An economic evaluation of teledermatology care delivery for chronic skin diseases
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Analyze the impact of nationwide implementation of teledermatological care for psoriasis. Methods: Develop a Markov model that estimates the impact of telehealth technology for treatment of moderate-to-severe psoriasis on health and healthcare expenditures compared with in-person clinical care. Results: Lower medical costs by US$1.5 billion and total social costs of US$4.3 billion over 5 years. Patients save more than 67 million hours in work absenteeism and travel time, valued at US$598 million. Employers save US$1.2 billion over 5 years due to decreased employee absenteeism. Conclusion: National implementation of telehealth for psoriasis care has the potential to substantially reduce both formal healthcare costs and informal costs for families and patients, while maintaining equivalent clinical outcomes as traditional in-person care.
Lay abstract
Recent innovations in telehealth (methods of accessing and managing healthcare using digital information and technologies, such as the computer or telephone) have allowed for convenient access to care for dermatology patients. A recent study found that psoriasis patients experienced similar quality of care outcomes when using telehealth services as they did when seeing a clinician in-person. This paper builds on previous work examining teledermatological care outcomes and aims to analyze the potential economic impacts of a nationwide implementation of telehealth for managing psoriasis. We model the impacts of healthcare utilization and costs, caregiver time loss, and work absenteeism costs between the telehealth and in-person care settings. These results produce cost savings to society of over US$4.3 billion over 5 years.
Background
Psoriasis affects more than 5,000,000 adults in USA, nearly two million of whom have 1% or greater of their body surface area (BSA) covered by psoriasis [1]. Psoriasis patients experience substantially reduced quality of life through physical and psychological discomfort brought on by their condition [2]. Many patients also experience difficulty in accessing dermatologists for care [3].
Recent technological innovations in telemedicine have created new opportunities for patients with psoriasis to access dermatological care. The collaborative connected health (CCH) model of teledermatology allows patients the opportunity to consult a dermatologist without leaving home. The patient sends photographs of lesions and other skin issues directly to the dermatologist, who then reviews the images and responds [4]. A recent study found teledermatological care improved quality of life and disease severity among patients with psoriasis as effectively as in-person care [4,5] and reduced transportation and appointment wait times [6] compared with traditional in-person care. Additionally, research has found no significant differences in the type and complexity of cases referred to in-person and telehealth providers [7]. This study models an impact analysis of universal adoption of online psoriasis care and identifies changes in healthcare costs, utilization and savings. The costs and benefits of these changes are studied from the patient, family, employer, and payer perspectives for 1-, 2-, 5- and 10-year time horizons. The study team used results from Armstrong et al. [5], Armstrong [4] and Ford et al. [6], and obtained other input values from national data sources and peer-reviewed literature to inform the model. This paper summarizes the primary findings of this analysis; reviews the methods and findings for Armstrong, Chambers et al. [4] and Armstrong, Ford et al. [5]; describes the modeling methods for this study; and presents the results of the impact analysis.
Overview of peer-reviewed research on the effectiveness of teledermatological care
The authors of Armstrong et al. [5], Armstrong et al. [4] and Ford et al. [6] conducted a clinical equivalency trial to investigate the effectiveness of teledermatological care in improving outcomes and access to care compared to traditional in-person care. The study sample included psoriasis patients at least 18 years old with access to the internet, a device with a camera, and an established primary care physician (PCP). Recruitment for the study occurred between February 2015 and August 2017 from the general population and clinics in California and Colorado. Researchers randomized 296 patients into two groups of 148 patients each: one for online care and one for in-person care. Study participants then communicated with a dermatologist either online or in person for 12 months.
The online setting allowed psoriasis care to be delivered asynchronously through an online platform in which either PCPs or patients could communicate with a dermatologist. Using this platform, the dermatologist could provide education or prescription information to the patients and their PCPs. Patients randomized to the in-person control arm of the study would access their dermatologists or PCPs in person. The frequency of consultation was determined by the dermatologist or PCP.
Outcomes were measured by changes in the Psoriasis Area and Severity Index (PASI), the Body Surface Area (BSA) scores and the Patient Global Assessment score (PtGA) for patients during the 12-month trial. PASI is an index that combines the affected surface area and lesion severity on a scale ranging from 0 to 72. BSA is a measure used to report the percentage of body surface area affected by psoriasis, ranging from 0 to 100%. PtGA measures psoriasis severity on an ordinal scale ranging from 0 to 6 from the patient's perspective. Armstrong, Chambers et al. used the mean improvement between PASI scores between 3-, 6-, 9- and 12-month follow-up sessions as their primary outcome [5]. The online and in-person mean changes in PASI score across all visits improved for both groups. The difference in these mean changes were not statistically significant. BSA scores were used as a secondary outcome measure and the differences in the decrease in psoriasis severity in the in-person and online groups were also found to not be statistically significant at the end of the 12 months. PtGA, a score reflecting the patient perspective of disease severity, showed greater improvement among patients in the online group than in the in-person group, suggesting online care may improve factors in addition to disease severity measured by BSA and PASI. Results of these studies indicated asynchronous online care was equivalent to in-person care in improving health outcomes.
Not surprisingly, the research also found that for each specialty care appointment, patients in the online care model spent significantly less time waiting for appointments and traveling to and from providers' clinics than those receiving in-person care. Ford et al. [6], found the in-person group spent an average of 24 days and 15.1 h per person in travel and in-office wait time over 12 months, while members of the online cohort spent an average of 0.1 h per person over 12 months. Additionally, psoriasis patients assigned to the online setting reported feeling their needs were being addressed and praised the effectiveness of telehealth care.
