Willingness to pay for a hypothetical malaria vaccine in Brazil: a cross-sectional study and the implications
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Malaria is an infection caused by protozoa of genus Plasmodium, considered the one associated with increasingly large outbreaks. Methods: A cross-sectional study was conducted with residents in the northern region of Brazil on the willingness to pay (WTP) for a hypothetical vaccine against malaria (effective protection of 80%). Results: Of 616 people interviewed, most interviewees were female (61%) and were employed (97%). The median individual maximum WTP for a hypothetical malaria vaccine was US$11.90 (BRL 50). Conclusion: The northern region of Brazil is one of the largest markets for a malaria vaccine due to its epidemiological relevance. Consequently, economic studies will be important to assist in the assessment of the potential price and value of new vaccines.
Malaria is an acute febrile infectious disease caused by protozoa of the Plasmodium genus, and transmitted to humans by the bite of the female mosquito of the Anopheles genus [1–3]. In Brazil, three species are associated with malaria known as Plasmodium vivax, Plasmodium falciparum and Plasmodium malariae [4].
The WHO considers malaria to be one of the most serious and complex health problems [5]. Data from the Pan American Health Organization (PAHO) showed that 219 million cases of malaria were reported in 90 countries in 2017, with 435,000 deaths due to malaria infections [6]. According to the Ministry of Health in Brazil, between January 2018 and March 2018, 50,877 new cases of malaria were reported in Brazil, while in the same period in 2019, 31,872 cases were recorded in which 99.6% were concentrated in the Amazon region, representing a 38% reduction in occurrence. This reinforces the importance of the government's efforts and initiatives to assist in the reduction of cases [7].
Overall, 194,271 cases of malaria were recorded in Brazil in 2018. Of these cases, there were 191,721 new cases identified in the Northern region, 45,705 of which were in the state of Pará alone, representing 23.8% of the cases in the region [8], with the highest number of cases in the country. The presence of several factors are associated with the proliferation of the transmitting vector in Northern Brazil. These include high temperatures and increasing deforestation in recent years [9].
Malaria is characterized as a symptomatic infection with manifestations such as fever, sweating, headaches, myalgia, nausea and vomiting [1,10]. In Brazil, malaria treatment is available free of charge throughout the country as part of Brazil's publicly funded healthcare system, Unified Health System (SUS). For patients with malaria, medicines such as artemisinin, lumefantrine, mefloquine and artesunate are used to help control the clinical manifestations. Other treatments include chloroquine and primaquine [10].
The National Immunization Program (PNI) created in 1973 by the Brazilian Ministry of Health has as its main objective the reduction of infections in the country Consequently, it offers immunobiological products according to the vaccination calendar and instigates information campaigns and other activities [11]. PNI is considered one of the most important Brazilian programs, and through PNI, 44 products have been made available including vaccines, serums and immunoglobulins. 96% of the vaccines and 100% of the serums provided by the program are produced in Brazil helping to keep costs down [12]. Diseases with high endemic potential, such as malaria, are usually combated with the use of vaccines; however, to date, no effective vaccine for malaria exists [13].
In 2019, the Brazilian Ministry of Health, together with the Bill and Melinda Gates Foundation, allocated R$10.2 million (BRL) and US$1 million, respectively, to conduct research aimed at the diagnosis and treatment of malaria, integrated and selective vector control and health promotion. In addition, in Brazil R$35,556,780 (BRL) was made available involving 24 states, with the objective of contributing to activities regarding the prevention, control and elimination of malaria and for surveillance activities for visceral leishmaniasis and Chagas disease [14]. Research has been initiated to search for therapies that are safe and effective against malaria [15,16] as well as the potential for future vaccines [17]. The development and commercialization of a vaccine against malaria, with affordable prices for the population living in endemic areas, is necessary to enhance control and eradication against this infection, which represents an increasing public health burden, with the prospect of significant cost savings for SUS in the future.
In recent years, several research programmes and studies have been conducted to develop a safe and effective vaccines for malaria prevention [18,19]. Among candidate vaccines, the most advanced vaccine is Mosquirix (RTS, S/AS01), This vaccine is Phase III clinical trials including 15,459 volunteers in seven countries (Burkina Faso, Gabon, Malawi, Mozambique, Ghana, Tanzania, Kenya) [20,21]. Overall, Mosquirix has been in development since 1987, with additional Phase III clinical trials conducted in recent years [21,22]. Studies indicate a schedule of administration in three doses, with a 6-month interval, followed by a booster dose at the eighteenth month [21,23]. In addition, the vaccine is designed to immunize only against Plasmodium falciparum [24,25] and showed an efficacy of 55.8% in children (5–17 months) and 31.3% in babies (6–12 weeks), observed at 12 months [25,26]. After 18 months, there was a reduction in this protection to 28.3 and 18.3%, in these respective groups [27]. However, with the application of a booster dose, the effectiveness was increased to 39.0% in children (5–17 months) [20,28]. Despite presenting limited effectiveness, RTS, S/AS01 has been shown to induce immunological resistance in vaccinated individuals and to have contributed to a 36% reduction in hospital admissions [21].
In Brazil, for a new pharmaceutical product to be placed on the market, registration with the National Health Surveillance Agency (ANVISA) is essential through validating its quality, efficacy and safety [29,30]. After registration, the Medicines Market Regulation Chamber (CMED) is responsible for defining the maximum prices for commercialization in the private market [31,32]. In their evaluation, CMED undertakes a survey of prices in a number of countries including Australia, Canada, France, Greece, Italy, New Zealand, Portugal, Spain and USA. The maximum price in Brazil cannot exceed the lowest price in these countries [33]. Following pricing negotiations, pharmaceutical companies can request that their products be included in the list of items made available by SUS. The pharmaceutical company responsible for the technology submits a series of documents to be evaluated by the National Technology Commission (CONITEC). Within this, CONITEC considers several studies involving analyzes of efficacy, safety and cost–effectiveness to inform decision-making about the value of this new technology for SUS and, consequently, the Brazilian population [32]. This includes willingness-to-pay (WTP) studies [31,34].
The Brazilian private market for health insurance is regulated by the National Regulatory Agency (ANS) for Private Health Insurance and Plans, which works on behalf of the Ministry of Health [35]. Private health insurance can either be purchased individually or obtained as a work benefit. The Brazilian people that decide to purchase private health insurance may still access public health services if they wish or need [36]. Having said this, Brazil has one of the largest and most complete public health systems in the world, treating basic patients to those with more complex needs including organ transplantation [37]. Despite this, SUS has some acknowledged weaknesses. Importantly, long waiting times for consultation with a specialist means that many patients purchase private health plans to ensure timely access to healthcare [33]. There are also concerns with the routine availability of medicines in the public healthcare system.
