Quality of life analysis measured with the Cervantes 16 scale in treated menopausal women with genitourinary syndrome
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the quality of life of menopausal women with genitourinary syndrome receiving local drugs (prasterone, estriol or promestriene). Methods: Prospective, longitudinal, randomized study in which quality of life was assessed using the 16-item Cervantes scale (EC16) before and after treatment. Results: A total of 45 women were assessed (35.6% received prasterone, 33.3% estriol and 31.1% promestriene). After treatment, statistically significant mean score differences were observed in EC16, mainly with prasterone. Improvement in EC16 score only shows a statistically significant relationship with age and drug use. Conclusion: The EC16 is an affordable and quick-to-apply tool that allows physicians and patients to know patients' self-perceived quality of life. Local treatment has been shown to improve the quality of life of menopausal patients with genitourinary syndrome.
During menopause there are a number of factors that can disrupt the quality of life of women, such as hot flashes, insomnia, vaginal dryness or palpitations. To control them and improve the quality of life, hormonal treatment can be administered [1]. However, the effects of the different treatments on these signs and symptoms must be analyzed objectively to evaluate whether their use has resulted in a significant improvement in the patient's quality of life, and not only a subjective improvement. This improvement may, in turn, lead to a higher degree of adherence to treatment.
Among the attributes that can be altered during menopause is vaginal health, understood as “the state of the vagina that maintains the physiological conditions appropriate to the evolution of the woman's age, that does not produce local symptomatology and allows a satisfactory sexual life” [1,2]. There are different treatment options to improve or maintain vaginal health, both systemic and local. Among the local ones, there are moisturizers, lubricants, local estrogens, estrogen analogs or the most recent molecules such as prasterone (analog of endogenous dehydroepiandrosterone). Treatment with these formulations can resolve syndromes as complex as genitourinary syndrome (GUS), which is defined as “signs and symptoms associated with the decrease of estrogens and other sex steroids such as androgens, which are responsible for anatomical, physiological, and functional changes in the vulvovaginal area (labia majora, labia minora, clitoris, vestibule, introitus, vagina) and urinary system (urethra and bladder)” [3]. According to some reviews, there is no clear improvement of one vaginal treatment over another, although there is superiority over placebo, with a similar rate of adverse events among the different therapies and no greater than against placebo [4].
Patients with poorer quality of life related to menopausal symptoms are those who start hormonal treatments earlier and have a higher adherence to them. They consult earlier and are more motivated [5]. Patients' perception of quality of life, their life situation in relation to their social context (culture, value system), their goals, aspirations and concerns can be identified by the concept of quality of life, a term that is variable and personal and comprises subjective and objective factors [6–8]. Other concepts to be taken into account are the patient-reported experience measure, which defines the patient's experience after a health intervention, and the patient-reported outcome measure, the results that the patient comments on or reports after a health intervention.
One of the methods used to measure quality of life in menopausal women is the 31-item Cervantes scale (EC31). This questionnaire is divided into four domains: menopause and health, sexuality, psychic and couple relationship, with the subdimensions of vasomotor symptomatology, health and aging. The overall score of the scale can range from 0 to 155 points, with patients' quality of life being worse the higher the score on the scale [9]. There is a shorter version with only 16 items (EC16). This reduced version includes the same domains over a total score of 100 points and, likewise, the higher the score, the worse the quality of life. According to the score obtained, quality of life can be defined as 20–40 points, very good; 40–60 points, good; 60–80 points, poor; and 80–100 points, very poor [10].
Our main hypothesis is that patients' quality of life improves after local treatment. Thus, the main objective of this study is to analyze the evolution of the quality of life of menopausal patients with GUS receiving different local drugs, using EC16 before and after treatment. As a secondary objective, the results of the application of three local vaginal treatments for GUS in menopausal women will be analyzed.
Patients & methods
Study design, participants & interventions
A prospective, longitudinal, randomized, parallel-group study was conducted in the gynecology consultation of Vithas Hospital in El Ejido (Almeria, Spain), from January 2019 to December 2020.
Women aged 55–70 years diagnosed with GUS attending a general gynecology consultation, who showed a desire to participate in the study and who were not under any systemic or local hormonal treatment, were included. After diagnosis of GUS, they were offered to participate in the study and, after obtaining informed consent, were asked to complete a survey for the collection of epidemiological data (Annex 1) and the EC16 (Annex 2). Patients were randomized to receive prasterone, estriol or promestriene, in a 1:1:1 ratio. In addition to topical treatment, all patients were recommended to use vaginal moisturizers, lubricants and dilators. The duration of treatment was 4 months, after which the patients were scheduled for a clinical evaluation and to complete a new questionnaire (Annex 3) and the EC16 to assess whether there were changes in their quality of life and whether any of their lifestyle habits had been modified.
The prescribed treatments had a different form of administration. Prasterone at a dose of 6.5 mg (presented in bullet-shaped pessary) was administered once daily, at bedtime. Estriol at a dose of 50 µg (presented in gel) was administered with an initial dose for 3 weeks of one application every night and subsequently one application twice a week. Promestriene (synthetic estrogenic derivative) at a dose of 10 mg (presented in cream) was administered with an initial dose for 3 weeks of one application every night and subsequently one application twice a week.
Statistical analysis
The variables analyzed were age, time since the onset of menopause, number of vaginal deliveries, whether or not the patient had a sexual partner, adherence to the recommendations, comfort with the use of the treatments, cervicovaginal cytology, frequency of coitus per month, degree of dyspareunia (visual analog scale from 0 to 5; 0 coitus without any pain and 5 unbearable pain), degree of GUS and EC16 score.
The Kolmogorov–Smirnov test was used to analyze the normality of the sample. As the variables had a normal distribution, parametric tests could be applied. Qualitative variables were compared using the χ2. Quantitative variables were compared with the McNemar's test.
