An economic and health outcome evaluation of telehealth in rural sepsis care: a comparative effectiveness study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Sepsis is a top contributor to in-hospital mortality and, healthcare expenditures and telehealth have been shown to improve short-term sepsis care in rural hospitals. This study will evaluate the effect of provider-to-provider video telehealth in rural emergency departments (EDs) on healthcare costs and long-term outcomes for sepsis patients. Materials & methods: We will use Medicare administrative claims to compare total healthcare expenditures, mortality, length-of-stay, readmissions, and category-specific costs between telehealth-subscribing and control hospitals. Results: The results of this work will demonstrate the extent to which telehealth use is associated with total healthcare expenditures for sepsis care. Conclusion: These findings will be important to inform future policy initiatives to improve sepsis care in rural EDs.
Clinical Trial Registration: NCT05072145 (ClinicalTrials.gov)
Plain language summary
Sepsis is a severe condition that results from infection. In addition to costly care, sepsis is a leading cause of death and disability. When comparing outcomes, those treated for sepsis in lower volume emergency departments fare worse and rural emergency departments often have lower patient volumes. While telehealth has been shown to improve sepsis care, the effect of telehealth on costs and long-term outcomes for patients is unclear. This study will use Medicare claims data to compare outcomes for people with sepsis in rural emergency departments who had video telehealth used with those who did not have video telehealth used, with the goal of measuring how telehealth affects healthcare costs, hospital readmissions and deaths after hospital discharge.
Background & rationale
Sepsis is a systemic response to infection that affects over 1.7 million adults and results in nearly 270,000 deaths in the USA annually [1]. Almost one out of every three in-hospital deaths can be linked to sepsis, and even among survivors, long-term disability and mortality are common [1–3]. Additionally, sepsis is the most expensive condition treated in US hospitals, costing over US$41.5 billion [4,5].
The Surviving Sepsis Campaign (SSC) develops evidence-based international guidelines for treating patients with sepsis to improve clinical outcomes. The SSC emphasizes the importance of early resuscitation by early recognition and management [6–10]. Emergency departments (EDs) provide an important service in ensuring timely and appropriate guideline-concordant care, as half of sepsis patients are admitted through EDs [11,12].
60 million residents in USA (19%), live in rural areas [13]. Rural EDs face unique challenges in providing time-sensitive critical care, including reduced staffing, surge capacity and greater proximity to specialty care [14,15]. Sepsis patients in low volume EDs have higher mortality and worse outcomes, which may be due, in part, to these EDs having lower compliance with SSC guidelines and bundles, compounding the challenges rural EDs already face [16–18].
Provider-to-provider ED-based telehealth (tele-ED) affords rural clinicians expert consultation for high-risk patients in rural EDs through a high-definition video connection. Access to specialized staff with expertise in treating time-sensitive conditions has been shown to expedite care in stroke, cardiac and trauma patients [19–21]. In one case series, 38% of rural tele-ED encounters began even before local physician evaluation, highlighting the role that telehealth can play in improving early access to specialty care [22]. Sepsis is uniquely suited to provider-to-provider telehealth, because it is a low-prevalence condition in many rural EDs, yet it requires very early care with complex treatment pathways that, fortunately, are not technology-intensive and can be administered in any rural ED. However, currently the benefit of tele-ED for sepsis care in terms of cost and patient outcomes remains largely undefined.
The objective of this paper is to report the methods planned for our study to evaluate the differences in costs and long-term outcomes for sepsis patients presenting to rural EDs with provider-to-provider tele-ED capabilities compared with sepsis patients presenting to rural non-telehealth-capable EDs. We hypothesize that telehealth will improve the quality of early care and reduce organ failure, hospital costs and post-discharge costs through decreased debility. We also hypothesize that decreased debility in tele-ED treated patients will lead to fewer readmissions and lower 90-day mortality.
Methods & analysis
Study design
This study is a multicenter retrospective propensity-matched comparative effectiveness study of tele-ED use for age-qualifying Medicare beneficiaries who present to a rural ED with sepsis from 2017 through 2019. We have identified hospitals that subscribe to a single large tele-ED provider as intervention hospitals, and we will identify similar hospitals without tele-ED services as control hospitals. This study will be reported using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement and the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) [23,24].
Study population
All age-qualifying (age ≥65 years) Medicare beneficiaries with at least one rural hospital ED visit followed by hospital admission for sepsis between 1 January 2017 and 31 December 2019 will be identified in Medicare beneficiary administrative claims data and included in the analysis. We defined a cohort of non-federal rural EDs that comprised all rural EDs subscribing to the single tele-ED service (n = 166, Table 1), and we will match these hospitals in a 1:2 ratio with a set of similar control hospitals. All included hospitals will be general medical and surgical hospitals with an on-campus ED in the rural USA. Hospitals will be classified as rural if their Rural Urban Commuting Area Code designates them as one of the categories of: large rural, small rural, or isolated, based on the hospital zip code [25,26]. Figure 1 shows the geographic distribution of intervention hospitals.
| Tele-ED capable hospitals (n = 166) | |
|---|---|
| Provider type, n (%) | |
| CAH | 159 (96) |
| RRC | 1 (1) |
| MDH | 1 (1) |
| MDH and RRC | 1 (1) |
| SCH | 2 (1) |
| SCH and RRC | 2 (1) |
| Annual ED visits, median (IQR) | 1925 (2710) |
| 0–1327, n (%) | 58 (35) |
| 1328–3350, n (%) | 61 (37) |
| 3351–6521, n (%) | 23 (14) |
| 6522–11574, n (%) | 19 (11) |
| 11575 or more, n (%) | 5 (3) |
| Annual facility inpatient days, median (IQR) | 1838 (3653) |
| 0–1004, n (%) | 50 (30) |
| 1005–1970, n (%) | 36 (22) |
| 1971–3367, n (%) | 28 (17) |
| 3368–6389, n (%) | 24 (14) |
| 6390 or more, n (%) | 28 (17) |
| Rural-urban commuting codes, n (%) | |
| Large Rural | 13 (8) |
| Small Rural | 47 (28) |
| Isolated | 106 (64) |
| Population density (population per square mile), median (IQR) | 25 (212) |
| 0–8.05, n (%) | 53 (32) |
| 8.05–45.95, n (%) | 42 (25) |
| 45.95–174.95, n (%) | 23 (14) |
| 174.95–599.4, n (%) | 31 (19) |
| 599.4 or more, n (%) | 17 (10) |
| Distance to nearest city of 100,000 people (kilometers), median (IQR) | 170 (164) |
These variables will be considered for the hospital-level propensity-matched cohort.
CAH: Critical access hospital; ED: Emergency department; IQR: Interquartile range; MDH: Medicare dependent hospital; RRC: Rural referral center; SCH: Sole community hospital; Tele-ED: Telehealth-capable ED.
