Discharges against medical advice and 30-day healthcare costs: an analysis of commercially insured adults
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Prior literature detailing the consequences of a discharge against medical advice (DAMA) has not focused on costs. We examine costs following a DAMA. Materials & methods: This retrospective cohort study utilized the IQVIA PharMetrics® Plus database to identify adults hospitalized during 2007–2015. We compared 30-day postdischarge healthcare costs between matched DAMA and routinely discharged groups. Results: Thirty-day healthcare costs for the DAMA group were US$1078 (95% CI: US$434–1730) higher, driven by inpatient readmissions (US$979; 95% CI: US$415–1543) and emergency department visits (US$79; 95% CI: US$56–102). Costs due to prescription drug fills were lower in the DAMA group. Conclusion: A DAMA was associated with higher 30-day postdischarge healthcare costs compared with routine discharges.
A discharge against medical advice (DAMA), when a patient leaves the hospital prior to a physician recommended discharge represents approximately 1–2% of all inpatient discharges in the USA [1]. Due to incomplete inpatient care, a DAMA has been found to be associated with a twofold increased risk of 30-day mortality and inpatient readmission, as well as a 2.5-times greater likelihood of an emergency department (ED) visit compared with a routine discharge [2–9]. Although the clinical consequences of a DAMA beyond the index hospitalization have been studied, only a few studies have examined the cost of a DAMA and the available studies have focused on the inpatient setting [10,11]. A prior study based on a sample of individuals with a pneumonia-related hospitalization found that a DAMA was associated with lower index hospitalization costs and a shorter length of stay compared with a routine discharge [11]. Another study based in a single urban hospital setting found the cost of a 30-day readmission after a DAMA to be 56% higher (US$10,761 vs US$3716) than the cost of the index hospitalization [10]. However, these studies quantified the cost burden due to a DAMA during the index hospitalization [11], focused on a specific disease area [11], or were limited to a single hospital setting or state system [10,11].
Beyond inpatient readmissions, little is known about the economic consequences of a DAMA in the postdischarge period. Specifically, there is uncertainty about whether reduced outpatient care coordination at the time of a DAMA has implications for cost accumulation in the postdischarge period [12,13]. The majority of patients with a DAMA do not receive prescriptions or discharge follow-up information [12,13]. Specifically, the proportion of individuals with a DAMA who receive medication prescriptions and outpatient follow-up plans at the time of discharge is less than one quarter and less than a third, respectively [12].
In light of these significant gaps in the literature, the objective of the present study was to evaluate the association between a DAMA and all-cause direct medical costs in the 30-day postdischarge period among commercially insured adults. Commercially insured adults account for approximately one in five discharges against medical advice [14]. An analysis of the economic consequences of a DAMA in this population provides a useful benchmark against which to compare future cost estimates and ultimately support the design of interventions and evidence-based decision making to improve postdischarge healthcare delivery.
We examine healthcare costs associated with a DAMA across all points of service including inpatient readmissions, ED visits, physician office visits, nonphysician outpatient services (e.g., pathology, radiology, outpatient surgical services), and prescription drug fills. We hypothesize that costs that may have been saved during a hospital admission that resulted in a DAMA (i.e., due to the shorter length of stay), will appear elsewhere in the healthcare system during the post-discharge period.
Materials & methods
Data source
This retrospective study utilized a 10% random sample of enrollees in the IQVIA PharMetrics Plus database, which is comprised of fully adjudicated administrative medical and pharmacy claims data and enrollment information for commercially insured individuals. The enrolled population in the database is considered to be generally representative of adults less than 65 years of age with commercial insurance (including a subset of commercial Medicare and Medicaid plans) in the US with respect to both age and gender. The database comprises over 70 contributing health plans and self-insured employer groups throughout the US for more than 140 million enrollees between 2006 and 2015. The database allows follow-up of individuals using medical claims, pharmacy claims and insurance eligibility. The medical claims file provides information on healthcare services provided in various care settings (e.g., inpatient, outpatient). The pharmacy claims file provides information on prescription drug fills in the retail, specialty and mail-order settings. The eligibility file provides individual-level demographic and insurance eligibility information.
Study population
We identified individuals that met the following inclusion criteria: an inpatient admission record between 1 January 2007 and 31 December 2015; age 18–64 years old at the time of admission; continuous medical and prescription drug coverage in the period 6-months prior (baseline period) to the date of admission through 30-days following hospital discharge (follow-up period). We excluded inpatient admissions that had a missing discharge disposition, resulted in an in-hospital death, or resulted in a discharge to a short-term hospital, skilled nursing facility, or any other type of facility. The first inpatient admission that met all the above criteria was defined as the index admission.
