Cost–effectiveness and cost-benefit analysis of oliceridine in the treatment of acute pain
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Oliceridine, a new class of μ-opioid receptor agonist, is selective for G-protein signaling (analgesia) with limited recruitment of β-arrestin (associated with adverse outcomes) and may provide a cost-effective alternative versus conventional opioid morphine for postoperative pain. Patients & methods: Using a decision tree with a 24-h time horizon, we calculated costs for medication and management of three most common adverse events (AEs; oxygen saturation <90%, vomiting and somnolence) following postoperative oliceridine or morphine use. Results: Using oliceridine, the cost for managing AEs was US$528,424 versus $852,429 for morphine, with a net cost savings of $324,005. Conclusion: Oliceridine has a favorable overall impact on the total cost of postoperative care compared with the use of the conventional opioid morphine.
Lay abstract
Oliceridine, a new class of opioid pain medication, given in a vein, is a unique medication in that it provides pain relief comparable to morphine and may have less costly side effects. It is given in a hospital or surgery center for the treatment of postoperative pain and can save money compared with other opioid pain medicines due to fewer side effects. An economic model was developed to compare morphine to oliceridine for common side effects and pain relief following surgery. Oliceridine use resulted in a cost saving (US$324,005; 2020 US dollars) when compared with morphine.
In the USA, approximately 30% of hospital admissions require a surgical intervention [1], and nearly 86% of patients undergoing surgery report postoperative pain, which is often moderate to severe in intensity. Further, most surgical patients require pharmaceutical treatment as a component of the postsurgical management of their pain [2]. Undertreatment of postsurgical pain has been linked to reduced quality of life, surgical complications, prolonged rehabilitation and development of chronic pain [3]. In contemporary clinical practice, surgeries are increasingly performed in an outpatient or ambulatory surgery clinical setting, where time becomes a critical variable in the healthcare delivery process [4,5]. This evolution in clinical care focuses attention on the particular choices for management of pain and associated symptoms since any accompanying adverse events (AEs) may prolong patients' time in the postanesthesia care unit (PACU) as well as their time to discharge, all of which may have substantial impact on the cost of care and net revenue from surgical cases [6]. Finally, the development of Enhanced Recovery After Surgery (ERAS) protocols and a focus on minimization of the use of opioid medications have dramatically altered the approach to managing acute pain postsurgery, with a greater focus on protocol-driven multimodal pain management [7,8].
In the midst of this changing healthcare landscape, intravenous (IV) opioid analgesia remains the backbone of postsurgical pain management [2]. Commonly used opioid analgesics for moderate-to-severe postoperative pain include morphine sulfate, fentanyl citrate and hydromorphone hydrochloride. These medications are associated with opioid-related adverse events (ORAEs) that may affect patients' health outcomes and satisfaction with care [9]. The occurrence of ORAEs can restrict dose escalation which may be required to achieve adequate analgesia, and thus compromise pain management at the bedside [10]. The incidence of ORAEs among surgical patients has been estimated to range from 1.8 to 13.6%, and patients with such events may experience prolonged lengths of stay (LOS) and higher hospital costs [9]. In a report on 135,379 surgical patients who received opioid analgesia, 14,386 (10.6%) experienced ORAEs which had significant economic impacts on hospitals [9]. Of note, this retrospective study utilized the International Classification of Diseases, Ninth Revision (ICD-9) codes to document ORAEs; mild ORAEs such as nausea, vomiting, pruritus, constipation and delirium may not be captured by ICD-9 coding [9]. In this large case series, patients who experienced ORAEs had US$8225 higher mean cost per admission ($25,599 per admission compared with $17,374 for patients with no ORAEs) after controlling for patient demographics, clinical risk factors and surgery type. Further, mean LOS in the hospital was 1.6 days longer for patients reporting ORAEs (6.8 days compared with 5.2 days for patients without events) [9].
It is therefore not surprising that the development of new analgesic drugs with a potential for lower risk of ORAEs may be expected to improve both patient outcomes and cost of care. Oliceridine is a new, recently US FDA-approved IV opioid analgesic that may have important tolerability differences from conventional IV opioid medications. A key attribute of oliceridine that differentiates it from conventional opioid analgesics is its potential improvements in AE profile that were measured in detail in its Phase III clinical development program. The pivotal evidence supporting FDA approval of oliceridine was based on two large, multisite, Phase III randomized placebo- and active (morphine used as a prototype to represent conventional opioids)-controlled clinical trials (APOLLO 1: orthopedic surgery – bunionectomy study; NCT02815709 and APOLLO 2: plastic surgery-abdominoplasty study; NCT02820324) [11,12]. In addition, the safety and tolerability of oliceridine as a first-line pain medication for surgical patients was examined in a real-world, prospective, Phase III observational study among a clinically diverse population of surgical patients studied in a variety of clinical practice settings, including hospital inpatient units, ambulatory surgery centers and hospital emergency departments (ATHENA; NCT02820324) [13]. Using the clinical trial and real-world data noted above, and integrating regional and national cost data, a cost–effectiveness model was developed, comparing the costs and ORAEs associated with the use of either oliceridine or morphine for the management of acute postoperative pain. The study followed the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) recommended for economic modeling studies [14].
Materials & methods
Sources & derived data
The clinical efficacy and adverse outcome data were obtained from published reports of the clinical development of oliceridine for the treatment of acute pain in the postoperative setting. Oliceridine was studied in two pivotal Phase III placebo- and active-controlled multisite clinical trials [11,12]. The APOLLO-1 trial (Study 1) examined the efficacy and safety of oliceridine for the treatment of postoperative pain following hard tissue orthopedic surgery in 389 patients undergoing first meta-tarsal bunionectomy with regional anesthesia [11]. Study 2 (APOLLO-2) examined the efficacy and safety of oliceridine for the treatment of postoperative pain following soft tissue plastic surgery in 401 patients undergoing an abdominoplasty procedure under general anesthesia [12]. In addition to the controlled clinical studies, a third study, ATHENA (Study 3) examined the safety and tolerability of oliceridine in an open-label real-world setting among 768 patients treated for a broad range of postoperative and post-procedural clinical care requiring the use of a parenteral opioid for the management of acute pain [13]. Details of the study designs, patient demographic and clinical information and study outcomes are reported elsewhere [11–13].
The pre-specified primary clinical efficacy outcome in the pivotal Phase III studies was the categorical outcome of response defined as patients who met the following criteria: at least a 30% improvement in final time-weighted sum of the pain intensity differences (SPID) from baseline at 48 h (SPID-48) for orthopedic surgery – bunionectomy or at 24 h (SPID-24) for plastic surgery-abdominoplasty; without use of rescue pain medication during the randomized treatment period; without early discontinuation of study medication for any reason and without reaching the study medication volume-based dosing limit.
Adverse outcomes of interest for the health economic analysis were directly observed in the clinical trials and included: oxygen desaturation defined as a measured oxygen saturation reaching an SpO2 <90%; vomiting and somnolence, the latter two outcomes both reported as Medical Dictionary for Regulatory Activities (MedDRA)-coded AEs. These adverse outcomes were selected as the focus in the model since they have been well characterized in the literature to be substantial postanesthesia economic contributors to the costs associated with the use of parenteral opioids in the postsurgical setting [15,16].
