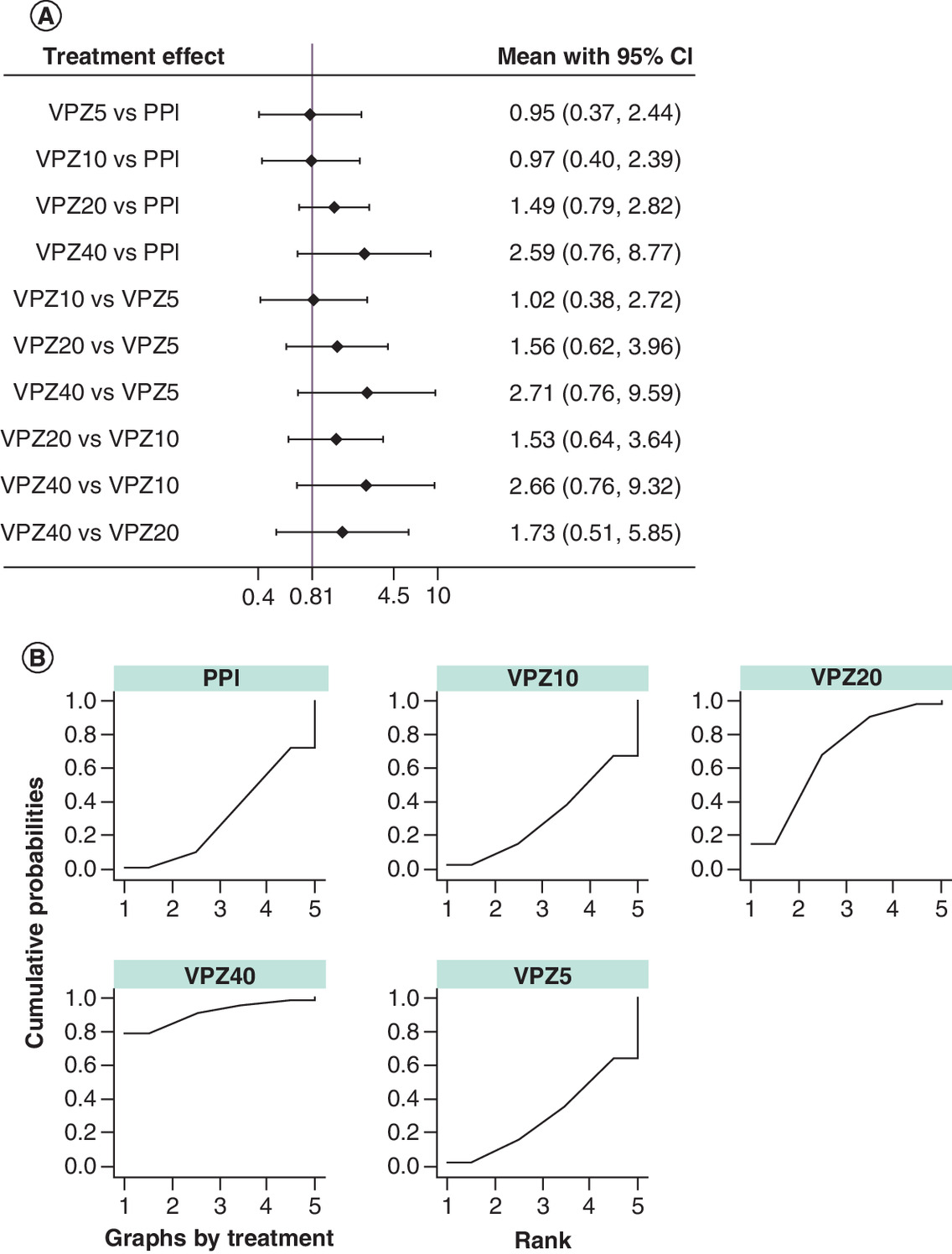
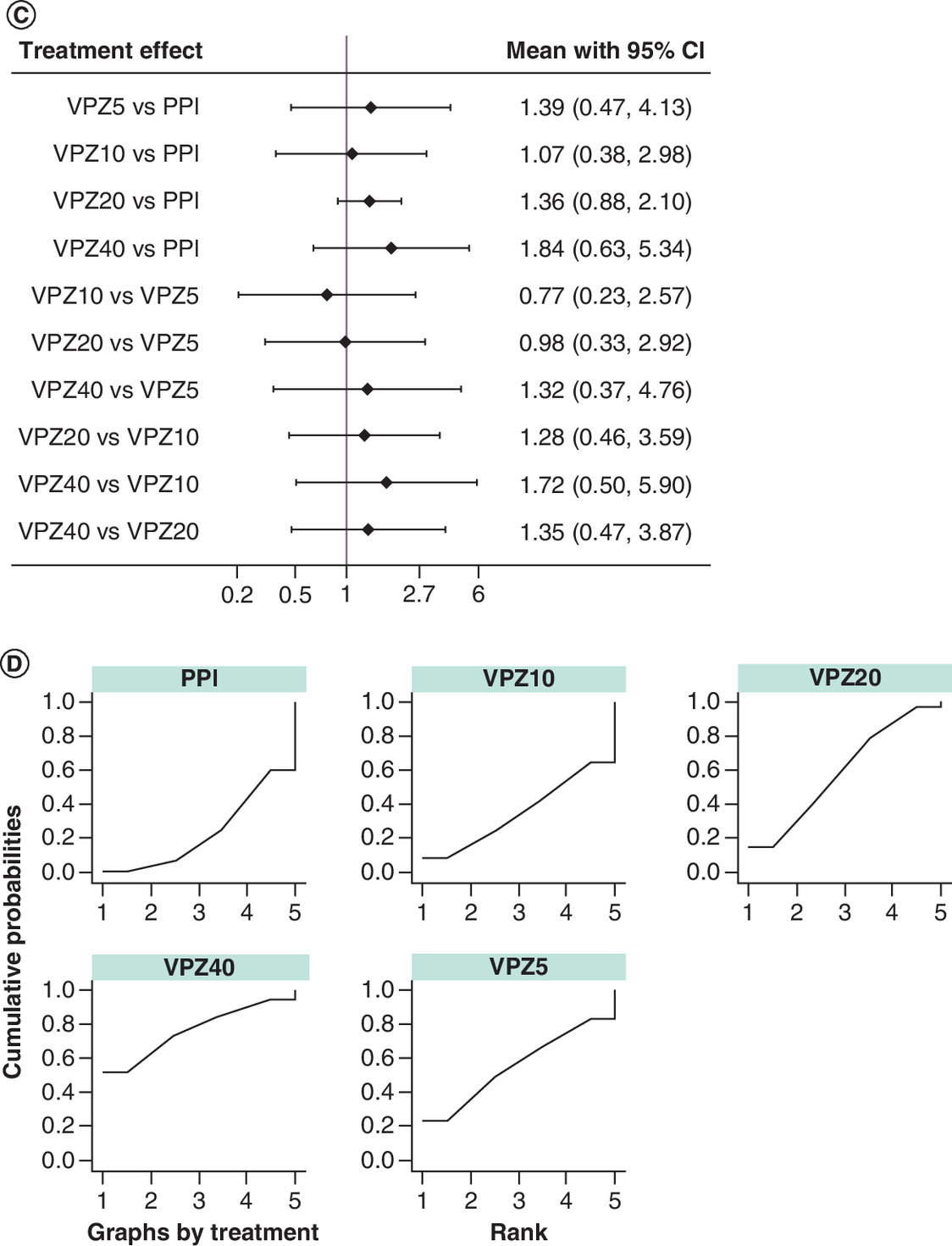
Figure 3. Relative efficacy and SUCRA of the endoscopic healing rates at (A & B) 4 and (C & D) 8 weeks.
PPI: Proton pump inhibitors; VPZ5: Vonoprazan 5 mg; VPZ10: Vonoprazan 10 mg; VPZ20: Vonoprazan 20 mg; VPZ40: Vonoprazan 40 mg; TEAEs: Treatment-emergent adverse events; SUCRA: Surface under the cumulative ranking.
Subgroup analysis of the endoscopic healing rate
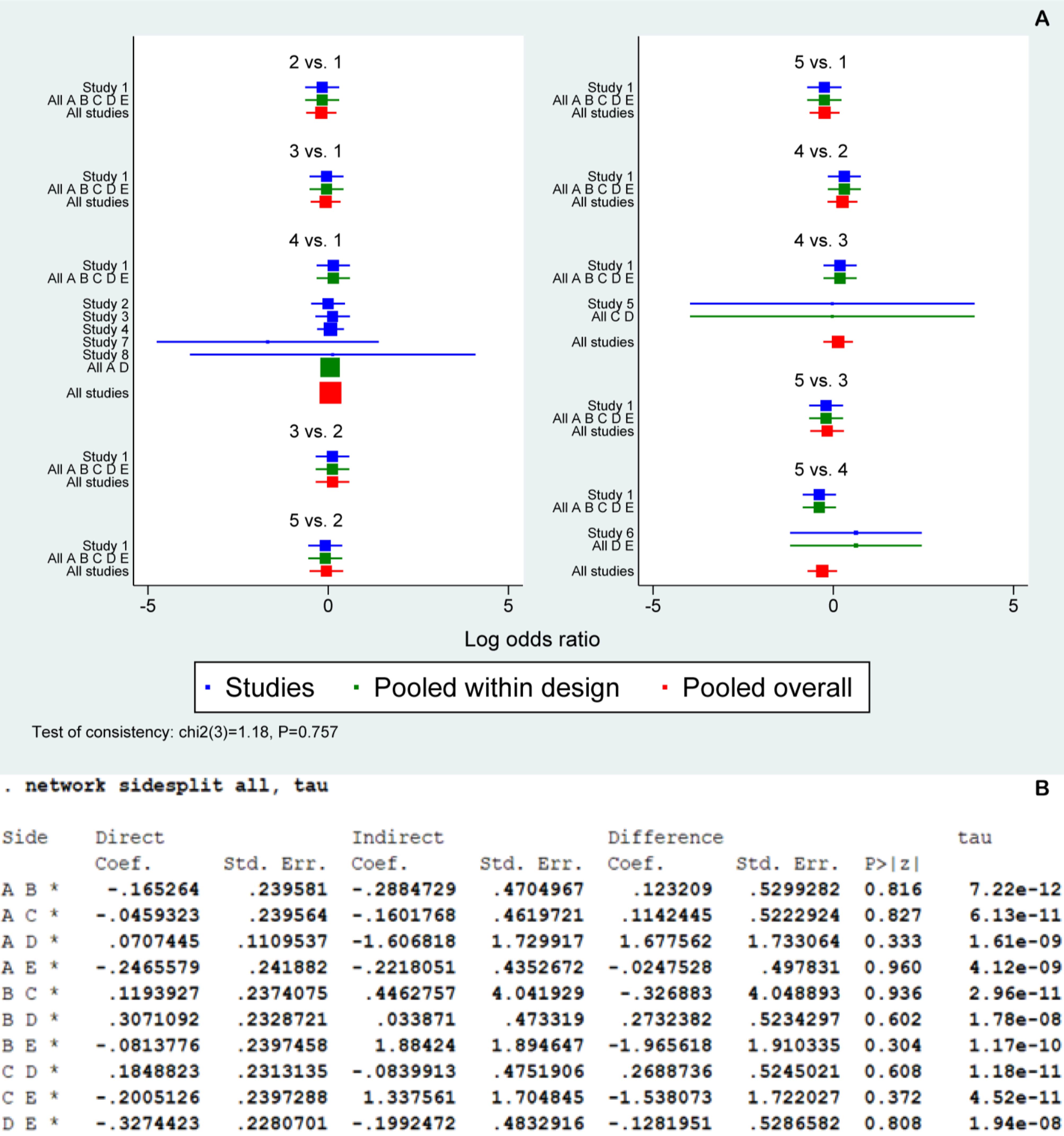
A total of five [6,18,35,37,40] and five [6,18,19,35,40] studies reported the endoscopic healing rate at 4 and 8 weeks in patients with severe erosive esophagitis, respectively. As shown in Supplementary Figure 4, no significant inconsistency was identified