Burden of tyrosine kinase inhibitor failure in Chinese chronic myeloid leukemia patients: a systematic literature review
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To conduct a systematic literature review of real-world evidence on the burden of tyrosine kinase inhibitor (TKI) failure in Chinese patients with chronic myeloid leukemia (CML). Methods: We identified 155 references in Chinese- and English-language journals from 2001 to 2021. Results: The age-adjusted mortality rate in Chinese CML patients was decreasing. Imatinib treatment had a higher annual treatment failure risk than nilotinib (0.199 vs 0.041). Patients with TKI treatment failure tended to be young (median: 38.6 years), have progressive disease (44.3%) and harbor BCR-ABL1 mutations (51.6%). The disease burden of TKI treatment failure included reduced health outcomes and increased health resource utilization and costs. Conclusion: CML relapse cases could continuously rise in China due to increasing TKI treatment failure over extended survival.
Chronic myeloid (myelogenous) leukemia (CML) is characterized by an increased, unregulated growth of myeloid cells in the bone marrow and subsequent accumulation of such cells in the blood [1]. The discovery of the Philadelphia chromosome, a balanced genetic translocation associated with CML, led to the development of imatinib [2], the first generation of tyrosine kinase inhibitor (TKI) treatment, which has significantly decreased morbidity and mortality in patients with CML [3]. However, the emergence of drug resistance, intolerance and nonadherence (i.e., treatment failure) in long-term TKI treatment imposes a formidable challenge in managing CML [4].
First-generation (1G) TKI imatinib was recommended as standard care for patients with newly diagnosed CML in China shortly after its 2002 approval [5]. Increasing treatment with imatinib and second-generation (2G) TKIs in Chinese patients with CML has reduced hematopoietic stem-cell transplantation (HSCT) from 29.6% in 2007 to 8% in 2016 [6]. However, up to one-third of patients with CML develop drug resistance or intolerance to first-line (1L) treatment with imatinib [7]. In addition, patients with the BCR-ABL1 kinase domain ‘gatekeeper’ T315I mutation [8] are highly resistant to the three TKIs approved in China (i.e., imatinib, nilotinib, dasatinib), and the disease management with all TKIs can be further complicated by compound mutations [9]. Although HSCT continues to play a role in managing CML secondary to TKI treatment failure, the access to HSCT for Chinese patients with CML is often limited by strict eligibility requirements and prohibitively high costs.
To date, no systematic literature review (SLR) has assessed the potentially wide-ranging dimensions of TKI treatment failure among patients with CML in mainland China. Therefore the aim of the present SLR was to evaluate real-world evidence (RWE) reflecting the disease burden and unmet medical needs of Chinese patients with CML that fails to respond to TKIs or is intolerant of these medications. These consequences include treatment responses, health-related quality of life (HRQoL), health resource utilization (HRU) and costs.
Materials & methods
We consulted the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Statement (http://www.prisma-statement.org/PRISMAStatement/) to design this SLR. In brief, we conducted a literature search of major English- and Chinese-language bibliographic databases of RWE studies from published, peer-reviewed articles concerning the disease burden and unmet medical needs of Chinese patients with CML and TKI treatment failure. Treatment failure was in turn defined as primary and secondary drug resistance or treatment intolerance associated with TKIs for CML since the approval of imatinib for treating CML in mainland China in 2002.
This SLR included real-world studies reporting: the epidemiology of CML; treatment failure and BCR-ABL1 mutations associated with the three approved TKIs for CML in China (imatinib, nilotinib and dasatinib); patient characteristics; disease progression; treatment information; treatment outcomes; HRQoL; HRU; and direct medical costs in Chinese patients with CML and TKI treatment failure.
Bibliographic databases & literature search strategies
We conducted a literature search of four major English bibliographic databases (MEDLINE, Embase, Web of Science and the Cochrane Library) and three major local bibliographic databases in mainland China (WANFANG, VIP and China National Knowledge Infrastructure). The publication date range was from 1 January 2001 (year of initial approvals of imatinib) to 16 June 2021 (date of original literature searches). Literature search strategies were developed to meet the requirements of indexed databases and searched study types, which included CML epidemiological studies and observational studies reporting evidence related to TKI treatment failure. Search strings used to search English bibliographic databases are listed in Supplementary Table 1.
Study eligibility
We assessed study eligibility using the population, intervention, comparator, outcome, study design criteria to maximize the inclusion of RWE studies with evidence indicating disease burden and unmet medical needs in Chinese patients with CML and TKI treatment failure. Included studies: implemented an observational study design (i.e., retrospective, cross-sectional or prospective); reported epidemiological data on CML (e.g., age-standardized incidence, age-standardized mortality); provided information on treatment failure and BCR-ABL1 mutation associated with currently approved 1G and 2G TKIs in mainland China; and/or summarized patient characteristics, disease prognosis, treatment information, treatment outcomes, HRQoL, HRU and costs for Chinese patients with CML and TKI treatment failure.
We excluded studies that: included patients with other (non-CML) hematological malignancies or experienced failure with treatments other than TKIs; did not involve RWE studies, including clinical trials (phase I, II, III and/or randomized controlled trials), preclinical (in vivo or in vitro) studies, case studies, case reports, non-original research articles (e.g., correspondence, editorials, commentaries, overviews, summaries, communications, consensus guidelines) and reviews; and/or lacked relevant evidence to extract.
Data extraction
Two research associates (HH and LT) conducted study eligibility assessments and data extraction by reviewing the full publications of the references meeting both the defined inclusion and exclusion criteria. Any disagreements between the two research associates during the process of study eligibility assessment and data extraction were resolved by consulting with the project lead (WC).
Excel-based data extraction forms were used to collect the following information from eligible articles: study design; study cohorts; epidemiological data (e.g., age-standardized incidence, age-standardized mortality); occurrence of TKI treatment failure; reasons for TKI treatment failure; distribution of BCR-ABL1 kinase domain mutations; patient demographic data, including distribution of disease phases (classified as chronic phase [CP], accelerated phase [AP] and blast phase [BP]), disease prognostic risk, previous TKI treatment and comorbidities; disease prognosis (disease progression from CP-CML to AP- or BP-CML, or overall survival [OS] in patients with AP- or BP-CML); treatment information (treatment setting, switched TKI treatments, HSCT, treatment compliance); treatment response outcomes including major molecular response (MMR), complete cytogenetic response (CCyR), progression-free survival, OS, disease-free survival, treatment adverse effects and complications of HSCT; HRQoL (health status, measurement instrument, measurement outcomes); HRU (outpatient visits, hospital admissions, hospital length of stay); and direct medical costs (health status, costing time periods, currency year, cost classifications). All costs were adjusted to the local currency in 2020 using the historical annual inflation rate in mainland China.
Newcastle–Ottawa Scale (NOS) scores were used to assess the quality of the included studies (high quality: NOS score 7–9; moderate quality: NOS score 4–6; low quality: NOS score 0–3) [10]. Publication bias of the conducted meta-analysis was assessed by funnel plot. We did not contact corresponding authors for additional or missing information because we seldom received a response to such requests in our previous literature review projects.
Evidence synthesis
Extracted data were synthesized using single-arm meta-analysis with a random effects model, which fully considers the uncertainty weighted by study sample sizes, for applicable data from more than one study. If extracted data were unsuitable for single-arm meta-analysis (e.g., owing to lack of standard deviation for continuous outcomes), the weighted mean or median method was used for pooled estimation. Original results from a single study were reported if evidence synthesis was not feasible. Time-to-event outcomes, including risk of TKI treatment failure, BCR-ABL1 kinase domain gene mutation and survival outcomes associated with switched TKI treatments and HSCT, were converted to annual risk using exponential survival functions before using the single-arm meta-analysis for pooled estimation. No sensitivity analyses were conducted in this SLR. The evidence synthesis analyses were conducted using statistical software R (v. 4.0; https://www.r-project.org/).
Results
Study selection
Outcomes of the literature search process for each type of evidence (epidemiology, treatment outcomes, HRQoL and costs) are illustrated in Figure 1. We identified the following types of studies: 204 epidemiological, 1120 with treatment outcomes, 302 with HRQoL data and 172 with cost information. After excluding irrelevant references by screening titles and abstracts, we identified 332 references for full publication review to determine further study eligibility. A total of 155 references after the exclusion of duplicated references (26 English- and 129 Chinese-language references) met the prespecified eligibility criteria and were included for data extraction and evidence synthesis.

Figure 1. Literature search process for real-world studies reporting evidence reflecting the disease burden of tyrosine kinase inhibitor treatment failure in Chinese patients with chronic myeloid leukemia.
CML:chronic myeloid leukemia
Epidemiology of CML
Four studies reported epidemiological outcomes of CML in mainland China [11–14]. One used the Global Burden of Disease Study 2017 as a data source and reported age-standardized incidence and age-standardized mortality of CML in mainland China in 1990 and 2017 [11]. The age-standardized incidences of CML for those two years were highly comparable: 0.16 per 100,000 in 2017 versus 0.19 per 100,000 in 1990. In contrast, age-standardized annual mortality in 2017 (0.06 per 100,000) was decreased by approximately one-half (46.2%) compared with 1990 (0.13 per 100,000).
Risk of TKI treatment failure
Pooled annual risks of treatment failure, drug resistance and drug intolerance of the three TKIs in Chinese patients with CML are shown in Figure 2. 21 studies reported treatment failure associated with imatinib in 4094 treatment-naive patients with CML [15–35]. The pooled annual risk of treatment failure associated with 1L imatinib was 0.199 (95% CI: 0.115–0.323), that for drug resistance was 0.097 (95% CI: 0.065–0.142) and that for treatment intolerance was 0.023 (95% CI: 0.013–0.042). Four studies with 119 patients reported that second-line (2L) nilotinib was associated with greater annual risks of treatment failure (0.277 vs 0.041) and drug resistance (0.198 vs 0.016) compared with 1L nilotinib [17,36–38]. The pooled annual risk of treatment intolerance associated with use of 2L nilotinib was 0.061 (95% CI: 0.022–0.157).
