Patterns of emergency department visits preceding colorectal cancer diagnosis: a population-based study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the patterns of emergency department (ED) visits in the 3 months preceding a diagnosis of colorectal cancer (CRC) in a real-world, population-based context. Materials & methods: Linked provincial registries in Alberta, Canada, were accessed and patients with CRC diagnosed between 2004 and 2018 were identified. The National Ambulatory Care reporting system was used to identify patients who visited an ED within 3 months of a diagnosis of CRC. Multivariable logistic regression analysis was used to identify factors associated with any ED visits as well as frequent (≥3) ED visits. Results: A total of 25,310 patients with CRC were included in the current study. These include 10,126 patients (40%) who had at least one visit to the ED in the 3 months before a diagnosis of CRC diagnosis and 613 patients (2.4%) who visited the ED multiple (≥3) times. The following factors were associated with any visit to an ED: older age (odds ratio [OR]: 1.010; 95% CI: 1.008–1.012), female gender (OR: 1.23; 95% CI: 1.16–1.30), higher comorbidity index (OR: 1.38; 95% CI: 1.35–1.41), metastatic disease (OR: 2.37; 95% CI: 2.23–2.53), proximal tumors (OR: 1.59; 95% CI: 1.50–1.68) and North zone (OR vs south zone: 1.75; 95% CI: 1.55–1.98). Conclusion: It is not uncommon for CRC patients to visit the ED at least once in the 3 months prior to having such a diagnosis. Factors associated with frequent pre diagnosis emergency visits included female gender, higher burden of comorbid disease, advanced stage, proximal tumors and living in the North zone of Alberta (where there is limited access to specialist care).
Colorectal cancer (CRC) represents a major cause of morbidity and mortality in Canada; 2019 cancer statistics confirm that CRC is the second most common cancer in males and the third most common cancer in females [1]. CRC screening has been shown to decrease CRC mortality and improve outcomes; although, compliance in the Canadian setting has been challenging [2,3].
One important quality indicator for CRC care is the proportion of patients diagnosed emergently versus electively because these patients are more likely to present at a more advanced stage [4,5]. Diagnosis through the emergency department (ED) is likely to be more costly to the healthcare system compared with diagnosis through outpatient ambulatory assessments [6,7]. Alberta is a large Canadian province with a universal healthcare model. Its administrative databases and centralized healthcare registries are thus suited to analyze questions related to patterns of presentation of CRC.
The aim of this study was to assess the patterns of ED visits in the 3 months preceding CRC diagnosis in the province of Alberta, Canada. Our secondary objectives were to identify risk factors and potentially avoidable causes for presentation to the emergency room in a real-world, population-based context. We aimed also to evaluate whether rates of ED visits have changed over time in relationship to implementation of population-based CRC screening.
Materials & methods
Data sources
Data of the current study are based on the Alberta Cancer Registry linked with emergency department (ED) visit data from the Canadian National Ambulatory Care Reporting System (NACRS). These visits were marked by an abstract code of E.
Initial administrative data extraction was conducted by Surveillance and Reporting team at Cancer Care Alberta (with no subsequent chart review of individual patients' files). This study was approved by the Health Research Ethics Board of Alberta (HREBA.CC-20-0215). Selection criteria for the current study included patients with a new diagnosis of colorectal carcinoma in Alberta (2004–2018) who were captured by the Alberta Cancer Registry. Cases with squamous cell carcinoma or neuroendocrine carcinoma were not included in the current analysis. For patients with more than one primary colorectal cancer (CRC) during the duration of the study, only the first one was included in the study cohort.
Healthcare in Alberta is publicly funded and ED visits done at any hospital in Alberta are centrally captured in the provincial database. Likewise, all new cancer cases diagnosed in Alberta are captured within the Alberta cancer registry. From a healthcare perspective, Alberta is classified into five zones (North zone, Edmonton zone, central zone, Calgary Zone and South zone). The most notable difference between zones is that the North zone represents the largest zone in terms of landmass within the province; but has the lowest population/landmass ratio with limited access to tertiary cancer care facilities [8]. Population-based CRC screening in the two big Albertan cancer centers (Edmonton and Calgary) has been implemented since 2008 [9], and then, it was rolled out to the rest of the province.
