Current practice of stakeholder engagement: researchers’ experiences in North America, DACH countries and China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To explore the current practice of stakeholder engagement in clinical trials and its evaluation in North America (USA and Canada), DACH countries (Germany, Austria and Switzerland) and China. Participants & methods: We conducted a web-based, anonymous, international, cross-sectional online survey for clinical researchers. Data were analyzed using descriptive and explorative statistical analysis including analysis of variance and analysis of covariance. Results: Stakeholder engagement is more prominent and higher accepted among researchers in North America. Researchers in DACH countries have less knowledge of the stakeholder engagement method and are less likely to apply it. Conclusion: Stakeholder engagement is perceived very differently among participants from DACH countries, North America and China. For a broader acceptance and implementation institutional support and motivational conditions might be needed.
Stakeholder engagement is defined as the active involvement of an ‘individual or group who is responsible for or affected by health – and healthcare-related decisions’ in a research process [1]. Methods of engagement include both in-person meetings (e.g., focus groups, one-on-one-discussions, interviews) and technology-based approaches, such as online surveys, webinars and social media platforms [2,3]. Proponents of stakeholder engagement predict increased quality, translation and implementation of research results, and an empowerment of stakeholders through engagement [4–6]. Furthermore, it is regarded as an important approach to an open ethical discourse, not exclusively led by specialists [7]. Originating in economics [8], stakeholder engagement gains growing attention within the medical field since the establishment of the Patient-Centered Outcomes Research Institute in 2010 [9].
Patient-Centered Outcomes Research Institute offers funding opportunities specifically for studies that engage stakeholders [10]. First reports revealed that stakeholder engagement led to changes in study design, allowed a deeper understanding of end-user needs and facilitated access to study populations [11–13]. Published articles mainly report engagement of patients and clinicians, mostly in early stages of research [14].
Infrastructure for stakeholder engagement and its evaluation is continuously growing in North America (USA and Canada) and the UK [5,15]. We were aware of the advanced progress stakeholder involvement in research in UK [16–18] and assumed that UK is at a similar level as North America. Therefore, we did not specially look into this region. We have no data about practice and reception of stakeholder engagement among researchers in DACH countries (country codes for Germany, Austria and Switzerland). Also, some previous studies reported stakeholder engagement in Europe [19], in China [20], or in other world regions, however, very little attention has been paid to understand their specifics and gaps with North America in a worldwide scope.
Our aim was to identify current practices of stakeholder engagement in different world regions and factors that encourage or discourage researchers from its application. We hypothesized that stakeholder engagement is more prominent and higher accepted among researchers in North America.
Materials & methods
We performed a cross-sectional study to assess current practices and opinions about potential advantages and challenges of stakeholder engagement among clinical researchers. We conducted an anonymous web-based survey to reach an international sample and ensure feasible access to the questionnaire in three different languages (English, German and Chinese).
Development
Through a broad literature review, we identified currently discussed aspects of stakeholder engagement in clinical research which formed the six questionnaire sections: knowledge and definition; relevance and practice; potential stakeholder groups; methods for engagement; levels and stages; and perceived challenges and potential of stakeholder engagement. Most questions were designed as three-dimensional sets of questions. These represent the respondent’s existing practice, normative beliefs and future expectations on the respective aspect of stakeholder engagement. This method was adopted from existing surveys exploring current state of what is important to respondents and to give perspectives for future generations [21]. Native speakers reviewed English and Chinese translations of the initial German version. After iterative pretesting of four independent testers and a technical function test the final web-version of the questionnaire comprised 18 pages with 29 questions determining participants’ opinions on stakeholder engagement as part of clinical research (Supplementary Material 1). For survey administration, we used the noncommercial software SoSci Survey [22]. Data were stored on a secured local German server, accessible only to study team members.