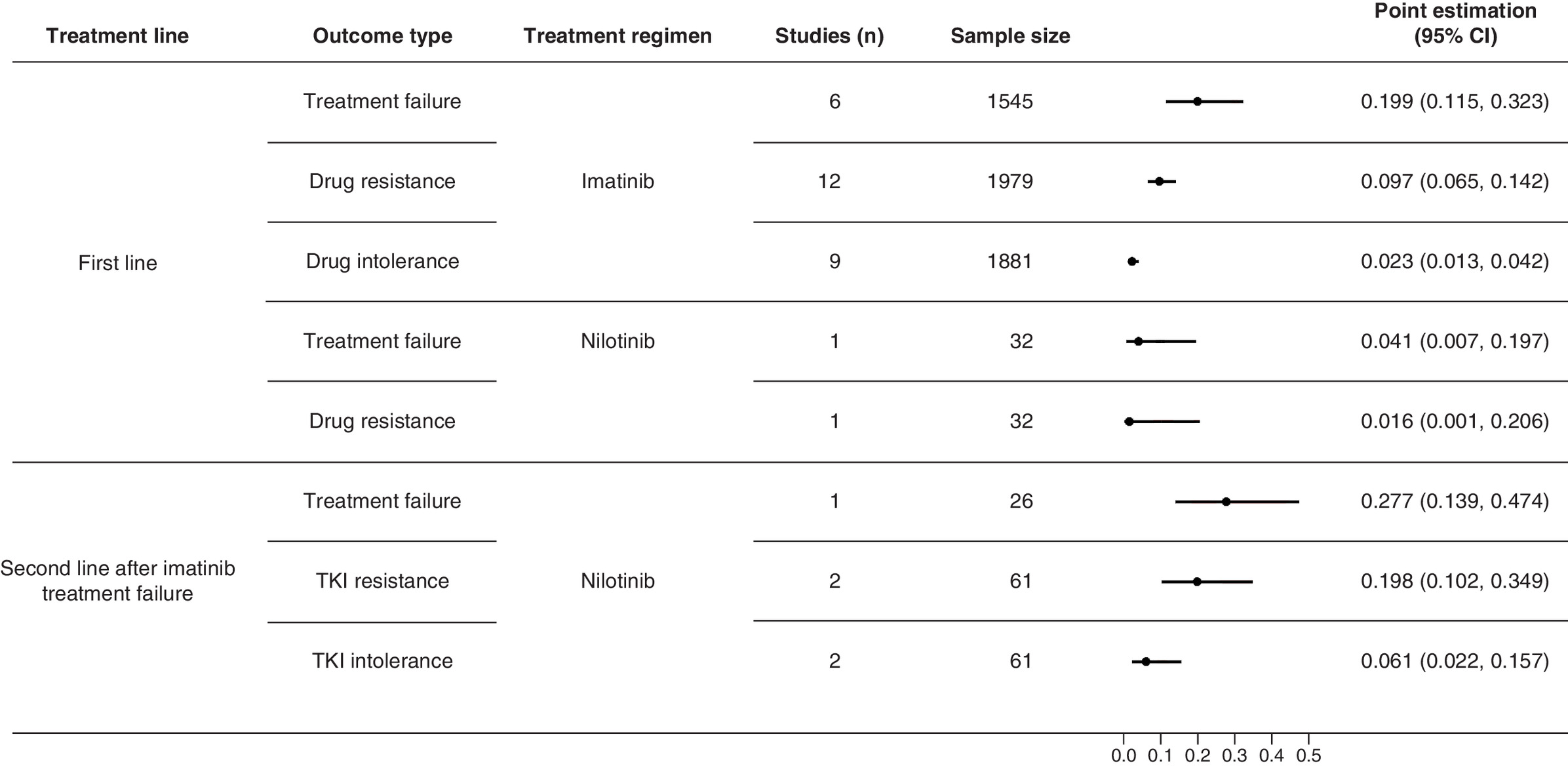
Figure 2. Pooled annual risks of tyrosine kinase inhibitor treatment failure, drug resistance and drug intolerance associated with imatinib, nilotinib and dasatinib in Chinese patients with chronic myeloid leukemia.
TKI: Tyrosine kinase inhibitor.
Pooled annual risks of BCR-ABL1 kinase domain point mutations for the three TKIs in varied treatment settings are illustrated in Figure 3. Five studies reported the risk of any BCR-ABL1 kinase domain gene mutation associated with 1L imatinib (0.218; 95% CI: 0.176–0.268), nilotinib (0.187; 95% CI: 0.064–0.438), 2L dasatinib after failing imatinib (0.083; 95% CI: 0.021–0.279) and third-line (3L) dasatinib after failing imatinib and nilotinib (0.208; 95% CI: 0.089–0.413) [39–43]. The risk of T315I mutation was assessed in patients with CML receiving imatinib, nilotinib or dasatinib in varied treatment settings. 2L nilotinib was associated with the greatest annual risk of T315I mutation (0.068; 95% CI: 0.028–0.159). This evidence indicated that previously treated patients were likely to have a higher risk of developing the T315I mutation than treatment-naive patients. According to the included studies, drug resistance was the predominant reason for 1L imatinib treatment failure (90.8%) and 2L nilotinib failure (85.3%) [17,18,36–38,40,42–49].

Patient characteristics & disease progression in patients with failed TKI treatment
Pooled baseline characteristics of Chinese patients with CML and TKI treatment failure are summarized in Table 1. Patients with CML and TKI treatment failure were overall young (median: 38.6 years) and predominantly male (64.3%; 95% CI: 62.6–66.1%) [17,19,23,36–61]. Most had CP-CML (71.2%) and prior imatinib treatment only (60.5%). Large minorities of patients had a high prognostic risk index (44.3%) and at least one comorbidity (37.1%), which included cardiovascular diseases and metabolic syndrome (10.3%). A total of 51.6% of patients had any BCR-ABL1 kinase domain gene mutation. Of these, T315I was the predominant genetic variant (observed in 10.6% of patients with TKI treatment failure).
| Patient characteristic | Studies (n) | Sample size | Point estimation | 95% CI | ||
|---|---|---|---|---|---|---|
| Demographics | Median age | 17 | 2649 | 38.6 | ||
| Male proportion | 20 | 2902 | 64.3% | 62.6% | 66.1% | |
| Sokal score | Low risk | 7 | 174 | 24.1% | ||
| Intermediate risk | 31.6% | |||||
| High risk | 44.3% | |||||
| Disease phase | CP | 10 | 584 | 71.2% | ||
| AP | 16.3% | |||||
| BP | 12.5% | |||||
| Previous TKI treatment | Imatinib | 8 | 1615 | 60.5% | ||
| Nilotinib | 19.0% | |||||
| Dasatinib | 19.0% | |||||
| Imatinib and nilotinib | 1.5% | |||||
| ABL kinase region point mutation | Any mutation | 19 | 1900 | 51.6% | 32.5% | 70.3% |
| T315i | 9 | 1626 | 10.6% | 6.5% | 16.9% | |
| F359V/I | 2 | 143 | 9.1% | 5.4% | 15.0% | |
| Y253H | 10 | 570 | 8.4% | 6.4% | 11.0% | |
| E255K/V | 5 | 1368 | 7.5% | 4.5% | 12.3% | |
| F359V/C/I | 2 | 941 | 7.4% | 4.6% | 11.5% | |
| Y253F/H | 2 | 1162 | 6.7% | 2.6% | 16.3% | |
| Comorbidity | Any comorbidity | 2 | 1209 | 37.1% | 26.7% | 48.8% |
| Cardiovascular diseases/metabolic syndrome | 1 | 116 | 10.3% | 6.0% | 17.3% | |
AP: Accelerated phase; BP: Blast phase; CP: Chronic phase; TKI: Tyrosine kinase inhibitor.
Five studies assessed the risk of disease progression from CP to an advanced disease phase (AP or BP) in 1478 patients with CML and failed TKI treatment (pooled annual risk: 0.102; 95% CI: 0.050–0.199) [15,19,47,50,62]. The pooled median OS in 788 patients in the advanced disease phase from 23 studies was 2.5 years (95% CI: 1.9–3.2) [33,34,37,54,60,63–80].
Treatment use & outcomes in patients with TKI treatment failure
Based on data from five studies of 239 patients with CML and failed imatinib treatment, most patients’ regimens were switched to a 2G TKI (nilotinib 61.9%; dasatinib 16.7%) [19,39,46,49,54]. Other subsequent treatments included adding interferon to imatinib (10.0%) and increasing imatinib dosage (5.0%). HSCT was conducted in 0.8% of patients with failed imatinib treatment. Subsequent treatments were unspecified for 6.4% of the pooled patients from the five studies.
Pooled responses for 12-month treatments with 2L nilotinib or dasatinib after switching from 1L imatinib are illustrated in Figure 4. Patients with advanced-phase CML tended to have lower 12-month MMR (5.6 vs 39.4%) and CCyR (22.2 vs 51.5%) rates compared with CP-CML with 12-month nilotinib treatment after imatinib treatment failure [54]. A similar trend toward poorer survival outcomes was observed with the use of nilotinib in patients with advanced-phase (vs CP) CML and failed imatinib treatment (median progression-free survival: 1.7 vs 12.8 years; median OS: 3.8 vs 10.0 years) [37,43,54]. In addition, the MMR rate associated with a 12-month treatment with 3L dasatinib (after treatment failure with imatinib and nilotinib) was approximately one-half (46.8%) of the MMR in the 2L treatment setting (after treatment failure with imatinib: 27.3 vs 58.3%; Figure 4) [40].

