Healthcare utilization and guideline-directed medical therapy in heart failure patients with reduced ejection fraction
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study examines the effect of guideline-directed medical therapy (GDMT) on healthcare utilization in patients with heart failure with reduced ejection fraction from Optum® Integrated File from 1 January 2007 to 30 June 2020. Materials & methods: Patients with both a beta blocker and either an ACE inhibitor (ACE-I), angiotensin receptor blocker (ARB) or angiotensin receptor neprilysin inhibitor were assigned to the GDMT cohort. All others were not on GDMT. Results: Estimated annual all cause hospitalizations and emergency department visits per 100 patients was 29% (80 vs 62 patients) and 26% higher (54 vs 43 patients; p < 0.0001) and annualized hospital days were longer (1.88 vs 1.64; p = 0.0020) for patients not on GDMT. Conclusion: In a real-world population, heart failure with reduced ejection fraction, patients not optimally managed on GDMT had higher annualized healthcare utilization when compared with patients on GDMT.
Cardiovascular disease is the leading cause of hospitalizations among older adults in the USA, and heart failure (HF) is the most common diagnosis [1]. An estimated one million hospitalizations per year are attributable to HF, with roughly half of those a result of HF with reduced ejection fraction (HFrEF). Presently the total cost of HF care, including direct and indirect costs, is estimated at US$43.6 billion. More than 70% of this is attributed to medical costs [2]. Rates of hospital readmission can exceed 20% within 30 days of discharge [3,4].
Guideline directed medical therapies (GDMT) as outlined by joint American College of Cardiology (ACC)/American Heart Association (AHA) guidelines have been shown to improve healthcare outcomes like survival and drastically reduce the number of subsequent health events [5]. They include at least one medicine from two categories, an angiotensin-converting enzyme inhibitor (ACE-I) or one of its alternatives, plus a beta blocker (BB). Frequently, mineralocorticoid receptor antagonists are also used as part of GDMT. Despite extensive evidence demonstrating the efficacy of recommended therapies, the majority of patients who experience HF are not treated with complete GDMT [6].
In this analysis, we examine the uptake and effect of GDMT among real-world HFrEF patients in the USA. The purpose of our study is to assess the impact of GDMT (and the lack thereof) on healthcare utilization.
Materials & methods
Data source
This study used data from the Optum® Integrated File, which contains data from both claims and electronic health records for patients across the USA [7]. To be included in this integrated file, patients must be enrolled in United Healthcare insurance and have at least one hospital encounter in the electronic health records data in the window of data availability (2007–Q3 2019). The combination of claims and clinical data provides a comprehensive view of a patient’s clinical interactions with the healthcare system. Optum data provides a continuum of treatment and cost information, such as medications by therapeutic area, provider notes with treatment rationale and cost by procedure and condition. For this analysis, we utilized the electronic health record data to assess ejection fraction since these measurements would be recorded in the hospital setting. We utilized the claims data to assess comorbidities, drug utilization and outcomes since this information is consistently contained in the longitudinal United Healthcare payer database versus the inconsistent information from the electronic health records portion of the integrated data.
Inclusion/exclusion criteria
Patients in the Optum Integrated File from 1 January 2007 through 30 June 2020 with a record of HFrEF were identified by a series of patient selection queries. HFrEF was measured by either: a record of an ejection fraction of ≤40% from the Humedica electronic health records portion of the Optum integrated database; or diagnosis of systolic HF via International Classification of Diseases (ICD) coding followed by at least one prescription fill for an angiotensin receptor neprilysin inhibitor (ARNI), which is almost exclusively used in patients with HFrEF, from the United Healthcare payer database. Patients were required to be 18 years of age or older and were excluded if they had Stage V chronic kidney disease (CKD) or end stage renal disease. Patients were required to have 6 months of continuous enrollment in the payer database both before and after their HFrEF index date to ensure information consistency in the payer database to capture comorbid conditions, HF drug utilization and other study variables. The initial 6 months after HFrEF diagnosis was considered a landmark period, during which drug regimens could be added and titrated according to recommendations [8]. Data used to perform this analysis was de-identified and accessed in compliance with the Health Insurance Portability and Accountability Act. As a retrospective analysis of a de-identified database, the research was exempt from Institutional Review Board (IRB) review under 45 Code of Federal Regulations (CFR) 46.101(b)(4).