Survey dissemination
Participants were recruited via e-mail and WeChat groups, addressed through lists of national and international researcher associations, among others from the field of epidemiology, public health, integrative medicine and oncology. We approached administrators of mailing lists based on their publicly available contact information or personal contacts. The questionnaire was nonmandatory, without incentive and not available on an open homepage. The study received approval from the Charité – Universitätsmedizin Berlin Ethic Committee on 3 May 2016 (Approval Number EA1/128/16) and data protection committee on 15 June 2016 (AZ 293/16). The survey was available online from 12 September 2016 to 31 October 2017. All participants were informed about the objectives of the study and could provide their informed consent by initiating the online survey. No personal identifying information or IP-addresses were collected.
Data & measurements
In the first part of the survey, sociodemographic data (year of birth, gender, first language and country of residence) and data regarding working context (professional context, position, main working field and years of working experiences) were collected.
Data regarding participants’ perspective on stakeholder engagement were collected in the second part of the survey through six questionnaire sections as above mentioned. Various types of questions were implemented, including polar question, dropdown selection, text input and predominantly scales from 0 to 10 (e.g., 0 = “do not agree at all” and 10 = “agree completely” for agreement and 0 = “never” and 10 = “always” for frequency).
Statistical analysis
Statistical analysis was performed with the open source statistical program R and R Studio [23–25]. We chose an ‘available-case’ analysis approach and included all cases with available data on sociodemographic background and general knowledge of stakeholder engagement (seventh page completed). Descriptive statistics was performed to characterize the sample and analysis of variance to compare the sample subgroups using a significance level of 5%. As different generations of researchers might answer questions differently, we controlled for the possible confounder ‘age of participant’ by conducting an explorative analysis of covariance (ANCOVA) with the covariate age. Results are reported as descriptive group means plus/minus standard deviation (SD) and p-values for group comparisons.
Results
Response rates
The newsletters and mailing lists reached about 7000 researchers. The survey recorded 842 unique site visitors, 311 respondents agreed to participate (participation rate 36.9%, Figure 1), and 154 participants submitted the last questionnaire page (completion rate 49.5%).