Methods
We developed a population-level Markov model to simulate the effects of universal adoption of a telehealthcare delivery model for patients with psoriasis on formal and informal costs based on findings from Armstrong et al. [5], Armstrong Ford et al. [4] and Ford et al. [6], over 1-, 2-, 5- and 10- year time horizons (Figure 1). In each year of the model, a new cohort of patients enters at the psoriasis diagnosis node shown in Figure 1 and receive either in-person or online psoriasis care for the duration of their time in the model. Patients exit the model due to death or recovery or are placed back into in-person or online care due to recurrence. Results in this paper used a 5-year time horizon. Table 1 summarizes the consequences and costs from the patient, family, employer, payer and societal perspectives.
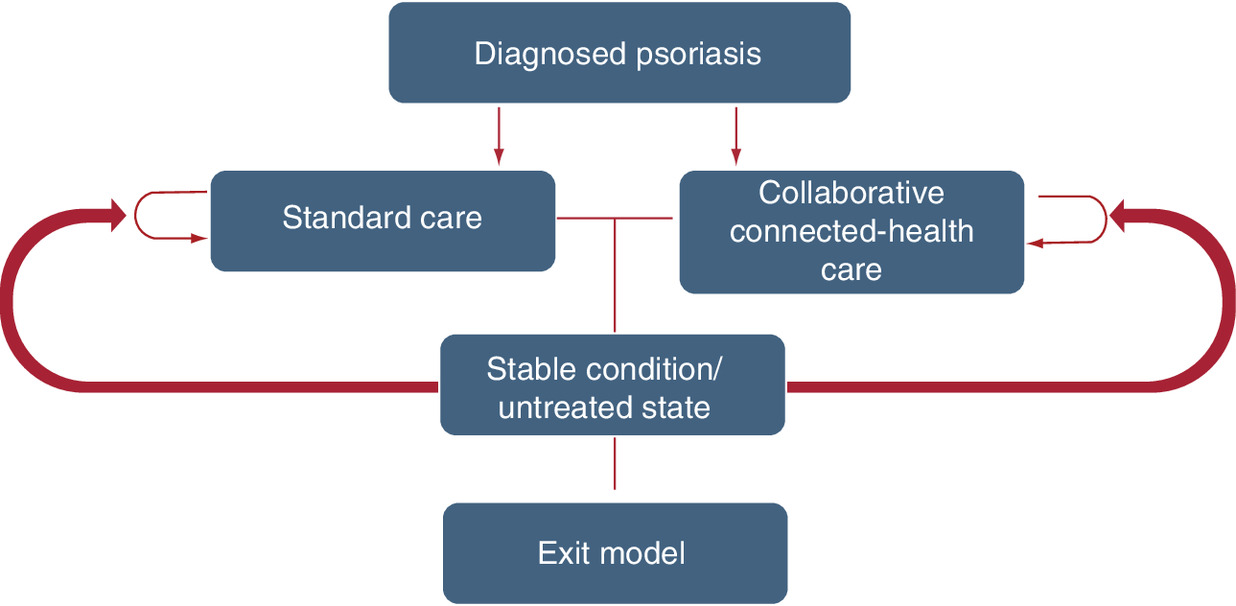
Figure 1. Diagram of the Markov model.
This figure shows the flow of patients through different treatment states in our population-level Markov model. We modeled patient outcomes at each of 1-, 2-, 5- and 10- year time horizons. Patients enter the model at the psoriasis diagnosis node and receive either in-person or collaborative connected healthcare (CCH), which may include both in-person and teledermatology care. Incident and recurrent patient cohorts are added each year of the model. Patients may exit the model due to death or recovery.
| Perspective | Consequence/cost | Model outcome |
|---|---|---|
| Formal healthcare sector impacts and costs | ||
| Patient | Healthcare utilization | Office visits |
| Patient | Healthcare utilization | Cost of prescription purchases |
| Patient | Healthcare direct medical costs | Out-of-pocket healthcare costs |
| Payer | Healthcare spending | Payer healthcare costs |
| Informal healthcare sector impacts and costs | ||
| Patient | Patient time | Patient hours |
| Patient | Cost of patient time | Patient time and travel costs |
| Family | Unpaid caregiver time | Total unpaid caregiving hours |
| Family | Cost of caregiver time | Unpaid caregiving costs |
| Non-healthcare sector impacts and costs | ||
| Employer | Hours of absenteeism | Work absenteeism hours |
| Employer | Total absenteeism cost | Employer productivity costs |
| Total societal costs | ||
| Societal | The sum of formal and informal healthcare costs | Total societal cost |
The model estimates healthcare utilization and costs, caregiver time loss and absenteeism costs across two treatment types: the current practice of in-person psoriasis care and telehealth care for all individuals affected by psoriasis. The model allows patient and societal costs to vary across the two treatment types.
We obtained feedback on the model from a clinical dermatologist, Dr Karen McKoy, three-times during the project. McKoy provided feedback and answered questions about psoriasis, the model structure, specific parameter estimates, billing for online and in-person psoriasis care and prescriptions, psoriasis population characteristics and model results. We also received input and feedback from Dr Thomas Hoerger, a modeling expert who provided comments on the model structure and a face validity check on the structure and results of the model.
