Meta-analysis of visual pretreatment for the prevention of emergence delirium in children undergoing ophthalmic surgery
Publication: Journal of Comparative Effectiveness Research
Abstract
Objective: To evaluate the role of visual pretreatment in preventing emergence delirium in children receiving ophthalmic surgery. Methods: Four randomized controlled trials were identified in four databases, and a meta-analysis was conducted using RevMan 5.3. Results: The meta-analysis demonstrated a significantly lower incidence of postoperative emergence delirium (risk ratio: 0.39; 95% CI: 0.31–0.49) and propofol rescue (risk ratio: 0.29; 95% CI: 0.13–0.65) but comparable modified Yale Preoperative Anxiety Scale score (mean difference: -3.66; 95% CI: -9.96 to 2.65) and incidence of adverse events in the visual pretreatment group. Conclusion: Visual pretreatment is effective in preventing postoperative emergence delirium in children undergoing ophthalmic surgery without significant adverse effects and can also decrease the incidence of propofol rescue.
Emergence delirium (ED) is a self-limiting condition in which those affected become inconsolable, irritable and uncooperative [1]. ED has a high incidence, ranging from 10 to 80% [2–4]. ED is reported in both children and adults; however, an increased incidence is observed in children, especially preschool children in whom anesthesia is maintained via the inhalation of sevoflurane [5]. The exact mechanism of ED has not yet been clarified, but several risk factors have been found to be associated with an increased risk of ED, including inhalational anesthesia, postoperative pain, young age, preoperative anxiety, child temperament and male sex [6–8]. Ophthalmic surgery has also been demonstrated to be an important risk factor for the occurrence of ED [9,10]. Despite numerous advancements in mechanisms and techniques, the pathogenesis of ED has not yet been sufficiently clarified [11].
ED has been found to be associated with an increased risk of several adverse events, including suture dehiscence and accidental removal of intravenous catheters resulting from a confused state and negative postoperative behavior [12]. Moreover, ED may disturb other patients present in the postanesthesia care unit and be related to long-term sequelae [11]. Currently, several anesthetics and sedatives are used for the prevention of ED [11,13–15]; however, these agents have been observed to not only prolong postanesthesia care unit stay but also cause many adverse events, such as postoperative nausea and vomiting (PONV) and breath holding [11]. Therefore, several nonpharmacological methods have been recommended to prevent the occurrence of postoperative ED in pediatric anesthesia patients [16].
Considering that the eyes are covered with ointment and patches after ophthalmic surgery, visual disturbances after surgery have been speculated to be a contributor to ED [17,18]. Thus, the use of prophylactic eye coverings the day before surgery may play a positive role in reducing the incidence of postoperative ED [17]. Recently, several studies have evaluated the efficacy and safety of visual pretreatment in the prevention of postoperative ED in children undergoing ophthalmic surgery [17,19–21]. However, due to the insufficient number of participants in most studies [17,20,21], a reliable conclusion has not yet been achieved. Therefore, the authors performed the current meta-analysis to comprehensively evaluate the efficacy and safety of visual pretreatment for the prevention of postoperative ED in children undergoing ophthalmic surgery.
Methods
The current study was designed as a systematic review and meta-analysis, and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines [22] were used as a guide for reporting pooled results.
Literature sources
Eligible studies published up to October 2021 were independently identified by two reviewers using four databases: PubMed, Embase, the Cochrane Library and China National Knowledgement Infrastructure. The terms ‘visual pretreatment’ and ‘ED’ and their analogs were used to develop the basic search query. References of included studies were also independently checked by two reviewers to identify additional studies. The detailed search strategy used in the individual databases is described in Supplementary Table 1.
Selection criteria
The authors included studies based on the following characteristics: study design (randomized controlled trials fully published in English and Chinese), participants (preschool children with American Society of Anesthesiologists physical status 1 and 2 assigned to receive elective ophthalmic surgery), intervention (visual pretreatment) and outcomes (incidence of ED, modified Yale Preoperative Anxiety Scale [m-YPAS] score, incidence of propofol rescue and adverse events). The exclusion criteria were as follows: ineligible study design (e.g., case reports and comments), essential data missed and not provided by corresponding author and repeated reports of the same group.
Data extraction
Two reviewers independently extracted the relevant data from the eligible studies. Data included author names, publication year, country of origin, study duration, type of surgery, total number of participants, baseline patient characteristics (mean age, sex), details of intervention and control regimens, outcomes and details of methodological quality. For data that were reported as median and interquartile range, the authors estimated mean and standard deviation according to recognized formulas [23]. Disagreements were resolved through consulting a third reviewer. When necessary, the authors contacted the corresponding author to obtain additional information.
Definition of outcomes
The incidence of postoperative ED was regarded as the primary outcome in this meta-analysis and was defined as a peak score of ≥10 on the Pediatric Anesthesia ED scale [24], a score of ≥3 on the Watcha scale [25] or a score of ≥2 on the Nursing Delirium Screening Scale [26]. The level of preoperative anxiety and the incidence of propofol rescue and adverse events (recorded by individual study) were recognized as secondary outcomes. The level of preoperative anxiety was evaluated using m-YPAS [27]. The incidence of propofol rescue was defined as the proportion of patients requiring an additional dose of propofol for the treatment of severe agitation [17].
Quality assessment
Two independent reviewers used the Cochrane risk of bias tool [28] to assess the methodological quality of individual eligible studies based on seven items: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting and other bias. According to the criteria of the Cochrane tool, the bias risk of each item was labeled low, unclear or high.
Statistical analysis
Pooled estimates of categorical and continuous variables were expressed as risk ratio and mean difference, respectively. A 95% CI was used for each effect size. Cochran's Q statistic [29] was used to qualitatively assess statistical heterogeneity, and the I2 statistic [30] was used to quantify the level of statistical heterogeneity across studies. Nevertheless, the authors used a random effects model [31] to perform all statistical analyses regardless of the level of heterogeneity because variations between studies could not be ignored in real settings. The authors did not draw a funnel plot to inspect publication bias because an insufficient number of eligible studies were identified [32]. A p < 0.05 was considered to indicate a statistically significant difference. The authors used RevMan 5.3 software (Cochrane Collaboration, London, UK) to perform statistical analysis [33].