Cost inputs & estimation methods
The current clinical practice of postoperative pain management recommends the use of enhanced recovery after surgery (ERAS) protocols to minimize the adverse outcomes associated with pain management during postsurgical care. Implementation of these protocols is rapidly evolving, and it can therefore be expected that today's actual current rate of ORAEs may be even lower than reported in the recent published literature, and correspondingly, that the cost of these adverse outcomes will be less than what is reported in the existing literature [17]. Therefore, to avoid an overestimation of the cost of ORAEs in the health economic model described here, the most recent representative national data (from the National Inpatient Sample dataset as described below) were used to estimate costs, and the mean marginal cost per day was selected as the analytical parameter of interest, because this is the most conservative statistical approach that could be employed. Further, since the most recent nationally representative data available are for 2017, cost estimates were inflated to reflect projected 2020 actual costs using the May 2020 medical care consumer price index (CPI) factor of 1.09647 (accessed at: www.bls.gov/cpi).
The mean cost and length of stay (LOS) for a group of eight surgical procedures highly likely to require the use of parenteral opioids for postoperative pain management were estimated using the 2017 National Inpatient Sample (NIS) dataset from the Healthcare Cost and Utilization Program (HCUP) [18]. All records for patients age 18 and older were extracted from the sample. Surgical admissions were identified by the International Classification of Diseases, Tenth Revision (ICD-10) procedure codes. These codes included surgical phenotype specifications for the following procedures: gastrectomy, gastric bypass, colon-rectal resection, knee arthroplasty, coronary artery bypass graft, spinal fusion, cholecystectomy and abdominal repairs. This restricted dataset included 467,796 adult admissions, which constitutes a representative sample of 2,338,979 US surgeries performed in 2017. Females comprised 56.6% of the total sample population. Racial distribution was 75.3% White, 10.0% Black and 9.5% Hispanic, with the balance of the sample distributed across Other, Mixed, or Undeclared race categories. Less than 1% of patients died during the surgical admission (0.84%). Mean patient age (standard deviation) was 61.0 years (SD: 16.7, range: 18–90). Mean LOS in hospital was 4.54 days (SD: 6.9, range: 0–334 days). The cost per admission was estimated by applying each hospital's cost-to-charge ratio to the total charges for the admission, a standard approach for summarizing HCUP data. The estimated mean cost per admission was $24,168 (median: $16,618, SD: $27,286, range: $19–$2,466,577). NIS sample weighted and unweighted values were identical, so the unweighted means were used for calculation of the marginal cost for model events [18]. The result of this analysis is provided in Supplementary Table 1.
The presence of respiratory depression after surgery has a well-documented association with LOS, increased cost and unplanned admission to the intensive care unit [15,19,20]. In the recently reported multisite PRODIGY trial (NCT02811302), mean LOS was 7.7 days (SD: 7.8 days) for patients without episodes of opioid-induced respiratory depression (OIRD), compared with 10.5 days (SD: 10.8 days) for patients with an OIRD episode [19]. This represents an increase of 36.4% in hospital LOS. Further, an economic analysis of US cost data in PRODIGY for 148 patients with OIRD reported a 15% higher cost per admission when compared with 272 propensity-score matched patients from the study sample who did not have an episode of OIRD [21].
Thus, based on the PRODIGY analysis, the cost of OIRD may be estimated as either 15% of the mean cost per surgery, or as the cost associated with an increase of 36.4% in hospital LOS [21]. However, the actual cost data from that trial may be assumed to be biased upward because they reflect costs in selected hospitals capable of undertaking such a large multisite clinical trial. This assumption is supported by the relatively longer LOS reported for PRODIGY trial patients (LOS 7.7 vs 10.5 days for non-OIRD and OIRD admissions, respectively) [19]. Therefore, to avoid bias in the estimation of OIRD-associated event costs, the health economic model reported here used the mean costs and LOS from a representative sample of US surgical admissions (Supplementary Table 1). The cost of an OIRD event was then calculated as 15% of the cost of an admission. Thus, the most conservative cost weight used in the model is $24,168*15% = $3625. This is equivalent to an increase of approximately 1.08 days in the hospital for patients with a median LOS of 3 days. If the PRODIGY estimate of 36.4% increase in LOS was used as the cost basis, the estimated cost per OIRD is mean LOS 4.54*36.4 = 1.65 days. At a median cost of $3365 per day, an OIRD event would add $5552 to an admission. The mean low and high estimated cost weights for OIRD events for selected types of surgeries are provided in Supplementary Table 2.
Postoperative nausea and vomiting (PONV), especially vomiting, has been identified as a significant contributor to increased morbidity and LOS, and decreased satisfaction with care among surgical patients [22,23]. The lowest reported marginal cost of PONV in the Premier Database study [15] showed a marginal cost increase for patients who experienced an episode of PONV of $1698 and higher LOS of 1.6 days. However, as noted above, since current practice recommends the use of ERAS protocols, which almost universally include the use of prophylactic antiemetic medication [24], and a focus on multimodal pain management [25], the health economic model reported here anticipated that the risk of PONV in current practice has been consequently reduced, and thus, data from earlier studies may overstate the effect of vomiting on LOS and cost of care. To avoid over-estimating the cost of vomiting in the model, the marginal cost of vomiting used was based on the values in the NIS 2017 surgical admissions dataset. ICD-10 codes for vomiting with and without nausea (R11.0, R11.11, R11.12 and K91) were used to identify an episode of vomiting. A multivariable model with a gamma-distributed log-link transformation was used to estimate the marginal cost increase for patients with a vomiting diagnosis. Episodes were controlled for age, sex and type of surgery in the model. The mean cost per admission for patients with a vomiting diagnosis was $23,382, compared with $22,410 for patients without the condition (p < 0.0001). Thus, the marginal cost of a vomiting episode is estimated at $972. This may be expected to be a low estimate because vomiting tends to be under-reported in discharge summaries, and vomiting will therefore be under-coded in billing data. When the effect of a vomiting diagnosis on LOS was examined, an increase of 0.51 days in LOS was estimated. Using the median cost per day estimated from the HCUP dataset (Supplementary Table 1), a mean increase of 0.51 day in LOS would result in an estimated marginal cost of vomiting of $3365*0.51, or a cost of $1716. Based on these analyses, $1344 (the median value between $972 and $1716 for the two costing results) was used as the cost weight for vomiting in the model.
The cost of somnolence or sedation was calculated for the health economic model. Somnolence or sedation was recorded as a MedDRA-coded AE among 19.9% of oliceridine-treated and 23.4% of morphine-treated patients in the pivotal Phase III orthopedic surgery – bunionectomy [11] and Phase III plastic surgery-abdominoplasty studies [12]. However, the recorded rate of somnolence as an AE in the large, multisite Phase III open-label safety study was 1.8% [13]. Rates of somnolence as an AE in archival records are much lower than rates recorded in clinical trials, making it difficult to identify the cost of these AEs under routine practice conditions. Using the ICD-10 code of R40.0, somnolence was coded among only 0.8% of the surgeries in the NIS 2017 dataset, and patients with this code had 1.33 days longer LOS and $6353 higher cost per admission than patients without a somnolence code after controlling for age, sex and surgery type. However, given the very low prevalence of recorded somnolence, this marginal cost estimate for somnolence is most likely biased upward because only the most severe cases were recorded. Thus, the use of this estimate in the economic model would likely bias results against morphine. As an additional observation, it is noted that Barra and colleagues estimated the cost of somnolence as an AE at 93% of the cost of a vomiting AE [16]. Using the 2017 cost data from the NIS surgical dataset, this would result in a median cost of $1344*93%=$1250. Based on this calculation, the more conservative cost weight of $1250 per somnolence event was included in the health economic model to capture the economic effect of this condition.