Main predictor variable
To identify individuals with a DAMA, we utilized the ‘Patient Status Code’ variable, representing the hospital discharge disposition of each individual in the dataset. The individuals with a DAMA were analyzed as the case group. The control group was a matched sample and comprised of individuals who were discharged to home/self-care or to a home health organization (hereafter referred to as routine discharge).
Demographic, clinical & hospitalization characteristics
The following variables were identified based on the index hospital admission: age, sex, region of residence, year of admission and timing of admission (weekday/weekend). The following variables were defined during the hospital stay: length of stay and evidence of any surgical procedure performed. Finally, during the 6-month baseline period, we used the Elixhauser algorithm to categorize comorbid conditions based on International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes [15,16].
Costs
All cost results were reported for the matched sample. All-cause direct healthcare costs were computed during the 30-day postdischarge period. These included costs for inpatient readmissions, ED visits, physician office visits and nonphysician outpatient services (e.g., pathology, radiology, outpatient surgical services). Further, the costs included pharmacy costs that represent medication fills for which claims were filed. The total healthcare cost was calculated by summing the medical and pharmacy costs. We conducted the analysis from a payer’s perspective and all costs represented those paid by the health plan to the provider for covered healthcare services rendered to the beneficiary. All costs were inflated to 2015 US dollars using the medical care component of the Consumer Price Index produced by the United States Bureau of Labor Statistics [17].
Statistical analysis
Descriptive analysis
We utilized t-tests to describe continuous variables (except cost) and chi-square tests to describe categorical variables. We utilized the Wilcoxon rank sum test to report results based on the cost of the index hospitalization. Summary statistics (mean, standard deviation and median) were reported for the cost outcomes.
Propensity score matching
Based on propensity scores, we used a 1:1 greedy matching algorithm to match cases and controls [18]. The propensity score model included the following variables: age, sex, region of residence, Elixhauser comorbidity index, year of inpatient admission, timing of inpatient admission (weekday/weekend), length of stay on the index hospitalization, cost of the index hospitalization and presence of any surgical procedure during the inpatient admission. These confounders were selected due to their association with both a DAMA and postdischarge healthcare costs. We used a maximal caliper width of 0.2 of the standard deviation of the logit of the propensity score to identify the best match between cases and controls [19]. We calculated standardized differences and utilized a maximum value of 0.1 to represent balance (based on observable measures) between cases and controls (see Supplementary Table 1 & Supplemental Digital Content 1) [20,21].
Regression analysis
Due to the skewed nature of the cost outcomes (see Supplementary Figure 1–6 & Supplemental Digital Content 1), we generated model coefficients using two-part models. These models help account for the substantial number of individuals that incur no medical costs during the 30-day follow-up period [22]. The first part utilizes a logistic regression model that predicts the probability of whether an individual generated zero or nonzero costs. The second part utilizes a generalized linear model that predicts cost conditional on generating strictly positive costs. The modified Park test was used to guide the choice of the probability distribution for the response variable [22].
In order to report an average cost in dollars (i.e., natural units of the response variable), we calculated the average marginal effect for the DAMA indicator (i.e., expected incremental 30-day cost attributable to a DAMA) [23]. We estimated the CI for the average marginal effect using the delta method [24]. All results based on the regression analysis are presented for the matched sample only. All analyses were conducted using SAS version 9.4, and statistical significance was set at α = 0.05.
Results
For the unmatched sample, we identified 457,530 individuals that met our inclusion criteria of which 0.5% had a DAMA during the study period. A consort diagram (see Supplementary Figure 7 & Supplemental Digital Content 1) provides the sample breakdown based on the application of study inclusion and exclusion criteria. A comparison of demographic, clinical and hospitalization characteristics across the DAMA and routine discharge groups is displayed in Table 1. A larger proportion of individuals in the DAMA group were younger (age group 18–29 years: 24 vs 20.9%, p < 0.01) compared with those discharged routinely. The DAMA group had a higher proportion of males (58.4 vs 33.1%, p < 0.01) as compared with the routine discharge group. Individuals with a DAMA also had a higher comorbidity burden at the time of the index admission (Elixhauser score of 3+: 27.6 vs 17.9%) as compared with those discharged routinely. Individuals with a DAMA had a shorter median length of stay for the index admission (1 day vs 2 days) and lower median cost for the index admission ($5028 vs 9860) as compared with those discharged routinely.
