Systematic literature review of evidence in amyloid light-chain amyloidosis
Publication: Journal of Comparative Effectiveness Research
Abstract
Introduction: Treatment of amyloid light-chain (AL) amyloidosis, a rare disease with a <5-year lifespan, remains challenging. This systematic literature review (SLR) aimed to evaluate the current evidence base in AL amyloidosis. Methods: Literature searches on clinical, health-related quality of life, economic and resource use evidence were conducted using the Embase, MEDLINE and Cochrane databases as well as gray literature. Results: This SLR yielded 84 unique studies from: five randomized controlled trials; 54 observational studies; 12 health-related quality of life studies, none with utility values; no economic evaluation studies; and 16 resource use studies, none with indirect costs. Conclusion: This SLR highlights a paucity of published literature relating to randomized controlled trials, utility values, economic evaluations and indirect costs in AL amyloidosis.
Amyloidosis is a rare disease affecting approximately 5–12 persons per million per year [1]. The disease is characterized by the extracellular accumulation of insoluble amyloid fibril deposits on various organs and tissues [1]. Amyloid light-chain (AL) amyloidosis, a clonal plasma cell disorder, is the most severe form of amyloidosis, accounting for approximately 70% of all cases [2,3]. The deposition of monoclonal light chains in multiple organs can be progressive and can result in organ dysfunction and death [4]. The most common and critical organs affected are the heart (70–80% of patients) and kidneys (50–60% of patients) [5]. Early diagnosis is critical in improving patient outcomes; however, given the nonspecific nature of the symptoms, most patients with AL amyloidosis will require evaluation by multiple specialists, resulting in significant delays in diagnosis of up to 3 years [6]. A real-world study evaluating trends in disease characteristics, management and outcomes in patients with newly diagnosed AL amyloidosis reported that over one-third of patients die within the first year following diagnosis, and the 4-year survival rate was reported to be 54% [7]. Prognosis is especially poor among patients with severe organ involvement [8,9], with a median overall survival of approximately 3 months in patients with Mayo stage IIIB at diagnosis [10]. Given the high symptom burden and complex process of diagnosis, it is not surprising that patients with AL amyloidosis report worse health-related quality of life (HRQoL) than the general population [11].
The choice of primary clinical end points varies across trials of this patient population and includes best overall hematologic response, hematologic complete response (CR) and progression-free survival (PFS) [12–15]. In addition, definitions of PFS have not been uniformly applied across trials [16]. A further source of heterogeneity between studies is the evolving definition of hematologic CR. In 2012 two alternative definitions of hematologic CR were published [9,17]. Since the publication of these first guidelines, understanding of AL amyloidosis, including the roles and prognostic value of various biomarkers, has advanced, as reflected by additional proposed definitions of hematologic CR [18–20]. A clarification to the International Society of Amyloidosis guidelines has recently been published [21]; unlike the earlier guidelines and recommendations, the current guidelines do not require free light chain (FLC) ratio to achieve CR if uninvolved FLC is greater than involved FLC.
In addition to clinical end point definitions, the treatment landscape in AL amyloidosis has also evolved over time. Anti-plasma cell therapies approved for the treatment of multiple myeloma have been used off-label to treat patients with AL amyloidosis. Treatments for AL amyloidosis focus on the destruction of the underlying plasma cell clone, thereby suppressing amyloidogenic light-chain formation and preserving organ function [1,22]. Autologous stem cell transplant (ASCT) is effective in patients with AL amyloidosis; however, only about 20% of patients are eligible [23], and transplantation-related mortality is higher with amyloidosis than with multiple myeloma [24]. Historically, the combination of bortezomib, cyclophosphamide and dexamethasone (VCd) has been the standard of care in many countries [10,25,26].
With the recent approval of the combination of daratumumab (an anti-CD38 monoclonal antibody) plus VCd (D-VCd) in AL amyloidosis, there is now a need to understand the treatment landscape and disease aspects critical to making informed treatment decisions for patients. Given the evolving understanding of the disease, and the heterogeneity that exists in the definition of response between trials, patient stage and treatments evaluated, the objective of this systematic literature review (SLR) was not to pool or compare trials, but rather to describe the current breadth of evidence in adults with AL amyloidosis relating to clinical, HRQoL, economic and resource use data, which are important considerations in healthcare decision-making. The results of this study will, therefore, provide a comprehensive overview of the literature to inform patient management and treatment decision-making for clinicians, regulators and payers.
Materials & methods
Literature searches
Four literature searches (clinical evidence, HRQoL evidence, economic evidence and resource use/indirect costs evidence) were conducted by an information specialist using a peer-reviewed search strategy. The Embase and MEDLINE databases and Cochrane Controlled Register of Trials (CENTRAL) were searched using the Ovid platform. The search strategies included a combination of controlled vocabulary (e.g., ‘amyloidosis’) and keywords (e.g., ‘light chain, amyloid’). Language and publication year were not restricted at the search stage. For the HRQoL, economic and resource utilization searches, study selection was not limited by line of therapy, interventions or comparators (i.e., studies including newly diagnosed or relapsed/refractory AL amyloidosis patients were included). The reference lists from all published, on-topic SLRs identified during the screening process were reviewed as a supplementary search for relevant articles. Gray literature searches were also conducted to supplement the evidence searches.
The clinical evidence search of this SLR is registered with PROSPERO international prospective register of systematic reviews (protocol #CRD42020175412) and is available at: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020175412.
Clinical evidence
The clinical evidence literature search focused on randomized controlled trials (RCTs) and observational studies of pharmacotherapies used as first-line treatment for adults with newly diagnosed AL amyloidosis (Supplementary Table 1). Observational studies were included because a paucity of RCTs in this rare disease space was anticipated.
Studies published prior to the publication date of the consensus opinion for organ involvement and response by the 10th International Symposium in Amyloid and Amyloidosis [27] and studies of nonpharmacological treatments (e.g., ASCT) were excluded. Of note, the clinical evidence searches permitted studies of patients at any stage of the disease.
Health-related quality of life evidence
The HRQoL evidence literature search focused on assessments of quality of life or algorithms used to derive utility values for adult patients with AL amyloidosis (Supplementary Table 2). During title and abstract screening, studies reporting any type of HRQoL data were included.
Studies were excluded at the full-text screening phase if they did not report any of the following commonly used HRQoL assessment instruments: European Quality of Life Five Dimension (EQ-5D), European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30), Short Form 36-Item Health Survey (SF-36), Short Form Six-Dimension Health Survey (SF-6D) and the Health Utilities Index.
Economic evidence
The economic evidence literature search captured cost–effectiveness analyses (CEAs) with a specific focus on cost–utility analyses (CUAs; i.e., model outcomes reported as cost per quality-adjusted life year [QALY]) for adult patients with AL amyloidosis (Supplementary Table 3).
Resource use/indirect costs evidence
The resource use/indirect costs evidence literature search aimed to capture direct and indirect burden of illness costs for adult patients undergoing treatment for AL amyloidosis (Supplementary Table 4).
To reflect more relevant and current costs for treatment of AL amyloidosis, publications prior to 2010 (i.e., older than the last ∼10 years) were excluded.
Screening
Full search strategies for the four types of evidence are presented in Supplementary Tables 5–9. After the removal of duplicate citations, titles and abstracts were reviewed by two independent reviewers for study eligibility according to prespecified inclusion and exclusion criteria established using the population, intervention, comparators, outcomes and study design framework. Non-English-language publications were excluded during title and abstract screening, provided that the publication language was identified.
Study screening was performed using the systematic review software DistillerSR (Evidence Partners, Ottawa, Canada). Studies that met the inclusion criteria and those that did not provide enough information for exclusion were further reviewed at the full-text screening phase. Full-text articles were reviewed by two independent reviewers. During both screening phases, any discrepancies between the two reviewers were resolved by consensus or by a third reviewer.
Data extraction was performed for studies meeting all inclusion criteria using a standardized spreadsheet to capture all relevant information. Information was extracted by one reviewer and validated by a second reviewer; a third reviewer was consulted to resolve discrepancies as necessary.
Quality assessment
Quality assessments of studies from the clinical evidence, HRQoL evidence and economic evidence literature searches were performed independently by two reviewers and conducted using the appropriate questionnaires [28–32]; quality assessments for included studies from the resource use/indirect costs literature search were not conducted. The evaluations were compared in order to ensure consensus.
Given the limited information available in abstracts, quality assessments were only performed for studies with an associated full-text publication.
Results
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [33] flow diagrams for the study selection in the four literature searches are presented in Figure 1.
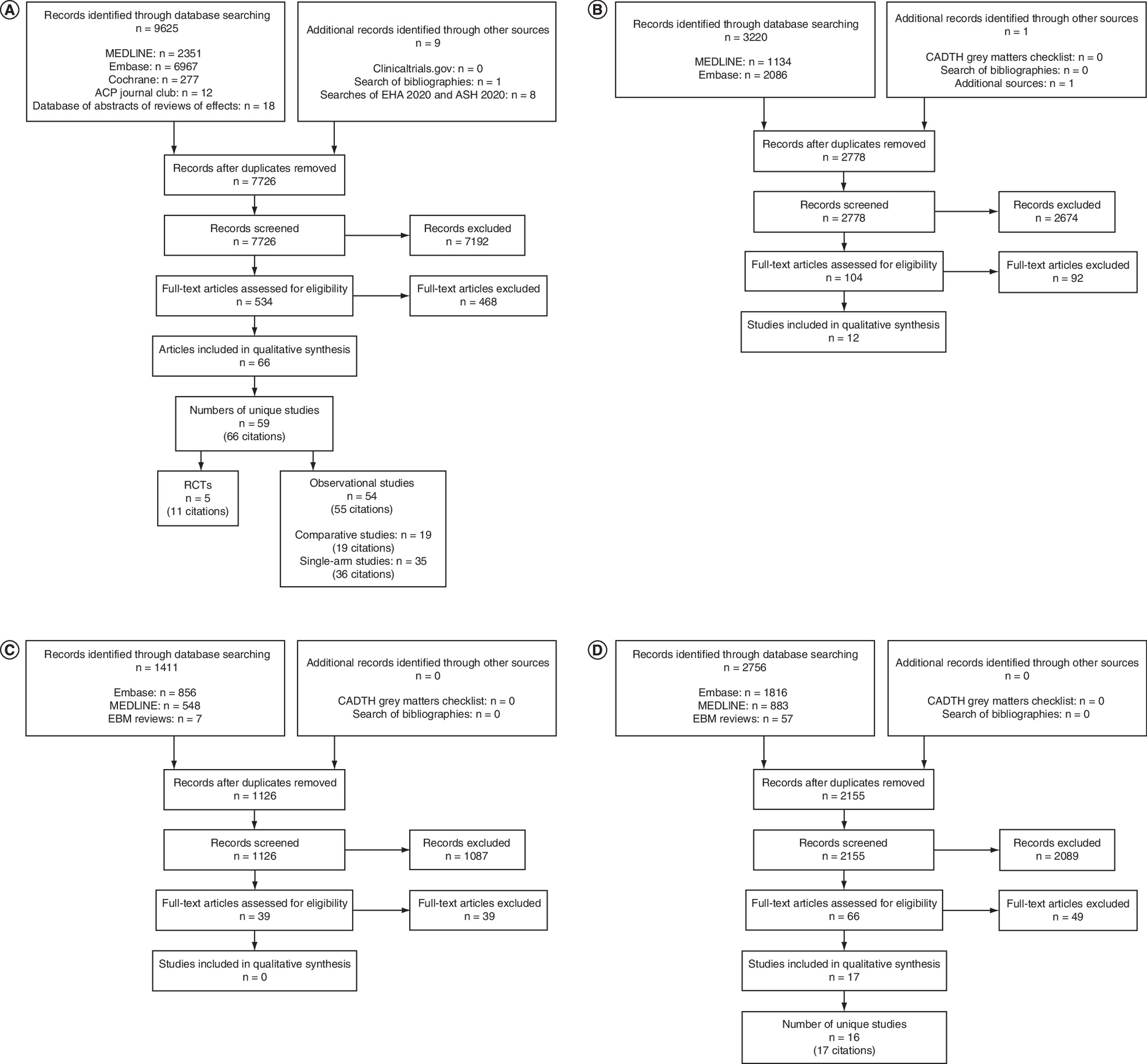
Figure 1. PRISMA flow diagram.