The cost analyses for representative US surgeries in 2017, were inflated to 2020 costs using the medical care consumer price index (CPI) from May 2020 of 1.09647, (US Bureau of Labor and Statistics: www.bls.gov/). The cost weights included in Supplementary Table 3 were adapted as the economic estimates in the analysis.
Economic model analytic framework
To estimate the value of oliceridine compared with morphine, a base model cost–effectiveness analysis was constructed from the Phase III clinical trial data (Study 1 and 2) which considered the use of oliceridine as a first-line pain medication for surgical patients compared with pain management with morphine. A decision tree was used to structure the data, using a 24-h time horizon because the greatest contribution of the marginal costs and benefits of postsurgical pain management are expected to materialize within this time period. Patients were grouped on the branches of the decision tree by the observed treatment response outcomes recorded in the Phase III pivotal studies, and by the presence or absence of adverse outcomes of interest, and by the clinical need for rescue pain medication due to lack of efficacy of the assigned treatment. Failure of oliceridine at the initial 0.35 mg dosing was assumed to lead to escalation of dosing to 0.5 mg, and then to the use of rescue analgesic medication if patients failed this higher dose. Failure to benefit from the morphine medication was assumed to lead directly to use of rescue analgesic medication, as occurred in the Phase III studies. An overview of the methodology is shown in Figure 1.
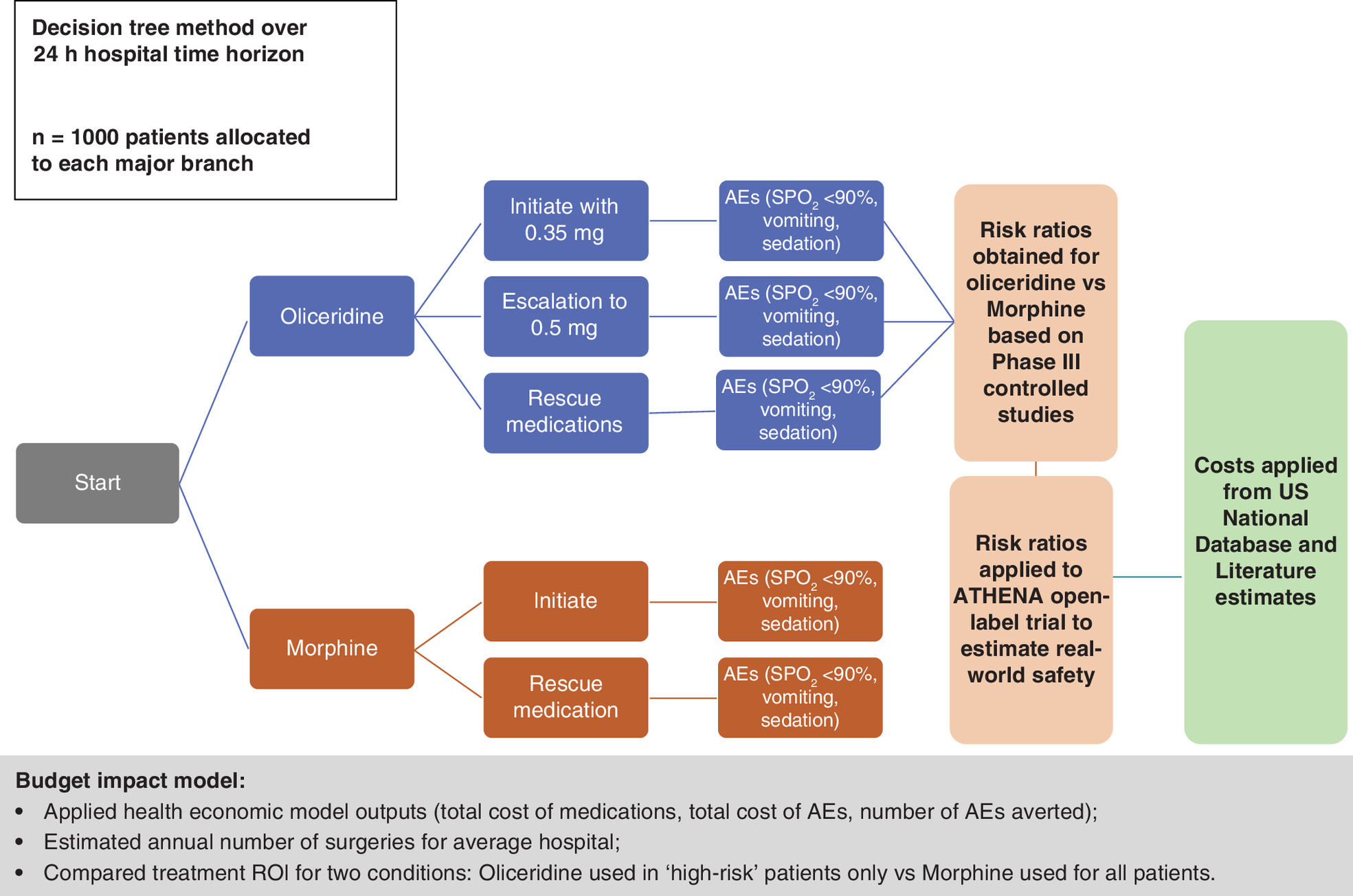
Figure 1. Overview of the economic model methodology.
The Phase III controlled studies were randomized, double-blind, placebo- and morphine-controlled studies in patients with moderate-to-severe acute pain following either orthopedic surgery – bunionectomy (APOLLO-1) [11], or plastic surgery-abdominoplasty (APOLLO-2) [12]. The National database used for cost calculations was the 2017 National Inpatient Sample dataset from the Healthcare Cost and Utilization Program (HCUP, accessed at: www.hcup.ahrq.gov). Literature sources included: the PRODIGY trial [19]; data from the Premier Healthcare Database that examined the prevalence of opioid-related respiratory and gastrointestinal adverse events in patients undergoing various surgical procedures [15]; and a study that examined the cost-consequence analysis utilizing non-opioids and opioids [16].
AE: Adverse event; n: Number; ROI: Return on investment; SpO2: Peripheral oxygen saturation.
The differential marginal costs focused on the presence of three common and costly AEs associated with the use of parenteral opioid pain medication, namely, oxygen desaturation, based on observed oxygen saturation levels (SpO2) <90%, vomiting and somnolence.
Since the Phase III pivotal trials were designed to test the efficacy and safety of the treatments in a controlled research setting, these studies by design did not permit the use of multimodal analgesia. Therefore, in order to prevent the economic model from using an excessively high estimation of the true incidence of the adverse outcomes of interest likely to be seen in actual clinical practice, risk ratios for oliceridine compared with morphine were derived from the pivotal randomized Phase III studies and then applied to the AE rates observed in the large multisite Phase III open-label safety study, ATHENA (Study 3). This latter study provided a more accurate representation of the tolerability and safety of oliceridine in a real-world practice setting under conditions of routine clinical care, where use of oliceridine in conjunction with clinician-directed multimodal analgesia was the norm. Therefore, this approach allowed a more accurate estimation of the true incidence of opioid-related adverse outcomes that would be expected in actual clinical practice.