Cohort definitions
Patients with a prescription record of both a BB and either ACE-I, angiotensin receptor blocker (ARB) or ARNI during the 6-month landmark period following their HFrEF diagnosis were considered to be on at least minimal GDMT and assigned to the GDMT cohort. Patients not meeting criteria were assigned to the not on GDMT cohort even if the they had a record of being on one of the two classes of medications. The GDMT cohort was further classified by patients having a record of filling prescriptions in both classes (BB and ACEI/ARB/ARNI) concurrently within the 6-month landmark period, which was labeled GDMT STRICT in the analysis. For GDMT STRICT, a patient had to have at least 1 day of overlapping prescriptions with up to a 7 day gap in both classes.
Outcomes of interest
Outcomes of interest for this analysis included the following healthcare utilization end points, on an annualized basis: all cause hospitalizations, cardiovascular (CV) related hospitalizations, hospital days, emergency department (ED) visits, outpatient visits and office visits. All outcomes were measured up to 2 years from the end of the landmark period (6 months after a patient’s diagnosis of HFrEF in which drug regimens were assessed).
Covariates of interest
The covariates for this analysis included patient demographics and comorbidities. Demographics included age, sex, race and region. Comorbidities of interest were identified using diagnosis codes that appeared in the 6-month period before a patient’s index diagnosis of HFrEF. Since patients with concomitant diseases may be contraindicated for certain GDMT therapies, patients with a record of the following comorbid conditions prior to their HFrEF diagnosis were considered: atrial fibrillation, hypertension, coronary artery disease and chronic kidney disease. Finally, although diuretics are not part of the strict definition of GDMT, patients with a record of loop diuretic usage during the landmark period were also followed.
Statistical analysis
All cohorts (GDMT, GDMT STRICT and not on GDMT) were described by patient characteristics and specific comorbid conditions. Descriptive analytics were presented as mean and standard deviation for continuous variables or count and percentage for categorical variables. All healthcare utilization outcomes were estimated for the GDMT versus the not on GDMT cohort using general linear models with multiple data distribution considerations. All models were adjusted for patient demographics with the following chronic conditions: atrial fibrillation, hypertension, coronary artery disease, chronic kidney disease and record of diuretic use. All utilization models were repeated for the GDMT STRICT versus not on GDMT cohort. Model results are reported as least square mean estimates and p-values.
Results
A total of 135,808 patients from 2007 through June of 2020 in Optum’s integrated database were identified as HFrEF by having either a record of an ejection fraction ≤40% (n = 126,482, 93%) or a diagnosis of systolic HF by ICD 9/10 coding and a record of at least one medication fill for an ARNI following the diagnosis of systolic HF (n = 9326, 7%; Figure 1). Patients were required to be adults, 18 years of age or older at the time of their HFrEF diagnosis, which reduced the sample to 135,090. In order to measure comorbidities prior to HFrEF diagnosis and assess pharmacologic response after, 6 months of continuous enrollment both before and after HFrEF diagnosis we required in Optum’s claims portion of their integrated database. This significantly reduced our sample size to less than 20%. After all inclusion criteria were applied, there were 12,575 patients in the GDMT cohort (69%) and 5601 patients in the not on GDMT cohort (31%). When the GDMT cohort was further restricted to having concurrent prescription drug usage, the GDMT cohort of 12,575 was reduced to 10,250 patients that made up the GDMT STRICT cohort.
