Indirect treatment comparison of idecabtagene vicleucel versus conventional care in triple-class exposed multiple myeloma
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the efficacy of idecabtagene vicleucel (ide-cel, bb2121) versus conventional care (CC) in triple-class exposed relapsed and refractory multiple myeloma (RRMM) patients. Patients & methods: A matching-adjusted indirect comparison was conducted using individual patient-level data from the pivotal, phase II, single-arm KarMMa trial (NCT03361748) and aggregate-level data from MAMMOTH, the largest independent observational study of CC in heavily pretreated RRMM patients. Results: Ide-cel improved overall response rate (odds ratio: 5.30; 95% CI: 2.96–9.51), progression-free survival (hazard ratio: 0.50; 95% CI: 0.36–0.70) and overall survival (hazard ratio: 0.37; 95% CI: 0.25–0.56) versus CC. Conclusion: These results suggest ide-cel offers improvements in clinical outcomes relative to CC in this heavily pretreated RRMM population.
Multiple myeloma (MM) is an incurable hematological malignancy, with an estimated incidence rate of 1.8 per 100,000 people worldwide in 2020 [1]. Over the past 2 decades, treatment with immunomodulatory drugs, proteasome inhibitors (PIs) and anti-CD38 monoclonal antibodies (mAbs) in early lines of therapy has successfully extended median overall survival (OS) for patients with MM; however, most patients eventually relapse and require further treatment [2,3]. Increasingly, patients who have received at least three prior therapies, including an immunomodulatory drug, a PI and an anti-CD38 mAb (i.e., triple-class exposed [TCE]) are still fit enough to receive further lines of therapy after disease relapse. However, subsequent relapses become more difficult to treat and therefore clinical outcomes in heavily pretreated patients are limited [4]. For this reason, there is a need for new interventions with alternative mechanisms of action to improve the outcomes for TCE patients with relapsed and refractory MM (RRMM).
B cell maturation antigen (BCMA)-directed chimeric antigen receptor (CAR)-modified T cell therapies are among the novel treatment classes under investigation for patients with RRMM. One such CAR T cell therapy, idecabtagene vicleucel (ide-cel, bb2121), was evaluated in the pivotal, phase II, single-arm KarMMa clinical trial (NCT03361748), in TCE patients with RRMM who were refractory to their last regimen [5]. Patients received ide-cel at a target dose of either 150 × 106, 300 × 106 or 450 × 106 CAR+ T cells. Ide-cel demonstrated frequent, deep and durable responses in the KarMMa trial, with an overall response rate (ORR) of 73% and a median progression-free survival (PFS) of 8.8 months, as of 7 April 2020 (median follow-up: 15.4 months) [6]. OS was immature as of the data cut off date, with an estimated 15-month event-free rate for OS of 71%. In the subgroup of patients receiving the target dose of 450 × 106 CAR T cells, the ORR was 81% and the median PFS was 12.2 months [6]. Ide-cel (Abecma®; Celgene, a Bristol Myers Company) was recently approved by the US FDA for the treatment of TCE patients with RRMM who have received four or more prior lines of therapy [7]. Ide-cel has also been approved by the European Medicines Agency (EMA) for the treatment of adult patients with TCE RRMM who have received at least three prior therapies and have demonstrated disease progression on the last therapy [8].
Other novel RRMM treatments with distinct mechanisms of action include belantamab mafodotin (a BCMA-directed immunoconjugate) and selinexor (a selective inhibitor of nuclear export), both of which have been granted accelerated approvals by the FDA, the former for the same indication as ide-cel and the latter for patients who have received at least four prior therapies and with disease refractory to at least two immunomodulatory drugs, at least two PIs and an anti-CD38 mAb [9,10]. The efficacy and safety of these agents have been demonstrated in TCE patients in phase II clinical trials without any comparator arms [11,12] and have been indirectly compared with ide-cel in a separate matching-adjusted indirect comparison (MAIC) study [13].
The conventional care (CC) regimens traditionally used to treat RRMM show little benefit in the heavily pretreated population, with an ORR of 31.3% and with a median OS and PFS of 9.3 and 3.4 months, respectively [4]. Furthermore, there is no consensus on the best treatments for the heavily pretreated, TCE RRMM population [14,15]. In the absence of randomized controlled trials (RCTs) comparing ide-cel with CC in this population, an indirect comparison of ide-cel with CC using individual patient-level data (IPD) from the KarMMa trial for ide-cel and IPD from KarMMa-real-world population (RW) for CC was performed. KarMMa-RW reflects a global, real-world study of CC in a population similar to that of KarMMa [16]. In that study, Jagannath et al. [16] compared TCE patients who were refractory to their last line of treatment in KarMMa-RW (n = 190) with patients treated with ide-cel from KarMMa (n = 128), in terms of ORR, PFS and OS, using propensity score weighting and regression analysis to adjust for differences in the distribution of prognostic factors. In the absence of an RCT and given the prespecified design of KarMMa-RW to align with eligibility from KarMMa and the availability of IPD, this comparison reflects the most robust method to adjust for between-study differences in the assessment of the average treatment effect. Additional comparisons of clinical outcomes from the KarMMa trial versus those from other CC real-world studies may be of interest to decision-makers.
A systematic literature review of clinical trials and RW studies evaluating treatments in TCE patients with RRMM previously identified the MAMMOTH study [4,17], the largest (n = 249) retrospective, RW study of CC in patients from the USA whose disease had progressed on or after therapy with anti-CD38 mAbs. As this study was published in 2019, it is likely that the regimens patients received post-progression are representative of the CC currently used in routine clinical practice. MAMMOTH has also been used to represent CC in indirect comparisons of other novel treatments for TCE RRMM [18–21]. Since direct evidence was lacking for the comparison of ide-cel versus CC, the aim of the current study was to indirectly compare the efficacy of ide-cel with CC in TCE patients with RRMM. In the absence of a connected network of RCTs in TCE RRMM, a traditional network meta-analysis was not feasible, and an unanchored indirect treatment comparison (ITC) was warranted. Given that only aggregate-level data were available from the MAMMOTH study, a MAIC was conducted, using IPD from the KarMMa trial and published RW, aggregate-level data from MAMMOTH.
Patients & methods
Evidence for ide-cel
IPD were available from the KarMMa clinical trial [5], which enrolled 140 patients (the overall population), 128 of which were treated with ide-cel (the treated population) at a target dose of either 150 × 106 (n = 4), 300 × 106 (n = 70) or 450 × 106 (n = 54) CAR+ T cells. Based on the dose response, 450 × 106 CAR+ T cells reflects the target dose. As of the 7 April 2020 data cut off, the median duration of follow-up after ide-cel infusion was 15.4 months (range: 0.2–24.2), with 91 (71.1%) patients followed for at least 12 months from ide-cel treatment initiation. The primary outcome, ORR, was defined based on the International Myeloma Working Group (IMWG) criteria [22]. PFS was measured from the infusion time (treated population) and from the time of leukapheresis (overall population) until progressive disease (PD) or death. OS was measured from the time of ide-cel infusion (treated population) and the time of leukapheresis (overall population) until death due to any cause.
Evidence for CC
Publications regarding the efficacy of CC were identified through a systematic review of RW studies and clinical trials evaluating treatments for TCE patients with RRMM [17], which identified 11 RW studies. Of these, the results from the retrospective study MAMMOTH [4,23,24] had the largest sample size, reported Kaplan–Meier (KM) data for time-to-event outcomes, and had the highest overall study quality as evaluated by the Downs and Black risk of bias assessment tool. Data on patient characteristics and outcomes were obtained from the published MAMMOTH article [4]. For PFS and OS, the IPD were reconstructed using the Guyot algorithm based on the digitized survival percentages from the KM curves [25] and the corresponding number of patients at risk over time.