(A) Clinical evidence. (B) Health-related quality of life evidence. (C) Economic evidence. (D) Resource use/indirect costs evidence. ACP: American College of Physicians; ASH: American Society of Hematology; CADTH: Canadian Agency for Drugs and Technologies in Health; EBM: evidence-based medicine; EHA: European Hematology Association; RCTs: randomized controlled trials.
Clinical evidence
The clinical evidence literature search identified five unique RCTs (Table 1) and 54 unique observational studies (Table 2) evaluating the efficacy and safety of several first-line pharmacological treatments for adults with AL amyloidosis (Figure 1A).
| Author, publication date | NCT # | Phase | Setting | Intervention | Comparator(s) | Primary end point | Median follow-up at time of publication, months | Ref. |
|---|---|---|---|---|---|---|---|---|
| Huang, 2014 | NCT01998503 | 3 | Single-center (China); patient enrollment Jun 2009 to Jun 2012 | Vd + HDM/ASCT† (n = 28) | HDM/ASCT† (n = 28) | Hematologic CR | 28 | [12] |
| ClinicalTrials.gov, 2010 | NCT01078454 | 3 | Multicenter (USA); patient enrollment Nov 2010 to Sept 2012 | VMDex (n = 5) | MDex (n = 6) | Hematologic ORR | NA | [34] |
| Kastritis, 2020 Palladini, 2020 Wechalekar, 2020 Suzuki, 2020 Sanchorwala, 2020 Minnema, 2020 Comenzo, 2020 | NCT03201965 | 3 | Multicenter (international); patient enrollment 5 Oct 2017 to NR | D-VCd (n = 195) | VCd (n = 193) | Hematologic CR | 17.6 11.4 9.4 | [15,35–40] |
| Kastritis, 2020 | NCT01277016 | 3 | Multicenter (Europe and Australia); patient enrollment 28 Jan 2011 to 15 Feb 2016 | VMDex (n = 53) | MDex (n = 56) | CR and PR | 50 | [14] |
| Shen, 2019 | NCT03401372 | NR | Multicenter (China); patient enrollment 21 Apr 2018 to 30 Jun 2019 | VCd + doxycycline (n = 56) | VCd (n = 55) | PFS | 6.1 | [13] |
†
Huang et al. (2014) investigated bortezomib as an induction treatment prior to ASCT. Because the focus of this SLR was pharmacological therapies for the treatment of AL amyloidosis (and not ASCT), only the outcomes related to bortezomib induction are discussed.
AL: Amyloid light-chain; ASCT: Autologous stem cell transplant; CR: Complete response; D-VCd: Daratumumab (subcutaneous) + bortezomib + cyclophosphamide + dexamethasone; HDM: High-dose melphalan; MDex: Melphalan + dexamethasone; NA: Not available; NR: Not reported; ORR: Overall response rate; PFS: Progression-free survival; PR: Partial response; SLR: Systematic literature review; VCd: Bortezomib + cyclophosphamide + dexamethasone; Vd: Bortezomib + dexamethasone; VMDex: Bortezomib + melphalan + dexamethasone.
| Author, publication date | Study design | Setting | Number of arms in study | List of arms | Ref. |
|---|---|---|---|---|---|
| Kastritis, 2017 | Retrospective | Single-center (Greece); patients treated 2005–2010 (Vd) or Jan 2011–2013 (VCd) | 2 | Vd VCd | [85] |
| Sayago, 2016 | Retrospective | Single-center (Spain); patients treated Jul 2005–May 2015 | 2 | V-based treatment Non-V-based treatment | [86] |
| Shen, 2017 | Retrospective | Single-center (China); patients treated 1 Jan 2009–1 Jan 2017 | 1 | V-based treatment | [87] |
| Shah, 2013 | Retrospective | Single-center (USA); patients treated 1 Apr 2011–1 Apr 2013 | 2† | V-based treatment (AL amyloidosis patients) V-based treatment (MM patients)§ | [88] |
| Kastritis, 2010 | Retrospective | Single-center (Greece, UK and Italy); patient enrollment time period NR | 2† | Vd (untreated AL amyloidosis patients) V ± d (previously treated AL amyloidosis patients)§ | [89] |
| Minnema, 2019 | Prospective | Multicenter (Netherlands, Germany and Belgium); patients enrolled Mar 2012–Apr 2016 | 1 | Vd§ | [44] |
| Cornell, 2015 | Retrospective | Single-center (USA); patients treated 2006–2012 | 2 | VCd¶ Vd¶ | [45] |
| Mahmood, 2019 | Retrospective | UK-based; study center(s) and patient enrollment time period NR | 2 | V + Meth Vd | [90] |
| Chong, 2019 | Retrospective | Single-center (Australia-based); patients treated Sept 2014–May 2019 | 1 | VCd | [91] |
| Lee, 2014 | Retrospective | Single-center (Korea); patients treated 2011–2013 | 1 | VMPrdl | [92] |
| Manwani, 2019 | Retrospective | Multicenter (UK); patient enrollment time period NR | 1 | Car-based treatment | [93] |
| Kastritis, 2019 | NR | Single-center (Greece); patient enrollment time period NR | 1 | V-based treatment | [41] |
| Liu, 2019 | Retrospective | Single-center (China); patients treated Jun 2012–Jan 2018 | 2 | TCd MDex | [94] |
| Ozga, 2019 | Retrospective | Single-center (USA); patient enrollment time period NR | 1 | Various treatments | [95] |
| Gilles, 2019 | Retrospective | Single-center (France); patients diagnosed in 2008 or later | 4 | dCV (sequential) VCd (sequential) VCd (combination) Other chemotherapy | [96] |
| Jaccard, 2014 | Retrospective | Multicenter (USA, UK and France); patients treated Nov 2008–Apr 2012 | 1 | VCd | [97] |
| Sperry, 2016 | Retrospective | Single-center (USA); patients treated 2004–2015 | 2 | Vd + AA Other regimens | [98] |
| Palladini, 2015 | Retrospective | Multicenter (UK and Italy); patients treated Aug 2006–Mar 2013 | 1 | VCd | [99] |
| Wechalekar, 2013 | Retrospective | Multicenter (UK, Italy, Germany and Greece); patients treated Jan 2001–Dec 2010 | 1 | Various treatments | [100] |
| Tuzovic, 2017 | Retrospective | Single-center (USA); patients treated Oct 2007–Jun 2014 | 2† | Various treatments (AL amyloidosis patients) Healthy controls‡ | [101] |
| Bochtler, 2014 | Retrospective | Single-center (Germany); patients treated Jun 2005–Aug 2012 | 1 | MDex | [102] |
| Sanchorawala, 2015 | Prospective | Single-center (USA); patients enrolled Jan 2010–Aug 2013 | 1 | Vd + HDM/ASCT§ | [46] |
| Hegenbart, 2017 | Prospective | Single-center (Germany); patients enrolled Apr 2009–Feb 2012 | 1# | RMDex Historical comparison: MDex | [103] |
| Kastritis, 2015 | Prospective | Single-center (Greece); patients treated Sept 2005–Dec 2012 | 3 | R Vd (full dose) Vd (risk-adapted) | [104] |
| Venner, 2014 | Retrospective | Single-center (UK); patients treated Jul 2008–Jul 2012 | 2 | VCd TCd | [105] |
| Palladini, 2014 | Retrospective | Single-center (Italy); patients treated 2005–2012 | 2 | VMDex MDex | [106] |
| Sanchorawala, 2010 | Retrospective | Single-center (USA); patients treated 2004–2009 | 1 | MDex | [107] |
| Palladini, 2014 | Retrospective | Single-center (Italy); patients treated 2004–2009 | 2 | Full dose MDex Attenuated dose MDex | [108] |
| Fernandez, 2019 | Retrospective | Single-center (Spain); patients diagnosed Mar 2012–Mar 2018 | 1 | Various treatments | [109] |
| Fernandez, 2019 | Retrospective | Multicenter (regions NR); patients diagnosed Mar 2012–Mar 2018 | 1 | Various treatments | [110] |
| Gatt, 2016 | Retrospective | Multicenter (Israel); patients treated Jan 2009–2013 | 2 | Vd Vd + AA | [111] |
| Cibeira, 2015 | Prospective | Multicenter (Spain); patients enrolled Sept 2010–Dec 2012 | 1 | RCd | [112] |
| Lebovic, 2008 | NR | Single-center (USA); patients treated Dec 2003–Feb 2007 | 1 | MDex¶ | [42] |
| Kastritis, 2019 | Prospective | Single-center (Greece); patients treated Mar 2017–Mar 2018 | 1# | VRd Matched comparison: VCd | [113] |
| Manwani, 2019 | Prospective | Single-center (UK); patients treated Feb 2010–Aug 2017 | 1 | V-based treatment | [114] |
| Chari, 2013 | Retrospective | Single-center (USA); patient enrollment time period NR | 1 | Various treatments | [115] |
| Huang, 2015 | Retrospective | Single-center (China); patients treated Nov 2006–Mar 2012 | 1 | Vd | [116] |
| Tazawa, 2008 | Prospective | Single-center (Japan); patient enrollment time period NR | 1 | VAD | [117] |
| Bochtler, 2015 | Retrospective | Single-center (Germany); patients treated Aug 2008–Aug 2013 (Vd) and Feb 2012–Sept 2013 (VCd) | 2 | Vd VCd | [118] |
| Jain, 2018 | Retrospective | Single-center (USA); patients treated Jan 2004–Dec 2015 | 2 | V + ASCT§ Non-V + ASCT§ | [47] |
| Palladini, 2009 | Prospective | Single-center (Italy); patients enrolled Nov 2004–Apr 2006 | 1 | MTDex | [119] |
| Wei, 2019 | Prospective | Single-center (region NR); patients enrolled 29 Sept 2018–1 Apr 2019 | 1 | Ixd | [120] |
| Huang, 2016 | Retrospective | Single-center (China); patients treated 2009–Jun 2014 | 1 | Vd | [121] |
| Basset, 2020 Basset, 2019 | NR | Single-center (Italy); patients enrolled 2009–2018 | 1 | VCd§ | [43,48] |
| Cappuccio, 2020 | Retrospective | Single-center (Italy); patients treated 2011–2019 | 2 | VCd¶ V-based treatment | [49] |
| Diaz-Paralles, 2020 | Retrospective | Single-center (Canada); patients treated Jan 2012–Aug 2018 | 1 | VCd | [122] |
| Dumas, 2020 | Retrospective | Single-center (USA); patients treated 2013–2017 | 2 | V-based treatment: presence of t(11;14) V-based treatment: absence of t(11;14) | [123] |
| Huang, 2021 | Retrospective | Single-center (China); patients undergoing ASCT 1 Jul 2010–30 Dec 2018 | 3 | V-based treatment§ Various treatments§ No treatment‡ | [50] |
| Kastritis, 2020 | Retrospective | Single-center (Greece); patient enrollment time period NR | 1 | V-based treatment | [124] |
| Nagano, 2020 | Retrospective | Single-center (Japan); patients treated Apr 2011–May 2017 | 1 | V-based treatment | [125] |
| Shen, 2020 | Retrospective | Single-center (China); patients treated 1 Jan 2009–1 Nov 2019 | 1 | V-based treatment | [126] |
| Vaxman, 2021 | Retrospective | Single-center (USA); patients treated Jan 2007–Aug 2017 | 1 | Various treatments + ASCT§ | [51] |
| Muchtar, 2020 | Prospective | USA-based; study center(s) and patient enrollment time period NR | 1 | CIxd | [127] |
| Palladini, 2020 | Prospective | Italy-based; study center(s) NR; patients treated May 2011–Oct 2019 | 1 | V-based treatment | [128] |
†
Study was presented as a two-arm study, but only contained one relevant arm per the study selection criteria; thus this study was considered as a single-arm study for the purpose of this review.