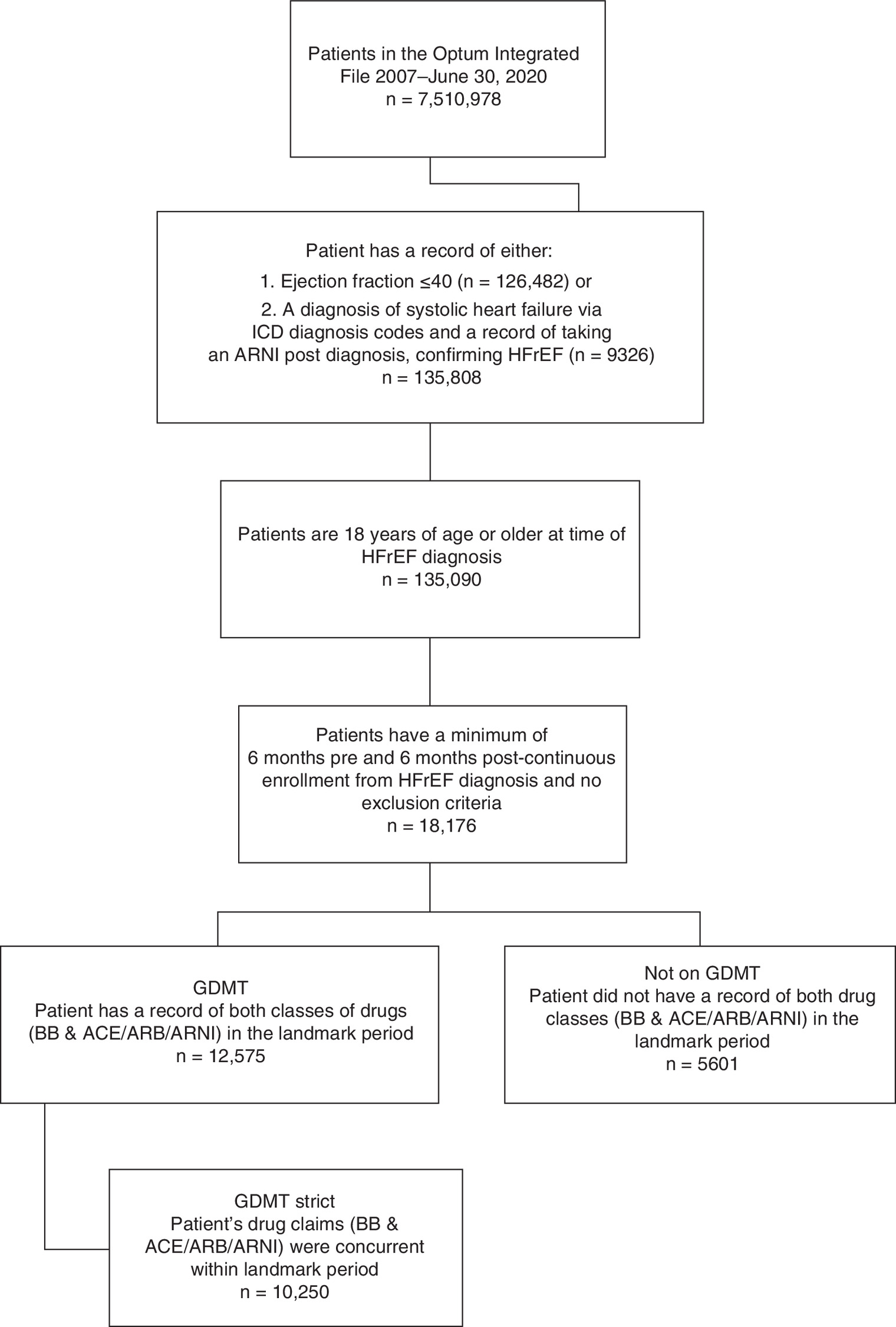
Figure 1. Patient attrition diagram.
Patients in the Optum database were selected for inclusion in the analysis using the steps below. Eligible HFrEF patients were then classified as GDMT (medications from at least two classes), GDMT STRICT (concurrent medications from at least two classes) and not on GDMT.
ACE-I: Angiotensin-converting enzyme inhibitor; ARB: Angiotensin receptor blocker; ARNI: Angiotensin receptor neprilysin inhibitor; BB: Beta blocker; GDMT: Guideline-directed medical therapy; HFrEF: Heart failure with reduced ejection fraction.