MAMMOTH was a retrospective chart review of patients with RRMM from 14 academic institutions in the USA who were refractory to daratumumab or isatuximab, administered alone or in combination, as part of a clinical trial or routine clinical practice. Patients with RRMM were required to have been treated for at least 4 weeks with a daratumumab- or isatuximab-containing regimen and with evidence of PD, as defined by the IMWG criteria [26,27], having progressed while on therapy or within 60 days after the last dose of the regimen. Time zero (T0) was defined as the time point when patients met the above criteria of progression. ORR was defined based on IMWG criteria [26,27]. PFS was measured from the onset of the next line of treatment until PD or death. OS was calculated from T0 until death and therefore included a period when patients were untreated before they began the next line of treatment.
Of the 275 patients included in MAMMOTH, 249 received at least one line of CC post-T0. These 249 patients formed the comparator group in MAMMOTH for this analysis. KM curves for OS and PFS were only presented for patients with available response data (228 out of the 249 patients) and were presented separately for each response level. The IPD reconstructed from KM curves were pooled for the OS and PFS outcomes to generate the respective KM dataset for the MAMMOTH population. An overview of baseline patient characteristics and study design for KarMMa and MAMMOTH is presented in both Table 1 & Supplementary Table 1.
| Characteristic | KarMMa (ide-cel-treated) (n = 128) | MAMMOTH (CC) (n = 249) |
|---|---|---|
| Age | ||
| Median (range), y | 60.5 (33–78) | 65 (27–90) |
| ≥65 y, n (%) | 45 (35) | ND |
| Race, n (%) | ||
| White | 103 (80) | 185 (74) |
| Black | 6 (5) | 38 (15) |
| Other | 19 (15) | 26 (10)† |
| Sex, male, n (%) | 76 (59) | 135 (54) |
| Years from initial diagnosis, median (range) | 6.0 (1.0–17.9) | 4.5 (0.4–19.4) |
| ISS stage at diagnosis, n (%)‡ | ||
| Stage I | 26/66 (39) | 63/212 (30) |
| Stage II | 22/66 (33) | 80/212 (38) |
| Stage III | 18/66 (27) | 69/212 (33) |
| Not evaluable | 62 | 37 |
| Immunoglobulin subtype, n (%) | ||
| IgG | 79 (62) | 130 (52) |
| IgA | 24 (19) | 51 (20) |
| Light chain | 19 (15) | 59 (24) |
| Other | 6 (5) | 9 (4) |
| Exposure to prior anti-myeloma regimens | ||
| Prior lines, median (range) | 6 (3–16) | 5 (2–17) |
| Bortezomib, n (%) | 125 (98) | ND |
| Carfilzomib, n (%) | 97 (76) | ND |
| Lenalidomide, n (%) | 128 (100) | ND |
| Pomalidomide, n (%) | 116 (91) | ND |
| Refractoriness to prior regimens, n (%) | ||
| Penta-refractory§ | 50 (39) | 63 (25) |
| Bortezomib | 78 (61) | 172 (69) |
| Carfilzomib | 85 (66) | 116 (47) |
| Ixazomib | 28 (22) | 31 (12) |
| Thalidomide | 22 (17) | 20 (8) |
| Lenalidomide | 97 (76) | 193 (78) |
| Pomalidomide | 100 (78) | 162 (65) |
| Elotuzumab | ND | 29 (12) |
| Daratumumab | 109 (85) | 230 (92) |
| Isatuximab | 13 (10) | 19 (8) |
| Prior autologous stem cell transplantation, n (%) | 120 (94) | 185 (74) |
| High-risk cytogenetic features, n (%)‡,¶ | 45/111 (41) | 71/229 (31) |
†
There were five Hispanic patients and 21 patients of other races in MAMMOTH.
‡
Percentages are calculated relative to the number of evaluable patients.
§
Refractory to one anti-CD38 monoclonal antibody, two proteasome inhibitors and two immunomodulatory drugs.
¶
t(4;14), t(14;16) or del17p.
CC: Conventional care; Ide-cel: Idecabtagene vicleucel; ISS: International Staging System; ND: Not determined; y: Years.
Patients in MAMMOTH received a range of different CC regimens, reflecting variation in the standard of care for TCE patients. Beyond outcomes for the treated population, median OS and PFS were reported for ten subgroups of patients according to various CC regimens (subgroups were not mutually exclusive). However, limited data on baseline patient characteristics were provided for these subgroups compared with the treated population. The following six subgroups represent the CC regimens that were most commonly received by patients evaluated in KarMMa-RW [16]. As such, these are among the most frequently used CC regimens in RW clinical practice and were relevant for this analysis: daratumumab + immunomodulatory drug (n = 41); elotuzumab + immunomodulatory drug (n = 19); carfilzomib + alkylator (n = 19); PACE-like regimens (where PACE is cisplatin, doxorubicin, cyclophosphamide and etoposide) (n = 24); daratumumab + PI (n = 13); and carfilzomib + immunomodulatory drug (n = 34). The remaining CC subgroups were not included in the analysis.
Patients in MAMMOTH were additionally categorized into groups defined by refractory status. OS data were presented for patients who were triple- or quad-refractory (n = 148), penta-refractory (n = 70) or non–triple-refractory (n = 57).
Matching-adjusted indirect comparisons
In the absence of an RCT comparing ide-cel with CC, unanchored ITCs were used to estimate the relative treatment effect between ide-cel and CC. Initially, the relative treatment effects were estimated without adjusting for any between-study differences – that is, a naive (unadjusted) ITC. Given the between-study differences identified (Supplementary Table 1), these differences were accounted for by means of a population-adjusted ITC.
As IPD were only available from KarMMa, an MAIC was used to adjust for between-study differences, as described in NICE Technical Support Document 18 [28]. This population-adjusted ITC uses IPD from the index trial (KarMMa) to match the distribution of baseline patient characteristics of the external study (MAMMOTH) [29]. A logistic propensity score model was used to reweight the IPD from KarMMa so that the weighted mean baseline characteristics matched those observed in MAMMOTH. Hazard ratios (HRs) and odds ratios (ORs) were then estimated for the comparison of ide-cel versus CC, using weighted logistic (for ORR) and weighted Cox (for OS and PFS) regression models, respectively. Robust estimates of the variance were calculated using sandwich estimators and presented as 95% CIs. For each outcome of interest, naive and adjusted treatment effects were estimated using a model without individual weights and a weighted MAIC model, respectively. Finally, the effective sample size (ESS) was calculated for each patient group in KarMMa to characterize the amount of overlap with the MAMMOTH population in terms of baseline patient characteristics [30]. All methods were consistent with the authors' previous study comparing KarMMa (ide-cel) with the STORM Part 2 (selinexor) and DREAMM-2 (belantamab mafodotin) clinical trials [13]. All analyses were performed using R version 4.0.4 (www.r-project.org).
Three patient groups were evaluated in KarMMa: the treated population (patients treated with ide-cel [n = 128] were included in the base case analysis for the comparisons of ORR, OS and PFS), whereas the overall population (n = 140) and the target-dose population (patients who received 450 × 106 CAR+ T cells [n = 54]) were considered as sensitivity analyses. For MAMMOTH, patients who received at least one line of CC treatment post-T0 (n = 249) constituted the comparator population. Finally, in another series of sensitivity analyses, PFS was compared between the ide-cel-treated population from KarMMa and the six relevant, individual CC subgroups from MAMMOTH; given the lack of KM data from these CC subgroups, only a qualitative comparison was made between the reweighted median PFS from the ide-cel-treated population (matched to each CC subgroup) and the observed median PFS from the comparator CC subgroups. Median OS was not reached for the ide-cel-treated population at the time of data cut-off; therefore, a sensitivity analysis was not conducted. Sensitivity analyses of OS were performed comparing the KarMMa populations with the triple-/quad-refractory and penta-refractory subgroups from MAMMOTH.