Data collection
The following data were collected from included patients where available: age at diagnosis, sex, Charlson comorbidity index, presence of metastatic disease at presentation, primary tumor site, side of the primary (proximal/right-sided: before splenic flexure; distal/left-sided: starting from splenic flexure), zone of residence, year of CRC diagnosis and first recorded treatment (within Alberta Cancer Registry database). Other reported information include recorded ED visit(s) in the 3 months before the date of cancer diagnosis (date of cancer diagnosis within Alberta Cancer Registry is presumably the date of pathological diagnosis of cancer), the number of these emergency visits and reasons for each visit. The reason for the visit was reported according to ICD-10 codes. When more than one visit was recorded within 1 day for the same patient, it was considered as a single visit and the second visit was omitted.
Statistical analysis
Differences in baseline characteristics between patients who have at least one emergency visit versus those who did not have any, as well as characteristics of patients with frequent (≥3) ED visits before cancer diagnosis were explored using Chi-Squared test for categorical variables and independent t-test for continuous variables. Further frequency analyses were conducted to examine the different reasons for ED visits (when more than one diagnosis was reported for a single visit, the first reported diagnosis only was included in this analysis). Furthermore, the frequency of three diagnoses of interest (anemia, abdominal pain and gastrointestinal hemorrhage), regardless of whether these were the first recorded diagnoses or not, was examined in some patient subgroups (according to age, gender and tumor side). These three diagnoses of interest were selected a priori as they are the most likely to be encountered by primary/ambulatory care providers (in addition to emergency presentations).
Multivariable logistic regression analysis was then used to examine factors associated with any visit to the ED in the 3 months before cancer diagnosis as well as factors associated with frequent (≥3) visits. The following factors were included in these models: age at diagnosis, gender, Charlson comorbidity index, presence of metastatic disease, side of the primary and zone of residence.
All the above statistical analyses were conducted through SPSS software (version 26.0, IBM, NY, USA).
Results
Patients’ characteristics
A total of 25,310 patients with colorectal cancer (CRC) were found eligible and were included in the current study (Figure 1 shows the selection process for patients). These include 10,126 patients (40%) who had at least one visit to the emergency department (ED) within 3 months before CRC diagnosis and 15,184 patients (60%) who had no recorded ED visits within 3 months before diagnosis. A total of 16,420 ED visits were recorded for the subgroup of patients who visited the ED within 3 months of CRC diagnosis (some patients visited the ED more than once). The percentage of patients with at least one ED visit across study years was described in Supplementary Figure 1 (percentage in 2004: 38.4%; percentage in 2018: 41.8%). There was no difference in percentage of patients with pre diagnosis ED visits before and after 2009 (date of rollout of colorectal screening among urban centers in Alberta) (40.5 vs 39.8%; p = 0.308).
Comparing patients who visited an ED versus those who did not visit an ED in the 3 months prior to a diagnosis, patients with ED visits were more likely to be older (p < 0.001), female (42.9 vs 37.8%; for males p < 0.001) and to have higher mean comorbidity index (p < 0.001), proximal tumor (48.3 vs 34.6% for distal tumors; p < 0.001), stage IV disease (55.5 vs 35.7% for less than stage IV disease; p < 0.001) and residence in the North zone (51.1 vs 37.7% for Edmonton zone; p < 0.001) (Table 1).