Results
Study retrieval & selection
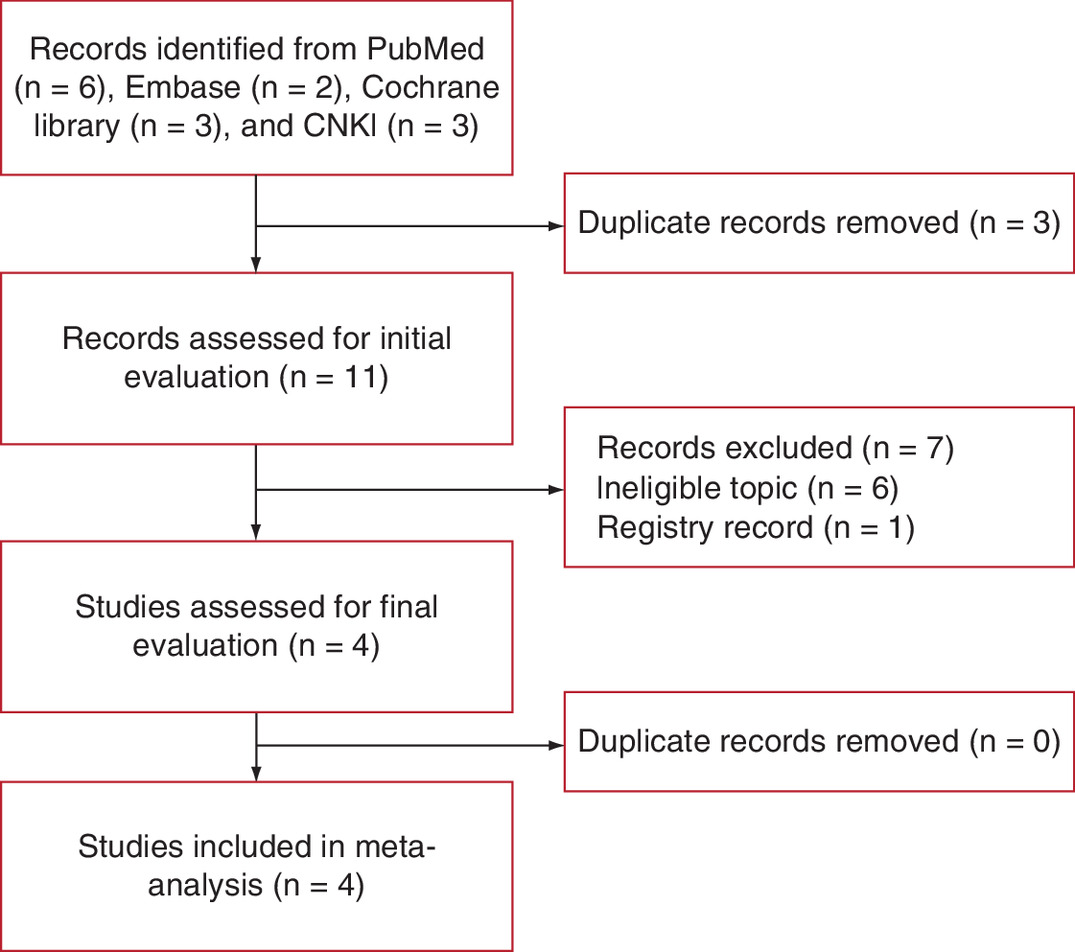
After initially searching four electronic databases, a total of 14 records were identified. The authors subsequently used literature management software (EndNote, Clarivate Analytics) to remove three duplicate records. Next, the authors excluded seven ineligible studies after carefully checking the titles and abstracts of the remaining 11 studies. At the final stage of the eligibility evaluation, no ineligible study was identified based on full texts. Finally, four studies involving 679 preschool children were included in the meta-analysis [17,19–21]. The process of study retrieval and selection is displayed in Figure 1.
Basic characteristics of the included studies
Of the four included studies, one was published in 2018 [17] and three were published in 2021 [19–21]. All included studies [17,19–21] were performed in China. The four included studies involved different types of surgeries. Three studies [17,19,21] were designed with two arms and one study [20] was designed with three arms. The sample size of the individual studies ranged from 95 to 279, with a total number of 679. The basic characteristics of the included studies are summarized in Table 1.
| Study | Country | Study duration | Condition | Group | Sample size (male/female) | Age, years | m-YPAS score | ED | Propofol rescue | PONV | Breath holding | SpO2 <95% | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lin, et al. | China | 01/2016–07/2017 | Cataract surgery | VP | 88 (47/42) | 5 | 37.9 ± 20.4 | 15 | 4 | 0 | 1 | 0 | [17] |
| C | 90 (51/39) | 4.8 | 39.0 ± 19.2 | 40 | 14 | 0 | 1 | 0 | |||||
| Wei, et al. | China | 01/2020–12/2020 | Strabismus surgery | VP | 46 (25/21) | 4.81 | n.a. | 9 | 3 | 2 | 2 | 1 | [21] |
| C | 49 (26/23) | 5.24 | n.a. | 27 | 11 | 4 | 2 | 1 | |||||
| Dong, et al. | China | 08/2019–07/2020 | Mixed | VP | 133 (73/60) | 4.84 | 36.36 ± 13.47 | 38 | n.a. | n.a. | n.a. | n.a. | [19] |
| C | 146 (76/70) | 4.8 | 45.45 ± 16.84 | 103 | n.a. | n.a. | n.a. | n.a. | |||||
| Liu, et al. | China | 06/2019–07/2020 | Bilateral chalazion resection | VP | 41 (22/19) | 3.4 | 35 ± 13 | 4 | n.a. | 0 | n.a. | n.a. | [20] |
| Dex | 43 (24/19) | 3.5 | 32 ± 9 | 5 | n.a. | 0 | n.a. | n.a. | |||||
| C | 43 (23/20) | 3.7 | 35 ± 10 | 13 | n.a. | 0 | n.a. | n.a. |
C: Control; Dex: Dexmedetomidine; ED: Emergence delirium; m-YPAS: Modified Yale Preoperative Anxiety Scale; n.a.: Not available; PONV: Postoperative nausea and vomiting; VP: Visual pretreatment.