| Variable | Total population (n = 457,530) (100%) | DAMA (n = 2245) (0.5%) | Routine discharge (n = 455,285) (99.5%) | p-value | |||
|---|---|---|---|---|---|---|---|
| n | Col % | n | Col% | n | Col% | ||
| Age (at admission): | <0.01 | ||||||
| – Mean ± SD, median (years) | 43 ± 13, 42 | 42 ± 14, 43 | 43 ± 13, 42 | ||||
| – 18–29 years | 95,447 | 20.9 | 538 | 24.0 | 94,909 | 20.9 | |
| – 30–39 years | 112,702 | 24.6 | 414 | 18.4 | 112,288 | 24.6 | |
| – 40–49 years | 80,489 | 17.6 | 498 | 22.2 | 79,991 | 17.6 | |
| – >50 years | 168,892 | 36.9 | 795 | 35.4 | 168,097 | 36.9 | |
| Gender: | <0.01 | ||||||
| – Female | 305,640 | 66.8 | 934 | 41.6 | 304,706 | 66.9 | |
| – Male | 151,890 | 33.2 | 1311 | 58.4 | 150,579 | 33.1 | |
| Region: | <0.01 | ||||||
| – East | 82,747 | 18.1 | 754 | 33.6 | 81,993 | 18.0 | |
| – Midwest | 145,580 | 31.8 | 489 | 21.8 | 145,091 | 31.9 | |
| – South | 194,204 | 42.5 | 869 | 38.7 | 193,335 | 42.5 | |
| – West | 34,999 | 7.6 | 133 | 5.9 | 34,866 | 7.6 | |
| Elixhauser score: | <0.01 | ||||||
| – 0 | 214,478 | 46.9 | 703 | 31.3 | 213,775 | 46.9 | |
| – 1–2 | 161,183 | 35.2 | 923 | 41.1 | 160,260 | 35.2 | |
| – >2 | 81,869 | 17.9 | 619 | 27.6 | 81,250 | 17.9 | |
| Timing of admission: | <0.01 | ||||||
| – Weekday | 382,844 | 83.7 | 1747 | 77.8 | 381,097 | 83.7 | |
| – Weekend | 74,686 | 16.3 | 498 | 22.2 | 74,188 | 16.3 | |
| Year of admission: | <0.01 | ||||||
| – 2007–2009 | 138,755 | 30.3 | 598 | 26.6 | 138,157 | 30.4 | |
| – 2010–2012 | 163,083 | 35.7 | 750 | 33.4 | 162,333 | 35.6 | |
| – 2013–2015 | 155,692 | 34.0 | 897 | 40.0 | 154,795 | 34.0 | |
| Surgery during stay: | <0.01 | ||||||
| – Yes | 269,727 | 58.9 | 290 | 12.9 | 269,437 | 59.2 | |
| – No | 187,803 | 41.1 | 1955 | 87.1 | 185,848 | 40.8 | |
| Length of stay (days): | <0.01 | ||||||
| – Mean ± SD, median | 2.89 ± 3.36, 2 | 2.21 ± 3.30, 1 | 2.90 ± 3.36, 2 | ||||
| Cost of index hospitalization (US$): | <0.01 | ||||||
| – Mean ± SD, median | 14,560 ± 17,573, 9836 | 7598 ± 14,595, 5028 | 14,594 ± 17,580, 9860 | ||||
DAMA: Discharge against medical advice.
The propensity-score matched sample consisted of 2245 cases and 2245 controls (see Supplementary Table 1 & Supplemental Digital Content 1). Reviewing the standardized differences, the cases and controls in the matched sample were comparable based on observable measures. Using the matched sample, we compared the proportion of individuals with healthcare utilization for different points of service across the DAMA and non-DAMA groups in the postdischarge period (Figure 1). A higher proportion of individuals with a DAMA had an ED visit compared with those discharged routinely (19 vs 9%, p < 0.01). In addition, a higher proportion of individuals with a DAMA had an inpatient readmission compared with those discharged routinely (20 vs 17%, p = 0.01). A lower proportion of individuals with a DAMA had a physician office visit (59 vs 63%, p < 0.01) and a prescription drug fill (71 vs 80%, p < 0.01) during the 30-day follow-up period. There was no statistically significant difference in the proportion of individuals with nonphysician outpatient service use (67 vs 69%, p = 0.2).