In addition, a multiple linear regression model was performed to study the adjusted effect of each variable on the outcome variables and to analyze whether the improvement found is due to the medical treatment or to the intervention of the other factors, all with a significance level of 5%. The analyses were performed with SPSS v.22.0.
Results
Patient characteristics
A total of 45 patients were evaluated: 16 received prasterone (35.6%), 15 estriol (33.3%) and 14 promestriene (31.1%). The demographic and clinical characteristics for each group and for the total population studied are presented in Table 1. The mean (standard deviation) age for all patients was 62.47 (4.44) years, with a range of 56–70 years. The mean time since onset of menopause was 11.0 (2.82) years, with a range of 6–15 years. The mean delivery rate was 1.78 (1.33) per patient, with a minimum of zero and a maximum of five deliveries. A total of 84.4% of the patients had a partner. In relation to the baseline clinical characteristics, 31.1% of the patients had an altered cytology. Mild GUS was present in 35.6%, moderate GUS in 51.1% and severe GUS in 13.3%. Dilators were used by 6.7% of the patients, vaginal moisturizers by 15.6% and lubricants by 17.8%.
| Variables | Patients with prasterone (n = 16) | Patients with estriol (n = 15) | Patients with promestriene (n = 14) | Total (n = 45) |
|---|---|---|---|---|
| Age, years, median (SD) | 62.56 (3.61) | 63.8 (4.26) | 60.93 (5.26) | 62.47 (4.44) |
| Time in menopause, years, mean (SD) | 11.38 (2.39) | 10.03 (2.74) | 10.64 (3.46) | 11.0 (2.82) |
| Partner, n (%) • Yes • No | 13 (81.3) 3 (18.8) | 14 (93.3) 1 (6.7) | 11 (78.6) 3 (21.4) | 38 (84.4) 7 (15.6) |
| Vaginal deliveries, n (%), median (SD) | 1.88 (1.40) | 2.07 (1.44) | 1.36 (1.08) | 1.78 (1.33) |
| Cytology, n (%) • Normal • Altered | 10 (62.5) 6 (37.5) | 12 (80.0) 3 (20.0) | 5 (35.7) 9 (64.3) | 31 (68.9) 14 (31.1) |
| Genitourinary syndrome, n (%) • Mild • Moderate • Severe | 6 (37.5) 8 (50.0) 2 (12.5) | 4 (26.7) 10 (66.7) 1 (6.7) | 6 (42.9) 5 (35.7) 3 (21.4) | 16 (35.6) 23 (51.1) 6 (13.3) |
| Adherence to the recommendations, n (%) • Dilators • Moisturizers • Lubricants | – 3 (18.8) 4 (25.0) | 1 (6.7) 2 (13.3) 3 (20.0) | 2 (14.3) 2 (14.3) 1 (7.1) | 3 (6.7) 7 (15.6) 8 (17.8) |
SD: Standard deviation.
Results after medical treatment
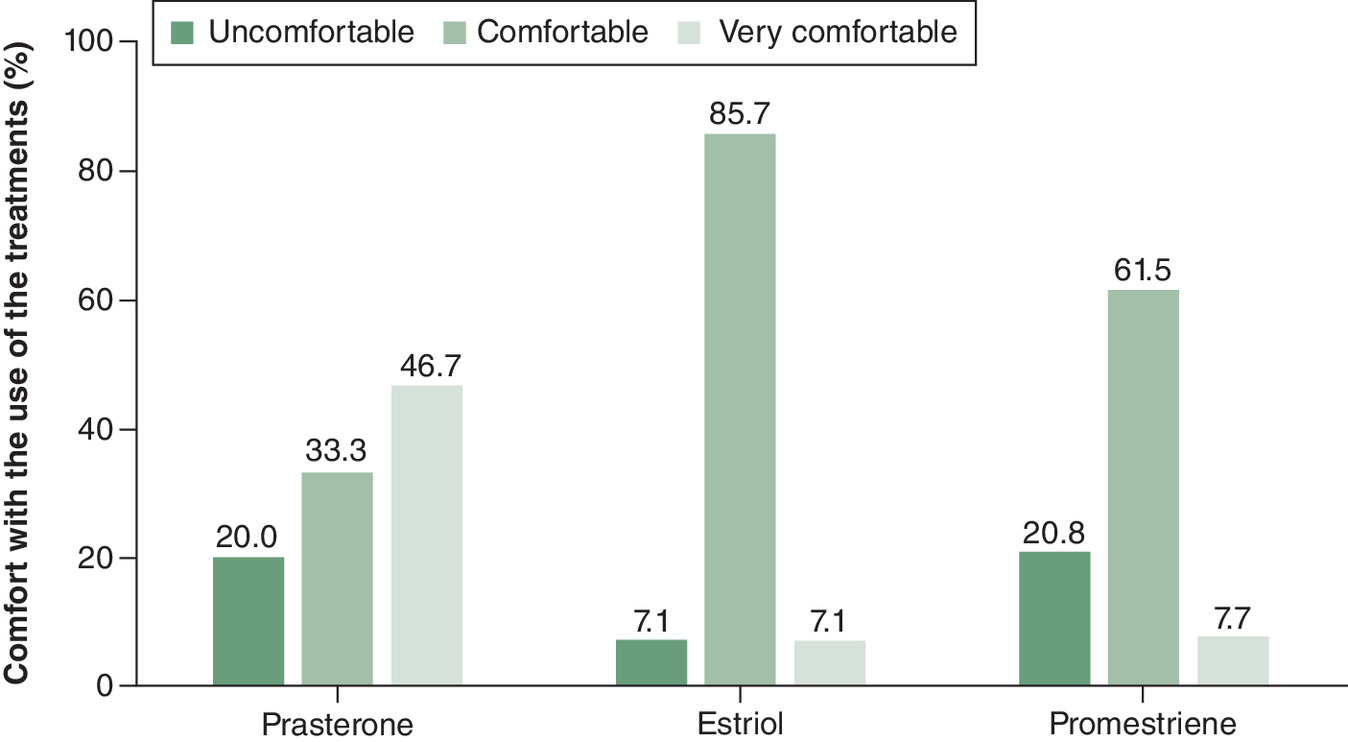
In the prasterone group, results were the following: mean increase in the frequency of coitus/month (p < 0.001); decrease in dyspareunia (p < 0.001); and improvement in EC16 score, with a mean decrease of 6.13 ± 4.35 points (p < 0.001). The treatment was comfortable or very comfortable for 80% of the patients.