‡
Data from this specific arm were not extracted because they did not meet the study selection criteria.
§
Chemotherapy was investigated as induction treatment prior to ASCT; thus only outcomes related to induction were extracted.
¶
Chemotherapy was investigated as induction therapy for ASCT-ineligible patients. After completion of induction therapy, the feasibility of ASCT was reassessed.
#
Described as a single-arm study but included a matched or historical comparison versus another treatment. Because both arms met the study selection criteria, this study was considered a comparative study in the context of this review.
AA: Alkylating agent; AL: Amyloid light-chain; ASCT: Autologous stem cell transplant; Car: Carfilzomib; CIxd: Cyclophosphamide + ixazomib + dexamethasone; d: Dexamethasone; dCV: Dexamethasone + cyclophosphamide + bortezomib (administered in sequential order); HDM: High-dose melphalan; Ixd: Ixazomib + dexamethasone; MDex: Melphalan + dexamethasone; Meth: Methylprednisolone; MM: Multiple myeloma; MTDex: Melphalan + thalidomide + dexamethasone; NR: Not reported; R: Lenalidomide; RCd: Lenalidomide + cyclophosphamide + dexamethasone; RMDex: Lenalidomide + melphalan + dexamethasone; TCd: Thalidomide + cyclophosphamide + dexamethasone; V: Bortezomib; VAD: Vincristine + doxorubicin + dexamethasone; VCd: Bortezomib + cyclophosphamide + dexamethasone; Vd: Bortezomib + dexamethasone; VMDex: Bortezomib + melphalan + dexamethasone; VMPrdl: Bortezomib + melphalan + prednisolone; VRd: Bortezomib + lenalidomide + dexamethasone.
Four of the five included RCTs were phase III trials [12,14,15,34–40]; none of the included RCTs were placebo-controlled trials. One RCT (NCT01998503) investigated the addition of bortezomib and dexamethasone (Vd) induction treatment prior to high-dose melphalan and ASCT [12], whereas the remaining four RCTs compared chemotherapy regimens (VCd vs VCd with doxycycline [13]; melphalan and dexamethasone [MDex] vs bortezomib, melphalan and dexamethasone [VMDex] [14,34]; VCd vs D-VCd [15,35–40]). Across the studies, where reported, the first patient was enrolled between 2009 and 2018, and the last patient between 2012 and 2019. Median follow-up at the time of publication ranged from 6.1 to 50 months (Table 1). Four studies were multicenter (two were international) and one was a single-center study.
Quality assessment could be completed for only two trials, as they had associated full-text publications [12,14]. Details of random sequence generation ranged from unclear to having a low risk of bias, based on the available detail provided. Both trials had a high risk of bias related to allocation concealment and blinding of patients and care providers, either due to an open-label trial design [14] or as a result of patients in one treatment arm receiving additional concomitant medications compared with the other treatment arm [12]. Of note, blinding of outcome assessors among these trials was deemed unclear or had a low risk of bias. Selective reporting and incomplete outcomes were deemed to have a low risk of bias for both trials. Overall, the quality of reporting varied between low, inconclusive and high, depending on the factors that were assessed. A summary of the assessment of risk of bias of the two RCTs is presented in Supplementary Table 10.
Among the included observational studies, there were 12 prospective studies, 39 retrospective studies and three studies that did not explicitly report the study design [41–43]. 20 studies were described as comparative, whereas 34 studies were described as single arm. However, three comparative studies each contained only one arm that was relevant per the study selection criteria; thus these were treated as single-arm studies in this SLR. Bortezomib-based therapy (e.g., Vd and VCd) and MDex were the most commonly investigated chemotherapies. Nine studies investigated chemotherapy regimens as an induction treatment prior to ASCT [42–51]; three of these had patient populations that were initially ASCT ineligible and investigated the feasibility of ASCT after pharmacological treatment [42,45,49]. The majority of observational studies reported the number of patients who received subsequent therapies; most of these therapies were chemotherapy regimens, although patients undergoing subsequent ASCT and heart transplant were also reported.
Across the observational studies, were reported, patient enrollment began between 2001 and 2018 and ended between 2006 and 2019 (Table 2); 43 studies were single-center and eight multicenter (four were international), while the remaining three did not include this information.
Quality assessment was completed for each comparative observational study with an associated full-text publication (16 of the 19 comparative observational studies). In total, one study was assessed using the criteria for case–control studies and 15 were assessed using the criteria for cohort studies. Overall, 15 of the 16 assessed comparative observational studies were deemed to be of high quality. The design of the remaining study precluded it from proper quality assessment [47]. Because the study involved induction treatment prior to ASCT, only the data pre-ASCT underwent quality assessment. Follow-up data were excluded from the quality assessment, thereby resulting in a lower quality score. All assessed studies reported high-quality patient selection, and the design of most of the studies allowed for suitable treatment comparison. Some variation was noted in the quality of outcome reporting due to differences in the length of follow-up and the number of patients lost to follow-up. Summaries of the risk of bias assessments for qualifying comparative observational studies are presented in Supplementary Tables 11 (case-control studies) & 12 (cohort studies).
The key clinical outcomes that were identified included hematologic response, organ response, time to hematologic response, overall survival, PFS and safety, which comprised dose reductions due to adverse events (AEs), withdrawal due to AEs, and incidence of the following AEs: infection, neuropathy, cytopenia, organ failure, syncope, hypokalemia, peripheral edema and diarrhea (Figure 2).
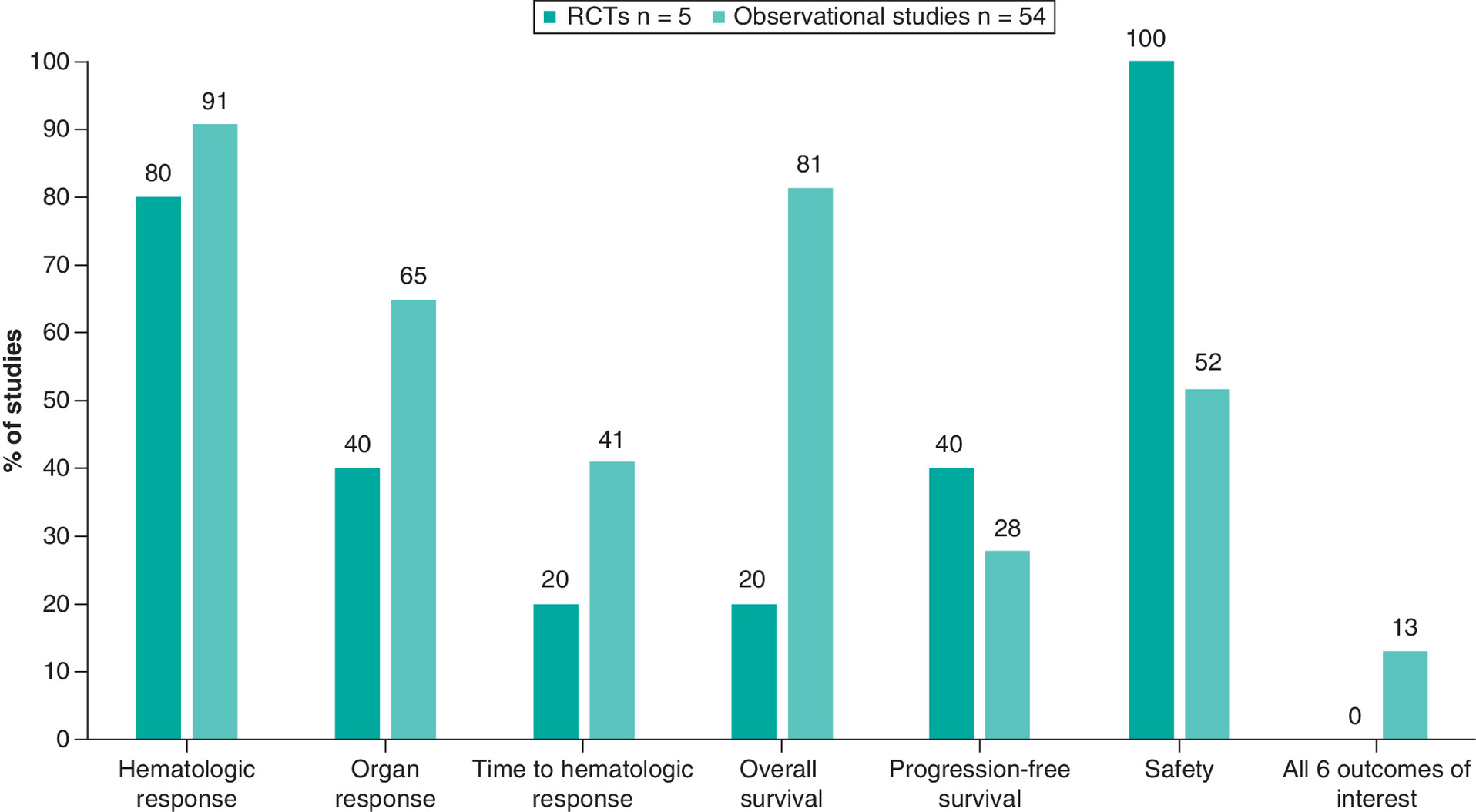
Figure 2. Proportion of randomized controlled trials and observational studies reporting clinical outcomes of interest.
For studies reporting induction treatment prior to autologous stem cell transplant, studies were counted only if they reported outcomes specific to the induction treatment.
HRQoL evidence
The HRQoL evidence literature search identified 12 relevant studies for which data extraction was performed (Figure 1B); all were published between 2004 and 2020 and were mostly from the USA and Italy (Table 3). The studies reporting HRQoL consisted of three RCTs [14,38,52], two of which had also been captured through the clinical evidence search [14,38], and nine observational studies. Five studies reported on newly diagnosed or treatment-naive patient populations [14,38,52–54]. Only five studies reported HRQoL outcomes as a result of an intervention, including high-dose melphalan with stem cell transplant [55,56], nutritional counseling [52] and bortezomib-based chemotherapy (VCd vs D-VCd [38] and VMDex vs MDex [14]).
| Author, publication date | Study design | Country | Population | Intervention | Utility instrument | External source of data† | Ref. |
|---|---|---|---|---|---|---|---|
| Bayliss, 2017 | Cross-sectional analysis | USA | AL amyloidosis | NR | SF-36v2 | AL amyloidosis patient health-related quality of life study (NCT02574676) | [11] |
| Sattianayagam, 2013 | Prospective study | UK | Newly diagnosed, treatment-naive AL amyloidosis | NR | EORTC QLQ-C30 | NA | [54] |
| Shu, 2016 | Prospective, observational study | USA | AL amyloidosis | NR | SF-36v1 | NCT00898235 | [129] |
| Caccialanza, 2015 | Two-arm (parallel assignment), open-label RCT | Italy | Treatment-naive AL amyloidosis | Nutritional counseling Usual care | SF-36v1‡ | NCT02055534 | [52] |
| Caccialanza, 2012 | Cross-sectional study | Italy | Newly diagnosed AL amyloidosis | NR | SF-36v1‡ | NA | [53] |
| McCausland, 2019 | Secondary data analysis from a non-interventional, longitudinal, online study | Various§ | AL amyloidosis | NR | SF-36v2 | AL amyloidosis patient health-related quality of life study (NCT02574676) | [61] |
| Rizio, 2018 | Data analysis from a non-interventional, longitudinal, online study | Various¶ | AL amyloidosis | NR | SF-36v2 | AL amyloidosis patient health-related quality of life study (NCT02574676) | [130] |
| Sanchorawala, 2017 | Retrospective data analysis | USA | AL amyloidosis | HDM/SCT Non-SCT chemotherapy | SF-36v1 | NA | [55] |
| Seldin, 2004 | Retrospective analysis | USA | AL amyloidosis | HDM/SCT | SF-36v1‡ | NA | [56] |
| White, 2017 | Non-interventional, longitudinal, observational study | USA | AL amyloidosis | NR | Study 1: SF-36v2 Study 2: SF-36v1 | Study 1: Data from AL amyloidosis patient health-related quality of life study (NCT02574676) Study 2: Data from clinic-based sample | [131] |
| Sanchorawala, 2020 | RCT | Various | Newly diagnosed AL amyloidosis | VCd D-VCd | EORTC QLQ-C30 EQ-5D-5L VAS SF-36v2 | NA | [38] |
| Kastritis, 2020 | RCT | Italy | Previously untreated AL amyloidosis | VMDex MDex | EORTC QLQ-C30 SF-36v2 | NA | [14] |
†
Indicates whether the analyses were conducted with data collected directly from patients enrolled in the study or performed using an existing dataset from another study.