Considering the future possible introduction of vaccine for malaria, a WTP study was proposed to examine the potential value of a vaccine for malaria from the Brazilian consumers perspective. Such an approach aims to estimate the maximum individual value to be allocated to a program, medical intervention or specific treatment, in order to more fully examine its monetary valuation. This type of study provides an opportunity to gauge the potential market value of such an intervention, in addition to supporting possible future decision-making [31,38,39].
Material & methods
A WTP study using contingent valuation was conducted to measure the maximum amount a person would be willing to offer for a hypothetical malaria vaccine [40]. A questionnaire was administered which required respondents to be provided with information regarding the characteristics of the intervention, as well as the condition and aspects relevant to the clinical context, before answering WTP questions [38]. To ensure transparency and comparability, it was essential that all participants received the same guidelines through training of all interviewers [31,38,40].
A questionnaire (Supplementary Material) with open and closed questions was developed by the researchers building on previous WTP studies involving licensed vaccines in Brazil [31] as well as hypothetical vaccines for Chikungunya [41] and Zika [34]. The questionnaire also built on previous publications [31,34,41]. In addition, the information about the mean effective protection for this hypothetical vaccine (80%), as well as the possibility of local (e.g., swelling at the site of application and pain) and systemic (e.g., fever and headache) adverse were included in the questionnaire.
Study design & location
The survey was conducted in 10 cities (Abaetetuba, Baião, Belém, Itupiranga, Jacundá, Marabá, Parauapebas, Rondón do Pará, São Domingos do Araguaia and São João do Araguaia) in the state of Pará, the ninth most populous state in Brazil, which in 2018, had 8.5 million inhabitants. The state of Pará is the most inhabited state in the Northern Region of Brazil which also presented the fourth worst Human Development Index (HDI) in the country, 0.698 [42]. In 2018, the region's average per capita monthly income was US$233.24 (863 BRL) [43,44]. The Northern region was chosen for this research since, as mentioned, it has the highest malaria registration rate (99.62%) in Brazil with Pará being one of the most endemic states [8].
The interviews were conducted by undergraduates of health courses, mainly by students of the Bachelor of Public Health course from the Federal University of the south and southeast of Pará (Unifesspa). All interviewees were trained by the researcher responsible for this study (IPDG) according to recommendations from previously published studies [31,34,40,41,45,46].
Data collection instrument
The WTP technique involves the application of a questionnaire with a presentation to the respondent to the characteristics of the disease and the hypothetical intervention of interest. As mentioned, it was reinforced that it was essential that all participants received the same information [31,34,38,39,45,46].
The questionnaire was divided into five sections: questions to test participants' knowledge regarding malaria; information about the disease, intervention and alternatives for prevention of the disease; questions to assess the understanding of the information provided; discrete choice, bidding game and open-ended questions [38] which included questions to identify whether individuals would pay US$23.77 (100 BRL) for the single dose of the hypothetical malaria vaccine, as well as questions to estimate the range of values that individuals would be willing to pay for the vaccine. Section five of the questionnaire included demographic and socioeconomic questions.
For the discrete choice technique, a value of US$23.77 (100 BRL) was established for a single dose of the vaccine for the prevention of malaria based on a series of surveys, analyzing the price list of CMED and from the factory price (PF) of vaccines in Brazil. It is noteworthy that Brazilian drugstores, as well as laboratories, distributors and importers, cannot charge more for medicines and vaccines above the price established by CMED. In addition, the list of maximum prices allowed for the sale of medicines/vaccines is made available for consultation by patients on a monthly basis [47]. This study selected the value of (100 BRL/discrete choice) considering a price observed, in general, for some vaccines (e.g., yellow fever) applied to the private market [48].
All questions related to the research context or difficulties in understanding any aspects applied to the interview were clarified by the interviewers beforehand. This included information related to the transmission, prevention and clinical manifestations of malaria and the effectiveness of the hypothetical vaccine (80%). Additionally, after providing context about malaria, a vaccine and the research question, some questions were asked to verify if the participants fully understood the content of the study. In addition, it was clarified during the interview that the vaccination scheme would be a single dose. An illustrative figure was used to facilitate understanding of the percentage of protection of the hypothetical vaccine against malaria.
Selection criteria & data collection
The selection of the respondents was performed in a random manner, and involved individuals from high circulation areas such as shopping mall, markets, fairs and squares. If there is a greater uncertainty that 50% of respondents agree to pay US$23.77 (100 BRL) for this hypothetical vaccine, a minimum of 600 respondents would be required in this study. This was based on a margin of error of 5% to a 95% CI. The value of US$23.77 (100 BRL) was utilized considering a mean value for the prices of vaccines approved in Brazil. The number of individuals to be interviewed in each of the ten cities was defined according to the relative population size of each the municipalities.
As previously reported, the respondents may or may not have a history of malaria. However, at the time of the interview participants could not have symptoms or a malaria diagnosis according to recommendations in previous publications [31,34,41]. As an inclusion criteria, individuals had to declare an income and be at least 18 years old. Individuals under 18 years and those with no income, individuals who would not use the vaccine even if it were freely available, and those who were willing to pay more than twice the amount of their declared monthly income, were excluded. This reinforces the fact that the values obtained in this economic approach need to be feasible and ‘acceptable’ within the economic scenario presented by each respondents [38]. In other words, this technique searches individual values that can be potentially applied to the purchase of this hypothetical product, considering the social, economic and clinical perceptions of the participants. All inclusion and exclusion criteria used in this study have been endorsed in previous publications [31,34,41,45,46] and the literature [38].
Data analysis
The WTP for a hypothetical malaria vaccine was estimated from the maximum median value declared by individuals who were willing to pay any amount greater than or equal to zero. The median of the maximum WTP among the groups defined by the covariates was compared using the Mann–Whitney test (two groups) or the Kruskal–Wallis test (three or more groups). The level of significance was set at 5%. The median ratio of the maximum WTP for the hypothetical malaria vaccine was assessed including all socioeconomic variables. For analysis involving the amount of WTP and education, the following categories were used ‘never studied or did not complete primary education’, ‘completed primary education’, ‘completed secondary education’ and ‘completed higher education or more’. This is in line with previous studies [31,34,41,45,46].
In addition, the frequency of participants who did or did not have private health insurance at the time of the interview was assessed. This is because participants who had private insurance may well be willing to pay more for a new effective vaccine. According to previous publications [49,50], individuals with higher income and education level demonstrate higher WTP for products and services. In addition, in study conducted by Godói and collaborators (2017), respondents with health insurance had higher income levels affecting their WTP values [31]. According to the National Supplementary Health Agency (ANS), which regulates private health insurance in Brazil, in Pará the coverage of private health insurance includes 807,453 beneficiaries or 10.3% of the State and 10.6% across the northern region. The national profile was 24.2% of the population for the same period [51]. In addition, the WTP of interviewees was evaluated controlling for variables including history of malaria, age and gender. For comparison purposes, the conversion value established by the Central Bank of Brazil, currency converter (BCB; 2020: US$1 = 4.2064 BRL) [52]. In addition, Microsoft Excel 2010 and Minitab 17 were used as a tool for statistical analysis.