The estriol group showed the following results: mean increase in the frequency of coitus/month (p < 0.001); decrease in dyspareunia (p < 0.001); and improvement in EC16 score, with a mean decrease of 2.93 ± 4.35 points (p < 0.001). The treatment was comfortable or very comfortable for 92.8% of the patients and acceptable for 85.7%.
The promestriene group showed mean increase in the frequency of coitus/month (p < 0.001); decrease in dyspareunia (p < 0.001); and improvement in the EC16 score, with a mean decrease of 2.50 ± 2.74 points (p < 0.001). It was the most uncomfortable treatment to use. The treatment was comfortable or very comfortable for 69.2% of the patients.
Tables 2–4 & Figures 1–4 show all the results.
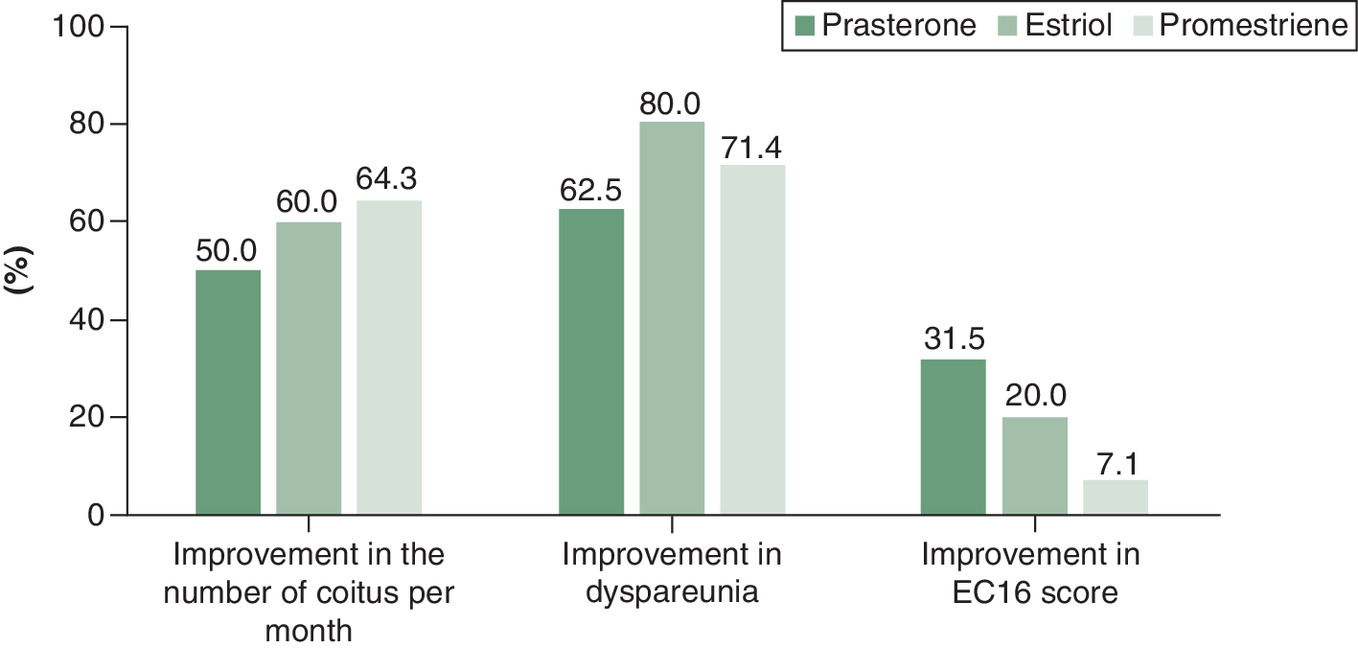
Figure 1. Percentage of improvement in frequency of coitus per month, improvement of dyspareunia and improvement in EC16.
EC16: 16-item Cervantes scale.