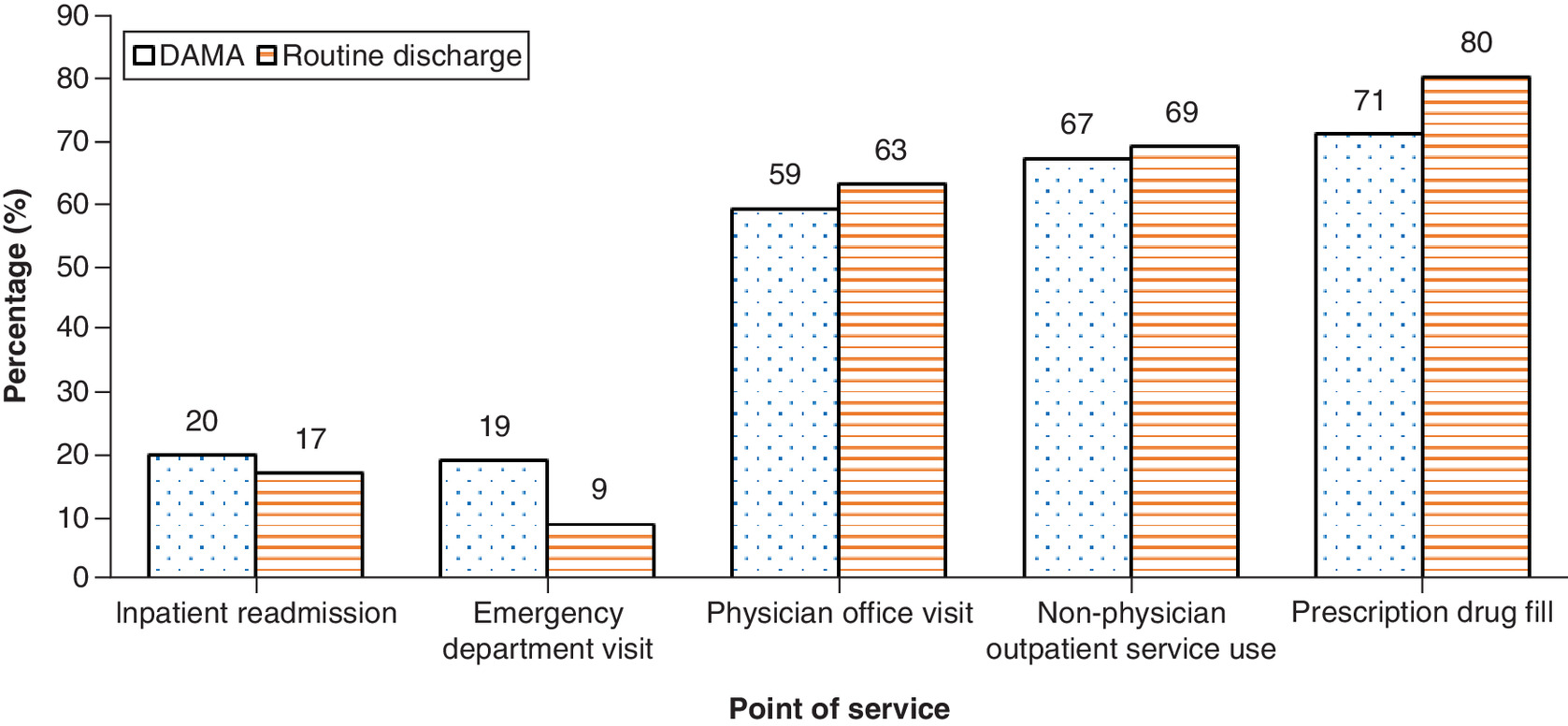
Figure 1. Proportion of individuals with healthcare utilization for the discharge against medical advice and routinely discharged groups.
DAMA: Discharge against medical advice.
Costs
Summary statistics
Table 2 illustrates healthcare costs in the 30-day postdischarge period across cases and controls in the matched sample. Individuals with a DAMA generated higher mean total healthcare costs ($4709 vs 3423) as compared with those discharged routinely. Similar findings were observed across both groups for mean costs attributable to inpatient readmissions ($2876 vs 1691), ED visits ($141 vs 62), and nonphysician outpatient services ($1301 vs 1210). The converse was observed across both groups for mean costs attributable to physician office visits ($125 vs 129) and prescription drug fills ($264 vs 329).
| Healthcare costs | DAMA (US$), n = 2245 | Routine discharge (US$), n = 2245 | ||
|---|---|---|---|---|
| Mean (SD) | Median | Mean (SD) | Median | |
| Total | 4709 (13,484) | 933 | 3423 (10,504) | 703 |
| Inpatient | 2876 (12,239) | 82 | 1691 (8,981) | 74 |
| Emergency department | 141 (497) | 0 | 62 (285) | 0 |
| Physician office | 125 (230) | 58 | 129 (204) | 65 |
| Nonphysician outpatient | 1301 (3896) | 94 | 1210 (3725) | 89 |
| Prescription drugs | 264 (780) | 20 | 329 (1425) | 26 |
DAMA: Discharge against medical advice.