Ethics statement
All interviews were conducted after reading and signing an informed consent form. In addition, all researchers of the project signed a confidentiality agreement prior to the inter-views. This study was approved by the Ethics and Research Committee of the Federal University of Pará (UFPA), under CAAE registration number 12943619.500.8607.
Results
Population characteristics
Of the 616 participants, interviews were conducted with individuals aged between 18 and 81 years old, with an average age of 37.7 ± 12.9 (SD) years, 39% were male and 97% worked at the time of the interview. Additionally, 8.5% declared a history of malaria, in which they used only the public health service, 14.5% reported that family members were affected by the disease at home, and 28.2% of the interviewees had a family income between one and two minimum wages (Table 1).
| Variable | n | (%) |
|---|---|---|
| Age (years), mean (standard deviation) | 37.7 | 6.1 |
| Male | 236 | 39.0 |
| Has children | 432 | 72.0 |
| Education level | ||
| Had never attended school | 6 | 1.0 |
| Completed elementary school | 195 | 31.7 |
| Completed high school | 307 | 49.8 |
| Completed college or more | 98 | 15.9 |
| Currently working | 583 | 97.0 |
| Have private health insurance | 162 | 27.0 |
| Had malaria | 51 | 8.5 |
| Reported that other people in the household had malaria | 84 | 14.5 |
| Family income (number of minimal wages†) | ||
| <1 | 41.6 | |
| 1–2 | 28.2 | |
| 2–3 | 11.9 | |
| 3–5 | 7.3 | |
| 5–10 | 3.1 | |
| 10–20 | 0.6 | |
| >20 | 0.0 |
7.3% of the respondents refused to respond to questions regarding family income. The difference to reach 100% for all questions is due to answers such as ‘don't know’ and ‘don't want to answer’; Brazilian minimum wage in 2019 was 998.00 BRL (US$237.25) per month.
WTP for a hypothetical malaria vaccine
Among the 616 respondents, 14 reported that they would not use the vaccine even if it was available for free. The reasons associated with non-use included efficacy concerns (14.3%), safety concerns (35.7%) and the non-use of any vaccine (50%). Additionally, one respondent was excluded as the respondent was found to be under 18 years of age, as demonstrated in the Figure 1. In this context, 601 respondents were considered eligible for the WTP analysis, of which 50.7% had completed high school; 26.9% reported having health insurance and 24.7% were self-employed.
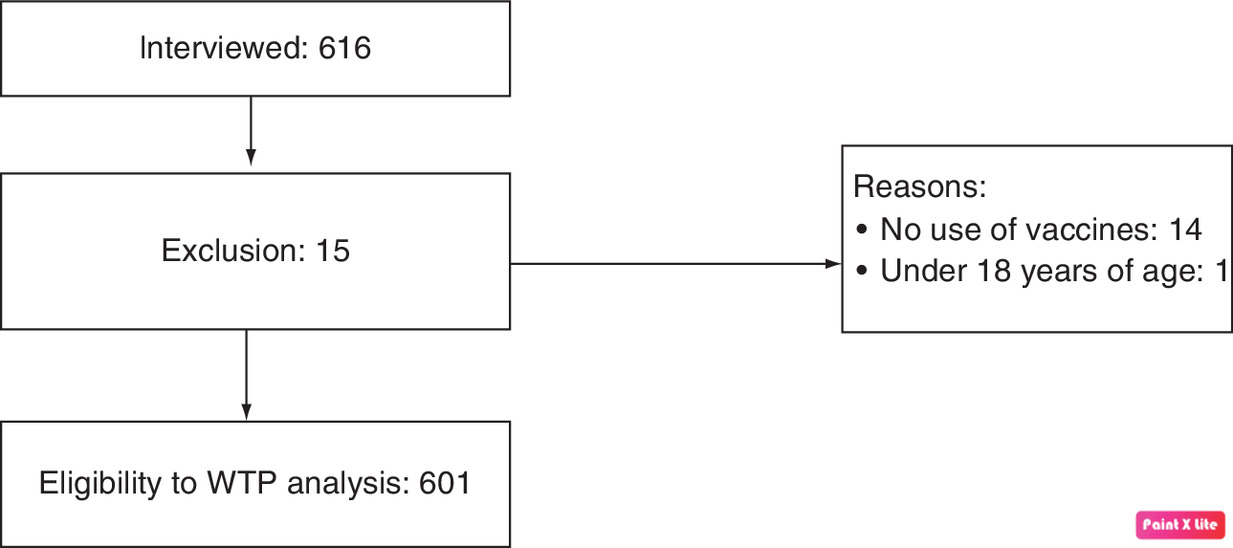
Figure 1. Flowchart of willingness to pay analysis applied to the respondents.
The legal penal age in Brazil is 18 years; WTP: Willingness to pay.
It was found that 46% of participants were willing to pay US$23.77 (100 BRL) for a single dose vaccine regimen. From the results, 30.8% of respondents were willing to pay between US$11.88 (50 BRL), to US$47.54 (200 BRL). The minimum and maximum WTP for a single dose malaria vaccine obtained in our study were 0 and 2000 BRL.
The value of WTP for the hypothetical malaria vaccine was US$11.88 (50 BRL) for the single dose regimen, which means that 50% of respondents declared the maximum value of WTP equal or less than US$11.88 (Figure 2).

Figure 2. Cumulative percentage of the willingness to pay for a hypothetical malaria vaccine according to the reported maximum values.
BRL: Brazilian real.
The comparative analyzes between the WTP medians were significant at the 5% level, namely: income (p < 0.001); history with malaria (p < 0.001); education (p = 0.004) and working at the time of the interview (p = 0.028), as presented in Table 2.
| Variable | Willingness to pay | p-value |
|---|---|---|
| Per capita household income | 200.00 BRL | 0.001 |
| Education level | 200.00 BRL | 0.004 |
| Gender | 50.00 BRL | 0.37 |
| Insurance health | 100.00 BRL | 0.55 |
| Working at the moment of the interview | 50.00 BRL | 0.028 |
| History with malaria | 200.00 BRL | 0.001 |
Individuals who had a history of malaria or knew someone who had the disease had a higher WTP to the hypothetical vaccine (US$47.54/200 BRL) compared with those who never had the disease and/or did not know anyone affected with malaria (US$11.88/50 BRL; p < 0.001) (Figure 3).