Model parameters
We identified the model parameters from a variety of sources (Table 2). Table A-1 in Appendix A details the ranges used for one-way sensitivity analysis and the distributions used for probabilistic sensitivity analysis.
| Parameter description | Parameter | Ref. |
|---|---|---|
| Population parameters | ||
| US adults 18 and older | 253,227,594 | [8] |
| Prevalence rate of psoriasis patients who have sought care | 682.9 per 100,000 | [1,9] |
| Incidence of psoriasis | 24.07 per 100,000 | [10] |
| Incidence of death | 63.75 per 100,000 psoriasis patients | [11] |
| Annual frequency of office visits for online group | 0.1 | [5] |
| Annual frequency of office visits for in-person group | 2.1 | [5] |
| Annual frequency of online visits for online group | 1.1 | [5] |
| Probabilities and fractions | ||
| Population with mild disease seeking care | 48.10% | [1,9] |
| Population with moderate disease seeking care | 40.42% | [1,9] |
| Population with severe disease seeking care | 11.48% | [1,9] |
| Percentage of prevalent patients who received UV-B phototherapy treatment | 6.27% | [12] |
| Percentage of prevalent of patients who received PUVA treatment | 0.73% | [12] |
| Percentage of prevalent patients expected to continue to have psoriasis after 5 years of treatment | 95% | K. McKoy (11 April 2019, PERSONAL COMMUNICATION) |
| Productivity loss multiplier for family | 38% | [13] |
| Impacts and costs† | ||
| Office visit cost | US$140.07 | [14] |
| Online cost | US$80.61 | [14] |
| Total prescription cost for patients with mild psoriasis (3-month supply; payer cost) | US$43.46 | [15] |
| Total prescription cost for patients with for moderate psoriasis (3-month supply; payer cost) | US$1,394.19 | [15] |
| Total prescription cost for patients with severe psoriasis (3-month supply; payer cost) | US$14,640.75 | [15] |
| Total PUVA cost for initial clearing phase (per visit; payer cost) | US$211.19 | [16] |
| Total PUVA cost for maintenance phase (per visit; payer cost) | US$222.55 | [16] |
| Total UV-B cost for induction phase (per visit; payer cost) | US$86.47 | [16] |
| Total UV-B cost for maintenance phase (per visit; payer cost) | US$94.02 | [16] |
| Out-of-pocket cost for in-person visit | US$28.23 | [15] |
| Out-of-pocket cost for online visit | US$16.25 | [14,15] |
| Out-of-pocket prescription cost for patients with mild psoriasis (3-month supply) | US$11.11 | [15] |
| Out-of-pocket prescription cost for patients with moderate psoriasis (3-month supply) | US$356.30 | [15] |
| Out-of-pocket prescription cost for patients with severe psoriasis (3-month supply) | US$3,741.58 | [15] |
| Travel cost per visit | US$33.20 | [17] |
| Hourly wage rate | US$29.95 | [18–20] |
| Hourly caregiver wage rate | US$16.90 | [21] |
†
Dollars are inflation adjusted to US 2018 values.
Population & clinical parameters
Patients within ten cohorts underwent treatment beginning the year they entered the model through the 10th and final year of the model. For the first year of our model, we determined the estimated prevalence of psoriasis from National Health and Nutrition Examination Survey (NHANES) data for 2013 and 2014 [1]. The distribution of disease severity was also derived from these data. To account for individuals diagnosed with psoriasis who do not seek treatment, we multiplied the number of patients estimated to have psoriasis by the proportion estimated to seek psoriasis treatment [9]. Patients reported to have mild, moderate and severe psoriasis were included in our population. This includes individuals with at least 1% BSA covered with psoriasis [1]. Our treated prevalence estimate equaled approximately 1.7 million US adults seeking care for their psoriasis for the first year of our model. In each subsequent year of the model, a new cohort of incident patients entered the model. Each new cohort began with approximately 60,000 incident patients seeking care. The subsequent cohorts were formed based on an estimate of the incidence of dermatologist-confirmed psoriasis cases [10]. This incidence rate was applied to the population of adults 18 and older in the United States and assumed the distribution of psoriasis severity in the incident population was the same as in the prevalent population [8].
Patients exited the model as a result of mortality and remission. Mortality was estimated based on population characteristics from a longitudinal study observing a random sample of psoriasis patients during a 16-year period [11]. We estimated remission occurred at a 5-year time horizon for 5% of the patients (K. McKoy, personal communication, 11 April 2019). Mortality was estimated at 63.75 per 100,000 patients. Values for psoriasis incidence and mortality were adjusted by the authors to include only those with at least 1% BSA covered with psoriasis, based on the NHANES psoriasis severity distribution estimate [1]. The office visit frequencies for the in-person and online groups were drawn from the research by Armstrong, Ford et al. [5]. The study team calculated the number of average annual in-person and online visits by dividing the count of each type of visit for each research arm [5] by the number of individuals in each arm. This included 315 in-person office and 0 online visits for the in-person group, and 161 online and 8 in-office visits for the 148 individuals in the online group. Patients randomized to the online model were asked to see the dermatologist in person as was deemed necessary, accounting for the number of in-person visits for the online population [6]. The study team obtained estimates from Takeshita et al. [12] for the percentages of the psoriasis population receiving UV-B phototherapy treatment as well as those receiving Psoralen plus UVA (PUVA), a treatment combining drug and ultraviolet light radiation.
Healthcare cost parameters
We calculated the phototherapy cost per visit by dividing the estimated total cost for phototherapy treatment determined by Beyer and Wolverton [16] by the total number of visits. The estimated total office visit costs for in-person and online care were drawn from Parsi, Chambers and Armstrong [14,22]. All estimated prescription costs were drawn from 2017 Medical Expenditure Panel Survey (MEPS) data [15]. The total drug costs were calculated based on prescriptions associated with at least one form of diagnosed psoriasis for individuals with ICD-10-CM code L40 in the MEPS 2017 Medical Conditions file [23]. The average costs were calculated across the three disease severity levels; these costs were the sum of the total cost paid by all payers, including out-of-pocket costs paid directly by patients. The out-of-pocket costs for in-person doctor visits were also calculated and inflated to 2018 dollars [15]. The data on out-of-pocket costs for online teledermatology visits were sparse and inconsistent. In the team's model, out-of-pocket costs for online visits were estimated by multiplying total online costs by the ratio between the out-of-pocket in-person costs to total in-person costs.