‡
Version number was not explicitly stated in publication and was inferred from bibliography.
§
Known countries of residence included USA, UK, Canada and Australia.
¶
Known regions of residence included North America and Europe.
AL: Amyloid light-chain; D-VCd: Daratumumab (subcutaneous) + bortezomib + cyclophosphamide + dexamethasone; EORTC QLQ-C30: European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire; HDM: High-dose melphalan; MDex: Melphalan + dexamethasone; NA: Not applicable; NR: Not reported; RCT: Randomized controlled trial; SCT: Stem cell transplant; SF-36: Short Form 36-Item Health Survey; VAS: Visual analog scale; VCd: Bortezomib + cyclophosphamide + dexamethasone; VMDex: Bortezomib + melphalan + dexamethasone. EQ-5D-5L VAS: EuroQol-5D-5L visual analog scale
Relevant HRQoL outcomes included direct utility measures and HRQoL survey scores with potential to be mapped to utility values (Figure 3). None of the included studies reported utility values or mapping algorithms. However, all studies reported HRQoL survey scores with potential for mapping to utility values. The vast majority of these studies reported scores obtained from the SF-36, and three studies reported scores from the EORTC QLQ-C30 [14,38,54]. One study reported scores from the EQ-5D-5L visual analog scale [38]. No studies reported Health Utilities Index outcomes. Most studies reported HRQoL survey scores at a single time point. In addition to the outcomes of interest, one study reported the use of a non-cancer-specific global assessment of functioning (on a scale of 0 to 100, where a higher score indicated better functioning) and the Patient Global Impression of Severity scale [11].

Figure 3. Number of studies reporting utility values and health-related quality of life scores (all identified publications).
Note: Studies that used more than one utility instrument were counted more than once. Six studies reported outcomes based on SF-36v1, six studies reported outcomes based on SF-36v2; one study reported outcomes from both versions of the questionnaire. Sanchorawala [27] reported difference in HRQoL survey score for D-VCd and VCd at multiple time points.
D-VCd: daratumumab (subcutaneous) + bortezomib + cyclophosphamide + dexamethasone; EORTC QLQ-C30: European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire; EQ-5D: European Quality of Life – five dimension; HRQoL: Health-related quality of life; SF-36: Short Form 36-Item Health Survey; SF-6D: Short Form 6-Dimension Health Survey; VCd: bortezomib + cyclophosphamide + dexamethasone.
Quality assessments demonstrated that patient populations were representative of the general AL amyloidosis patient population. Although the number of patients lost to follow-up varied, most studies had high response rates (100% in seven of the included studies and 77.6–95% in four studies) to the particular HRQoL instrument described in the study. All studies reported: a patient population likely to match the population of interest; the use of a preference-based instrument; and change in HRQoL measures reported directly by the patient. Seven of the 12 studies included satisfied the criterion of valuation of changes in patients’ HRQoL measures being assessed against that of the general population. As all studies reported values for the subscales of the HRQoL instrument, they could not be assessed for the technique used to value health states. A summary of the risk of bias assessments for the HRQoL studies is presented in Supplementary Table 13.
Economic evidence
Overall, 39 studies reporting economic evidence were identified for full-text review. No CEAs, CUAs or CUA assessments relevant to AL amyloidosis were identified (Figure 1C). One conference abstract discussed a targeted literature search for drug prices and incremental QALYs of newly approved orphan drugs from health technology assessment publications [57]. Although AL amyloidosis was among the rare diseases identified in the search, the abstract was ultimately excluded due to a lack of sufficient information. In total, 21 studies eligible for full-text review were excluded due to their patient populations. Of these 21 studies, 14 did not discuss AL amyloidosis or failed to report economic outcomes specific to AL amyloidosis, while the remaining seven studies described other forms of amyloidosis such as hereditary and transthyretin amyloidosis. One study discussed economic outcomes among patients with AL and transthyretin amyloidosis but was excluded as disaggregated outcomes were not reported specifically for AL amyloidosis [58]. Similarly, a briefing on a study evaluating ixazomib for the treatment of relapsed and/or refractory AL amyloidosis was excluded as it did not report any outcomes [59]. Two studies were excluded based on the reported outcome, as they did not report costs [60,61]. 15 studies were excluded due to study design (i.e., they were not CEAs or CUAs) [62–76]. Of these, 14 were either cost-of-illness studies or resource utilization studies and reported costs and resource utilization related to AL amyloidosis [62–66,68–76]; the remaining citation was a letter [67]. Of the 14 studies, four focused on patients with AL amyloidosis and reported outcomes such as the number of hospitalizations and length of stay, as well as costs related to treatment, inpatient care and outpatient care [63,68–70].
After full-text review, none of the publications identified by this search fulfilled the criteria for formal inclusion in the final review and thus, data extraction and quality assessment were not performed.
Resource use/indirect costs evidence
The resource use/indirect costs evidence literature search identified 16 unique studies (one relevant SLR and 15 observational studies) published between 2017 and 2020 (Figure 1D & Table 4). Ten studies reported outcomes among patients with AL amyloidosis, including the SLR conducted by Lin et al. [77]. Six studies reported outcomes among a cardiac amyloidosis population [71–73,75,76,78–81]. Of note, these studies were included as it was implied within the publications that their patient populations could include individuals with AL amyloidosis. Most studies were of USA origin and reported costs in US dollars.
| Author, publication date | Study design | Population | Sample size | Country/region | Currency (cost year) | Ref. |
|---|---|---|---|---|---|---|
| McCausland, 2019 | Secondary data analysis from a non-interventional, longitudinal, online study | AL amyloidosis | 224 | USA, UK, Canada, Australia† | NR | [61] |
| Hester, 2019 | Claims database analysis | AL amyloidosis | 1313 | USA | NR | [132] |
| Lin, 2017 | SLR | AL amyloidosis | NR | Various‡ | US dollars, UK pounds (various) | [77] |
| Gilstrap, 2019 | Claims database analysis | Cardiac amyloidosis | Incident cases: 38,254 Prevalent cases: 121,122 | USA | NR | [78] |
| Quock, 2018 | Claims data analysis | AL amyloidosis | Prevalent patients: 7326 Incident patients: 2018 | USA | US dollars (2015) | [70] |
| Quock, 2018 | Retrospective, matched case–control study | Newly diagnosed AL amyloidosis Disease-free controls§ | Newly diagnosed AL amyloidosis: 249 Disease-free controls: 747 | USA | US dollars (2016) | [69] |
| Kastritis, 2019 | NR | AL amyloidosis | VRd: 34 VCd: 68 | Greece | NR | [133] |
| Attwood, 2019 | Audit | Cardiac AL amyloidosis | 8 | UK | NR | [81] |
| Guinault, 2016 | Retrospective | AL amyloidosis Secondary amyloidosis§ | AL amyloidosis: 52 Secondary amyloidosis: 14 | France | NR | [134] |
| Hari, 2018 | Retrospective | AL amyloidosis¶ | First-line treatment: 334 Second-line treatment: 144 | USA | US dollars (2015) | [68] |
| Quock 2019 | Retrospective cohort study | Cardiac amyloidosis | 3239 | USA | US dollars (2016) | [71] |
| Dastmalchi, 2020 | Claims database analysis | Heart failure with cardiac amyloidosis Heart failure without cardiac amyloidosis§ | Overall: 9,682,870 With cardiac amyloidosis: 13,600 | USA | US dollars (NR) | [72] |
| Isath, 2020 Isath, 2020 | Claims database analysis | Cardiac amyloidosis with arrhythmias Cardiac amyloidosis without arrhythmias Cardiac amyloidosis with ICD implantation Cardiac amyloidosis without ICD implantation | Overall: 145,920 With arrhythmias: 56,199 Without arrhythmias: 89,721 With ICD implantation: 1381 Without ICD implantation: 144,539 | USA | US dollars (NR) | [73,75] |
| Sepehrvand, 2020 | Retrospective analysis | Cardiac amyloidosis Without cardiac amyloidosis§ | Overall: 214,438 With cardiac amyloidosis: 982 | Canada | NR | [79] |
| Thakkar, 2020 | Claims database analysis | Cardiac amyloidosis with arrhythmias Cardiac amyloidosis without arrhythmias | Overall: 5585 With arrhythmias: 2020 Without arrhythmias: 3565 | USA | US dollars (NR) | [76] |
| Vaishnav, 2020 | Retrospective analysis | Cardiac AL amyloidosis Cardiac ATTR amyloidosis§ | Overall: 44 With cardiac AL amyloidosis: 17 | USA | US dollars (NR) | [80] |
†
Patients were stated to be from additional countries/regions that were not further specified.
‡
Countries discussed included USA, UK and China.
§
Data from this specific arm were not extracted because they did not meet the study selection criteria.
¶
Patients receiving first- or second-line treatment were studied, but resource use outcomes pertain to those receiving second-line treatment.
AL: Amyloid light-chain; ATTR: Transthyretin; ICD: Implantable cardioverter-defibrillator; NR: Not reported; SLR: Systematic literature review; VCd: Bortezomib + cyclophosphamide + dexamethasone; VRd: Bortezomib + lenalidomide + dexamethasone.
Relevant outcomes for the resource use evidence literature search included usage and cost of various healthcare resources, including but not limited to hospitalization, admission to the intensive care unit (ICU) or emergency department, inpatient care, outpatient care, readmission and treatment (Figure 4). Outcomes related to hospitalization and ICU stay were most commonly reported among the included studies and were reported as the number of stays and length of stay. Outcomes related to emergency department use, outpatient care and readmission were less commonly reported across the included studies.