Incremental cost analysis
We report the average incremental costs for individuals with a DAMA compared with those discharged routinely (Table 3). For individuals with a DAMA, the total 30-day adjusted postdischarge incremental costs were significantly higher (US$1078; 95% CI: US$434–1730) compared with those discharged routinely. These costs were driven by inpatient readmissions (US$979; 95% CI: US$415–1543) and ED visits (US$79; 95% CI: US$56–102). Conversely, incremental costs for prescription drug fills (US$-65; 95% CI: US$-130 to -0.4) were lower among those with a DAMA compared with those discharged routinely. No statistically significant difference was observed across both groups in terms of costs attributable to physician office visits (US$-4; 95% CI: US$-17 to 9) and nonphysician outpatient services (US$91; 95% CI: US$-132 to 314).
| Incremental cost (US$) | 95% CI | |
|---|---|---|
| Total | 1078 | 434–1730 |
| Inpatient | 979 | 415–1543 |
| Emergency department | 79 | 56–102 |
| Physician office | -4 | -17 to 9 |
| Nonphysician outpatient | 91 | -132 to 314 |
| Prescription drug | -65 | -130 to -0.4 |
Discussion
Using administrative claims data for a commercially insured population over a 9-year study period, we quantified the economic consequences associated with a DAMA in the postdischarge period. We found that compared with a routine discharge, hospitalizations ending in a DAMA generated higher mean total 30-day post-discharge healthcare costs. Cost differences were distributed across the spectrum of care, with higher costs for DAMA driven primarily by inpatient readmissions and to a lesser extent by ED visits, but not by prescription drug fills, physician office visits or nonphysician outpatient services.
Our findings on the prevalence of a DAMA (0.5%) differ from prior estimates (1–2%) reported in the literature. Prior studies evaluating a DAMA are based on mixed payer populations, primarily composed of publicly insured or uninsured stays that comprise a disproportionate amount of all discharges against medical advice nationally [2–8,14]. Conversely, hospital stays covered by commercial insurance are the lowest proportion of all DAMA [14]. Compared with routine discharges, our findings on the demographic and admission characteristics of individuals within the DAMA group are consistent with prior literature [4].
Contrary to prior literature [2–8], we found no significant difference in the prevalence of 30-day inpatient readmission across the DAMA and routinely discharged groups. This may be attributable to differences between our study population and those used in prior studies. For example, prior studies utilized mixed payer populations of older age (mean age 55 years and older) and reported a higher comorbidity burden as compared with our commercially insured sample [2–8]. We found that 30-day inpatient readmission costs were higher for the DAMA group compared with those with a routine discharge. This may be attributable to a longer length of stay associated with a readmission after a DAMA. For example, HIV-infected patients with a history of drug abuse and a DAMA were more likely to have a longer length of stay on their readmission compared with their index hospitalization [25].
We also found that individuals with a DAMA had higher ED costs as compared with those with a routine discharge during the postdischarge period. These findings may be explained by the increased likelihood of ED utilization after a DAMA as compared with a routine discharge [2]. Our findings of lower costs associated with outpatient care may be due to a range of factors. In this study population, patients with a DAMA were more likely to have greater comorbidity burden at the time of discharge and may have needed more inpatient and ED services after leaving the hospital prematurely. Patients with a DAMA may also be less engaged with outpatient providers and thus less likely to return for care there. This may be due to persistent stigma these patients experience in the inpatient environment [26], challenges with access to timely outpatient care, or patient preference for inpatient or ED care. Qualitative studies to identify patient's perspectives on post-discharge costs could help to identify potential barriers to the use of outpatient care.
This study evaluated broad, healthcare system costs attributable to a DAMA beyond inpatient and ED readmissions. Our findings have implications for how hospitals approach transitional care planning in the postdischarge period as well as for payers who bear the burden of postdischarge costs regardless of where they occur across the spectrum of care. Given our findings related to inpatient- and ED-related costs, hospitals can redouble efforts to optimize coordination of care with patients’ outpatient providers, their outpatient medication regimen, and other outpatient services. Based on qualitative studies of reasons for a DAMA, patients are receptive to outpatient follow-up from the hospital after the hospital stay [27,28].