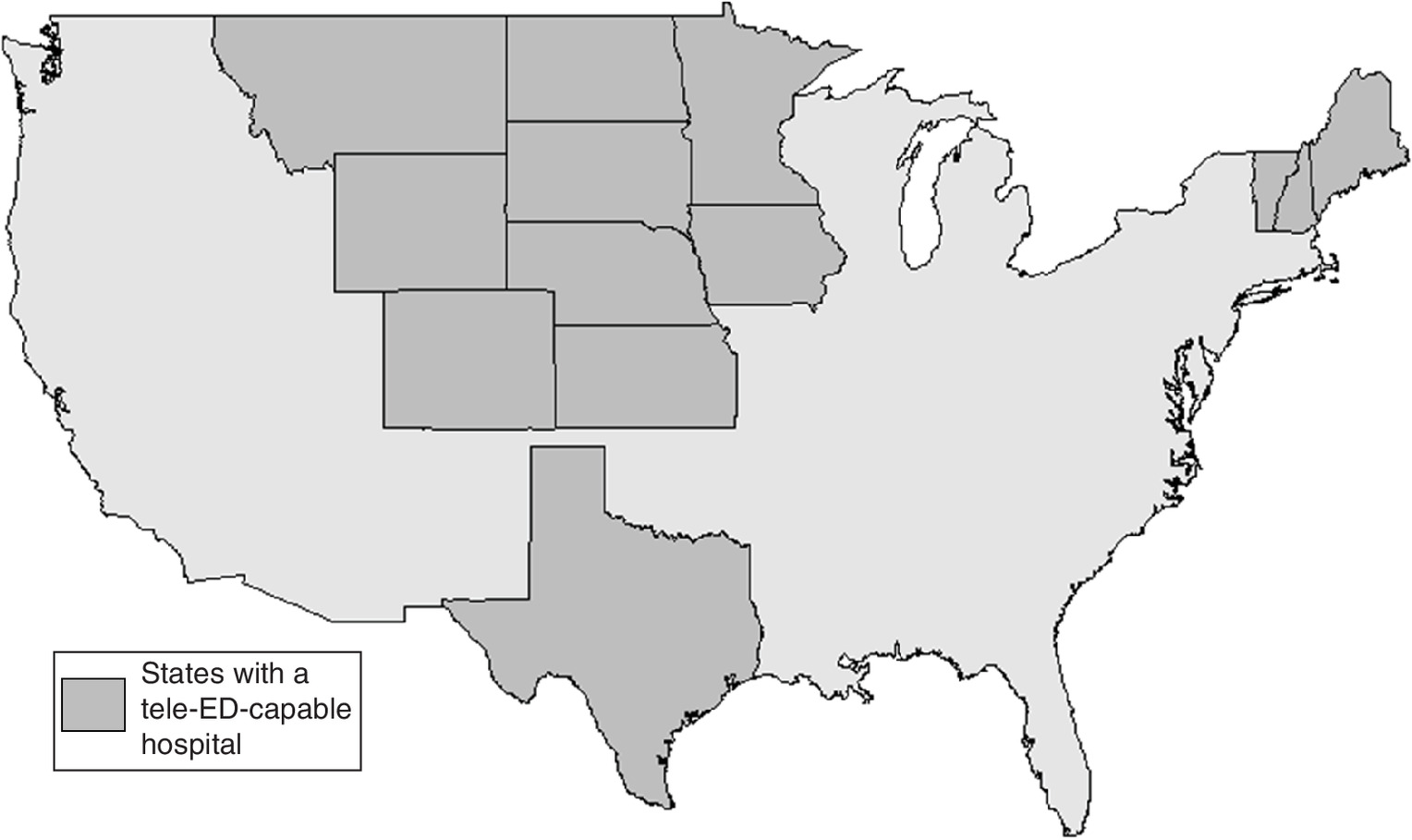
Figure 1. Geographic spread of emergency department telehealth-capable hospitals.
Tele-ED: Telehealth-capable ED.
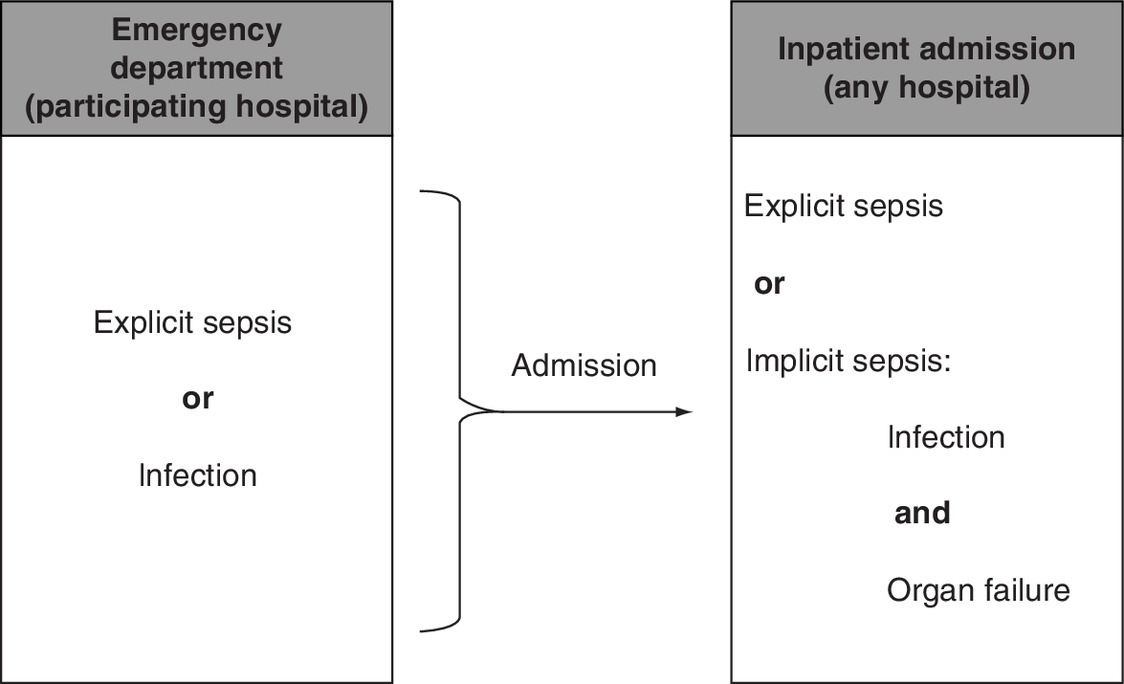
In our study, we will define sepsis according to International Classification of Diseases, 10th edition (ICD-10) diagnosis codes (Supplemental Appendix 1). We will use an inclusive definition of sepsis, using both explicit and implicit (coexisting infection and organ failure codes) diagnosis codes from hospital inpatient discharge [27]. Further, we will then require that the corresponding rural ED visit includes either an explicit diagnosis code of sepsis or infection, to exclude hospital-acquired cases of sepsis (Figure 2). We will also conduct a sensitivity analysis using only cases diagnosed with severe sepsis, with or without shock. Cases will be included only if the initial ED visit occurs in hospitals identified as part of our initial cohort of hospitals (either tele-ED intervention hospitals or matched control hospitals); however, inpatient admission may have occurred at the same or a different hospital after inter-hospital transfer. We will exclude patients with hospital length-of-stay of greater than 30 days. Considering that this study relies on administrative claims data alone, no clinical or physiologic severity of illness criteria will be applied.