Quality assessment of included articles
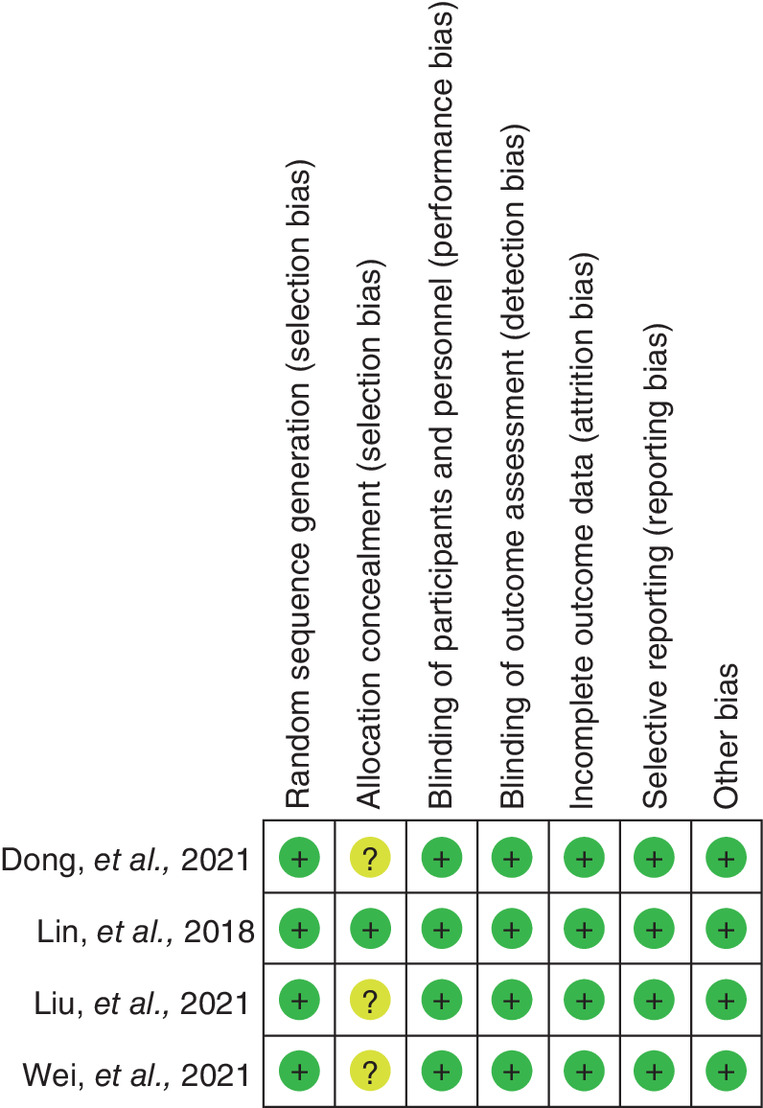
The Cochrane risk of bias tool was applied to assess the methodological quality of the four included articles, and the risk of bias summary is shown in Figure 2. Results suggested that all included studies [17,19–21] correctly generated a random sequence; however, only one study [17] reported the details of allocation concealment with the appropriate method. The authors labeled all included studies [17,19–21] with low risk of bias in performance bias because behaviors of participants and personnel could not bias outcomes. With regard to the remaining four items, the four included studies were deemed to have a low risk of bias. Overall, the methodological quality of the included studies was moderate to high.
Meta-analysis incidence of ED
All included studies [17,19–21] reported the incidence of postoperative ED. Based on results of the statistical heterogeneity examination, it was observed that there was no obvious statistical heterogeneity in the incidence of postoperative ED between the visual pretreatment and standard control groups (I2 = 0%; p = 0.96). The results revealed that the estimate of the incidence of postoperative ED in the visual pretreatment and standard control groups was 0.39 (95% CI: 0.31–0.49). In summary, the difference in the incidence of postoperative ED between both groups was statistically significant (21.43 vs 55.79%; Z = 8.09; p < 0.001) (Figure 3). In addition, one study investigated the comparative efficacy of visual pretreatment versus dexmedetomidine, and the meta-analysis suggested no statistical difference in terms of incidence of postoperative ED (risk ratio: 0.84; 95% CI: 0.24–2.91; p = 0.78).