| Parameter | ED visits within 3 months before diagnosis (10,126 patients) | No ED visits within 3 months before diagnosis (15,184 patients) | p-value |
|---|---|---|---|
| Age (mean; SD) | 69.60; 14.06 | 66.73; 12.06 | <0.001 |
| Sex –Males –Females | 5463 (37.8%) 4663 (42.9%) | 8987 (62.2%) 6197 (57.1%) | <0.001 |
| Charlson comorbidity index (mean; SD) | 0.97; 1.39 | 0.50; 0.95 | <0.001 |
| Presence of metastatic disease (stage IV) –Non-metastatic –Metastatic | 7087 (35.7%) 3039 (55.5%) | 12,750 (64.3%) 2434 (44.5%) | <0.001 |
| Sidedness† –Proximal/right-sided (up to splenic flexure) –Distal/left-sided (starting from splenic flexure) | 4539 (48.3%) 5380 (34.6%) | 4849 (51.7%) 10162 (65.4%) | <0.001 |
| First recorded treatment –Surgery –Other treatments –None/observation/refused | 6924 (37.1%) 1560 (36.8%) 1642 (67.4%) | 11,723 (62.9%) 2668 (63.2%) 793 (32.6%) | <0.001 |
| Zone of residence† –South Zone –Calgary zone –Central zone –Edmonton zone –North zone | 807 (37.9%) 3082 (37.8%) 1628 (42.7%) 3180 (37.7%) 1428 (51.1%) | 1324 (62.1%) 5062 (62.2%) 2184 (57.3%) 5244 (62.3%) 1367 (48.9%) | <0.001 |
†
There were 380 patients who have unknown side of the primary tumor; and there were four patients who have unknown zone of residence.
ED: Emergency department.
Within the study cohort, 613 patients (2.4%) visited the ED multiple times (≥ three-times) in the 3 months before their CRC diagnosis. Those patients were more likely to be female (p < 0.001) and to have a higher mean comorbidity index (p < 0.001), proximal tumor (p < 0.001), stage IV disease (p < 0.001) and residence in the North zone (p < 0.001).