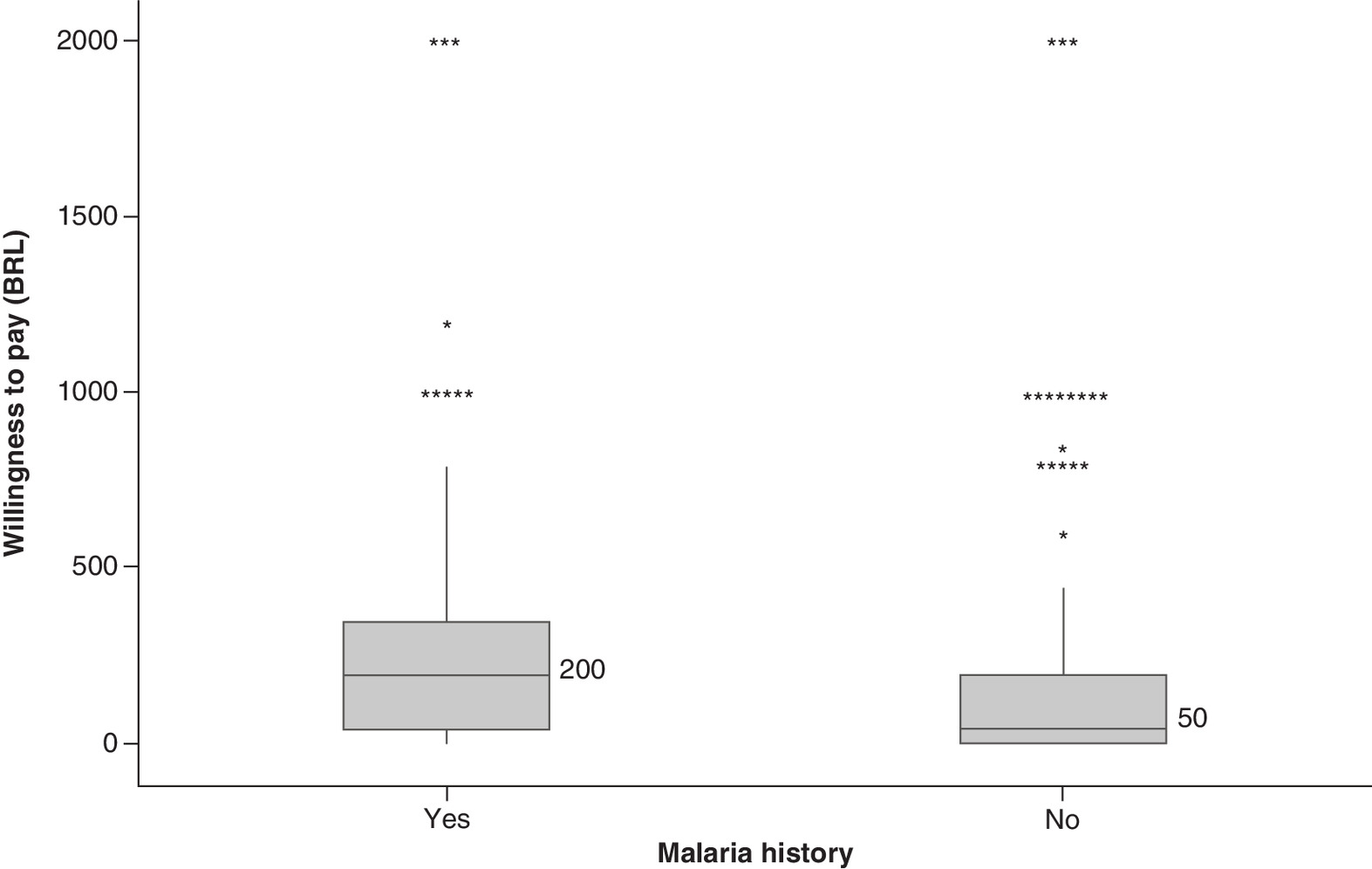
Figure 3. Willingness to pay for hypothetical vaccine for malaria according to malaria history.
BRL: Brazilian real.
The participants with a higher level of education declared a higher WTP for the hypothetical vaccine for the prevention of malaria (US$47.54/200 BRL), compared with those with the respondents with less education (US$10.69/45 BRL; p = 0.004) as shown in Figure 4.
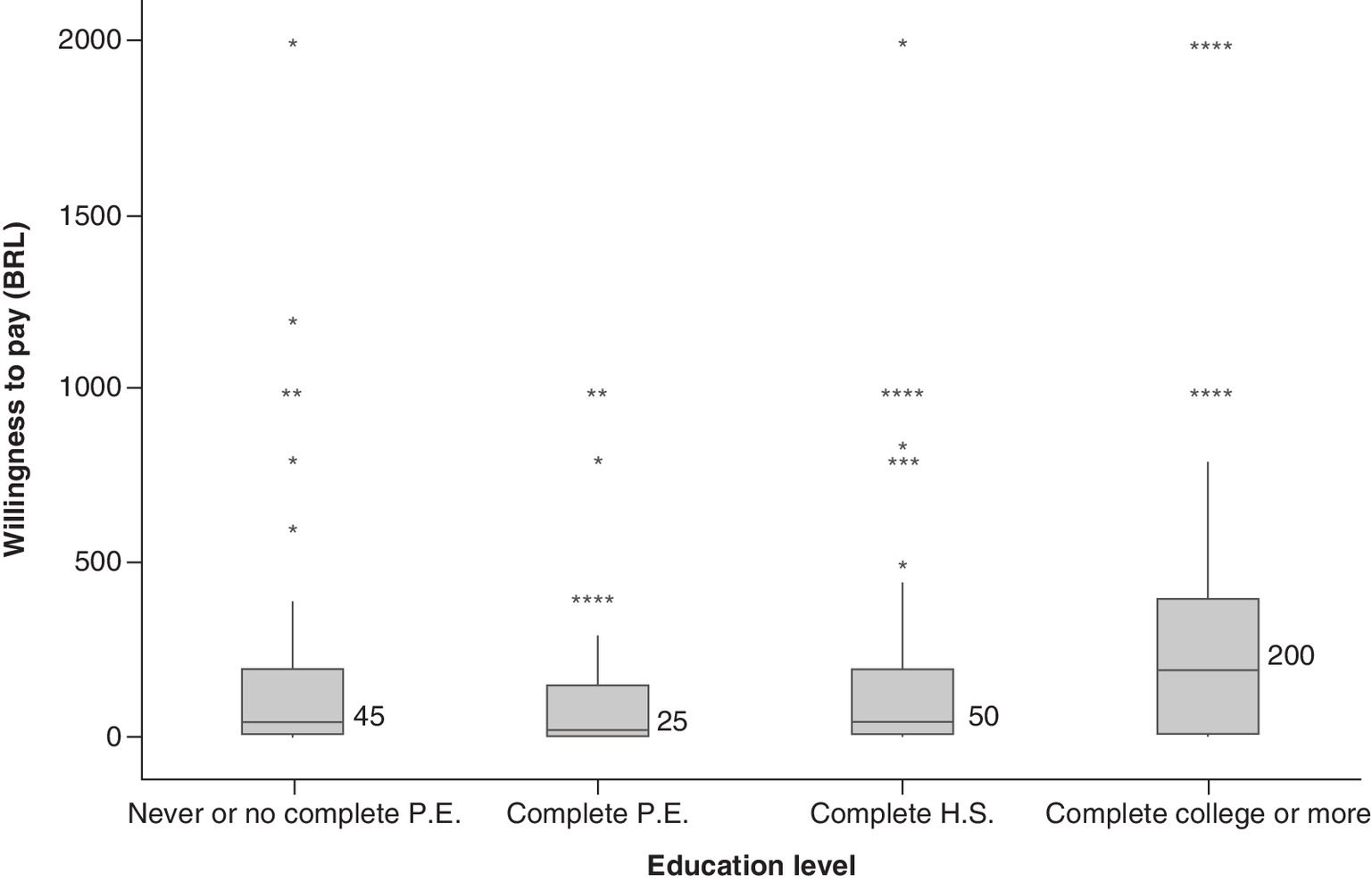
Figure 4. Box plots indicating willingness to pay for hypothetical vaccine for malaria according to education level.