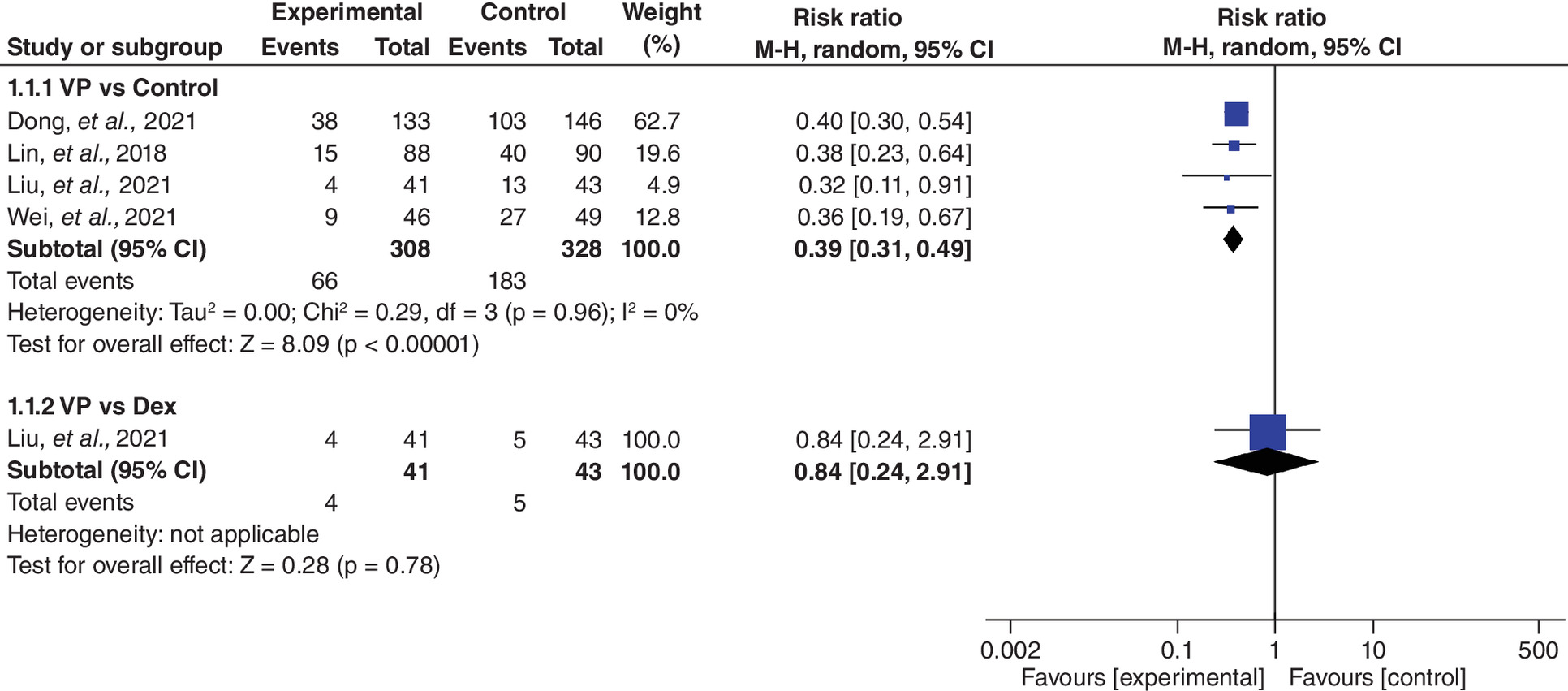
Figure 3. Forest plot of meta-analysis of the incidence of emergence delirium.
Dex: Dexmedetomidine; VP: Visual pretreatment; CI: confidence interval; M-H: Mantel-Haenszel.
Meta-analysis of m-YPAS score
The authors analyzed the differences in m-YPAS score between the visual pretreatment and standard control groups (Figure 4). Based on results of the heterogeneity examination, obvious statistical heterogeneity was detected in m-YPAS score between the two groups (I2 = 81%; p = 0.005). The results revealed that the pooled effect of the m-YPAS score in both groups was -3.66 (95% CI: -9.96 to 2.65). In summary, the m-YPAS score in the visual pretreatment group was numerically lower than that observed in the standard control group, although the difference was not statistically significant (Z = 1.14; p = 0.26). The meta-analysis also suggested no statistical difference in terms of m-YPAS score between the visual pretreatment and dexmedetomidine groups (mean difference: 3.00; 95% CI: -1.98 to 7.98; p = 0.24).
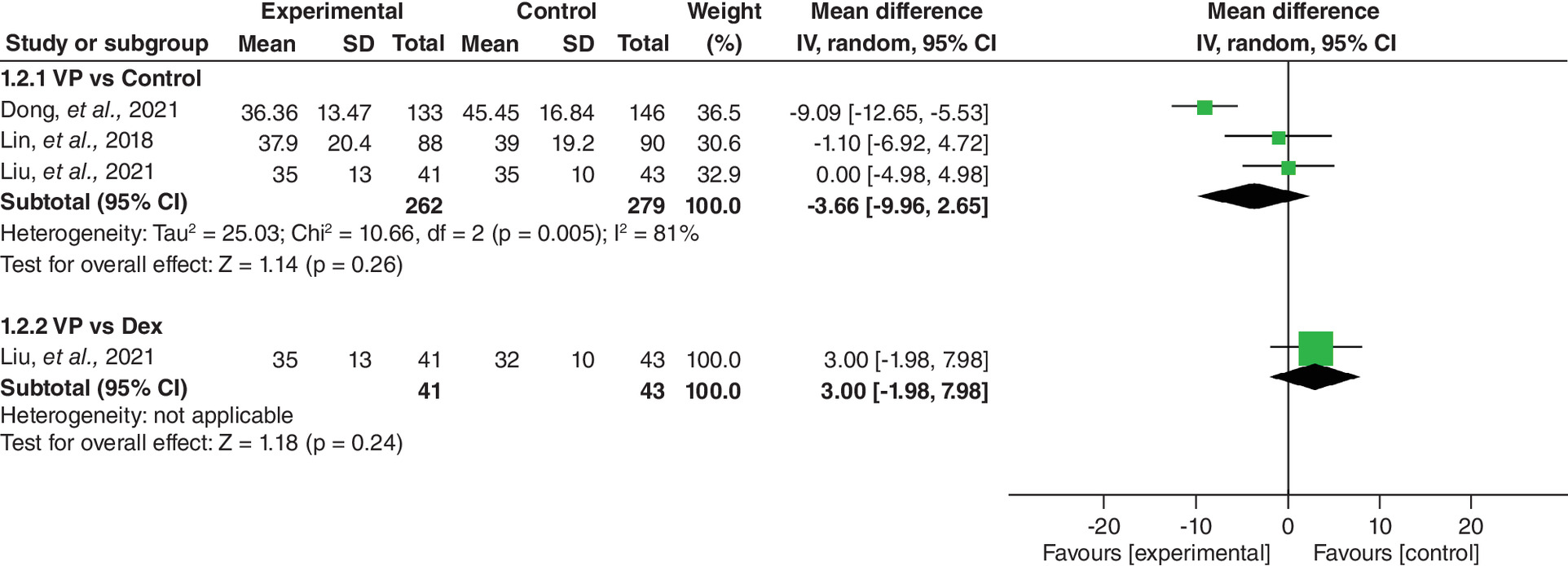
Figure 4. Forest plot of meta-analysis of modified Yale Preoperative Anxiety Scale scores.