for outcomes at 4 and 8 weeks by the global inconsistency test (A and B) and the node-split test (C and D). Meanwhile, as shown in Supplementary Figure 3, the loop-specific inconsistency test did not detect inconsistency for all closed loops of the endoscopic healing rate at 4 (C) and 8 (D) weeks. We selected a consistency model to estimate the relative efficacy of different treatment strategies. As shown in Figure 4, the pooled results suggested comparable mucosal healing rates between different treatment strategies at both 4 (A) and 8 (C) weeks. However, SUCRA results told that VPZ20 had the largest probability of being the best healing rate at 4 weeks (B) (80.7%), followed by VPZ40 (74.6%), PPI (43.5%), VPZ5(30.7%), and VPZ10 (20.6%), and VPZ20 had the largest probability of being the best in healing rate at 8 weeks (D) (76.8%), followed by VPZ40 (56.9%), VPZ5(43.9%), PPI (41.9%), and VPZ10 (30.5%).
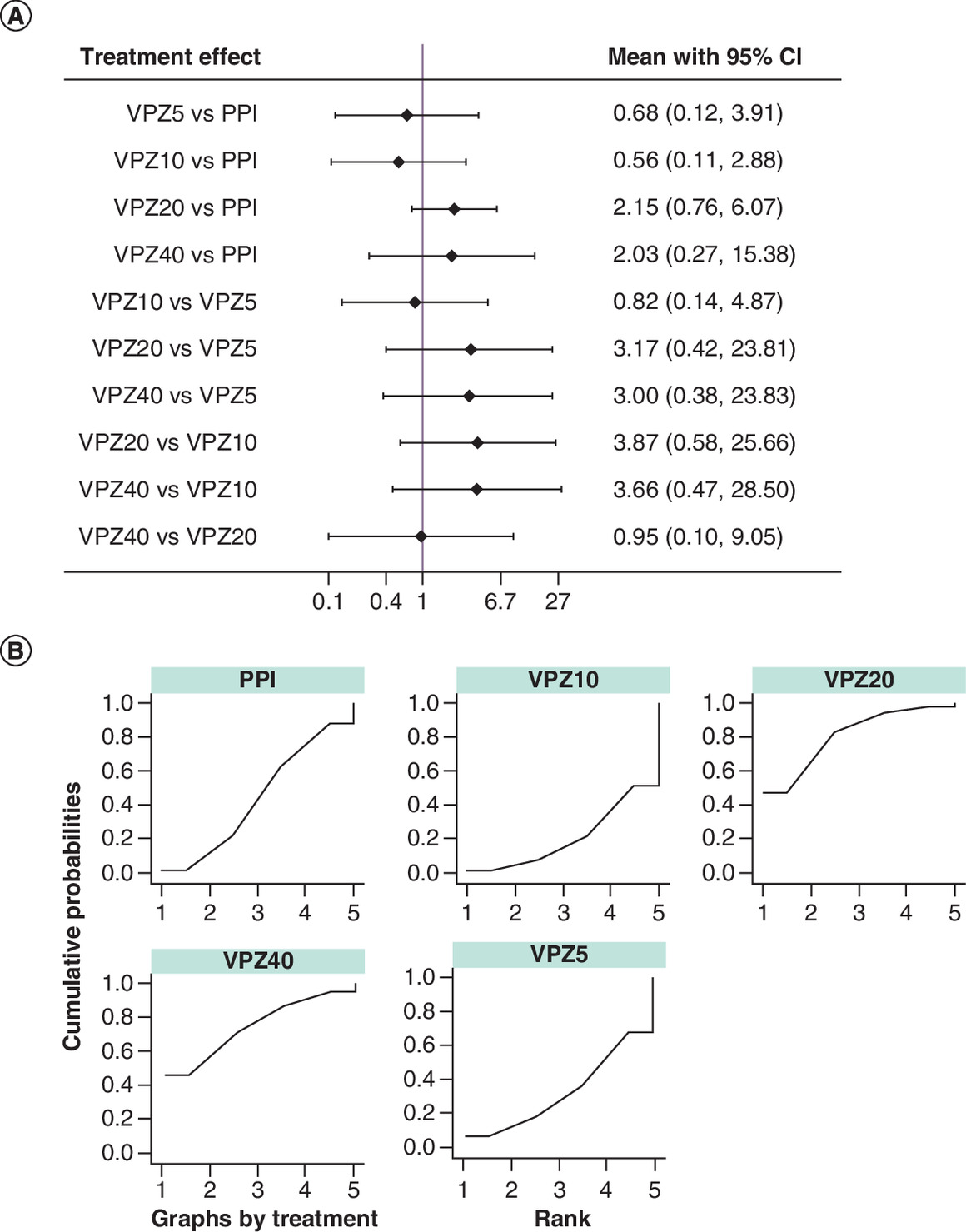
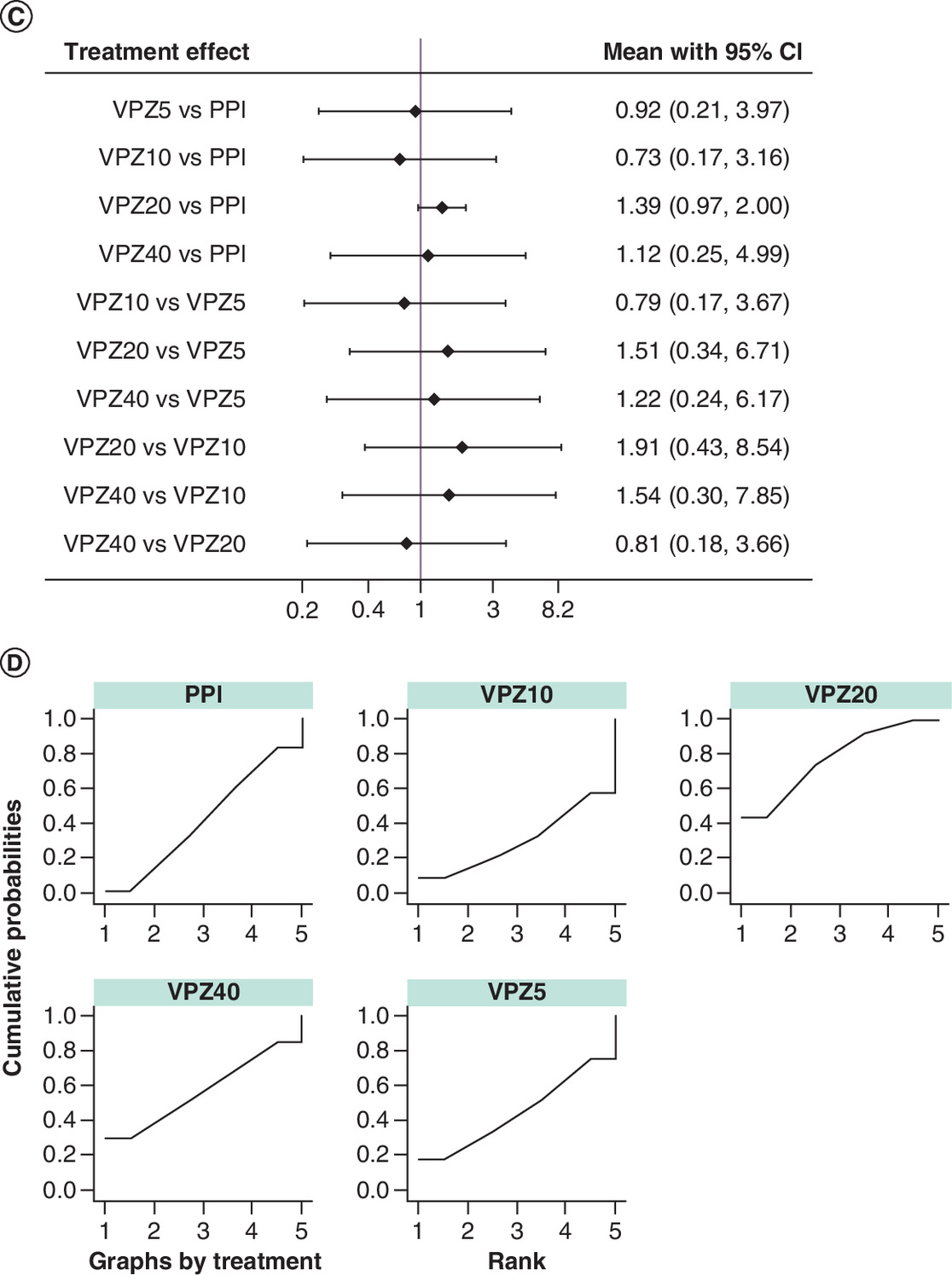
Figure 4. Relative efficacy and SUCRA of the endoscopic healing rates among patients with grade C/D at (A & B) 4 and (C & D) 8 weeks.
PPI: Proton pump inhibitors; VPZ5: Vonoprazan 5 mg; VPZ10: Vonoprazan 10 mg; VPZ20: Vonoprazan 20 mg; VPZ40: Vonoprazan 40 mg; TEAEs: Treatment-emergent adverse events; SUCRA: The surface under the cumulative ranking.
Meta-analysis of the incidence of TEAEs
A total of eight studies [6,18,19,35–38,40] were analyzed in this network. As shown in Supplementary Figure 5, no significant inconsistency was identified by the global inconsistency test (A) and the node-split test (B). Meanwhile, as presented in Supplementary Figure 3, the loop-specific inconsistency test did not detect inconsistency for all closed loops (E). Therefore, the consistency model was used to estimate the comparative safety of different treatment strategies. As shown in Figure 5, the pooled results suggested no statistical difference in TEAEs rate between different treatment strategies, although the results of SUCRA suggested that n VPZ40 ranked best (49.1%), followed by VPZ5 (33.7%), VPZ10 (29.8%), PPI (39.4%), and VPZ20 (50.3%).

Figure 5. (A) Relative efficacy and (B) SUCRA of treatment-emergent adverse events during treatment.