BRL: Brazilian real; PE: Primary education; HS: High school.
Discussion
We believe this is the first study conducted in Brazil to ascertain the WTP of a potential vaccine against malaria to help guide future decision making in Brazil once a vaccine becomes available. We found the WTP for the hypothetical malaria vaccine, in a single dose, with 80% effectiveness was US$11.88 (50 BRL). A hypothetical efficacy of 80% was based on effectiveness levels of vaccines already incorporated and made available to the Brazilian population by SUS, and similar to other studies conducted in the country for the same scenario [31,41]. This means that 50% of the interviewees declared the maximum amount to be paid, equal or less than US$11.88. The median value is generally used to assess the WTP [31,34,39,40,53,54] to minimize the interference of extreme values verified in the data collection. Our WTP figure is appreciably higher than the study conducted in the Peruvian Amazon region where 60% of the interviewees declared a WTP of US$2.21 for a hypothetical malaria vaccine with 70% effectiveness [55] and in Nigeria where the WTP for three hypothetical malaria vaccines, with efficacies of 75, 85 and 95%, was US$6.77; 6.70 and 5.06, respectively [56]. The authors indicated that the WTP was influenced by vaccine price, socioeconomic status, and those who experienced illness among community members [56]. In this context, we did find that the interviewees who had a history of malaria had a higher WTP for this hypothetical vaccine (p < 0.001), in agreement with other publications [56,57]. Similar to other studies [31,34,41], there appeared to be no correlation between age and gender regarding WTP for this hypothetical vaccine.
However, we found a statistical correlation between the income variable (p < 0.001) and the WTP value, similar to the other publications applied to the first dengue vaccine approved in Brazil (p = 0.003) [31]; a hypothetical Zika vaccine (p < 0.001) [34] and a hypothetical chikungunya vaccine (p = 0.002) [41] conducted in the country. Additionally, it was found that the higher the education level (p = 0.004), the higher the reported WTP values for the vaccine. In this study, the percentage of families that declared a family income below the minimum wage was 41.6%, similar to that seen generally for the Brazilian people living in the Northern region who have an average income of 883 BRL, lower at BRL 807 for the state of Pará [43,44]. In addition, 27% of respondents reported having a private health plan, similar with the national average of 28.5% [58]. In addition, the leve of private health plans in most cases is associated with the industrialization level, income and employment levels in a region [36,59]. This reinforces the low coverage rate of private insurance health in the North Region at 10.6% where 55.3% of the population seeks health services in the public health system [36,58]. This lower coverage rate (10.6%) can be associated with the low income of the inhabitants of this region when compared with other studies conducted in the southeast region in the country [31,34]. In addition, wide rural areas and low demographic density can be associated with the lower industrialization levels of the northern region of Brazil [59,60].
Yasunaga and collaborators demonstrated that the choice of treatment for tropical diseases depends on cultural, economic and social reasons [61]. Another study showed that WTP is generally related to income similar to our findings that demonstrated individuals with higher income had higher WTP for the hypothetical malaria vaccine (p < 0.001) [60]. In addition, some studies demonstrated that inhabitants of endemic regions are willing to pay more, and were more likely to accept a hypothetical vaccine [34,38,62].
According to the National Institute for Space Research [63], there were approximately 10,129 km2 of deforestation in the Brazilian Legal Amazon (ALB), from August 2018 to June 2019, with 84.56% corresponding to the states of Pará, Mato Grosso, Amazonas and Rondônia, in which Pará contributed 41.19% of this rate [63]. A team from the Institute of Applied Economic Research (IPEA), associated deforestation data with disease statistics in 773 municipalities of the Brazilian Legal Amazon, between 2004 and 2012, and concluded that for each 1% of de-forestation per year, an increase of 23% was observed in malaria cases [64].
Recently, the WHO recommended the large-scale use of RTS, S/ASO1 vaccine in sub-Saharan Africa and in areas of moderate and high transmissibility of the disease caused by P. falciparum. The vaccination program will be instigated in children aged from 5 months of age, adopting a four-dose schedule. This immunizing agent has demonstrated satisfactory results in studies involving three African countries, with a 30% reduction in severe cases of malaria in children and represents a milestone in the history of malaria [65].
Overall, Brazil has a comprehensive immunization program with coverage for a considerable number of infections. In the future, we believe public health systems purchasing the malaria vaccine should conduct cost-effectiveness and budget impact analyzes to inform the optimal use of healthcare resources. Comparisons with other vaccines prices and effectiveness for diseases with similar burden may also contribute to political decisions regarding the possibility of incorporating this technology into public health systems at acceptable and reasonable prices.
There are several limitations associated with this study. Firstly, we discussed a hypothetical vaccine and some participants may not have been fully motivated to express the real value that they would be willing to pay. Second, this research was undertaken based on a vaccine with 80% effectiveness, which means that vaccines with different effectiveness rates may well have a different WTP value, and third the results in this study may not be representative of other regions of the country. However, we deliberately chose the region with the highest prevalence of malaria. In addition, the profile of the respondents resembles some aspects with the Brazilian population including a higher percentage of women (61%), a low number of individuals with no education (1%) and who only completed primary education (31.7%). In addition, the higher percentage of individuals with insurance health at 27.5% in our study compared with the Northern region and Pará state, respectively, 10.6 and 10.3%, is nearer the national average for Brazil, and can be associated with a higher percentage of respondents with employment at the time of the interview at 97%. This higher rate of private insurance we believe enhances the contextualization of our study results to Brazil. Overall, despite these limitations, we believe our findings are robust and should help enhance discussions regarding future pricing of vaccines for malaria when available.
Conclusion
This is the first study to address the WTP for a hypothetical malaria vaccine in Brazil. Of 601 respondents, 50% of respondents demonstrated the WTP of US$11.88 (50 BRL) for a hypothetical vaccine with an 80% effectiveness. Individuals who had a history of malaria or knew someone who had the disease had a higher WTP of US$47.54 (200 BRL), similar with respondents who had a higher level of education (200 BRL). The findings should stimulate and reinforce the need for governmental initiatives and industry to accelerate the development of a vaccine for malaria and its potential pricing.