Dex: Dexmedetomidine; VP: Visual pretreatment; IV: Inverse Variance.
Meta-analysis of incidence of propofol rescue
The authors compared and analyzed differences in the incidence of propofol rescue between the visual pretreatment and standard control groups (Figure 5). Statistical heterogeneity examination revealed no significant heterogeneity (I2 = 0%; p = 0.99), and results of the meta-analysis suggested a significantly lower incidence of propofol rescue in the visual pretreatment group compared with the standard control group (5.22 vs 17.99%; risk ratio: 0.29; 95% CI: 0.13–0.65; Z = 3.01; p = 0.003).

Figure 5. Forest plot of meta-analysis of incidence of propofol rescue.
M-H: Mantel-Haenszel; CI: confidence interval.
Meta-analysis of incidence of adverse events
Among included studies, three studies [17,20,21] reported the incidence of PONV, and two studies [17,21] reported the incidence of breath holding and SpO2 <95%. Statistical heterogeneity examinations did not detect obvious heterogeneity in terms of the incidence of PONV (heterogeneity not applicable), breath holding (I2 = 0%; p = 0.98) or SpO2 <95% (heterogeneity not applicable). Results of the meta-analyses revealed a comparable incidence between the visual pretreatment and standard control groups in terms of PONV (1.14 vs 2.20%), breath holding (2.24 vs 2.16%) and SpO2 (0.75 vs 0.72%) (Figure 6).
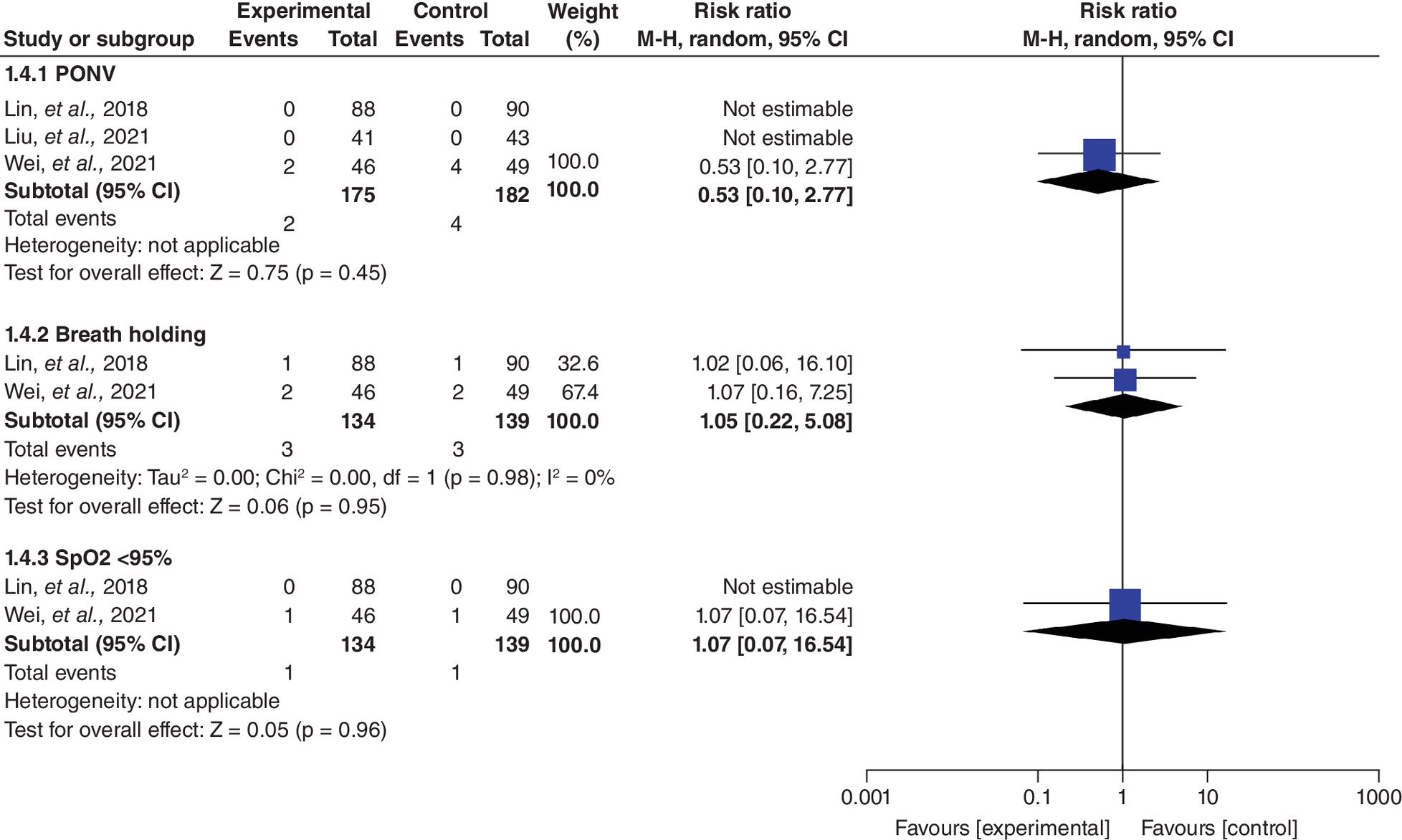
Figure 6. Forest plot of meta-analysis of incidence of adverse events.
