Outcomes of patients with nonmetastatic gastric adenocarcinoma according to perioperative treatment strategy: a real-world, population-based study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the survival outcomes of patients with nonmetastatic gastric cancer according to the type of perioperative treatment strategy used (surgery-only, adjuvant chemo-radiotherapy, adjuvant chemotherapy, perioperative chemotherapy) in a population-based setting. Materials & methods: Surveillance, Epidemiology and End Results research-plus database was explored, and patients with nonmetastatic gastric cancer who were treated with an oncologic surgery were reviewed. Multivariable Cox regression analysis was used to examine the impact of treatment strategy on overall and cancer-specific survival. Results: A total of 11,526 patients were found to be eligible and they were included in the current analysis. Looking at the percentages of different treatment strategies throughout the study years (2006–2017), the use of the following strategies increased: adjuvant chemotherapy (20.1 vs 10.6%), and perioperative chemotherapy (21.3 vs 0.5%); while the use of the following strategies decreased: surgery only (36.2 vs 58.2%), and adjuvant chemo-radiotherapy (22.4 vs 30.6%). Using multivariable Cox regression analysis, the following factors were associated with worse overall survival: older age (hazard [HR]: 1.021; 95% CI: 1.018–1.023), males (HR: 1.09; 95% CI: 1.04–1.14), Black race (HR: 1.11; 95% CI: 1.04–1.19), cardia subsite (HR: 1.09; 95% CI: 1.02–1.17), grade 3–4 (HR:1.32; 95% CI: 1.25–1.40), diffuse histology (HR: 1.46; 95% CI: 1.35–1.58), clinically node positive (HR:1.43; 95% CI: 1.34–1.53), total gastrectomy (HR: 1.20; 95% CI: 1.13–1.28), and surgery-only approach (HR: 1.65; 95% CI: 1.55–1.75). Conclusion: Among patients with localized gastric cancer, patients who were treated with surgery-only, and to a less extent, patients who were treated with surgery followed by adjuvant chemotherapy have worse survival outcomes; while those treated with perioperative chemotherapy have the best survival outcomes.
Gastric cancer represents a global health problem with many patients presenting in an incurable advanced stage [1,2]. Even among patients with nonmetastatic disease, there is a high chance of subsequent progression to metastatic disease [3,4]. Therefore, greater emphasis has been put on perioperative treatment(s) in the hope that it would decrease the chances of cancer recurrence.
Over the past two decades, many perioperative treatment strategies have been examined for the management of patients with nonmetastatic gastric cancer [5–7]. These include adjuvant chemoradiation, adjuvant chemotherapy and perioperative chemotherapy [8]. These strategies have been shown to have superior efficacy compared with surgery alone, however, direct comparison between these strategies, in a real-world setting has been lacking. There is thus a need to examine the differences in outcomes of those patients in a population-based context.
Surveillance, Epidemiology and End Results (SEER) database is considered one of the most credible sources of real-world datasets, as it covers approximately 28% of cancer patients diagnosed in the United States, with rigorous data collection and quality assurance procedures. Therefore, it was used in the current study.
Objective
To assess the survival outcomes of patients with nonmetastatic gastric cancer according to the type of perioperative treatment strategy used.
Materials & methods
Data sources
The current study is based on SEER-18 research-plus database (2000–2017), with survival follow-up up to December 2017 [9]. This specialized database has been selected for the current study as it contains information about the sequencing of chemotherapy/radiation therapy with surgical resection.
Inclusion criteria for this study included diagnosis with gastric adenocarcinoma, no evidence of metastatic disease (M0 as per AJCC 6th and 7th versions), and treatment with an oncologic surgery. Records of second primary gastric cancer (after a previous diagnosis of gastric cancer) were excluded. Patients with upfront surgery who have a diagnosis of TX-1/NX-0/M0 were excluded (as those patients are not routinely offered perioperative treatment).
Data collection
The following data were collected from each patient, age at diagnosis, race, sex, subsite (cardia vs noncardia), grade (according to 4-tiered grading system), histology (diffuse, intestinal, not otherwise specified or others), clinical N stage, type of surgery, and treatment strategy (including surgery-only, surgery followed by adjuvant chemo/radiotherapy, surgery followed by adjuvant chemotherapy, and perioperative chemotherapy).
The definition of perioperative chemotherapy was limited to patients who received chemotherapy before and after surgery (and patients who received any additional perioperative radiotherapy were excluded). The reason for this approach is to avoid any potential confounding effect of perioperative radiotherapy on survival outcomes. Other treatment scenarios (e.g., preoperative chemo-[radiation] without postoperative chemotherapy) were not included in the current study. The reason for this approach (i.e., exclusion of patients who received preoperative but not postoperative chemotherapy) was the inability to determine if the absence of postoperative chemotherapy was a preplanned strategy from the very beginning or it was because of lack of fitness for postoperative chemotherapy among those patients.