Future perspective
In the coming years, there will be advances in the development of a malaria vaccine. In the near future, we hope for promising safety and efficacy results of Mosquirix (RTS, S/AS01) as well other vaccines candidates. A vaccine that is safe and effective to combat malaria will be welcomed in Brazil and wider considering the 219 million cases of malaria reported in 90 countries in 2017 and 435,000 deaths due to this infection. We also believe that WTP studies, such as these, combined with submissions by pharmaceutical companies, will help guide subsequent pricing and reimbursement decisions in Brazil for possible new medicines including new vaccines to be incorporated into the Brazilian Public Health System. In addition, we will be monitoring the developments of new vaccines, which represent an important approach for endemic countries. In this context, we recommend that the search for a vaccine and a price based on the profile of consumers continue. In this respect, we continue to support more efforts and government investments from the most affected countries and companies to encourage the development of medicines and vaccines for malaria. This is the first study conducted in the context of the willingness to pay for a hypothetical malaria vaccine in Brazil, and can contribute to decision-making about potential prices for a future vaccine once it becomes available in the country.
•
In the most recent outbreak in Brazil, 82,479 new cases have been reported considering only the period between January and March of 2018 and 2019 greatest for the Amazon region (north of the country).
•
In Brazil, malaria treatment is available free of charge throughout the national territory at SUS units, and the development of an effective vaccine for malaria prevention represents an important strategy for the control of the disease.
•
This study estimated the WTP of Brazilian consumers for a hypothetical malaria vaccine through an analysis of contingent valuation.
•
50% of the interviewees were willing to pay US$11.88 (50 BRL) for the hypothetical vaccine against malaria.
•
The study can contribute to the pricing of any potential vaccine once available, and the socioeconomic data might be useful in the discussions about the introduction of the vaccine onto the SUS in Brazil and into the market.
Author contributions
MJL da Costa, GC Nascimento, TS Athie, EA Reis and IPD Godói undertook the study and MJL da Costa, EA Reis and IPD Godói conducted the analysis, with BB Godman and A Martin contributing to the literature review. MJL da Costa, GC Nascimento, TS Athie, EA Reis, J de Sales Silva, AP Martin, B Godman and IP Dias Godói subsequently revised the draft and produced the final and revised manuscripts. All authors approved the final and revised manuscripts. All authors also agree to be accountable for all aspects of the work.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (supplementary materials.pdf)
- Download
- 89.56 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Mace KE, Arguin PM, Tan KR. Malaria surveillance – United States. MMWR Surveil. Summ. 67(7), 1–28 (2018).
• Important to complement our knowledge of malaria.
2.
Brasil. Ministério da Saúde. Malária: o que é, causas, sintomas, tratamento, diagnóstico e prevenção (2013). http://saude.gov.br/saude-de-a-z/malaria
3.
Schindler T, Robaina T, Sax J et al. Molecular monitoring of the diversity of human pathogenic malaria species in blood donations on Bioko Island, Equatorial Guinea. Malar. J. 18(1), 9 (2019).
4.
Fundação Osvaldo Cruz. Malária (2013). https://agencia.fiocruz.br/malária
• Important to complement our knowledge of malaria.
5.
World Health Organization. Management of severe malaria (2012). https://apps.who.int/iris/bitstream/handle/10665/79317/9789241548526_eng.pdf?sequence=1
6.
Organização Pan Americana da Saúde. Folha Informativa Malária (2019). https://www.paho.org/bra/index.php?option=com_content&view=article&id=5682:folha-informativa-malaria&Itemid=812
• Important to complement our knowledge of malaria.
7.
Brasil. Agência Brasil: brasil reduz 38% casos de malária em relação a 2018 (2019). https://www.saude.gov.br/noticias/agencia-saude/45391-brasil-reduz-em-38-casos-de malaria-em-relacao-a-2018
8.
Brasil. Brasil reduz em 38% casos de malária em relação a 2018 (2019). https://www.gov.br/pt-br/noticias/saude-e-vigilancia-sanitaria/2019/04/brasil-reduz-em-38-casos-de-malaria-em-relacao-a-2018
9.
Parente AT. Incidence of Malaria in the State of Pará and its relationship with regional climatic variability. Masters dissertation. 99 (2007).
10.
Brasil. Guia de tratamento da malária no Brasil (2020). https://portalarquivos2.saude.gov.br/images/pdf/2020/janeiro/29/af-guia-tratamento-malaria-28jan20-isbn.pdf
11.
Brasil. Ministério da Saúde. Critérios para orientar o processo de decisão para introdução da vacina contra dengue no Programa Nacional de Imunizações (PNI) (2016). https://portalarquivos2.saude.gov.br/images/pdf/2016/maio/05/relatorio-01-criterios-orientar-decisao-vacina-dengue.pdf
12.
Domingues CMAS, Teixeira AMS. Vaccine coverage and vaccine-preventable diseases in Brazil from 1982 to 2012: advances and challenges of the National Immunization Program. Epidemiologia e Serviços de Saúde 22(1), 9–27 (2013).
13.
Pan American Health Organization. Malária (2016). https://www.paho.org/bra/index.php?option=com_content&view=article&id=5287:malaria-2&Itemid=875
•• Important reference source associated with the development of vaccines for malaria.
14.
Brasil. Ministério da Saúde. Boletim Epidemiológico (2020). https://antigo.saude.gov.br/images/pdf/2020/April/24/Boletim-epidemiologico-SVS-17-.pdf
15.
Aguiar ASC, Rocha EMM, Souza NB, França TC, Krettli AU. New approaches in antimalarial drug discovery and development. Mem. Inst. Oswaldo Cruz. 107(7), 831–845 (2012).
16.
Andrews KA, Wesche D, McCarthy J et al. Model-Informed drugs development for malaria therapeutics. Annu. Rev. Pharmacol. Toxicol. 58, 567–582 (2018).
17.
Fundação Osvaldo Cruz. Resultados de pesquisa podem ajudar no desenvolvimento de vacina contra malária. (2018). https://portal.fiocruz.br/noticia/resultados-de-pesquisa-podem-ajudar-no-desenvolvimento-de-vacina-contra-malaria
18.
Hoffman SL, Vekemans J, Richie TL et al. The march toward malaria vaccines. Am. J. Med. Ant. 49(6S4), S319–S333 (2015).
19.
Frimpong A, Kusi KA, Ofori MF, Ndifon W. Novel strategies for malaria vaccine design. Front Immunol. 9, 2769 (2018).
20.
Condessa ALC. Antimalarial vaccination: RTS, S and inactivated sporozoite vaccines from Plasmodium falciparum. Dissertation (Integrated Master in Medicine) – University of Lisbon 41 (2018).
