The use and meaning of the parachute metaphor in biomedicine: a citation analysis of a systematic review and a randomized trial of the parachute for freefall
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: Numerous authors have used the ‘parachute' analogy to comment on the importance of and need for randomized, controlled trials (RCTs) in the hierarchy of medical evidence. Methods: The authors completed a retrospective literature analysis examining publications citing the 2003 parachute paper by Smith and Pell and a 2018 RCT of a parachute by Yeh et al. For all of the articles that directly analogized a medical intervention to a parachute, the authors identified the desired outcome of the practice and searched PubMed for relevant RCTs. Results: Authors citing the parachute analogy are often critical of RCTs and often draw comparisons to interventions that are not parachutes.
Nearly two decades have passed since the publication of the tongue-in-cheek observation that there are no randomized, controlled trials (RCTs) of parachutes [1]. Since then, the paper by Smith and Pell has been cited numerous times by both proponents and critics of RCTs, and the parachute analogy has been applied to specific medical practices, as well as the broader role and importance of RCTs in medical practice.
Prior investigations have sought to study the impact of the 2003 parachute paper in biomedicine. A citation analysis conducted by Hayes et al. found that many of these citations misused the parachute analogy. Specifically, Hayes et al. found that authors analogized specific medical practices to parachutes, but in the majority of instances these practices had been tested in randomized trials, suggesting that the medical community did not believe they were parachutes [2]. Moreover, among practices analogized to parachutes that were successful, none had an absolute risk reduction of over 90%, as parachutes do.
More recently, Yeh et al. extended the original satire by conducting an actual RCT on the use of parachutes, which found, after a rigorous statistical analysis, that parachute use does not significantly reduce death or major injury [3]. The Yeh paper showed that investigators and participants would not leap from an airplane with a parachute unless that plane were parked on the ground. Thus, the null results of their RCT may be misinterpreted to mean that parachutes do not provide benefit, when the specific conduct of the trial precludes meaningful conclusion. This argument – that negative RCTs occur because providers are unwilling to randomize patients who would benefit – has been used in biomedicine, for instance, to explain the null results of renal artery stenting for hypertension and stenotic disease [4]. Just like how parachutes have no survival benefit when a participant jumps out of a plane parked on the ground, renal artery stents have no benefit if interventionalists exclude participants in whom they feel stenting must be performed. The limitation to this argument is that to date there is no RCT evidence that stenting stenotic renal arteries improves outcomes in any cohort.
In the current era, RCTs are recognized as the highest level of evidence [5]. However, not every field of medicine relies on them equally for a number of reasons. Some believe that RCTs are only as useful as their interpretation [6], while others believe that other study designs to be more suitable for certain practices [7]. There are also some commenters who believe RCTs to be either fundamentally flawed [8] or unreliable due to conflicted interests of investigators [9,10].
In this analysis, the authors sought to study the attitudes and arguments among authors citing the original 2003 parachute paper and the 2018 paper by Yeh et al. When these articles were cited, what was the intent and meaning imbued to them by subsequent authors? The present work hopes to capture the various attitudes of authors who have been interested in the parachute analogy. How has this analogy been interpreted in biomedicine?
Methods
Search strategy
The authors used Google Scholar to identify all citations to the original 2003 parachute paper by Smith and Pell [1], as well as the 2018 RCT of a parachute by Yeh et al. [3]. Google Scholar was selected because empirical evidence shows it has the most comprehensive citation tracking in its searches [11]. All articles from April 2016 to September 2020 were analyzed. Articles prior to 2016 were excluded, as these were already described in the paper by Hayes et al. and predate the publication of Yeh et al. The authors considered including the 2018 paper by Hayes et al. Unfortunately, it has been cited infrequently (<20-times), and so they decided to omit it.
Eligibility & study selection
The authors excluded all citing articles written in languages other than English, duplicate articles and citations from books (due to COVID-19, the authors were unable to access physical books). After analyzing the contents of the search, the authors excluded the articles without a parachute reference and the articles that could not be accessed. There were some articles that cited the Smith and Pell paper and the Yeh paper for incorrect or unrelated reasons (i.e., a paper about actual parachutes [12]) and some articles that only commented on the use of satire in either paper [13]; because these articles do not address a stance toward RCTs, they were excluded as well. The selection process is shown in Figure 1.