Figure 4. Reported treatment response associated with second-generation tyrosine kinase inhibitors at 12 months in Chinese patients with chronic myeloid leukemia and tyrosine kinase inhibitor treatment failure.
AP: Accelerated phase; BP: Blast phase; CCyR: Complete cytogenetic response; CP: Chronic phase.
Grade 3–4 adverse events reported in association with switching treatment to nilotinib were mainly hematological and included thrombocytopenia (40.9%), anemia (24.9%) and neutropenia (17.8%) [37,38,41,42]. Pooled treatment outcomes for allo-HSCT in patients with advanced-phase CML and failed TKI treatment also revealed poorer survival outcomes (vs those with CP-CML and failed TKI treatment) and included a 5-year disease-free survival rate of 24.2% (vs 61.2%), a 5-year OS rate of 36.4% (vs 75.6%) [63,69–102] and a greater risk of complications (acute graft-versus-host disease: 50.3 vs 39.1%; chronic graft-versus-host disease: 50.0 vs 40.1%; cytomegalovirus infection: 35.5 vs 24.1%) [63,69,75–77,80,82,84,85,87,89,91,93–98,100,102–104].
Quality of life in patients with TKI treatment failure
HRQoL findings, categorized by disease phase and measurement instrument used, are summarized in Table 2. One study assessed the impact of TKI treatment failure on HRQoL using the European Organisation for Research and Treatment of Cancer Core Quality of Life Questionnaire (EORTC-QLQ-C30) [105]. Compared with patients with satisfactory TKI treatment response, TKI treatment failure was associated with a lower (worse) score for physical functioning (80.0 vs 93.3) and social functioning (50.0 vs 83.3) and a higher (worse) score for financial difficulties (100 vs 33.3) and fatigue (55.6 vs 11.1). Differences in these domain scores between patients with (vs without) satisfactory treatment responses were greater than the previously reported minimum clinically important difference, which was 6 for EORTC-QLQ-C30 domain scores in patients with hematological malignancies [106]. In addition, patients with AP-CML (115.3) or BP-CML (119.3) had a lower (worse) Functional Assessment of Cancer Therapy – Leukemia (FACT-Leu) total score than those with CP-CML (122.8) [107]. The difference in FACT-Leu total scores between AP-CML and CP-CML was in the previously reported minimum clinically important difference range for the FACT-Leu total score (6–12 points) [108].
| Disease phase | Health status | Instrument | Assessment outcomes | Studies (n) | Sample size | Point estimation | 95% CI | |
|---|---|---|---|---|---|---|---|---|
| CP | Satisfactory treatment response | EORTC QLQ-C30 | Physical functioning (median) | 1 | 85 | 93.3 | ||
| Social functioning (median) | 83.3 | |||||||
| Financial difficulties (median) | 33.3 | |||||||
| Fatigue (median) | 11.1 | |||||||
| Warning | Physical functioning (median) | 16 | 86.7 | |||||
| Social functioning (median) | 58.3 | |||||||
| Financial difficulties (median) | 66.7 | |||||||
| Fatigue (median) | 11.1 | |||||||
| Treatment failure | Physical functioning (median) | 11 | 80.0 | |||||
| Social functioning (median) | 50.0 | |||||||
| Financial difficulties (median) | 100.0 | |||||||
| Fatigue (median) | 55.6 | |||||||
| Unspecified | FACT-Leu | Total score | 2 | 286 | 122.8 | 120.9 | 124.7 | |
| Physical well-being | 20.1 | 18.2 | 22.0 | |||||
| Social well-being | 21.5 | 21.2 | 21.8 | |||||
| Emotional well-being | 17.8 | 17.6 | 18.1 | |||||
| Functional well-being | 15.5 | 15.1 | 15.8 | |||||
| LEUS domain | 48.5 | 47.9 | 49.1 | |||||
| AP | Unspecified | FACT-Leu | Total score | 1 | 6 | 115.3 | 84.1 | 146.5 |
| Physical well-being | 18.6 | 12.8 | 24.3 | |||||
| Social well-being | 19.6 | 13.7 | 25.5 | |||||
| Emotional well-being | 17.2 | 10.3 | 24.0 | |||||
| Functional well-being | 17.0 | 9.7 | 24.3 | |||||
| LEUS domain | 43.0 | 29.4 | 56.6 | |||||
| BP | Unspecified | FACT-Leu | Total score | 1 | 4 | 119.3 | 112.8 | 125.7 |
| Physical well-being | 19.8 | 17.9 | 21.6 | |||||
| Social well-being | 21.0 | 20.1 | 21.9 | |||||
| Emotional well-being | 17.0 | 15.6 | 18.4 | |||||
| Functional well-being | 15.8 | 11.4 | 20.1 | |||||
| LEUS domain | 45.8 | 38.9 | 52.6 | |||||
AP: Accelerated phase; BP: Blast phase; CP: Chronic phase; EORTC QLQ-C30: European Organisation for Research and Treatment of Cancer Core Quality of Life Questionnaire; FACT-LEU: Functional Assessment of Cancer Therapy – Leukemia; LEUS: Leukemia Subscale.
HRU & medical costs associated with TKI treatment failure
Table 3 summarizes HRU data and medical costs for patients with CML and TKI treatment failure. One study leveraged real-world data on HRU for patients with CML in several cities across China (Nanjing, Beijing, Hangzhou and Tianjin) to estimate annual HRU by patients with CML according to disease phase [109]. On average, patients with advanced-phase CML had more annual outpatient visits (14.8 vs 9.4) and hospitalizations (2.9 vs 0.4), as well as longer annual hospital stay length (55.8 vs 3.0 days), than patients with CP-CML.
| Outcome measurement | Treatment line | Disease phase | Intervention | Studies (n) | Sample size | Point estimation | 95% CI | ||
|---|---|---|---|---|---|---|---|---|---|
| Health resources utilization | Annual hospital admission | Unspecified | CP | Unspecified | 1 | NA | 0.4 | ||
| AP/BP | 1 | NA | 2.9 | ||||||
| Annual hospital stay length (days) | CP | 1 | NA | 3.0 | |||||
| AP/BP | 1 | NA | 55.8 | ||||||
| Annual outpatient visits | CP | 1 | NA | 9.4 | |||||
| AP/BP | 1 | NA | 14.8 | ||||||
| Medical costs | Annual outpatient costs | Second-line after imatinib treatment failure | AP/BP | Nilotinib/high-dose imatinib | 1 | NA | ¥9071 | ||
| CP | 1 | NA | ¥4201 | ||||||
| Annual hospital costs | Second-line after imatinib treatment failure | AP/BP | 1 | NA | ¥111,545 | ||||
| CP | 1 | NA | ¥4285 | ||||||
| Annual non-drug costs | First-line | CP | Imatinib | 1 | NA | ¥24,288 | |||
| Dasatinib | 1 | NA | ¥41,118 | ||||||
| Nilotinib | 1 | NA | ¥31,994 | ||||||
| Second-line after imatinib treatment failure | CP | Nilotinib | 1 | NA | ¥109,819 | ||||
| HSCT costs | TKI treatment failure | AP | HSCT | 1 | 51 | ¥296,605 | ¥235,739 | ¥357,470 | |
| BP | 1 | 23 | ¥371,183 | ¥295,366 | ¥446,999 | ||||
| CP | 2 | 637 | ¥220,798 | ¥202,456 | ¥239,140 | ||||
| Annual total medical costs after HSCT | NA | First year after HSCT | Post-HSCT management | 1 | 30 | ¥71,919 | |||
| Second year after HSCT | ¥32,260 | ||||||||
| Third year after HSCT | ¥16,574 | ||||||||
| Annual outpatient costs after HSCT | First year after HSCT | ¥13,910 | ¥11,951 | ¥15,869 | |||||
| Second year after HSCT | ¥6363 | ¥5251 | ¥7475 | ||||||
| Third year after HSCT | ¥3847 | ¥3106 | ¥4589 | ||||||
| Annual hospital costs after HSCT | First year after HSCT | ¥58,008 | ¥45,511 | ¥70,505 | |||||
| Second year after HSCT | ¥25,897 | ¥19,701 | ¥32,092 | ||||||
| Third year after HSCT | ¥12,726 | ¥10,767 | ¥14,686 | ||||||
AP: Accelerated phase; BP: Blast phase; CP: Chronic phase; HSCT: Hematopoietic stem-cell transplantation; NA: Not applicable; TKI: Tyrosine kinase inhibitor.
According to four studies reporting medical costs by disease phase for patients undergoing TKI treatment, patients with advanced-phase CML had on average 14-times greater annual medical costs (¥120,616 vs ¥8486), which were mainly ascribed to greater hospital costs (¥111,545 vs ¥4285), compared with patients with CP-CML [109]. 2L nilotinib in patients with failed imatinib treatment was also associated with a nearly threefold increase of annual nondrug cost compared with 1L nilotinib (¥109,819 vs ¥31,994) [110]. On average, HSCT cost more for patients with advanced-phase CML and failed TKI treatment (BP-CML ¥371,183; AP-CML: ¥296,605) compared with CP-CML and failed TKI treatment (¥220,798) [86,111].