Intervention
All tele-ED-capable hospitals for this study are those hospitals that subscribe to a single tele-ED provider. Avera eCARE, based in Sioux Falls, South Dakota, is the largest tele-ED service provider in North America. The provider-to-provider tele-ED service provides 24-h high-definition on-demand video telehealth services to subscribing hospitals. Local clinical staff connect virtually with an ED nurse and board-certified emergency physician by activating a button on the ED wall. Tele-ED staff have access to the local electronic medical record, and they make recommendations on clinical care, provide nursing charting, physician order entry and coordination of care for inter-hospital transfers. eCARE uses standardized call log software with decision-support, screening protocols, and checklists designed to enable adherence with treatment guidelines. In 2017, eCARE implemented a standard sepsis screening and treatment tool for use in tele-ED subscribing hospitals. This process recommended that triage nurses using a standard SIRS-based electronic trigger, and it recommended tele-ED activation for sepsis screen-positive cases with hypotension, altered mental status or organ failure evidenced on standard sepsis laboratory screening [28].
Patient/public involvement
Patients and the public have not contributed to the study design. They also will not be engaged in the implementation of the study.
Data sources
Data for this project will be obtained from telehealth provider data, Medicare claims and hospital-level data:
1.
Avera eCARE Tele-ED Subscription Log – Telehealth initiation dates were used to identify hospitals subscribing to the eCARE service, which confirms hospitals in our sample with EDs that have telehealth capability.
2.
Emergency Medicine Network's (EMNet) National ED-Inventory (NEDI)-USA Survey (2016–2018) – The NEDI-USA survey, which is sent to all non-federal, non-specialty US EDs, allows us to determine which hospitals use telehealth in the ED [29,30]. Responses to the survey question “Does your ED receive telemedicine services for patient evaluation?” can confirm control hospitals with EDs that have no telehealth capability. To address non-response, a control hospital was defined as a hospital with a ‘no’ response in all years, a ‘no’ response in at least 1 year with remaining responses being missing, or inclusion of control data for 2 years only from hospitals with a ‘no’ in 2016 and 2017 and a ‘yes’ in 2018.
3.
American Hospital Association (AHA) Annual Survey (2018) –AHA Annual Survey data will be used to obtain hospital-level covariates for both tele-ED and non-tele-ED hospitals [31].
4.
5.
Medicare Claims Data (2017–2019) – Medicare claims for patient-level administrative data containing data from the Master Beneficiary Summary File (MBSF, including chronic conditions, and other chronic conditions), inpatient, outpatient, carrier claims, home health, hospice, skilled nursing and durable medical equipment will be used to identify care delivered, long-term clinical outcomes and cost of care for our outcomes.
6.
Avera eCARE Call Log (2017–2019) – the call log contains identifiers on all tele-ED contacts during the study period. These data will be used to identify which patients in Medicare data had tele-ED used in the rural ED. Data from the call log will be linked with Medicare data using a probabilistic algorithm matched on patient date of birth and/or age, ED date of service, sex and treating hospital, as we have previously [20,21,34–36].
Our cohort will ultimately be generated by matching in a 1:2 ratio all identified tele-ED-capable hospitals subscribing to the Avera eCARE service between 2017 and 2019 with non-tele-ED control hospitals using variables from the AHA Survey and US Census data, matching only to hospitals confirmed not to have another telehealth provider based on the NEDI-USA data. The justification for 1:2 matching is that tele-ED cases in participating hospitals are limited, so we want to maximize power for analytic efficiency and sample size reduction while excluding hospitals that are qualitatively different.
Exposure of interest
Primary exposure
The primary exposure of interest is treatment within a tele-ED-capable hospital, defined as being treated in a hospital with an active Avera eCARE tele-ED subscription.
Secondary exposure
The secondary exposure of interest is being treated with the use of tele-ED care. Treatment with the use of tele-ED care is defined as having a Medicare-identified rural ED visit that probabilistically matches to a case in the eCARE call log (see Data Sources). Cases in tele-ED-capable hospitals without a matching case in the call log are assumed not to have had tele-ED used. We anticipate that with the low case volumes in rural EDs, linking known identifiers on a given date of service will have very high linkage accuracy.
Outcomes
Primary outcome
The primary outcome is reimbursed total healthcare expenditures among index hospitalization survivors. This calculation will include all Medicare-reimbursed costs from inpatient, observation, and outpatient visits, Medicare-covered skilled nursing facility care, ambulance service, home health, durable medical equipment and hospice from admission to 30 days post-discharge (Table 2). No outpatient medication costs will be included in this calculation because Part D coverage is voluntary for Medicare beneficiaries.
| Category | Time frame | Specific costs included |
|---|---|---|
| Total healthcare expenditures | Index ED visit until 30 days after discharge | • All inpatient costs • All observation stay costs • All emergency department costs • All clinic visit costs • All ambulance costs • All residential treatment (nursing home, acute rehabilitation, long term acute care, and other residential care facilities) costs (if covered by Medicare only) • All home health costs • All durable medical equipment costs (if covered by Medicare only) • All hospice costs |
| Total index ED costs | Index ED visit until discharge from initial hospitalization | • All ED costs • ED portion of inpatient hospitalizations (by charge center) |
| Total index hospitalization costs | Index ED visit until discharge from index hospitalization | • All inpatient costs • All observation stay costs |
| Total transfer costs | Index ED visit until discharge from index hospitalization | • All ambulance costs |
| Total post-discharge costs | Index hospitalization discharge until 30 days after discharge | • All post-discharge inpatient costs • All post-discharge emergency department costs • All clinic visit costs • All post-discharge ambulance costs • All residential treatment (nursing home, acute rehabilitation, long term acute care and other residential care facilities) costs (if covered by Medicare only) • All home health costs • All durable medical equipment costs (if covered by Medicare only) • All hospice costs |
| Total inpatient readmission costs | Index hospitalization discharge until 30 days after discharge | • All post-discharge inpatient costs (including the emergency department costs for any emergency department visits that lead to hospital admission) |
| ED: Emergency department. | ||
Secondary outcomes
Secondary outcomes include 90-day mortality (measured from hospital admission), hospital length-of-stay, hospital 30-day readmissions, and category-specific costs such as total ED costs (index hospitalization), total inpatient costs (index hospitalization), transfer costs, post-discharge costs (after index hospitalization) and inpatient readmission costs.