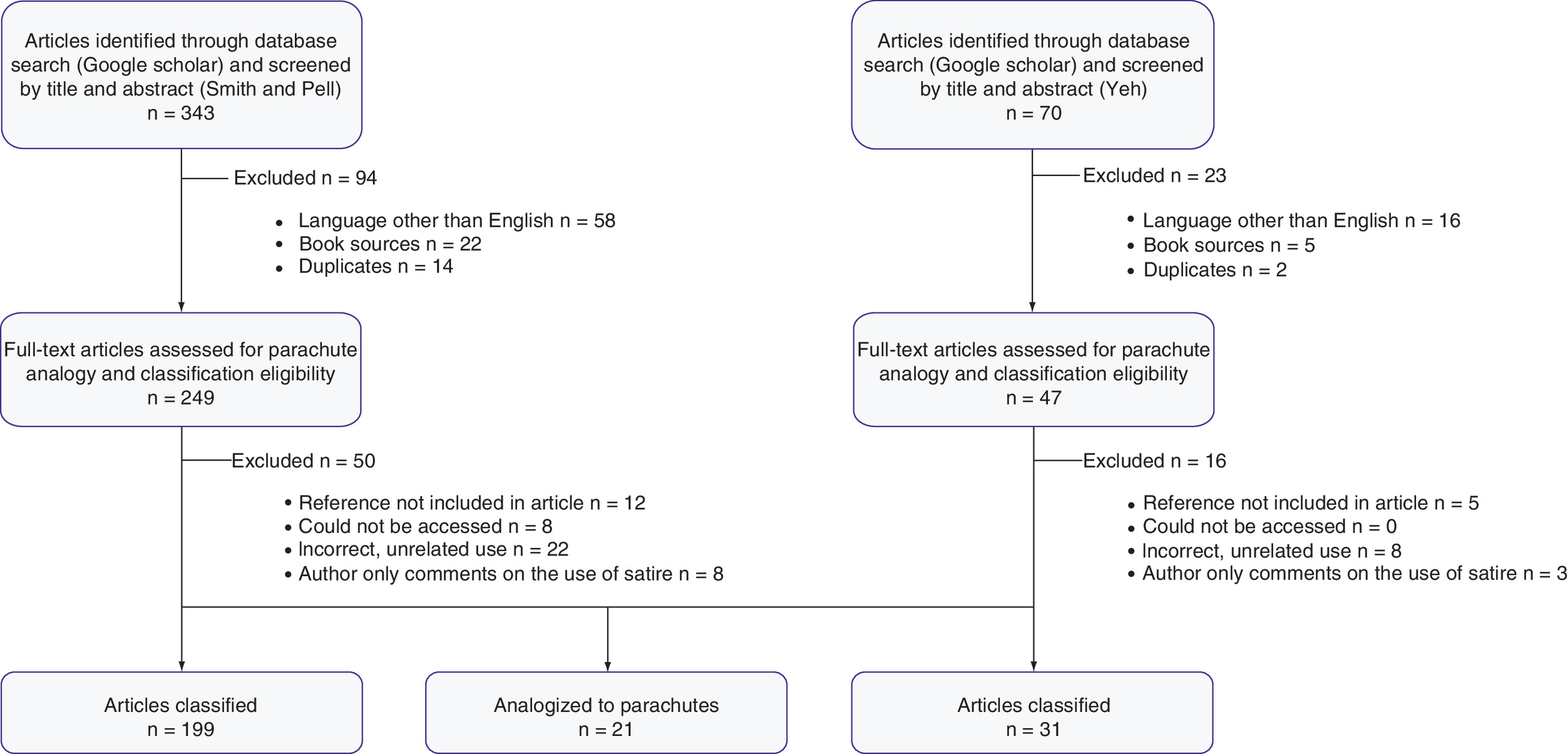
Figure 1. Baseline characteristics of study.
Analysis of 413 articles citing either the Smith and Pell paper (n = 343) or the Yeh paper (n = 70) found in a Google Scholar search.
Classification of attitudes
Manuscripts were assessed based on the stance they took toward RCTs, and classifications were continuously added throughout the process. A total of eight stances toward RCTs were assigned: RCTs are the gold standard of evidence; RCTs are only useful when interpreted rigorously; other study designs can replace RCTs for certain interventions; some unproven interventions should be used without RCTs because based, on common sense, they should work; certain interventions cannot be tested with an RCT, as the trial will either not accrue patients or be impossible to design; it is ethically impermissible to either conduct RCTs or require RCTs for lifesaving interventions; conflicting motives of investigators and/or flawed trial design leads to unreliable RCT data; and RCTs are fundamentally flawed and should not be the gold standard for causal inference in biomedicine.