Study quality assessment & publication bias assessment
Of the included 155 references, 151 references with full publications were assessed for their study quality. There were 39 references (25.8%) with an NOS score of 7 or above (high quality) and 112 (74.2%) with an NOS score of 4–6 (moderate quality). None of the assessed references had an NOS score indicating low quality. The publication bias assessment for the conducted meta-analysis observed right-skewed funnel plots for the pooled results of annual TKI resistance rate in patients who failed with imatinib and median OS in CML-AP patients.
Discussion
To our knowledge, the present SLR is the first comprehensive evaluation of RWE related to disease burden and unmet medical needs in Chinese patients with CML and TKI treatment failure. Encompassing 20 years of RWE data, our literature search ensured inclusion of relevant evidence released after approval of the first TKI for CML in China (imatinib). Although the findings of stable age-standardized incidence and sharply decreased age-standardized mortality rates are encouraging, our SLR also adds substantial dimensions to the known burdens of TKI failure in CML. These include: an elevated risk of developing treatment failure associated with 1L and subsequent-line treatments; a considerable prevalence of BCR-ABL1 kinase domain mutations (especially the T315I gatekeeper); and rapid disease progression. Patients with more advanced CML and/or those with greater numbers of TKI treatment lines (secondary to treatment resistance and failure) experienced: compromised treatment outcomes, including lower molecular and cytogenetic responses and survival; marked and clinically meaningful decrements in HRQoL; and sharply increased resource utilization and costs of care.
Like epidemiological patterns in other countries, China has had a stable age-standardized incidence and decreasing age-standardized mortality of CML, largely reflecting the advent and era of TKI therapy. Although imatinib was approved for the treatment of CML in 2002, Chinese patients with CML had limited access to TKIs until the recent approval of a reimbursement schedule and substantial price decreases for imatinib via a volume-based procurement policy [112]. Therefore a great expansion of patient access to imatinib is expected, which could further decrease CML-related mortality in China. One study forecast that the US prevalence of CML will increase from the year 2000 to a plateau by 2050 because of TKI treatments [113]. Because China has a similar crude incidence rate of CML to the USA (1–1.3 per 100,000) [114], the prevalence of CML in China could follow a similar trend. Future epidemiological studies are needed to confirm the trend of CML prevalence and provide robust evidence predicting the CML population size in China.
CML is difficult to cure, and the present review shows that imatinib was associated with the greatest risk of treatment failure (~20% per year) among the three approved TKIs in China. Although patients with failed imatinib treatment could be switched to nilotinib or dasatinib for continued treatment, the present review shows that treatment with 2G TKIs after imatinib treatment failure was associated with even greater risks of drug resistance and treatment intolerance. Consequently, such patients might face a greater risk of treatment failure. Absent an effective solution for TKI treatment failure, patients with such unmet needs could outnumber patients with controlled disease and become the main driver of CML-related burden in China.
TKI treatment failure in CML constitutes a formidable public health complication that can amplify the disease burden in many ways. For example, the pooled median age of Chinese patients with failed TKI treatment in our included studies (38.6 years) was approximately 10 years younger than that of patients with CML receiving imatinib as front-line treatment in China (49 years) [115]. This finding corroborated the relationship between age and risk of disease relapse in the ISAV study [116], which reported that patients younger than 45 years had a significantly greater rate of CML relapse (95%) compared with those aged between 45 and 65 (42%) or older than 65 (33%). There is no conclusive explanation for the relationship between age and disease relapse associated with imatinib; nevertheless, findings from the ISAV study suggested that younger age in patients with TKI treatment failure could substantially worsen the disease burden by extending disease duration. The proportion of high prognostic risk in patients with TKI treatment failure in our review (42.5%) was also approximately three-times that in previously untreated patients (13%) [117]. This relationship indicates that patients with failed TKI treatment had more rapid progression to advanced disease than those with previously untreated CML, which was associated with poor survival prognosis, decreased HRQoL and increased HRU and medical costs, based on evidence reported in the present SLR.
According to our present findings, the real-world risk of TKI treatment failure in Chinese patients with CML was much greater than was reported in the randomized trial setting. Our SLR showed that the pooled risk of treatment failure associated with 1L imatinib was approximately 20% per year, which is three- to four-times greater than those reported in the DASISION trial (4.8% per year) [118] and the IRIS trial (7.0% per year) [119]. Our review also found that the risk of treatment failure associated with 1L nilotinib was approximately 25% of that for imatinib but approached 30% for 2L nilotinib after failing imatinib. Given that more than 50% of patients with failed imatinib treatment subsequently received nilotinib, Chinese populations with CML and TKI treatment failure could be much larger than expected. Pooled evidence from the studies included in the present SLR confirmed that drug resistance was the predominant reason for treatment failure associated with the three approved TKIs in Chinese patients. Correlations between TKI resistance and BCR-ABL1 kinase domain gene mutations have been well established [120]. Consequently, it was not surprising to find an elevated risk of drug resistance in our studies, in which 51.6% of Chinese patients with failed TKI treatment had at least one BCR-ABL1 kinase domain mutation. Of these, T315I was the most prevalent, occurring in 10.6% of patients with TKI treatment failure. In addition, the risk of developing T315I mutations in the 2L treatment setting was nearly three-times greater than that associated with 1L imatinib. Because the T315I mutation confers resistance against both nilotinib and dasatinib [8], these genetic variants, as well as compound mutations (some including T315I), might contribute to a greater burden of TKI treatment failure in the future.
Treatment outcomes, including cytogenetic and molecular responses (and survival), were worse in patients with CML and failed TKI treatment. Nearly 80% of Chinese patients with CML were switched to a 2G TKI (mainly nilotinib) after imatinib treatment failure. Compared with the 1-year CCyR (80.1%) and MMR (44.0%) rates reported for 1L nilotinib in patients with CP-CML in the ENESTnd study [121], real-world treatment responses with 12-month nilotinib in Chinese patients with failed imatinib treatment (CCyR: 51.5%; MMR: 39.4%) were approximately 10–30% lower. Similarly, the 1-year CCyR rate with dasatinib in Chinese patients with failed imatinib treatment (47.7%) was nearly 60% of that reported for 1L dasatinib (83.4% in the DASISION study [118]). Treatment responses of the two TKIs were also decreased in the 3L setting and in patients with advanced-phase CML. A similar trend was reported for poorer survival outcomes associated with nilotinib in patients with advanced-phase CML that failed imatinib treatment.
Safety is a major potential concern when administering two 2G TKIs in patients with a history of treatment failure. According to pooled characteristics in the present SLR, more than 30% of patients with failed TKI treatment had at least one comorbidity, including approximately 10% with cardiovascular disease, which increases the relative risk of recurrent (vs initial) events with nilotinib or dasatinib [122]. Given the relatively young age of the patient population in the present SLR, safety issues might be more meaningful in more heterogeneous populations including older patients, who are more likely to have treatment-limiting chronic comorbidities. In addition, there is a high incidence of serious hematological events associated with nilotinib which can be life threatening and require hospital care [123]. Thus the two approved 2G TKIs might not completely meet the medical needs of patients with TKI treatment failure. In the event of disease relapse after treatment with nilotinib or dasatinib, HSCT is likely the only remaining treatment option. However, HSCT is associated with clinical issues and administrative hurdles such as strict eligibility requirements, prohibitively high costs, considerable risk of serious complications, and low success rate in patients with AP- or BP-CML [124].
Emerging challenges of TKI treatment failure have opened avenues for pharmacological innovation. For example, in 2015 the US FDA approved the third-generation TKI ponatinib for patients with CML and failed TKI treatment because of its marked antileukemic efficacy in patients with heavily pretreated CML, including those with T315I mutations. According to the PACE trial [125], the 1-year CCyR reported for ponatinib in patients with CP-CML that failed 2G TKIs was 46%, which was approximately 50% less in patients with AP- or BP-CML (vs CP-CML). Compared with allogeneic HSCT, ponatinib treatment was associated with survival benefits in patients with T315I-mutated CP-CML (4-year OS rate: 72.7 vs 55.8%) but not T315I-mutated AP-CML or BP-CML [126]. The promising effects of ponatinib have been tempered somewhat by reports of cardiotoxicity, arterial occlusive events, heart failure, venous thromboembolism and hepatotoxicity (along with other issues such as pancreatitis), which have resulted in black box warnings in the USA and other package labeling [127]. Ponatinib is the most cardiotoxic of 23 TKIs, with a potential mechanism of stimulating cardiomyocyte apoptosis [128–130]. In the PACE trial [125], 37% of patients receiving ponatinib had thrombocytopenia, 19% serious arterial and 5% venous occlusive adverse events. Ponatinib has not been approved in mainland China. With better understanding of the impact of patient characteristics (age, prognostic risk, comorbidity), disease molecular profiles and TKI toxicity profiles on the risk of TKI treatment failure, tailoring TKI treatments according to these factors could be another potential solution to control the emerging disease burden associated with TKI treatment failure in Chinese CML patients [131].