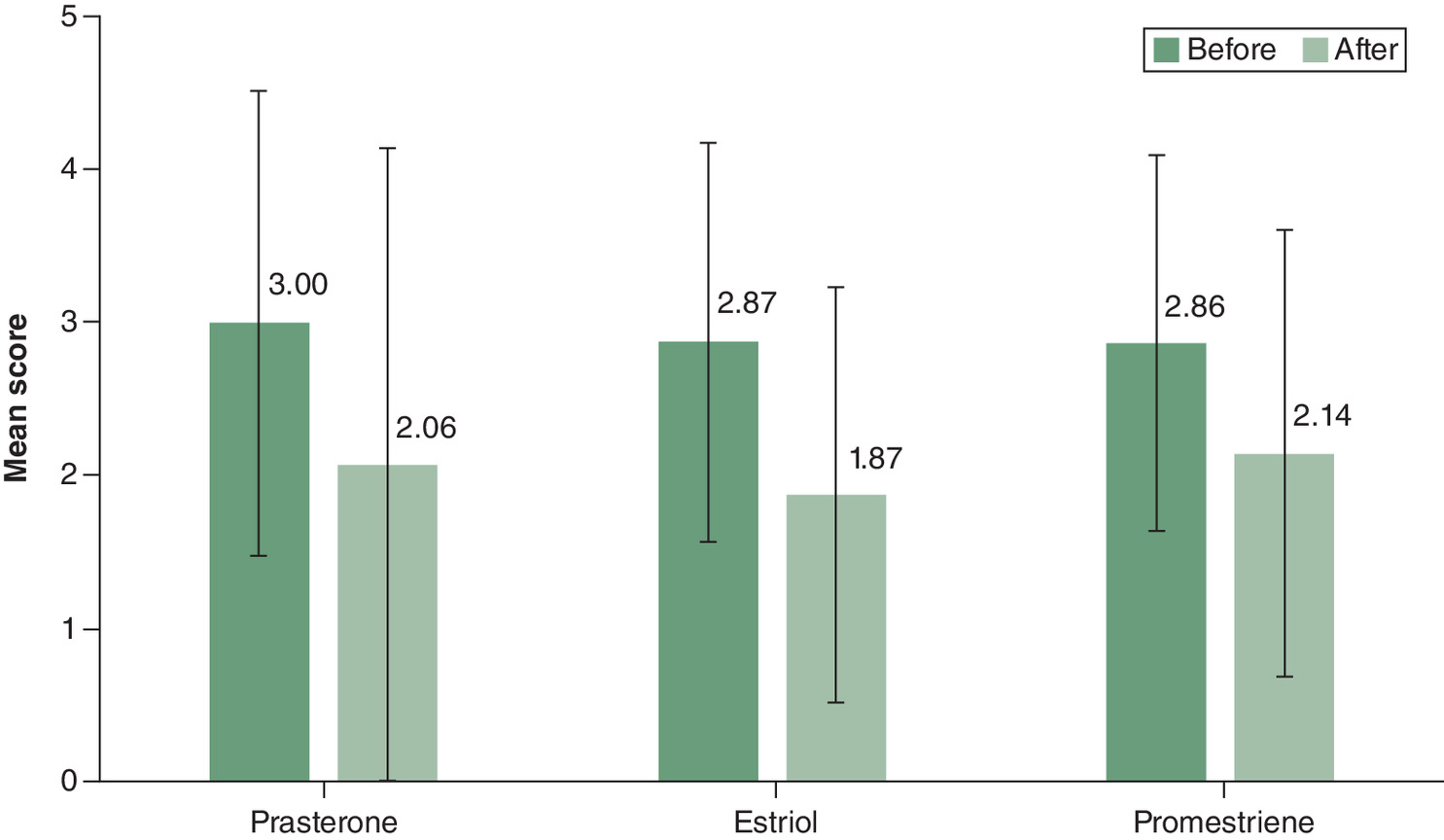
Figure 2. Evolution of dyspareunia before and after treatment.
5: Unbearable pain; 4: Very painful; 3: Pain; 2: Bearable pain; 1: Slight pain; 0: No pain.
| Patients with prasterone (n = 16) | |||
|---|---|---|---|
| Coitus/month | Mean (SD) | p-value | 95% CI |
| • Before • After • Difference | 1.50 (1.79) 2.00 (2.13) +0.50 (0.34) | < 0.001 | -0.78–(-0.23) |
| Dyspareunia† | Mean (SD) | p-value | 95% CI |
|---|---|---|---|
| • Before • After • Difference | 3.00 (1.51) 2.06 (2.08) -0.94 (0.57) | < 0.001 | 0.48–1.39 |
| Comfort of use | n (%) | p-value | |
|---|---|---|---|
| • Uncomfortable • Acceptable • Very comfortable | 3 (20.0) 5 (33.3) 7 (46.7) | < 0.001 | |
| Patients with estriol (n = 15) | |||
|---|---|---|---|
| Coitus/month | Mean (SD) | p-value | 95% CI |
| • Before • After • Difference | 1.53 (1.36) 2.13 (1.41) +0.60 (0.05) | < 0.001 | -0.81–(-0.32) |
| Dyspareunia† | Mean (SD) | p-value | 95% CI |
|---|---|---|---|
| • Before • After • Difference | 2.87 (1.30) 1.87 (1.36) -1.00 (0.06) | < 0.001 | 0.58–1.41 |
| Comfort of use | n (%) | p-value | |
|---|---|---|---|
| • Uncomfortable • Acceptable • Very comfortable | 1 (7.1) 12 (85.7) 1 (7.1) | < 0.001 | |
| Patients with promestriene (n = 14) | |||
|---|---|---|---|
| Coitus/month | Mean (SD) | p-value | 95% CI |
| • Before • After • Difference | 2.29 (1.94) 2.93 (2.13) +0.64 (0.19) | < 0.001 | -0.93–(-0.36) |
| Dyspareunia† | Mean (SD) | p-value | 95% CI |
|---|---|---|---|
| • Before • After • Difference | 2.86 (1.23) 2.14 (1.46) -0.72 (0.23) | < 0.001 | 0.444–0.985 |
| Comfort of use | n (%) | p-value | |
|---|---|---|---|
| • Uncomfortable • Acceptable • Very comfortable | 4 (30.8) 8 (61.5) 1 (7.7) | < 0.001 | |
†
Visual analog scale from 0 to 5; 0 coitus without any pain and 5 unbearable pain.
SD: Standard deviation.
| Patients with prasterone (n = 16) | Mean (SD) | p-value | d Cohen | 95% CI |
|---|---|---|---|---|
| • Before • After • Difference | 48.88 (18.98) 42.75 (19.03) -6.13 (4.35) | < 0.001 | 0.228 | 3.81–8.44 |
| Patients with estriol (n = 15) | ||||
|---|---|---|---|---|
| • Before • After • Difference | 44.73 (13.30) 41.80 (14.00) -2.93 (4.35) | < 0.001 | 0.152 | 0.524–5.342 |
| Patients with promestriene (n = 14) | ||||
|---|---|---|---|---|
| • Before • After • Difference | 43.43 (18.38) 40.93 (19.17) -2.5 (2.7) | < 0.001 | 0.094 | 0.919–4.081 |
EC16: 16-item Cervantes scale; SD: Standard deviation.