Figure 1. Flowchart of the response to the survey stakeholder engagement in clinical research.
WeChat: Chinese messaging, social media and mobile payment app.
DACH: Germany (D), Austria (A) and Switzerland (CH).
North America: USA and Canada.
Sample characteristics
From overall 311 survey participants, 245 completed the online survey until at least the seventh page and were included to further analysis.
A total of 27 (11%) participants stated to live in North America, 55 (22%) in DACH countries and 127 (51.84%) in China, whereas 36 (15%) indicated another or no specific country of residence. The mean age of participants from North America was 53.78 ± 10.2 years (mean ± sd), from DACH countries 48.35 ± 11.8 years, and from China 37.47 ± 8.8 years. Among participants from North America, the majority worked as principal investigators (63%). In DACH countries, principal investigators represented 49% of all participants and in China 40%, respectively.
All collected sample characteristics are given in Table 1.
| Characteristic | DACH n = 55 | North America n = 27 | China n = 127 |
|---|---|---|---|
| Age in years, mean (SD) | 48.35 (11.77) | 53.78 (10.27) | 37.47 (8.84) |
| Gender, n (%) | |||
| – Male | 23 (41.8) | 12 (44.4) | 44 (34.6) |
| – Female | 28 (50.9) | 14 (51.9) | 80 (63.0) |
| – Other | 0 (0.0) | 0 (0.0) | 1 (0.8) |
| – Prefer not to say | 2 (3.6) | 0 (0.0) | 2 (1.6) |
| – Not available | 2 (3.6) | 1 (3.7) | 0 (0.0) |
| First language, n (%) | |||
| – German | 50 (90.9) | 2 (7.4) | 0 (0.0) |
| – English | 0 (0.0) | 23 (85.2) | 1 (0.8) |
| – Chinese | 0 (0.0) | 0 (0.0) | 125 (98.4) |
| – Other | 3 (5.5) | 2 (7.4) | 0 (0.0) |
| – Not available | 2 (3.6) | 0 (0.0) | 1 (0.8) |
| Professional context, n (%) | |||
| – Industry | 4 (7.3) | 0 (0.0) | 7 (5.5) |
| – University | 34 (61.8) | 17 (63.0) | 42 (33.1) |
| – Hospital or clinic | 4 (7.3) | 9 (33.3) | 69 (54.3) |
| – Other research institution | 12 (21.8) | 1 (3.7) | 9 (7.1) |
| – Not available | 1 (1.8) | 0 (0.0) | 0 (0.0) |
| Position, n (%) | |||
| – Principal investigator | 27 (49.1) | 17 (63.0) | 51 (40.2) |
| – Research assistant | 21 (38.2) | 2 (7.4) | 35 (27.6) |
| – PhD student | 1 (1.8) | 0 (0.0) | 10 (7.9) |
| – Master student | 1 (1.8) | 0 (0.0) | 16 (12.6) |
| – Other | 4 (7.3) | 8 (29.6) | 14 (11.0) |
| – Not available | 1 (1.8) | 0 (0.0) | 1 (0.8) |
| Main working field, n (%) | |||
| – Basic research | 8 (14.5) | 2 (7.4) | 13 (10.2) |
| – Clinical and/or health service research | 29 (52.7) | 15 (55.6) | 54 (42.5) |
| – Teaching | 2 (3.6) | 1 (3.7) | 10 (7.9) |
| – Patient care | 6 (10.9) | 6 (22.2) | 38 (29.9) |
| – Other | 9 (16.4) | 3 (11.1) | 12 (9.4) |
| – Not available | 1 (1.8) | 0 (0.0) | 0 (0.0) |
| Work experience in years, mean (SD) | 12.74 (7.86) | 18.74 (9.43) | 9.85 (8.10) |