Analysis of relevant RCTs
For articles that directly analogized medical interventions or practices to parachutes, the authors searched PubMed and Clinicaltrials.gov for completed RCTs that investigate the particular subject described. These RCTs were reviewed to ascertain whether they supported the article's claim, rejected the article's claim or had mixed results. This is similar to the analysis of Hayes et al. [2].
Patient & public involvement
The development of the research question was inspired by the 2018 Hayes et al. paper titled ‘Most medical practices are not parachutes: a citation analysis of practices felt by biomedical authors to be analogous to parachutes’ With the shifting viewpoints of the present-day medical community along with the increased prevalence of RCTs, the authors thought it would be interesting to additionally study the context in which parachutes are analogized. This study was not submitted for institutional review board approval, as it does not involve personally identifiable data nor were patients involved in the design, analysis or interpretation of this study. All of the information used is publicly available.
Results
Between April 2016 and September 2020, the authors found a total of 343 articles citing the Smith and Pell paper and 70 articles citing Yeh et al. on Google Scholar. The authors identified 199 and 31 manuscripts that could be classified, respectively, and among these, 21 manuscripts that directly analogized a practice to a parachute.
Out of the 199 analyzed articles citing the papers by Smith and Pell, 32 (16%) believed that RCTs are the gold standard on the hierarchy of medical evidence; 16 (8%) believed that RCTs are only useful when interpreted and designed rigorously; 12 (6%) believed that alternative study designs can be just as good if not better at providing evidence for certain practices; 59 (30%) believed that some unproven interventions should be used without RCTs due to common sense; 18 (9%) believed that certain interventions by nature cannot be tested via RCT, as the trial would either not accrue patients or the design would not lead to any meaningful conclusions; 41 (21%) believed that it is unethical to either conduct or require RCTs for certain interventions; 15 (8%) believed that RCTs are unreliable due to either faulty trial design or conflicting interests of investigators; and six (3%) believed that RCTs are fundamentally flawed and should not be the gold standard for medical evidence.
Out of the 31 analyzed articles citing the paper by Yeh et al., one (3%) believed that RCTs are the gold standard on the hierarchy of medical evidence; three (10%) believed that RCTs are only useful when interpreted and designed rigorously; one (3%) believed that alternative study designs can be just as good if not better at providing evidence for certain practices; eight (26%) believed that some unproven interventions should be used without RCTs because common sense would suggest that work; three (10%) believed that certain interventions by nature cannot be tested via RCT, as the trial would either not accrue patients or the design would not lead to any meaningful conclusions; four (13%) believed that it is unethical to either conduct or require RCTs for certain interventions; 11 (35%) believed that RCTs are unreliable due to either faulty trial design or conflicting interests of investigators; and zero (0%) believed that RCTs are fundamentally flawed and should not be the gold standard for medical evidence. This is shown in Figure 2.