| Variables | Crude model | Adjusted model | ||||
|---|---|---|---|---|---|---|
| Coefficient | p-value | 95% CI | Coefficient | p-value | 95% CI | |
| Age | -0.02 | 0.188 | -0.05–0.01 | 0.563 | 0.033 | 0.05–1.01 |
| Years with menopause | -0.03 | 0.239 | -0.07–0.02 | -0.244 | 0.334 | -1.11–(-0.39) |
| Has partner | -0.07 | 0.689 | -0.41–0.27 | -0.002 | 0.992 | -4.81–4.76 |
| Childbirth | 0.03 | 0.856 | -0.28–0.34 | 0.184 | 0.219 | -0.36–1.51 |
| Altered cytology | 0.83 | 0.530 | -0.18–0.35 | 0.097 | 0.518 | -1.84–3.57 |
| Genitourinary syndrome | 0.10 | 0.271 | -0.82–0.28 | 0.041 | 0.850 | -2.44–2.95 |
| Dilators | 0.21 | 0.382 | -0.27–0.70 | 0.145 | 0.380 | -3.07–7.86 |
| Moisturizers | 0.07 | 0.689 | -0.27–0.41 | 0.032 | 0.834 | -3.09–3.81 |
| Lubricants | 0.24 | 0.124 | -0.70–0.56 | 0.014 | 0.926 | -3.11–3.41 |
| Drugs | -0.12 | 0.104 | -0.27–0.03 | -0.418 | 0.008 | -3.65–(-0.589) |
Analysis using EC16
The mean score for the overall population was 45.80 (16.87) before treatment and 41.87 (17.17) after treatment (p < 0.001). Independently, all drugs decreased the mean EC16 score, but the decrease was more significant with prasterone. After treatment with prasterone, the mean EC16 score decreased 6.13 (4.30) (p < 0.001), with estriol it decreased 2.93 (4.35) (p < 0.001) and with promestriene it decreased 2.5 (2.7) (p < 0.001) (Table 3).
In the multiple regression analysis, considering the effect of all variables (age, years of menopause, having a partner, childbirth, altered cytology, severity of GUS, use of dilators, moisturizing gel, lubricant and drugs) on the improvement in the EC16 score, only the patient's age and the use of drugs (promestriene, estriol or prasterone) show a statistically significant relationship: for each year of age the EC16 score increases 0.56-fold (95% CI: 0.04–1.01) and the use of medical treatment decreases the score by 0.42-fold (95% CI: -3.65–[-0.59]) (Table 4).
The older the patient gets, the worse the quality of life as shown in the EC16 scale. Although there is a significant improvement after treatment, the decrease with age is maintained. Patients who have been in menopause for more than 10 years report a worse quality of life compared with those who have been in menopause for less than 10 years; after medical intervention, the percentage of women who report a very poor quality of life decreases. Before treatment, there was a significant relationship between women's quality of life and the frequency of coitus per month. Women with fewer occasions of coitus reported poorer quality of life. After treatment, women with more occasions of coitus increases quality of life.
No statistically significant differences were observed according to the use or non-use of recommendations, nor were statistically significant differences observed in terms of quality of life between women who had children and those who did not, either before (p = 0.897) or after treatment (p = 0.669), or according to cytology (normal/altered).
In summary, the quality of life of patients improves after local treatment, measured objectively with the EC16.
Discussion
Only about 60% of those with GUS discuss this disorder with their healthcare provider, mainly because women believe that this condition is a natural part of the aging phenomenon or that symptoms are not bothersome enough to warrant discussion [11]. Thus, the global assessment of patients is fundamental to provide quality healthcare and increase the possibilities of assistance. The use of quality of life scales allows addressing of a number of issues that, due to lack of time or lack of practice, could be missed. In addition, the use of these scales makes possible comparison of results between health professionals and between different treatments administered.
Previous studies have assessed the quality of life of women and its relationship with menopause and GUS. Two large studies – Vaginal Health: Insights, Views and Attitudes, and Real Women's Views of Treatment Options for Menopausal Vaginal Changes – were carried out by direct interviews with postmenopausal women, and provided important information about how GUS can influence relationships and, more generally, how it impacts quality of life [12,13]. Other studies demonstrated the association between sexual dysfunction and symptoms related to GUS by analyzing the quality of life of these women through the menopausal quality of life questionnaire [14]. This is a self-administered questionnaire that includes 30 items organized in four domains: vasomotor, physical, psychosocial and sexual, and a global quality of life question. The sexual domain contains three items: change in sexual desire, vaginal dryness during intercourse and avoiding intimacy [15]. In our study we use EC16 to assess the quality of life of menopausal women with GUS before and after receiving local drugs. This questionnaire maintains the original dimensional structure and psychometric properties of the original EC31 but, as a shorter version, the EC16 can be completed more quickly, making it particularly suitable for routine medical practice [2].
GUS has an important sexual and psychological effect, and makes women feel older, uncomfortable, less feminine, frustrated, worried, anxious and depressed [11]. The main clinical manifestations of GUS include genital symptoms of dryness, burning and irritation; sexual symptoms of lack of lubrication, discomfort or pain, and impaired function; as well as urinary symptoms of urgency, dysuria and recurrent urinary tract infections [16–19]. The most common and bothersome symptom is vaginal dryness [20,21]. Vaginal dryness generates discomfort in women, not only during sexual intercourse, but at any time. The loss of balance between the vaginal microbiota and the consequent alteration of the pH, favored by the drop in estrogens, can lead to repeated urinary tract infections, pain with sexual intercourse and recurrent vaginal infections. All this would be encompassed within the GUS [2,22]. These patients often require a long-term treatment to improve sexual health and quality of life, as the condition does not tend to diminish over time if left untreated [23]. For this reason, patients often prefer local treatments. Health professionals should inform patients about all pharmacological presentations and forms of administration, and recommend the most appropriate treatment in each case. When therapeutic decisions are shared between physicians and patients, adherence improves and better outcomes are achieved.