The following histological subtypes were pooled under the diffuse histological category (linitis plastica and signet ring carcinoma), and tubular histology was pooled under the intestinal histology category. Information about clinical T stage was not available. Pathological T and N stages were not considered in the study as some patients have received preoperative treatment, thus, pathological stage could have been affected in those cases by the preoperative treatment received.
End points of the current study included overall survival (defined as the time from cancer diagnosis till death of any reason), and cancer-specific survival (defined as the time from cancer diagnosis till death ascribed to the gastric cancer diagnosis).
Statistical analysis
Chi-Squared testing and independent t-test were initially used to compare baseline characteristics between individuals who were treated with each of the studied 4 strategies. Kaplan–Meier analysis and log-rank estimates were used to examine the impact of treatment strategy on overall survival. Multivariable Cox regression analysis was then done to explore factors associated with overall and cancer-specific survival. Factors included in each model included age at diagnosis, race, sex, subsite, grade, histology, clinical N stage, type of surgery and treatment strategy. As a sensitivity analysis, these models were repeated incorporating only patients without unknown values. All statistical analyses were conducted through SPSS software (version 23.00, IBM, NY, USA).
Results
Patients’ characteristics
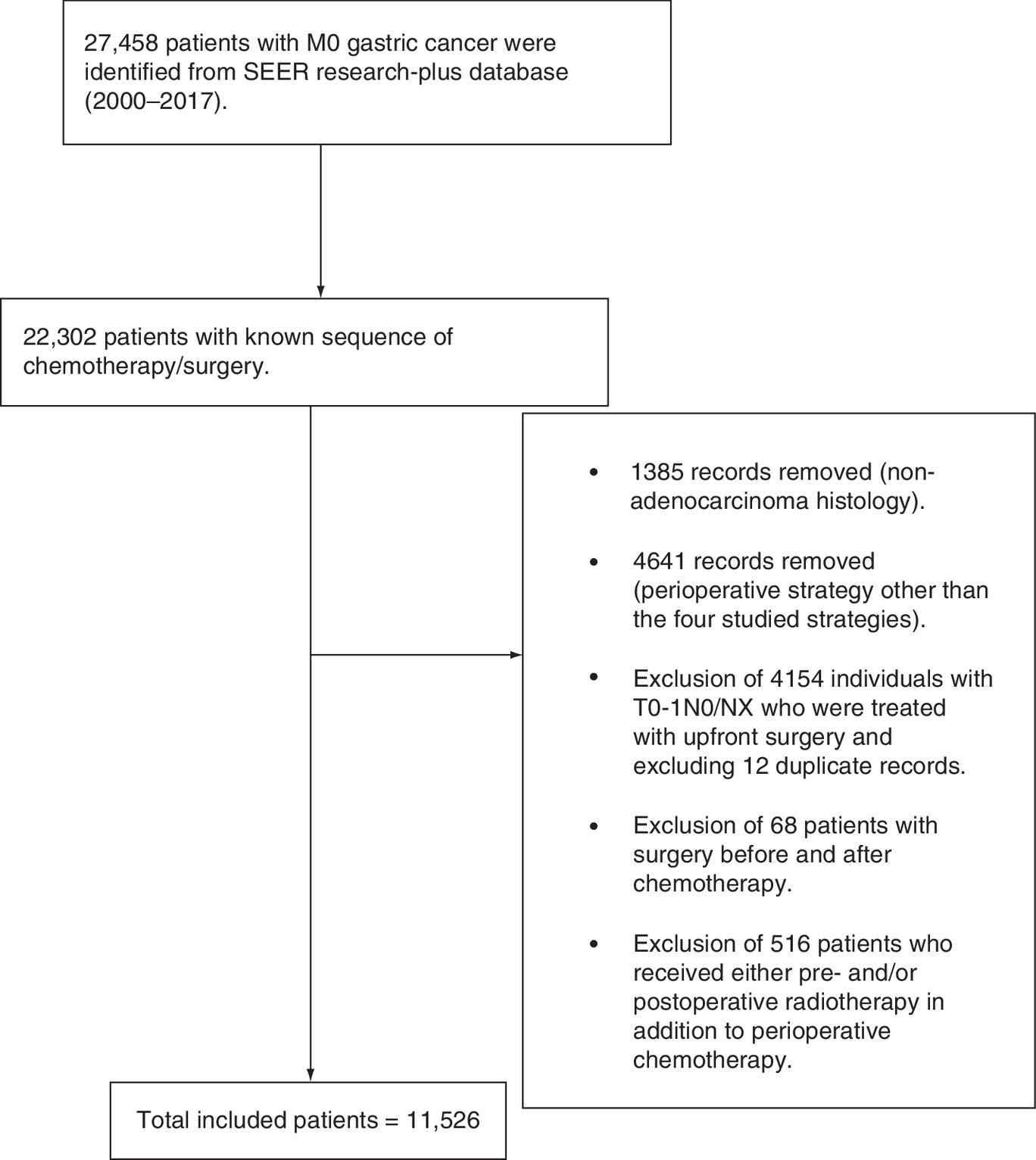
Figure 1 summarizes the patient selection process. A total of 11,526 patients were found to be eligible and they were included in the current analysis. These included 5407 patients who were treated with surgery only, 3582 patients who were treated with surgery followed by adjuvant chemo/radiotherapy, 1705 patients who were treated with surgery followed by adjuvant chemotherapy, and 832 patients who were treated with pre-and postoperative chemotherapy in addition to surgery. Comparing the four groups together, individuals treated with perioperative chemotherapy were likely to be younger (p < 0.001), males (p = 0.001), White (p < 0.001), have cardia primary site (p < 0.001), clinically node-positive (p < 0.001), and have total gastrectomy as the type of surgery (p < 0.001) (Table 1). Although the examined SEER registry covers the period from 2000 to 2017, eligible patients for the current study were diagnosed only from 2006 to 2017.