Patient demographics (age, sex, region, race and insurance type) and presence of atrial fibrillation, hypertension, coronary artery disease, chronic kidney disease and diuretic usage during the landmark period are shown for the three cohorts in Table 1. Demographic variables were fairly similar across the three cohorts with (average ages from 69–70). The majority of patients were male (over 60%), Caucasian (over 80%), from the Midwest (40% or more) and insured with Medicare (67–70%). The mean Elixhauser comorbidity score was slightly higher for the GDMT cohorts (6.3 for GDMT and GDMT STRICT compared with 5.5 for not on GDMT). When comparing GDMT to not on GDMT, there were higher rates of hypertension (41.7 vs 29.8%), coronary artery disease (73.2 vs 58.8%) and diuretic use during the landmark period (73.8 vs 51.7%) in the GDMT cohort. However, rates of atrial fibrillation (39.2%) and chronic kidney disease (25.8 vs 26.8%) were similar across groups.
| Characteristics | GDMT | GDMT STRICT | Not on GDMT |
|---|---|---|---|
| Number of patients | 12,575 | 10,250 | 5601 |
| Age Mean (SD) | 68.75 (12.26) | 68.35 (12.32) | 70.11 (13.35) |
| Gender | |||
| – Female | 4286 (34.08%) | 3529 (34.43%) | 2172 (38.78%) |
| – Male | 8284 (65.88%) | 6718 (65.54%) | 3427 (61.19%) |
| Race | |||
| – Asian | 131 (1.04%) | 115 (1.12%) | 61 (1.09%) |
| – Black | 1471 (11.70%) | 1243 (12.13%) | 441 (7.87%) |
| – Caucasian | 10,279 (81.74%) | 8289 (80.87%) | 4851 (86.61%) |
| – Unknown | 694 (5.52%) | 603 (5.88%) | 248 (4.43%) |
| Region | |||
| – Midwest | 5182 (41.21%) | 4052 (39.53%) | 2472 (44.13%) |
| – Northeast | 2090 (16.62%) | 1768 (17.25%) | 848 (15.14%) |
| – South | 3321 (26.41%) | 2824 (27.55%) | 1240 (22.14%) |
| – West | 1641 (13.05%) | 1342 (13.09%) | 851 (15.19%) |
| – Unknown | 341 (2.71%) | 264 (2.58%) | 190 (3.39%) |
| Payor | |||
| – Commercial | 3684 (29.30%) | 3011 (29.38%) | 1538 (27.46%) |
| – Medicaid | 376 (2.99%) | 340 (3.32%) | 156 (2.79%) |
| – Medicare | 8515 (67.71%) | 6899 (67.31%) | 3907 (69.76%) |
| Comorbid conditions of interest | |||
| Atrial fibrillation in pre period | 4935 (39.24%) | 3905 (38.10%) | 2198 (39.24%) |
| Complicated hypertension in pre period | 5249 (41.74%) | 4231 (41.28%) | 1671 (29.83%) |
| Coronary artery disease in pre period | 9194 (73.11%) | 7484 (73.01%) | 3295 (58.83%) |
| Chronic kidney disease in pre period | 3249 (25.84%) | 2547 (24.85%) | 1501 (26.80%) |
| Concurrent diuretics in landmark period | 9275 (73.76%) | 7520 (73.37%) | 2895 (51.69%) |
GDMT STRICT = Guideline-directed medical therapy with concurrent medications.
Pre period = 6 months prior to HFrEF diagnosis.
Landmark period = 6 months following HFrEF diagnosis.
GDMT: Guideline-directed medical therapy; HFrEF: Heart failure with reduced ejection fraction; SD: Standard deviation.
Figure 2 displays the estimated annualized number of all cause hospitalizations, CV related hospitalizations and ED visits per 100 patients. Patients not on GDMT had 29% (80 vs 62 patients) higher annual all cause hospitalizations (p < 0.0001), 21% (29 vs 24 patients) higher annual CV related hospitalizations (p < 0.0079) and 26% (54 vs 43 patients) higher annual ED visits (p < 0.0001) than patients not on GDMT. Table 2 report the least square mean estimates based on multivariable models for number of hospital days, outpatient visits and office visits. All outcomes are annualized and were assessed up to 2 years post landmark period. Patients not on GDMT have statistically significant higher annual hospital days (1.88 vs 1.64; p = 0.0020) than patients on GDMT. There was no difference in utilization of care, specifically in the form of outpatient or office visits. When modeling the stricter GDMT cohort (GDMT+), where patients have a record of concurrent drug therapy, versus not on GDMT, similar results were found.