The present SLR identified important knowledge gaps that need to be bridged to better understand the disease burden and unmet medical needs of patients with CML failing TKI treatments in China. First, there is an absence of definitive quantitative evidence to support the premise that the prevalence of CML and TKI treatment failure will increase in China. It is therefore difficult to estimate the size of the future population of patients with failed TKI treatment, which subsequently complicates the decision-making process for reimbursement. Second, much of the evidence in the present SLR was based on 1L imatinib treatment failure; therefore, disease progression, risk of gene mutation, treatment outcomes and treatment intolerance in patients with CML that failed nilotinib and dasatinib treatments remain unclear. On the basis of limited evidence, TKI treatment failure in the 2L and 3L settings could inflict a heavier disease burden than 1L failure. Third, evidence reported in the present SLR should be considered in the context of certain limitations. Some findings, such as risks of BCR-ABL1 gene mutations with the three TKIs and treatment outcomes of the two 2G TKIs in patients with failed imatinib treatment were based on a single study with a limited sample size. Potential selection bias and uncertainty could decrease the generalizability of this evidence. Resistance to TKIs, as defined in this SLR, included both primary and secondary (acquired) resistance because most studies did not classify the outcome in this manner. Consequently, the pooled annual risk of TKI resistance could be overestimated. The included studies did not follow up with patients for sufficient durations to record survival outcomes. The present SLR used reported short-term survival data to extrapolate median outcomes using the exponential survival function assumption; thus these pooled survival outcomes need to be validated in future research. In addition, future studies are needed to fill evidence gaps and improve the robustness of the evidence for HRQoL and costs. Because Chinese publications were the main evidence source for the present SLR, the reported evidence related to treatment outcomes could be heavily biased by study quality. Finally, the common limitations associated with the nature of real-world studies could introduce bias in the reported evidence. These limitations and evidence gaps reflect a need for a representative CML patient registry to collect further, longitudinal real-world data on patients and their disease management, hence improving the validity and reliability of RWE for CML in China. Under whatever limitations, this review has comprehensively characterized the emerging disease burden and unmet medical needs in Chinese patients with CML and TKI treatment failure. Further, the synthesized evidence in this review can support future health economic evaluations for the coming third-generation TKIs which can effectively treat CML patients who failed with 1G and 2G TKIs.
Conclusion
This SLR of RWE shows that the disease burden of TKI treatment failure in Chinese patients with CML is substantial and poised to burgeon because of: a potentially longer disease course associated with relatively young patient age at disease onset; a high prevalence of BCR-ABL1 kinase domain mutations, which can confer TKI resistance and erode treatment outcomes; more rapid disease progression; limited treatment effectiveness associated with 2G TKIs in patients with TKI treatment failure; and the impaired HRQoL and increased HRU and medical costs associated with disease resistance and progression. New and novel, effective, well-tolerated, quality of life-enhancing and affordable treatments targeting TKI-resistant gene mutations, such as T315I and compound mutations, are urgently needed to address the unmet medical needs of Chinese patients with CML and TKI treatment failure.
•
Consistent with the transformational effects of tyrosine kinase inhibitors (TKIs) on the chronic myeloid leukemia (CML) treatment landscape, CML age-standardized mortality in Chinese patients has decreased by nearly 50% despite a stable age-standardized incidence, potentially leading to increasing numbers of cases in the future.
•
Compared with their counterparts without resistance or intolerance to TKIs, those with TKI treatment failure experience markedly reduced health-related quality of life, as well as sharp increases in health resource utilization and costs.
•
In addition to patients with more advanced CML, individuals who experience more TKI switches secondary to BCR-ABL1 kinase domain mutations have reduced treatment responses.
•
Nondrug costs were also nearly three-times higher in patients receiving second-line (vs first-line) TKI treatment.
•
The gatekeeper T315I mutation, which confers resistance against first- and second-generation TKIs, was the leading genetic variant, occurring in 10.6% of patients with BCR-ABL1 kinase domain mutations.
•
Treatment with the first-generation TKI imatinib was associated with the highest risk of treatment failure (20% per year).
Author contributions
YZ and W Chen were responsible for study conception, planning and design. Y Zhang was responsible for the planning and design of the systematic literature review. W Chen was responsible for data acquisition. All authors participated in data interpretation, drafting the manuscript (and/or making substantive intellectual contributions), reviewing the final version and agreeing to be accountable for the study and its findings.
Acknowledgments
The authors would like to thank H Huang and L Tan for their work on the literature search, study eligibility assessment, study quality assessment and data extraction in this study. S Gutkin and N Ogba, with Ascentage, provided substantive input in manuscript research and preparation.
Financial & competing interests disclosure
This study was sponsored by Ascentage Pharma Group Corp., Ltd. (Hong Kong), which contributed to the study design, interpretation of data and the decision to submit the article for publication. W Chen is an employee of Normin Health Consulting, Ltd., which received consulting fees from Ascentage Pharma Group, Inc. A Pathak, Y Yang, D Yang and Y Zhang are employees of Ascentage Pharma Group, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No funded writing assistance was used in the creation of this manuscript.
Data sharing statement
Extracted data from the included studies can be accessed by contacting the corresponding author.
Supplementary Material
File (supplementary materials.docx)
- Download
- 16.04 KB
References
Papers of special note have been highlighted as: • of interest
1.
Kalidas M, Kantarjian H, Talpaz M. Chronic myelogenous leukemia. JAMA 286(8), 895–898 (2001).
2.
Druker BJ, Lydon NB. Lessons learned from the development of an ABL tyrosine kinase inhibitor for chronic myelogenous leukemia. J. Clin. Invest. 105(1), 3–7 (2000).
3.
Hochhaus A, Larson RA, Guilhot F et al. Long-term outcomes of imatinib treatment for chronic myeloid leukemia. N. Engl. J. Med. 376(10), 917–927 (2017).
4.
Jabbour EJ, Cortes JE, Kantarjian HM. Resistance to tyrosine kinase inhibition therapy for chronic myelogenous leukemia: a clinical perspective and emerging treatment options. Clin. Lymphoma Myeloma Leuk. 13(5), 515–529 (2013).
5.
Chinese Society of Hematology, Chinese Medical Association. The guidelines for diagnosis and treatment of chronic myelogenous leukemia in China (2020 edition). Zhonghua Xue Ye Xue Za Zhi. 41(5), 353–364 (2020).
6.
Huang XJ. Hematopoietic stem cell transplantation in China: current status and prospects. Am. J. Blood Res. 1(1), 90–97 (2011).
7.
Bixby D, Talpaz M. Seeking the causes and solutions to imatinib-resistance in chronic myeloid leukemia. Leukemia 25, 7–22 (2011).
8.
Lange T, Ernst T, Gruber FX et al. The quantitative level of T315I mutated BCR-ABL predicts for major molecular response to second-line nilotinib or dasatinib treatment in patients with chronic myeloid leukemia. Haematologica 98(5), 714–717 (2013).
9.
Osman AE, Deininger MW. Chronic myeloid leukemia: modern therapies, current challenges and future directions. Blood Reviews 49, 100825 (2021).
10.
Wells GA, Shea B, O’Connell D et al. The Newcastle–Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (2011). www.ohri.ca/programs/clinical_epidemiology/oxford.asp
11.
Lin Q, Mao L, Shao L et al. Global, regional, and national burden of chronic myeloid leukemia, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Front. Oncol. 10, 580759 (2020).
12.
Bao PP, Wu CX, Zhang ML et al. Analysis of the characteristics and trends of the main subtypes of leukemia in Shanghai. J. Diagn. Concepts Pract. 16, 484–491 (2017).
13.
Linet MS, Gilbert ES, Dores GM et al. A retrospective cohort study of cause-specific mortality and incidence of hematopoietic malignancies in Chinese benzene-exposed workers. Int. J. Cancer 137, 2184–2197 (2015).
14.
Hua JJ, Xu ZK, Du JK, Han JH, Jia DD, Liang H. Analysis on the incidence of leukemia among workers in Shajing in Shenzhen. Chin. Prev. Med. 15, 260–263 (2014).
15.
Yu L, Qin YQ, Lai YY, Shi HX, Huang XJ, Jiang Q. Severe hematological adverse reactions during the period of taking tyrosine kinase inhibitors in patients with chronic myelogenous leukemia and their effects on treatment response. Chin. J. Hematol. 40(4), 281–287 (2019).
16.
Huang J, Wang L, Chen L et al. Changing treatment may affect the predictive ability of European treatment outcome study scoring for the prognosis of patients with chronic myeloid leukemia. Turk. J. Hematol. 34, 10–15 (2017).
17.
Zhang JJ, Yang LJ, Zhu Y et al. The efficacy and safety of imatinib or nilotinib in the first-line treatment of elderly patients with chronic myeloid leukemia in the chronic phase. J. Nanjing Med. Univ. (Nat. Sci.) 8, 1197–1201 (2019).
18.
Yin H, Chen Y, Chen L et al. Real-world evidence of molecular response to tyrosine kinase inhibitors from China supports European LeukemiaNet 2013 recommendations for the management of chronic myeloid leukaemia. Hemasphere 2, 875–876 (2018).
19.
Zhou M, Qiu HY, He GS et al. Multivariate analysis of drug resistance during the treatment of chronic myelogenous leukemia with imatinib. Chin. J. Hematol. 34(5), 395–398 (2013).
20.
Zhao HF, Zhang YL, Zu YL et al. Clinical observation of the effect of clonal chromosomal abnormalities in Philadelphia chromosome-negative cells on the curative effect of chronic myeloid leukemia. Chin. J. Intern. Med. 803, 4–7 (2019).
21.
Wang J, Gao SK, Li Z, Li MJ, Zhang LL, Song YP. Adverse hematological reactions in 435 patients with chronic myeloid leukemia after treatment with imatinib mesylate. J. Leuk. Lymphoma 12, 479–482 (2015).
22.
Chen J. The clinical dose and efficacy of imatinib in the treatment of chronic myeloid leukemia. World Clin. Med. 11, 87–88 (2017).
23.
Zhang CJ, Zheng XL, Zheng DD, Xia WL, Su XL. Comparative analysis of the prognostic system and factors of tyrosine kinase inhibitors in the treatment of chronic myeloid leukemia. Chin. Youjiang Med. J. 48(5), 339–344 (2020).
24.
Huang J, Zhao XL. Comparison of three prognostic scoring systems in evaluating the prognosis of chronic myeloid leukemia. J. Central South Univ. (Med. Sci.) 41(08), 809–814 (2016).