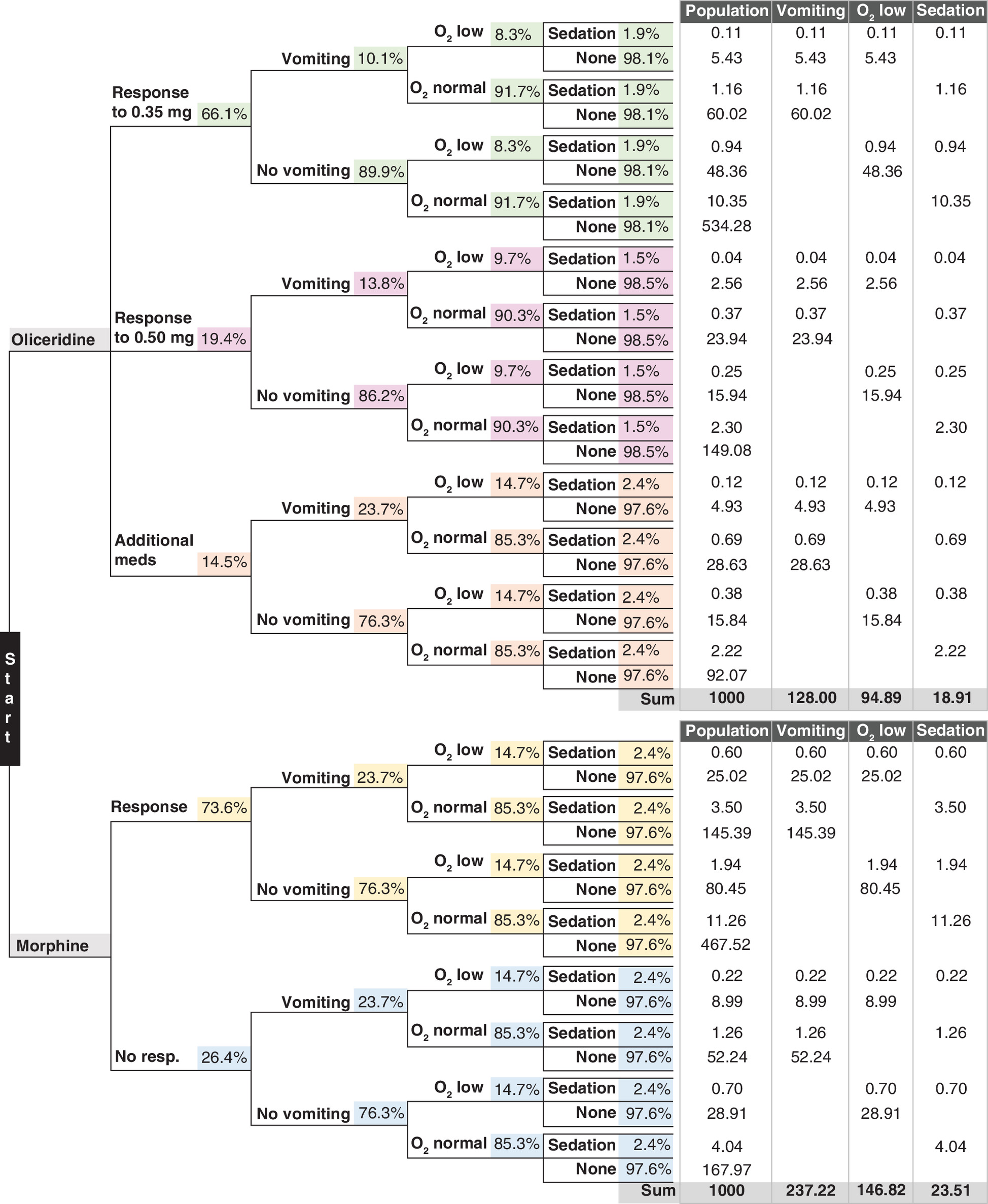
The data inputs used in the construction of the health economic model are shown in Tables 1, 2A & 2B. Overall costs were enumerated as differences in the cost of pain medication and differences in resource use required to manage the three common and costly adverse outcomes of interest in this model during the first 24 h after surgery. Costs of pain medication, rescue therapy and antiemetic drugs were tabulated based on rates observed in the pivotal Phase III studies. The model presumed a 24-h total weighted cost of postoperative pain medication of $108.14 for oliceridine and $15 for morphine. Other model parameters are derived from the published literature and observational cost data as discussed above in the Source and derivative data section. Figure 2 shows the relationships between the main inputs from the clinical study results, the approach to calculation of risk ratios for the two treatments considered in the model, the cost inputs applied and the resulting model parameters and outputs for the health economic model. All calculations for the decision tree and economic model were programmed in Excel (Microsoft Corporation, WA, USA). A schematic representation of the model inputs in a tabular form together with distributions is shown in Figure 3.
| Input parameter | Treatment allocation | % |
|---|---|---|
| Efficacy (responder %) | Oliceridine 0.35 mg demand dose initial responders | 66.1 |
| Oliceridine 0.5 mg demand dose incremental proportion of responders | 19.4 | |
| Morphine 1 mg demand dose | 73.6 | |
| Rescue analgesic medication use (%) | Oliceridine 0.35 mg demand dose | 17.0 |
| Oliceridine 0.5 mg demand dose | 14.5 | |
| Morphine 1 mg demand dose | 12.0 | |
| Rescue antiemetic medication use (%) | Oliceridine 0.35 mg demand dose | 45.3 |
| Oliceridine 0.5 mg demand dose | 51.1 | |
| Morphine 1 mg demand dose | 62.9 |
The data shown here are obtained from the two randomized placebo- and morphine-controlled Phase III studies (pivotal) in patients with moderate-to-severe acute pain following either orthopedic surgery – bunionectomy (APOLLO-1, Study 1), or plastic surgery-abdominoplasty (APOLLO-2, Study 2) [11,12]. The pre-specified primary clinical efficacy outcome in the pivotal Phase III studies was the categorical outcome of response defined as patients who met the following criteria: at least a 30% improvement in final time-weighted sum of the pain intensity differences (SPID) from baseline at 48 h (SPID-48) for orthopedic surgery – bunionectomy or at 24 h (SPID-24) for plastic surgery-abdominoplasty; without use of rescue pain medication during the randomized treatment period; without early discontinuation of study medication for any reason; and without reaching the study medication volume-based dosing limit.
| Adverse event | Treatment allocation | ||
|---|---|---|---|
| Oliceridine 0.35 mg demand dose | Oliceridine 0.5 mg demand dose | Morphine 1 mg demand dose | |
| Adverse event incidence and Risk ratio computation from pooled pivotal Phase III RCTs (orthopedic surgery – bunionectomy study and plastic surgery-abdominoplasty study).† | |||
| Low O2 saturation | |||
| Value (%) | 14.6 | 17.0 | 22.2 |
| Risk ratio applied | 1.52 | 1.16 | – |
| Vomiting | |||
| Value (%) | 30.3 | 41.5 | 51.9 |
| Risk ratio applied | 1.71 | 1.37 | – |
| Somnolence/sedation | |||
| Value (%) | 19.0 | 15.1 | 23.5 |
| Risk ratio applied | 1.24 | 0.8 | – |
| Estimation of expected adverse event incidence in real-world conditions derived from Phase III open-label safety study data.‡ | |||
|---|---|---|---|
| Low O2 saturation | |||
| Value (%) | 8.3 | 9.7 | 14.7 |
| Vomiting | |||
| Value (%) | 10.1 | 13.8 | 23.7 |
| Somnolence/sedation | |||
| Value (%) | 1.5 | 1.9 | 2.4 |
†
‡
Data shown for all treatment groups are derived from the pivotal randomized Phase III studies (APOLLO-1 and -2 as shown in Table 2A) [11,12] and then applied to the adverse event rates observed in the large multisite Phase III open-label safety study (ATHENA, Study 3) [13]. This large study was an open-label safety study of oliceridine conducted in 768 patients following a wide range of surgical procedures or nonsurgical medical conditions [13]. All patients in the study had at least one medical comorbidity. Almost half of all patients (46%) were obese with a BMI ≥30 kg/m2 and 32% were aged 65 years or older.