PPI: Proton pump inhibitors; VPZ5: Vonoprazan 5 mg; VPZ10: Vonoprazan 10 mg; VPZ20: Vonoprazan 20 mg; VPZ40: Vonoprazan 40 mg; TEAEs: Treatment-emergent adverse events; SUCRA: Surface under the cumulative ranking.
Sensitivity analysis & publication bias
For the primary outcome, as shown in Supplementary Figure 6, sensitivity analysis confirmed the robustness of the pooled results after excluding two studies that included only patients with refractory erosive esophagitis. Small study effects for individual outcomes were examined using adjusted funnel plots. As shown in Supplementary Figure 7, assumptions of small study effects were established for the endoscopic healing rate at 4 and 8 weeks and the incidence of TEAEs throughout treatment because all funnel plots were visually inspected to be asymmetric.
Discussion
GERD has become a prevalent gastrointestinal disorder worldwide, often leading to the development of erosive esophagitis [5]. Currently, PPIs remain the most common first-line therapeutic agents for esophageal mucosal healing and symptom control in patients with erosive esophagitis [7,42,43]. However, multiple doses may be needed to achieve maximal acid suppression and symptom improvement because many PPIs have a slow and cumulative onset of action [44]. Fortunately, as a new potassium-competitive acid blocker, VPZ has more rapid, potent, and sustained acid inhibition than conventional PPIs [13,15]. The non-inferiority of VPZ to PPIs in mucosal healing rate in erosive esophagitis has been demonstrated in a previous meta-analysis [17]. However, it's difficult to determine the optimal dose because the relative efficacy of multiple doses of VPZ has only been investigated in a single study [18]. In the current network meta-analysis, nine eligible studies, including 2305 patients, were included, and the pooled results showed no statistical differences for all comparisons in terms of all outcomes. However, based on SUCRA results, VPZ40 ranked first for the endoscopic healing rate and TEAEs in patients with erosive esophagitis, and VPZ20 ranked worst for the incidence of TEAEs.
To date, only one pair-wise meta-analysis [17] has been performed to investigate the efficacy and safety of a standard dose of VPZ compared with PPIs in the treatment of GERD. In this meta-analysis of six eligible studies, the non-inferiority of the standard VPZ dose (VPZ20) was demonstrated compared with PPIs. In addition, patients with severe erosive esophagitis obtained more benefits from VPZ20, reporting a safety profile comparable to PPIs. Compared with this meta-analysis, the present study consistently confirmed the non-inferiority of VPZ20 in treating erosive esophagitis with similar safety compared with PPIs. However, our network meta-analysis could not confirm the inferiority of VPZ20 in patients with severe erosive esophagitis. It should be noted that previous meta-analysis has simultaneously included data from different time points into a separate quantitative synthesis, significantly increasing the bias caused by the analysis unit error. In contrast, our network meta-analysis investigated the efficacy of all strategies separately according to different time points, which significantly increased the reliability of the pooled results. In addition, our network meta-analysis also ranked different doses of VPZ after determining their relative efficacy, providing clinicians with more practical recommendations for decision-making.
The current network meta-analysis has several strengths: (a) the main methodological advantage is the use of a comprehensive literature retrieval strategy that allows us to identify more eligible studies, (b) the network meta-analysis allows us to estimate the relative efficacy of different doses of VPZ by combining direct and indirect evidence, (c) the SUCRA method was used to rank all treatment strategies, which benefits to select the optimal strategy in clinical practice, and (d) the overall methodological quality of each study was quantified using the Cochrane risk of bias assessment method, which incorporated the level of evidence into pooled results for decision-making.
We must acknowledge that our pooled results should also be interpreted with caution due to several limitations as follows: (a) a small study effect was detected for all outcomes based on asymmetric funnel plots, which may introduce some bias for our pooled results; (b) the limited number of eligible studies with limited sample size was included in this network meta-analysis, which may have a significantly negative influence on the robustness of the pooled results; (c) All studies were conducted in Asian countries, including Japan and China, and therefore our findings should be generalized with caution before further validation in other ethnic groups. More specifically, as differences in drug metabolism between ethnic groups have been demonstrated in many studies, additional studies should be conducted to assess the role of Vonoprazan in Caucasian patients. (d) two studies enrolled patients who were confirmed refractory erosive esophagitis, but sensitivity analysis was performed to confirm the robustness of the pooled results.
Conclusion
In conclusion, multiple doses of VPZ are comparable in efficacy and safety, but VPZ40 may come out on top in effectiveness and safety. More studies are also required to validate our findings further because this network meta-analysis has several limitations. In addition, more studies should be conducted to evaluate the role of Vonoprazan in Caucasian patients because there are differences in metabolic speed between Asians and Caucasians.
Expert opinion
With the great advancement of diagnostic techniques, gastroesophageal reflux disease (GERD) has become one of the most common gastrointestinal diseases that could be easily and effectively diagnosed. By its definition, GERD is thought to be the result of the retrograde flow of gastric contents into the esophagus. More specifically, GERD is characterized by troublesome symptoms and complications such as heartburn and acid regurgitation.
From the perspective of endoscopic results, GERD can be divided into two subtypes: non-erosive reflux disease and erosive esophagitis. In both subtypes, erosive esophagitis is defined as endoscopy-proven erosion of the esophageal mucosa, and patients reported distressing symptoms such as heartburn. Compared with non-erosive esophagitis, treating erosive esophagitis caused by mucosal injury requires more effective therapeutic strategies.