Reasons for ED visits
The most frequent ED diagnoses were: digestive disorders (17.2%), nonspecific symptoms/signs (11%), abdominal/pelvic pain (10.1%), intestinal obstruction (8.4%), contact with health services (e.g., encounter with health services for examination, investigations or other reasons) (7.2%), gastrointestinal hemorrhage (GI) (7.2%), anemia (6.3%) (Supplementary Table 1, Figure 2 & Supplementary Figure 2).
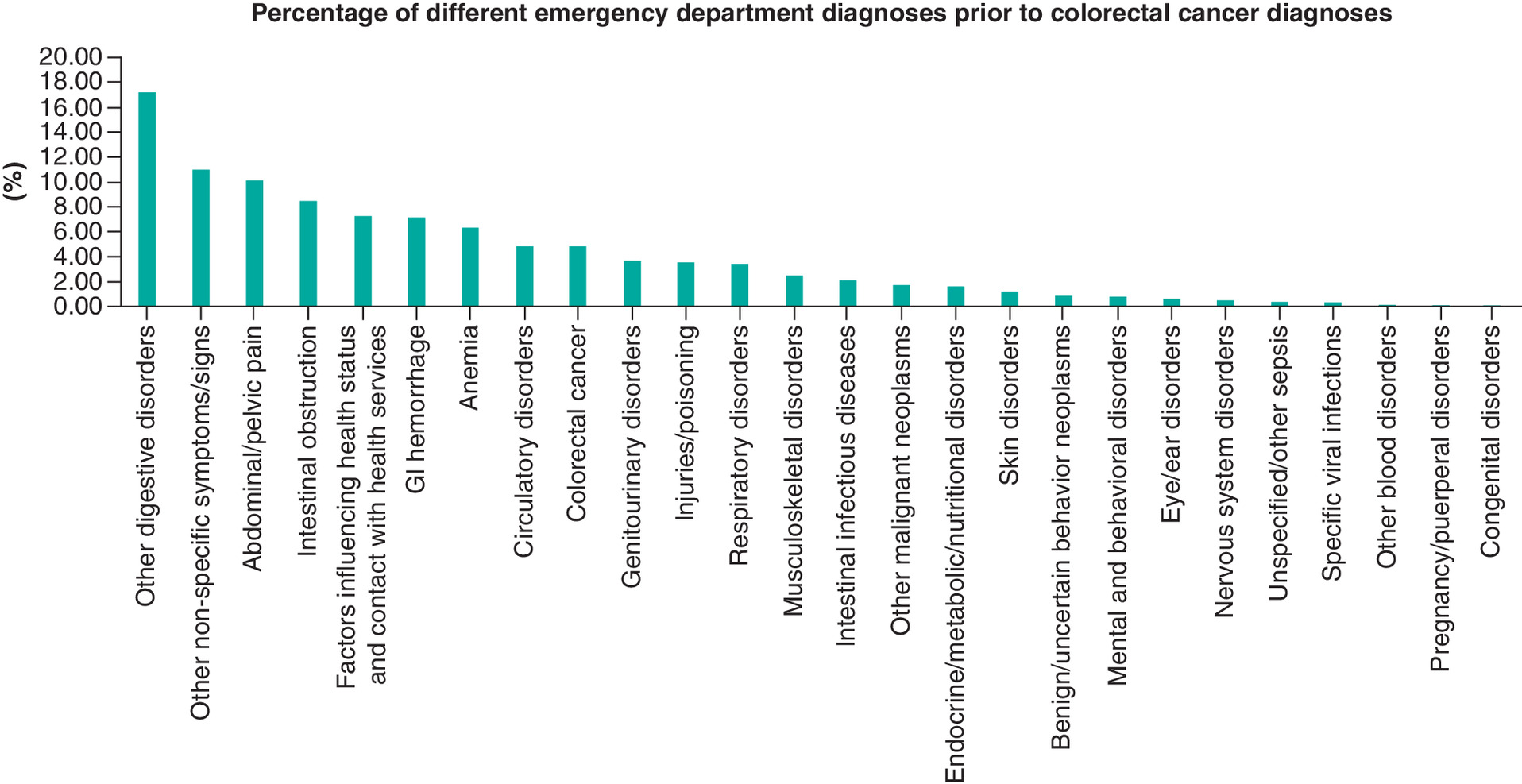
Figure 2. Percentage of first-recorded emergency department visit diagnoses within the included patients.
GI: Gastrointestinal.
The frequency of certain ED diagnoses of interest (anemia, abdominal pain and gastrointestinal hemorrhage) within certain patient subgroups (according to age, gender and tumor sidedness) was further detailed in Figure 3.
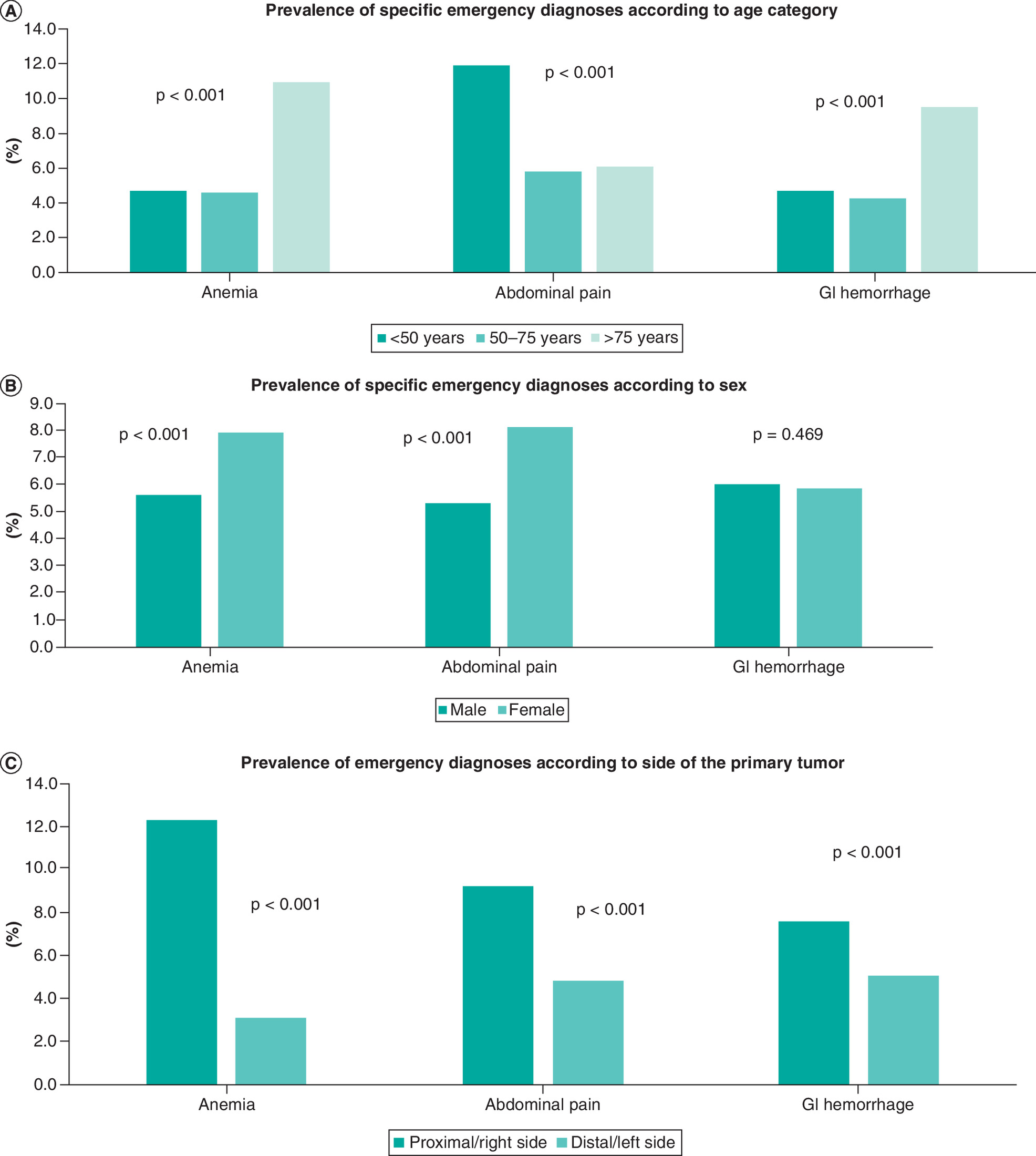
Figure 3. Prevalence of specific emergency diagnoses.
Prevalence of specific emergency diagnoses according to (A) age category; (B) sex; (C) side of the primary tumor.
GI: Gastrointestinal.
Factors associated with ED visits
In the multivariable logistic regression analysis, the following factors were associated with any visit to ED: older age (OR: 1.010; 95% CI: 1.008–1.012), female gender (OR: 1.23; 95% CI: 1.16–1.30), higher comorbidity index (OR: 1.38; 95% CI: 1.35–1.41), metastatic disease (OR: 2.37; 95% CI: 2.23–2.53), proximal tumors (OR: 1.59; 95% CI: 1.50–1.68) and North zone (OR vs south zone: 1.75; 95% CI: 1.55–1.98) (Table 2).