From a payer’s perspective, 30-day inpatient readmission holds the greatest cost-savings potential as costs remained higher in our study even though there was no difference in the prevalence of 30-day inpatient readmissions across both groups. Our study was designed to quantify the direct medical costs to payers and did not measure direct nonmedical, indirect or intangible costs following a hospital discharge. Further investigation of these costs from a patient or family perspective will shed more light on tradeoffs patients reportedly make when choosing to delay their acute care needs to care for other family members, avoid lost productivity at work, manage fear of losing employment, and to offset the financial implications of hospitalization [27,28]. In addition, it will be important to identify best practices for provider-patient communication that address patient tradeoffs between promoting their health and other obligations.
This study’s strengths lie in its contribution to the limited evidence regarding the direct medical costs following a DAMA. Our review of the literature identified two DAMA cost studies [9,10]. Both cost studies focused on the inpatient setting: either summing costs based on the index hospital admission or summing costs based on hospital readmissions that occurred within 30 days of the index hospital admission [9,10]. Given the imbalance between the DAMA and routinely discharged groups in the cost of the index hospitalization, we included index hospitalization costs in the propensity score model. Extending prior studies, we adopted a health system-wide view of postdischarge utilization and included utilization from all points of service within the healthcare system. We also extended beyond prior studies by reporting the incremental costs of a DAMA relative to matched controls. The matching process was important given baseline differences between the DAMA group and routine discharge groups. In future work using larger datasets, the incremental cost of a DAMA should be quantified for clinically important subgroups with an above-average prevalence of DAMA, such as individuals diagnosed with mental health or substance use disorders.
There are limitations to this study. The study was conducted among individuals with commercial insurance and our findings do not generalize to publicly insured samples. We were unable to include individual-level factors that may correlate with costs such as measures of disease severity, employment status, and income. The use of propensity score methods to balance both comparison groups on observable sources of confounding does not preclude the possibility of residual confounding. In the absence of mortality data, we were unable to account for death. Given the age demographics of the sample, we do not expect high or differential postdischarge mortality rates for the DAMA group. At last, although there is some evidence of attenuation in the relationship between DAMA and readmissions over time, we did not examine variation in the cost of DAMA for different follow-up periods [6,29]. It is unclear whether this variation persists in the ED and outpatient settings. Despite these limitations, we expect that our results provide a reasonable characterization of the postdischarge direct medical costs associated with a DAMA across points of care.
Conclusion
Among individuals with commercial insurance, discharges against medical advice are uncommon. At the same time, hospitalizations ending in a DAMA are associated with higher costs during the 30-day post-discharge period, compared to routine discharges. Specifically, a DAMA was associated with higher hospital readmissions and ED costs as well as lower prescription drug costs, compared to routine discharges. This study reports on the direct medical costs associated with a DAMA in the postdischarge period. The results suggest a need for increased care coordination across inpatient and outpatient settings following a DAMA. More information is needed from the patient’s perspective and from publicly insured samples to better understand the cost burden and inform care coordination strategies following a DAMA.
•
A discharge against medical advice (DAMA), when a patient leaves the hospital prior to a physician recommended discharge, represents approximately 1–2% of all inpatient discharges in the United States.
•
While the clinical consequences of a DAMA are well-documented, less is known about the costs of a DAMA. The available cost studies are limited in number and in scope, focusing on the inpatient setting or on a single institution.
•
We examine whether direct medical costs that may have been saved during a hospital admission that resulted in a DAMA (i.e., due to the shorter length of stay) appear elsewhere in the healthcare system, namely, in terms of postdischarge utilization of inpatient services, outpatient services and prescription drugs.
•
The total 30-day adjusted postdischarge incremental costs of a DAMA were significantly higher (US$1078; 95% CI: US$434–1730) compared with routine discharges.
•
Costs due to 30-day inpatient (US$979; 95% CI: US$415–1543) and emergency department services (US$79; 95% CI: US$56–102) were higher in the DAMA group.
•
Costs due to 30-day prescription drug fills (US$-65; 95% CI: US$-130 to -0.4) were lower in the DAMA group. There were no significant differences in physician office visit and nonphysician outpatient services costs across both groups.
•
Future research should determine whether these findings extend to publicly insured and uninsured individuals where the prevalence of DAMA is higher. Future studies, based on the patient perspective, should include direct nonmedical and indirect postdischarge costs.
Author contributions
E Onukwugha was responsible for study conception, design, interpretation of study results, data acquisition, drafting and revision of the manuscript; AB Gandhi was responsible for design, data analysis and interpretation of study results, drafting and revision of the manuscript; D Alfandre was responsible for interpretation of study results, drafting and revision of the manuscript.