| Parameter | Surgery (5407 patients) | Adjuvant chemo/RT (3582 patients) | Adjuvant chemotherapy (1705 patients) | Perioperative chemotherapy (832 patients) | p-value |
|---|---|---|---|---|---|
| Age (mean, SD)† | 73.21; 11.10 | 62.40; 12.14 | 64.30; 12.56 | 59.94; 12.24 | <0.001 |
| Sex – Males – Females | 3192 (59%) 2215 (41%) | 2217 (61.9%) 1365 (38.1%) | 996 (58.4%) 709 (41.6%) | 539 (64.8%) 293 (35.2%) | 0.001 |
| Race – White – Black – Asian/Pacific Islander – American Indian – Unknown | 3520 (65.1%) 772 (14.3%) 1067 (19.7%) 34 (0.6%) 14 (0.3%) | 2117 (59.1%) 634 (17.7%) 803 (22.4%) 15 (0.4%) 13 (0.4%) | 1038 (60.9%) 262 (15.4%) 371 (21.8%) 23 (1.3%) 11 (0.6%) | 527 (63.3%) 111 (13.3%) 180 (21.6%) 9 (1.1%) 5 (0.6%) | <0.001 |
| Subsite – Cardia – Specified noncardia site – Overlapping lesion | 871 (16.1%) 3602 (66.6%) 934 (17.3%) | 511 (14.3%) 2504 (69.9%) 567 (15.8%) | 242 (14.2%) 1104 (64.8%) 359 (21.1%) | 175 (21%) 516 (62%) 141 (16.9%) | <0.001 |
| Grade – Grade 1–2 – Grade 3–4 – Unknown | 1765 (32.6%) 3495 (64.6%) 147 (2.8%) | 853 (23.8%) 2647 (73.9%) 82 (2.3%) | 389 (22.8%) 1263 (74.1%) 53 (3.1%) | 174 (20.9%) 604 (72.6%) 54 (6.5%) | <0.001 |
| Histology – Diffuse – Intestinal – Adenocarcinoma, NOS – Others | 1233 (22.8%) 1131 (20.9%) 2554 (47.3%) 489 (9%) | 1243 (34.7%) 621 (17.3%) 1428 (39.9%) 290 (8.1%) | 602 (35.3%) 313 (18.4%) 655 (38.4%) 135 (7.9%) | 318 (38.2%) 130 (15.6%) 331 (39.8%) 53 (6.4%) | <0.001 |
| Clinical N stage – N0 – N+ – Unknown | 3337 (61.7%) 576 (10.7%) 1494 (27.6%) | 2152 (60.1%) 601 (16.8%) 829 (23.1%) | 1061 (62.2%) 303 (17.8%) 341 (20%) | 377 (45.3%) 414 (49.8%) 41 (4.9%) | <0.001 |
| Type of surgery – Partial gastrectomy – Total/near total gastrectomy ‑ Gastrectomy with resection of adjacent organs – Gastrectomy, NOS | 3770 (69.7%) 879 (16.3%) 590 (10.9%) 168 (3.1%) | 2344 (65.4%) 650 (18.1%) 479 (13.4%) 109 (3.1%) | 1067 (62.6%) 362 (21.2%) 232 (13.6%) 44 (2.6%) | 447 (53.7%) 248 (29.8%) 114 (13.7%) 23 (2.8%) | <0.001 |
†
Patients older than 85 years were reported in the SEER database as 85 years.