Non-healthcare cost parameters
To estimate the informal costs borne by patients, employers and the family members who accompanied the patient to an appointment or helped guide the patient online to communicate with the dermatologist, we used estimates of waiting and travel time for each appointment. The estimated mean transportation and in-office waiting time for in-person appointments was 4 h (Ford et al.). In consultation with the clinical expert, Dr McKoy (9 May 2019, Personal Communication), the study team estimated patients receiving care online spent approximately 30 min sending images of their skin lesions or video chatting with a dermatologist. To determine the cost of employee absenteeism to employers, these times were multiplied by an hourly wage rate of US$29.95, based on a nationally representative median wage rate plus 30% for fringe benefits and the labor force participation rate [18–20].
To analyze family impacts, the study team assumed 37.6% of patients would be accompanied by a companion based on the rate of patient accompaniment reported by Wolff and Roter [13]. We included productivity losses for family members who accompanied patients to in-person appointments or helped set up equipment for online appointments; we assumed an average hourly caregiver wage rate of US$16.90 for family members, based on the 2018 median wage rate of nursing and home health aides [21].
We estimate two-way travel costs of US$33.20 using research from Rothstein et al. who associated a mean expense of US$16.60 for one-way travel to a dermatology clinic [17].
Sensitivity analyses
One-way & probabilistic sensitivity analyses
We conducted one-way sensitivity analyses at the 5-year time horizon for total patient and total societal costs to assess the sensitivity of the base analysis findings. Each parameter is varied while all other parameters are held constant at their base values, to show a range of possible model outcomes. We also conducted probabilistic sensitivity analysis for a 5-year time horizon using 1000 iterations of the model, assuming distributions for each input, to obtain credible ranges for the cost savings.
Additional sensitivity analyses
Additionally, we conducted a scenario analyses of uptake exclusively among the rural psoriasis population. One area of potential for telehealth is increasing access to care for those in rural areas poorly served by specialists. We use the Economic Research Service's 2013 Rural-Urban Continuum Codes to estimate the number of Americans living in nonmetropolitan counties and assume the distribution of the psoriasis population is the same in both rural and urban settings [24].
Technological barriers and patient and provider preferences will affect the adoption of the CCH model of care. An underlying assumption of the primary findings is that the entire psoriasis prevalent population will adopt a CCH model of care. As an additional sensitivity analysis, we determined potential cumulative cost savings by perspective at different levels of adoption of the CCH model of care. In preparing these estimates, we assumed a constant rate of model adoption for 5 years, although savings at different levels of adoption or different time horizons are a straightforward calculation of multiplying the preferred level of adoption as a proportion of the psoriasis population by the estimated potential savings at any time horizon.
Results
Significant cost and time savings are gained through national implementation of the online care model (Tables 3 and A.2). We find 67,632,338 fewer hours spent at or in transit to or from a provider for a 5-year time horizon, which equated to 7.5 h saved per patient per year. This equates to savings of 25,429,759 h (2.82 h per patient annually) and 42,608,373 h (4.73 h annually per patient) for family caregiving and employee absenteeism, respectively. In the online model, annual per-patient savings in formal medical costs equal about US$39. Total societal cost savings per patient equal about US$479 annually.
| Outcome | Status quo in-person care model | Online CCH care model | Total savings | Annual per-patient savings |
|---|---|---|---|---|
| Utilization | ||||
| Number of in-person provider office visits | 18,937,052 | 901,764 | 18,035,288 | 2.00 |
| Number of online provider interactions | 0 | 9,809,734 | -9,809,734 | -1.09 |
| Total provider interactions | 18,937,052 | 10,711,498 | 8,225,553 | 0.91 |
| Patient perspective | ||||
| Absenteeism (h) | 75,748,218 | 8,115,879 | 67,632,338 | 7.50 |
| Informal costs (transportation) | US$628,710,208 | US$29,938,577 | US$598,771,630 | US$66.40 |
| Formal medical costs | US$22,075,679,857 | US$21,725,949,020 | US$349,730,837 | US$38.78 |
| Total costs | US$22,704,390,065 | US$21,755,887,597 | US$948,502,467 | US$105.18 |
| Payer perspective | ||||
| Formal medical costs | US$65,000,566,120 | US$63,488,535,538 | US$1,512,030,582 | US$167.67 |
| Family perspective | ||||
| Unpaid caregiving time (h) | 28,481,330 | 3,051,571 | 25,429,759 | 2.82 |
| Total cost of unpaid caregiving | US$481,334,475 | US$51,571,544 | US$429,762,931 | US$47.66 |
| Employer perspective | ||||
| Productivity loss (h) | 47,721,377 | 5,113,004 | 42,608,373 | 4.73 |
| Total cost of productivity loss | US$1,429,255,247 | US$153,134,470 | US$1,276,120,777 | US$141.51 |
| Societal perspective | ||||
| Total formal medical costs | US$87,076,245,977 | US$85,214,484,558 | US$1,861,761,419 | US$206.46 |
| Total costs | US$89,615,545,907 | US$85,295,994,680 | US$4,319,551,227 | US$479.01 |
The online care settings results in cost savings for family, patients, employers and payers for the 1-, 2-, 5- and 10-year time horizons (Table 4). Total societal savings are estimated to exceed US$4 billion in 5 years and more than US$9 billion in 10 years, respectively.
| Time horizon | All payers | Medicare | Medicaid | Private payers |
|---|---|---|---|---|
| 1 year | US$288 | US$58 | US$38 | US$192 |
| 2 years | US$584 | US$117 | US$78 | US$390 |
| 5 years | US$1512 | US$303 | US$201 | US$1009 |
| 10 years | US$3193 | US$639 | US$424 | US$2130 |
Costs by payer
Using approximate estimates of the share of the psoriasis population covered by different insurers, we estimated the formal medical cost savings associated with the full adoption by payers of the CCH model of care (Table 4). We assumed that the psoriasis-prevalent population aged 65 and older was covered by Medicare, that 13% of the psoriasis-prevalent population aged 18–64 was covered by Medicaid, and that the remainder of the population was covered by private payers. We obtained estimates of the age distribution of the psoriasis-prevalent population from National Health and Nutrition Examination Survey data for 2013 and 2014 and estimates of the distribution of insurance coverage from the Medicaid and CHIP Payment and Access Commission's (MACPAC) 2018 report to Congress [25]. Based on these estimates, we calculated the following distribution of medical cost savings from expanding the CCH model nationwide: 20% to Medicare, 10% to Medicaid and the remaining 70% of savings to private payers.