RCT: Randomized controlled trial.
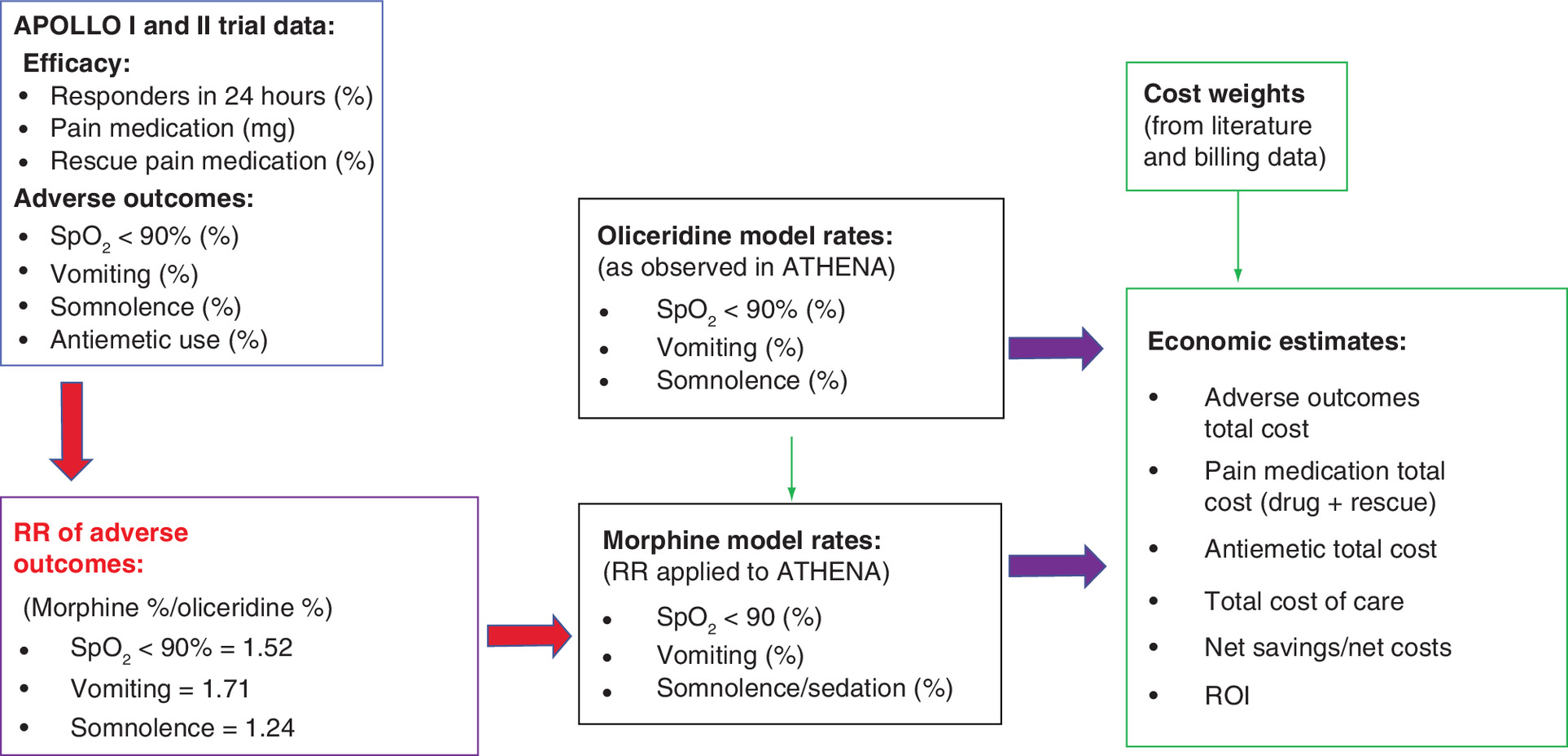
Figure 2. Summary of the analytic framework and methodology used to design the oliceridine health economic model.
The Phase III APOLLO controlled trials were randomized, double-blind, placebo- and morphine-controlled studies in patients with moderate-to-severe acute pain following either orthopedic surgery – bunionectomy (APOLLO-1) [11], or plastic surgery-abdominoplasty (APOLLO-2) [12]. The pre-specified primary clinical efficacy outcome in the pivotal Phase III studies was the categorical outcome of response defined as patients who met the following criteria: at least a 30% improvement in final time-weighted SPID from baseline at 48 h (SPID-48) for orthopedic surgery – bunionectomy or at 24 h (SPID-24) for plastic surgery-abdominoplasty; without use of rescue pain medication during the randomized treatment period; without early discontinuation of study medication for any reason and without reaching the study medication volume-based dosing limit. Adverse outcomes of interest for the health economic analysis were directly observed in the clinical trials and included: oxygen desaturation defined as a measured oxygen saturation reaching an SpO2 <90%; vomiting and somnolence, the latter two outcomes both reported as MedDRA-coded adverse events.
The ATHENA trial was an open-label safety study of patients with moderate-to-severe acute pain following a surgical procedure or due to a medical condition in a total of 768 patients receiving at least one dose of oliceridine [13].
MeDRA: Medical Dictionary for Regulatory Activities; ROI: Return on investment; SPID: Sum of the pain intensity differences; SpO2: Peripheral oxygen saturation.
Approaches used for issues related to skewed, missing or censored data are described in the published reports of the clinical trials. The study parameters were weighed for appropriate representation in the cost calculations by the proportion of patients contributing to the study's contribution to the overall model parameter.
Sensitivity analyses
Two approaches were used to test the sensitivity of the model. In the first method, the health economic model estimates were examined using a one-way sensitivity analysis approach to document the model's response to: changes in average daily cost of oliceridine (ranging from $60 to $150); a 20% change (increase or decrease) in the expected rate of each of the adverse outcomes; assuming the cost of each of the adverse outcomes to be 20% higher or 20% lower than in the base model; assuming that additional pain medication cost was 50% higher or lower; and assuming that the response to oliceridine was 10% better or 10% worse. A second approach to test the sensitivity of the model was performed using a Monte Carlo simulation applied to the base model, again using a population sample of 1000 surgeries in each of the allocated treatment conditions. Simulations were conducted in Excel using Crystal Ball software for estimation (Oracle Crystal Ball v 11.1.2.4, Oracle Software, 2017). Ten thousand simulations were run to evaluate the combined effects of randomly varying the model parameters together, assuming a Γ distribution for cost variables and a β distribution for event rates. The ranges used in the simulation runs are provided in Supplementary Table 4.