25.
Wang PP, Zhang PP, Zhang J, Xi YM. The estimated value of different scoring systems for the clinical efficacy of newly diagnosed patients with chronic myeloid leukemia. J. Exp. Hematol. 27(03), 723–728 (2019).
26.
Yang AL, Liu X, Wang XB et al. Efficacy of the first and second generation TKIs in the treatment of chronic myeloid leukemia. J. Med. Inf. 32(23), 78–81 (2019).
27.
Huang Q, Liu H, Li Y, Zhang XY, Wang XM. Early effect of domestic imatinib mesylate in the treatment of chronic myelogenous leukemia patients. Cancer Res. Clin. 28(12), 811–814 (2016).
28.
Zhang JZ, Bao Y, Chen SM et al. Comparative analysis of clinical efficacy and drug safety of domestic imatinib and original imatinib in the treatment of newly diagnosed chronic myelogenous leukemia in the chronic phase. J. Clin. Hematol. 30(4), 527–531 (2017).
29.
Jiang H, Zhi LT, Hou M, Wang JX, Wu DP, Huang XJ. Comparison of the efficacy and safety of domestic and original imatinib in the treatment of newly diagnosed chronic myelogenous leukemia. Chin. J. Hematol. 38(07), 566–571 (2017).
30.
Tan L, Xie Y, Yang J, Liu L. Curative efficacy of first generation TKI in the treatment of CML-CP combined with vPh and analysis of its genetic characteristics. J. Exp. Hematol. 28(04), 1162–1166 (2020).
31.
Zhong JS, Meng FY, Xu D et al. Follow-up observation of imatinib in the treatment of chronic myeloid leukemia in chronic phase. J. Pract. Med. 28(5), 811–813 (2012).
32.
Wang YM. Discussion on the safety and efficacy of imatinib in the treatment of patients with chronic myeloid leukemia. Chin. Pract. Med. 11(22), 129–130 (2016).
33.
Zhou KS, Wang CC, Zhao YZ et al. Long-term efficacy observation of imatinib in the treatment of 135 cases of chronic myeloid leukemia. J. Leuk. Lymphoma 11, 646–650 (2010).
34.
Jin FF, Lai BB, Zhang YY, Xia HF. Comparison of efficacy and drug resistance of tyrosine kinase inhibitors in chronic and advanced stages of chronic myelogenous leukemia. Chin. J. Prev. Control Chronic Dis. 26(2), 146–150 (2018).
35.
Chen YL, Yin H, Chen LF et al. Feasibility study of switching to nilotinib after first-line imatinib in the chronic phase of chronic myeloid leukemia. Clin. Lymphoma Myeloma Leuk. 20(2), E43–E49 (2020).
36.
Xu L, Zhu H, Hu J et al. Superiority of allogeneic hematopoietic stem cell transplantation to nilotinib and dasatinib for adult patients with chronic myelogenous leukemia in the accelerated phase. Front. Med. 9, 304–311 (2015).
37.
Wang AH, Zhou L, You JH, Wang L, Li JM, Hu J et al. Clinical analysis of nilotinib in the treatment of chronic myeloid leukemia resistant or intolerant to imatinib. Chin. J. Hematol. (1), 11–15 (2010).
38.
Wei YQ, Zhang X, Chen WW, Cao R, Yin CX, Feng R et al. Long-term follow-up study of nilotinib in the treatment of imatinib-resistant or intolerant chronic myeloid leukemia. J. Southern Med. Univ. 32(7), 1000–1003 (2012).
39.
Zu YL, Zhang YL, Zhou J et al. Interferon combined with imatinib in the treatment of chronic myeloid leukemia with mutations in ABL kinase region. Chin. J. Intern. Med. 55(10), 794–796 (2016).
• ABL kinase region mutation is the leading cause of tyrosine kinase inhibitor (TKI) treatment failure that drives the disease burden of chronic myeloid leukemia (CML).
40.
Liu D, Liu Y, Xue M et al. Responses to dasatinib as a second- and third-line tyrosine kinase inhibitor in chronic phase chronic myeloid leukaemia patients. Acta Haematol. 142, 79–86 (2019).
• ABL kinase region mutation is the leading cause of TKI treatment failure that drives the disease burden of CML.
41.
Xu JJ, Du X, Lou J et al. Clinical analysis of nilotinib in the treatment of imatinib-resistant chronic myeloid leukemia. J. Clin. Hematol. 4, 458–461 (2013).
• ABL kinase region mutation is the leading cause of TKI treatment failure that drives the disease burden of CML.
42.
Pan LQ, Liu WX, Zhu Y et al. Clinical study of nilotinib in the treatment of imatinib-resistant or intolerant chronic myeloid leukemia patients. J. Exp. Hematol. 22(6), 1545–1549 (2014).
• ABL kinase region mutation is the leading cause of TKI treatment failure that drives the disease burden of CML.
43.
Jiang H, Chen SS, Jiang B et al. To evaluate the effect of baseline ABL kinase region point mutations on the efficacy of nilotinib in the treatment of imatinib-resistant or intolerant chronic myeloid leukemia. Chin. J. Hematol. 33(2), 123–126 (2012).
• ABL kinase region mutation is the leading cause of TKI treatment failure that drives the disease burden of CML.
44.
Zhang D, Zhu HL. Clinical outcome and influencing factors of patients with chronic myelogenous leukemia in the chronic phase receiving tyrosine kinase inhibitor treatment and clinical analysis. Int. J. Blood Transfus. Hematol. 42(2), 127–133 (2019).
45.
Qin Y, Chen S, Jiang B et al. Characteristics of BCR-ABL kinase domain point mutations in Chinese imatinib-resistant chronic myeloid leukemia patients. Ann. Hematol. 90, 47–52 (2011).
46.
Jing Y, Yang L, Liu DH. Efficacy of TKI in the treatment of chronic myeloid leukemia and related influencing factors analysis of deep molecular response. J. Exp. Hematol. 25(6), 1597–1604 (2017).
47.
Ren WR, Lu SJ, Ren NN, Li XL, Zhu HL. Analysis of the efficacy and safety of tyrosine kinase inhibitors in the treatment of chronic myeloid leukemia in the elderly in chronic phase. Int. J. Blood Transfus. Hematol. 39, 471–475 (2016).
48.
Jiang Q, Hu J, Zheng F et al. Baseline characteristics and early monitoring of Chinese CML patients treated with dasatinib: report from a multicenter, observational registry-based study. Blood 128(22), 5439 (2016).
49.
Qiao JH, Zhang ZC, Yao B et al. Efficacy of switching to second-generation tyrosine kinase inhibitors in chronic myeloid leukemia patients with poor response to imatinib. J. Exp. Hematol. 23(1), 65–69 (2015).
50.
Yuan T, Lai YY, Qin YQ et al. Analysis of the efficacy and influencing factors of nilotinib and dasatinib as second and third-line drugs in the treatment of chronic myelogenous leukemia patients in the chronic and accelerated phases. Chin. J. Hematol. 41(2), 93 (2020).
51.
Lu L, Qiao C, Hong M et al. Mean erythrocyte volume can be used as a predictor of the efficacy of chronic myeloid leukemia. J. Exp. Hematol. 26(2), 382–388 (2018).
52.
Shi DY, Qin YQ, Lai YY, Shi HX, Huang XJ, Jiang Q. Distribution of BCR-ABL kinase region mutations in patients with tyrosine kinase inhibitor-resistant chronic myeloid leukemia and its influencing factors. Chin. J. Hematol. 41, 469–476 (2020).
53.
Chen C, Liao LB, Xu D et al. Clinical characteristics of T315I gene mutation in chronic myeloid leukemia and the efficacy of ponatinib. J. Southern Med. Univ. 39(3), 364 (2019).
54.
Lu SJ, Zhu HL, Li XL et al. Clinical efficacy analysis of second-generation tyrosine kinase inhibitors in the treatment of chronic myeloid leukemia. J. Sichuan Univ. (Med. Sci.) 47, 287–291 (2016).
55.
Chen YL, Wang L, Yuan GL et al. Efficacy and safety analysis of domestic dasatinib in the second-line treatment of chronic myelogenous leukemia patients. Chin. J. Hematol. 40(2), 98 (2019).
56.
Yu L, Qin YQ, Lai YY et al. A comparative study of nilotinib and imatinib in the first-line treatment of patients with newly diagnosed chronic myelogenous leukemia. Chin. J. Hematol. 40(12), 996 (2019).
57.
Chen DY, Wang J, Zhang LD, Cheng Y, Zhang HB. Analysis of related factors of point mutations in ABL kinase region in patients with TKI-resistant chronic myeloid leukemia. J. Modern Med. Health 37, 569–571 (2021).
58.
Chen LF, Yuan GL, Zhong ZD et al. Efficacy and safety of generic dasatinib as a second-line treatment for patients with chronic myeloid leukemia: a multicenter retrospective study in Hubei province, China. Curr. Med. Sci. 38, 1005–1011 (2018).
59.
Wu LL, Zeng QS, Yang MZ et al. Detection of ABL kinase region point mutations in patients with chronic myeloid leukemia after imatinib treatment. J. Exp. Hematol. 1, 49–53 (2010).
60.
Li XL, Zhu HL, Liu HY et al. Clinical efficacy analysis of tyrosine kinase inhibitors in the treatment of chronic myeloid leukemia. J. Sichuan Univ. (Med. Sci.) 45, 647–651 (2014).
61.
Wang J, Zhang YL, Zu YL et al. Comparison of the characteristics and efficacy of Ph+ acute lymphoblastic leukemia and chronic myeloid leukemia with T315I mutation. Chin. J. Hematol. 37(2), 110 (2016).