It is known that intravaginal estriol is well absorbed by an atrophic epithelium [24]. Intravaginal estriol has shown to improve symptoms of GUS, sexual health and, more generally, women's quality of life [25]. The ultralow-dose estriol vaginal gel formulation (0.005%), which significantly enhances estriol delivery to vaginal tissue compared with existing formulations, allows the use of much lower doses of estriol to treat vaginal atrophy [26]. The main concerns regarding estrogen administration are side effects and its use in hormone receptor-positive breast cancer. However, few adverse events have been observed for intravaginal estriol (mainly local), and no correlations have been found between intravaginal estriol administration and increased endometrial thickness [27,28]. Although clinicians suspect that the hormones absorbed through the vaginal wall may stimulate cancer recurrence, the low-dose estriol therapy in patients during aromatase inhibitor treatment suffering from GUS-related issues can be considered as safe and efficacious because this method of treatment does not increase estradiol and estrogen levels [29].
Unlike estrogen-based therapy, prasterone is a revolutionary molecule that corrects sex steroid deficiency by delivering both estrogens and androgens into the vagina, and restores vaginal anatomic and morphological changes [30]. This drug is recommended by the North American Menopause Society as an option for the treatment of GUS of menopause, including vulvovagival atrophy, in postmenopausal women [31]. Approval of prasterone is too recent to have been included in the European Menopause and Andropause Society guidelines [32]. In the EU, prasterone is indicated for the treatment of vulvar and vaginal atrophy in postmenopausal women having moderate-to-severe symptoms [33]. In addition to the long-term efficacy improving signs and symptoms of vulvovagival atrophy [34], prasterone also appeared to improve sexual dysfunction in postmenopausal women, and those treated with intravaginal prasterone pessary displayed a high degree of user satisfaction [35,36]. All these data seem to be in accordance with the results of our study, which shows a significant improvement in the quality of life of patients over the other topical drugs used.
The main limitation of the study is that EC16 is not designed specifically to assess the quality of life according to vulvar and vaginal health. So, it would be necessary to develop quality of life scales that would include more specific issues of vulvar and vaginal health. By asking a patient about her sexual habits, vaginal health, sleep quality or other issues related to menopause, we are closer to detecting needs that patients do not raise from the outset.
Conclusion
GUS is a very frequent pathology among menopausal women who, with proper health education and appropriate treatment, can improve their quality of life, as measured by a validated questionnaire such as the EC16. This questionnaire is an affordable and quick-to-apply tool that allows physicians and patients to know patients' self-perceived quality of life, and to evaluate if the intervention helps to assess patients' quality of life.
•
Vaginal health is an important element of a woman's overall health, so the treatment of possible disorders, such as genitourinary syndrome, is a priority.
•
The use of moisturizers, lubricants and vaginal dilators can help with mild stages of genitourinary syndrome, but in moderate or severe stages it is necessary to use local hormonal treatment with estrogens, estrogen analogues or new generation molecules such as prasterone.
•
The effects of treatments on these disorders must be analyzed objectively to evaluate whether their use has resulted in a significant improvement in the patient's quality of life, and not only a subjective improvement.
•
The 16-item Cervantes scale (EC16) is a shorter version of the 31-item Cervantes scale that is used to assess quality of life in menopausal women.
•
The improvement in EC16 score only shows a statistically significant relationship with the patient's age and with the use of drugs (promestriene, estriol or prasterone). The older the patient gets, the worse the quality of life as shown in the EC16 scale.
•
After treatment with prasterone, estriol or promestriene, statistically significant mean score differences were observed in EC16. The best improvement in the EC16 was obtained with prasterone.
Author contributions
P Romero Duarte: study design, study execution, collection of results, preparation of the article and study presentation. MT Maroto Martín: statistical analysis and preparation of the article. MM Martín Moya: bibliographic search and collection of results. P Abad Prados: review of the study and analysis of the results. All authors read and approved the final manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Medical writing assistance was received for this article. The authors wish to thank Content Ed Net (Madrid, Spain) and F Sánchez Barbero for their support on the preparation of this manuscript.
Ethical conduct of research
The authors state that they have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Sánchez Borrego R, Llaneza Coto P, Mendoza Ladrón De Guevara N et al. AEEM-SEGO position statement on menopausal hormone therapy. Prog. Obstet. Ginecol. 61(3), 230–234 (2018).
•• Recommendations for the use of hormonal therapy in women with menopause according the Spanish Menopause Society (Asociación Española para el Estudio de la Menopausia) and the Spanish Society of Gynecology and Obstetrics (Sociedad Española de Ginecología y Obstetricia).
2.
Cancelo-Hidalgo MJ, Barrera Coello L. Genitourinary syndrome of the menopause: vaginal health and microbiota. In: Menopause. Cano A (Ed.). Springer, Cham, Switzerland, 91–107 (2017).
3.
Palacios S, Cancelo Hidalgo MJ, González SP, Manubens M, Sánchez-Borrego R. Genitourinary syndrome of menopause: recommendations from the Spanish Society of Obstetrics and Gynecology. Prog. Obstet. Ginecol. 62(2), 141–148 (2019).
•• Recommendations for the prevention and treatment of genitourinary syndrome of menopause according to the Spanish Society of Obstetrics and Gynecology.
4.
Lethaby A, Ayeleke RO, Roberts H. Local oestrogen for vaginal atrophy in postmenopausal women. Cochrane Database Syst. Rev. (8) CD001500, (2016).
5.
Fasero M, Hernández A, Varillas-Delgado D, Coronado PJ. Women with low quality of life by Cervantes short-form scale choose menopausal hormone therapy. Eur. J. Obstet. Gynecol. Reprod. Biol. 252, 43–49 (2020).
6.
Bobula J. PWH4 vasomotor symptoms and quality of life (QoL) in postmenopausal women. Value in Health 6(6), 707 (2003).
7.