Figure 2. Multivariable modeling results estimated annualized number of hospitalizations – all cause, cardiovascular related and emergency department visits per 100 patients GDMT versus not on GDMT.
When GDMT STRICT is compared with not GDMT – the results are significant with 30% higher annual all cause, 17% CV related hospitalizations and 26% higher annual ER visits. GDMT definitions: Patients with a prescription record of both a beta blocker and either ACE-I, ARB or ARNI during the 6-month landmark period following their heart failure with reduced ejection fraction diagnosis were considered to be on at least minimal GDMT and assigned to the GDMT cohort. Patients not meeting this criterion, regardless of whether they had a record of one class of medication or none, were assigned to the not GDMT (not on GDMT) cohort. The GDMT cohort was further classified by those patients having a record of prescription fills for both classes of medications (beta blocker and ACE I/ARB/ARNI) concurrently within the 6-month landmark period; this subset was labeled GDMT Strict (GDMT STRICT) in the analysis. All models adjust for: patient demographics, comorbid conditions and diuretic usage.
CV: Cardiovascular; GDMT: Guideline-directed medical therapy.
| Model results LS Mean estimates | GDMT | Not on GDMT | p-value |
|---|---|---|---|
| – Hospital days | 1.64 | 1.88 | 0.0020 |
| – Outpatient visits | 7.0 | 7.4 | 0.0765 |
| – Office visits | 10.9 | 10.8 | 0.5864 |
| Model results LS Mean estimates | GDMT STRICT | Not on GDMT | p-value |
| – Hospital days | 1.59 | 1.86 | 0.0007 |
| – Outpatient visits | 6.9 | 7.3 | 0.1313 |
| – Office visits | 11.0 | 10.7 | 0.2595 |
All models adjust for: patient demographics, comorbid conditions and diuretic usage.
LS: Least squares mean.
Discussion
This retrospective analysis found that patients treated with GDMT had significantly lower healthcare utilization compared with patients who did not receive GDMT, with outcomes diverging even further in the comparison of GDMT STRICT versus not on GDMT. Patients treated with GDMT spent fewer days in the hospital (24%) and required fewer emergency room visits (11%). They also had lower rates of all-cause (18%) and CV (5%), hospitalization (18%) compared with not on GDMT. This is consistent with recent publications suggesting improvements among all-cause and CV hospitalizations in patients receiving more aggressive medical therapy [9,10]. A 2014 study found patients treated with an ARNI in place of enalapril showed a 21% decreased risk of being hospitalized for HF [11]. Similar results toward healthcare outcomes are seen for beta blockers via OPTIMIZE-HF and other large trials focused on carvedilol [12–15]. While separate components of GDMT have been studied for their impact on healthcare utilization, this study is unique in assessing the full picture of annualized healthcare utilization in real-world patients on GDMT compared with a not on GDMT cohort.
Several studies have highlighted the association between medication changes and hospitalization, suggesting acute inpatient care may be a critical window for pharmacologic adjustments. Hospitalization has been shown in multiple publications as a crucial time in patient care to initiate, discontinue or titrate GDMT [16–18]. Evidence suggests that HF hospitalization marks a turning point in the progression of the disease after which survival rates drop sharply, providing not just a sense of urgency but a clear indicator that a patient’s treatment regimen must be continuously re-evaluated [19]. Data from CHAMP-HF shows that only about 1% of patients are treated with all three classes of GDMT for systolic HF at target doses. This finding was also in the setting of a clinical trial with broad inclusion criteria, suggesting that significant room for improvement exists with getting patients to achieve GDMT and thus improving outcomes as described [17–19].