NOS: Not otherwise specified; RT: Radiotherapy; SD: Standard deviation; SEER: Surveillance, Epidemiology and End Results.
Looking at the percentages of different treatment strategies throughout the study years (2006–2017), the use of the following strategies increased: adjuvant chemotherapy (20.1 vs 10.6%), and perioperative chemotherapy (21.3 vs 0.5%); while the use of the following strategies decreased: surgery only (36.2 vs 58.2%) and adjuvant chemo-radiotherapy (22.4 vs 30.6%; Figure 2).
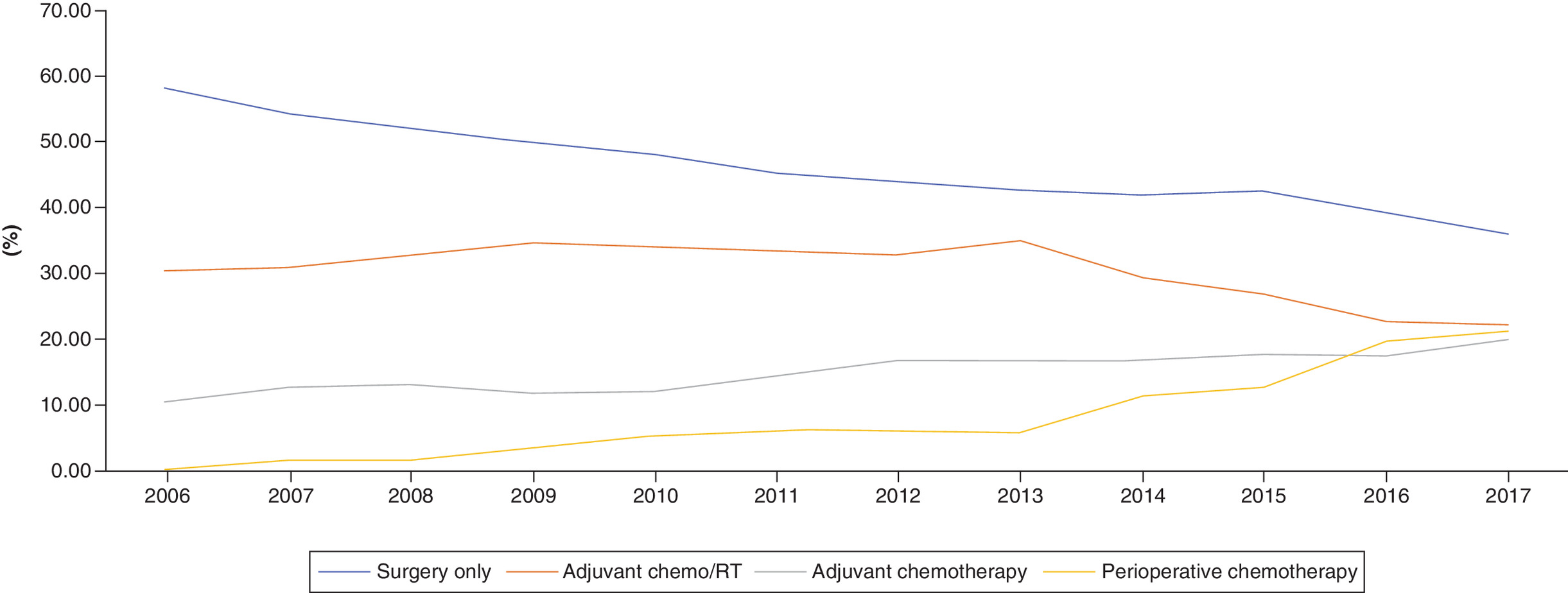
Figure 2. Percentages of different treatment strategies for localized gastric cancer throughout the study years (2006–2017).
RT: Radiotherapy.
Survival outcomes according to treatment strategies
Through Kaplan–Meier estimates, the strategies of surgery only and surgery followed by adjuvant chemotherapy were associated with worse overall survival (p < 0.001; Figure 3).