Results
Cost and outcomes from this analysis were estimated for 1000 patients each, allocated to either treatment option, oliceridine or morphine. The model presumed a 24-h total weighted cost of $108.14 for oliceridine and $15 for morphine with a difference of $94.13 per patient in a 24-h period. The cost of pain medication for the 1000 patient surgeries was $30,558 and $127,181 for morphine and oliceridine treated patients, respectively, with 166 ORAE avoided for an added expenditure of $96,623 US dollars in the oliceridine treated patients, in incremental cost–effectiveness ratio (ICER) of $582/ORAE avoided from pharmacy budget costing perspective. In general, patients allocated to oliceridine experienced fewer ORAEs of respiratory depression, postoperative vomiting and somnolence, resulting in $324,005 cost savings from a hospital cost perspective. As oliceridine was the economically dominant treatment using the cost perspective of the hospital, an ICER could not be calculated. To illustrate the economic values of oliceridine from a hospital cost perspective, we employed a cost-benefit approach and estimated the net present value (NPV) per patient treated to be $3240 and a benefit–cost ratio (BCR) or return on investment (ROI) to be 3.4. These estimates calculated from the Base Model are summarized in Table 3.
| Input parameter | Oliceridine [0.35 mg with escalation to 0.5 mg for nonresponse] (n = 1000) | Morphine 1 mg (n = 1000) | Difference (oliceridine − morphine) |
|---|---|---|---|
| Cost of pain medication for 24 h/patient | $108.14 | $15.00 | $93.14 |
| Response rate (%) | 66.1% | 73.6% | (7.5%) |
| Escalated to 0.5 mg (%) | 19.4% | N/A | N/A |
| Total number of AEs | 242 | 408 | (166) |
| Respiratory depression (SpO2 <90%), n | 95 | 147 | (52) |
| Vomiting (n) | 128 | 237 | (109) |
| Somnolence (n) | 19 | 24 | (5) |
| Cost of pain medication | $127,181 | $30,558 | $96,623 |
| Cost of adverse outcomes | $528,424 | $852,429 | ($324,005) |
| Total cost | $656,775 | $885,229 | ($228,454) |
The model results shown here were based on an assumed average daily cost of oliceridine of US$100/day for the 0.35 mg dose and $124/day for the 0.5 mg dose, resulting in $108.14 as the weighted cost for day 1. The total cost also includes the cost of antiemetics: $1170 in the oliceridine arm and $2242 in the morphine arm.
AE: Adverse event; SpO2: Peripheral oxygen saturation.
Sensitivity analyses
In the one-way sensitivity analysis approach, the model estimates were resilient to major changes in cost and effectiveness assumptions. The results of the various sensitivity parameters and their impact on the base model outputs are shown in the Supplementary Table 5. The base model estimates were most sensitive to cost changes in the price of oliceridine and the cost assumptions for two of the safety events of interest: the proportion of patients experiencing oxygen desaturation below 90% and the proportion of patients experiencing vomiting. Assumptions related to the analgesic efficacy of oliceridine, the cost of additional pain medications and the cost associated with the adverse outcome of somnolence have only minor effects on the expected total cost savings by the substitution of oliceridine for morphine.
The results of the Monte Carlo simulations showed that the median number of adverse outcomes avoided was predicted to be 162 events per 1000 surgeries, with a range of 151 to 176. Similarly, the median predicted net total cost savings was $206,179, with a range of $155,000 to $280,000 savings from the hospital perspective when oliceridine is used rather than morphine for every 1000 surgeries.
Based on these Monte Carlo probabilistic sensitivity analyses, it can be concluded that the base model estimates are robust and relatively insensitive to variations in the model parameters.
Discussion
The economic model and the analysis show that oliceridine may be expected to have an economic advantage to a hospital in the treatment of acute pain in the postoperative setting compared with the conventional opioid, morphine. Although the cost of pain medication was increased in the oliceridine group, the reduced costs of ORAEs in this group provided an economically meaningful hospital cost offset. The health economic model for oliceridine reported here is based on the risk ratios (differences in adverse outcomes) of the pooled results from two large, multisite, randomized placebo- and active-controlled pivotal Phase III trials. These risk ratios were applied to effectiveness levels recorded for oliceridine in a large, multisite Phase III single-cohort pragmatic safety study. This approach is transparent and avoids issues associated with external validity of using clinical trial results for economic evaluations. The operationalization of the model in Excel makes it possible for readers to examine all data and consider both structural model assumptions and issues related to the validity of the model parameters.
The most important model assumption is that the pooled estimates of events observed in the controlled clinical trials for oliceridine and morphine are valid measures of differential effects expected under real-world practice conditions. While it is recognized that this assumption cannot be tested, the pivotal studies used in the model were the basis for FDA approval of oliceridine and this assumption is employed in clinical practice every time trial evidence is used to inform practice conditions. The model has been limited to capturing differences in categorical analgesic response outcome and is specifically focused on three major ORAEs that have been shown in the literature to be important drivers of resource use related to pain management after surgery [15,16]. We believe that this makes the model quite conservative in its predictions. It is possible that the inclusion of other variables (such as nausea) would increase savings. However, our goal was a conservative estimate that captured the main ‘economic footprint’ of the intervention, not all benefits.
Although use of oliceridine resulted in $96,623 greater expenditures for pain medications, these costs were more than offset by the cost savings associated with the reduced incidence of adverse outcomes and reductions in the overall cost of care ($228,454).
Limitations
Decision analysis models are simplifications of the many factors that affect clinical outcomes and cost under real practice conditions. However, our model was designed for maximal transparency in its structure, was populated with the most conservative parameters and our report clearly describes the origin of the data and the assumptions imbedded in the model. Thus, we are confident that the estimates produced are as conservative and unbiased as it is possible to achieve with the available data.
The time horizon of the model is limited to 24 h. This time frame was selected to reflect the evidence available from the clinical trial. This short time perspective may tend to underestimate the savings associated with very complex procedures for patients with numerous comorbid conditions, such as those included in the PRODIGY study [19], and those with longer postoperative recuperation paths. However, the estimated cost savings may indeed be larger when considering a hospital setting having a large percentage of such patients.
Conclusion
The cost–effectiveness and cost-benefit results presented here are conservative in approach and indicate that oliceridine has a favorable overall impact on the total cost of postoperative care compared with the use of the conventional opioid morphine, despite a modest increase in pharmacy costs.
Future perspective
Pain management post-surgery is changing rapidly as a result of insights gained from the opioid epidemic. New pain medications with fewer side effects will have important roles in the evolving pain management protocols both because of their efficacy against pain, and because medications with fewer side effects may facilitate faster mobilization, earlier feeding, and more rapid discharge to home. Pain management protocols should be assessed using economic modeling studies to ensure that decision makers consider the value that these protocols deliver in terms of benefits, direct protocol costs, and savings associated with decreased adverse events and earlier discharges. Outcomes and costs after discharge should also be examined to better understand how either effective or ineffective postoperative pain management can affect pain trajectory and subsequent patient wellbeing. From the perspective of the hospital facility, our ROI estimates are important to consider to determine the value of new pharmacotherapeutic modalities.