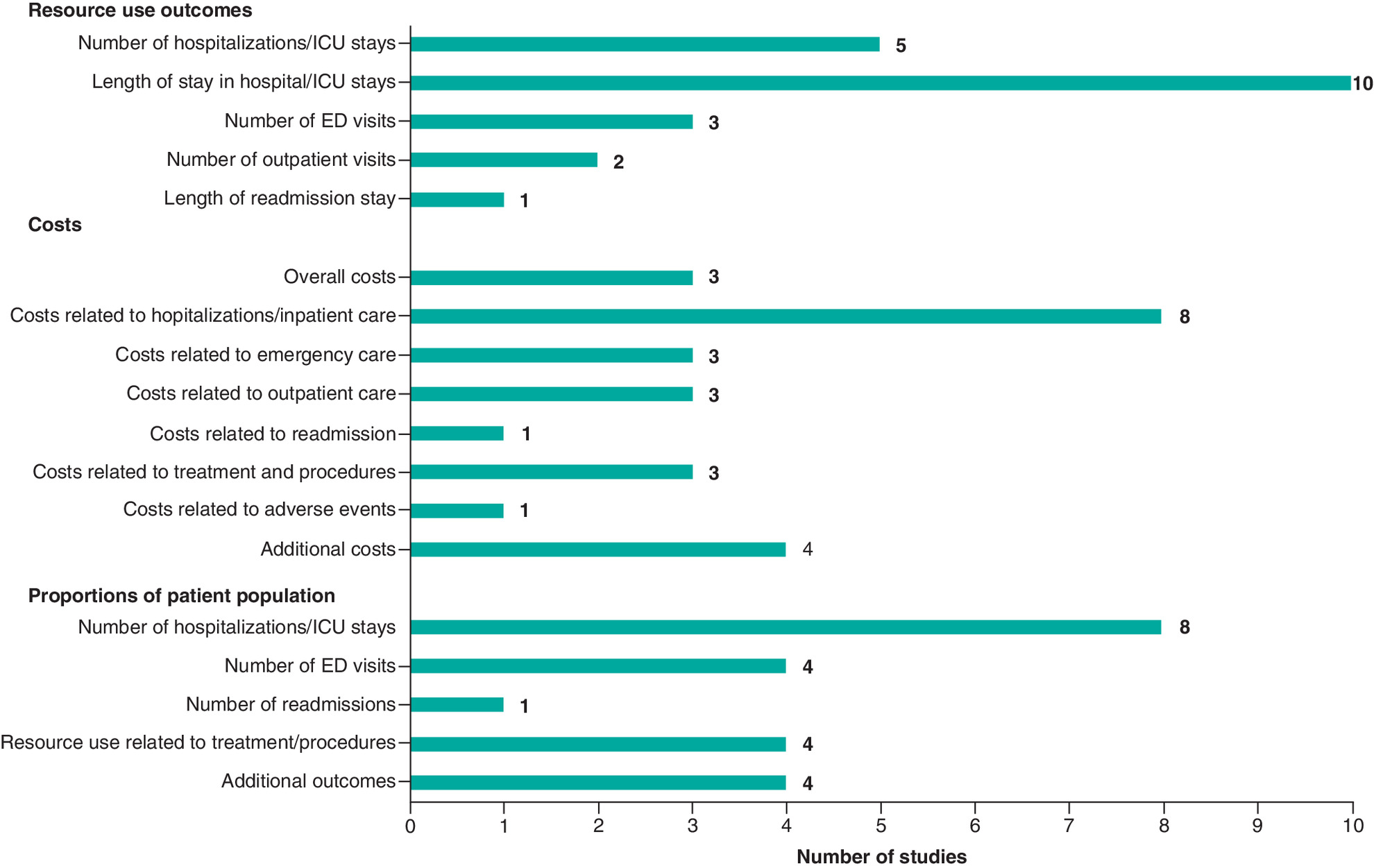
Figure 4. Number of studies reporting resource use and cost outcomes (all identified publications).
Studies that reported more than one outcome were counted more than once.
ED: Emergency department; ICU: Intensive care unit.
Descriptions of costs reported across the studies varied. Costs related to hospitalization and inpatient care were reported in eight studies [68–73,75–77], and three studies reported costs related to both emergency and outpatient care [68–70]. Three studies reported various costs related to the treatment of amyloidosis, including chemotherapy, ASCT, organ transplant and various other procedures [68,71,77]. One study reported costs related to hospital readmission [71]. The 2017 study by Lin et al., an SLR of evidence related to AL amyloidosis, reported the costs associated with treating anemia, neutropenia and thrombocytopenia, all of which are common AEs resulting from chemotherapy treatment for AL amyloidosis [77]. These AE costs were reported for the general cancer population, but they were deemed applicable to the AL amyloidosis patient population as well [77]. No articles reporting indirect costs were identified in this search.
Discussion
AL amyloidosis affects up to 12 persons per million per year [82]. Patients with this disease have poor survival rates, although life expectancy has improved with the adoption of new treatment modalities. Given the rarity of the disease, it is of interest to researchers and decision-makers to understand the status of the available literature and any information gaps. In this regard, this study was designed to evaluate the extent of the current clinical, HRQoL, economic and resource use evidence base for adults with AL amyloidosis.
The clinical evidence literature search identified five relevant RCTs and 54 observational studies (19 comparative studies and 35 single-arm studies; 12 prospective studies, 39 retrospective studies and three studies with undetermined study design) evaluating the efficacy and safety of various pharmacotherapies in adults newly diagnosed with AL amyloidosis. Overall, bortezomib-based therapies and therapies involving MDex were the most commonly investigated treatments across the included studies. Most RCTs and observational studies reported hematologic response, whereas organ response and time to hematologic response were less commonly reported. Relevant survival outcomes were reported in two RCTs; overall survival and/or PFS were often available in the observational studies. All RCTs reported key safety outcomes, whereas just over half of the observational studies reported these outcomes. Four of the five RCTs and eight of the 54 observational studies were multicenter, and there were also differences noted between studies in the start of enrollment across both the RCTs and observational trials (9- and 17-year time spans, respectively from earliest to latest). The literature search of HRQoL evidence identified 12 relevant studies. Although no studies reported utility values or mapping algorithms related to AL amyloidosis, all included studies did report scores from HRQoL questionnaires with potential to be mapped to utility values. The SF-36 was the most frequently used HRQoL questionnaire across the studies.
Screening of 1126 articles for AL amyloidosis economic evidence failed to identify any relevant published CUAs or CEAs, thereby highlighting an important data gap for economic modeling studies in this rare disease area. Of note, several relevant healthcare resource utilization studies that were identified and excluded from the economic evidence search were ultimately captured in the resource use/indirect costs evidence literature search [62,68–73,75,76].
The literature search of resource use/indirect costs evidence identified 16 unique studies that reported a variety of resource use outcomes and costs, mostly in the USA setting; no indirect costs were reported. The most commonly reported resource use outcomes and costs were related to hospitalizations and ICU stays.
The results of this SLR demonstrate that there is a paucity of clinical evidence related to non-ASCT therapies in patients with newly diagnosed AL amyloidosis; in particular, published data from RCTs in this rare disease are lacking. The need for more RCTs is critical because many patients with AL amyloidosis are ineligible for ASCT and therefore have limited proven treatment options [22,83]. Only five RCTs were identified, two of which had full-text publications available at the time of the search. One of these investigated VMDex chemotherapy as a first-line regimen (not as induction) [14], and the other investigated bortezomib-based induction prior to ASCT [12]. The ongoing phase III ANDROMEDA trial investigated the efficacy of D-VCd versus VCd in patients with newly diagnosed AL amyloidosis. The clinical evidence search returned a full-text publication reporting the results of the safety run-in cohort [35], as well as several abstracts based on the randomized portion of the study [15,36–40]. The primary analysis was published in July 2021, after the SLR had been completed [84].
Several studies reported relevant HRQoL questionnaire scores with potential to be mapped to utility values, but there remains a need for studies directly reporting utility values to better quantify the HRQoL disease burden and inform CUAs. In addition, there were no published CUAs identified within the economic evidence literature search, suggesting that a data gap exists for economic models and evaluations reporting the cost and QALY benefits of first-line treatments in patients with AL amyloidosis.
Although a few studies reporting costs related to AL amyloidosis were identified, there remains a need for additional studies to better understand patterns in cost-of-illness and resource utilization related to this rare disease. Most of these studies were from the USA and Italy, with limited information on burden and costs in other countries and regions. Moreover, the absence of data pertaining to indirect costs should be noted. Future studies reporting indirect costs may allow a more complete assessment of the burden on patients with AL amyloidosis and their caregivers, as well as clinicians and health systems.
A strength of this SLR is that it adheres to best practices for the conduct and reporting of systematic reviews. All literature searches were performed and peer-reviewed by experienced information specialists, with detailed search strategies, PRISMA flow diagrams and full study inclusion/exclusion lists, per PRISMA guidelines [33].
A limitation of this SLR is that included studies were restricted to English-language publications during the study screening phase. This is likely a minor limitation, as most clinical studies are published in English-language journals. Notably, the search strategies were not restricted solely to articles in English; therefore the search strategies conducted for these literature searches may be used to capture potentially relevant non-English-language articles without the restriction at title and abstract screening. Across all four literature searches, 776 articles were excluded due to language during both phases of screening; the relevance of these articles to AL amyloidosis is unknown. In addition, although the search strategy for the clinical evidence literature search aimed to capture relevant chemotherapy comparators by searching for specific drug names, it is possible that some studies could be missed if they were indexed in the databases as general chemotherapies rather than by individual drug names.
Another potential limitation is the indexing of conference or manuscript publications relative to the time of the database search. For example, although the database searches aimed to capture records published before February 2021, it is possible that the indexing of some conference proceedings taking place in the last year had not occurred by then; as a result, potentially relevant records from these conferences may not be captured in the database search. To address the impact of this limitation, particularly to the clinical evidence literature search, relevant records were hand-searched from two key conferences and were presented as additional records to those included from database searching.
The heterogeneity seen in the results reflects the evolving nature of the study and treatment of this disease, such as the variable definition of hematologic response in AL amyloidosis across the time span of the included studies. Of note, the clinical SLR was limited to literature published after 2005, at which time there was an international consensus made on organ response definition [27] and as such this would not be expected to provide a major source of variability in the results. A further source of heterogeneity in the results may be the study setting, with a mix of multicenter and single-center studies; not limiting the searches to any specific disease stage may also contribute to variability across the results.
The objective of this study was focused on identification of the current available evidence; however, assessment of that evidence, including evaluation of survival based on different definitions of response, is an important topic for future research.
Conclusion
Overall, this SLR identified and compiled evidence from 84 unique studies reporting on clinical, HRQoL, economic and resource use/indirect costs evidence relevant to AL amyloidosis. Although a relative lack of available data was expected given the rarity of AL amyloidosis, the results of these literature searches confirm the paucity of evidence for this disease state. This SLR highlights the need for additional published RCTs (for front-line pharmacological treatments), utility values, economic evaluations and indirect costs pertaining to the treatment of patients with AL amyloidosis. In addition, there is a need for studies with clinical and HRQoL outcomes that better align to current consensus criteria. These could potentially create opportunities for future comparative analyses that could further benefit decision-makers. Recently published and forthcoming results from studies such as ANDROMEDA will change the landscape for the treatment of patients with AL amyloidosis and will fill in gaps identified by this SLR regarding costs, utilization and clinical outcomes.
•
Amyloid light-chain (AL) amyloidosis, a clonal plasma cell disorder, is the most common and severe form of amyloidosis, which is a rare disease characterized by the extracellular accumulation of insoluble amyloid fibril deposits on various organs and tissues.
•
The availability of new and approved therapies is changing the treatment landscape in AL amyloidosis and is increasing awareness about this disease, allowing for earlier diagnosis and treatment.
•
The objective of this systematic literature review was to evaluate the breadth of clinical, health-related quality of life, economic and resource use/indirect costs evidence for adults (aged ≥18 years) with AL amyloidosis.
•
The results of this systematic literature review revealed a paucity of published literature for AL amyloidosis, particularly with respect to randomized controlled trials (for front-line pharmacological treatments), utility values, economic evaluations and indirect costs.