Traditionally, three essential aspects are especially emphasized in treating erosive esophagitis under the consideration of the pathology of this condition, including relieving symptoms, accelerating esophageal mucosal healing, and preventing complications. Based on these three aspects, a series of therapeutic strategies have been developed and then used in route practice. However, medication is still the mainstay of GERD treatment.
Among the current therapeutic agents, proton pump inhibitors (PPIs) have been extensively used for the treatment of GERD. The effectiveness and safety of PPIs have also been clearly demonstrated in accelerating esophageal mucosal healing and relieving symptoms because PPIs can strongly inhibit the secretion of gastric acid. As a result, PPIs have also been considered the most common first-line therapeutic agent for treating erosive esophagitis in clinical practice. It's regrettable that, approximately 20–40% of patients do not achieve satisfactory therapeutic effects because mucosal erosions do not reach mucosal healing or satisfactory symptom relief.
Because some patients could not benefit from PPIs, many novel acid-inhibitory agents have been developed and routinely used in practice. Among the available new potassium-competitive acid blockers, vonoprazan (VPZ) has been found to strongly inhibit H+, and K+ ATPase in a competitive and reversible manner. Compared with early-generation PPIs, VPZ may have stronger and more sustained acid suppression but less variation in time to onset of action. It's exciting that the efficacy and safety of VPZ 20 mg (VPZ20) in the treatment of GERD have been clearly demonstrated in several clinical studies. More importantly, a recent meta-analysis also suggested that VPZ20 is non-inferior to PPIs and even more effective than PPIs for patients with severe erosive esophagitis, with a similar safety profile. VPZ20 may become a preferred therapeutic agent in the treatment of erosive esophagitis.
It must be noted that, except for the standard dose of 20 mg, VPZ has also been prescribed for the treatment of erosive esophagitis in different doses in clinical practice, including 5 mg, 10 mg and 40 mg, which greatly confound practitioners to make a clinical decision in route practice effectively. More importantly, despite this confusion, only one study directly compared all dosages of VPZ in an individual study. Considering these facts, the present study comprehensively investigated the comparative efficacy and safety of available doses of VPZ with network meta-analysis technology on the basis of available evidence.
Based on these findings from this network meta-analysis, different doses of VPZ are comparable in efficacy and safety, but VPZ40 may come out on top in both efficacy and safety. Nevertheless, we suggest more studies to further directly compare various doses of VPZ due to only limited evidence in this network meta-analysis. In addition, more studies should be conducted to evaluate the role of Vonoprazan in Caucasian patients because there are differences in metabolic speed between Asians and Caucasians.
Summary points
•
Vonoprazan is effective for treating erosive esophagitis.
•
Multiple doses of vonoprazan are available in routine practice.
•
It is unclear which doses of vonoprazan may be best for erosive esophagitis.
•
Nine studies involving 2305 patients were included in this network meta-analysis.
•
Different doses of vonoprazan were comparable in efficacy and safety.
•
Vonoprazan 20 mg and 40 mg were comparable to PPI in healing rate.
•
Vonoprazan 40 mg ranked best for healing rate and treatment-emergent adverse events.
•
Vonoprazan 20 mg ranked worst for treatment-emergent adverse events.
Author contributions
Substantially contributed to conception or design: Y Sun, J He. Contributed to acquisition, analysis, or interpretation of data: J He. Drafted the manuscript for important content: J He, Y Gao. Critically revised the manuscript for important intellectual content: G Bai, J Wang. Gave final approval: all authors.
Acknowledgments
The authors appreciate all authors who performed all eligible studies which have been included in the present network meta-analysis.
Financial & competing interests disclosure
This work was supported by National Nature Science Foundation of China under Grant NO.81874402 and NO.82174128. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Data availability statement
All data generated or analyzed during this study are included in this published article/as supplementary information files.
Supplementary Material
File (supplementary figure 1.jpg)
- Download
- 821.22 KB
{kind=link}
File (supplementary figure 2.jpg)
- Download
- 687.49 KB
{kind=link}
File (supplementary figure 3.jpg)
- Download
- 804.38 KB
{kind=link}
File (supplementary figure 4.jpg)
- Download
- 636.38 KB
{kind=link}
File (supplementary figure 5.jpg)
- Download
- 775.37 KB
{kind=link}
File (supplementary figure 6.jpg)
- Download
- 224.50 KB
{kind=link}
File (supplementary figure 7.jpg)
- Download
- 145.32 KB
{kind=link}
File (supplementary table 1.docx)
- Download
- 20.38 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am. J. Gastroenterol. 101(8), 1900–1920; quiz 43 (2006).
2.
Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli F, Ford AC. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut 67(3), 430–440 (2018).
3.
Savarino E, de Bortoli N, De Cassan C et al. The natural history of gastro-esophageal reflux disease: a comprehensive review. Dis. Esophagus 30(2), 1–9 (2017).
4.
Altomare A, Guarino MP, Cocca S, Emerenziani S, Cicala M. Gastroesophageal reflux disease: update on inflammation and symptom perception. World J. Gastroenterol. 19(39), 6523–6528 (2013).
5.
Goh KL. Gastroesophageal reflux disease in Asia: a historical perspective and present challenges. J. Gastroenterol. Hepatol. 26(Suppl. 1), 2–10 (2011).
6.
Ashida K, Sakurai Y, Hori T et al. Randomised clinical trial: vonoprazan, a novel potassium-competitive acid blocker, vs. lansoprazole for the healing of erosive oesophagitis. Aliment. Pharmacol. Ther. 43(2), 240–251 (2016).
• Vonoprazan was not inferior to lansoprazole in erosive oesophagitis, and in the long-term maintenance study, vonoprazan was well tolerated and effective.