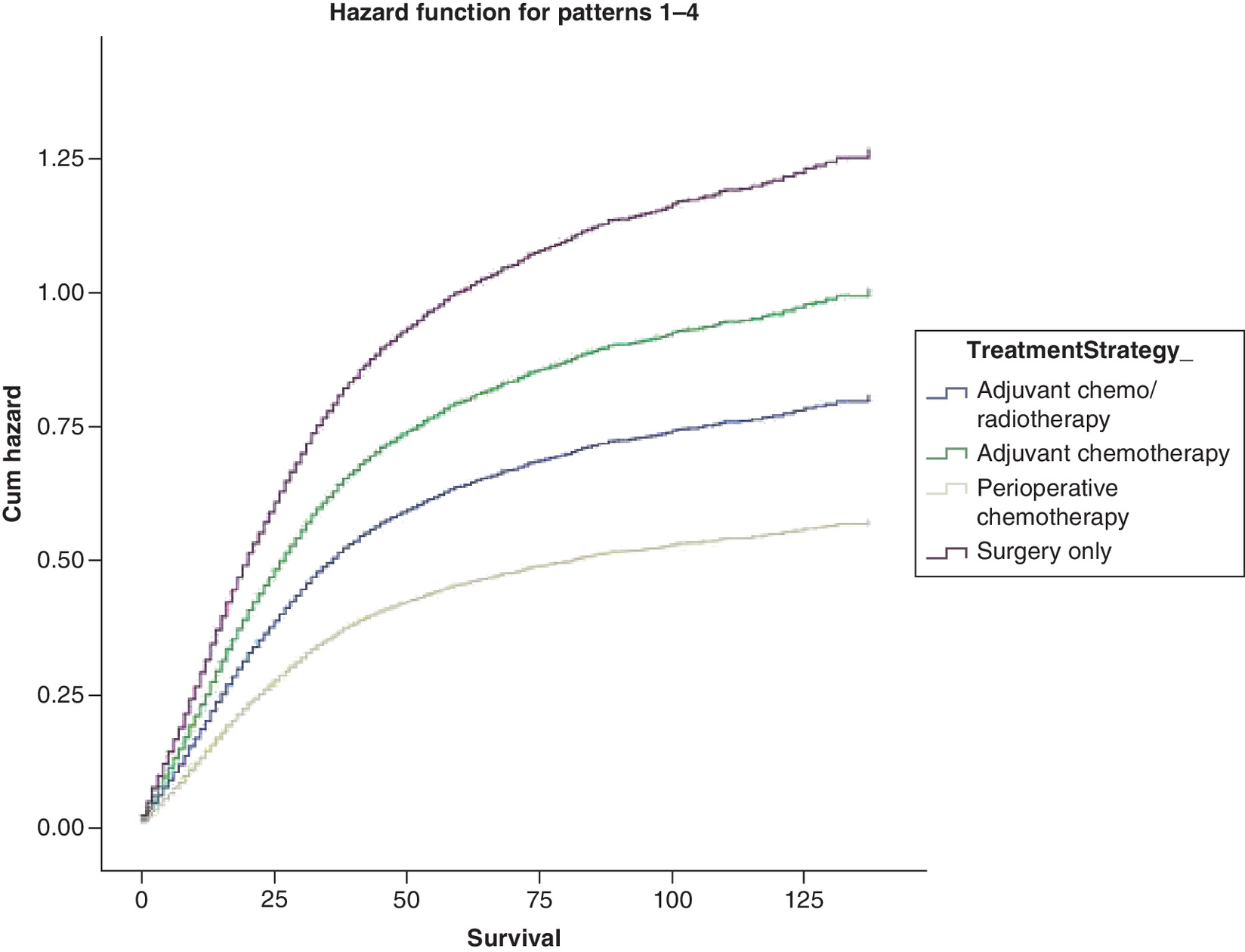
Using multivariable Cox regression analysis, the following factors were associated with worse overall survival: older age (hazard [HR]: 1.021; 95% CI: 1.018–1.023), males (HR: 1.09; 95% CI: 1.04–1.14), Black race (HR: 1.11; 95% CI: 1.04–1.19), cardia subsite (HR: 1.09; 95% CI: 1.02–1.17), grade 3–4 (HR: 1.32; 95% CI: 1.25–1.40), diffuse histology (HR: 1.46; 95% CI: 1.35–1.58), clinically node positive (HR: 1.43; 95% CI: 1.34–1.53), total gastrectomy (HR 1.20; 95% CI: 1.13–1.28) and surgery-only approach (HR: 1.65; 95% CI: 1.55–1.75). Likewise, the following factors were associated with worse cancer-specific survival: older age (HR: 1.015; 95% CI: 1.013–1.017), Black race (HR: 1.08; 95% CI: 1.00–1.17), cardia subsite (HR: 1.14; 95% CI: 1.05–1.24), grade 3–4 (HR: 1.43; 95% CI: 1.33–1.53), diffuse histology (HR: 1.59; 95% CI: 1.45–1.74), clinically node positive (HR: 1.51; 95% CI: 1.40–1.63) and surgery-only approach (HR: 1.56; 95% CI: 1.46–1.67; Table 2). Differences in adjusted cancer-specific mortality hazard between different treatment strategies were summarized in Figure 4, which showed that the highest cancer-specific mortality hazard is among individuals treated with only surgery; while the lowest cancer-specific mortality hazard is among individuals treated with perioperative chemotherapy.