Author contributions
C Lee and A Lam designed the analysis. T Kangappaden, P Olver, S Kane and D Tran performed the systematic literature reviews and the analyses. All authors participated in data interpretation, contributed to drafting of the manuscript and provided final approval for submission.
Financial & competing interests disclosure
These analyses were funded by Janssen Global Services LLC. The database search strategies were developed and performed by M Fiander of Fiander Consulting and J Bielecki of EVERSANA and funded by Janssen Global Services, LLC. T Kangappaden, P Olver, S Kane and D Tran are employees of EVERSANA, which was contracted by Janssen to conduct this research. C Lee, A Lam and E Ammann are employees of Janssen Global Services LLC. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support was provided by K Pemberton of Eloquent Scientific Solutions and was funded by Janssen Global Services, LLC.
Supplementary Material
File (al_amyloidosis_slr_supplementary_materials.docx)
- Download
- 163.66 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Sanchorawala V. Light-chain (AL) amyloidosis: diagnosis and treatment. Clin. J. Am. Soc. Nephrol. 1(6), 1331–1341 (2006).
2.
Badar T, D'souza A, Hari P. Recent advances in understanding and treating immunoglobulin light chain amyloidosis. F1000Res. 7, 1348 (.2018).
3.
Vaxman I, Gertz M. Recent advances in the diagnosis, risk stratification, and management of systemic light-chain amyloidosis. Acta Haematol. 141(2), 93–106 (2019).
4.
Cai Y, Xu S, Li N, Li S, Xu G. Efficacy of chemotherapies and stem cell transplantation for systemic AL amyloidosis: a network meta-analysis. Front. Pharmacol. 10, 1601 (2019).
5.
Muchtar E, Dispenzieri A, Magen H et al. Systemic amyloidosis from A (AA) to T (ATTR): a review. J. Intern. Med. 289(3), 268–292 (2021).
6.
McCausland KL, White MK, Guthrie SD et al. Light chain (AL) amyloidosis: the journey to diagnosis. Patient 11(2), 207–216 (2018).
7.
Muchtar E, Gertz MA, Kumar SK et al. Improved outcomes for newly diagnosed AL amyloidosis between 2000 and 2014: cracking the glass ceiling of early death. Blood 129(15), 2111–2119 (2017).
8.
Weiss BM, Hebreo J, Cordaro DV et al. Increased serum free light chains precede the presentation of immunoglobulin light chain amyloidosis. J. Clin. Oncol. 32(25), 2699–2704 (2014).
9.
Palladini G, Dispenzieri A, Gertz MA et al. New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: impact on survival outcomes. J. Clin. Oncol. 30(36), 4541–4549 (2012).
10.
Palladini G, Schönland S, Merlini G et al. First glimpse on real-world efficacy outcomes for 2000 patients with systemic light chain amyloidosis in Europe: a retrospective observational multicenter study by the European Myeloma Network. Blood 136, 50–51 (2020).
11.
Bayliss M, Mccausland KL, Guthrie SD, White MK. The burden of amyloid light chain amyloidosis on health-related quality of life. Orphanet J. Rare Dis. 12(1), 1–10 (2017).
•• This survey quantified the burden of amyloid light-chain (AL) amyloidosis in terms of health-related quality of life (HRQoL).
12.
Huang X, Wang Q, Chen W et al. Induction therapy with bortezomib and dexamethasone followed by autologous stem cell transplantation versus autologous stem cell transplantation alone in the treatment of renal AL amyloidosis: a randomized controlled trial. BMC Med. 12, 2 (2014).
13.
Shen K, Dong Y, Fu W et al. Doxycycline combined with bortezomib-cyclophosphamide-dexamethasone chemotherapy for newly diagnosed patients with Mayo 2004 stage II–III light-chain amyloidosis: a randomized controlled multicenter study. Blood 134(Suppl. 1), 1870 (2019).
14.
Kastritis E, Leleu X, Arnulf B et al. Bortezomib, melphalan, and dexamethasone for light-chain amyloidosis. J. Clin. Oncol. 38(28), 3252–3260 (2020).
•• Phase III RCT investigating the efficacy and safety of VMDex for the treatment of patients with newly diagnosed AL amyloidosis.
15.
Kastritis E, Palladini G, Minnema M et al. Subcutaneous daratumumab + cyclophosphamide, bortezomib, and dexamethasone (CyBorD) in patients with newly diagnosed light Chain (AL) amyloidosis: primary results from the phase 3 ANDROMEDA study. 25th Congress of the European Hematology Association. Virtual (11-21 June 2020).
•• Phase III RCT (ANDROMEDA) evaluating the efficacy of D-VCd versus VCd in patients with newly diagnosed AL amyloidosis.
16.
Amyloidosis Research Consortium. Guidance for industry: AL amyloidosis – developing drugs for treatment (2016). www.arci.org/wp-content/uploads/2018/04/Guidance-for-Industry-AL-Amyloidosis-Developing-Drugs-for-Treatment-12_16.pdf
17.
Comenzo RL, Reece D, Palladini G et al. Consensus guidelines for the conduct and reporting of clinical trials in systemic light-chain amyloidosis. Leukemia 26(11), 2317–2325 (2012).
18.
Manwani R, Sharpley F, Mahmood S et al. Achieving a difference in involved and uninvolved light chains (dFLC) of less than 10 mg/l is the new goal of therapy in systemic AL amyloidosis: analysis of 916 patients treated upfront with bortezomib-based therapy. Blood 132, 3262 (2018).
19.
Muchtar E, Dispenzieri A, Leung N et al. Optimizing deep response assessment for AL amyloidosis using involved free light chain level at end of therapy: failure of the serum free light chain ratio. Leukemia 33(2), 527–531 (2019).
20.
Sidana S, Dispenzieri A, Murray DL et al. Revisiting complete response in light chain amyloidosis. Leukemia 34(5), 1472–1475 (2020).
21.
Palladini G, Schonland SO, Sanchorawala V et al. Clarification on the definition of complete haematologic response in light-chain (AL) amyloidosis. Amyloid 28(1), 1–2 (2021).
22.
Mahmood S, Palladini G, Sanchorawala V, Wechalekar A. Update on treatment of light chain amyloidosis. Haematologica 99(2), 209–221 (2014).
23.
Gertz MA. Immunoglobulin light chain amyloidosis: 2020 update on diagnosis, prognosis, and treatment. Am. J. Hematol. 95(7), 848–860 (2020).
24.
Sanchorawala V. Light-chain (AL) amyloidosis: diagnosis and treatment. Clin. J. Am. Soc. Nephrol. 1(6), 1331–1341 (2006).
25.
Schutz N, Nucifora E, Fantl D et al. AL amyloidosis: real world evidence from Argentina. Presented at: 21st congress of the European Hematology Association. Copenhagen, Denmark (9-12 June 2016).
26.
Dispenzieri A, Zonder J, Hoffman J et al. Real-world treatment patterns in patients with light chain (AL) amyloidosis: analysis of the Optum US electronic health records (EHR) and commercial claims database. Blood 136, 4–5 (2020).
27.
Gertz MA, Comenzo R, Falk RH et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): a consensus opinion from the 10th International Symposium on Amyloid and Amyloidosis, Tours, France, 18–22 April 2004. Am. J. Hematol. 79(4), 319–328 (2005).
28.
Drummond MF, Jefferson TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ. The BMJ Economic Evaluation Working Party. BMJ 313(7052), 275–283 (1996).
29.
National Institute for Health and Care Excellence. Single technology appraisal: user guide for company evidence submission template. www.nice.org.uk/process/pmg24/chapter/clinical-effectiveness#quality-assessment-of-the-relevant-clinical-effectiveness-evidence
30.
National Institute for Health and Care Excellence: Decision Support Unit. Technical Support Document 9: the identification, review and synthesis of health state utility values from the literature. http://nicedsu.org.uk/wp-content/uploads/2016/03/TSD9-HSUV-values_FINAL.pdf
31.
Papaioannou D, Brazier J, Paisley S. Systematic searching and selection of health state utility values from the literature. Value Health 16(4), 686–695 (2013).
32.
Ottawa Hospital Research Institute. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. www.ohri.ca/programs/clinical_epidemiology/oxford.asp
33.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. Open Med. 3(3), e123–130 (2009).
34.
Clinicaltrials.gov. Melphalan and dexamethasone with or without bortezomib in treating patients with previously untreated systemic light-chain amyloidosis. https://clinicaltrials.gov/show/NCT01078454 (2010).
35.
Palladini G, Kastritis E, Maurer MS et al. Daratumumab plus CyBorD for patients with newly diagnosed AL amyloidosis: safety run-in results of ANDROMEDA. Blood 136(1), 71–80 (2020).
36.
Wechalekar A, Palladini G, Merlini G et al. Rapid and deep hematologic responses are associated with improved major organ deterioration progression-free survival in newly diagnosed AL amyloidosis: results from andromeda. Blood 136(Suppl. 1), 6–7 (2020).
37.
Suzuki K, Wechalekar A, Kim K et al. Subcutaneous daratumumab (DARA SC) + bortezomib, cyclophosphamide, and dexamethasone (VCd) in Asian patients with newly diagnosed light chain (AL) amyloidosis: subgroup analysis from the phase 3 ANDROMEDA study. Presented at: 62nd ASH Annual Meeting Exposition. Virtual Meeting (5-8 December 2020).
38.
Sanchorawala V, Palladini G, Minnema M et al. Health-related quality of life in patients with AL amyloidosis treated with daratumumab, bortezomib, cyclophosphamide, and dexamethasone: results from the phase 3 ANDROMEDA study. Blood 136(Suppl. 1), 37–40 (2020).
• This Phase III RCT is an HRQoL analysis of the ANDROMEDA trial and reported the effects of pharmacological treatment on patient reported outcomes in patients with newly-diagnosed AL amyloidosis.
39.
Minnema M, Dispenzieri A, Merlini G et al. Outcomes by cardiac stage in newly diagnosed AL amyloidosis: results from ANDROMEDA. Blood 136(Suppl. 1), 44–45 (2020).
40.
Comenzo R, Kastritis E, Palladini G et al. Reduction in absolute involved free light chain and difference between involved and uninvolved free light chain is associated with prolonged major organ deterioration progression-free survival in patients with newly diagnosed AL amyloidosis receiving bortezomib, cyclophosphamide, and dexamethasone with or without daratumumab: results from ANDROMEDA. Presented at: 62nd ASH Annual Meeting and Exposition. Virtual Meeting (5-8 December 2020).
41.
Kastritis E, Gavriatopoulou M, Roussou M et al. Clinical impact of an early response and of early initiation of salvage therapy in patients with systemic light chain (AL) amyloidosis. Blood 134( Suppl. 1), 1894 (2019).
42.
Lebovic D, Hoffman J, Levine BM et al. Predictors of survival in patients with systemic light-chain amyloidosis and cardiac involvement initially ineligible for stem cell transplantation and treated with oral melphalan and dexamethasone. Br. J. Haematol. 143(3), 369–373 (2008).
43.
Basset M, Milani P, Foli A et al. Sequential therapy with cyclophosphamide, bortezomib and dexamethasone followed by autologous stem cell transplant is safe and highly effective in AL amyloidosis. Blood 134(Suppl. 1), 3312 (2019).
44.
Minnema MC, Nasserinejad K, Hazenberg B et al. Bortezomib-based induction followed by stem cell transplantation in light chain amyloidosis: results of the multicenter HOVON 104 trial. Haematologica 104(11), 2274–2282 (2019).
45.
Cornell RF, Zhong X, Arce-Lara C et al. Bortezomib-based induction for transplant ineligible AL amyloidosis and feasibility of later transplantation. Bone Marrow Transplant. 50(7), 914–917 (2015).
46.