| Variables | Any ED visit | Multiple ED visits |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| Age (included as a continuous predictor) | 1.010 (1.008–1.012) | 0.997 (0.990–1.003) |
| Sex –Males –Females | Reference 1.23 (1.16–1.30) | Reference 1.53 (1.30–1.81) |
| Charlson comorbidity index (included as a continuous predictor) | 1.38 (1.35–1.41) | 1.32 (1.26–1.40) |
| Presence of metastatic disease (stage IV) –Non metastatic –Metastatic | Reference 2.37 (2.23–2.53) | Reference 1.83 (1.53–2.18) |
| Sidedness –Distal (starting from splenic flexure) –Proximal (up to splenic flexure) | Reference 1.59 (1.50–1.68) | Reference 1.30 (1.10–1.54) |
| Zone of residence –South zone –Calgary zone –Central zone –Edmonton zone –North zone | Reference 1.02 (0.92–1.14) 1.19 (1.06–1.33) 0.93 (0.84–1.03) 1.75 (1.55–1.98) | Reference 0.33 (0.23–0.46) 1.33 (0.99–1.80) 0.45 (0.33–0.61) 2.02 (1.50–2.72) |
ED: Emergency department; OR: Odds ratio.
Similarly, the following factors were associated with frequent (≥3) ED visits: female gender (OR: 1.53; 95% CI: 1.30–1.81), higher comorbidity index (OR: 1.32; 95% CI: 1.26–1.40), metastatic disease (OR: 1.83; 95% CI: 1.53–2.18), proximal tumors (OR: 1.30; 95% CI: 1.10–1.54) and North zone (OR: 2.02; 95% CI: 1.50–2.72) (Table 2).