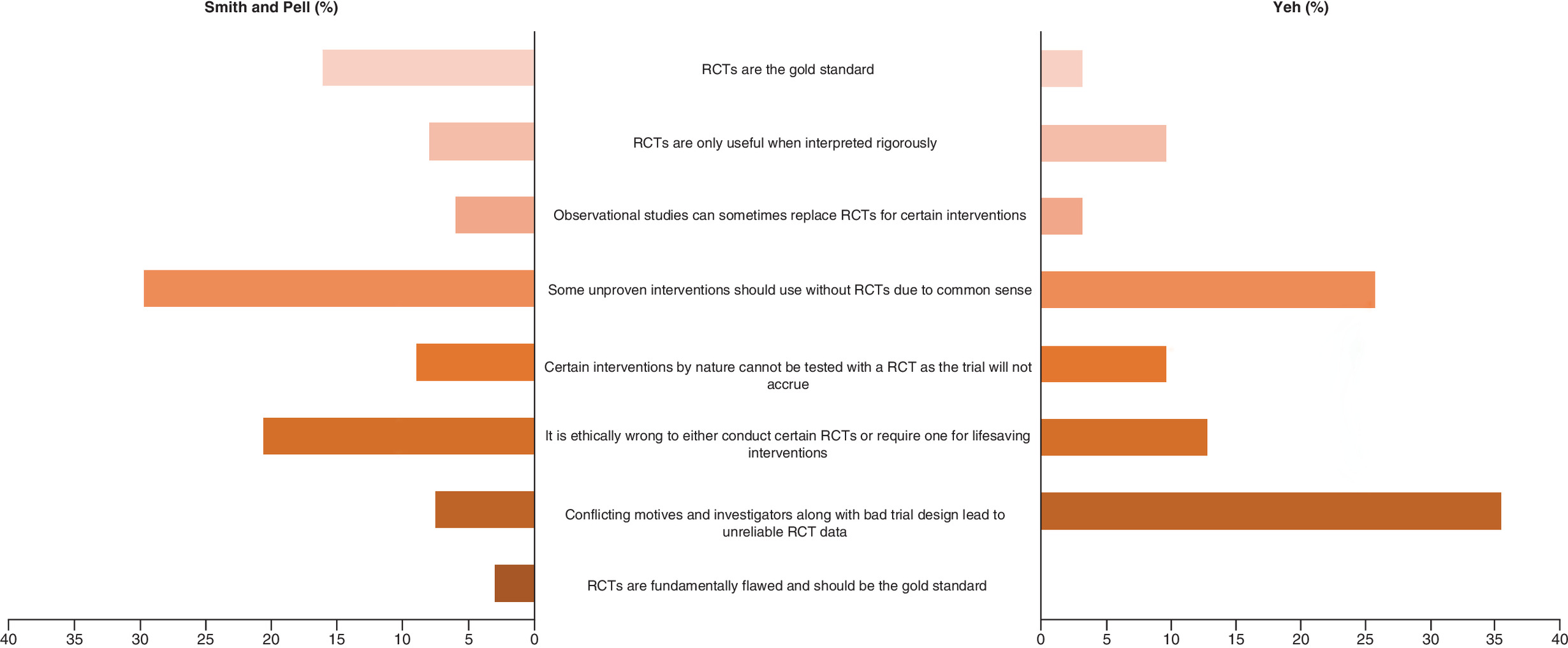
Figure 2. Bar graphs of the various attitudes of authors citing Smith and Pell/Yeh papers (%).
RCT: Randomized controlled trial.
Medical practices analogized to parachutes
Out of the 21 manuscripts analogizing a practice to a parachute, 14 (67%) were found to have had completed RCTs testing the outcome (Table 1). Some examples include vitamin D administration in critically ill patients, nusinersen for spinal muscular atrophy and massive proactive infusion of platelets and plasma in trauma settings. Of these, six (43%) concerned mortality and eight (57%) concerned a lesser outcome such as a reduction in hospitalizations or cardiovascular events. This is shown in Figure 3.
| Claim | RCT | Overall clinical outcome | Trial outcome | Magnitude of outcome met in trial | |
|---|---|---|---|---|---|
| Fassio et al., 2019 | Vitamin D deficiency in critically ill patients is the cause of the problem, so common sense should indicate administration of vitamin D without a RCT | Effect of high-dose vitamin D3 on hospital length of stay in critically ill patients with vitamin D deficiency the VITdAL-ICU randomized clinical trial | Reduction in mortality | Refuted claim | – |
| Singh et al., 2018 | Using chest roentgenography, computerized tomography or ultrasonography for the critically ill is common sense and akin to a parachute | Immediate total-body CT scanning vs conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): a randomised controlled trial | Reduction in mortality | Refuted claim | – |
| Stone et al., 2019 | Use of transcatheter mitral valve repair (TMVr) in patients with mitral regurgitation (MR) is common sense and should not be subject to RCT | Transcatheter mitral-valve repair in patients with heart failure | Reduction in hospitalizations | Supported claim | Rate of hospitalizations decreased from 67.9% to 35.8%; ARR: 32.1, NNT: 3.11 |
| Ho et al., 2016 | Proactive use of massive plasma/platelet infusions in trauma is common sense and akin to a parachute | Plasma-first resuscitation to treat haemorrhagic shock during emergency ground transportation in an urban area: a randomised trial and Saline vs plasma-lyte A in initial resuscitation of trauma patients: a randomized trial | Reduction in mortality | Refuted claim | – |
| Crawford et al., 2017 | Standard of care for treatment of spinal muscular atrophy cannot be ethically randomized and is impossible to blind | Nusinersen vs sham control in later-onset spinal muscular atrophy | Increase in rates of motor function improvement from baseline (HMFSE score) | Supported claim | Rates of HMFSE score improvement increased from 26% to 57%; ARR: 31, NNT: 3.23 |
| Schonewille et al., 2020 | Intraarteriolar thrombolysis is akin to a parachute for stroke patients | Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke | Reduction in disability | Supported claim | Rates of disability decreased from 52.4% to 45.2%; ARR: 7.2, NNT: 14 |
| Cornelissen et al., 2018 | Surgical treatment of malignant mesothelioma is common sense and akin to a parachute | Extra-pleural pneumonectomy vs no extra-pleural pneumonectomy for patients with malignant pleural mesothelioma: clinical outcomes of the Mesothelioma and Radical Surgery (MARS) randomised feasibility study | Reduction in mortality | Refuted claim | – |