Selection of patient characteristics for propensity model
The prognostic factors to consider for inclusion in the MAIC model were identified by means of reviewing previously published ITCs in RRMM [16,31] and interviews with clinical experts. Of the identified prognostic elements, those with differences between KarMMa and MAMMOTH were included as covariates in the propensity model: median number of prior treatments, median time since diagnosis and refractoriness to carfilzomib, pomalidomide, bortezomib and lenalidomide. Prior autologous stem cell transplantation and high-risk cytogenetic features were initially included in the model but often precluded convergence and were therefore removed from the final model. Although International Staging System (ISS) staging was considered an important prognostic factor, it was not incorporated into the analyses, since data on ISS were collected at different time points in MAMMOTH (at diagnosis) and KarMMa (at treatment initiation) (Supplementary Table 1). A sensitivity analysis was conducted to explore the addition of sex, race and age to the model, as these covariates are commonly included in population-adjusted ITCs in oncology. None of the included covariates had missing data in KarMMa or in MAMMOTH overall population.
Limited patient characteristics were reported for the individual CC subgroups in MAMMOTH, which led to the inclusion of the median number of prior treatments and refractoriness to carfilzomib and to pomalidomide. Very few patients in the carfilzomib + alkylator and carfilzomib + immunomodulatory drug subgroups in MAMMOTH were refractory to carfilzomib; therefore, this variable was not included in the weighting algorithm for these two subgroups. Due to the very small sample sizes, weights were trimmed when matching to the individual CC subgroups in MAMMOTH so that weights greater than the 95% quantile were replaced with the 95% quantile.
Results
Baseline characteristics were well balanced between KarMMa and MAMMOTH following the matching process (Supplementary Table 2). The ESS was reduced by 48% (ESS: 67) for the ide-cel-treated population (base case), and by 46% (ESS: 75) and 38% (ESS: 33), respectively, for the overall and target-dose populations.
Compared with CC, ide-cel was associated with an improved clinical response in both the naive and adjusted comparisons (Table 2). The unadjusted ORR for the ide-cel-treated population was 73.4% compared with 31.3% for CC (OR: 6.06; 95% CI: 3.77–9.75 [Table 2]; equivalent to relative risk: 2.26; 95% CI: 1.78–2.87). The weighted MAIC resulted in similar estimates, with a slight reduction in the OR versus CC, which remained statistically significant (OR: 5.30; 95% CI: 2.96–9.51) (Table 2 & Figure 1). Compared with the ide-cel-treated population, the overall population showed slightly less improvement for ide-cel versus CC (OR: 3.94; 95% CI: 2.28–6.82), whereas results for the ide-cel 450 × 106 CAR+ T cell target-dose population demonstrated greater benefit in ORR versus CC (OR: 7.31; 95% CI: 3.06–17.46) based on the MAIC (Figure 2).
| KarMMa (ide-cel) | MAMMOTH (CC) | Ide-cel vs CC, OR HR (95% CI) | |||
|---|---|---|---|---|---|
| Observed (n = 128) | Matched to MAMMOTH (ESS = 67) | Observed (n = 249) | Naive comparison | MAIC | |
| ORR, % | 73.4 | 70.8 | 31.3 | OR: 6.06 (3.77–9.75) | OR: 5.30 (2.96–9.51) |
| Median PFS, months | 8.8 | 8.9 | 3.4 | HR: 0.50 (0.39–0.64) | HR: 0.50 (0.36–0.70) |
| 12–month PFS, % | 38.3 | 40.1 | 11.8 | ND | ND |
| Median OS, months | Not reached | Not reached | 9.9 | HR: 0.38 (0.28–0.53) | HR: 0.37 (0.25–0.56) |
| 12–month OS, % | 77.9 | 78.8 | 40.8 | ND | ND |
CC: Conventional care; CI: Confidence interval; ESS: Effective sample size; HR: Hazard ratio; Ide-cel: Idecabtagene vicleucel; MAIC: Matching-adjusted indirect comparison; ND: Not determined; OR: Odds ratio; ORR: Overall response rate; OS: Overall survival; PFS: Progression-free survival.
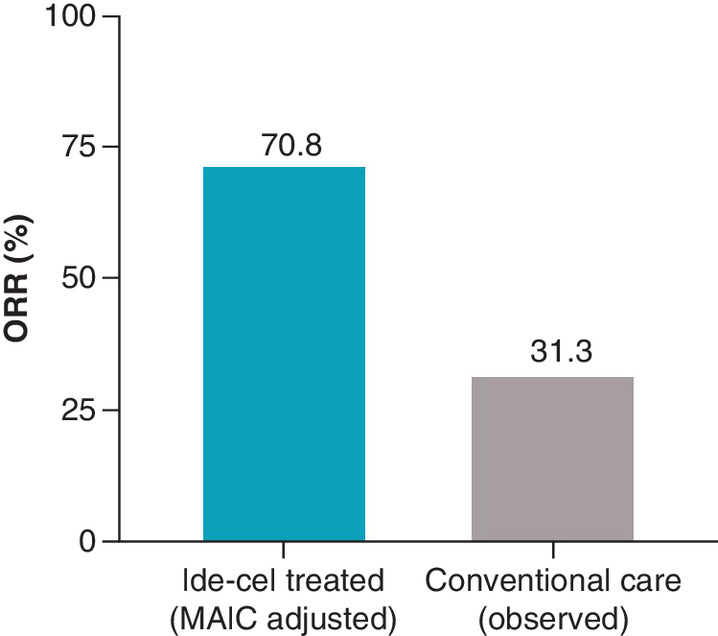
Figure 1. Overall response rate for the idecabtagene vicleucel-treated population (adjusted) versus conventional care (observed).
Ide-cel: Idecabtagene vicleucel; MAIC: Matching-adjusted indirect comparison; ORR: Overall response rate.
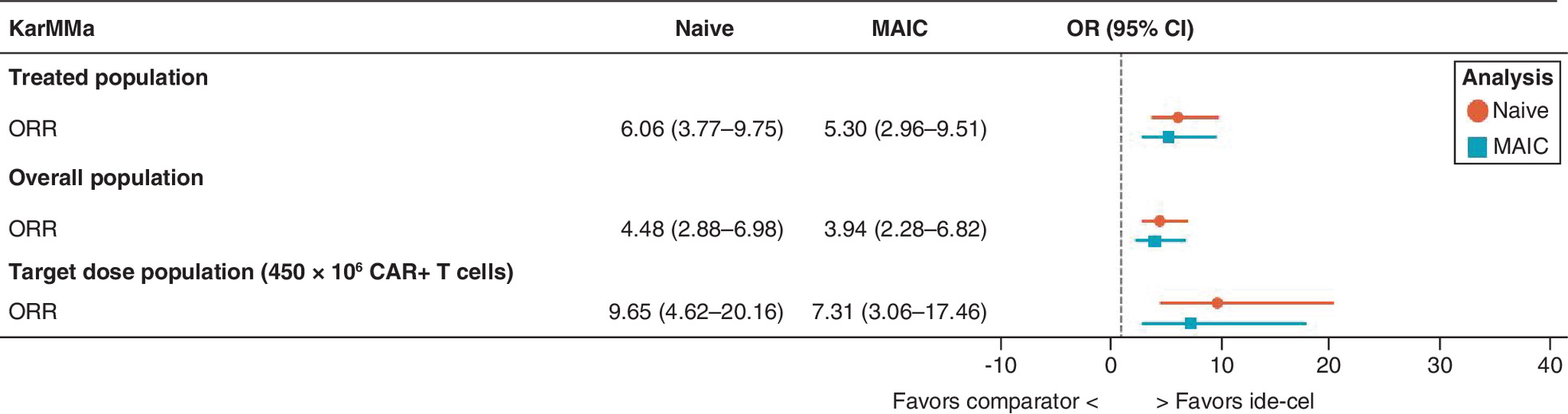
Figure 2. Odds ratio of overall response rate for idecabtagene vicleucel versus conventional care for the base case and sensitivity analyses.