Discussion
The current study reviewed patterns of emergency department (ED) visits before colorectal cancer (CRC) diagnosis in a large Canadian province. Almost 40% of patients diagnosed with CRC visited the ED at least once in the 3 months prior to their diagnosis. Factors associated with frequent pre diagnosis emergency visits included female gender, comorbidity burden, advanced disease, proximal tumors and residence within the North zone of the province (where there is limited access to specialist care).
It is notable also that a small percentage of patients have an ED diagnosis of CRC (although, these visits happened before the date of pathological diagnosis of CRC). A possible reason might be related to the fact that some of these patients might have radiological or other nonpathological evidence of CRC (e.g., rectal mass on rectal examination) and so a provisional diagnosis of CRC was made at the ED before pathological confirmation of the disease.
Several explanations can be provided for the observed gender differences in ED visits. In a previous qualitative synthesis of evidence regarding delays in cancer presentation, there was an observed reluctance for men compared with women with regards to seeking help for potential cancer-related symptoms [10]. Likewise, a UK study has suggested that, within a study sample of 3.8 million individuals, women were more likely to visit their general practitioner to report health-related issues compared with men [11]. The geographical disparities in ED visits (particularly for the North zone vs other provincial zones) are striking and are consistent with previously published data from our group suggesting challenges in access to routine healthcare within the North zone of the province [12]. This is probably related to low population to landmass ratio in this part of Alberta, longer driving time to elective ambulatory healthcare facilities, and, thus, more diagnoses of CRC were based on emergency visits rather than routine assessments through family physicians and specialists. This is also consistent with publicly available mortality data from the province of Alberta showing higher cancer mortality within the North zone of the province [13]. A higher likelihood of proximal (rather than distal) CRC is possibly related to the current standard of CRC screening in Canada, where sigmoidoscopy (rather than colonoscopy) is the endoscopic intervention of choice for screening of CRC [14] or it could be related to likelihood of noticing hematochezia, a change in the caliber of stool, tenesmus, etc., in distal tumors when compared with more proximal tumors [15]. As shown previously by our group, a sigmoidoscopy-based approach is likely to be associated with missed proximal cancers and; thus, more likelihood for these cancers to present emergently [16].
Distribution of the three emergency diagnoses of interest (anemia, abdominal pain and gastrointestinal hemorrhage) within subsets of CRC patients is also relevant. Notably, anemia and gastrointestinal hemorrhage were more likely among elderly individuals, while abdominal pain was more likely among younger individuals. Likewise, the fact that proximal tumors were more likely to be associated with a higher prevalence of the three diagnoses might be related to the higher possibility of ED visits among patients with proximal tumors versus those with distal tumors.
The current study has several limitations that need to be acknowledged. First, reported diagnoses in this study are based on recorded diagnoses by emergency physicians for each case. It is possible that for some CRC patients with a main presenting emergency diagnosis of (e.g., intestinal obstruction, gastrointestinal hemorrhage or nonspecific abdominal pain) that those patients have had other diagnoses (e.g., anemia) that was either not captured at the level of the ED or it was captured as a secondary diagnosis. Second, the retrospective nature of data collection might be associated with potential biases (e.g., related to missed information or unaccounted-for confounders) which might have impacted the veracity of the study analyses. Third, although we exercised our best efforts to ensure the veracity of the results of the current analysis, there is still a margin of error related to the coding process of ED diagnoses as well as coding process within the provincial cancer registry. Fourth, data for cancer diagnoses as well as ED visits are limited to healthcare facilities within Alberta. Therefore, if a person moves to or from Alberta (in the period between ED visit(s) and CRC diagnosis), this person’s encounter with ED would not be captured in the current study (as there is no centralized interprovincial registry of healthcare use among different Canadian jurisdictions). Fifth, as described in the methods section, this study is based on administrative databases rather than chart-level data mining. Thus, we cannot establish whether each of these emergency visits were the reason(s) behind cancer diagnosis in each case. These limitations need to be weighed against the strengths of the current study: most notably, the reliance on data collection within a single-payer public health system where central coding of all hospital encounters of all patients in the province is entertained.