7.
Moraes-Filho JP, Navarro-Rodriguez T, Barbuti R, Eisig J, Chinzon D, Bernardo W. Guidelines for the diagnosis and management of gastroesophageal reflux disease: an evidence-based consensus. Arq. Gastroenterol. 47(1), 99–115 (2010).
8.
Fuchs KH, Babic B, Breithaupt W et al. EAES recommendations for the management of gastroesophageal reflux disease. Surg. Endosc. 28(6), 1753–1773 (2014).
9.
Iwakiri K, Kinoshita Y, Habu Y et al. Evidence-based clinical practice guidelines for gastroesophageal reflux disease 2015. J. Gastroenterol. 51(8), 751–767 (2016).
10.
Hungin AP, Hill C, Molloy-Bland M, Raghunath A. Systematic review: patterns of proton pump inhibitor use and adherence in gastroesophageal reflux disease. Clin. Gastroenterol. Hepatol. 10(2), 109–116 (2012).
11.
Richter JE, Kahrilas PJ, Johanson J et al. Efficacy and safety of esomeprazole compared with omeprazole in GERD patients with erosive esophagitis: a randomized controlled trial. Am. J. Gastroenterol. 96(3), 656–665 (2001).
12.
Mizuno H, Matsuhashi N, Sakaguchi M et al. Recent effectiveness of proton pump inhibitors for severe reflux esophagitis: the first multicenter prospective study in Japan. J. Clin. Biochem. Nutr. 57(3), 233–238 (2015).
13.
Hori Y, Matsukawa J, Takeuchi T, Nishida H, Kajino M, Inatomi N. A study comparing the antisecretory effect of TAK-438, a novel potassium-competitive acid blocker, with lansoprazole in animals. J. Pharmacol. Exp. Ther. 337(3), 797–804 (2011).
14.
Matsukawa J, Hori Y, Nishida H, Kajino M, Inatomi N. A comparative study on the modes of action of TAK-438, a novel potassium-competitive acid blocker, and lansoprazole in primary cultured rabbit gastric glands. Biochem. Pharmacol. 81(9), 1145–1151 (2011).
15.
Kondo M, Kawamoto M, Hasuoka A, Kajino M, Inatomi N, Tarui N. High-throughput screening of potassium-competitive acid blockers. J. Biomol. Screen. 17(2), 177–182 (2012).
16.
Hoshino S, Kawami N, Takenouchi N et al. Efficacy of vonoprazan for proton pump inhibitor-resistant reflux esophagitis. Digestion 95(2), 156–161 (2017).
17.
Cheng Y, Liu J, Tan X et al. Direct comparison of the efficacy and safety of vonoprazan versus proton-pump inhibitors for gastroesophageal reflux disease: a systematic review and meta-analysis. Dig. Dis. Sci. 66(1), 19–28 (2021).
•• Vonoprazan was non-inferior to PPIs as therapy for patients with gastroesophageal reflux disease, and vonoprazan was more effective than PPIs for patients with severe erosive esophagitis.
18.
Ashida K, Sakurai Y, Nishimura A et al. Randomised clinical trial: a dose-ranging study of vonoprazan, a novel potassium-competitive acid blocker, vs. lansoprazole for the treatment of erosive oesophagitis. Aliment. Pharmacol. Ther. 42(6), 685–695 (2015).
• Vonoprazan 20 mg or higher was highly efficacious for severe erosive oesophagitis.
19.
Iwakiri K, Sakurai Y, Shiino M et al. A randomized, double-blind study to evaluate the acid-inhibitory effect of vonoprazan (20 mg and 40 mg) in patients with proton-pump inhibitor-resistant erosive esophagitis. Therap. Adv. Gastroenterol. 10(6), 439–451 (2017).
• Vonoprazan 20 mg and 40 mg effectively resulted in an erosive esophagitis healing rate of more than 60.0%.
20.
Dias S, Caldwell DM. Network meta-analysis explained. Arch. Dis. Child. Fetal Neonatal Ed. 104(1), F8–F12 (2019).
21.
Hutton B, Salanti G, Caldwell DM et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162(11), 777–784 (2015).
22.
Salanti G, Ades AE, Ioannidis JP. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J. Clin. Epidemiol. 64(2), 163–171 (2011).
23.
Higgins JP, Altman DG, Gotzsche PC et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343, d5928 (2011).
24.
Cipriani A, Higgins JP, Geddes JR, Salanti G. Conceptual and technical challenges in network meta-analysis. Ann. Intern. Med. 159(2), 130–137 (2013).
25.
Salanti G. Indirect and mixed-treatment comparison, network, or multiple-treatments meta-analysis: many names, many benefits, many concerns for the next generation evidence synthesis tool. Res. Synth. Methods 3(2), 80–97 (2012).
26.
Tu YK. Using generalized linear mixed models to evaluate inconsistency within a network meta-analysis. Value Health 18(8), 1120–1125 (2015).
27.
Higgins JP, Jackson D, Barrett JK, Lu G, Ades AE, White IR. Consistency and inconsistency in network meta-analysis: concepts and models for multi-arm studies. Res. Synth. Methods 3(2), 98–110 (2012).
28.
Yu-Kang T. Node-splitting generalized linear mixed models for evaluation of inconsistency in network meta-analysis. Value Health 19(8), 957–963 (2016).
29.
Lu G, Ades AE. Assessing evidence inconsistency in mixed treatment comparisons. J. Am. Stat. Assoc. 101(474), 447–459 (2006).
30.
Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat. Med. 23(20), 3105–3124 (2004).
31.