HF is already a leading, if not the leading driver of healthcare utilization and healthcare expenditure. As the population ages and survival rates increase, this economic burden will only increase with time [2]. The failure to optimize HF management has clear consequences despite the reasons being less obvious. A better understanding of systemic failures to treat HF in line with guideline recommendations, the costs associated with this and an understanding of patient barriers (comorbidities, drug tolerability, etc.) is needed to improve the standard of care and create more opportunities for intervention.
Strengths
The major strength of this study is that it characterizes HF by ejection fraction, which many large retrospective studies cannot due to the limited types of data available in an administrative claims database. In addition, there is limited data on the association between GDMT and healthcare utilization costs. Much of the current research to date has cohorts stratified by ejection fraction, type of medication, gender or a given comorbidity. This study uses a cohort of nonoptimally treated patients to more meaningfully examine the direct relationship between GDMT and utilization outcomes such as days spent in the hospital. In this analysis, claims data are combined with electronic health records and adjustments were made for patient characteristics known to affect prognosis and; therefore, intensity of care. The broad selection criteria employed in the use of a large dataset also helped preserve generalizability.
Limitations
As with all studies that rely on automated sources of data, it is possible that parameters such as billing codes could be biased and proxies could fail to capture certain factors difficult to ascertain from the available clinical data. Our use of a proxy (prescription of ARNI) for reduced EF as an alternative to echocardiogram may skew our cohorts toward a higher percentage of patients on GDMT, since ARNI is one qualifying component of the drug regimen. However, 94.2% of our HFrEF population of interest had a record of an echocardiogram result of an ejection fraction of ≤40% and only a small percentage (7%) relied on ICD coding and a record of taking an ARNI to meet inclusion criteria. We were unable to adjust for vital signs, laboratory data, region and other potential confounding measures due to the lack of clinical parameters in this real world data source. Consequently, we were unable to differentiate patients that are not eligible for GDMT (due to heart rate, blood pressure, renal function, etc.), also recognizing that inability to tolerate GDMT portends worse outcomes. However, we adjusted for baseline differences in many comorbid conditions that may deem patients ineligible for GDMT, for example, chronic kidney disease.
Finally, a continuous enrollment both 6 months prior to and after HFrEF diagnosis was needed for inclusion. This stringent criterion was necessary to ensure data collection on baseline comorbidities and medication regimens, but may induce bias toward healthier patients (i.e., those with early death during the first 6 months would not be included in the analysis). We expect that the relationship between GDMT and healthcare utilization should be preserved, as the same continuous enrollment periods were applied to each cohort. Patient adherence may also be inadequately captured by the use of prescription fills to determine medication status, as not everyone who fills their prescription is taking the drugs as intended. We treated cohort status as static during the outcome period; although, it is possible that patients could have changed cohorts by altering their drug regimen more than 6 months after their HFrEF index date to either be on GDMT or not on GDMT. This cohort crossover could have biased our results. Given the patients represented in our analysis, results are generalizable only to the commercially insured patient population.
Conclusion
In a real-world population setting, a sizeable amount of HFrEF patients (31–44%) were not optimally managed on GDMT. The absence of GDMT was independently associated with increased annual healthcare utilization, in particular annualized hospitalizations, hospital days and emergency room visits. There are a variety of barriers to GDMT for HF patients, especially given the high rate of comorbidities for this demographic, but improving clinical implementation of combined pharmacologic therapies and augmenting this with surgery and novel devices is an effective path for improving health outcomes.
•
Heart failure (HF) is a leading cause of hospitalizations in the USA, and is characterized by ejection fraction.
•
Guideline directed medical therapies (GDMT) for HF as defined by ACC/AHA guidelines include one medication from at least two classes, either an angiotensin-converting enzyme inhibitor (ACE-I) or one of its alternatives, plus a beta blocker. Mineralocorticoid receptor antagonists are also a common component of GDMT.
•
Despite extensive evidence supporting the efficacy of these interventions, large gaps in clinical implementation persist and few patients are maintained on the recommended regimens in full.
•
In this study we characterize the uptake of GDMT in HF patients with reduced ejection fraction and assess their rates of healthcare utilization.