62.
Zhang F. Study on the efficacy of imatinib in the treatment of chronic myelogenous leukemia. Med. Community 9, 1 (2020).
63.
Chen YK, Zhang Y, Liu QF et al. Long-term survival analysis of allogeneic hematopoietic stem cell transplantation for chronic myeloid leukemia. J. Intern. Med. Concepts Pract. 1, 5 (2010).
64.
Chen K, He YY. The morphological characteristics and prognosis of bone marrow cells in chronic myelogenous leukemia with acute granulosis and acute lymphoblastic change. Chin. J. Clin. Res. 30(8), 3 (2017).
65.
Chen H, Jiang YQ, Shen YF et al. A clinical study on second-generation tyrosine kinase inhibitors as first-and second-line treatments in chronic myeloid leukemia. Chin. J. Biomed. Eng. 23(6), 479–483 (2017).
66.
Dai LX, Tu XQ, Cai BB. Clinical study of dasatinib in the treatment of patients with chronic myeloid leukemia in different clinical stages. J. Chin. Oncol. 24(10), 997–1001 (2018).
67.
Zhang C. CHG pre-excitation regimen combined with imatinib mesylate in the treatment of acute myeloid transformation of chronic myeloid leukemia. J. Chin. Pract. Diagn. Ther. 28(4), 409–410 (2014).
68.
Pan CY, Li YJ, Li MX et al. Treatment overview and medication compliance analysis of 140 patients with chronic myeloid leukemia. Chongqing Med. 48, 2014–2017 (2019).
69.
Jiang Q, Xu LP, Liu DH et al. Imatinib mesylate versus allogeneic hematopoietic stem cell transplantation for patients with chronic myelogenous leukemia in the accelerated phase. Blood 117, 3032–3040 (2011).
70.
Xu XH, Xu Y, Ouyang YJ et al. Efficacy of allogeneic hematopoietic stem cell transplantation in the treatment of chronic myeloid leukemia. Jiangsu Med. J. 38, 2405–2407 (2012).
71.
Zhang Y, Chen YK, Fan ZP et al. Analysis of the effect of HLA matching on chronic myeloid leukemia allogeneic hematopoietic stem cell transplantation. J. Southern Med. Univ. 31(3), 438–442 (2011).
72.
Zhang X, Chen XH, Gao L et al. Clinical observation of 52 cases of acute and chronic leukemia treated with allogeneic peripheral blood stem cell transplantation. J. Clin. Hematol. 21(5), 458–460 (2008).
73.
Xia LH, Fang J, Liu F et al. Analysis of curative effect of related allogeneic hematopoietic stem cell transplantation in the treatment of chronic myeloid leukemia in 30 cases. Chin. J. Organ Transplant. 28(1), 55–56 (2007).
74.
Wang XB, Liu HL, Geng LQ et al. Allogeneic hematopoietic stem cell transplantation from HLA-contracted donors for treatment of 40 cases of chronic myeloid leukemia. Chin. J. Tissue Eng. Res. 13, 2618–2622 (2009).
75.
Li MX, Wang JS, Zhang Y, Sun ZQ, Zhao P, Lu YH. Clinical observation of imatinib combined with stem cell transplantation in the treatment of chronic myeloid leukemia. Chongqing Med. 42(29), 3554–3556 (2013).
76.
Song AX, Yang DL, Wei JL et al. Preliminary analysis of the efficacy and prognosis of allogeneic hematopoietic stem cell transplantation in the treatment of advanced chronic myeloid leukemia. J. Exp. Hematol. 19, 149–153 (2011).
77.
Zhang LL, Liu HL, Geng LQ et al. Treatment of advanced chronic myeloid leukemia with non-blood cord blood transplantation. J. Leuk. Lymphoma 21(6), 349–352 (2012).
78.
Zhao YL, Zhang JP, Ji SQ et al. HLA haploidentical hematopoietic stem cell transplantation for treatment of advanced chronic myeloid leukemia. Chin. J. Organ Transplant. 33(2), 73–76 (2012).
79.
Zhou M, Sha XS, Qiu HY et al. Retrospective analysis of imatinib and allogeneic hematopoietic stem cell transplantation in the treatment of chronic myeloid leukemia. Chin. J. Hematol. 35, 126–128 (2014).
80.
Feng SQ, Liu ZB, Yao YH et al. Effect of stratified intervention therapy after allogeneic hematopoietic stem cell transplantation in chronic myelogenous leukemia. J. Clin. Hematol. 31(1), 44–48 (2018).
81.
Li F, Zhang XJ, Zhang RY et al. Imatinib first-line treatment of chronic myeloid leukemia patients in chronic phase-a single-center retrospective analysis. Chin. J. Clin. Oncol. 43, 432–437 (2016).
82.
Wang XB, Sun ZM, Liu HL et al. Efficacy observation and cost analysis of HLA-contracted allogeneic hematopoietic stem cell transplantation for the first chronic phase of chronic myeloid leukemia. J. Clin. Intern. Med. 26(4), 257–260 (2009).
83.
Wang WQ, Bai QX, Chen XQ et al. The efficacy and quality of life follow-up of 34 patients with chronic myeloid leukemia allogeneic hematopoietic stem cell transplantation. Chin. J. Tissue Eng. Res. 11, 9268–9271 (2007).
84.
Zou J, Li WM, Xia LH et al. Differences in efficacy and safety of imatinib mesylate and allogeneic hematopoietic stem cell transplantation in the treatment of chronic myeloid leukemia in chronic phase. Chin. J. Tissue Eng. Res. 12, 10184–10188 (2008).
85.
Zhu KE, Xu Y, Zhong J, Chen ST, Zeng HL. BU-CTX2 pretreatment regimen for the treatment of 60 cases of leukemia with allogeneic hematopoietic stem cell transplantation. Chin. J. Hematol. 23, 349–352 (2002).
86.
Xue J, Wang YG, Huang H, Lin MF. Detection of minimal residual disease after unrelated allogeneic bone marrow transplantation in chronic myeloid leukemia by RT-nest-PCR method. J. Clin. Hematol. 20(2), 93–95 (2007).
87.
Xu LP, Guo NL, Huang XJ et al. Effect of interferon alpha on the prognosis of allogeneic bone marrow transplantation in patients with chronic myeloid leukemia. Chin. J. Hematol. 22(11), 589–591 (2001).
88.
Xu MZ, Sun AN, Wu DP et al. Efficacy and prognostic factors analysis of allogeneic hematopoietic stem cell transplantation in the treatment of chronic myeloid leukemia. Shandong Med. J. 51(49), 88–90 (2011).
89.
Wang JM, Zhang WP, Chen L et al. Standard dose and reduced dose preconditioning peripheral blood stem cell transplantation in the treatment of chronic myeloid leukemia clinical research. Chin. J. Pract. Intern. Med. S1, 20 (2007).
90.
Tong XZ, Li J, Tan EX et al. Efficacy and prognostic factors analysis of allogeneic hematopoietic stem cell transplantation from HLA-contracted donors in the treatment of chronic myeloid leukemia. Chin. J. Clin. Oncol. 28, 545–548 (2006).
91.
Song XM, Wang JM, Ju XP et al. Clinical study of allogeneic peripheral blood stem cell transplantation in the treatment of chronic myeloid leukemia. Med. J. Chin. People’s Liberation Army 26, 295–297 (2001).
92.
Qian SX, Wu HX, Hong M et al. Allogeneic hematopoietic stem cell transplantation for chronic myeloid leukemia. Chin. J. Organ Transplant. 5, 309–310 (2009).
93.
Liu QF, Fan ZP, Sun J et al. Analysis of curative effect of hematopoietic stem cell transplantation in the treatment of chronic myeloid leukemia. J. Southern Med. Univ. 24(11), 1227–1229 (2004).
94.
Li WM, Xia LH, You Y, Liu XY, Zhong ZD, Zou P. A clinical comparative study of related allogeneic hematopoietic stem cell transplantation and STI571 in the treatment of chronic myeloid leukemia. J. Clin. Hematol. 20, 216–219 (2007).
95.
Huang L, Huang H, Cai Z et al. Effect of interferon alpha before transplantation on the prognosis of unrelated allogeneic bone marrow transplantation in patients with chronic myeloid leukemia. Zhejiang Med. J. 28(8), 607–609 (2006).
96.
He Y, Feng SZ, Wang M et al. HLA-related allogeneic hematopoietic stem cell transplantation for the treatment of chronic myeloid leukemia in the first chronic phase of 51 cases. Chin. J. Hematol. 26(7), 389–392 (2005).
97.
Gao XD, Wu W, Zhao WL, Tang W, Shen ZX, Hu J. The clinical significance of BCR-ABL fusion gene detection and pretreatment in patients with chronic myeloid leukemia before and after transplantation. J. Diagn. Concepts Pract. 6(4), 374–375 (2007).
98.
Ding JH, Ma Y, Chen BA et al. Nonmyeloablative peripheral blood stem cell transplantation for chronic myeloid leukemia in chronic and accelerated phases. J. Exp. Hematol. 16, 373–376 (2008).
99.
Cai X, Wei J, He Y et al. A modified busulfan and cyclophosphamide preparative regimen for allogeneic transplantation in myeloid malignancies. Int. J. Clin. Pharm. 37, 44–52 (2014).
100.
Gao GL, Xu N, Zhou X et al. Efficacy analysis of imatinib mesylate and allogeneic hematopoietic stem cell transplantation in the chronic phase of chronic myeloid leukemia. Natl Med. J. China 93, 3035–3039 (2013).
101.