•• Important reference source associated with the development of vaccines for malaria.
21.
Van den Berg M, Ogutu B, Sewankambo NK, Biller-Andorno N, Tanner M. RTS, S malaria vaccine pilot studies: addressing the human realities in large-scale. clinical trials. Trials 20(1), 316 (2019).
22.
Laurens MB. RTS, S/AS01 vaccine (Mosquirix). An overview. Hum. Vaccin. Immunother. 16(3), 480–489 (2020).
23.
Bell GJ, Loop MS, Mvalo T et al. Environmental modifiers of RTS, S/AS01 malaria vaccine efficacy in Lilongwe, Malawi. BMC Public Health 20(1), 910 (2020).
24.
Chandramohan D, Dicko A, Zongo I et al. Seasonal malaria vaccination: protocol of a phase 3 trial of seasonal vaccination with the RTS, S/AS01 vaccine, seasonal malaria chemoprevention and the combination of vaccination and chemoprevention. BMJ Open 10(9), e035433 (2020).
25.
Kazmin D, Nakaya HI, Lee EK et al. Systems analysis of protective immune responses to RTS, S malaria vaccination in humans. Proc. Natl Acad. Sci. USA 114(9), 2425–2430 (2017).
26.
Dobaño C, Sanz H, Sorgho H et al. Concentration and avidity of antibodies to different circumsporozoite epitopes correlate with RTS, S/AS01E malaria vaccine efficacy. Nat. Commun. 10(1), 2174 (2019).
27.
Collins KA, Snaith R, Cottingham MG, Gilbert SC, Hill AVS. Enhancing protective immunity to malaria with a highly immunogenic virus-like particle vaccine. Sci. Rep. A7, 46621 (2017).
28.
Vandoolaeghe P, Schuerman L. The RTS, S/AS01 malaria vaccine in children 5 to 17 months of age at first vaccination. Expert Rev Vaccines. 15(12), 1481–1493 (2016).
29.
Santana RS, Lupatini EO, Leite SN. The regulation and adoption of health technologies under Brazil's Unified Health System: barriers to access to medicines for diseases of poverty? Ciên Saúde Coletiva 22(5), 1417–1428 (2017).
30.
Brasil. Registros de novos medicamentos: saiba o que e preciso (2020). http://portal.anvisa.gov.br/noticias/-/asset
31.
Godói IP, Santos AS, Brandão CMR et al. Consumer willingness to pay for Dengue vaccine (CYD-TDV, Dengvaxia®) in Brazil; implications for future pricing considerations. Front. Pharmacol. 8(41), 1–9 (2017).
32.
Brasil. Comissão Nacional de Incorporação de Tecnologias no Sistema Único de Saúde. A comissão (2020). http://conitec.gov.br/entenda-a-conitec-2
33.
Farias CML, Giovanella L, Oliveira AE, Santos Neto ET. Tempo de espera e absenteísmo na atenção especializada: um desafio para os sistemas universais de saúde. Saúde em Debate 43(Suppl. 5), 190–204 (2019).
34.
Muniz Júnior RL, Godói IP, Reis EA et al. Consumer willingness to pay for a hypothetical Zika vacine in Brazil and the implications. Expert Rev. Pharmacoecon. Outcomes Res. 19(4), 473–482 (2018).
35.
Brasil. Agência Nacional de Saúde Suplementar. Quem Somos (2020). http://www.ans.gov.br/aans/quem-somos
36.
Albuquerque C, Piovesan MF, Santos IS, Martin AC, Fonseca AL, Sasson D. The current situation of the private health plans and insurance Market in Brazil and trends for the future. Ciên Saúde Coletiva 13(5), 1421–1430 (2008).
37.
Brasil. Sistema Único de Saúde: estrutura, princípios, e como funciona (2020). http://www.ans.gov.br/aans/quem-somos
38.
Haab T, McConnell K. Valuing Environmental and Natural Resources: the economics of non-market valuation. New Horizons in Environmental Economics. Edward Elgar Publishing Limited, UK (2002).
•• Important to complement our knowledge of willingness to pay approach.
39.
Lee JS, Mogasale V, Lim JK, Carabali M, Sirivichayakul C. Tho le H. A multi-country study of the household willingness-to-pay for Dengue Vaccines: household surveys in Vietnam, Thailand, and Colombia. PLoS Negl. Trop. Dis. 9(6), e0003810 (2015).
40.
Drummond M, Sculpher M, Torrance G, O'Brien B, Stoddard G. Methods for the economic evaluation of health care programmes. Oxford University Press, UK (2015).
41.
Sarmento TTR, Godói IP, Reis EA et al. Consumer willingness to pay for a hypothetical chikungunya vaccine in Brazil and the implications. Expert Rev Pharmacoecon. Outcomes Res. 19(4), 473–482 (2019).
42.
Instituto Brasileiro de Geografia e Estatística. Cidades-Panorama (2018). https://cidades.ibge.gov.br/brasil/pa/maraba/panorama
43.
Instituto Brasileiro de Geografia e Estatística. IBGE divulga o rendimento domiciliar per capita e o coeficiente de desequilíbrio regional 2019 (2019). https://agenciadenoticias.ibge.gov.br/agencia-sala-de-imprensa/2013-agencia-de-noticias/releases/27810-ibge-divulga-o-rendimento-domiciliar-per-capita-e-o-coeficiente-de-desequilibrio-regional-2019
44.
Agência Brasil. IBGE: rendimento domiciliar per capita (2019). http://agenciabrasil.ebc.com.br/renda_domiciliar_per_capita_2019.pdf
45.
Athie TS, Nascimento GC, da Costa MJL et al. Consumer willingness to pay for a hypothetical Chagas disease vaccine in Brazil: a cross-sectional study and the implications. Expert Rev Pharmacoecon. Outcomes Res. 10(8), 659–672 (2021).
•• Important to complement our knowledge of willingness to pay approach.
46.
Godói IPD, Sarmento TTR, Reis EA et al. Acceptability and willingness to pay for a hypothetical vaccine against SARS CoV-2 by the Brazilian consumer: a cross-sectional study and the implications. Expert Rev. Pharmacoecon. Outcomes Res. (2021).
47.
Brasil. Agência Nacional de Vigilância Sanitária. Resolução CMED n° 2, de 05 de março de 2004 (2004). https://www.gov.br/anvisa/pt-br/assuntos/medicamentos/cmed/legislacao/arquivos/arquivos-resolucoes/6324json-file-1
48.
Agência Nacional de Vigilância Sanitária. Preços máximo de medicamentos por princípio Ativo (2020). https://www.gov.br/anvisa/pt-br
49.
Al-Hanaw MK, Vaidya K, Alsharqi O, Onwujekwe O. Investigating the willingness to pay for a contributory National Health Insurance Scheme in Saudi Arabia: a cross-sectional stated preference approach. Appl. Health Econ. Health Policy 16(2), 259–271 (2018).