| Meier et al., 2019 | Patent foramen ovale closure in stopping cerebral embolism is akin to a parachute and the conclusions RCTs are unreliable due to the publication rigor of journals | Closure of patent foramen ovale vs medical therapy after cryptogenic stroke | Reduction in recurrent stroke | Mixed results | – |
| Steinsapir et al., 2019 | Chlorhexidine use for surgery is common sense and is akin to a parachute | Effectiveness of 0.12% chlorhexidine gluconate oral rinse in reducing prevalence of nosocomial pneumonia in patients undergoing heart surgery, Oropharyngeal and nasopharyngeal decontamination with chlorhexidine gluconate in lung cancer surgery: a randomized clinical trial and Randomized controlled trial to reduce bacterial colonization of surgical drains with the use of chlorhexidine-coated dressings after breast cancer surgery | Reduction in rate of infection | Mixed results | – |
| Dardis et al., 2016 | Thrombopoietin receptor agonist use in chemotherapy-induced thrombocytopenia is common sense and akin to a parachute | Eltrombopag vs placebo for low-risk myelodysplastic syndromes with thrombocytopenia (EQoL-MDS): phase 1 results of a single-blind, randomised, controlled, phase 2 superiority trial | Increase in platelet response | Supported claim | Platelet responses increased from 3% to 47%; ARR: 44, NNT: 2.3 |
| Arulkumaran et al., 2020 | Uterine balloon tamponade use for the treatment of postpartum hemorrhage is common sense and is akin to a parachute | The effectiveness and safety of introducing condom-catheter uterine balloon tamponade for postpartum haemorrhage at secondary level hospitals in Uganda, Egypt and Senegal: a stepped wedge, cluster-randomised trial and Uterine balloon tamponade as an adjunct to misoprostol for the treatment of uncontrolled postpartum haemorrhage: a randomised controlled trial in Benin and Mali | Reduction in mortality | Refuted claim | – |
| Keane et al., 2020 | RCTs that have disproved hydroxychloroquine's affect in COVID-19 patients are unreliable | A randomized trial of hydroxychloroquine as postexposure prophylaxis for COVID-19 and Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: open label, randomised controlled trial | Reduction in symptoms and incidence of COVID-19 | Refuted claim | – |
| Magini et al., 2017 | Polytetrafluoroethylene (ePTFE)-covered stents use in TIPS is common sense and akin to a parachute | Transjugular intrahepatic portosystemic shunts with covered stents increase transplant-free survival of patients with cirrhosis and recurrent ascites | Reduction in mortality | Supported claim | Mortality decreased from 93% to 52%; ARR: 41, NNT: 2.4 |
| White et al., 2019 | Current RCTs in renal stenting that have rejected the practice are unreliable and cannot be applied to the general population | Stenting and medical therapy for atherosclerotic renal-artery stenosis | Reduction in cardiovascular events | Refuted claim | – |
ARR: Absolute risk reduction; HMFSE: Hammersmith functional motor scale – expanded; NNT: Number needed to treat; RCT: Randomized, controlled trial.

Upon analysis, seven (50%) manuscripts were refuted by RCTs, five (36%) manuscripts were supported by RCTs and two (14%) had mixed results. For the five manuscripts supported by RCTs, the absolute risk reduction (ARR) ranged from 7.2 to 44 and the number needed to treat (NNT) ranged from 2.3 to 14. This is shown in Figure 4.

Figure 4. Randomized clinical trials for authors' claims.
ARR: Absolute risk reduction; NNT: Number needed to treat.