Acknowledgments
The statements, findings, conclusions, views, and opinions contained and expressed in this manuscript are based in part on data obtained under license from IQVIA. Source: IQVIA PharMetrics® Plus January 2006 – December 2015, IQVIA. All Rights Reserved. The statements, findings, conclusions, views and opinions contained and expressed herein are not necessarily those of IQVIA or any of its affiliated or subsidiary entities. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the US Department of Veterans Affairs, the US Government or the VA National Center for Ethics in Health Care.
Financial & competing interests disclosure
The authors acknowledge the support of the University of Maryland, Baltimore, Institute for Clinical & Translational Research (ICTR) through the ICTR Voucher Program. E Onukwugha reports grants from Bayer Healthcare Pharmaceuticals, grants from Pfizer, Inc., outside this submitted work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This study was approved by the University of Maryland, Baltimore Institutional Review Board (HP-00081497).
Supplementary Material
File (supplementary materials.docx)
- Download
- 224.03 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Alfandre DJ. “I'm going home”: discharges against medical advice. Mayo Clin. Proc. 84(3), 255–260 (2009).
• This much-cited review paper provides a useful overview of discharge against medical advice (DAMA) studies to date.
2.
Baptist AP, Warrier I, Arora R, Ager J, Massanari RM. Hospitalized patients with asthma who leave against medical advice: characteristics, reasons, and outcomes. J. Allergy Clin. Immunol. 119(4), 924–929 (2007).
3.
Fiscella K, Meldrum S, Barnett S. Hospital discharge against advice after myocardial infarction: deaths and readmissions. Am. J. Med. 120(12), 1047–1053 (2007).
4.
Kumar N. Burden of 30-day readmissions associated with discharge against medical advice among inpatients in the United States. Am. J. Med. 132(6), 708–717.e704 (2019).
5.
Kwok CS, Walsh MN, Volgman A et al. Discharge against medical advice after hospitalisation for acute myocardial infarction. Heart 105(4), 315–321 (2019).
6.
Onukwugha E, Mullins D, Loh FE, Saunders E, Shaya FT, Weir MR. Readmissions after unauthorized discharges in the cardiovascular setting. Med. Care 49(2), 215–224 (2011).
7.
Patel B, Prousi G, Shah M et al. Thirty-day readmission rate in acute heart failure patients discharged against medical advice in a matched cohort study. Mayo Clin. Proc. 93(10), 1397–1403 (2018).
8.
Southern WN, Nahvi S, Arnsten JH. Increased risk of mortality and readmission among patients discharged against medical advice. Am. J. Med. 125(6), 594–602 (2012).
9.
Tan SY, Feng JY, Joyce C, Fisher J, Mostaghimi A. Association of hospital discharge against medical advice with readmission and in-hospital mortality. JAMA Netw. Open 3(6), e206009–e206009 (2020).
10.
Aliyu Z. Discharge against medical advice: sociodemographic, clinical and financial perspectives. Int. J. Clin. Pract. 56(5), 325–327 (2002).
•• Includes results on the cost of a DAMA.
11.
Saitz R, Ghali WA, Moskowitz MA. The impact of leaving against medical advice on hospital resource utilization. J. Gen. Intern. Med. 15(2), 103–107 (2000).
•• Reports on the cost of a DAMA.
12.
Edwards J, Markert R, Bricker D. Discharge against medical advice: how often do we intervene? J. Hosp. Med. 8(10), 574–577 (2013).
13.
Stearns CR, Bakamjian A, Sattar S, Weintraub MR. Discharges against medical advice at a county hospital: provider perceptions and practice. J. Hosp. Med. 12(1), 11–17 (2017).
14.
Hospitalizations in which Patients Leave the Hospital against Medical Advice (AMA), 2007. HCUP Statistical Brief #78. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb78.pdf
15.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med. Care 36(1), 8–27 (1998).
16.
The Epidemiology and Outcomes of Critical Illness in Manitoba. http://mchp-appserv.cpe.umanitoba.ca/reference/MCHP_ICU_Report_WEB_(20120403).pdf
17.
Measuring Price Change in the CPI: medical care. https://www.bls.gov/cpi/factsheets/medical-care.htm
18.
Austin PC. A comparison of 12 algorithms for matching on the propensity score. Stat. Med. 33(6), 1057–1069 (2014).
19.
Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 10(2), 150–161 (2011).
20.
Austin PC, Mamdani MM. A comparison of propensity score methods: a case-study estimating the effectiveness of post-AMI statin use. Stat. Med. 25(12), 2084–2106 (2006).