Cost perspective
For this study, we are taking the perspective of the payer. Medicare reimbursements are expected to approximate actual costs of hospital care. Reimbursement will be obtained from the Medicare Claims data.
Time Horizon
Total costs will be measured between hospital admission and 30 days after hospital discharge (to align with the Medicare readmission metrics). Mortality rates will be assessed at 90 days post-hospital admission.
Discount Rate & Currency
We will calculate all costs in 2019 US dollars (2019 $USD). Costs will use a discount rate calculated from the Consumer Price Index for Medical Care, as it contains medical care services and medical care commodities and reflects temporal changes in the cost of medical care broadly [37].
Covariates
Additional variables are defined for use in the propensity score and risk-adjustment models. For hospital-level matching, potential covariates will be identified based on theory, and we will include variables in the final model that have an association (p < 0.20) with Avera tele-ED subscription. We plan to use the following hospital-level covariates:
•
Special hospital designation status defined under Medicare reimbursement structure (Critical Access Hospital [CAH], Rural Referral Center [RRC], Medicare Dependent Hospital [MDH], Sole Community Hospital [SCH], dual designation of RRC and MDH and dual designation of RRC and SCH);
•
Number of hospital emergency department visits in a 12-month period determined as fiscal or calendar year by the hospital [31];
•
Number of inpatient occupied bed-days in a 12-month period determined as fiscal or calendar year by the hospital [31];
•
Distance to nearest city of at least 100,000 population;
•
Population per square mile at census tract level;
•
Distance to the nearest Avera eCARE-subscribing hospital.
For patient-level severity of illness adjustment, we will use the following covariates:
•
Age (categorical);
•
Sex;
•
Race;
•
Organ dysfunction (based on ICD-10 codes);
•
Source of infection (based on ICD-10 codes);
•
Nursing home residence (before index visit);
•
Year (to capture temporal trends in sepsis diagnosis and outcomes).
Missing data
This analysis will be conducted as a complete case analysis. No imputation techniques will be used. Medicare beneficiaries not included in the call log will be assumed not to have had telehealth used.
Causal model
We hypothesize that the use of tele-ED for sepsis patients in rural hospitals will lead to reduced costs and more favorable long-term outcomes. This pathway is hypothesized to result from more timely high-quality resuscitation care (early appropriate antibiotics, fluid resuscitation, improved use of vasoactive medications, rapid diagnostic studies) associated with tele-ED use that leads primarily to reductions in organ failure. Prior data have shown that early appropriate antibiotics are associated with a lower rate of subsequent septic shock [40]. We expect that avoiding organ failure will lead to fewer complications, fewer procedures, fewer ICU admissions, shorter length-of-stay in the ICU and hospital and fewer discharges to skilled nursing facilities. We also expect cost-savings to result from decreased debility, fewer readmissions and improved functional outcomes at discharge.
Because it is likely that the highest severity patients are the ones that receive tele-ED care, our primary analysis will be done at the level of the hospital assignment. We assume that severity of illness will be similar across rural hospitals, which minimizes the effect of selection bias from only the most severe patients being treated with tele-ED. This assumption is necessary because there is no physiologic severity of illness measure provided in the claims data. We hypothesize that having tele-ED available will lead to better aggregate outcomes in the hospital-level analysis, and that the effect size would be even larger in a risk-adjusted patient-level analysis.
Assumptions
We assume that Medicare reimbursement is a close approximation of cost of care, and we assume that all healthcare for Medicare beneficiaries is billed to Medicare. We assume that all deaths are reported to and validated by Medicare with accurate death dates. In obtaining our cohort of matched hospitals, we assume that the covariates most useful in identifying similar hospitals are those that are the most strongly associated with a hospital subscribing to tele-ED services. While we recognize that tele-ED is likely used for patients with greater illness severity [41], we assume that the aggregate illness severity across all the patients treated in a participating hospital is similar between hospitals. This assumption is based on our prior work showing that rural hospital bypass is rare in sepsis care [42].
Proposed statistical methods & analysis
Hospital matching
We will use a hospital-level matching strategy for data reduction to identify a cohort of non-tele-ED hospitals that are similar to our tele-ED hospitals.
Propensity score
We will use a propensity score to estimate the probability that a hospital is a tele-ED hospital in our sample of rural hospitals. This propensity score will be built with each US rural hospital representing one record, with hospital-level characteristics included to predict tele-ED subscription. Hospital-level characteristics will include hospital size, volume, rurality, geographical proximity to the nearest city with 100,000 residents (Euclidean distance), and the residing city's population size. Variable selection for the covariates to include in this model will be performed by comparing Akaike information criteria (AIC) between models, in a purposeful selection manner.
Since cost is a primary outcome in our study, balancing the hospitals' reimbursement model (special designation status) is essential. We will match this variable exactly to ensure that we are comparing costs within a fixed reimbursement structure. Facilities will be divided into CAHs, RRCs, MDHs, SCHs, dually designated MDH and RRC, and dually designated SCH and RRC. CAHs comprise 159 (96%) of the tele-ED hospitals included, and three hospital designations have only one tele-ED subscribing hospital. Because of this, the propensity score will be calculated using all the hospitals, and then matching will take place within each subset of hospital designation separately.
Proximity
To minimize geospatial distance between tele-ED and control hospitals, we will calculate the distance between each candidate control hospital to the nearest tele-ED hospital. This variable will be used in matching (below), but we will not include it in the propensity score.
Matching
The hospital matching process will have four main steps:
•
A logistic regression model (propensity score) will be used to calculate the predicted probability of tele-ED subscription using hospital-level variables (ED visits, rurality, facility inpatient days, population size and distance to nearest city);
•
Hospitals and their corresponding predicted probabilities will be stratified by their special hospital designation status (financial reimbursement model);
•
Within each designation, candidate control hospitals within an empirically defined caliper width of predicted probabilities between tele-ED and non-tele-ED hospitals will be considered for matching;
•
The two control hospitals with the shortest distance to the corresponding tele-ED hospital will be selected.
Balance will be measured after matching using standardized mean differences. Because the goal of using hospital matching will be for data reduction only, we will accept ‘best possible’ matches even if matching is imperfect, to prioritize sample size over match proximity at this stage. We will also conduct analyses clustering standard errors on hospital.
Primary analysis
We will assign participants to tele-ED-exposed versus unexposed cohorts based on whether they presented initially to a tele-ED-capable hospital for our primary analysis, regardless of whether tele-ED was used for their care.
We will analyze reimbursable total healthcare costs using generalized estimating equations (GEE) models, clustered on presenting hospital, with total healthcare costs as the outcome and treatment within a tele-ED-capable hospital as the exposure of interest. We will include potentially confounding factors associated with severity of illness (as described in Covariates) in our model. An identity link and exchangeable correlation matrix will be used. For continuous secondary outcomes such as hospital length-of-stay and category-specific costs, we will use a similar model, and for dichotomous outcomes (90-day mortality, hospital 30-day readmissions), we will use a logit link function.