•
Majority of patients undergoing surgery experience postoperative pain and require pharmacological therapies as a component of management.
•
Opioids have long been an important part of therapy for moderate and severe acute pain, however, opioid-related adverse events (ORAEs) associated with conventional opioids can result in poor patient outcomes compromising postoperative recovery.
•
Oliceridine, a new class of μ-opioid receptor agonist, is selective for G-protein signaling (analgesia) with limited recruitment of β-arrestin (associated with adverse events) and may provide a cost-effective alternative versus conventional opioid (e.g., morphine) for postoperative pain.
•
US FDA approval of oliceridine was based on two large, multisite, Phase III randomized placebo- and active (morphine)-controlled clinical trials (APOLLO-1: orthopedic surgery – bunionectomy study; APOLLO-2: plastic surgery-abdominoplasty study); and an additional, prospective, Phase III safety study (ATHENA) among a clinically diverse population of surgical patients (inpatient/ambulatory/emergency departments).
•
Here we have presented a health economics model that compared the clinical outcomes and hospital costs associated with the use of oliceridine versus morphine for the management of acute postoperative pain.
•
We directly compared costs and outcomes of patients managed with demand-dosing of oliceridine (0.35 and 0.5 mg) to those with morphine (1 mg), using a decision tree with a 24-h time horizon, the time period during which the greatest contribution of marginal costs and benefits of postsurgical pain management are expected to materialize; costs were estimated for a sample population of 1000 surgeries allocated to each arm.
•
Adverse outcomes of interest for this health economic analysis were oxygen desaturation (SpO2 <90%), vomiting, and somnolence, AEs that have been well characterized in the literature to be substantial economic contributors in post anesthesia care units (PACUs) with the use of parenteral opioids in the postsurgical setting.
•
To avoid an overestimation of cost of ORAEs in the model, the most recent representative national data projected to 2020 costs were used for cost estimates; the mean marginal cost per day was selected as the analytical parameter of interest.
•
Outputs from the health economic model showed that patients allocated to oliceridine experienced fewer AEs, resulting in US$324,005 less total cost for AEs; although the use of oliceridine resulted in $96,623 greater pharmacy expenditures for pain medications, overall hospital costs decreased.
•
Based on our decision analysis model, oliceridine is expected to have a favorable overall impact on the total cost of postoperative care compared with the use of the conventional opioid morphine, despite a modest increase in pharmacy costs.
Author contributions
KN Simpson developed the model described in this manuscript. MA Demitrack drafted the manuscript. All other authors were involved in revising it critically for intellectual content. All authors approved the final draft that was submitted. All authors had access to the data included in the economic model.
Acknowledgments
The authors would like to thank K Sridharan, MS, employee at Trevena, Inc. for providing editorial assistance during development of the manuscript and T Wandstrat, employee at Trevena, Inc. for assistance during addressing reviewer comments.
Financial & competing interests disclosure
KN Simpson is a consultant for Trevena, Inc. All other authors are employees of Trevena, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
S Parthasarathy of Innovation Communications Group helped with the logistics of submission to the journal, funding for which was provided by Trevena, Inc.
Ethical conduct of research
No institutional review was required as the data included in the model described here was of previously published, de-identified data. The studies adhered to the principles outlined in the Declaration of Helsinki.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 23.64 KB
References
Papers of special note have been highlighted as: • of interest
1.
McDermott KW, Freeman WJ, Elixhauser A. Overview of operating room procedures during inpatient stays in U.S. hospitals, 2014: Statistical Brief #233. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality, MD, USA (2014).
2.
Small C, Laycock H. Acute postoperative pain management. Brit. J. Surg. 107(2), e70–e80 (2020).
3.
Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J. Pain Res. 10, 2287–2298 (2017).
4.
Karaca Z, McDermott KW. High-volume invasive, therapeutic ambulatory surgeries performed in hospital-owned facilities, 2016: Statistical Brief #252. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality, MD, USA (2016).
5.
Carey K, Burgess JF Jr, Young GJ. Hospital competition and financial performance: the effects of ambulatory surgery centers. Health Econ. 20(5), 571–581 (2011).
6.
Waddle JP, Evers AS, Piccirillo JF. Postanesthesia care unit length of stay: quantifying and assessing dependent factors. Anesth. Analges. 87(3), 628–633 (1998).
7.
Echeverria-Villalobos M, Stoicea N, Todeschini AB et al. Enhanced Recovery After Surgery (ERAS): a perspective review of postoperative pain management under ERAS pathways and its role on opioid crisis in the United States. Clin. J. Pain 36(3), 219–226 (2020).
8.
Brown JK, Singh K, Dumitru R, Chan E, Kim MP. The benefits of Enhanced Recovery After Surgery programs and their application in cardiothoracic surgery. Methodist DeBakey Cardiovasc. J. 14(2), 77–88 (2018).
9.
Shafi S, Collinsworth AW, Copeland LA et al. Association of opioid-related adverse drug events with clinical and cost outcomes among surgical patients in a large integrated health care delivery system. JAMA Surg. 153(8), 757–763 (2018).
• Examined the incidence of opioid-related adverse drug events (ORAEs) in patients undergoing hospital-based surgical and endoscopic procedures and reported on the association of ORAEs with clinical and cost outcomes. Reduction in ORAEs in the postsurgical setting were noted as opportunities to reduce cost and improve patient safety.
10.
Sinatra R. Causes and consequences of inadequate management of acute pain. Pain Med. 11(12), 1859–1871 (2010).
11.
Viscusi ER, Skobieranda F, Soergel DG, Cook E, Burt DA, Singla N. APOLLO-1: a randomized placebo and active-controlled Phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the micro-opioid receptor, for management of moderate-to-severe acute pain following bunionectomy. J. Pain Res. 12, 927–943 (2019).
• Pivotal Phase III study of oliceridine in 389 patients with moderate-to-severe acute pain following orthopedic surgery – bunionectomy, treated for up to 48 h.
12.
Singla NK, Skobieranda F, Soergel DG et al. APOLLO-2: a randomized, placebo and active-controlled Phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the mu-opioid receptor, for management of moderate-to-severe acute pain following abdominoplasty. Pain Pract. 19(7), 715–731 (2019).
• Pivotal Phase III study of oliceridine in 401 patients with moderate-to-severe acute pain following plastic surgery-abdominoplasty and treated for up to 24 h.
13.
Bergese SD, Brzezinski M, Hammer GB et al. ATHENA: a Phase III, open-label study of the safety and effectiveness of oliceridine (TRV130), a G-protein selective agonist at the µ-opioid receptor, in patients with moderate-to-severe acute pain requiring parenteral opioid therapy. J. Pain Res. 12, 3113–3126 (2019).
• Phase III, open-label safety study of oliceridine in a real-world population of patients (n = 768) with moderate-to-severe acute pain across a broad range of surgical procedures and nonsurgical medical conditions. Most patients received multimodal analgesic treatment concomitant with oliceridine.
14.
Husereau D, Drummond M, Petrou S et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Value Health 16(2), e1–5 (2013).
15.
Oderda GM, Senagore AJ, Morland K et al. Opioid-related respiratory and gastrointestinal adverse events in patients with acute postoperative pain: prevalence, predictors, and burden. J. Pain Palliative Care Pharmacother. 33(3–4), 82–97 (2019).