PONV: Postoperative nausea and vomiting; SPO2: pulse oxygen saturation; CI: confidence interval; M-H: Mantel-Haenszel.
Discussion
Summary of main findings
ED is commonly observed in children undergoing pediatric anesthesia, especially preschool children maintained via the inhalation of sevoflurane [11]. Nonpharmacological methods have been suggested to reduce the incidence of postoperative ED because anesthetics and sedatives have been found to be associated with an increased risk of many undesirable side effects [16]. In the present meta-analysis of four eligible studies, the authors demonstrated that, as a nonpharmacological method, visual pretreatment is effective in decreasing the incidence of postoperative ED and propofol rescue without significant adverse effects in children undergoing ophthalmic surgery.
Potential reasons for results
Application of eye ointment and an eye patch after ophthalmic surgery may play a critically important role in the occurrence of postoperative ED [17]. Owing to immature neural development, visual disturbance has been considered to be the main reason for the high incidence of postoperative ED [34], and therefore visual pretreatment using an eye patch on the eyes the day before surgery has been speculated to have a positive impact on the occurrence of postoperative ED in children undergoing ophthalmic surgery [17,18]. All studies [17,19–21] included in the current meta-analysis consistently revealed a beneficial effect of visual pretreatment with regard to reducing the incidence of postoperative ED. The authors' meta-analysis further demonstrated the beneficial role of visual pretreatment in the prevention of postoperative ED through increasing statistical power after combining the results of individual studies [33]. It should be noted that the use of visual pretreatment is also comparable to dexmedetomidine in the prevention of postoperative ED [20]. Moreover, the authors' meta-analysis suggested that visual pretreatment significantly reduces the proportion of patients requiring propofol rescue, which further confirms the preventive efficacy of visual pretreatment for postoperative ED in children undergoing ophthalmic surgery.
Preoperative anxiety has been speculated to be associated with the occurrence of postoperative ED in children undergoing ophthalmic surgery [35]. To date, several studies have investigated the relationship between preoperative anxiety and the incidence of postoperative ED [11]; however, conflicting results were reported [36–38]. Of the three included studies [17,19,20] that reported preoperative anxiety, only one [19] reported a significant reduction in m-YPAS score in the visual pretreatment group. In this meta-analysis, the authors detected a greater reduction in m-YPAS score in the visual pretreatment group, although no statistical difference was observed. Moreover, Lin et al. suggested that preoperative anxiety was still an independent risk factor for postoperative ED [17], although preoperative anxiety scores were comparable between both groups studied. Thus, it is necessary to further clarify whether preoperative anxiety is related to the occurrence of postoperative ED in children undergoing ophthalmic surgery.
As mentioned previously, because pharmacological interventions are associated with a higher risk of adverse effects, several nonpharmacological methods have been developed and recommended for the alleviation of ED [16]. In the current meta-analysis, the authors detected a comparable incidence of PONV, breath holding and SpO2 <95% between the visual pretreatment and standard control groups, which further demonstrates the safety profile of visual pretreatment in practice.
Limitations & strengths
Certainly, the authors' meta-analysis has some limitations that should be further explained. First, as is the case with some studies, most included studies had a relatively insufficient sample size, which may introduce choice, biasing the authors' results. Second, only four eligible studies were included in this meta-analysis, which might weaken the robustness and credibility of the authors' findings. Third, although all included studies used visual pretreatment regimens as an intervention, a variety of components were used in the design of the visual pretreatment protocols (Table 2). Because of the insufficient number of eligible studies, the authors could not conduct subgroup analysis to eliminate the possible impact of components on pooled results. Fourth, various ophthalmic surgeries were utilized in the included studies, which may also introduce bias, negatively affecting the authors' results. Fifth, different scales were used to identify ED in all included studies, and it is impossible to eliminate the impact of scales on the pooled results. Sixth, all studies included in this meta-analysis were conducted in China, and therefore the authors' findings should be cautiously interpreted in different clinical settings. Seventh, the formal protocol of the present meta-analysis was not registered on a public platform; however, the authors performed this meta-analysis in strict accordance with the Cochrane handbook. In spite of these limitations, the authors' study has two major advantages: it is the first meta-analysis to systematically evaluate the efficacy and safety of visual pretreatment for the prevention of postoperative ED in children undergoing ophthalmic surgery, and a systematic literature search was utilized to significantly reduce the risk of reporting bias.
| Study | Group | Details of regimen | Ref. |
|---|---|---|---|
| Lin, et al., 2018 | VP | Prophylactic treatment with eye patch by covering the eye to be operated on for at least 3 h the day before surgery | [17] |
| C | Programmed explanation† | ||
| Wei, et al., 2021 | VP | Prophylactic treatment with eye patch by covering the eye to be operated on for 1 h 3 days before surgery | [21] |
| C | Programmed explanation† | ||
| Dong, et al., 2021 | VP | Prophylactic treatment with eye patch by covering the eye to be operated on the day before surgery | [19] |
| C | Programmed explanation† | ||
| Liu, et al., 2021 | VP | Prophylactic treatment with eye patch by covering the eye to be operated on 2 days before surgery | [20] |
| Dex | 0.5 μg/kg for 15 min | ||
| C | Programmed explanation† |
†
Discussion regarding how the surgery will be performed and what will happen after the surgery using words and cartoons.
C: Control; Dex: Dexmedetomidine; VP: Visual pretreatment.
Conclusion
A total of four relevant studies were included in this meta-analysis to systematically evaluate the clinical efficacy and safety of visual pretreatment for the prevention of postoperative ED. In summary, the results suggested that visual pretreatment can effectively reduce the incidence of postoperative ED and propofol rescue and can significantly reduce preoperative anxiety. In addition, visual pretreatment has a desirable safety profile. We therefore suggest the use of visual pretreatment in clinical practice, although more studies are required to clarify the association between preoperative anxiety and postoperative ED.