Patient-level propensity score matching
We will derive a patient-level propensity score using logistic regression within cases presenting to tele-ED-capable hospitals only. This score will include patient-level predictors (as described in Covariates), with the outcome of tele-ED use. No patients presenting to non-tele-ED hospitals will be included in the derivation of this propensity score.
The regression function derived from this propensity score will be applied to patients presenting to all non-tele-ED hospitals to calculate a predicted probability of tele-ED use (had tele-ED been available in those facilities). Each case in the entire dataset will have a predicted probability of tele-ED use (even those in non-tele-ED-capable hospitals). We will match each case that had tele-ED used to a case from a non-tele-ED hospital with a similar propensity score using an optimal matching algorithm within an empirically derived caliper width to minimize differences between groups while maintaining adequate sample size. We will use standardized mean differences to evaluate balance between groups, using a threshold of 0.1 to indicate good balance on available covariates. We will use a 1:1 match for this analysis because we prioritize balance between the groups over sample size. Subsequent analyses will be conducted using conditional regression techniques clustered on the matching pair.
Additionally, validation of the matching process will be done by comparing cases in tele-ED-capable hospitals, who did not have tele-ED used to matched controls from non-tele-ED hospitals. If there is no difference in costs, this supports our matching process. If the cost is lower for the tele-ED hospital patients, this may indicate benefits of being treated in a tele-ED hospital even when tele-ED was not used in care.
Secondary analysis
The secondary patient-level analysis will stratify participants into whether they had telemedicine used, compared with similar patients in non-tele-ED hospitals. The tele-ED-used cohort will be compared with the propensity-matched patients in the non-tele-ED-capable hospitals.
We will use a doubly robust regression model to ensure adjustment for residual confounding from imperfect matching, as appropriate. This conditional linear regression will include treatment group as a predictor variable in addition to any covariates with poor balance, using our primary outcome of total healthcare expenditures. We will use an identity link and exchangeable correlation matrix. Secondary analyses will be conducted using an identity link for continuous outcomes and a logit link for dichotomous outcomes, as described above.
Additional subgroup analyses will be conducted among patients who require surgery, patients who are transferred, and patients with diagnosis codes for septic shock (the most severe form of sepsis).
Sample size
In a sample of tele-ED CAHs (n = 18) in the upper Midwest that subscribed to Avera tele-ED, we found that these rural EDs had a mean of 16 sepsis cases annually [43]. Extended to our cohort of 500 hospitals for Medicare beneficiaries only (estimated 60% of sepsis cases), this would result in an estimated 14,400 sepsis cases over the years of 2017–2019 [44]. Using Medicare cost data, with 80% power, this would allow for a minimal detectable difference of US$878 (α = 0.05, μ = US$28,242, σ = $17,719, allocation ratio = 2), with the mean case cost of US$28,242.
Anticipated results
Through prior work demonstrating the association of tele-ED use in treating sepsis with improved short-term outcomes, the long-term perspective on costs is important. Prior quality improvement initiatives that optimize early sepsis care have been shown to decrease healthcare costs, through decreased health resource utilization through improved clinical outcomes [45,46]. Furthermore, earlier sepsis diagnosis is also associated with decreased cost [47]. Because the tele-ED intervention is expected to improve adherence with sepsis guidelines very early in treatment, we expect that tele-ED will also be associated with reduced need for ICU care, less discharge debility, improved long-term survival and decreased index hospitalization costs, all of which are expected to lead to a decrease in overall expenditures [48]. We expect to see a modest decrease in expenses in our primary hospital-level analysis. If we see that our patient-level analysis shows a more substantial decrease, that finding will further support our hypothesis that telehealth use in sepsis care is associated with less disability and lower costs. If our patient-level analysis shows that tele-ED-enabled cases have higher expenses, we will conclude that our severity of illness measure was imperfect, but we will use the secondary outcomes to better understand the mechanism of the effect (e.g., categories in which expenses were different). If we see that expenses are higher in our primary analysis and that mortality is lower, we will conclude that increased costs are related to improved survival – a patient-relevant and important explanation for the overall effect observed (Table 3). Figure 3 outlines the analysis proposed for this project.
| Hospital-level expenses | Patient-level expenses | 28-day hospital-free days | Readmissions | Interpretation |
|---|---|---|---|---|
| Reduced | Reduced | Increased | Reduced | Tele-ED is associated with improved early care, which decreases organ failure and long-term disability |
| Reduced | Increased | Reduced | Increased | Tele-ED patients were the most severely ill. Because aggregate hospital-level analysis shows decreased expenses, tele-ED is associated with reduced expenses, but it is applied to a very selected sample of patients |
| Increased | Increased | Reduced, through longer length-of-stay and reduced mortality | Increased | Tele-ED is associated with prolonged hospital survival, which may be associated with increased survival to discharge, but more disability in survivors |
| Tele-ED: Telehealth-capable ED. | ||||
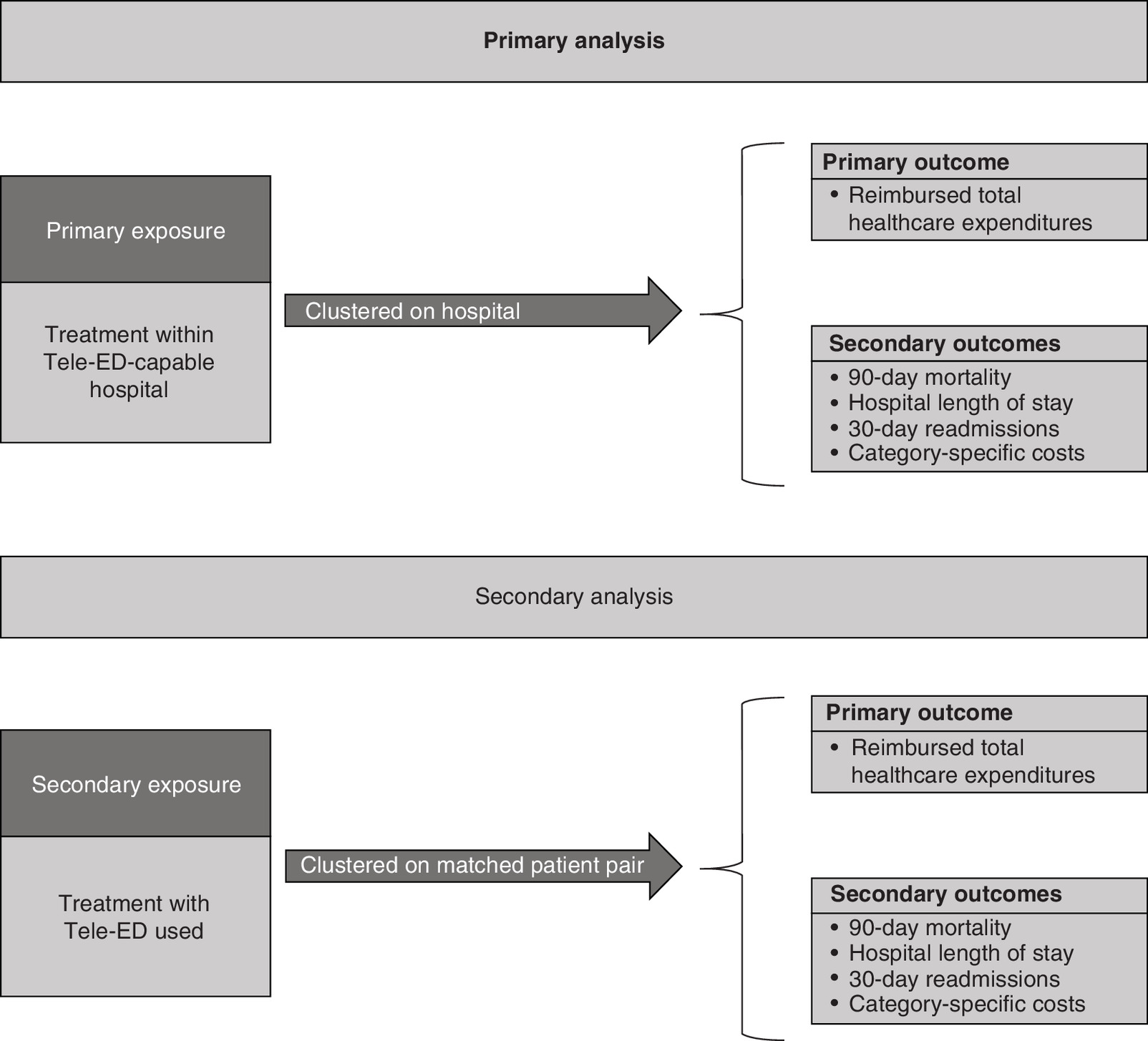
Figure 3. Diagram that shows the proposed analysis.