| Parameters | Overall survival | Cancer-specific survival |
|---|---|---|
| HR (95% CI) | HR (95% CI) | |
| Age | 1.021 (1.018–1.023) | 1.015 (1.013–1.017) |
| Sex – Females – Males | Reference 1.09 (1.04–1.14) | Reference 1.04 (0.99–1.10) |
| Race – White – Black – Asian/Pacific Islander – American Indian | Reference 1.11 (1.04–1.19) 0.77 (0.72–0.82) 1.42 (1.10–1.85) | Reference 1.08 (1.00–1.17) 0.77 (0.71–0.82) 1.45 (1.09–1.93) |
| Subsite – Specified noncardia site – Cardia – Overlapping lesion | Reference 1.09 (1.02–1.17) 1.26 (1.18–1.34) | Reference 1.14 (1.05–1.24) 1.27 (1.19–1.37) |
| Grade – Grade 1–2 – Grade 3–4 | Reference 1.32 (1.25–1.40) | Reference 1.43 (1.33–1.53) |
| Histology – Intestinal – Diffuse – Adenocarcinoma, NOS – Others | Reference 1.46 (1.35–1.58) 1.13 (1.06–1.21) 1.14 (1.03–1.26) | Reference 1.59 (1.45–1.74) 1.20 (1.10–1.30) 1.23 (1.10–1.38) |
| Clinical N stage – N0 – N+ | Reference 1.43 (1.34–1.53) | Reference 1.51 (1.40–1.63) |
| Type of surgery – Partial gastrectomy – Total/near total gastrectomy – Gastrectomy with resection of adjacent organs – Gastrectomy, NOS | Reference 1.20 (1.13–1.28) 1.25 (1.16–1.34) 1.14 (0.99–1.30) | Reference 1.26 (1.18–1.35) 1.33 (1.23–1.44) 1.18 (1.01–1.37) |
| Treatment strategy – Adjuvant Chemo/RT – Surgery only – Adjuvant chemotherapy – Perioperative chemotherapy | Reference 1.65 (1.55–1.75) 1.23 (1.14–1.33) 0.69 (0.61–0.79) | Reference 1.56 (1.46–1.67) 1.24 (1.14–1.35) 0.71 (0.62–0.82) |
†
Patients with unknown race, grade and clinical N stage were included in the analysis but not reported in this table.
HR: Hazard ratio; NOS: Not otherwise specified; RT: Radiotherapy.
When the analyses were repeated after limiting it to only 8538 patients with complete information about different variables, similar findings (with regards to differences between treatment approaches) were observed (Supplementary Table 1).
Discussion
The current study evaluated the impact of treatment strategy on survival outcomes among patients with nonmetastatic gastric cancer. It suggested that individuals who were treated with surgery only, and to a less extent, individuals who were treated with surgery followed by adjuvant chemotherapy have worse survival outcomes. On the other hand, those treated with perioperative chemotherapy have the best survival outcomes.
The change in the percentages of patients receiving each of the four treatment strategies over the study years seems to coincide with different landmark publications introducing different strategies evaluated in the current study. Adjuvant chemo-radiotherapy was a predominant (peri)operative treatment strategy in the early part of the study, possibly following the results of the intergroup study published in 2001 which has suggested superiority of this approach compared with surgery alone [10]. Subsequently, the publication of Phase III CLASSIC trial (conducted in South Korea) in 2014, suggesting the superiority of adjuvant chemotherapy compared with a surgery-only strategy (among patients undergoing D2 gastrectomy) has coincided with an increased uptake of adjuvant chemotherapy as a potential option (particularly given increased concerns about the tolerability of the intergroup protocol for adjuvant chemo-radiotherapy) [11]. Likewise, the publication of the UK MAGIC Phase III trial (initially published in 2006) suggesting the superiority of a perioperative treatment approach compared with a surgery-alone strategy has prompted increased consideration of this strategy [12]. The subsequent introduction of the perioperative FLOT protocol (shown to be better than perioperative epirubicin/cisplatin/fluorouracil [ECF] protocol in 2017) has further bolstered this strategy as an option for many patients [13].
The Dutch CRITICS trial compared perioperative chemotherapy to preoperative chemotherapy and postoperative chemoradiotherapy, and it did not show any difference in overall survival between the two treatment strategies [14]. These results cannot be compared with the current study results as patients who received any form of perioperative radiotherapy (in addition to perioperative chemotherapy) were excluded from the cohort of perioperative chemotherapy in the current analysis.