• Report of the incidence (per ICD-9 codes) of and factors influencing opioid-related respiratory depression and postoperative nausea and vomiting and associated hospital length of stay and related costs based on adult patients undergoing a surgical procedure in the Premiere Healthcare database.
16.
Barra M, Remák E, Liu DD, Xie L, Abraham L, Sadosky AB. A cost-consequence analysis of parecoxib and opioids vs opioids alone for postoperative pain: chinese perspective. ClinicoEcon. Outcomes Res. 11, 169–177 (2019).
• Analysis of the assessment of direct medical costs related to opioid-related clinically meaningful events (CMEs) based on a Phase III trial comparing parecoxib (COX-2 inhibitor) plus opioids versus opioids alone for the treatment of postoperative pain following major orthopedic, abdominal, gynecologic or noncardiac thoracic surgery.
17.
Morrison B, Kelliher L, Jones C. The economic benefits of enhanced recovery after surgery programmes. Digestive Med. Res. 2, 20 (2019).
18.
US Department of Health and Human Services – Agency for Healthcare Research and Quality (AHRQ). The Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS) dataset. https://hcupnet.ahrq.gov/
19.
Khanna AK, Bergese SD, Jungquist CR et al. Prediction of opioid-onduced respiratory depression on inpatient wards using continuous capnography and oximetry: an international prospective, observational trial. Anesth. Analges. 131(4), 1012–1024 (2020).
• Prospective international observational trial that developed a risk-prediction model for the PRediction of Opioid-induced respiratory Depression In patients monitored by capnoGraphY (PRODIGY trial) and oximetry; study was conducted at 16 sites in USA, Europe and Asia.
20.
Rao VK, Khanna AK. Postoperative respiratory impairment is a real risk for our patients: the intensivist's perspective. Anesth. Res. Pract. 2018, 3215923 (2018).
21.
Saager L, Jiang W, Khanna AK et al. Respiratory depression on general care floors increases cost of care: results from the PRODIGY trial, Abstract #2242. Presented at: Anesthesiology 2019 Meeting. 19–23 October FL, USA, www.asaabstracts.com/strands/asaabstracts/abstract.htm?year=2019&index=17&absnum=1858
22.
Hill RP, Lubarsky DA, Phillips-Bute B et al. Cost–effectiveness of prophylactic antiemetic therapy with ondansetron, droperidol, or placebo. Anesthesiology 92(4), 958–967 (2000).
23.
Phillips C, Brookes CD, Rich J, Arbon J, Turvey TA. Postoperative nausea and vomiting following orthognathic surgery. Int. J. Oral Maxillofac. Surg. 44(6), 745–751 (2015).
24.
Schwartz J, Gan TJ. Management of postoperative nausea and vomiting in the context of an Enhanced Recovery after Surgery program. Best Pract. Res. Clin. Anaesthesiol. 34(4), 687–700 (2020).
25.
Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential elements of multimodal analgesia in Enhanced Recovery After Surgery (ERAS) guidelines. Anesthesiol. Clin. 35(2), e115–e143 (2017).
Information & Authors
Information
Published In
Pages: 1107 - 1119
PubMed: 34240625
Copyright
© 2021 Trevena, Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 30 April 2021
Accepted: 21 June 2021
Published online: 9 July 2021
Keywords:
Topics
Authors
Funding Information
Trevena Inc.
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness and cost-benefit analysis of oliceridine in the treatment of acute pain. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0107
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Dengyun Hu, Panpan Ding, Junjie Liu, Kaixiang Cao, Hongyun Bi, Jinfeng Bao, Linghui Huang, Tingting Zhang, Xin Wang, A two-phase randomized study of oliceridine versus sufentanil for gastrointestinal endoscopy, Frontiers in Pharmacology, 10.3389/fphar.2026.1853405, 17, (2026).
- Xi Liu, Suna Wang, Xiaoxiao Chen, Yuanyuan Tian, Junli Sun, Aizhong Wang, Qi Li, Hui Zhang, A Comparison of Oliceridine versus Sufentanil for Patient-Controlled Analgesia After Total Knee Arthroplasty in Elderly Patients: A Double-Blinded Randomized Controlled Study, Drug Design, Development and Therapy, 10.2147/DDDT.S587944, Volume 20, (1-10), (2026).
- Zhenzhen Zhao, Lingling Ge, Xiaolin Wang, Xiandong Wang, Jie Huang, Yaqin Xiao, Ying Zhang, Yan Zhou, Rui Bao, Jia-feng Wang, EC50 of Remifentanil for Inhibiting Cardiovascular Responses to Tracheal Intubation in Patients Treated by Different Doses of Oliceridine: A Randomized Controlled Trial Using Up-and-Down Sequential Allocation Methodology, Drug Design, Development and Therapy, 10.2147/DDDT.S571007, Volume 20, (1-9), (2026).
- Zongxing Ke, Ying He, Qinqing Hu, Dehao Zheng, Zanmin Yao, Wuzhao Zhou, A comparison of the effects of oliceridine and sufentanil on the quality of recovery after hysteroscopic surgery: a prospective double-blind randomized controlled trial, Journal of Anesthesia, 10.1007/s00540-025-03578-8, 40, 2, (235-244), (2025).
- Kun Yi, Wenjie Sun, Wen Yu, Shibiao Chen, Overview and Prospects of the Clinical Application of Oliceridine, Drug Design, Development and Therapy, 10.2147/DDDT.S525471, Volume 19, (5415-5430), (2025).
- Baoyu Ma, Ying Li, Cuibo Leng, Aozhang Ji, Ning Zhang, Xinyi Tao, Qianqian Cao, Shoushi Wang, A Comparative Evaluation of the Safety and Efficacy of Oliceridine and Sufentanil in Gastrointestinal Endoscopy: A Single-Center, Randomized Controlled Trial, Drug Design, Development and Therapy, 10.2147/DDDT.S512529, Volume 19, (5111-5121), (2025).
- Daniela Arévalo-Villa, Andrea Figueroa Morales, Roberto de Jesús Jiménez-Contreras, Víctor M. Whizar-Lugo, Postoperative Analgesia in Plastic Surgery Procedures, Topics in Postoperative Pain, 10.5772/intechopen.112930, (2023).
- Suzana Bojic, Nebojsa Ladjevic, Ivan Palibrk, Ivan Soldatovic, Ivana Likic-Ladjevic, Winfried Meissner, Ruth Zaslansky, Ulrike M Stamer, Philipp Baumbach, Dusica Stamenkovic, Cost-effectiveness of the Perioperative Pain Management Bundle a registry-based study, Frontiers in Public Health, 10.3389/fpubh.2023.1157484, 11, (2023).
- Neil Daksla, Ashley Wang, Zhaosheng Jin, Abhishek Gupta, Sergio D Bergese, Oliceridine for the Management of Moderate to Severe Acute Postoperative Pain: A Narrative Review, Drug Design, Development and Therapy, 10.2147/DDDT.S372612, Volume 17, (875-886), (2023).
- Han Xie, Si-Huang Chen, Li Li, Wei-Hong Ge, The cost-effectiveness analysis of analgesic treatment options for postoperative pain following laparotomy surgeries, International Journal of Clinical Pharmacy, 10.1007/s11096-022-01473-w, 45, 2, (355-363), (2022).