Tele-ED: Telehealth-capable ED.
Data storage & management
Data will be stored on a secure, restricted access, password-protected server accessible only to the study team. The original data will be stored in a locked vault with keycard and biometric access required to enter. All Medicare Beneficiary ID numbers will be encrypted, and the dataset will be deidentified prior to analysis. All identifiable data will be transmitted by encrypted portable media or secure encrypted file transfer. We will report only aggregate data, and cells with fewer than ten observations will be concealed to minimize the risk of loss of patient confidentiality. The study principal investigator (PI) will have access to the final dataset and will take ultimate responsibility for its integrity.
Ethics & dissemination
Ethics approval
The study protocol was reviewed and approved by the institutional review board (IRB) at both the University of Iowa and Avera eCARE under waiver of informed consent.
Dissemination & data sharing
We will disseminate the results of this analysis by publication in peer-reviewed journals, presentations at scientific meetings, and production of research and policy briefs. Data sets will not be available for dissemination because of the data use requirements for each of our data sets, but we encourage cross-institution collaborations. The study team will collaborate with interested investigators to conduct additional analyses while maintaining the security of the dataset using a standard written request process that is evaluated by the study executive committee.
Strengths & limitations
Strengths
The main strength of this study is that we will be measuring the real-world application of tele-ED care in an existing and functioning tele-ED network. Other studies have reported the results of pilot programs under highly controlled conditions unlikely to be replicated in real-world practice. Our work will report the actual experience in a network functioning at scale.
The second strength is that we will be conducting this work using data available from non-tele-ED hospitals for comparative-effectiveness analysis. Care in hospitals with telehealth services can evolve even in non-telehealth patients over time because of interactions with the hub network, limiting the ability to observe differences between telehealth-enabled care and control cases [21,34,49–51]. By using a large database that compares outcomes within hospitals with EDs that participate in the network and others with EDs without telehealth capabilities, we will be able to see differences that may not be apparent within facilities already participating in a telehealth program alone.
Third, conducting this analysis at the hospital level, then using a propensity score to limit cases in non-tele-ED capable hospitals for the participant-level analysis is a strong strategy to reduce the effect of confounding by indication. Telehealth studies in acute care are often challenged by the strong relationship between severity, indication and telehealth use. By selecting only cases in non-telehealth capable EDs to compare with telehealth-enabled cases will reduce confounding by removing cases very unlikely to have had telehealth used. Comparing cases within a hospital only can be subject to confounding by indication because cases that are seemingly similar on measured covariates still had a reason telehealth was used – and this reason could be associated with our outcomes. This effect is not observable when controls come from other hospitals.
Finally, our use of cost as an outcome is a strength. Cost–effectiveness is one of the most important, yet difficult questions in telehealth policy. Using a Medicare-based analysis with a robust control group is a powerful way to estimate the cost avoidance associated with improved care from telehealth use.
Limitations
The two greatest limitations of this work are its observational design and the lack of a robust severity of illness variable. Because our primary data source is administrative data, we will be able to access a very large sample, even in hospitals that do not participate in a telehealth network. The disadvantage, though, is that administrative claims contain minimal information about the clinical interventions performed as part of clinical care or physiologic severity of illness measures. This limitation may allow some residual confounding that cannot be adjusted with the variables we include in our propensity score methods. Another limitation is that our intervention hospitals all come from participation in a single tele-ED network and all patients are age-qualifying Medicare beneficiaries. The findings from that network may not generalize to all tele-ED interventions or to non-Medicare patients.
Conclusion
The proposed study is the first large-scale robust comparative effectiveness study of clinical and cost outcomes in a mature acute care telehealth network. Measuring the effect of tele-ED consultation on outcomes in rural sepsis care is important because of the prevalence of sepsis in rural hospitals and the improved outcomes associated with its appropriate early treatment. Future work will focus on optimizing specific telehealth-based strategies and identifying characteristics associated with patients most likely to be affected by tele-ED care.
•
This study will measure the effect of provider-to-provider telehealth in rural emergency departments on total costs of care and post-discharge outcomes in sepsis patients.
•
Cost is an important outcome in telehealth comparative effectiveness studies.
•
Measuring the effect between telehealth-capable and non-telehealth-capable hospitals and also using a propensity matched cohort design for participant-level stratification are strengths to limit the effect of confounding by indication.
•
Using Medicare administrative data allows for a very large sample with non-telehealth controls, but it limits data available for risk adjustment on physiologic severity of illness.