The current study has also shown survival differences between different ethnic groups with regards to gastric cancer outcomes. Compared with White patients, African Americans seem to have worse outcomes, likely related to socioeconomic differences in access to care (as shown by other studies) [15,16]; whereas Asian Americans seem to have better survival outcomes, which is consistent with prior studies as well [17].
Several limitations should be considered when reviewing the results of the current analysis. First, there is no information about comorbidity or performance status among included patients. This likely has played a role in the choice of different perioperative treatments. That said, it should be remembered that all included patients have undergone some form of oncologic surgery. Thus, it is unlikely that any of those patients would have poor performance or significant, life-limiting comorbidity at the time of gastric cancer diagnosis. Second, details about the dose/schedules of chemotherapy and radiation therapy used within different strategies are unknown. Thus, the results of this study cannot be used to compare specific chemotherapy regimens to each others. Third, the extent of lymph node dissection was not reported. This is especially relevant for patients assigned to the adjuvant chemotherapy strategy. Thus, it is unclear if the lower survival observed with adjuvant chemotherapy (compared with adjuvant chemo-radiotherapy) is related to an inherent weakness in this strategy, infrequent use of D2 dissection, or ethnic/biological differences between Asian patients and Western patients (leading to lower efficacy of adjuvant chemotherapy among Western patients). Fourth, within the perioperative chemotherapy cohort, all patients have received pre-and postoperative chemotherapy. In prior studies evaluating perioperative chemotherapy, it is known that some patients would drop out following surgery and won't be fit to receive any further treatment because of surgical complications [13]. Thus, it seems that the current cohort of perioperative chemotherapy have a better than average perioperative course that they were able to receive the full planned course of treatment. Fifth, information about microsatellite instability (MSI) status is not available. Given the recent data suggesting differential activity of perioperative chemotherapy according to MSI status among gastric cancer patients, this could have confounded some of the results of the current study [18]. Overall, these limitations indicate that the current study is likely to inform association rather than causation and further prospective studies would be needed to confirm or refute these results. On the other hand, the current study has a few strengths that should be remembered, most notably, the large sample size of the study.
The current study highlights the need for additional prospective studies comparing perioperative strategies to each other (instead of comparing these strategies to a surgery-only approach). The incorporation of newer agents (especially immune checkpoint inhibitors) is also likely to impact treatment paradigms of patients with localized gastric cancer. There is also a need to consider the potential differences between Asian patients versus patients from other parts of the world when designing/conducting these studies.
In conclusion, among patients with localized gastric cancer, patients who were treated with surgery-only, and to a less extent, patients who were treated with surgery followed by adjuvant chemotherapy have worse survival outcomes; while those treated with perioperative chemotherapy have the best survival outcomes. Further prospective studies are needed to confirm the results of the current study.
•
The study aims to assess the survival outcomes of patients with nonmetastatic gastric cancer according to the type of perioperative treatment strategy used.
•
Surveillance, Epidemiology and End Results research-plus database was explored.
•
Patients with nonmetastatic gastric cancer who were treated with an oncologic surgery were reviewed.
•
Multivariable Cox regression analysis was used to examine the impact of treatment strategy on overall and cancer-specific survival.
•
A total of 11,526 patients were found to be eligible and they were included in the current analysis.
•
Throughout the study years (2006–2017), the use of the following strategies increased: adjuvant chemotherapy (20.1 vs 10.6%), and perioperative chemotherapy (21.3 vs 0.5%).
•
While the use of the following strategies decreased: surgery only (36.2 vs 58.2%), and adjuvant chemo-radiotherapy (22.4 vs 30.6%).
•
Using multivariable Cox regression analysis, the following factors were associated with worse overall survival: older age (hazard ratio [HR]: 1.021; 95% CI: 1.018–1.023), males (HR: 1.09; 95% CI: 1.04–1.14), Black race (HR: 1.11; 95% CI: 1.04–1.19), cardia subsite (HR: 1.09; 95% CI: 1.02–1.17), grade 3–4 (HR: 1.32; 95% CI: 1.25–1.40), diffuse histology (HR: 1.46; 95% CI: 1.35–1.58), clinically node positive (HR: 1.43; 95% CI: 1.34–1.53), total gastrectomy (HR: 1.20; 95% CI: 1.13–1.28) and surgery-only approach (HR: 1.65; 95% CI: 1.55–1.75).
Financial & competing interests disclosure
The author has served on advisory boards with Eisai Canada, Roche Canada, and Lilly Canada. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
As this study is based on a publicly available database without identifying patient information, neither IRB approval nor informed consent was required.
Supplementary Material
File (suppl_file.docx)
- Download
- 12.75 KB
References
Papers of special note have been highlighted as: • of interest
1.