Sanchorawala V, Brauneis D, Shelton AC et al. Induction therapy with bortezomib followed by bortezomib-high dose melphalan and stem cell transplantation for light chain amyloidosis: results of a prospective clinical trial. Biol. Blood Marrow Transplant. 21(8), 1445–1451 (2015).
47.
Jain T, Kosiorek HE, Kung ST et al. Treatment with bortezomib-based therapy, followed by autologous stem cell transplantation, improves outcomes in light chain amyloidosis: a retrospective study. Clin. Lymphoma Myeloma Leuk. 18(7), 486–492.e481 (2018).
48.
Basset M, Milani P, Nuvolone M et al. Sequential response-driven bortezomib-based therapy followed by autologous stem cell transplant in AL amyloidosis. Blood Adv. 4(17), 4175–4179 (2020).
49.
Cappuccio I, Pugliese N, De Novellis D et al. Autologous stem cell transplant after induction therapy improves outcome in initially ineligible patients with systemic immunoglobulin light chain amyloidosis. HemaSphere 4(Suppl. 1), 486–487 (2020).
50.
Huang X, Ren G, Chen W et al. The role of induction therapy before autologous stem cell transplantation in low disease burden AL amyloidosis patients. Amyloid 28(2), 75–83 (2021).
51.
Vaxman I, Sidiqi MH, Al Saleh AS et al. Depth of response prior to autologous stem cell transplantation predicts survival in light chain amyloidosis. Bone Marrow Transplant. 56(4), 928–935 (2021).
52.
Caccialanza R, Palladini G, Cereda E et al. Nutritional counseling improves quality of life and preserves body weight in systemic immunoglobulin light-chain (AL) amyloidosis. Nutrition 31(10), 1228–1234 (2015).
53.
Caccialanza R, Palladini G, Klersy C et al. Nutritional status independently affects quality of life of patients with systemic immunoglobulin light-chain (AL) amyloidosis. Ann. Hematol. 91(3), 399–406 (2012).
54.
Sattianayagam PT, Lane T, Fox Z et al. A prospective study of nutritional status in immunoglobulin light chain amyloidosis. Haematologica 98(1), 136–140 (2013).
55.
Sanchorawala V, Mccausland KL, White MK et al. A longitudinal evaluation of health-related quality of life in patients with AL amyloidosis: associations with health outcomes over time. Br. J. Haematol. 179(3), 461–470 (2017).
• This study longitudinally assessed HRQoL in patients with AL amyloidosis and examined associations with health outcomes.
56.
Seldin DC, Anderson JJ, Sanchorawala V et al. Improvement in quality of life of patients with AL amyloidosis treated with high-dose melphalan and autologous stem cell transplantation. Blood 104(6), 1888–1893 (2004).
57.
Dabbous O, Zhou ZY, Tang C, Harvey M, Wu EQ, Arjunji R. RO2 Assessing the relationship between lifelong value and pricing for orphan drugs in ultra-rare diseases. Value Health 22(Suppl. 2), S388 (2019).
58.
Quock TP, Yan T, Tieu R, Souza AD, Broder M. Untangling hospitalizations in systemic amyloidosis: patient characteristics, economic cost and clinical outcomes. HemaSphere 2(Suppl. 2), 297 (2018).
59.
National Institute for Health Research. Ixazomib in combination with oral dexamethasone for relapsed or refractory systemic light chain (AL) amyloidosis. (2014). www.io.nihr.ac.uk/wp-content/uploads/migrated/2585.05573742.Ixazomibcitrate_amyloidosis_March2014.pdf
60.
Douglas K, Sinclair J, Mcquaker G et al. A proactive approach to plerixafor use and subsequent apheresis can reduce failed autologous PBSC mobilization rates to virtually zero after two mobilization attempts: a single-centre series of 40 consecutive PBSC mobilization episodes using plerixafor. Bone Marrow Transplant. 46, S334 (2011).
61.
McCausland KL, Rizio AA, White MK, Bayliss MS, Quock TP. Associations between health-related quality of life and self-reported emergency room department visits and inpatient hospitalizations: insights from a secondary data analysis of patients with light-chain (AL) amyloidosis. Pharmacoecon. Open 3(3), 367–375 (2019).
62.
Blanco M, Gordillo CA, Mapara MY, Satwani P, Reshef R. Healthcare resource utilization for patients undergoing autologous stem cell transplantation: identification of cost drivers. Biol. Blood Marrow Transplant. 24(3 Suppl. 1), S311 (2018).
63.
Quock TP, Yan JT, Chang E, Guthrie SD, Broder MS. Healthcare utilization and costs in commercially insured patients with AL amyloidosis. Blood 130(Suppl. 1), 4659 (2017).
64.
Quock TP, Yan T, Tieu R, Souza AD, Broder M. Economic and clinical outcomes of hospital care in patients with cardiac amyloidosis. Eur. Heart J. 39(Suppl. 1), 505 (2018).
65.
Quock TP, Yan T, Tieu RS, Souza AD, Broder MS. Understanding patterns of 30-day readmission in patients with cardiac amyloidosis. Value Health 21(Suppl. 3), S462 (2018).
66.
Taduru SS, Roy SD, Taneja A et al. Trends of cardiac transplantation in cardiac amyloidosis in the United States from 2008–2014. J. Card. Fail. 23(8 Suppl. 1), S124 (2017).
67.
Dhakal B, Souza AD, Arce-Lara C et al. Superior efficacy but higher cost of plerixafor and abbreviated-course G-CSF for mobilizing hematopoietic progenitor cells (HPC) in AL amyloidosis. Bone Marrow Transplant. 50(4), 610–612 (2015).
68.
Hari P, Lin HM, Asche CV et al. Treatment patterns and health care resource utilization among patients with relapsed/refractory systemic light chain amyloidosis. Amyloid 25(1), 1–7 (2018).
•• This retrospective observational study which evaluated treatment patterns for both newly diagnosed and relapsed/refractory AL amyloidosis, and assessed clinical outcomes, healthcare costs and resource utilization during the first year following a diagnosis of relapsed/refractory AL amyloidosis.
69.
Quock TP, Chang E, Munday JS, Souza AD, Gokhale S, Yan T. Mortality and healthcare costs in Medicare beneficiaries with AL amyloidosis. J. Comp. Eff. Res. 7(11), 1053–1062 (2018).
70.
Quock TP, Yan T, Chang E, Guthrie S, Broder MS. Healthcare resource utilization and costs in amyloid light-chain amyloidosis: a real-world study using US claims data. J. Comp. Eff. Res. 7(6), 549–559 (2018).
•• This study, utilizing data from claims databases, estimated annual healthcare utilization and costs associated with AL amyloidosis.
71.
Quock TP, Yan T, Tieu R, Souza AD, Broder MS. Untangling the clinical and economic burden of hospitalization for cardiac amyloidosis in the United States. Clinicoecon. Outcomes Res. 11, 431–439 (2019).
72.
Dastmalchi LN, Atanda AC, Krepp J. An analysis of patients hospitalized with cardiac amyloidosis and heart failure in the United States: insight from the National Inpatient Sample. J. Am. Coll. Cardiol. 75(11), 1057 (2020).
73.
Isath A, Correa A, Siroky GP et al. Trends, burden, and impact of arrhythmia on cardiac amyloid patients: a 16-year nationwide study from 1999 to 2014. J. Arrhythm. 36(4), 727–734 (2020).
74.
Isath A, Padmanabhan D, Perimbeti S et al. Trends, predictors and impact of arrhythmias in cardiac amyloidosis: a 16-year analysis (1999–2014). J. Am. Coll. Cardiol. 75(11), 371 (2020).
75.
Isath A, Perimbeti S, Correa A et al. Trends and impact of implantable cardioverter defibrillator implantations in patients with cardiac amyloidosis: a 16-year analysis. J. Am. Coll. Cardiol. 75(11), 448 (2020).
76.
Thakkar S, Patel HP, Chowdhury M et al. Impact of arrhythmias on hospitalizations in patients with cardiac amyloidosis. Am. J. Cardiol. 143, 125–130 (2020).
77.
Lin HM, Gao X, Cooke CE et al. Disease burden of systemic light-chain amyloidosis: a systematic literature review. Curr. Med. Res. Opin. 33(6), 1017–1031 (2017).
78.
Gilstrap LG, Dominici F, Wang Y et al. Epidemiology of cardiac amyloidosis-associated heart failure hospitalizations among fee-for-service Medicare beneficiaries in the United States. Circ. Heart Fail. 12(6), e005407 (2019).
79.
Sepehrvand N, Youngson E, Fine N et al. The incidence rates of cardiac amyloidosis over two decades in Alberta, Canada. Can. J. Cardiol. 36(Suppl. 10), S75–S76 (2020).
80.
Vaishnav J, Hubbard A, Chasler JE et al. Management of heart failure in cardiac amyloidosis using an ambulatory diuresis clinic. Am. Heart J. 233, 122–131 (2020).
81.
Attwood C, Sado D, Rice C et al. Safety of delivery of bortezomib to patients with cardiac AL amyloidosis: the impact of cardiac monitoring. Br. J. Haematol. 185(Suppl. 1), 97–98 (2019).
82.
Fotiou D, Dimopoulos MA, Kastritis E. Systemic AL amyloidosis: current approaches to diagnosis and management. Hemasphere 4(4), e454 (2020).
83.
Chaulagain C, Comenzo R. How we treat systemic light-chain amyloidosis. Clin. Adv. Hematol. Oncol. 13(5), 315–324 (2015).
84.
Kastritis E, Palladini G, Minnema MC et al. Daratumumab-based treatment for immunoglobulin light-chain amyloidosis. N. Engl. J. Med. 385(1), 46–58 (2021).
85.
Kastritis E, Gavriatopoulou M, Roussou M et al. Addition of cyclophosphamide and higher doses of dexamethasone do not improve outcomes of patients with AL amyloidosis treated with bortezomib. Blood Cancer J. 7(6), e570 (2017).
86.
Sayago I, Krsnik I, Gomez-Bueno M et al. Analysis of diagnostic and therapeutic strategies in advanced cardiac light-chain amyloidosis. J. Heart Lung Transplant. 35(8), 995–1002 (2016).
87.
Shen KN, Feng J, Huang XF et al. At least partial hematological response after first cycle of treatment predicts organ response and long-term survival for patients with AL amyloidosis receiving bortezomib-based treatment. Ann. Hematol. 96(12), 2089–2094 (2017).
88.
Shah G, Kaul E, Fallo S et al. Bortezomib subcutaneous injection in combination regimens for myeloma or systemic light-chain amyloidosis: a retrospective chart review of response rates and toxicity in newly diagnosed patients. Clin. Ther. 35(10), 1614–1620 (2013).
89.
Kastritis E, Wechalekar AD, Dimopoulos MA et al. Bortezomib with or without dexamethasone in primary systemic (light chain) amyloidosis. J. Clin. Oncol. 28(6), 1031–1037 (2010).
90.
Mahmood AS, Sachchithanantham S, Harrison S et al. Bortezomib-high dose methylprednisolone offers improved haematological responses and overall survival compared to bortezomib-dexamethasone in systemic light chain amyloidosis. HemaSphere 3(Suppl. 1), 958 (2019).
91.
Chong YS, Hutani F, Ting S, Lasica M, Gibbs S. Bortezomib, cyclophosphamide, and dexamethasone (CyBorD) as front-line treatment for systemic AL amyloidosis (AL): a real-world experience at a single centre. Clin. Lymphoma Myeloma Leuk. 19(Suppl. 10), e308–e309 (2019).
92.
Lee JY, Lim SH, Kim SJ et al. Bortezomib, melphalan, and prednisolone combination chemotherapy for newly diagnosed light chain (AL) amyloidosis. Amyloid 21(4), 261–266 (2014).
93.