Author contributions
NM Mohr: conception and study design, acquisition of data, analysis and interpretation of data, drafting and revising the manuscript; AR Schuette: analysis and interpretation of data, drafting and revising the manuscript; F Ullrich: acquisition of data, analysis and interpretation of data, critically revising the manuscript for important intellectual content; LJ Mack, K DeJong, A Bell, M Pals: study design, acquisition of data, interpretation of data, critically revising the manuscript for important intellectual content; CA Camargo, KS Zachrison, KM Boggs, AR Schuette: acquisition of data, interpretation of data, and critically revising the manuscript for important intellectual content; DM Shane, KD Carter: study design, interpretation of data, and critically revising the manuscript for important intellectual content; KAS Merchant: interpretation of analysis and critically revising the manuscript for important intellectual content; MM Ward: conception and study design, acquisition of data, analysis and interpretation of data, critically revising the manuscript for important intellectual content.
Acknowledgments
The authors would like to acknowledge W Berg (Avera eCARE) for his help with data management; and N Kramer (University of Iowa) for his editorial assistance.
Financial & competing interests disclosure
This research is funded by the Rural Telehealth Research Center which is funded by a cooperative agreement from the Health Resources and Services Administration (HRSA, cooperative agreement U1C RH29074). NM Mohr is additionally supported by the Agency for Healthcare Research and Quality (AHRQ, grant K08 HS025753). The views expressed are those of the authors only and do not represent the position of the funders or the US government. LJ Mack, K DeJong, A Bell, M Pals are employed by an organization that provides emergency department-based telehealth services. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval for all human subjects research activities.
Supplementary Material
File (supplemental appendix 1.docx)
- Download
- 26.42 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Rhee C, Dantes R, Epstein L et al. Incidence and Trends of Sepsis in US Hospitals Using Clinical vs Claims Data, 2009–2014. JAMA 318(13), 1241–1249 (2017).
2.
Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA 304(16), 1787–1794 (2010).
3.
Prescott HC, Osterholzer JJ, Langa KM, Angus DC, Iwashyna TJ. Late mortality after sepsis: propensity matched cohort study. BMJ 353, i2375 (2016).
4.
Buchman TG, Simpson SQ, Sciarretta KL et al. Sepsis Among Medicare Beneficiaries: 1. The Burdens of Sepsis, 2012–2018. Crit. Care Med. 48(3), 276–288 (2020).
5.
Mcdermott KW, Roemer M. Most Frequent Principal Diagnoses for Inpatient Stays in U.S. Hospitals, 2018: Statistical Brief #277. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality (US), MD, USA (2006).
6.
Rhodes A, Evans LE, Alhazzani W et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 43(3), 304–377 (2017).
7.
Rivers E, Nguyen B, Havstad S et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N. Engl. J. Med. 345(19), 1368–1377 (2001).
8.
Kent N, Fields W. Early recognition of sepsis in the emergency department: an evidence-based project. J. Emerg. Nurs. 38(2), 139–143 (2012).
9.
Kumar A, Roberts D, Wood KE et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 34(6), 1589–1596 (2006).
10.
Yealy DM, Kellum JA, Huang DT et al. A randomized trial of protocol-based care for early septic shock. N. Engl. J. Med. 370(18), 1683–1693 (2014).
11.
Rhee C, Jones TM, Hamad Y et al. Prevalence, Underlying Causes, and Preventability of Sepsis-Associated Mortality in US Acute Care Hospitals. JAMA Network Open 2(2), e187571–e187571 (2019).
12.
Wang HE, Jones AR, Donnelly JP. Revised National Estimates of Emergency Department Visits for Sepsis in the United States. Crit. Care Med. 45(9), 1443–1449 (2017).
13.
US Census Bureau. One in Five Americans Live in Rural Areas. www.census.gov/library/stories/2017/08/rural-america.html
14.
Feazel L, Schlichting AB, Bell GR et al. Achieving regionalization through rural interhospital transfer. Am. J. Emerg. Med. 33(9), 1288–1296 (2015).
15.
Williams JM, Ehrlich PF, Prescott JE. Emergency medical care in rural America. Ann. Emerg. Med. 38(3), 323–327 (2001).
16.
Kocher KE, Haggins AN, Sabbatini AK, Sauser K, Sharp AL. Emergency department hospitalization volume and mortality in the United States. Ann. Emerg. Med. 64(5), 446–457.e446 (2014).
17.
Mohr NM, Harland KK, Shane DM, Ahmed A, Fuller BM, Torner JC. Inter-hospital transfer is associated with increased mortality and costs in severe sepsis and septic shock: an instrumental variables approach. J. Crit. Care 36, 187–194 (2016).
18.
Gaieski DF, Edwards JM, Kallan MJ, Mikkelsen ME, Goyal M, Carr BG. The relationship between hospital volume and mortality in severe sepsis. Am. J. Respir. Crit. Care Med. 190(6), 665–674 (2014).
• Highlights the importance of hospital characteristics on sepsis outcomes, and it demonstrates that care in a low-volume hospital is a specific risk factor for poor outcomes.
19.
Miller AC, Ward MM, Ullrich F, Merchant KS, Swanson MB, Mohr NM. Emergency department telemedicine consults are associated with faster time-to-electrocardiogram and time-to-fibrinolysis for myocardial infarction patients. Telemed JE Health 26(12), 1440–1448 (2020).
20.
Mohr NM, Young T, Harland KK et al. Telemedicine is associated with faster diagnostic imaging in stroke patients: a cohort study. Telemed JE Health 25(2), 93–100 (2019).
21.
Mohr NM, Vakkalanka JP, Harland KK et al. Telemedicine use decreases rural emergency department length of stay for transferred North Dakota trauma patients. Telemed. J. E-health 24(3), 194–202 (2018).
22.
Heppner S, Mohr NM, Carter KD, Ullrich F, Merchant KaS, Ward MM. HRSA's evidence-based tele-emergency network grant program: multi-site prospective cohort analysis across six rural emergency department telemedicine networks. PLoS ONE 16(1), e0243211 (2021).
23.
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370(9596), 1453–1457 (2007).
24.
Husereau D, Drummond M, Petrou S et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)--explanation and elaboration: a report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health 16(2), 231–250 (2013).
25.
WWAMI Rural Health Research Center. Ruca Data: Zip Code RUCA Approximation. (2021). https://depts.washington.edu/uwruca/ruca-approx.php
26.
WWAMI Rural Health Research Center. RUCA Data Code Definitions. https://depts.washington.edu/uwruca/ruca-codes.php
27.
Rudd KE, Johnson SC, Agesa KM et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet 395(10219), 200–211 (2020).
28.
Mohr NM, Skow B, Wittrock A et al. Improving Access to High Quality Sepsis Care in a South Dakota Emergency Telemedicine Network. https://ruraltelehealth.org/briefs/2017-8-23_Access%20to%20Sepsis%20Care%20Emergency%20Telemedicine.pdf
29.
Zachrison KS, Boggs KM, Hayden EM, Espinola JA, Camargo CA. A national survey of telemedicine use by US emergency departments. J. Telemed. Telecare 26(5), 278–284 (2020).
30.
Sullivan AF, Richman IB, Ahn CJ et al. A profile of US emergency departments in 2001. Ann. Emerg. Med. 48(6), 694–701 (2006).