†
All characteristics were self-reported by the study participants. Percentages may not sum up to 100% because of rounding.
DACH: Germany (D), Austria (A) and Switzerland (CH); North America: USA and Canada.
SD: Standard deviation.
Knowledge & definition
Almost all participants from North America stated knowing the term ‘stakeholder engagement’ (96.30%), while it were 65% among participants from DACH and 56% among those from China (Figure 2).

Figure 2. Participant’s knowledge of the term ‘stakeholder engagement’ by country of residence.
DACH: Germany (D), Austria (A) and Switzerland (CH); North America: USA and Canada.
In the course of the survey, we introduced a stakeholder engagement definition (Box 1) [1] for which participants from North America showed the highest agreement, however, without a statistically significant difference between groups (Figure 3).
Stakeholder engagement is the active inclusion and participation of different individuals or groups in a research process. Stakeholders are characterized by holding an interest in or being affected by the conducted research.
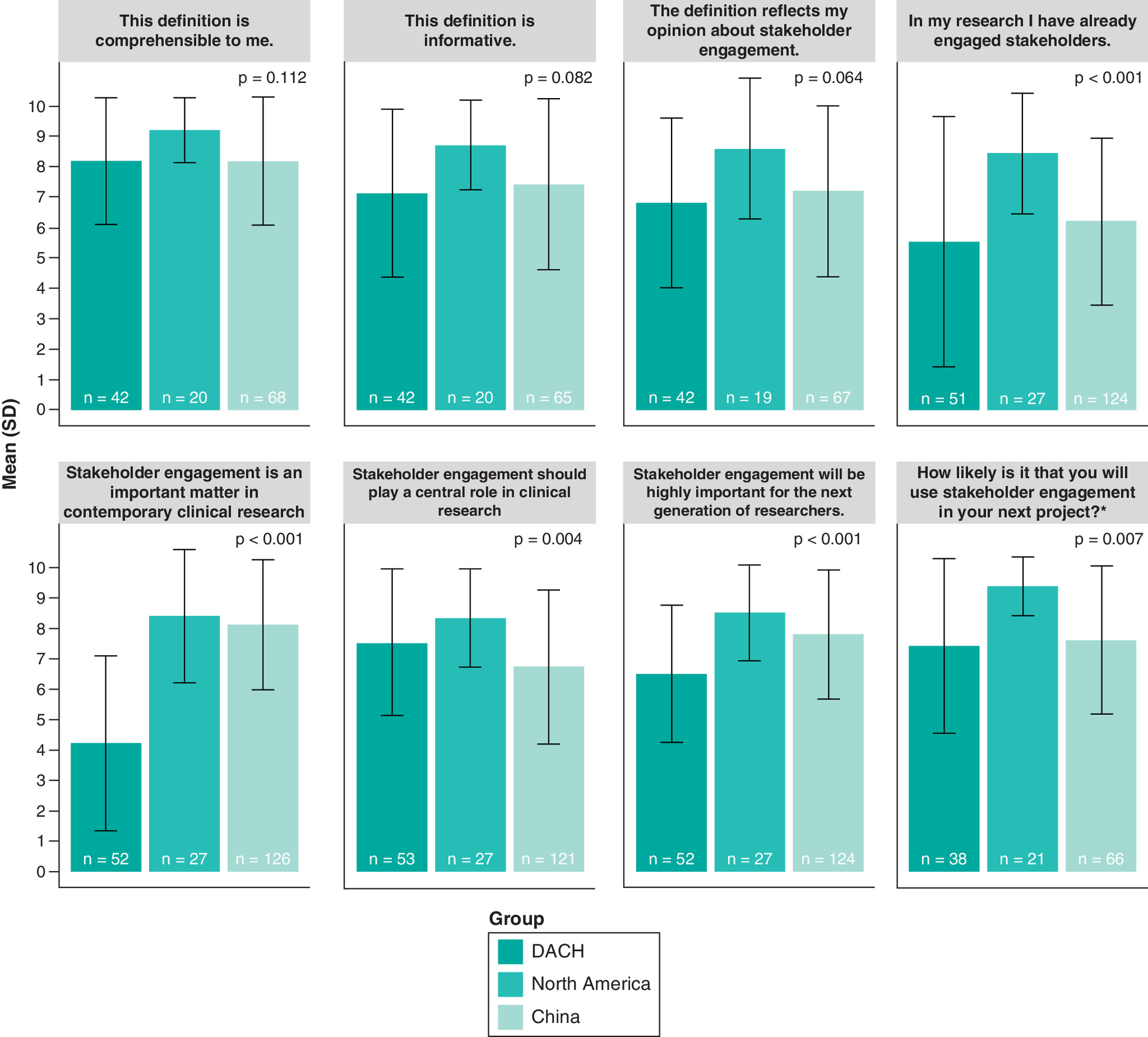
Figure 3. Opinion on stakeholder definition and relevance reported in the survey.
Shown values are the means of the responses by group on a scale from 0 to 10 with 0 = do not agree at all and 10 = agree completely; error bars indicate the standard deviation; p-values are from a one-way ANOVA.
*This item was scaled from 0 to 10 with 0 = very unlikely and 10 = very likely.
DACH: Germany (D), Austria (A) and Switzerland (CH); North America: USA and Canada.
ANOVA: Analysis of variance; SD: Standard deviation.
Relevance & practice
The perception of stakeholder engagement as an important matter in contemporary clinical research varied between the groups, measured on a scale from 0 = do not agree at all to 10 = agree completely (North America: 8.41 ± 2.2, DACH: 4.23 ± 2.9, China: 8.12 ± 2.1; p <.001). When asked if they had already included stakeholders in research, participants from North America showed the highest and from DACH countries the lowest agreement (North America: 8.44 ± 2.0, DACH: 5.53 ± 4.1, China: 6.22 ± 2.7; p < 0.001). Concerning the question if stakeholder engagement should form an important part of future clinical research, participants from North America rated with a mean of 8.33 ± 1.6, from DACH countries with 7.51 ± 2.4 and from China with 6.74 ± 2.5 (p = 0.004).
The likelihood of engaging stakeholders in an upcoming project was rated on a scale from 0 = very unlikely to 10 = very likely with a high mean in North America (9.38 ± 1.0), while participants from DACH countries (7.42 ± 2.9) and China (7.61 ± 2.4) achieved a comparably lower one (p = 0.007).