•
Emergence delirium (ED) is a self-limiting condition in which those affected become inconsolable, irritable and uncooperative.
•
ED has a high incidence, especially in children.
•
Pediatric ophthalmic surgery has also been demonstrated to be an important risk factor for the occurrence of ED.
•
A significantly high risk of adverse events limits the clinical application of anesthetics and sedatives for the prevention of ED.
•
Prophylactic eye coverings the day before surgery may play a positive role in reducing the incidence of postoperative ED, as visual disturbances after surgery have been speculated to be a contributor to ED.
•
Visual pretreatment is considered to be an easy-to-use and inexpensive nonprophylactic eye covering strategy.
•
Several original studies investigating the role of visual pretreatment in the prevention of ED in children undergoing ophthalmic surgery have reported conflicting findings.
•
This meta-analysis included four eligible randomized controlled trials and suggested that visual pretreatment significantly lowers the incidence of postoperative ED and propofol rescue.
•
However, no statistical difference was observed between visual pretreatment and control strategies in terms of modified Yale Preoperative Anxiety Scale score and incidence of adverse events.
Author contributions
D She designed the study, wrote the original draft and reviewed and edited the manuscript. Z-Y Wang designed the study, wrote the original draft and reviewed and edited the manuscript. F Wu reviewed and edited the manuscript as well as English usage. Y-Q Zhang reviewed and edited the manuscript. Q Ao supervised and reviewed the manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (supplementary materials.docx)
- Download
- 14.00 KB
References
Papers of special note have been highlighted as: • of interest
1.
Malarbi S, Stargatt R, Howard K, Davidson A. Characterizing the behavior of children emerging with delirium from general anesthesia. Paediatr. Anaesth. 21(9), 942–950 (2011).
• Interesting study for this meta-analysis.
2.
Doerrfuss JI, Kramer S, Tafelski S, Spies CD, Wernecke KD, Nachtigall I. Frequency, predictive factors and therapy of emergence delirium: data from a large observational clinical trial in a broad spectrum of postoperative pediatric patients. Minerva Anestesiol. 85(6), 617–624 (2019).
3.
Card E, Pandharipande P, Tomes C et al. Emergence from general anaesthesia and evolution of delirium signs in the post-anaesthesia care unit. Br. J. Anaesth. 115(3), 411–417 (2015).
• Interesting study for this meta-analysis.
4.
Lin Y, Chen Y, Huang J et al. Efficacy of premedication with intranasal dexmedetomidine on inhalational induction and postoperative emergence agitation in pediatric undergoing cataract surgery with sevoflurane. J. Clin. Anesth. 33, 289–295 (2016).
5.
Goa KL, Noble S, Spencer CM. Sevoflurane in paediatric anaesthesia: a review. Paediatr. Drugs 1(2), 127–153 (1999).
• Interesting study for this meta-analysis.
6.
Mason KP. Paediatric emergence delirium: a comprehensive review and interpretation of the literature. Br. J. Anaesth. 118(3), 335–343 (2017).
7.
Kain ZN, Caldwell-Andrews AA, Mayes LC et al. Family-centered preparation for surgery improves perioperative outcomes in children: a randomized controlled trial. Anesthesiology 106(1), 65–74 (2007).
8.
Frederick HJ, Wofford K, De Lisle Dear G, Schulman SR. A randomized controlled trial to determine the effect of depth of anesthesia on emergence agitation in children. Anesth. Analg. 122(4), 1141–1146 (2016).
9.
Chen JY, Jia JE, Liu TJ, Qin MJ, Li WX. Comparison of the effects of dexmedetomidine, ketamine, and placebo on emergence agitation after strabismus surgery in children. Can. J. Anaesth. 60(4), 385–392 (2013).
10.
Cho EJ, Yoon SZ, Cho JE, Lee HW. Comparison of the effects of 0.03 and 0.05 mg/kg midazolam with placebo on prevention of emergence agitation in children having strabismus surgery. Anesthesiology 120(6), 1354–1361 (2014).
11.
Grotmol OG, Nesarajah N, Hansen TG. Postoperative emergence delirium in children: a narrative review of recent publications. Signa Vitae 17(3), 10–20 (2021).
12.
Hilly J, Hörlin AL, Kinderf J et al. Preoperative preparation workshop reduces postoperative maladaptive behavior in children. Paediatr. Anaesth. 25(10), 990–998 (2015).
13.
Patel A, Davidson M, Tran MC et al. Dexmedetomidine infusion for analgesia and prevention of emergence agitation in children with obstructive sleep apnea syndrome undergoing tonsillectomy and adenoidectomy. Anesth. Analg. 111(4), 1004–1010 (2010).
14.
Kim MS, Moon BE, Kim H, Lee JR. Comparison of propofol and fentanyl administered at the end of anaesthesia for prevention of emergence agitation after sevoflurane anaesthesia in children. Br. J. Anaesth. 110(2), 274–280 (2013).
15.
Rosen HD, Mervitz D, Cravero JP. Pediatric emergence delirium: Canadian pediatric anesthesiologists' experience. Paediatr. Anaesth. 26(2), 207–212 (2016).
16.
Aldecoa C, Bettelli G, Bilotta F et al. European Society of Anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur. J. Anaesthesiol. 34(4), 192–214 (2017).
• Interesting study for this meta-analysis.
17.
Lin Y, Shen W, Liu Y et al. Visual preconditioning reduces emergence delirium in children undergoing ophthalmic surgery: a randomised controlled trial. Br. J. Anaesth. 121(2), 476–482 (2018).
18.
Xie YQ, Cai JL. Effects of cognitive behavioral therapy on fear and pain in preschoolers during wound suture removal. Mod. Clin. Nurs. 10(4), 10–12 (2011).
• Interesting study for this meta-analysis.
19.
Dong PF, Qiao DN, Chen HL et al. Study on the effects of eye-covering pretreatment on acute delirium after ophthalmic surgery with general anesthesia in pre-school aged children. Chin. J. Emerg. Crit. Care Nurs. 2(2), 106–111 (2021).