Sensitivity & scenario analyses
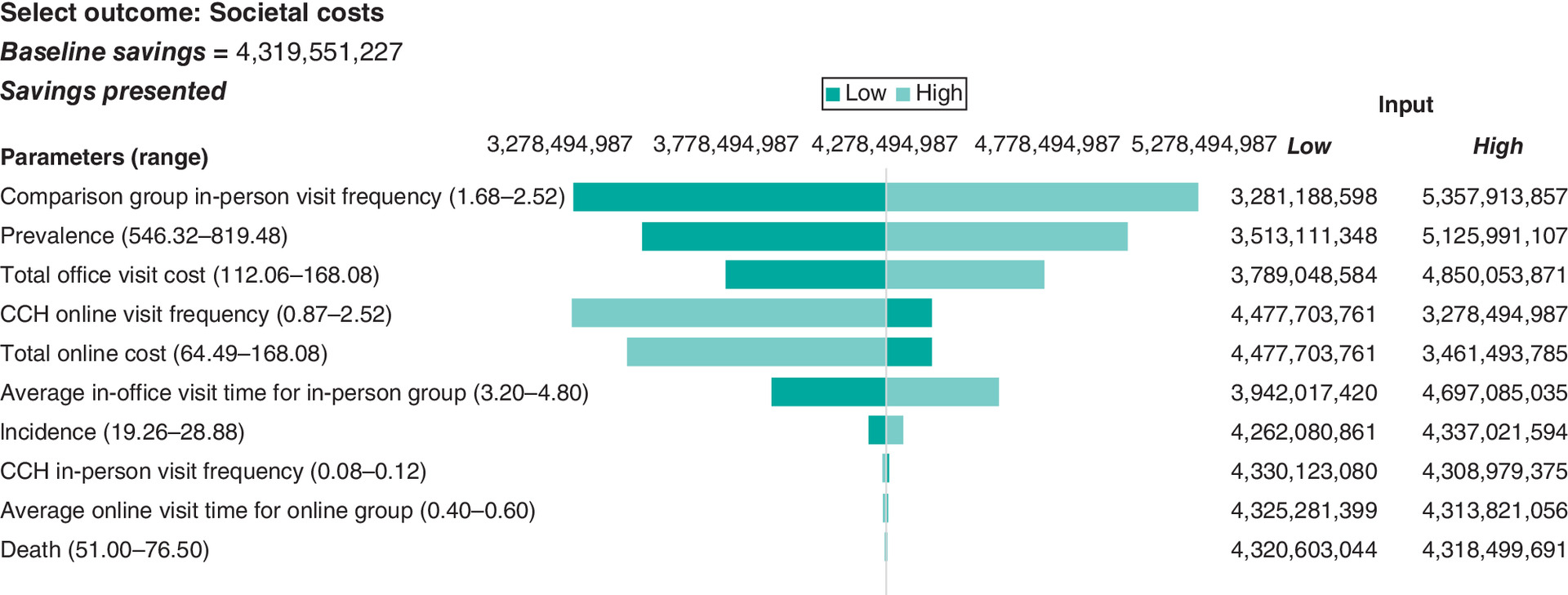
Figures 2 & 3 show the range of potential savings and distributional assumptions about each input parameter. Tornado diagrams were produced to visualize the sensitivity of model outcomes.
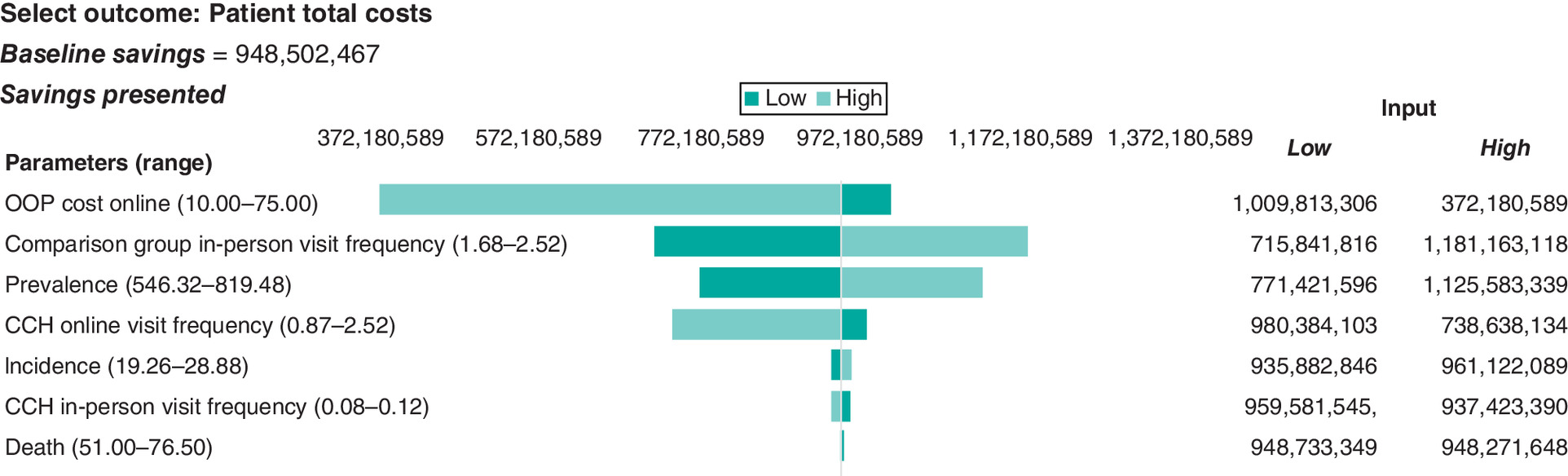
When calculating the sensitivity analysis, we allowed online out-of-pocket costs to have wide upper and lower bounds to account for the large variation in billing practices for this service (K. McKoy, Personal Communication, 9 May 2019). Our model assumes an out-of-pocket cost for online care of US$16.25, with a range of US$10 to US$75. Additionally, we examine potential infrastructure costs required to do telehealth which may limit uptake. Using findings from Parsi et al. and Chambers et al., we estimate computer and equipment costs for online care at US$10.70 per session [14,22]. This figure is derived from an estimate using straight-line depreciation over 3 years. These potential equipment costs would have to increase by US$59.46 per session to meet the cost of an in-person visit. When accounting for costs from lost wages and travel equipment costs would need to increase at least US$447.42 over 1 year of online care.