CI: Confidence interval; CAR: Chimeric antigen receptor; Ide-cel: Idecabtagene vicleucel; MAIC: Matching-adjusted indirect comparison; OR: Odds ratio; ORR: Overall response rate.
The observed KM plots for PFS and OS shifted minimally in the MAIC adjustments for the ide-cel-treated population (Figure 3). For PFS, ide-cel demonstrated a greater improvement than CC (HR: 0.50; 95% CI: 0.36–0.70) based on the adjusted estimates for the ide-cel-treated population. Ide-cel was also associated with statistically significant improvements in OS versus CC (HR: 0.37; 95% CI: 0.25–0.56). Findings from the PFS and OS analyses were consistent across all three patient groups in KarMMa based on both the naive and adjusted estimates (Figure 4).
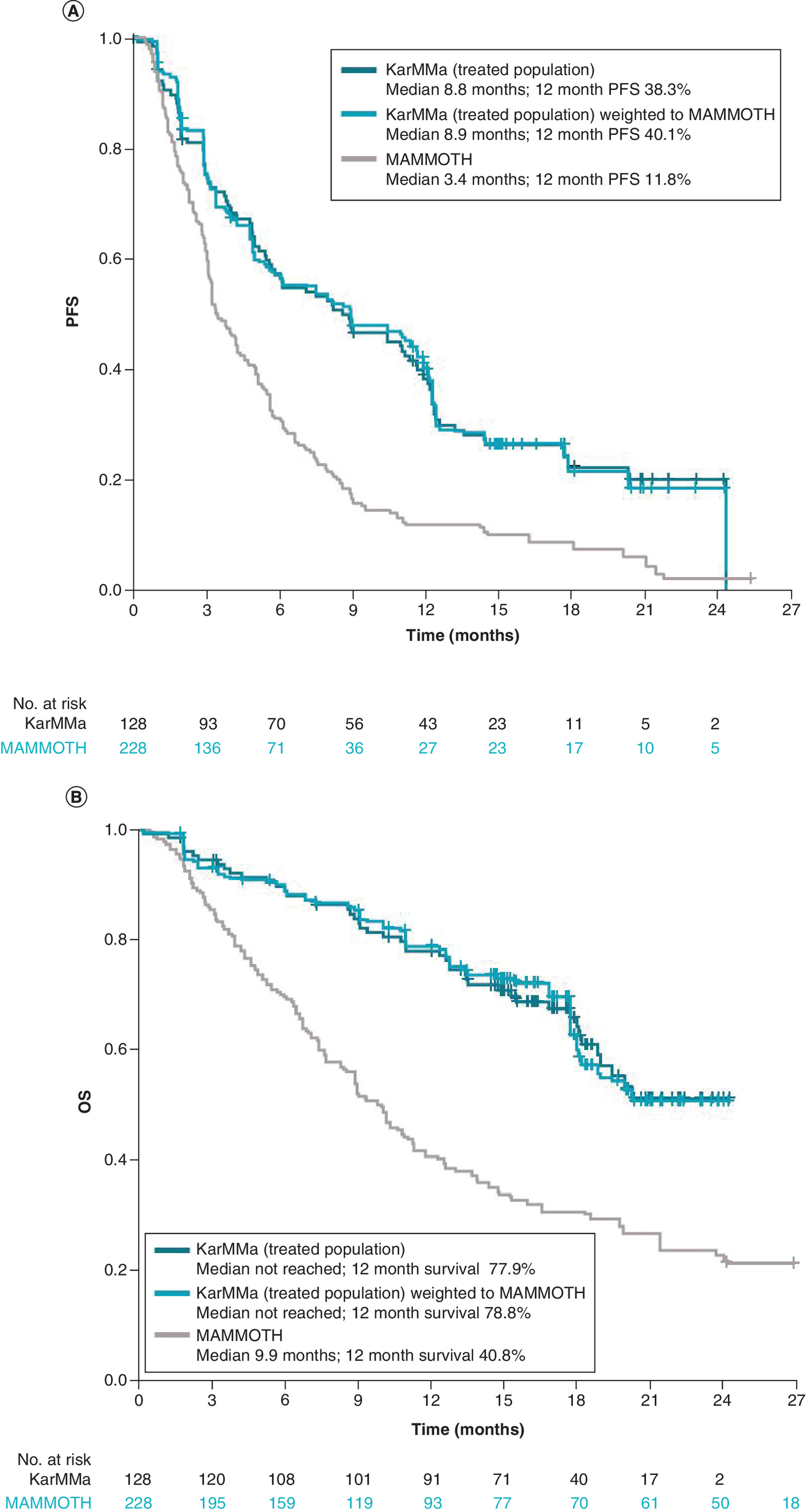
Figure 3. Kaplan–Meier plots for idecabtagene vicleucel-treated population (observed and adjusted) versus conventional care.
(A) Progression-free survival and (B) overall survival.
CI: Confidence interval; Ide-cel: Idecabtagene vicleucel; m: Month(s); OS: Overall survival; PFS: Progression-free survival.
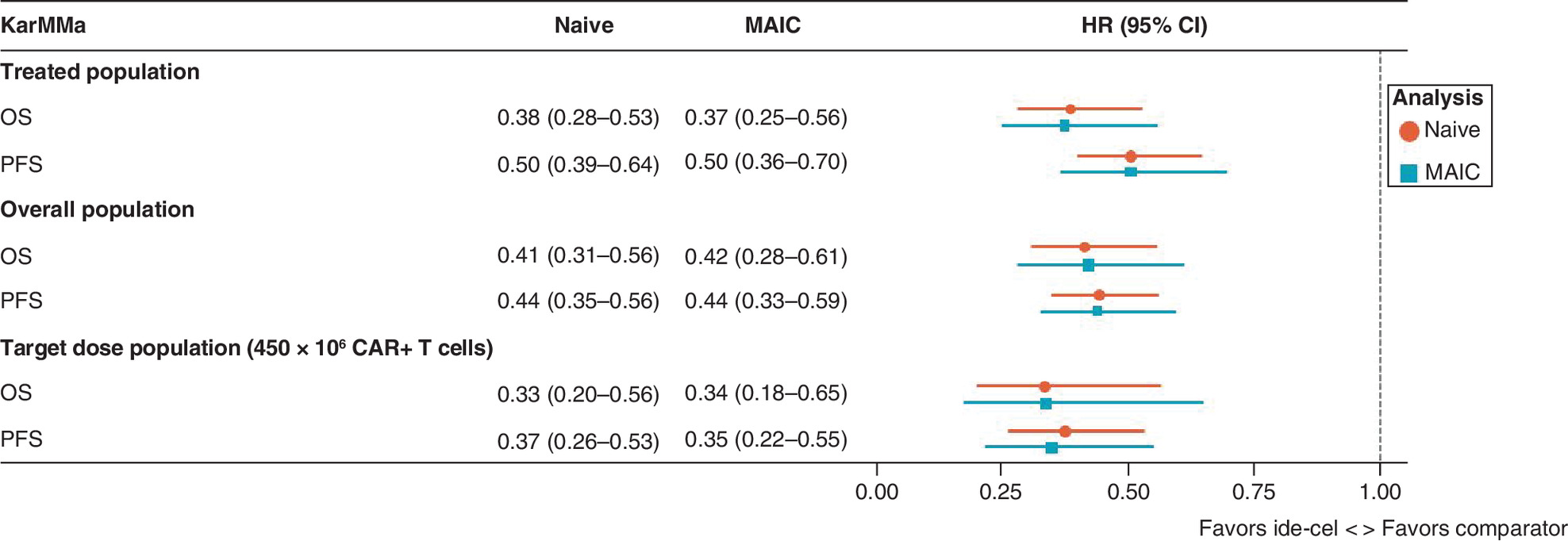
Figure 4. Hazard ratios of progression-free survival and overall survival for idecabtagene vicleucel versus conventional care for the base case and sensitivity analyses.