50.
Jofre-Bonet M, Kamara J. Willingness to pay for health insurance in the informal sector of Sierra Leone. PLoS One 13(5), e0189915 (2018).
51.
Agência Nacional de Saúde Suplementar. Cadernos de Informações da Saúde Suplementar: Beneficiários, Operadoras e Planos (2019). http://www.ans.gov.br/images/stories/Materiais_para_pesquisa/Perfil_setor/Dados_e_indicadores_do_setor/total-cad-info-jun-2019.pdf
52.
Brasil. Banco Central do Brasil. Conversor de Moedas (2020). https://www.bcb.gov.br/conversao
53.
Palanca-Tan R. The demand for a dengue vaccine: a contingent valuation survey in Metro Manila. Vaccine 26(7), 914–923 (2008).
54.
Hadisoemarto PF, Castro MC. Public acceptance and willingness-to-pay for a future Dengue vaccine: a community-based survey in Bandung, Indonesia. PLoS Negl. Trop. Dis. 7(9), e2427 (2013).
55.
White SE, Harvey SA, Meza G et al. Acceptability of a herd immunity-focused, transmission-blocking malaria vaccine in malaria-endemic communities in the Peruvian Amazon: an exploratory study. Malar. J. 17(1), 179 (2018).
56.
Udezi WA, Usifoh CO, Ihimekpen OO. Willigness to pay for three hypothetical malaria vaccines in Nigeria. Clin. Ther. 32(8), 1533–1544 (2010).
57.
Harapan H, Fajar JK, Kuch U et al. Dengue vaccine acceptance and willingness to pay. Hum. Vaccine Imunother. 13(4), 786–790 (2017).
58.
IBGE. PNS 2019: sete em cada dez pessoas que procuram o mesmo serviço de saúde vão à rede pública (2020). https://agenciadenoticias.ibge.gov.br/agencia-sala-de-imprensa/2013-agencia-de-noticias/releases/28793-pns-2019-sete-em-cada-dez-pessoas-que-procuram-o-mesmo-servico-de-saude-vao-a-rede-publica
59.
Silveira RP, Pinheiro R. Understanding the need for doctors in innerstate Amazon – Brazil. Rev. Bra Edu. Med. 38(4), 451–459 (2014).
60.
Rathgeber EM, Vlassoff C. Gender and tropical diseases: a new focus. Soc. Sci. Med. 37(4), 513–520 (1993).
61.
Yasunaga H, Ide H, Imamura T, Ohe K. Willingness to pay for health services in cold detachment, common retinal, and myocardial infarction: an internet survey in Japan. BMC Health Serv. Res. 6, 12 (2006).
62.
Kim SY, Sagiraju HK, Russell LB. Willingness to pay for vaccine in low and middle-income countries: a systematic review. Ann. Vaccines Immun. 1(1), 1001 (2014).
63.
Instituto Brasileiro de Pesquisas Espaciais. A taxa consolidada de desmatamento por corte raso para os nove estados da Amazônia Legal (AC, AM, AP, MA, MT, PA, RO, RR e TO) em 2019 é de 129 km2. (2020) http://www.inpe.br/noticias/noticia.php?Cod_Noticia=5465
64.
Instituto de Pesquisa Econômica Aplicada (IPEA). A ameaça do desmatamento (2015). https://www.ipea.gov.br/desafios/index.php?option=com_content&id=3176
65.
Organização Pan-Americana da Saúde (OPAS). OMS recomenda vacina inovadora contra malária para crianças em risco (2021). https://www.paho.org/pt/noticias/6-10-2021-oms-recomenda-vacina-inovadora-contra-malaria-para-criancas-em-risco
•• Important reference source associated with the development of vaccines for malaria.
Information & Authors
Information
Published In
Pages: 263 - 274
PubMed: 35029122
Copyright
© 2022 Future Medicine Ltd.
History
Received: 18 March 2021
Accepted: 29 November 2021
Published online: 14 January 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Willingness to pay for a hypothetical malaria vaccine in Brazil: a cross-sectional study and the implications. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0073
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Obinna Felix Dim, Uzochukwu Emmanuel Chima, Francis Chibuike Iloabuchi, Chigozie Gloria Anene-Okeke, Chukwuemeka Augustine Nwachuya, Jennifer Chinaecherem Onyehalu, Anthony Uche Umeh, Chinonso Anne Agbo, Juliet Ekenedilichukwu Agbo, Abdulmuminu Isah, Awareness, acceptability, and willingness to pay for the R21/Matrix-M malaria vaccine: a cross-sectional study among pregnant women and nursing mothers in Enugu State, Nigeria, BMC Public Health, 10.1186/s12889-025-25405-1, 25, 1, (2025).
- Muhammad Sale Musa, Abdulwahab Kabir Sulaiman, Fatimah Isma'il Tsiga-Ahmed, Abdulaziz Tijjani Bako, Sahabi Kabir Sulaiman, Acceptance of malaria vaccine among mothers of under-five children in Nigeria: Results from the M-VAN survey, Vacunas (English Edition), 10.1016/j.vacune.2024.10.005, 25, 4, (439-447), (2024).
- Muhammad Sale Musa, Abdulwahab Kabir Sulaiman, Fatimah Isma'il Tsiga-Ahmed, Abdulaziz Tijjani Bako, Sahabi Kabir Sulaiman, Acceptance of malaria vaccine among mothers of under-five children in Nigeria: Results from the M-VAN survey, Vacunas, 10.1016/j.vacun.2024.06.007, 25, 4, (439-447), (2024).
- Vinícius Gonçalves Nogueira, Edna Afonso Reis, Brian Godman, Antony Paul Martin, Isabella Piassi Dias Godói, Acceptability and willingness to pay for a hypothetical HIV vaccine in Brazil and the implications: a cross-sectional study, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2024.2384543, 25, 1, (91-100), (2024).
- Omer Ben-Aharon, Ruslan Sergienko, Georgi Iskrov, Dan Greenberg, Willingness to pay for an mRNA-based anti-cancer treatment: results from a contingent valuation study in Israel, Israel Journal of Health Policy Research, 10.1186/s13584-024-00594-z, 13, 1, (2024).
- Catterina Ferreccio, How Did We Get Here: The Best Vaccines Ever Facing the Highest Public Hesitancy?, Vaccines, 10.3390/vaccines11081323, 11, 8, (1323), (2023).
- Gesiane Cavalcante Nascimento, Maria José Labis da Costa, Thannuse Silva Athie, Juliana de Sales Silva, Edna Afonso Reis, Celline Cardoso Almeida-Brasil, Brian Godman, Isabella Piassi Dias Godói, Acceptability and Consumer Willingness to pay for a hypothetical HIV vaccine in Northern Brazil: A cross-sectional study and the implications, Journal of HIV/AIDS & Social Services, 10.1080/15381501.2022.2029660, 21, 2, (145-166), (2022).