Assuming 100% of Americans with psoriasis living in nonmetropolitan counties (14.9% of US population) seek teledermatological care, we estimate cost savings of US$644 million (Table 5). We estimate up to US$160 million in savings if 25% of Americans with psoriasis living in nonmetropolitan counties (3.7% of US population) seek teledermatological care.
| Analysis perspective | |||||
|---|---|---|---|---|---|
| Level of adoption of CCH | Patient cost | Payer medical cost | Employer cost | Family cost | Societal cost |
| 100% of Americans living in Nonmetro counties (14.9% of US population) | US$141 | US$225 | US$190 | US$64 | US$644 |
| 75% of Americans living in Nonmetro counties (11.2% of US population) | US$106 | US$169 | US$143 | US$48 | US$484 |
| 50% of Americans living in Nonmetro counties (7.5% of US population) | US$71 | US$113 | US$96 | US$32 | US$324 |
| 25% of Americans living in Nonmetro counties (3.7% of US population) | US$35 | US$56 | US$47 | US$16 | US$160 |
At different levels of adoption of the CCH model of care, we estimated a savings of US$1 billion after 5 years if 25% of psoriasis patients seeking care used the online model of care, and over US$4 billion in savings after 5 years if all psoriasis patients adopted the online model of care (data not shown).
Discussion
Some researchers have found that despite the cost savings virtual visits provide, telehealth increases utilization among patients causing an increase in spending [26]. This research used claims and enrollment data for patients suffering from acute respiratory infections and found a US$45 increase in health spending per telehealth patient despite lower costs per provider–patient interaction. In contrast, the randomized controlled trial conducted by Armstrong et al. showed a smaller number of patient–provider interactions in their online cohort [5]. Armstrong et al. note the frequency of online and in-person visits in their study was determined by medical necessity.
Uptake in telehealth has been increasing, but the outbreak of COVID-19 has seen a spike in telehealth usage. One health system in New York saw a 683% increase in telehealth visits between 2 March and 14 April 2020 [27]. One medical department who documented their transition from in-person care to telehealth found psoriasis amenable to telehealth [28]. Physicians in this department noted limitations in costs of adopting telehealth, inability to conduct procedures and differences across medical record platforms.
Limitations
This study has some potential limitations that are centered around the availability of information for specific parameter estimates. First, as a result of the wide variability in out-of-pocket costs for online psoriasis care across USA, accurately estimating those costs was challenging. We accounted for the variability in out-of-pocket costs in the sensitivity analyses by using a plausible range of US$10 to US$75 for out-of-pocket online care spending. We set these bounds based on conversations with Dr McKoy (Personal Communication, 9 May 2019) and our estimates for out-of-pocket costs for in-person dermatology visits.
Second, the studies by Armstrong [5], and Armstrong et al. [4], reported large differences in frequency of provider interaction across the online and in-person models, with patients in the online model averaging 1.09 provider interactions per year compared with 2.1 per year in the in-person model. This results in a large decline in patient–provider interactions in our model. As a sensitivity analysis, the study team allowed the upper bound of the annual online dermatology visit model parameter to match the in-person office frequency. Even with no reduction in the total number of specialist appointments for psoriasis care, the study team found the adoption of the teledermatology care model resulted in substantial savings.
Our model compares two patient care settings, online CCH and in-person care and estimates cost savings by assuming uptake in online care. One deficiency of this approach is we are not able to make estimates of the current population receiving teledermatological care. As a result our estimated savings may be biased upwards.
Additionally, we assume the finding from the patient sample in Armstrong et al. [5] and other model inputs would map onto the US psoriasis population. But this may not be the case. For example, we do not have precise information about the distribution of health insurance coverage among psoriasis patients, which may differ from the sample in Armstrong, Chambers et al. [5]. Other model inputs, including values for informal costs borne by patients, employers, and patients' family members, were obtained from nationally representative sources. To the extent, the true values of these inputs for psoriasis patient population vary from the general population our model results may be biased.
We also assume a constant level of technological capacity over time, and that the relative costs between in-person and online psoriasis care would remain unchanged over the 10-year time horizon. In the future, technological capacity could change and effect the relative costs or relative effectiveness of care between in-person and online psoriasis care.
A final assumption (and potential limitation) we made was that all the new cohorts entering the model would experience the same visit frequency as the preceding cohorts. Depending on any changes in the practice of care for patients with psoriasis, our model may overestimate savings if future care recommends or requires fewer annual clinical consultations or underestimate savings if future care recommends additional annual clinical consultations. Our sensitivity analysis that estimates savings for a range of the number of annual clinical consultations likely reflects savings under the CCH model even if the practice of care for psoriasis changes in the future.