Karimi P, Islami F, Anandasabapathy S, Freedman ND, Kamangar F. Gastric cancer: descriptive epidemiology, risk factors, screening, and prevention. Cancer Epidemiol. Biomarkers Prev. 23(5), 700–713 (2014).
2.
Guggenheim DE, Shah MA. Gastric cancer epidemiology and risk factors. J. Surg. Oncol. 107(3), 230–236 (2013).
3.
Machlowska J, Baj J, Sitarz M, Maciejewski R, Sitarz R. Gastric cancer: epidemiology, risk factors, classification, genomic characteristics and treatment strategies. Int. J. Mol. Sci. 21(11), 4012 (2020).
4.
Giryes A, Oweira H, Mannhart M, Decker M, Abdel-Rahman O. Exploring the differences between early-onset gastric cancer and traditional-onset gastric cancer. J. Gastrointest. Oncol. 9(6), 1157–1163 (2018).
5.
Choi AH, Kim J, Chao J. Perioperative chemotherapy for resectable gastric cancer: MAGIC and beyond. World J. Gastroenterol. 21(24), 7343–7348 (2015).
6.
Aoyama T, Yoshikawa T. Adjuvant therapy for locally advanced gastric cancer. Surg. Today 47(11), 1295–1302 (2017).
7.
Ronellenfitsch U, Schwarzbach M, Hofheinz R et al. Preoperative chemo(radio)therapy versus primary surgery for gastroesophageal adenocarcinoma: systematic review with meta-analysis combining individual patient and aggregate data. Eur. J. Cancer 49(15), 3149–3158 (2013).
8.
Beeharry MK, Zhang TQ, Liu WT, Gang ZZ. Optimization of perioperative approaches for advanced and late stages of gastric cancer: clinical proposal based on literature evidence, personal experience, and ongoing trials and research. World J. Surg. Oncol. 18(1), 51 (2020).
9.
Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence - SEER Research Plus Data, 18 Registries, Nov 2019 Sub (2000–2017) - Linked To County Attributes - Total U.S., 1969–2018 Counties. National Cancer Institute, DCCPS, Surveillance Research Program (2020). www.seer.cancer.gov
10.
MacDonald JS, Smalley SR, Benedetti J et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N. Engl. J. Med. 345(10), 725–730 (2001).
11.
Noh SH, Park SR, Yang H-K et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised Phase III trial. Lancet Oncol. 15(12), 1389–1396 (2014).
12.
Cunningham D, Allum WH, Stenning SP et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 355(1), 11–20 (2006).
13.
Al-Batran S-E, Homann N, Pauligk C et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, Phase II/III trial. Lancet 393(10184), 1948–1957 (2019).
14.
Cats A, Jansen EPM, Van Grieken NCT et al. Chemotherapy versus chemoradiotherapy after surgery and preoperative chemotherapy for resectable gastric cancer (CRITICS): an international, open-label, randomised Phase III trial. Lancet Oncol. 19(5), 616–628 (2018).
15.
Abdel-Rahman O. Impact of socioeconomic status on presentation, treatment and outcomes of patients with pancreatic cancer. J. Comp. Eff. Res. 9(17), 1233–1241 (2020).
16.
David R, Collins JW Jr. Why does racial inequity in health persist? J. Perinatol. 41(2), 346–350 (2021).
17.
Abdel-Rahman O. Asian Americans have better outcomes of non-metastatic gastric cancer compared to other United States racial groups: a secondary analysis from a randomized study. World J. Gastrointest. Oncol. 11(12), 1151–1160 (2019).
18.
Pietrantonio F, Miceli R, Raimondi A et al. Individual patient data meta-analysis of the value of microsatellite instability as a biomarker in gastric cancer. J. Clin. Oncol. 37(35), 3392–3400 (2019).
• Evaluates the impact of microsatellite instability status on the outcomes of nonmetatstatic gastric cancer in the setting of different perioperative treatment strategies.
Information & Authors
Information
Published In
Pages: 1143 - 1151
PubMed: 34515496
Copyright
© 2021 Future Medicine Ltd.
History
Received: 11 May 2021
Accepted: 2 August 2021
Published online: 13 September 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Outcomes of patients with nonmetastatic gastric adenocarcinoma according to perioperative treatment strategy: a real-world, population-based study. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0113
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Jiajun Luo, Ziwei Wang, Adjuvant chemotherapy and lymph node examination interact to shape survival in older adults (≥ 75 years) with resected gastric cancer: a SEER-based propensity score–matched and competing-risk analysis, World Journal of Surgical Oncology, 10.1186/s12957-026-04390-8, 24, 1, (2026).