•
Using real-world data from the Optum® Integrated File, patients 18 and over with HF with reduced ejection fraction were assigned to the (GDMT) cohort if they were prescribed both a beta blocker and either an ACE-I, ARB or ARNI during the post period. The rest were assigned to the (not on GDMT) cohort.
•
The outcomes used to measure healthcare utilization were estimated annual number of all cause hospitalizations and emergency department visits, annualized hospital days and outpatient visits.
•
Covariates of interest included patient demographics and comorbidities such as atrial fibrillation and hypertension.
•
Patients not on GDMT were found to have 26% higher emergency department visits, 21% higher cardiovascular-related hospitalizations and 29% higher all cause hospitalizations, annually.
Author contributions
All authors contributed significantly to the work and meet the criteria for authorship; all have read and approved the manuscript.
Financial & competing interests disclosure
Relevant industry relationships and financial interests are as follows: CM Barker, DP Cork, PA Mc Cullough, HS Mehta, M Ryan and C Gunnarsson have consulting relationships with Edwards Lifesciences. CM Barker is an advisory board member for Medtronic and Boston Scientific. DP Cork has a consulting relationship with Abbott Laboratories and participates in a speaker’s bureau for Boston Scientific. HS Mehta has a consulting relationship with Abbott Laboratories, Boston Scientific and participates in a speaker’s bureau for Actelion Pharmaceuticals, Bayer Healthcare Pharmaceuticals and Bristol-Myers Squibb Company. JV Houten and S Mollenkopf are employees of Edwards Lifesciences, the study sponsor. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
All data used to perform this analysis were de-identified and accessed in compliance with the Health Insurance Portability and Accountability Act. As a retrospective analysis of a de-identified database, the research was exempt from IRB review under 45 CFR 46.101(b)(4). This manuscript has not been published previously and is not currently under consideration for publication by any other journal.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Centers for Disease Control and Prevention – National Center for Health Statistics. Underlying Cause of Death 1999–2016 on CDC WONDER online database, released December 2017. Data Are from the Multiple Cause of Death Files, 1999–2016, as Compiled from Data Provided by the 57 Vital Statistics Jurisdictions through the Vital Statistics Cooperative Program.(2017). http://wonder.cdc.gov/ucd-icd10.html
2.
Urbich M, Globe G, Pantiri K et al. A systematic review of medical costs associated with heart failure in the USA (2014–2020). Pharmacoeconomics 38(11), 1219–1236 (2020).
• Provides detailed breakdowns of various heart failure (HF)-related costs to better examine the economic burden of the condition, concluding that the key driver of costs is hospitalization.
3.
Reddy YNV, Borlaug BA. Readmissions in heart failure: it's more than just the medicine. Mayo Clin. Proc. 94(10), 1919–1921 (2019).
4.
Ziaeian B, Fonarow GC. The prevention of hospital readmissions in heart failure. Prog. Cardiovasc. Dis. 58(4), 379–385 (2016).
5.
Yancy CW, Jessup M, Bozkurt B et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J. Am. Coll. Cardiol. 62(16), e147–239 (2013).
6.
Deschaseaux C, McSharry M, Hudson E, Agrawal R, Turner SJ. Treatment initiation patterns, modifications, and medication adherence among newly diagnosed heart failure patients: a retrospective claims database analysis. J. Manag. Care Spec. Pharm. 22(5), 561–571 (2016).
• An examination of treatment patterns for newly diagnosed HF patients in the USA, looking at modifications, hospitalizations and treatment adherence.
7.
Optum Inc., Clinformatics® Data Mart (2017). www.optum.com/content/dam/optum3/optum/en/resources/white-papers/clinformatics-data-mart.pdf
8.
Naegele M, Flammer AJ, Enseleit F, Ruschitzka F. Medical therapy of heart failure with reduced ejection fraction: current evidence and new developments. Swiss Med. Wkly 146, w14295 (2016).
9.
Sanam K, Bhatia V, Bajaj NS et al. Renin-angiotensin system inhibition and lower 30-day all-cause readmission in Medicare beneficiaries with heart failure. Am. J. Med. 129(10), 1067–1073 (2016).
10.