Discussion
The authors investigated the attitudes and beliefs of authors citing two prominent papers on the parachute analogy to biomedicine. Specifically, in a 2003 paper, a parachute was cited as an intervention of obvious benefit, with a massive effect size that could not possibly be tested in randomized trials and had never been. In a 2018 paper, a parachute RCT was conducted. However, participants and investigators were unable to randomize patients jumping from higher than a plane safely parked on the tarmac. Thus, the results were uninformative. The present study sought to assess the attitudes among 230 articles citing these papers and found that the general attitude was either critical or dismissive of RCTs.
Notably, the authors found different patterns of interpretation for the two studies (Figure 2). The plurality of references to the paper by Smith and Pell was to argue that it was common sense a practice worked, and it could not be tested in RCTs. The plurality of references to the paper by Yeh and colleagues argued that conflicting motives of investigators and/or flawed trial design made the conclusions reached by RCTs unreliable, spurious or limited.
In general, many citing papers are critical of the need for, importance of or feasibility of RCTs. To some degree, this may reflect real barriers to randomization, such as cost [14] and bureaucratic hurdles [15], but it may also reflect a lack of awareness of the virtue of randomization [16]. A recent paper found that among the American public, few were willing to participate in randomized trials [17]; other studies show that some are unclear as to their purpose [18,19].
When specific medical practices were analogized to parachutes, the present study found that most of the interventions have already been tested with one or more RCTs. Among these interventions, less than half were outright supported by the evidence and not a single one was found to have an ARR close to that of a parachute. Notably, the AFF for a parachute is 99.999+%, while that of the single most effective practice this study identified was 44%.
Limitations
This analysis has three limitations. First, it places a degree of reliance on the ability of Google Scholar to capture all of the articles citing the two papers. Although this search engine possesses the greatest citation network for this purpose [10], the authors may not have captured every article. Second, as with any paper that seeks to interpret the use of language, this study relied on human interpretations, which are subjective and can be debated. The authors encourage others to study this space and classify articles they believe appropriate. Third, use of the parachute analogy is constantly evolving and subject to change as authors continuously reference the two papers.
Conclusion
The authors studied the nature of citations in two prominent papers on parachutes. The first paper pointed out that there were no RCTs of parachutes, and the second conducted an RCT of the parachute from a short height and was incapable of answering a meaningful question. Many citations to these papers (86%) are critical of the need for, validity of or generalizability of RCTs. Occasionally, authors name specific medical practices that are analogous to parachutes. When these are named, the majority (67%) have RCTs and less than half are positive (36%). The parachute analogy appears to be misused and misunderstood in biomedicine.
•
The authors conducted a retrospective literature analysis of papers, citing a 2003 paper by Smith and Pell and a 2018 paper by Yeh et al. comparing therapeutic interventions to parachutes.
•
Selection included multi-level stratification through 413 papers within Google Scholar, including papers that analogize therapeutics to parachutes.
•
A qualitative assessment of all reviewed papers was done categorizing the citations into eight categories.
•
In general, the authors found that the academic medical community primarily utilizes the parachute analogy described in the two papers as a way of describing fault in the effectiveness of randomized, controlled trials (RCTs).
•
Papers that directly analogized a specific therapeutic intervention to a parachute were further analyzed, and the authors successfully found RCTs describing clinical efficacy for roughly two-thirds of these interventions.
•
The authors analyzed the RCTs for a quantifiable value for efficacy in the form of absolute risk reduction ratio and compared these values with that of a parachute.
•
The majority of the biomedical, scientific community that uses the analogizes of therapeutic interventions to parachutes do so to discount the need for RCTs in the evaluation of therapeutic interventions in the clinical setting.
•
Many of the interventions that are directly described in this way have already been evaluated by means of RCT and carry absolute risk reductions that are far from those of parachutes.
Financial & competing interests disclosure
V Prasad discloses research funding from Arnold Ventures; royalties from Johns Hopkins Press, Medscape and MedPage; consulting fees from UnitedHealthcare; and speaking fees from Evicore and New Century Health; Plenary Session podcast has Patreon backers. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
References
1.
Smith GCS, Pell JP. Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ 327(7429), 1459–1461 (2003).
2.
Hayes MJ, Kaestner V, Mailankody S, Prasad V. Most medical practices are not parachutes: a citation analysis of practices felt by biomedical authors to be analogous to parachutes. CMAJ Open 6(1), e31–e38 (2018).
3.
Yeh RW, Valsdottir LR, Yeh MW et al. Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial. BMJ 363, k5094 (2018).
4.