CAR: Chimeric antigen receptor; CI: Confidence interval; HR: Hazard ratio; Ide-cel: Idecabtagene vicleucel; MAIC: Matching-adjusted indirect comparison; OS: Overall survival; PFS: Progression-free survival.
In the sensitivity analyses for the individual CC subgroups in MAMMOTH, the ide-cel weighted median PFS was around 8.6 months for the ide-cel-treated population when matched to the CC subgroups (Table 3). The observed median PFS ranged from 1.8 months (daratumumab + PI) to 5.7 months (carfilzomib + alkylator) across the individual CC subgroups in MAMMOTH. No treatment effect was derived for these comparisons because only median values were reported for the individual CC subgroup in MAMMOTH, rather than the time-to-event data in a KM curve. The effect of ide-cel was more favorable when compared with the triple-/quad- and penta-refractory subsets of MAMMOTH patients as opposed to the treated population used in the base case (Supplementary Figures 1 & 2). Finally, results from the sensitivity analysis that additionally included sex, race and age as covariates were consistent with those of the base case model (results not presented).
| Daratumumab + IMiD® agent (n = 41) | Elotuzumab + IMiD agent (n = 19) | Carfilzomib + alkylator† (n = 19) | PACE-like regimens (n = 24) | Daratumumab + PI (n = 13) | Carfilzomib + IMiD agent† (n = 34) | |
|---|---|---|---|---|---|---|
| Individual CC subgroups | ||||||
| Observed median PFS, months (95% CI) | 4.5 (2.8–6.3) | 2.6 (1.1–4.1) | 5.7 (1.6–9.7) | 3.0 (2.5–3.4) | 1.8 (1.2–2.5) | 4.1 (3.1–5.1) |
| Ide-cel-treated population (n = 128)‡ | ||||||
| Weighted median PFS, months (95% CI) | 8.6 (5.4–12.2) | 8.6 (4.9–12.1) | 8.6 (4.9–12.1) | 8.6 (5.7–11.9) | 8.8 (5.8–11.9) | 8.6 (5.4–12.1) |
| Target dose of 450 × 106 CAR+ T cells (n = 54)‡ | ||||||
| Weighted median PFS, months (95% CI) | 12.2 (11.1–NE) | 11.3 (8.6–12.4) | 11.6 (8.6–13.1) | 12.1 (8.8–NE) | 11.3 (7.5–NE) | 12.1 (8.6–NE) |
†
Only median number of prior treatments and refractoriness to pomalidomide were adjusted for in this comparison.
‡
Observed median PFS, months: ide-cel-treated population; 8.8 and target dose of 450 × 106 CAR+ T cell; 12.2.
CAR: Chimeric antigen receptor; CC: Conventional care; CI: Confidence interval; Ide-cel: Idecabtagene vicleucel; IMiD®: Immunomodulatory drug, lenalidomide and pomalidomide; NE: Not estimable; PACE: Cisplatin, doxorubicin, cyclophosphamide and etoposide; PFS: Progression-free survival; PI: Proteasome inhibitor.
Discussion
This study showed that ide-cel was associated with clinically meaningful improvements in ORR, PFS and OS compared with CC in heavily pretreated patients with RRMM. These findings were consistent regardless of the analyzed patient group from KarMMa or the analysis approach (naive or MAIC-adjusted). Specifically, ide-cel was associated with improved ORR and estimated HRs for both PFS and OS across all KarMMa patient groups analyzed. Generally, the weighted MAIC estimates did not vary substantially from the naive comparisons, although the MAIC estimates tended to be slightly more uncertain, given the decrease in ESS across all patient groups. Although treatment effects were not derived for the sensitivity analyses versus individual CC subgroups in MAMMOTH due to lack of KM data, the weighted median PFS in the ide-cel-treated population was consistently longer than the observed values across the CC subgroups. In another sensitivity analysis, sex, race and age were additionally included in the model, which did not influence estimates substantially. Overall, findings from this study were consistent with the results from the authors' previous analysis of KarMMa versus MAMMOTH, which was based on shorter follow-up data from KarMMa [32].
While the definitions for ORR and PFS were generally consistent between KarMMa and MAMMOTH, the definition of OS was different between the two studies. In KarMMa, OS was measured from either the time of ide-cel infusion (treated population) or the time of leukapheresis (overall population); in MAMMOTH, it was calculated from the time of PD on daratumumab or isatuximab. This difference in the definition of OS favors MAMMOTH, since it additionally includes the time from PD on the last line of treatment until initiation of the next line of treatment for that study, which was not quantified in MAMMOTH. Therefore, the treatment effect estimates comparing ide-cel with CC in terms of OS may be conservative in this respect.
As previously mentioned, Jagannath et al. [16] incorporated IPD from the CC population from KarMMa-RW and the ide-cel-treated population from KarMMa to compare ide-cel versus CC in terms of ORR, PFS and OS. Similarly, the current study also incorporated IPD from KarMMa; however, for the comparator CC population, only aggregate data were available from MAMMOTH. Although the exact CC regimens were not specified in the USA-based MAMMOTH study [4], the most frequently used combinations of CC categories in MAMMOTH were broadly similar to those in the global KarMMa-RW study, which included some patients from Europe. Despite the mentioned differences, the estimated treatment effects between ide-cel and CC were similar between Jagannath et al. [16] (ORR relative risk: 2.4; PFS HR: 0.54; OS HR: 0.45) and the current analysis (ORR relative risk: 2.26; PFS HR: 0.50; OS HR: 0.37). Of note, in Jagannath et al. [16], the estimated average treatment effects (ATEs) were representative of the effect of treatments in an 'average' of the KarMMa and KarMMa-RW populations, whereas the current analysis could only assess the average treatment in control, since IPD were only available from KarMMa. This difference in the populations of the two analyses may help explain the slight differences between their estimates.
Another recent observational study in the RRMM population was conducted by Mehra et al. [33], which used the Flatiron MM core registry to investigate the treatment patterns and outcomes in 251 patients from the USA with triple-class refractory MM who went on to receive a subsequent line of treatment. Findings from that study [33] were similar to those of MAMMOTH and KarMMa-RW, in that the most common subsequent treatment regimens after achieving triple-class refractory status were elotuzumab-, pomalidomide- and carfilzomib-containing regimens. In addition, median PFS and OS from treatment initiation were 4.8 months and 11 months, respectively [33], similar to the results from MAMMOTH (3.4 months and 9.9 months, respectively). Furthermore, a recent ITC study [34] used MAICs to compare the efficacy of belantamab mafodotin versus selinexor plus dexamethasone and CC (using the MAMMOTH study) in patients with RRMM. Prawitz et al. [34] showed that belantamab mafodotin improved OS versus CC (covariate adjusted HR: 0.29; 95% CI: 0.16–0.54; p < 0.001). The margin of benefit observed in the current study was greater for comparison of ide-cel with CC (HR: 0.37; 95% CI: 0.25–0.56).