Gilstrap LG, Fonarow GC, Desai AS et al. Initiation, continuation, or withdrawal of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers and outcomes in patients hospitalized with heart failure with reduced ejection fraction. J. Am. Heart Assoc. 6(2), e004675 (2017).
11.
McMurray JJ, Packer M, Desai AS et al. PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 371(11), 993–1004 (2014).
12.
Hernandez AF, Hammill BG, O'Connor CM, Schulman KA, Curtis LH, Fonarow GC. Clinical effectiveness of beta-blockers in heart failure: findings from the OPTIMIZE-HF (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure) registry. J. Am. Coll. Cardiol. 53(2), 184–192 (2009).
• A combination of medicare claims data with records from the OPTIMIZE-HF trial that evaluates the effectiveness of beta blockers.
13.
Fonarow GC, Abraham WT, Albert NM et al. Influence of beta-blocker continuation or withdrawal on outcomes in patients hospitalized with heart failure: findings from the OPTIMIZE-HF program. J. Am. Coll. Cardiol. 52(3), 190–199 (2008).
14.
Krum H, Roecker EB, Mohacsi P et al. Effects of initiating carvedilol in patients with severe chronic heart failure: results from the COPERNICUS study. JAMA 289(6), 712–8 (2003).
15.
Packer M, Coats AJ, Fowler MB et al. Carvedilol prospective randomized cumulative survival study group. Effect of carvedilol on survival in severe chronic heart failure. N. Engl. J. Med. 344(22), 1651–1658 (2001).
16.
Srivastava PK, DeVore AD, Hellkamp AS et al. Heart failure hospitalization and guideline-directed prescribing patterns among heart failure with reduced ejection fraction patients. JACC Heart Fail. 9(1), 28–38 (2021).
• An analysis of the relationship between guideline directed medical therapies changes and hospitalization.
17.
Greene SJ, Butler J, Albert NM et al. Medical therapy for heart failure with reduced ejection fraction: the CHAMP-HF registry. J. Am. Coll. Cardiol. 72(4), 351–366 (2018).
•• The CHAMP-HF (Change the Management of Patients with HF) registry is a study of HF with reduced ejection fraction outpatients that analyzed their treatment patterns and found only 1% of eligible patients were receiving target doses of the three indicated medication classes simultaneously.
18.
Bhagat AA, Greene SJ, Vaduganathan M et al. Initiation, continuation, switching, and withdrawal of heart failure medical therapies during hospitalization. JACC Heart Fail. 7(1), 1–12 (2019).
19.
Steinberg BA, Fang JC. Long-term outcomes of acute heart failure: where are we now? J. Am. Coll. Cardiol. 70(20), 2487–2489 (2017).
• An overview of various clinical trials and a look at the role of ejection fraction and hospitalization in treatment trajectories.
Information & Authors
Information
Published In
Pages: 1055 - 1063
PubMed: 34225473
Copyright
© 2021 Joanna Van Houten. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 20 May 2021
Accepted: 18 June 2021
Published online: 6 July 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Healthcare utilization and guideline-directed medical therapy in heart failure patients with reduced ejection fraction. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0118
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Joshua A. Jacobs, Tom Greene, Megan E. Vanneman, Jacob Kean, Spencer J. Carter, Kevin S. Shah, Ambarish Pandey, Catherine G. Derington, Alexander R. Zheutlin, James Fang, Josef Stehlik, Gregg C. Fonarow, Adam P. Bress, Time to Quadruple Therapy After Initial Diagnosis of Heart Failure With Reduced Ejection Fraction, JAMA Cardiology, 10.1001/jamacardio.2026.0375, 11, 6, (506), (2026).
- Radha Dhingra, Hanzhang Xu, Bradley G. Hammill, Scott M. Lynch, Jessica S. West, Michael D. Green, Eric D. Peterson, Lesley H. Curtis, Matthew E. Dupre, Association Between Socioeconomic Disadvantage and Risks of Early and Recurrent Admissions Among Patients With Newly Diagnosed Heart Failure, Circulation: Cardiovascular Quality and Outcomes, 10.1161/CIRCOUTCOMES.124.011141, 17, 12, (2024).