21.
Normand S-LT, Landrum MB, Guadagnoli E et al. Validating recommendations for coronary angiography following acute myocardial infarction in the elderly: a matched analysis using propensity scores. J. Clin. Epidemiol. 54(4), 387–398 (2001).
22.
Glick HA, Doshi JA, Sonnad SS, Polsky D. Economic Evaluation in Clinical Trials. Oxford University Press, Oxford, UK (2014).
23.
Onukwugha E, Bergtold J, Jain R. A primer on marginal effects—part II: health services research applications. Pharmacoeconomics 33(2), 97–103 (2015).
24.
Greene W. Econometric Analysis. Prentice Hall, NJ, USA (2012).
25.
Anis AH, Sun H, Guh DP, Palepu A, Schechter MT, O'Shaughnessy MV. Leaving hospital against medical advice among HIV-positive patients. CMAJ 167(6), 633–637 (2002).
26.
Alfandre D. Reconsidering against medical advice discharges: embracing patient-centeredness to promote high quality care and a renewed research agenda. J. Gen. Intern. Med. 28(12), 1657–1662 (2013).
• Useful paper for considering patient-centeredness in the context of discharges against medical advice.
27.
Onukwugha E, Saunders E, Mullins CD et al. A qualitative study to identify reasons for discharges against medical advice in the cardiovascular setting. BMJ Open 2(4), e000902 (2012).
28.
Onukwugha E, Saunders E, Mullins CD, Pradel FG, Zuckerman M, Weir MR. Reasons for discharges against medical advice: a qualitative study. BMJ Qual. Saf. 19(5), 420–424 (2010).
29.
Choi M, Kim H, Qian H, Palepu A. Readmission rates of patients discharged against medical advice: a matched cohort study. PLoS ONE 6(9), e24459 (2011).
Information & Authors
Information
Published In
Pages: 169 - 177
PubMed: 34783251
Copyright
© 2021 Future Medicine Ltd.
History
Received: 1 February 2021
Accepted: 28 October 2021
Published online: 16 November 2021
Keywords:
Topics
Authors
Funding Information
University of Maryland, Baltimore, Institute for Clinical & Translational Research (ICTR) through the ICTR Voucher Program
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Discharges against medical advice and 30-day healthcare costs: an analysis of commercially insured adults. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0024
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Jennifer K Shah, Mollie B Smith, Clifford C Sheckter, Care at Burn Centers Is Associated With Reduced Discharge Against Medical Advice: A National, Multi-Database Analysis, Journal of Burn Care & Research, 10.1093/jbcr/irag089, (2026).
- Aditya Kaliath, Jamie L Romeiser, Aaron Shaykevich, Ivayla I Geneva, The Determinants of Against Medical Advice Hospital Discharges, Cureus, 10.7759/cureus.97691, (2025).
- Yahya Alnashri, Elena Andreyeva, Theodoros V. Giannouchos, Trends and predictors of leaving before medically advised in US emergency departments from 2016 to 2021, The American Journal of Emergency Medicine, 10.1016/j.ajem.2024.12.081, 90, (47-54), (2025).
- Nam Yong Cho, Amulya Vadlakonda, Saad Mallick, Joanna Curry, Sara Sakowitz, Zachary Tran, Peyman Benharash, Discharge against medical advice in trauma patients: Trends, risk factors, and implications for health care management strategies, Surgery, 10.1016/j.surg.2024.06.007, 176, 3, (942-948), (2024).
- Hannah C. Decker, Casey M. Silver, Dave Graham-Squire, Logan Pierce, Hemal K. Kanzaria, Elizabeth C. Wick, Association of Homelessness with Before Medically Advised Discharge After Surgery, The Joint Commission Journal on Quality and Patient Safety, 10.1016/j.jcjq.2024.05.002, 50, 9, (655-663), (2024).
- Lauren E. Powell, Alexis Knutson, Alyssa J. Meyer, Melanie McCormick, Alexandra M. Lacey, A 15-year review of characteristics and outcomes of patients leaving against medical advice, Burns, 10.1016/j.burns.2023.10.006, 50, 3, (616-622), (2024).
- Kaleb Foster, Anne Caswell, Liz James, Hussain Jessani, Angie Polanco, Matthew Viggiano, Chase Jennings, Ho-Man Yeung, The risk factors, consequences, and interventions of discharge against medical advice - A narrative review, The American Journal of the Medical Sciences, 10.1016/j.amjms.2023.04.007, 366, 1, (16-21), (2023).