To ensure the variables included in the propensity score analyses were relevant for the clinical outcomes in the TCE RRMM, they were identified based on a review of previously published ITCs as well as clinical expert opinion. A total of six covariates were used, consistent with previous MAICs, as identified by Phillippo et al. [30]. Following adjustments for these covariates, the sample size reductions were 48% (ESS: 67) for the ide-cel-treated population and 46% (ESS: 75) and 38% (ESS: 33) for the overall population and target-dose population, respectively, similar to the ESS and percentage reduction reported for other recent MAICs in oncology [30]. It is noteworthy that the small ESS was associated with the target-dose population, which may be explained by its relatively small sample size in KarMMa. Although the target-dose population had similar overlap with the MAMMOTH population compared with the treated and overall populations, the MAIC estimates for the target-dose population should be interpreted with more caution, as the sample size and ESS of this subset are reasonably small. A larger sample size would strengthen these findings.
Although the methods used in this MAIC align with the existing recommendations from NICE [28], it is important to highlight that the analysis was limited to the published aggregate data from MAMMOTH. Having IPD for both independent studies is preferred, given that it provides more power, requires less severe assumptions and permits the exploration of alternative assumptions. Using the MAIC method, the efficacy of ide-cel could only be estimated in a population similar to that of MAMMOTH, whereas an IPD-to-IPD analysis could have estimated the efficacy of CC in a population similar to KarMMa or compared the efficacy of ide-cel and CC in an ‘average’ population (similar to the approach taken in Jagannath et al. [16]). Furthermore, without comparator IPD, the extent of residual bias in the treatment effect estimates could not be quantified and some confounding variables (e.g., ISS stage at treatment initiation, Eastern Cooperative Oncology Group performance status) likely remain unbalanced. Despite this, the present model did include indicators of prior treatment experience, which are among the most impactful prognostic elements in the heavily pretreated RRMM population [31]. It is also possible that differences in unmeasured factors persisted. The inclusion/exclusion criteria in a clinical trial are typically more stringent than in RW studies, and patients in MAMMOTH may have had a poorer health status or organ function than those enrolled in KarMMa, although these details were not clearly reported, which may have biased estimates. Finally, follow-up durations were limited in both studies; given the immaturity of the OS data in the ide-cel-treated population in KarMMa, it will be important to update the current analyses as longer follow-up data become available from that trial to better understand the long-term survival estimates.
Conclusion
Despite the known limitations of unanchored MAIC, results from the current study suggest that, when compared with CC, ide-cel offers meaningful improvements in efficacy outcomes that are important in the RRMM population. Results from the comparisons versus the overall CC population in MAMMOTH were consistent with those of the individual CC subgroups, suggesting ide-cel was superior regardless of the specific comparator CC regimen. There is an unmet need for novel treatments for heavily pretreated patients with RRMM, as evidenced by the poor outcomes achieved with CC in MAMMOTH and KarMMa-RW. The current study emphasizes the benefits of ide-cel, and CAR T cell therapy by extension, as a suitable candidate for the treatment of this population.
•
For patients with relapsed and refractory multiple myeloma (RRMM) who have been triple-class exposed to an immunomodulatory agent, a proteasome inhibitor and an anti-CD38 monoclonal antibody, outcomes are poor and there are limited therapeutic options.
•
Idecabtagene vicleucel (ide-cel), a B cell maturation antigen-directed chimeric antigen receptor (CAR) T cell therapy, showed frequent, deep and durable responses in this patient population in the pivotal, phase II, single-arm KarMMa trial.
•
In the current study, a matching-adjusted indirect comparison was conducted to compare the efficacy of treatment with ide-cel with traditional conventional care regimens in heavily pretreated patients with RRMM.
•
Individual-level data from the KarMMa trial and aggregate-level data from MAMMOTH, the largest independent observational study of conventional care regimens in the heavily pretreated RRMM population, were analyzed.
•
Three patient groups from KarMMa were evaluated: the ide-cel-treated population (n = 128) was included in the base analysis for comparison of overall response rate, overall survival and progression-free survival, while the overall population (n = 140) and the target-dose population (450 × 106 CAR+ T cells) (n = 54) were examined in sensitivity analyses.
•
Ide-cel offered clinically meaningful improvements versus conventional care in overall response rate (odds ratio: 5.30; 95% CI: 2.96–9.51), progression-free survival (hazard ratio: 0.50; 95% CI: 0.36–0.70) and overall survival (hazard ratio: 0.37; 95% CI: 0.25–0.56).
•
These findings were consistent across the three patient groups from KarMMa and across analysis approaches (naive or matching-adjusted indirect comparison-adjusted).
•
The current study highlights the benefits of ide-cel, and therefore CAR T cell therapy, as a suitable treatment option for heavily pretreated patients with RRMM.
Author contributions
Conception/design was performed by A Mojebi, D Ayers, S Cope, S Dhanasiri and D Dhanda. Provision of study material and patient data was performed by S Dhanasiri and D Dhanda. Collection and/or assembly of data was performed by A Mojebi, D Ayers and S Cope. Data analysis and interpretation were performed by N Shah, A Mojebi, D Ayers, S Cope, S Dhanasiri, FE Davies, P Hari, P Patel, K Hege and D Dhanda. Manuscript writing was performed by A Mojebi and S Cope. Final approval of the manuscript was provided by N Shah, A Mojebi, D Ayers, S Cope, S Dhanasiri, FE Davies, P Hari, P Patel, K Hege and D Dhanda.
Acknowledgments
The authors received editorial assistance in the preparation of this manuscript from N Burke of Excerpta Medica, funded by Bristol Myers Squibb. The authors are fully responsible for all content and editorial decisions for this manuscript.
Financial & competing interests disclosure
This study was supported by Bristol Myers Squibb. N Shah reports participation in advisory board for Amgen, CareDx, CSL Behring, GSK, Indapta Therapeutics, Karyopharm, Kite, Oncopeptides and Sanofi; research funding from Bluebird Bio, BMS (Celgene), Janssen, Nektar, Poseido, Precision Biosciences, Sutro Biopharma and Teneobio. A Mojebi, D Ayers and S Cope report employment with PRECISIONheor, which received funding from BMS for this study. D Dhanda, S Dhanasiri and P Patel report employment and equity from BMS. FE Davies reports consultancy fees from BMS (Celgene) and Janssen and participation in advisory boards for BMS (Celgene), Constellation, GSK, Janssen, Oncopeptides, Sanofi and Takeda. P Hari reports employment with Iovance Biotherapeutics; consultancy fees from Amgen, BMS, GSK, Karyopharm and Takeda; honoraria from Amgen, BMS, Janssen, Sanofi and Takeda; participation in advisory board for Millennium; and research funding from Amgen, BMS (Celgene), GSK, Millennium, Sanofi and Takeda. K Hege reports employment from BMS (Celgene); equity from Arcus Biosciences, BMS, Graphite Bio and Mersana Therapeutics; participation in board of directors for Graphite Bio and Mersana Therapeutics; and leadership or fiduciary role for Graphite Bio, Mersana Therapeutics and Society for the Immunotherapy of Cancer and reports patents planned, issued or pending for BMS. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors received editorial assistance in the preparation of this manuscript from N Burke of Excerpta Medica, funded by Bristol Myers Squibb.