Perceived challenges & potential contribution of stakeholder engagement
Participants evaluated requirements for successful stakeholder engagement and possible advantages/disadvantages of stakeholder engagement (Table 2). The necessity of ‘stakeholders interest in participation’ was rated with high means across all groups: 9.05 ± 2.2 for North America, 8.76 ± 1.7 for DACH countries and 8.72 ± 1.7 for China (p = 0.754). In contrast, the statement ‘stakeholder engagement leads to additional financial costs’ was rated relatively low, with a mean of 2.74 ± 2.5 for North America, 3.08 ± 3.2 for DACH countries and 3.48 ± 2.8 for China (p = 0.572). Furthermore, the need for a guideline publication to foster stakeholder engagement was rated with a lower mean in DACH countries (5.69 ± 3.2), but a higher one in North America (8.47 ± 1.8) and China (8.95 ± 1.8; p < 0.001). Correspondingly, the need for institutional infrastructure was rated lower in DACH countries (6.55 ± 2.55) than in North America (8.33 ± 1.78) and China (8.72 ± 1.79); p < 0.001). Asked, if funding programs to support researchers adopting stakeholder engagement are necessary, researchers from DACH countries rated with a lower mean (6.74 ± 3.08) than researchers from North America (8.37 ± 2.27) and China (8.74 ± 1.78; p < 0.001). To the potential positive impact of stakeholder engagement on transparency of research institutions, participants agreed in a variable extent, with a lower mean (5.13 ± 2.7) for DACH countries, and higher ones for North America (7.56 ± 1.6) and China (8.42 ± 1.4; p < 0.001). The results for other aspects of stakeholder engagement are given in Table 2.
| Question/group | DACH mean (SD) | North America mean (SD) | China mean (SD) | p-value§ |
|---|---|---|---|---|
| Which of the following factors are necessary to foster stakeholder engagement in research?† | ||||
| Standardized definition of stakeholder engagement | 5.84 (2.91) | 6.26 (2.75) | 9.19 (1.40) | <0.001 |
| Stakeholders interest in participation | 8.73 (1.71) | 9.05 (2.16) | 8.72 (1.71) | 0.754 |
| Publication of guidelines for stakeholder engagement | 5.69 (3.20) | 8.47 (1.78) | 8.95 (1.77) | <0.001 |
| Institutional infrastructure | 6.55 (2.55) | 8.33 (1.78) | 8.72 (1.79) | <0.001 |
| Funding programs to support researchers adopt stakeholder engagement | 6.74 (3.08) | 8.37 (2.27) | 8.74 (1.78) | <0.001 |
| Funding to do research about stakeholder engagement | 6.45 (2.84) | 7.16 (2.57) | 8.55 (1.81) | <0.001 |
| Stakeholder engagement…‡ | ||||
| Leads to additional financial costs | 3.08 (3.18) | 2.74 (2.49) | 3.48 (2.76) | 0.572 |
| Places a high burden on the human resources of a research team | 8.00 (3.24) | 6.42 (2.99) | 5.44 (3.14) | 0.049 |
| Will not lead to widely applicable study results because it only takes individual perspectives into consideration | 3.87 (3.25) | 2.28 (2.24) | 4.29 (3.24) | 0.060 |
| Leads to lobbyism, meaning the organized influence of particular groups on clinical research | 6.33 (2.76) | 5.05 (2.55) | 7.05 (2.91) | 0.026 |
| Implies higher workload for researchers | 7.38 (2.98) | 7.00 (2.91) | 6.46 (2.88) | 0.300 |
| Constitutes a higher workload for potential stakeholders | 7.58 (2.33) | 7.00 (2.52) | 6.28 (2.87) | 0.058 |
| Enables external persons to participate in a research project | 7.36 (2.43) | 8.37 (1.61) | 8.17 (1.90) | 0.100 |
| Integrates individual perspectives of decision makers into the research process, which may lead to more relevant research | 8.05 (2.42) | 8.75 (1.74) | 7.71 (2.29) | 0.200 |
| Includes empirical values/data in the research process | 8.05 (2.70) | 7.11 (1.78) | 7.35 (2.28) | 0.247 |
| Strengthens patients’ rights to participate in healthcare decision-making | 6.42 (3.19) | 7.32 (2.52) | 8.30 (1.85) | 0.001 |
| Increases the relevance of research questions and outcomes | 6.95 (2.80) | 8.05 (2.33) | 8.37 (1.79) | 0.009 |
| Leads to implementable research results | 6.25 (2.71) | 6.95 (2.57) | 8.39 (1.68) | <0.001 |
| Has a positive impact on the transparency of research institutions | 5.13 (2.68) | 7.56 (1.62) | 8.42 (1.43) | <0.001 |
| Strengthens the trust in research results of all persons involved | 7.43 (2.67) | 8.15 (2.28) | 8.31 (1.77) | 0.141 |
| Enhances the adherence of study participants | 6.05 (2.86) | 6.32 (2.69) | 8.23 (1.91) | <0.001 |
| Facilitates recruitment | 4.69 (2.73) | 6.74 (2.96) | 7.72 (2.07) | <0.001 |
†
This item was scaled from 0 to 10 with 0 = not necessary at all and 10 = very necessary.