Mbuagbaw L, Rochwerg B, Jaeschke R et al. Approaches to interpreting and choosing the best treatments in network meta-analyses. Syst. Rev. 6(1), 79 (2017).
32.
Sterne JA, Egger M, Smith GD. Systematic reviews in health care: investigating and dealing with publication and other biases in meta-analysis. BMJ 323(7304), 101–105 (2001).
33.
White I. Network: stata module to perform network meta-analysis. Statistical software components (2017). https://econpapers.repec.org/software/bocbocode/S458319.htm
34.
Chaimani A, Higgins JP, Mavridis D, Spyridonos P, Salanti G. Graphical tools for network meta-analysis in STATA. PLoS One 8(10), e76654 (2013).
35.
Chen M, Dai N, Fei G, Chong CF, Funao N, Zhang S. A phase 3, randomized, double-blind, multicentre study to evaluate the safety and efficacy of TAK-438 20 mg once daily compared to lansoprazole 30 mg once daily in patients with erosive esophagitis: results from a chinese subcohort. United European Gastroenterol. J. 6(8), A513 (2018).
36.
Huang B, Cui DJ, Zhao X et al. Clinical efficacy and safety of vonoprazan in the treatment of refractory reflux esophagitis [in Chinese]. Chin. J. Clin. Rational Drug Use 14(9A), 18–20 (2021).
• Vonoprazan was effective in treating refractory reflux esophagitis.
37.
Okanobu H, Kohno T, Mouri R et al. Efficacy of vonoprazan 10 mg compared with 20 mg for the initial treatment in patients with erosive esophagitis: a randomized pilot study. Esophagus 18(3), 669–675 (2021).
• This revealed that initial treatment with vonoprazan 10 mg might be useful especially in patients with mild erosive esophagitis.
38.
Sakurai K, Suda H, Fujie S et al. Short-term symptomatic relief in gastroesophageal reflux disease: a comparative study of esomeprazole and vonoprazan. Dig. Dis. Sci. 64(3), 815–822 (2019).
• Showed no substantial differences in the symptom relief between the esomeprazole (20 mg/day) and vonoprazan (20 mg/day) groups at any time point.
39.
Uemura N, Kinoshita Y, Haruma K et al. Sa1194 – 1-year interim analysis results of vision trial: a randomized, open-label study to evaluate a long-term safety of vonoprazan as maintenance treatment in patients with erosive esophagitis. Gastroenterology 156(1 Suppl. 6), S-302–S-3 (2019).
40.
Xiao Y, Zhang S, Dai N et al. Phase III, randomised, double-blind, multicentre study to evaluate the efficacy and safety of vonoprazan compared with lansoprazole in Asian patients with erosive oesophagitis. Gut 69(2), 224–230 (2020).
• This study demonstrated the non-inferior efficacy of vonoprazan versus lansoprazole in terms of erosive oesophagitis healing rate at 8 weeks.
41.
Li MJ, Li Q, Sun M, Liu LQ. Comparative effectiveness and acceptability of the FDA-licensed proton pump inhibitors for erosive esophagitis: a PRISMA-compliant network meta-analysis. Medicine (Baltimore) 96(39), e8120 (2017).
42.
Friedenberg FK, Hanlon A, Vanar V et al. Trends in gastroesophageal reflux disease as measured by the National Ambulatory Medical Care Survey. Dig. Dis. Sci. 55(7), 1911–1917 (2010).
43.
Halpern R, Kothari S, Fuldeore M et al. GERD-related health care utilization, therapy, and reasons for transfer of GERD patients between primary care providers and gastroenterologists in a US managed care setting. Dig. Dis. Sci. 55(2), 328–337 (2010).
44.
Tytgat GN. Shortcomings of the first-generation proton pump inhibitors. Eur. J. Gastroenterol. Hepatol. 13(Suppl. 1), S29–S33 (2001).
Information & Authors
Information
Published In
Copyright
© 2023 Becaris Publishing Limited.
History
Received: 10 September 2022
Accepted: 4 July 2023
Published online: 20 July 2023
Keywords:
Topics
Authors
Funding Information
National Nature Science Foundation of China: NO.81874402 and NO.82174128
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Network meta-analysis of multiple doses of vonoprazan for the treatment of erosive esophagitis. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2022-0165
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Adnan Ur Rehman, Muhammad Shoaib Khan, Muhammad Iltaf, Wiqas Ahmad, Naeem Jan, Vonoprazan Therapy in Gastroesophageal Reflux Disease (GERD): Effects on the Severity and Frequency of GERD in Relation to Hiatus Hernia, Cureus, 10.7759/cureus.97186, (2025).
- Sang Pyo Lee, In-Kyung Sung, Oh Young Lee, Myung-Gyu Choi, Kyu Chan Huh, Jae-Young Jang, Hoon Jai Chun, Joong-Goo Kwon, Gwang Ha Kim, Nayoung Kim, Poong-Lyul Rhee, Sang Gyun Kim, Hwoon-Yong Jung, Joon Seong Lee, Yong Chan Lee, Hye-Kyung Jung, Jae Gyu Kim, Sung Kook Kim, Chong-il Sohn, Randomized Multicenter Study to Evaluate the Efficacy and Safety of Fexuprazan According to the Timing of Dosing in Patients With Erosive Esophagitis, Journal of Neurogastroenterology and Motility, 10.5056/jnm24032, 31, 1, (86-94), (2024).
- György Miklós Buzás, A káliumkompetitív savgátlók szerepe a felső emésztőtraktus savfüggő betegségeinek kezelésében, Orvosi Hetilap, 10.1556/650.2023.32937, 164, 50, (1967-1973), (2023).