Conclusion
The online model for psoriasis care has the potential to save society an estimated US$4 billion over 5 years in costs as a result of reduced employee absenteeism and family caregiver time and savings in payer and patient costs from the lower cost burden of online care. We estimated reduced absenteeism from work will save employers more than US$1.2 billion and families of patients more than US$429 million. Patients will save an estimated more than 67 million in absenteeism and travel time, or US$599 million in informal patient costs all over 5 years. These findings have shown to be robust to parameter adjustments via sensitivity analyses.
Background
•
Telehealth for psoriasis care has been found to to have similar quality outcomes as in-person dermatological care. This creates new opportunities for patients to access dermatological care.
•
The aim of this paper is to analyze the potential economic impact of nationwide implementation of teledermatological care for managing psoriasis.
Methods
•
This paper develops a population-level Markov model to simulate the effects of universal adoption of telehealth for psoriasis patients.
•
Our model is based on findings from previous research indicating that telehealth technology is equally effective as traditional in-person clinical care in managing psoriasis.
•
The model estimates healthcare utilization and costs, caregiver time loss, and work absenteeism costs across two treatment types: 1) the current practice of in-person psoriasis care, and 2) telehealth care for all individuals affected by psoriasis.
Results
•
The use of telehealth for psoriasis could reduce formal medical costs by an estimated US$1.5 billion over five years, and an estimated US$4.3 billion for total societal costs equaling over US$479 per patient annually.
•
Patients were estimated to save more than 67 million hours in work absenteeism and travel time, or US$598 million in informal patient costs.
•
Employers could save more than US$1.2 billion over 5 years due to decreased employee absenteeism time.
Conclusion
•
National implementation of telehealth for psoriasis care has the potential to substantially reduce both formal healthcare costs and informal costs for families and patients, while maintaining equivalent clinical outcomes as traditional in-person care.
Acknowledgments
The authors gratefully acknowledge funding for this study from the Patient-Centered Outcomes Research Institute. The authors also thank K McKoy, A Armstrong and T Hoerger for valuable feedback.
Disclaimer
The contents of this work are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology Committee.
Financial & competing interests disclosure
Research reported in this manuscript was funded through a contract with the Patient-Centered Outcomes Research Institute (PCORI) (IDIQ-SOW #16-INSIGHT-AOSEPP-ENG). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
HHS CDC NCHS (U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics). (2015). NHANES questionnaire data 2013–2014 [Dataset]. https://wwwn.cdc.gov/nchs/nhanes/search/datapage.aspx?Component=Questionnaire&CycleBeginYear=2013
2.
Kolli SS, Amin SD, Pona A, Cline A, Feldman SR. Psychosocial impact of psoriasis: a review for dermatology residents. Cutis 102(5), 21–25 (2018).
3.
Glazer A, Farberg A, Winkelmann R, Rigel D. Analysis of trends in geographic distribution and density of US dermatologists. JAMA Dermatol. 153(4), 322–325 (2017).
4.
Armstrong AW, Ford AR, Chambers CJ et al. Online care versus in-person care for improving quality of life in psoriasis: a randomized controlled equivalency trial. J. Invest. Dermatol. 139(5), 1037–1044 (2018).
•• Presents quality of life results as measured by the Dermatology Life Quality Index between patients in the online and in-person groups.
5.
Armstrong AW, Chambers CJ, Maverakis E et al. Effectiveness of online vs in-person care for adults with psoriasis: a randomized clinical trial. JAMA Network Open 1(6), e183062 (2018).
•• Presents the results of the PASI and BSA scores between patients in the online and in-person groups.
6.
Ford AR, Gibbons CM, Torres J et al. Access to dermatological care with an innovative online model for psoriasis management: results from a randomized controlled trial. Telemed. J. E. Health 5(7), 619–627 (2018).
•• Presents the results of travel distance and time between the online and in-person groups.
7.
Krupinski E, Barker G, Rodriguez G et al. Telemedicine versus in-person dermatology referrals: an analysis of case complexity. Telemed. J. E. Health 8(2), 143–147 (2002).
8.
U.S. Census Bureau. Quickfacts: United States (2018). https://www.census.gov/quickfacts/fact/table/US/PST045218
9.
Armstrong AW, Robertson AD, Wu J, Schupp C, Lebwohl MG. Undertreatment, treatment trends, and treatment dissatisfaction among patients with psoriasis and psoriatic arthritis in the United States: findings from the National Psoriasis Foundation surveys, 2003–2011. J. Am. Acad. Dermatol. 149(10), 1180–1185 (2013).
10.
Icen M, Crowson CS, McEvoy MT, Dann FJ, Gabriel SE, Maradit Kremers H. Trends in incidence of adult-onset psoriasis over three decades: a population-based study. J. Am. Acad. Dermatol. 60(3), 394–401 (2009).
11.
Ogdie A, Haynes K, Troxel AB et al. Risk of mortality in patients with psoriatic arthritis, rheumatoid arthritis and psoriasis: a longitudinal cohort study. Ann. Rheum. Dis. 73(1), 149–153 (2014).
12.
Takeshita J, Gelfand JM, Li P et al. Psoriasis in the US Medicare population: prevalence, treatment, and factors associated with biologic use. J. Invest. Dermatol. 135(12), 2955–2963 (2015).
13.
Wolff JL, Roter DL. Family presence in routine medical visits: a meta-analytical review. Soc. Sci. Med. 72(6), 823–831 (2011).
14.
Parsi K, Chambers CJ, Armstrong AW. Cost-effectiveness analysis of a patient-centered care model for management of psoriasis. J. Am. Acad. Dermatol. 66(4), 563–570 (2012).