Manwani R, Mahmood S, Sachchithanantham S et al. Carfilzomib is an effective upfront treatment in AL amyloidosis patients with peripheral and autonomic neuropathy. Br. J. Haematol. 187(5), 638–641 (2019).
94.
Liu B, Wang Y, Bai M et al. Cyclophosphamide + thalidomide + dexamethasone versus melphalan + dexamethasone for the treatment of amyloid light-chain amyloidosis with kidney involvement: a retrospective study in Chinese patients. Clin. Ther. 41(6), 1186–1198 (2019).
95.
Ozga M, Zhao Q, Benson DM et al. The effect of cytogenetic abnormalities on organ involvement and survival in patients with AL amyloidosis. Blood 134(Suppl. 1), 1833 (2019).
96.
Gilles F, Damy T, Bodez D et al. Effect on mortality of combined or sequential chemotherapy in patients with cardiac light-chain amyloidosis. Arch. Cardiovasc. Dis. Suppl. 11(1), 44–45 (2019).
97.
Jaccard A, Comenzo RL, Hari P et al. Efficacy of bortezomib, cyclophosphamide and dexamethasone in treatment-naive patients with high-risk cardiac AL amyloidosis (Mayo Clinic stage III). Haematologica 99(9), 1479–1485 (2014).
98.
Sperry BW, Ikram A, Hachamovitch R et al. Efficacy of chemotherapy for light-chain amyloidosis in patients presenting with symptomatic heart failure. J. Am. Coll. Cardiol. 67(25), 2941–2948 (2016).
99.
Palladini G, Sachchithanantham S, Milani P et al. A European collaborative study of cyclophosphamide, bortezomib, and dexamethasone in upfront treatment of systemic AL amyloidosis. Blood 126(5), 612–615 (2015).
100.
Wechalekar AD, Schonland SO, Kastritis E et al. A European collaborative study of treatment outcomes in 346 patients with cardiac stage III AL amyloidosis. Blood 121(17), 3420–3427 (2013).
101.
Tuzovic M, Kobayashi Y, Wheeler M et al. Functional cardiac recovery and hematologic response to chemotherapy in patients with light-chain amyloidosis (from the Stanford University Amyloidosis Registry). Am. J. Cardiol. 120(8), 1381–1386 (2017).
102.
Bochtler T, Hegenbart U, Kunz C et al. Gain of chromosome 1q21 is an independent adverse prognostic factor in light chain amyloidosis patients treated with melphalan/dexamethasone. Amyloid 21(1), 9–17 (2014).
103.
Hegenbart U, Bochtler T, Benner A et al. Lenalidomide/melphalan/dexamethasone in newly diagnosed patients with immunoglobulin light chain amyloidosis: results of a prospective phase 2 study with long-term follow up. Haematologica 102(8), 1424–1431 (2017).
104.
Kastritis E, Roussou M, Gavriatopoulou M et al. Long-term outcomes of primary systemic light chain (AL) amyloidosis in patients treated upfront with bortezomib or lenalidomide and the importance of risk adapted strategies. Am. J. Hematol. 90(4), E60–65 (2015).
105.
Venner CP, Gillmore JD, Sachchithanantham S et al. A matched comparison of cyclophosphamide, bortezomib and dexamethasone (CVD) versus risk-adapted cyclophosphamide, thalidomide and dexamethasone (CTD) in AL amyloidosis. Leukemia 28(12), 2304–2310 (2014).
106.
Palladini G, Milani P, Foli A et al. Melphalan and dexamethasone with or without bortezomib in newly diagnosed AL amyloidosis: a matched case-control study on 174 patients. Leukemia 28(12), 2311–2316 (2014).
107.
Sanchorawala V, Seldin DC, Berk JL, Sloan JM, Doros G, Skinner M. Oral cyclic melphalan and dexamethasone for patients with AL amyloidosis. Clin. Lymphoma Myeloma Leuk. 10(6), 469–472 (2010).
108.
Palladini G, Milani P, Foli A et al. Oral melphalan and dexamethasone grants extended survival with minimal toxicity in AL amyloidosis: long-term results of a risk-adapted approach. Haematologica 99(4), 743–750 (2014).
109.
Fernandez R, Soto AS, Cepeda F et al. Outcome of first-line therapy for patients with systemic light-chain amyloidosis: monocentric analysis. HemaSphere 3(Suppl. 1), 979 (2019).
110.
Fernandez R, Soto AS, Muniz S et al. Outcome of first-line therapy in patients with systemic light-chain amyloidosis: a multicentre analysis. Clin. Lymphoma Myeloma Leuk. 19(Suppl. 10), e333–e334 (2019).
111.
Gatt ME, Hardan I, Chubar E et al. Outcomes of light-chain amyloidosis patients treated with first-line bortezomib: a collaborative retrospective multicenter assessment. Eur. J. Haematol. 96(2), 136–143 (2016).
112.
Cibeira MT, Oriol A, Lahuerta JJ et al. A phase II trial of lenalidomide, dexamethasone and cyclophosphamide for newly diagnosed patients with systemic immunoglobulin light chain amyloidosis. Br. J. Haematol. 170(6), 804–813 (2015).
113.
Kastritis E, Dialoupi I, Gavriatopoulou M et al. Primary treatment of light-chain amyloidosis with bortezomib, lenalidomide, and dexamethasone. Blood Adv. 3(20), 3002–3009 (2019).
114.
Manwani R, Cohen O, Sharpley F et al. A prospective observational study of 915 patients with systemic AL amyloidosis treated with upfront bortezomib. Blood 134(25), 2271–2280 (2019).
115.
Chari A, Barley K, Jagannath S, Osman K. Safety and efficacy of triplet regimens in newly diagnosed light chain amyloidosis. Clin. Lymphoma Myeloma Leuk. 13(1), 55–61 (2013).
116.
Huang B, Li J, Xu X, Zheng D, Zhou Z, Liu J. Successful treatment of renal light chain (AL) amyloidosis with bortezomib and dexamethasone (VD). Pathol. Biol. (Paris) 63(1), 17–20 (2015).
117.
Tazawa K, Matsuda M, Yoshida T et al. Therapeutic outcome of cyclic VAD (vincristine, doxorubicin and dexamethasone) therapy in primary systemic AL amyloidosis patients. Intern. Med. 47(17), 1517–1522 (2008).
118.
Bochtler T, Hegenbart U, Kunz C et al. Translocation t(11;14) is associated with adverse outcome in patients with newly diagnosed AL amyloidosis when treated with bortezomib-based regimens. J. Clin. Oncol. 33(12), 1371–1378 (2015).
119.
Palladini G, Russo P, Lavatelli F et al. Treatment of patients with advanced cardiac AL amyloidosis with oral melphalan, dexamethasone, and thalidomide. Ann. Hematol. 88(4), 347–350 (2009).
120.
Wei Z, Zhang Y, Li J, Liu P. Upfront ixazomib plus dexamethasone induce promptly hematological response in patients with light-chain amyloidosis. Blood 134(Suppl. 1), 1908 (2019).
121.
Huang X, Wang Q, Chen W, Ren G, Liu Z. Bortezomib with dexamethasone as first-line treatment for AL amyloidosis with renal involvement. Amyloid 23(1), 51–57 (2016).
122.
Diaz-Pallares C, Lee H, Luider J et al. Cyclophosphamide, bortezomib and dexamethasone (CyBorD) for the treatment of newly diagnosed AL amyloidosis: impact of response on survival outcomes. Clin. Lymphoma Myeloma Leuk. 20(6), 394–399 (2020).
123.
Dumas B, Yameen H, Sarosiek S, Sloan JM, Sanchorawala V. Presence of t(11;14) in AL amyloidosis as a marker of response when treated with a bortezomib-based regimen. Amyloid 27(4), 244–249 (2020).
124.
Kastritis E, Fotiou D, Theodorakakou F et al. Timing and impact of a deep response in the outcome of patients with systemic light chain (AL) amyloidosis. Amyloid 28(1), 3–11 (2020).
125.
Nagano N, Yano T, Fujita Y et al. Assessment of prognosis in immunoglobulin light chain amyloidosis patients with severe heart failure: a predictive value of right ventricular function. Heart Vessels 35(4), 521–530 (2020).
126.
Shen KN, Miao HL, Zhang CL et al. Posttreatment dFLC less than 10mg/l predicts superior organ response and longer time to next treatment in newly diagnosed light-chain amyloidosis patients treated with bortezomib. Leuk. Lymphoma 62(4), 874–882 (2020).
127.
Muchtar E, Gertz M, Laplant B et al. Phase 2 trial of ixazomib, cyclophosphamide and dexamethasone for treatment of previously untreated light chain amyloidosis. Blood 136(Suppl. 1), 52–53 (2020).
128.
Palladini G, Milani P, Celant S et al. The Italian Medicines Agency prospective registry of bortezomib-based treatment in AL amyloidosis. Blood 136(Suppl. 1), 22 (2020).
129.
Shu J, Lo S, Phillips M et al. Depression and anxiety in patients with AL amyloidosis as assessed by the SF-36 questionnaire: experience in 1226 patients. Amyloid 23(3), 188–193 (2016).
130.
Rizio AA, White MK, Mccausland KL et al. Treatment tolerability in patients with immunoglobulin light-chain amyloidosis. Am. Health Drug. Benefits 11(8), 430–437 (2018).
131.
White MK, Mccausland KL, Sanchorawala V, Guthrie SD, Bayliss MS. Psychometric validation of the SF-36 health survey in light chain amyloidosis: results from community-based and clinic-based samples. Patient Relat. Outcome Meas. 8, 157–167 (2017).
132.
Rowen D, Brazier J, Roberts J. Mapping SF-36 onto the EQ-5D index: how reliable is the relationship? Health Qual Life Outcomes 7, 27 (2009).
133.
Hester LL, Gifkins DM, Bellew KM et al. Diagnostic delay and characterization of the clinical prodrome in AL amyloidosis: data from 1313 US commercially insured patients between 2006–2018. Blood 134(Suppl. 1), 5517 (2019).
134.
Kastritis E, Gavriatopoulou M, Fotiou D et al. Primary treatment of light chain (AL) amyloidosis with bortezomib, lenalidomide and dexamethasone (VRD) or with bortezomib, cyclophosphamide and dexamethasone (VCD/CyBorD): efficacy and toxicity. Clin. Lymphoma Myeloma Leuk. 19(Suppl. 10), e320–e321 (2019).
135.
Guinault D, Canet E, Huart A et al. Short- and long-term outcomes of AL amyloidosis patients admitted into intensive care units. Br. J. Haematol. 174(6), 868–875 (2016).
Information & Authors
Information
Published In
Pages: 451 - 472
PubMed: 35188424
Copyright
© 2022 Future Medicine Ltd.
History
Received: 22 October 2021
Accepted: 31 January 2022
Published online: 21 February 2022
Keywords:
Topics
Authors
Funding Information
Janssen Global Services
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Systematic literature review of evidence in amyloid light-chain amyloidosis. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0261
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Tobias Sydendal Grand, Shijie Ren, James Hall, Daniel Oudin Åström, Stephane Regnier, Praveen Thokala, Issues, Challenges and Opportunities for Economic Evaluations of Orphan Drugs in Rare Diseases: An Umbrella Review, PharmacoEconomics, 10.1007/s40273-024-01370-2, 42, 6, (619-631), (2024).
- Efstathios Kastritis, Arpit Misra, Laura Gurskyte, Florint Kroi, Andre Verhoek, Jessica Vermeulen, Eric Ammann, Annette Lam, Sarah Cote, Ashutosh D. Wechalekar, Assessing the prognostic utility of hematologic response for overall survival in patients with newly diagnosed AL amyloidosis: results of a meta-analysis, Hematology, 10.1080/16078454.2022.2157581, 28, 1, (2023).