Although each of anemia and gastrointestinal bleeding accounted for less than 10% of total emergency room diagnoses, these clinical scenarios are likely to be encountered by family physicians and highlight the importance of considering CRC as a potential underlying etiology for patients presenting with any of these presentations. Alberta is creating a CRC diagnosis pathway with a clinical checklist for iron deficiency anemia and rectal bleeding to help family physicians identify patients who may have an underlying diagnosis of CRC [17]. Referrals for endoscopy will be prioritized based on the clinical checklist with the aim to accelerate CRC diagnosis and treatment, hopefully resulting in a concomitant reduction in ED utilization.
Conclusion
Almost 40% of CRC patients visit the ED at least once within the 3 months preceding their diagnosis. Factors associated with frequent pre diagnosis emergency visits included female gender, higher comorbidity burden, advanced disease, proximal tumors and living within the North zone of Alberta (where there is limited access to specialist care). Further efforts are needed to reduce emergency diagnosis of CRC.
•
Linked provincial registries in Alberta, Canada, were accessed and patients with colorectal cancer (CRC) diagnosed between 2004 and 2018 were identified.
•
The National Ambulatory Care reporting system was used to identify patients who visited an emergency department (ED) within 3 months of a diagnosis of CRC.
•
Multivariable logistic regression analysis was used to identify factors associated with any ED visits as well as frequent (≥3) ED visits.
•
A total of 25,310 patients with CRC were included in the current study. These include 10,126 patients (40%) who had at least one visit to the ED in the 3 months before a diagnosis of CRC diagnosis and 613 patients (2.4%) who visited the ED multiple (≥3) times.
•
The following factors were associated with any visit to an ED: older age (OR: 1.010; 95% CI: 1.008–1.012), female gender (OR: 1.23; 95% CI: 1.16–1.30), higher comorbidity index (OR: 1.38; 95% CI: 1.35–1.41), metastatic disease (OR: 2.37; 95% CI: 2.23–2.53), proximal tumors (OR: 1.59; 95% CI: 1.50–1.68) and North zone (OR vs south zone: 1.75; 95% CI: 1.55–1.98).
Acknowledgments
The authors would like to thank the analytical teams at surveillance and reporting, Cancer Care Alberta for their help in data extraction.
O Abdel-Rahman: Advisory boards/public speaking: Roche, Eisai, Lilly, Bayer, Ipsen. PA Tang: Advisory boards from Roche Canada, Eisai Canada, Teva, Pfizer, Novartis Canada, BMS, Merck, Astrazeneca Canada.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
References
Papers of special note have been highlighted as: • of interest
1.
Canadian Cancer Society. Release notice - Canadian cancer statistics 2019. Health Promot. Chronic Dis. Prev. Can. 39(8–9), 255 (2019).
2.
Abdel-Rahman O. Patterns and trends of cancer screening in Canada: results from a contemporary National Survey. J. Natl Compr. Canc. Netw. 19(1), 68–76 (2021).
3.
Click B, Pinsky PF, Hickey T, Doroudi M, Schoen RE. Association of colonoscopy adenoma findings with long-term colorectal cancer incidence. JAMA 319(19), 2021–2031 (2018).
4.
Decker KM, Lambert P, Nugent Z, Biswanger N, Samadder J, Singh H. Time trends in the diagnosis of colorectal cancer with obstruction, perforation, and emergency admission after the introduction of population-based organized screening. JAMA Netw. Open 3(5), e205741 (2020).
• Reviews the patterns of emergency presentations of patients with colorectal cancer.
5.
Weithorn D, Arientyl V, Solsky I et al. Diagnosis setting and colorectal cancer outcomes: the impact of cancer diagnosis in the emergency department. J. Surg. Res. 255, 164–171 (2020).
6.
Ortiz-Ortiz KJ, Ríos-Motta R, Marín-Centeno H, Cruz-Correa MR, Ortiz AP. Emergency presentation and short-term survival among patients with colorectal cancer enrolled in the government health plan of Puerto Rico. Health Serv. Res. Manag. Epidemiol. 3, 2333392816646670 (2016).
7.