Xu L, Xu Z, Zhang X, Chen H, Chen Y, Huang X. Allogeneic stem cell transplantation for patients with T315I BCR-ABL mutated chronic myeloid leukemia. Bone Marrow Transplant. 51, S158–S159 (2016).
102.
Liu QF, Xu XJ, Chen YK et al. Long-term outcomes of HLA-matched sibling compared with mismatched related and unrelated donor hematopoietic stem cell transplantation for chronic phase chronic myelogenous leukemia: a single institution experience in China. Ann. Hematol. 90, 331–341 (2011).
103.
Li WM, Xia LH, You Y, Liu XY, Zhong ZD, Zou P. Comparison of the effects of related allogeneic hematopoietic stem cell transplantation and STI571 in the treatment of non-chronic stage chronic myeloid leukemia. Chin. J. Tissue Eng. Res. 11(24), 4742–4746 (2007).
104.
Lu YJ, Sun ZM, Liu HL et al. Allogeneic hematopoietic stem cell transplantation in the treatment of advanced chronic myelogenous leukemia – efficacy analysis of transplantation of non-blood cord blood and sibling donors. Chin. J. Hematol. 35(3), 253–255 (2014).
105.
Shu M, Sun Y, Wang XD. Investigation of health-related quality of life in patients with chronic myeloid leukemia in the chronic phase. J. Modern Med. Health 36, 203–206 (2020).
106.
Goswami P, Ionova T, Oliva EN et al. Final development of the first generic quality of life and symptoms measure specific for hematological malignancies: the HM-PRO. Blood 134, 3484–3484 (2019).
107.
Wang YL, Chen FJ, Luo YQ, Leng YM, Zhu HL. The Chinese version of FACT-Leu scale is used to assess the quality of life of CML patients and analysis of influencing factors. J. Chengdu Med. Coll. 14, 234–239 (2019).
108.
Kantarjian HM, Mamolo CM, Gambacorti-Passerini C et al. Long-term patient-reported outcomes from an open-label safety and efficacy study of bosutinib in Philadelphia chromosome–positive chronic myeloid leukemia patients resistant or intolerant to prior therapy. Cancer 124(3), 587–595 (2018).
109.
Huang CF, Shen LJ, Liu YH. Analysis of the budgetary impact of the inclusion of nilotinib in medical insurance for the treatment of imatinib-resistant or intolerant myeloid leukemia patients. Chin. Health Econ. 37(11), 59–63 (2018).
110.
Li N, Zheng B, Cai HF et al. Cost effectiveness of imatinib, dasatinib, and nilotinib as first-line treatment for chronic-phase chronic myeloid leukemia in China. Clin. Drug Invest. 38, 79–86 (2018).
111.
Wang JX, Huang XJ, Wu DP et al. Investigation and analysis of the incidence of chronic myeloid leukemia and current diagnosis and treatment models in 15 hospitals in China. Chin. J. Hematol. 30, 721–725 (2009).
112.
Tang M, He J, Chen M et al. “4+ 7” city drug volume-based purchasing and using pilot program in China and its impact. Drug Discoveries & Therapeutics 13(6), 365–9 (2019).
113.
Huang X, Cortes J, Kantarjian H. Estimations of the increasing prevalence and plateau prevalence of chronic myeloid leukemia in the era of tyrosine kinase inhibitor therapy. Cancer 118(12), 3123–3127 (2012).
114.
Arias E. United States Life Tables, 2006. Natl Vital Stat. Rep. 58(21), 1–40 (2010).
115.
Yang X, Bai Y, Shi M et al. Validation of the EUTOS long-term survival score in Chinese chronic myeloid leukemia patients treated with imatinib: a multicenter real-world study. Cancer Manag. Res. 12, 1293–1301 (2020).
116.
Mori S, Vagge E, Le Courted P et al. Age and d PCR can predict relapse in CML patients who discontinued imatinib: the ISAV study. Am. J. Hematol. 90(10), 910–914 (2015).
117.
Xia L, Qian W, Yang M, Li Q, Liu F, Xie Y. Comparison of the utility and applicability of the Sokal, Hasford, and EUTOS scores in a population of Chinese patients with chronic-phase chronic myeloid leukemia undergoing imatinib therapy. Onco Targets Ther. 8, 2485–2492 (2015).
118.
Kantarjian HM, Shah NP, Cortes JE et al. Dasatinib or imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: 2-year follow-up from a randomized phase 3 trial (DASISION). Blood 119(5), 1123–1129 (2012).
119.
Hochhaus A, O’Brien S, Guilhot F et al. Six-year follow-up of patients receiving imatinib for the first-line treatment of chronic myeloid leukemia. Leukemia 23, 1054–1061 (2009).
120.
Patel AB, O’Hare T, Deininger MW. Mechanisms of resistance to ABL kinase inhibition in chronic myeloid leukemia and the development of next generation ABL kinase inhibitors. Hematol. Oncol. Clin. North Am. 31(4), 589–612 (2017).
121.
Mealing S, Barcena L, Hawkins N et al. The relative efficacy of imatinib, dasatinib and nilotinib for newly diagnosed chronic myeloid leukemia: a systematic review and network meta-analysis. Exp. Hematol. Oncol. 2(1), 1–9 (2013).
122.
Leong D, Aghel N, Hillis C et al. Tyrosine kinase inhibitors in chronic myeloid leukaemia and emergent cardiovascular disease. Heart 107(8), 667–673 (2021).
123.
Wang Z, Jiang L, Yan H, Xu Z, Luo P. Adverse events associated with nilotinib in chronic myeloid leukemia: mechanisms and management strategies. Expert Review of Clinical Pharmacology 14(4), 445–56 (2021).
124.
Oyekunle A, Klyuchnikov E, Ocheni S et al. Challenges for allogeneic hematopoietic stem cell transplantation in chronic myeloid leukemia in the era of tyrosine kinase inhibitors. Acta Haematologica 126(1), 30–9 (2011).
125.
Cortes J, Kim DW, Pinilla-Ibarz J et al. Ponatinib efficacy and safety in heavily pretreated leukemia patients: 3-year results of the PACE trial. Haematologica 100(Suppl. 1), 64 (2015).
126.
Nicolini FE, Basak GW, Kim DW et al. Overall survival with ponatinib versus allogeneic stem cell transplantation in Philadelphia chromosome-positive leukemias with the T315I mutation. Cancer 123(15), 2875–2880 (2017).
127.
Gainor JF, Chabner BA. Ponatinib: accelerated disapproval. The Oncologist. 20(8), 847 (2015).
128.
Sharma A, Burridge PW, McKeithan WL et al. High-throughput screening of tyrosine kinase inhibitor cardiotoxicity with human pluripotent stem cells. Sci. Transl. Med. 9(377), 2584 (2017).
129.
Singh AP, Glennon MS, Umbarkar P et al. Ponatinib-induced cardiotoxicity: delineating the signalling mechanisms and potential rescue strategies. Cardiovasc. Res. 115(5), 966–977 (2019).
130.
Singh AP, Umbarkar P, Tousif S, Lal H. Cardiotoxicity of the BCR-ABL1 tyrosine kinase inhibitors: emphasis on ponatinib. Int. J. Cardiol. 316, 214–221 (2020).
131.
Ciftciler R, Haznedaroglu IC. Tailored tyrosine kinase inhibitor (TKI) treatment of chronic myeloid leukemia (CML) based on current evidence. Eur. Rev. Med. Pharmacol. Sci. 25(24), 7787–7798 (2021).
Information & Authors
Information
Published In
Pages: 621 - 637
PubMed: 35411807
Copyright
© 2022 Future Medicine Ltd.
History
Received: 15 February 2022
Accepted: 25 March 2022
Published online: 12 April 2022
Keywords:
Topics
Authors
Funding Information
Ascentage Pharma Group Corp Ltd. (Hong Kong)
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Burden of tyrosine kinase inhibitor failure in Chinese chronic myeloid leukemia patients: a systematic literature review. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0032
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Zhenglei Shen, Honghua Cao, Yeying Zhou, Wenwen Mao, Kunmei Liu, Jingying Zhu, Ming He, Yunru Mao, Ni Luo, Lei Feng, Heng Le, Liying Song, HuaXian Li, Yasar Mehmood Yousafzai, Asad Zia, Xuezhong Gu, Shiwen Zhang, Exosome and BCR-ABL mediated molecular alterations in endothelial cells in chronic myeloid leukemia: identification of seven genes and their regulatory network, PeerJ, 10.7717/peerj.20371, 13, (e20371), (2025).
- Carol Yuk Man Cheung, Chung Yin Ha, Bonnie Kho, Chi Kuen Lau, June Sze Man Lau, Shek Ying Lin, Vivien Wai Man Mak, Raymond Siu Ming Wong, Yok Lam Kwong, Management of chronic-phase CML in later lines: a Hong Kong consensus recommendation, Annals of Hematology, 10.1007/s00277-025-06416-9, 104, 6, (3091-3101), (2025).
- Zilin Li, Yiling Xi, Linglan Tu, Xu Zhang, Yue Huang, Huizong Nie, Cheng Peng, Haohuan Chai, Shenxin Zeng, Xiaoliang Zheng, Liyan Cheng, Investigation of the mechanism of USP28-mediated IFITM3 elevation in BCR-ABL-dependent imatinib resistance in CML, Biomedicine & Pharmacotherapy, 10.1016/j.biopha.2024.116315, 173, (116315), (2024).
- Romeo G. Mihăilă, Advances in the Treatment of Chronic Myeloid Leukemia, Recent Patents on Anti-Cancer Drug Discovery, 10.2174/1574892818666230111115040, 19, 1, (1-17), (2024).