Brazier JE, Roberts J, Platts M, Zoellner YF. Estimating a preference-based index for a menopause specific health quality of life questionnaire. Health Qual. Life Outcomes 3(1), 13 (2005).
8.
Blumel JE, Castelo-Branco C, Binfa L et al. Quality of life after the menopause: a population study. Maturitas 34(1), 17–23 (2000).
9.
Sánchez Borrego R, García-García P, Mendoza N, Soler López B, Álamo González C. Grupo De Estudio Cervantes. Assessment of quality of life in postmenopausal women through the Cervantes scale: impact of treatment in clinical practice. Prog. Obstet. Ginecol. 58(4), 177–182 (2015).
•• Study that used the Cervantes scale to assess the quality of life of menopausal women and determine the effect of treatment.
10.
Coronado PJ, Borrego RS, Palacios S, Ruiz MA, Rejas J. Structural validity of a 16-item abridged version of the Cervantes health-related quality of life scale for menopause: the Cervantes Short-Form Scale. Menopause 22(3), 325–336 (2015).
•• Study that validated the 16-item short-form version of the Cervantes health-related quality of life scale for menopause women.
11.
Nappi RE, Particco M, Biglia N et al. Attitudes and perceptions towards vulvar and vaginal atrophy in Italian post-menopausal women: evidence from the European REVIVE survey. Maturitas 91, 74–80 (2016).
12.
Simon JA, Kokot-Kierepa M, Goldstein J, Nappi RE. Vaginal health in the United States: results from the Vaginal Health: Insights, Views and Attitudes survey. Menopause 20(10), 1043–1048 (2013).
• Vaginal Health: Insights, Views and Attitudes survey that assessed US postmenopausal women's knowledge of and attitudes toward vaginal atrophy.
13.
Kingsberg SA, Wysocki S, Magnus L, Krychman ML. Vulvar and vaginal atrophy in postmenopausal women: findings from the REVIVE (Real Women's Views of Treatment Options for Menopausal Vaginal Changes) survey. J. Sex. Med. 10(7), 1790–1799 (2013).
• Real Women's Views of Treatment Options for Menopausal Vaginal Changes survey that characterized postmenopausal women's experience with and perception of vulvar and vaginal atrophy symptoms, interactions with healthcare professionals and available treatment options.
14.
Pinkerton JV, Bushmakin AG, Komm BS, Abraham L. Relationship between changes in vulvar-vaginal atrophy and changes in sexual functioning. Maturitas 100, 57–63 (2017).
15.
Hilditch JR, Lewis J, Peter A et al. A menopause-specific quality of life questionnaire: development and psychometric properties. Maturitas 24(3), 161–175 (1996).
16.
Portman DJ, Gass ML. Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the International Society for the Study of Women's Sexual Health and the North American Menopause Society. Menopause 21(10), 1063–1068 (2014).
17.
Farrell Am E. Genitourinary syndrome of menopause. Aust. Fam. Physician 46(7), 481–484 (2017).
18.
Patnaik SS, Lagana AS, Vitale SG et al. Etiology, pathophysiology and biomarkers of interstitial cystitis/painful bladder syndrome. Arch. Gynecol. Obstet. 295(6), 1341–1359 (2017).
19.
Gardella B, Iacobone AD, Porru D et al. Effect of local estrogen therapy (LET) on urinary and sexual symptoms in premenopausal women with interstitial cystitis/bladder pain syndrome (IC/BPS). Gynecol. Endocrinol. 31(10), 828–832 (2015).
20.
Palma F, Xholli A, Cagnacci A, as the Writing Group of the Agata Study. The most bothersome symptom of vaginal atrophy: evidence from the observational AGATA study. Maturitas 108, 18–23 (2018).
21.
Cagnacci A, Xholli A, Sclauzero M et al. Vaginal atrophy across the menopausal age: results from the ANGEL study. Climacteric 22(1), 85–89 (2019).
22.
Shifren JL. Genitourinary syndrome of menopause. Clin. Obstet. Gynecol. 61(3), 508–516 (2018).
23.
Naumova I, Castelo-Branco C. Current treatment options for postmenopausal vaginal atrophy. Int. J. Womens Health 10, 387–395 (2018).
• Article that reviews the current treatment options for postmenopausal women with vaginal atrophy.
24.
Mattsson LA, Cullberg G. Vaginal absorption of two estriol preparations. A comparative study in postmenopausal women. Acta Obstet. Gynecol. Scand. 62(5), 393–396 (1983).
25.
Buchholz S, Mogele M, Lintermans A et al. Vaginal estriol–lactobacilli combination and quality of life in endocrine-treated breast cancer. Climacteric 18(2), 252–259 (2015).
26.
Caruso S, Cianci S, Vitale SG, Matarazzo MG, Amore FF, Cianci A. Effects of ultralow topical estriol dose on vaginal health and quality of life in postmenopausal women who underwent surgical treatment for pelvic organ prolapse. Menopause 24(8), 900–907 (2017).
27.
Rueda C, Osorio AM, Avellaneda AC, Pinzón CE, Restrepo OI. The efficacy and safety of estriol to treat vulvovaginal atrophy in postmenopausal women: a systematic literature review. Climacteric 20(4), 321–330 (2017).
28.
Ali ES, Mangold C, Peiris AN. Estriol: emerging clinical benefits. Menopause 24(9), 1081–1085 (2017).
29.
Donders G, Neven P, Moegele M et al. Ultra-low-dose estriol and Lactobacillus acidophilus vaginal tablets (Gynoflor®) for vaginal atrophy in postmenopausal breast cancer patients on aromatase inhibitors: pharmacokinetic, safety, and efficacy phase I clinical study. Breast Cancer Res. Treat. 145(2), 371–379 (2014).
30.
Archer DF, Labrie F, Montesino M, Martel C. Comparison of intravaginal 6.5 mg (0.50%) prasterone, 0.3 mg conjugated estrogens and 10 mug estradiol on symptoms of vulvovaginal atrophy. J. Steroid Biochem. Mol. Biol. 174, 1–8 (2017).