ASTRAL Investigators, Wheatley K, Ives N et al. Revascularization versus medical therapy for renal-artery stenosis. N. Engl. J. Med. 361(20), 1953–1962 (2009).
5.
Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plast. Reconstr. Surg. 128(1), 305–310 (2011).
6.
Van Poucke S, Thomeer M, Heath J, Vukicevic M. Are randomized controlled trials the (g)old standard? From clinical intelligence to prescriptive analytics. J. Med. Internet Res. 18(7), e185 (2016).
7.
Pagnamenta F. Evidence generation for wound care dressing selection: reviewing the issues. J. Wound Care 26(9), 545–550 (2017).
8.
Reid B. Avoiding philosophy as a trump-card in sociological writing. A study from the discourse of evidence-based healthcare. Soc. Theory Health 15(4), 369–387 (2017).
9.
Svendsen K, Arnesen E, Retterstøl K. Saturated fat – a never ending story? Food Nutr. Res. 61(1), 1377572 (2017).
10.
Monsen K. Better medical apps for healthcare practitioners through interdisciplinary collaboration: lessons from transfusion medicine. PhD Diss. University of Edinburgh (2017).
11.
Gehanno J-F, Rollin L, Darmoni S. Is the coverage of Google Scholar enough to be used alone for systematic reviews. BMC Med. Inform. Decis. Mak. 13, 7 (2013).
12.
Richardson JJ, Liang K, Lisi F et al. Controlling the growth of metal-organic frameworks using different gravitational forces. Eur. J. Inorg. Chem. 2016(27), 4499–4504 (2016).
13.
Bover J, Ureña-Torres P, Mateu S et al. Evidence in chronic kidney disease – mineral and bone disorder guidelines: is it time to treat or time to wait? Clin. Kidney J. 13(4), 513–521 (2020).
14.
Sertkaya A, Wong H-H, Jessup A, Beleche T. Key cost drivers of pharmaceutical clinical trials in the United States. Clin. Trials Lond. Engl. 13(2), 117–126 (2016).
15.
Califf RM. Clinical trials bureaucracy: unintended consequences of well-intentioned policy. Clin. Trials Lond. Engl. 3(6), 496–502 (2006).
16.
Dellson P, Nilsson K, Jernström H, Carlsson C. Patients' reasoning regarding the decision to participate in clinical cancer trials: an interview study. Trials 19(1), 528 (2018).
17.
Unger JM, Cook E, Tai E, Bleyer A. The role of clinical trial participation in cancer research: barriers, evidence, and strategies. Am. Soc. Clin. Oncol. Educ. Book Am. Soc. Clin. Oncol. Annu. Meet. 35, 185–198 (2016).
18.
Ridgeway JL, Asiedu GB, Carroll K, Tenney M, Jatoi A, Radecki Breitkopf C. Patient and family member perspectives on searching for cancer clinical trials: a qualitative interview study. Patient Educ. Couns. 100(2), 349–354 (2017).
19.
Mills EJ, Seely D, Rachlis B et al. Barriers to participation in clinical trials of cancer: a meta-analysis and systematic review of patient-reported factors. Lancet Oncol. 7(2), 141–148 (2006).
Information & Authors
Information
Published In
Pages: 383 - 390
PubMed: 35189694
Copyright
© 2022 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 15 July 2021
Accepted: 28 January 2022
Published online: 22 February 2022
Keywords:
Topics
Authors
Funding Information
Arnold Ventures: N/A
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The use and meaning of the parachute metaphor in biomedicine: a citation analysis of a systematic review and a randomized trial of the parachute for freefall. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0171
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Frank Ursin, Katharina Fürholzer, Sabine Salloch, Metaphors in digital radiology: ethical implications for responsibility assignments of human-AI imaginaries, AI & SOCIETY, 10.1007/s00146-025-02270-5, 40, 7, (5139-5149), (2025).
- Matthew A. Albrecht, Razi Hasan, Reliable crash analysis: Comparing biases and error rates of empirical Bayes before-after analyses to mixed-models, Accident Analysis & Prevention, 10.1016/j.aap.2025.107921, 212, (107921), (2025).
- Mariana Barosa, Euzebiusz Jamrozik, Vinay Prasad, The Ethical Obligation for Research During Public Health Emergencies: Insights From the COVID-19 Pandemic, Medicine, Health Care and Philosophy, 10.1007/s11019-023-10184-6, 27, 1, (49-70), (2023).