• Interesting study for this meta-analysis.
20.
Liu G, Liu ZN, Wang HS, Lin Y, Tao J, Liu C. Effects of visual pretreatment on the prevention of emergence delirium from general anesthesia in children undergoing ophthalmic operation. Int. J. Anaesthesiol. Resusc. 42(04), 351–354 (2021).
• Interesting study for this meta-analysis.
21.
Wei W, Sun ZT, Zhang ZM et al. Prevention of emergence delirium using eye shading pretreatment in preschool children after strabismus surgery. Zhengzhou Da Xue Xue Bao Yi Xue Ban 56(5), 727–730 (2021).
22.
Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
23.
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 14, 135 (2014).
24.
Aouad MT, Yazbeck-Karam VG, Nasr VG, El-Khatib MF, Kanazi GE, Bleik JH. A single dose of propofol at the end of surgery for the prevention of emergence agitation in children undergoing strabismus surgery during sevoflurane anesthesia. Anesthesiology 107(5), 733–738 (2007).
25.
Bajwa SA, Costi D, Cyna AM. A comparison of emergence delirium scales following general anesthesia in children. Paediatr. Anaesth. 20(8), 704–711 (2010).
26.
Gaudreau JD, Gagnon P, Harel F, Tremblay A, Roy MA. Fast, systematic, and continuous delirium assessment in hospitalized patients: the nursing delirium screening scale. J. Pain Symptom Manage. 29(4), 368–375 (2005).
27.
Kain ZN, Mayes LC, Cicchetti DV, Bagnall AL, Finley JD, Hofstadter MB. The Yale Preoperative Anxiety Scale: how does it compare with a ‘gold standard’? Anesth. Analg. 85(4), 783–788 (1997).
28.
Higgins JP, Altman DG, Gotzsche PC et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343, d5928 (2011).
29.
Bowden J, Tierney JF, Copas AJ, Burdett S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med. Res. Methodol. 11, 41 (2011).
30.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat. Med. 21(11), 1539–1558 (2002).
31.
Kanters S. Fixed- and random-effects models. Methods Mol. Biol. 2345, 41–65 (2022).
32.
Page MJ, McKenzie JE, Higgins JPT. Tools for assessing risk of reporting biases in studies and syntheses of studies: a systematic review. BMJ Open 8(3), e019703 (2018).
33.
Dersimonian R, Laird N. Meta-analysis in clinical trials. Control. Clin. Trials 7(3), 177–188 (1986).
34.
Vlajkovic GP, Sindjelic RP. Emergence delirium in children: many questions, few answers. Anesth. Analg. 104(1), 84–91 (2007).
35.
Kim J, Kim SY, Lee JH, Kang YR, Koo BN. Low-dose dexmedetomidine reduces emergence agitation after desflurane anaesthesia in children undergoing strabismus surgery. Yonsei Med. J. 55(2), 508–516 (2014).
36.
Takzare A, Sadrossadat H, Sanatkar M, Roustaie S, Goudarzi M. Effect of ondansetron on post-anesthesia delirium in sevoflurane-anesthetized children undergoing eye surgery in Farabi Hospital in 2015. Int. J. Pharm. Res. 11, 1781–1785 (2019).
37.
Kain ZN, Caldwell-Andrews AA, Maranets I et al. Preoperative anxiety and emergence delirium and postoperative maladaptive behaviors. Anesth. Analg. 99(6), 1648–1654 (2004).
38.
Berghmans JM, Poley M, Weber FVDVM et al. Does the child behavior checklist predict levels of preoperative anxiety at anesthetic induction and postoperative emergence delirium? A prospective cohort study. Minerva Anestesiol. 81(2), 145–156 (2015).
Information & Authors
Information
Published In
Pages: 679 - 688
PubMed: 35531783
Copyright
© 2022 Future Medicine Ltd.
History
Received: 24 February 2022
Accepted: 13 April 2022
Published online: 9 May 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Meta-analysis of visual pretreatment for the prevention of emergence delirium in children undergoing ophthalmic surgery. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0037
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Sunyu Tang, Jikai Liu, Zheng Ding, Ting Shan, The effect of dexmedetomidine on emergence delirium of postanesthesia events in pediatric department: A systematic review and meta-analysis of randomized controlled trials, Medicine, 10.1097/MD.0000000000039337, 103, 36, (e39337), (2024).
- Xiaoxia Shi, Lili Su, Yue Sun, Caixia Ma, Zhiwen Wang, Non-pharmacological interventions for preventing emergence delirium in children under general anesthesia: A scoping review, Journal of Pediatric Nursing, 10.1016/j.pedn.2024.03.014, 77, (e38-e53), (2024).
- Yi-Chen Chen, Jann Foster, Man-Ling Wang, Iftitakhur Rohmah, Yu-Hsin Tseng, Hsiao-Yean Chiu, Global prevalence and risk factors of emergence delirium in pediatric patients undergoing general anesthesia: A systemic review and meta-analysis, Journal of Pediatric Nursing, 10.1016/j.pedn.2024.03.010, 77, (74-80), (2024).
- Xinyu Cao, Bei Wang, Meinv Liu, Jianli Li, Effect of recorded mother's voice on emergence delirium in pediatric patients: a systematic review with meta-analysis, Jornal de Pediatria, 10.1016/j.jped.2023.08.008, 100, 3, (231-241), (2024).
- Debas Yaregal Melesse, Tadesse Teshale Tesema, Zemenay Ayinie Mekonnen, Wubie Birlie Chekol, Biruk Adie Admass, Misganaw Mengie Workie, Predictors of postoperative delirium in paediatric patients undergoing surgery under general anaesthesia at Amhara Regional State Tertiary Hospitals: a multicenter prospective study, Frontiers in Pediatrics, 10.3389/fped.2024.1348789, 12, (2024).