31.
The Nams Hormone Therapy Position Statement Advisory Panel. The 2017 hormone therapy position statement of The North American Menopause Society. Menopause 24(7), 728–753 (2017).
32.
Hirschberg AL, Bitzer J, Cano A et al. Topical estrogens and non-hormonal preparations for postmenopausal vulvovaginal atrophy: an EMAS clinical guide. Maturitas 148, 55–61 (2021).
33.
EMA. Prasterone product information.2022). www.ema.europa.eu/en/documents/product-information/intrarosa-epar-product-information_en.pdf
34.
Labrie F, Archer DF, Bouchard C et al. Prasterone has parallel beneficial effects on the main symptoms of vulvovaginal atrophy: 52-week open-label study. Maturitas 81(1), 46–56 (2015).
35.
Labrie F, Derogatis L, Archer DF et al. Effect of intravaginal prasterone on sexual dysfunction in postmenopausal women with vulvovaginal atrophy. J. Sex. Med. 12(12), 2401–2412 (2015).
36.
Bouchard C, Labrie F, Derogatis L et al. Effect of intravaginal dehydroepiandrosterone (DHEA) on the female sexual function in postmenopausal women: ERC-230 open-label study. Horm. Mol. Biol. Clin. Investig. 25(3), 181–190 (2016).
Information & Authors
Information
Published In
Pages: 1365 - 1374
PubMed: 36331051
Copyright
© 2022 Future Medicine Ltd.
History
Received: 12 May 2022
Accepted: 14 October 2022
Published online: 4 November 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Quality of life analysis measured with the Cervantes 16 scale in treated menopausal women with genitourinary syndrome. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0086
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- E. V. Shlyakhto, I. I. Dedov, V. N. Serov, G. T. Sukhikh, G. P. Arutyunov, I. A. Suchkov, O. M. Drapkina, O. N. Tkacheva, Ya. A. Orlova, I. I. Baranov, E. N. Andreeva, S. V. Yureneva, M. I. Yarmolinskaya, A. A. Smetnik, S. V. Villevalde, N. A. Koziolova, I. V. Sergienko, I. S. Yavelov, O. B. Irtyuga, O. R. Grigoryan, E. N. Dudinskaya, I. A. Zolotukhin, E. A. Ilyukhin, Russian eligibility criteria for prescription of menopausal hormone therapy to patients with cardiovascular and metabolic diseases. Agreement document of RKO, ROAG, RAE, EAT, AFR, RNMOT, RAGG, Bulletin of Reproductive Health, 10.14341/brh12788, 1, (40-69), (2026).
- С.О. Дубровина, А.А. Михельсон, О.С. Карачевская, ФОКУС НА НОВЫЕ ВОЗМОЖНОСТИ ТЕРАПИИ ГЕНИТОУРИНАРНОГО МЕНОПАУЗАЛЬНОГО СИНДРОМА И ВУЛЬВОВАГИНАЛЬНОЙ АТРОФИИ, Issues of practical colposcopy. Genital infections, 10.46393/27826392_2026_1_6-10, 1, (6-10), (2026).
- E. V. Shlyakhto, I. I. Dedov, V. N. Serov, G. T. Sukhikh, G. P. Arutyunov, I. A. Suchkov, O. M. Drapkina, O. N. Tkacheva, Ya. A. Orlova, I. I. Baranov, E. N. Andreeva, S. V. Yureneva, M. I. Yarmolinskaya, A. A. Smetnik, S. V. Villevalde, N. A. Koziolova, I. V. Sergienko, I. S. Yavelov, O. B. Irtyuga, O. R. Grigoryan, E. N. Dudinskaya, I. A. Zolotukhin, Е. А. Ilyukhin, Russian eligibility criteria for prescription of menopausal hormone therapy to patients with cardiovascular and metabolic diseases. Agreement document of RKO, ROAG, RAE, EAT, AFR, RNMOT, RAGG, Problems of Endocrinology, 10.14341/probl13694, 71, 6, (108-137), (2026).
- E. V. Shlyakhto, I. I. Dedov, V. N. Serov, G. T. Sukhikh, G. P. Arutyunov, I. A. Suchkov, O. M. Drapkina, O. N. Tkacheva, Ia. A. Orlova, I. I. Baranov, E. N. Andreeva, S. V. Yureneva, M. I. Yarmolinskaya, A. A. Smetnik, S. V. Villevalde, N. A. Koziolova, I. V. Sergienko, I. S. Yavelov, O. B. Irtyuga, O. R. Grigoryan, E. N. Dudinskaya, I. A. Zolotukhin, E. A. Ilyukhin, Russian Eligibility Criteria for Prescribing Menopausal Hormone Therapy to Patients With Cardiovascular and Metabolic Diseases. Consensus Document of RSC, RSOG, RAE, EUAT, RAP, RSMSI, RAGG, Kardiologiia, 10.18087/cardio.2025.11.n3056, 65, 11, (24-47), (2025).
- María A. Belardo, Magali Galarza Taborda, Marina Canepa, Agustina P. Starvaggi, Roshel Silva Naranjo, DHEA intravaginal, una nueva alternativa para el síndrome genitourinario de la menopausia, Revista del Hospital Italiano de Buenos Aires, 10.51987/Rev.Hosp.Ital.B.Aires.vi.708, 45, 3, (e0000708), (2025).
- Carlo Ronsini, Irene Iavarone, Natalino Lacerenza, Giada Andreoli, Maria Giovanna Vastarella, Pasquale De Franciscis, Mario Passaro, Raffaella De Simone, Domenico Giraldi, Rosalia Lizza, Giampaolo Mainini, Stable Ozonides plus Vitamin E Acetate (Ozoile) for Treatment of Genitourinary Syndrome, Medicina, 10.3390/medicina60060880, 60, 6, (880), (2024).