31.
American Hospitial Association. American Hospital Association Annual Survey. www.aha.org/
32.
United States Census Bureau. American Hospital Association Annual Survey. www.census.gov/en.html
33.
Environmental Systems Research Institute, Inc. (Esri). American Hospital Association Annual Survey. www.esri.com/en-us/home
34.
Mohr NM, Harland KK, Chrischilles EA, Bell A, Shane DM, Ward MM. Emergency department telemedicine is used for more severely injured rural trauma patients, but does not decrease transfer: a cohort study. Acad. Emerg. Med. 24(2), 177–185 (2017).
35.
Mohr NM, Young T, Harland KK et al. Emergency department telemedicine shortens rural time-to-provider and emergency department transfer times. Telemed. JE Health 24(8), 582–593 (2018).
36.
Vakkalanka JP, Harland KK, Wittrock A et al. Telemedicine is associated with rapid transfer and fewer involuntary holds among patients presenting with suicidal ideation in rural hospitals: a propensity matched cohort study. J. Epidemiol. Community Health 73(11), 1033–1039 (2019).
37.
US Bureau of Labor Statistics. Measuring the Price Change in the Consumer Price Index: Medical Care. www.bls.gov/cpi/factsheets/medical-care.htm
38.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med. Care 36(1), 8–27 (1998).
39.
Quan H, Sundararajan V, Halfon P et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 43(11), 1130–1139 (2005).
40.
Whiles BB, Deis AS, Simpson SQ. Increased time to initial antimicrobial administration is associated with progression to septic shock in severe sepsis patients. Crit. Care Med. 45(4), 623–629 (2017).
41.
Mohr N, Harland K, Chrischilles E, Bell A, Shane D, Ward M. Emergency department telemedicine is used for more severely injured rural trauma patients, but does not decrease transfer: a cohort study. Acad. Emerg. Med. 24(2), 177–185 (2017).
42.
Mohr NM, Harland KK, Shane DM et al. Rural patients with severe sepsis or septic shock who bypass rural hospitals have increased mortality: an instrumental variables approach. Crit. Care Med. 45(1), 85–93 (2017).
43.
Mohr NM, Harland KK, Okoro UE et al. TELEmedicine as an intervention for sepsis in emergency departments: a multicenter, comparative effectiveness study (TELEvISED Study). J Comp Eff Res 10(2), 77–91 (2021).
• The televised study is a related study using different methods, but upon which the current study methodology is based.
44.
Elixhauser A, Friedman B, Stranges E. Septicemia in U.S. Hospitals, 2009: Statistical Brief #122. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality (US), MD, USA (2006).
45.
Afshar M, Arain E, Ye C et al. Patient outcomes and cost-effectiveness of a sepsis care quality improvement program in a health system. Crit. Care Med. 47(10), 1371–1379 (2019).
46.
Huang DT, Angus DC, Dremsizov TT, Rivers EP, Clermont G. Cost-effectiveness of early goal-directed therapy in the treatment of severe sepsis and septic shock. Crit. Care 7(2), P232 (2003).
47.
Paoli CJ, Reynolds MA, Sinha M, Gitlin M, Crouser E. Epidemiology and costs of sepsis in the United States—an analysis based on timing of diagnosis and severity level*. Crit. Care Med. 46(12), 1889–1897 (2018).
48.
Mohr NM, Campbell KD, Swanson MB, Ullrich F, Merchant KA, Ward MM. Provider-to-provider telemedicine improves adherence to sepsis bundle care in community emergency departments. J Telemed Telecare 27(8), 518–526 (2021).
•• This study demonstrated that early telehealth for rural ED sepsis care was associated with improved compliance with Surviving Sepsis Campaign guideline adherence.
49.
Zhu X, Merchant KaS, Mohr NM, Wittrock AJ, Bell AL, Ward MM. Real-Time Learning Through Telemedicine Enhances Professional Training in Rural Emergency Departments. Telemed J E Health 27(4), 441–447 (2021).
• This qualitative study finds that the provider-to-provider telehealth has a benefit of providing ongoing professional education to rural providers through mentored patient interactions, which was a significant perceived reason to encourage its use.
50.
Moreno A, Schwamm LH, Siddiqui KA et al. Frequent hub-spoke contact is associated with improved spoke hospital performance: results from the Massachusetts General Hospital Telestroke Network. Telemed. JE Health 24(9), 678–683 (2018).
51.
Sharma R, Zachrison KS, Viswanathan A et al. Trends in telestroke care delivery: a 15-year experience of an academic hub and its network of spokes. Circ. Cardiovasc. Qual. Outcomes 13(3), e005903 (2020).
Information & Authors
Information
Published In
Pages: 703 - 716
PubMed: 35608080
Copyright
© 2022 Future Medicine Ltd.
History
Received: 1 February 2022
Accepted: 27 April 2022
Published online: 24 May 2022
Keywords:
Topics
Authors
Funding Information
Health Resources and Services Administration: U1C RH29074
Agency for Healthcare Research and Quality: K08 HS025753
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
An economic and health outcome evaluation of telehealth in rural sepsis care: a comparative effectiveness study. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0019
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Stefano Larcher, Giuseppe Marini, Alessandro Rigobello, Silvia De Rosa, Management of trauma in remote and austere settings: civilian implications of military-derived prolonged field care principles — A narrative review, Medicina Intensiva (English Edition), 10.1016/j.medine.2026.502564, (502564), (2026).
- Nicholas M. Mohr, Kimberly A.S. Merchant, Brian M. Fuller, Brett Faine, Luke Mack, Amanda Bell, Katie DeJong, Edith A. Parker, Keith Mueller, Elizabeth Chrischilles, Christopher R. Carpenter, Michael P. Jones, Steven Q. Simpson, Marcia M. Ward, The role of telehealth in sepsis care in rural emergency departments: A qualitative study of emergency department sepsis telehealth user perspectives, PLOS One, 10.1371/journal.pone.0321299, 20, 4, (e0321299), (2025).
- Nicholas M. Mohr, Tracy Young, J. Priyanka Vakkalanka, Knute D. Carter, Dan M. Shane, Fred Ullrich, Allison R. Schuette, Luke J. Mack, Katie DeJong, Amanda Bell, Mark Pals, Carlos A. Camargo, Kori S. Zachrison, Krislyn M. Boggs, Adam Skibbe, Marcia M. Ward, Provider‐to‐provider telehealth for sepsis patients in a cohort of rural emergency departments, Academic Emergency Medicine, 10.1111/acem.14857, 31, 4, (326-338), (2024).
- Kevin J Tu, Cole Wymore, Nedelina Tchangalova, Brian M Fuller, Nicholas M Mohr, The impact of telehealth in sepsis care: A systematic review, Journal of Telemedicine and Telecare, 10.1177/1357633X231170038, 31, 1, (3-13), (2023).