• Compares costs of online and in-person psoriasis care at an academic medical center.
15.
HHS AHRQ (Agency for Healthcare Research and Quality) (2019). MEPS HC-201: 2017 Full Year Consolidated Data File [Dataset]. https://meps.ahrq.gov/mepsweb/data_stats/download_data_files_detail.jsp?cboPufNumber=HC-201
16.
Beyer V, Wolverton SE. Recent trends in systemic psoriasis treatment costs. J. Am. Acad. Dermatol. 146(1), 46–54 (2010).
17.
Rothstein BE, Gonzalez J, Cunningham K et al. Direct and indirect patient costs of dermatology clinic visits and their impact on access to care and provider preference. Cutis 100(6), 405–410 (2017).
18.
BLS DOL (2018). Earnings, median usual weekly earnings, employed full time, 2018, by quarter. Labor force statistics from the Current Population Survey. Series ID LEU0252881500. https://www.bls.gov/cps/
19.
BLS DOL (Bureau of Labor Statistics, U.S. Department of Labor) (2019). Employer costs for employee compensation for December 2018. https://www.bls.gov/regions/southwest/news-release/employercostsforemployeecompensation_regions.htm
20.
BLS DOL (Bureau of Labor Statistics, U.S. Department of Labor) (2018). Civilian labor force participation rate, seasonally adjusted total for all months in 2018. https://www.bls.gov/charts/employment-situation/civilian-labor-force-participation-rate.htm
21.
BLS DOL (Bureau of Labor Statistics, U.S. Department of Labor) (2018). Earnings, median usual weekly earnings, employed full time, 2018. Labor force statistics from the Current Population Survey. Series ID LEU0254543600, LEU0258117500. https://www.bls.gov/cps/
22.
Chambers CJ, Parsi K, Schupp C et al. Patient-centered online management of psoriasis: a randomized controlled equivalency trial. J. Am. Acad. Dermatol. 66(6), 948–953 (2011).
23.
HHS AHRQ (Agency for Healthcare Research and Quality) (2019). MEPS HC-199: 2017 Medical Conditions File [Dataset]. https://meps.ahrq.gov/mepsweb/data_stats/download_data_files_detail.jsp?cboPufNumber=HC-199
24.
USDA ERS (Economic Research Service) (2013). 2013 Rural-Urban Continuum Codes [Dataset]. https://www.ers.usda.gov/data-products/rural-urban-continuum-codes/
25.
MACPAC (Medicaid and CHIP Payment and Access Commission) (2018). Report to Congress on Medicaid and CHIP: june 2018. https://www.macpac.gov/wp-content/uploads/2018/06/June-2018-Report-to-Congress-on-Medicaid-and-CHIP.pdf
26.
Ashwood JS, Mehrotra A, Cowling D, Uscher-Pines L. Direct-to-consumer telehealth may increase access to care but does not decrease spending. Health Aff. 36(3), 485–491 (2017).
27.
Mann DM, Chen J, Chunara R, Testa PA, Nov O. COVID-19 transforms health care through telemedicine: evidence from the field. J. Am. Med. Inform. Assoc. ocaa072, https://doi.org/10.1093/jamia/ocaa072 (2020).
28.
Perkins S, Cohen JM, Nelson CA, Bunick CG. Teledermatology in the era of COVID-19: experience of an academic department of dermatology. JAMA Dermatol. 83(1), e43–e44 (2020).
• Describes the experience of caring for patients in a dermatology clinic using telehealth during COVID-19.
Information & Authors
Information
Published In
Copyright
© 2021 Future Medicine Ltd.
History
Received: 14 March 2021
Accepted: 7 October 2021
Published online: 8 November 2021
Keywords:
Topics
Authors
Funding Information
Patient-Centered Outcomes Research Institute: IDIQ-SOW #16-INSIGHT-AOSEPP-ENG
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
An economic evaluation of teledermatology care delivery for chronic skin diseases. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0062
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Julia L Armstrong, Salma Bennis, Jessica N Smock, Marc M Kesselman, Teledermatology for Older Adults With a Focus on Nursing Home Residents: A Scoping Review of Clinical and System-Level Benefits, Cureus, 10.7759/cureus.102891, (2026).
- Julia Beck, Renielle Goncalves De Lira, Lara Valeska Maul, Florian Anzengruber, Christiane Brockes, Barbara Meier-Schiesser, Ralph P. Braun, Christian Greis, Teledermatological services at a Swiss university hospital - evaluation of patient benefits and economic impact , Journal of Dermatological Treatment, 10.1080/09546634.2025.2555189, 36, 1, (2025).
- Thanh Lu, Sophia D'Angelo, Zohra Tayebali, Matthew Dempsey, Kristen Giombi, Olga Khavjou, Impact analysis of expanded access to ketamine for treatment-resistant depression, Journal of Comparative Effectiveness Research, 10.57264/cer-2024-0233, 14, 6, (2025).
- Sarah N. Rimmer, Jessica N. Pixley, Steven R. Feldman, Digital health in psoriasis, The Digital Doctor, 10.1016/B978-0-443-15728-8.00029-X, (387-416), (2025).
- Rachael Pattinson, Nirohshah Trialonis-Suthakharan, Tim Pickles, Jennifer Austin, Allison FitzGerald, Matthias Augustin, Christine Bundy, Measurement properties and interpretability of the Patient-Reported Impact of Dermatological Diseases (PRIDD) measure, British Journal of Dermatology, 10.1093/bjd/ljae267, 191, 6, (936-948), (2024).
- Kristen Fernandez, Albert T. Young, Abhishek Bhattarcharya, Ayan Kusari, Maria L. Wei, Artificial Intelligence and Teledermatology, Teledermatology, 10.1007/978-3-031-27276-9_18, (173-182), (2023).