Esteva M, Ruidíaz M, Sánchez MA et al. Emergency presentation of colorectal patients in Spain. PLoS ONE 13(10), e0203556 (2018).
8.
Alberta Health Services. AHS map and zone overview. https://www.albertahealthservices.ca/assets/about/publications/ahs-ar-2019/zones.html
9.
Wang H, Gies N, Wong C, Sadowski D, Moysey B, Fedorak RN. Patients undergoing colorectal cancer screening underestimate their cancer risk and delay presentation for screening. Can. J. Gastroenterol. 26(7), 419–423 (2012).
10.
Smith LK, Pope C, Botha JL. Patients' help-seeking experiences and delay in cancer presentation: a qualitative synthesis. Lancet 366(9488), 825–831 (2005).
11.
Wang Y, Hunt K, Nazareth I, Freemantle N, Petersen I. Do men consult less than women? An analysis of routinely collected UK general practice data. BMJ Open 3(8), e003320 (2013).
12.
Abdel-Rahman O, Koski S, Mulder K. Real-world patterns of chemotherapy administration and attrition among patients with metastatic colorectal cancer. Int. J. Colorectal Dis. (2020) (Epub ahead of print).
13.
Cancer Care Alberta. The 2019 report on cancer statistics in Alberta (ROCSIA). https://public.tableau.com/profile/cancercontrol.ab#!/vizhome/The2019ReportonCancerStatisticsinAlberta/Highlights?publish=yes
14.
Canadian Task Force on Preventive Health Care. Recommendations on screening for colorectal cancer in primary care. Can. Med. Assoc. J. 188(5), 340–348 (2016).
15.
Odeny TA, Farha N, Hildebrandand H et al. Association between primary perioperative CEA ratio, tumor site, and overall survival in patients with colorectal cancer. J. Clin. Med. 9(12), 3848 (2020).
16.
Abdel-Rahman O, Cheung WY. Population-based assessment of the performance of sigmoidoscopy in the detection of colorectal cancer: implications for future screening recommendations. J. Gastrointest. Oncol. 10(2), 354–356 (2019).
17.
Alberta Health Services. Provincial colorectal cancer andlymphoma diagnosis pathways. https://www.albertahealthservices.ca/assets/about/scn/ahs-scn-cancer-colorectal-cancer-and-lymphoma-diagnosis-pathways.pdf#:∼:text=Provincial%20Colorectal%20Cancer%20and%20Lymphoma%20Diagnosis%20Pathways.%20While,process,%20and%20long%20periods%20of%20time%20in
Information & Authors
Information
Published In
Pages: 311 - 318
PubMed: 35189709
Copyright
© 2022 Future Medicine Ltd.
History
Received: 3 July 2021
Accepted: 17 December 2021
Published online: 22 February 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Patterns of emergency department visits preceding colorectal cancer diagnosis: a population-based study. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0163
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Christine Huynh, Prisca C. Obidike, Britney He, Christopher L. Cramer, Florence E. Turrentine, Charles M. Friel, Traci Hedrick, Sook C. Hoang, Influence of Patient Demographics, Symptoms, and Initial Provider Type on Timeliness of Rectal Cancer Diagnosis, Journal of Surgical Research, 10.1016/j.jss.2026.04.041, 324, (191-199), (2026).
- Ruth Swann, Georgios Lyratzopoulos, Greg Rubin, Lucy Elliss-Brookes, Sean McPhail, Predictors and consequences of different pathways to emergency diagnosis of cancer in England: Evidence from linked national audit and cancer registration data, Cancer Epidemiology, 10.1016/j.canep.2024.102607, 92, (102607), (2024).
- Anna Pujadas Botey, Ashley J. Watson, Paula J. Robson, Improving colorectal cancer in Alberta, Canada: a qualitative study of patients and close contacts’ perceptions on diagnosis following an emergency department presentation, BMC Health Services Research, 10.1186/s12913-024-11508-9, 24, 1, (2024).
- Omar Abdel-Rahman, Sunita Ghosh, Patterns of emergency department visits before diagnosis with digestive neuroendocrine neoplasms, International Journal of Colorectal Disease, 10.1007/s00384-023-04443-4, 38, 1, (2023).