Ethical conduct of research
Both KarMMa clinical trial (Munshi NC et al. N. Engl. J. Med. 384[8], 705–716 [2021]) and the MAMMOTH study (Gandhi UH et al. Leukemia 33[9], 2266–2275 [2019]) were conducted in accordance with the International Council for Harmonization guidelines for Good Clinical Practice and the principles of Declaration of Helsinki. The KarMMa protocol and associated amendments were approved by local or institutional review boards or ethics committees at participating sites. All patients provided informed consent. The MAMMOTH study received approval from the institutional review board of the coordinating institution (University of Alabama at Birmingham) and subsequently from all participating institutions. This research was waived from the obligation to obtain written informed consent.
Data sharing statement
Bristol Myers Squibb policy on data sharing may be found at www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
{kind=link}
{kind=link}
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
World Health Organization, International Agency for Research on Cancer (IARC). GLOBOCAN 2020: estimated multiple myeloma incidence, mortality and prevalence worldwide in 2020. IARC, Lyon, France (December 2020). Available at: https://gco.iarc.fr/today/data/factsheets/cancers/35-Multiple-myeloma-fact-sheet.pdf
2.
Braunlin M, Belani R, Buchanan J, Wheeling T, Kim C. Trends in the multiple myeloma treatment landscape and survival: a U.S. analysis using 2011–2019 oncology clinic electronic health record data. Leuk. Lymphoma 62(2), 377–386 (2021).
3.
Fonseca R, Abouzaid S, Bonafede M et al. Trends in overall survival and costs of multiple myeloma, 2000–2014. Leukemia 31(9), 1915–1921 (2017).
4.
Gandhi UH, Cornell RF, Lakshman A et al. Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia 33(9), 2266–2275 (2019).
•• Details outcomes of patients with multiple myeloma refractory to anti-CD38 monoclonal antibodies (MAMMOTH).
5.
Munshi NC, Anderson LD, Shah N et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N. Engl. J. Med. 384(8), 705–716 (2021).
•• Describes efficacy and safety data for patients with relapsed and refractory multiple myeloma treated with idecabtagene vicleucel in the pivotal, phase II KarMMa trial.
6.
Anderson LD, Munshi NC, Shah N et al. Idecabtagene vicleucel (ide-cel, bb2121), a BCMA-directed CAR T cell therapy, in relapsed and refractory multiple myeloma: updated KarMMa results. J. Clin. Oncol. 39(Suppl. 15), S8016 (2021).
• Outlines updated efficacy and safety results from the KarMMa trial.
7.
Celgene. ABECMA (idecabtagene vicleucel). Celgene Corporation, a Bristol Myers Squibb Company, Summit, NJ, USA (2021). Available at: https://packageinserts.bms.com/pi/pi_abecma.pdf
8.
Celgene. Abecma (idecabtagene vicleucel) [summary of product characteristics]. Celgene Europe B.V, Utrecht, Netherlands (25 August 2021). Available at: www.ema.europa.eu/documents/product-information/abecma-epar-product-information_en.pdf
9.
Karyopharm. XPOVIO (selinexor). Karyopharm Therapeutics, Inc., Newton, MA, USA (2019). Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2019/212306s000lbl.pdf
10.
GlaxoSmithKline. BLENREP (belantamab mafodotin-blmf). GlaxoSmithKline, Research Triangle Park, NC, USA (2020). Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2020/761158s000lbl.pdf
11.
Chari A, Vogl DT, Gavriatopoulou M et al. Oral selinexor-dexamethasone for triple-class refractory multiple myeloma. N. Engl. J. Med. 381(8), 727–738 (2019).
• Describes efficacy and safety data for patients with triple-class refractory multiple myeloma treated with oral selinexor-dexamethasone.
12.
Lonial S, Lee HC, Badros A et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): a two-arm, randomised, open-label, phase 2 study. Lancet Oncol. 21(2), 207–221 (2020).
• Outlines the safety and activity of belantamab mafodotin in heavily pretreated patients with relapsed or refractory multiple myeloma (DREAMM-2).
13.
Rodriguez-Otero P, Ayers D, Cope S et al. Matching adjusted indirect comparisons of efficacy outcomes for idecabtagene vicleucel (ide-cel, bb2121) versus selinexor + dexamethasone and belantamab mafodotin in relapsed and refractory multiple myeloma. Leuk. Lymphoma 62(10), 2482–2491 (2021).
14.
Moreau P, San Miguel J, Sonneveld P et al. Multiple myeloma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 28(Suppl. 4), iv52–iv61 (2017).
15.
Madduri D, Hagiwara M, Parikh K et al. Real-world treatment patterns, healthcare use and costs in triple-class exposed relapsed and refractory multiple myeloma patients in the USA. Future Oncol. 17(5), 503–515 (2021).
16.
Jagannath S, Lin Y, Goldschmidt H et al. KarMMa-RW: comparison of idecabtagene vicleucel with real-world outcomes in relapsed and refractory multiple myeloma. Blood Cancer J. 11(6), 116 (2021).
•• Describes a retrospective study (KarMMa-RW) comparing real-world outcomes in triple-class exposed patients with relapsed and refractory multiple myeloma with patients treated with idecabtagene vicleucel in KarMMa.
17.
Davies F, Rodriguez-Otero P, Weisel K et al. A systematic literature review to assess efficacy of treatments in triple-class exposed relapsed and refractory multiple myeloma patients. HemaSphere 4(Suppl. 1), S476 (2020).
• A systematic review of studies evaluating the efficacy of treatments for triple-class exposed patients with relapsed and refractory myeloma.
18.
Blade Creixenti J, Mateos MV, Oriol A et al. HORIZON (OP-106) versus MAMMOTH: an indirect comparison of efficacy outcomes for patients with relapsed/refractory multiple myeloma refractory (RRMM) to anti-CD38 monoclonal antibody therapy treated with melflufen plus dexamethasone versus conventional agents. Blood 136(Suppl. 1), S2–S4 (2020).
19.
Suvannasankha A, Kapetanakis V, Prawitz T et al. Assessing efficacy via indirect comparison of single-agent belantamab mafodotin (belamaf; GSK2857916) in DREAMM-2 versus STORM or MAMMOTH studies in relapsed/refractory multiple myeloma (RRMM). Clin. Lymphoma Myeloma Leuk. 20(Suppl. 1), S300–S301 (2020).
20.
Costa LJ, Hari P, Kumar SK et al. Overall survival of triple class refractory, penta-exposed multiple myeloma (MM) patients treated with selinexor plus dexamethasone or conventional care: a combined analysis of the STORM and MAMMOTH studies. Blood 134(Suppl. 1), S3125 (2019).
21.
Costa LJ, Lin Y, Martin TG et al. Cilta-cel versus conventional treatment in patients with relapse/refractory multiple myeloma. J. Clin. Oncol. 39(Suppl. 15), S8030 (2021).
22.
Kumar S, Paiva B, Anderson KC et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 17(8), e328–e346 (2016).
23.
Cornell R, Parameswaran H, Tang S et al. Real world vs. clinical trial outcomes of triple class refractory penta-exposed multiple myeloma (MM). Clin. Lymphoma Myeloma Leuk. 19(Suppl. 10), e115–e116 (2019).
24.
Cornell RF, Gandhi UH, Lakshman A et al. Subsequent treatment outcomes of multiple myeloma refractory to CD38-monoclonal antibody therapy. Blood 132(Suppl. 1), S2015 (2018).
25.
Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan–Meier survival curves. BMC Med. Res. Methodol. 12, 9 (2012).
26.
Durie BG, Harousseau JL, Miguel JS et al. International uniform response criteria for multiple myeloma. Leukemia. 20(9), 1467–1473 (2006).
27.
Rajkumar SV, Harousseau JL, Durie B et al. Consensus recommendations for the uniform reporting of clinical trials: report of the International Myeloma Workshop Consensus Panel 1. Blood 117(18), 4691–4695 (2011).
28.
Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU technical support document 18: methods for population-adjusted indirect comparisons in submission to NICE. National Institute for Health and Care Excellence (NICE) Decision Support Unit, Sheffield, UK (2016). Available at: http://nicedsu.org.uk/wp-content/uploads/2017/05/Population-adjustment-TSD-FINAL.pdf
29.
Signorovitch JE, Sikirica V, Erder MH et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health 15(6), 940–947 (2012).
30.
Phillippo DM, Dias S, Elsada A, Ades AE, Welton NJ. Population adjustment methods for indirect comparisons: a review of National Institute for Health and Care Excellence technology appraisals. Int. J. Technol. Assess. Health Care. 35(3), 221–228 (2019).
31.
Cope S, Toor K, Popoff E et al. Critical appraisal of published indirect comparisons and network meta-analyses of competing interventions for multiple myeloma. Value. Health 23(4), 441–450 (2020).
32.
Shah N, Ayers D, Davies FE et al. A matching-adjusted indirect comparison of efficacy outcomes for idecabtagene vicleucel (ide-cel, bb2121), a BCMA-directed CAR T cell therapy versus conventional care in triple-class-exposed relapsed and refractory multiple myeloma. Blood 136(Suppl. 1), S6–S7 (2020).
•• Findings from the authors' previous analysis of efficacy outcomes for KarMMa versus MAMMOTH, which was based on shorter follow-up (13.3 months) data from KarMMa.
33.
Mehra M, Vogel M, Valluri S et al. Patient characteristics, treatment patterns and outcomes in patients with triple class refractory multiple myeloma. HemaSphere 4(Suppl. 1), S475–S476 (2020).
34.
Prawitz T, Popat R, Suvannasankha A et al. DREAMM-2: indirect comparisons of belantamab mafodotin vs. selinexor + dexamethasone and standard of care treatments in relapsed/refractory multiple myeloma. Adv. Ther. 38(11), 5501–5518 (2021).
Information & Authors
Information
Published In
Pages: 737 - 749
PubMed: 35485211
Copyright
© 2022 Nina Shah. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 March 2022
Accepted: 13 April 2022
Published online: 29 April 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Indirect treatment comparison of idecabtagene vicleucel versus conventional care in triple-class exposed multiple myeloma. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0045
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Naresh Bumma, Hans C. Lee, Joshua Richter, James E. Hoffman, Jeffrey A. Zonder, Mirko Fillbrunn, Viviana Garcia-Horton, Zheng-Yi Zhou, Yingxin Xu, Heather Burnett, James Harnett, Timothy J. Inocencio, Michelle Little, Katherine Knorr, Glenn S. Kroog, Wanning Xu, Qiufei Ma, Sundar Jagannath, A systematic review of indirect treatment comparisons among recently approved chimeric antigen receptor T-cell and bispecific antibody therapies for triple-class exposed relapsed/refractory multiple myeloma, Current Medical Research and Opinion, 10.1080/03007995.2026.2686032, 42, 5, (971-985), (2026).
- Jing Christine Ye, Noa Biran, Sandhya Nair, Xiwu Lin, Keqin Qi, Eric M. Ammann, Thomas Renaud, Bonnie W. Lau, Jenny Zhang, Trilok Parekh, Kathleen S. Gray, Xinke Zhang, Luciano J. Costa, Relative Effectiveness of Talquetamab Versus Real-World Physician’s Choice Treatment Regimens in Patients With Relapsed/Refractory Multiple Myeloma: Updated Results From an Indirect Treatment Comparison, Clinical Lymphoma Myeloma and Leukemia, 10.1016/j.clml.2025.12.009, 26, 4, (e525-e535.e3), (2026).
- Lotte Delemarre, Isabelle Huys, Walter Van Dyck, Steven Simoens, Addressing clinical uncertainties in ATMP reimbursement: a review of methodological guidelines and European practice, Frontiers in Pharmacology, 10.3389/fphar.2026.1749386, 17, (2026).
- Melissa Alsina, Nina Shah, Sundar Jagannath, Jonathan L. Kaufman, David Siegel, Nikhil C. Munshi, Jacalyn Rosenblatt, Yi Lin, Andrzej J. Jakubowiak, Benjamin A. Derman, Aojun Li, Pingping Mao, Maeva Fincker, Ashish Yeri, Nathan Martin, Timothy B. Campbell, Olivia Finney, Anna Truppel-Hartmann, Fabio Petrocca, Jesus G. Berdeja, Noopur Raje, Anti–B-cell Maturation Antigen Chimeric Antigen Receptor T-cell Therapy bb21217 for Relapsed and Refractory Multiple Myeloma: Results from the Phase I CRB-402 Study, Cancer Immunology Research, 10.1158/2326-6066.CIR-24-0527, 14, 4, (528-542), (2026).
- Cyrille Touzeau, Brea Lipe, Abdullah M. Khan, Binod Dhakal, Sandhya Nair, Jianming He, João Mendes, Seina Lee, Carolina Lonardi, Ana Slaughter, Nikoletta Lendvai, Jordan M. Schecter, Diana Chen, Man Zhao, Tzu-min Yeh, Xavier Leleu, Noemí Puig, Dominik Dytfeld, Elena Zamagni, Katja Weisel, Lionel Karlin, Michel Delforge, Paolo Corradini, Roberto Mina, Wilfried Roeloffzen, Surbhi Sidana, Comparative Effectiveness of Ciltacabtagene Autoleucel in CARTITUDE-4 Versus Real-World Physician’s Choice of Therapy from the Flatiron Registry in Lenalidomide-Refractory Multiple Myeloma, Advances in Therapy, 10.1007/s12325-025-03308-2, 42, 10, (5023-5041), (2025).
- Jing Christine Ye, Noa Biran, Sandhya Nair, Xiwu Lin, Keqin Qi, Anil Londhe, Eric Ammann, Thomas Renaud, Colleen Kane, Trilok Parekh, Kathleen Gray, Steve Peterson, Luciano J. Costa, Talquetamab Versus Real-World Physician's Choice Treatment: Comparative Effectiveness in Patients With Triple-Class Exposed Relapsed/Refractory Multiple Myeloma, Clinical Lymphoma Myeloma and Leukemia, 10.1016/j.clml.2024.08.003, 25, 2, (124-134.e5), (2025).
- Ning Lyu, Zahra Majd, Bilqees Fatima, Zhen Zeng, Hua Chen, Susan Abughosh, Treatment refractoriness and response rates in patients with relapsed/refractory multiple myeloma: a retrospective analysis of real-world data, Cancer Treatment and Research Communications, 10.1016/j.ctarc.2025.100921, 43, (100921), (2025).
- Irene Strassl, CAR-T cell therapy for relapsed or refractory multiple myeloma in 2024—clinically available treatment options in Austria, memo - Magazine of European Medical Oncology, 10.1007/s12254-024-00996-4, 17, 4, (242-246), (2024).
- Dylan Maciel, Jeroen P. Jansen, Sven L. Klijn, Kevin Towle, Devender Dhanda, Bill Malcolm, Shannon Cope, Implementing Multilevel Network Meta-Regression for Time-To-Event Outcomes: A Case Study in Relapsed Refractory Multiple Myeloma, Value in Health, 10.1016/j.jval.2024.04.017, 27, 8, (1012-1020), (2024).
- Zainul S. Hasanali, Beatrice Razzo, Sandra P. Susanibar-Adaniya, Alfred L. Garfall, Edward A. Stadtmauer, Adam D. Cohen, Chimeric Antigen Receptor T Cells in the Treatment of Multiple Myeloma, Hematology/Oncology Clinics of North America, 10.1016/j.hoc.2023.12.004, 38, 2, (383-406), (2024).
- See more