‡
This item was scaled from 0 to 10 with 0 = do not agree at all and 10 = agree completely.
§
p-value from a one-way ANOVA.
DACH: Germany (D), Austria (A) and Switzerland (CH); North America: USA and Canada.
ANOVA: Analysis of variance; SD: Standard deviation.
Levels & stages of engagement
In the evaluation of the question if stakeholders should be engaged as consulting partners in clinical research, means were consistent and relatively high across all groups (North America: 7.90 ± 2.4, DACH: 8.11 ± 2.6, China: 7.91 ± 2.6; p = 0.924). Concerning a collaborative engagement, analysis showed similar results, but with a slightly lower mean in DACH countries (North America: 8.20 ± 2.1, DACH: 7.05 ± 2.8, China: 8.07 ± 2.5; p = 0.112). When asked if stakeholders should have a leading role in research, participants from DACH countries rated with the lowest mean (4.45 ± 3.3) and participants from China with the highest (6.55 ± 3.2; p = 0.005). Regarding stakeholder engagement in different research stages, from topic selection to publication and implementation of results, participants from DACH countries rated with the lowest means over all items, with an exception of the ‘implementation of results’ (Supplementary Material 2).
Stakeholder groups
Participants were asked which groups of stakeholders should be engaged in future clinical research, namely: patients, clinicians, researchers, payers, industry, hospitals & health systems, policy makers and training institutions. With an exception of the item ‘payers’ (DACH: 6.61 ± 3.1, North America: 5.62 ± 3.2, China: 5.80 ± 3.8, p = 0.379), means in the DACH group were slightly lower over all items ( Supplementary Material 2).
Methods for engagement
The study presented 15 methods to engage stakeholders. Participants rated the frequency of how often they should be used. For all digital/technical methods (e.g., webinar, online-survey), means of the DACH-group remained lower than means of the other two groups (e.g., item ‘webinar’: DACH: 5.07 ± 2.9, North America: 7.11 ± 2.3, China: 8.09 ± 2.6; p < 0.001). In contrast, DACH countries reached the highest mean for the item ‘personal meeting’ (DACH: 7.85 ± 2.4, North America: 7.20 ± 2.3, China: 7.49 ± 2.8; p = 0.631, Supplementary Material 2).
Communication tools
Participants rated how often specific communication tools should be used to engage stakeholders. In all groups means were high for contacting stakeholders via email. Biggest mean differences were found for the items ‘Instant messaging’, ‘Smartphone Application’ and ‘SMS (text message)’, where participants from China rated the highest and from DACH countries the lowest (e.g., item ‘Smartphone Application’ DACH: 4.67 ± 2.6, North America: 5.94 ± 2.7, China: 8.79 ± 2.3; p < 0.001). Compared with the other groups, DACH countries rated also lower for digital tools like ‘Online Blog’, ‘Online Forum’, ‘Social network’, but higher for the direct contact through ‘Personal meeting’ (DACH: 8.80 ± 1.9, North America: 8.11 ± 2.2, China: 7.49 ± 3.1; p = 0.045, Supplementary Material 2).
We conducted an ANCOVA to adjust for the observed age difference between groups. This analysis showed that group differences did not disappear when controlling for the age of participants.
Discussion
The results of this international, cross-sectional study indicate that the researchers in North America are more familiar with the method and definition of stakeholder engagement. In comparison, among the participating researchers from DACH countries stakeholder engagement is not broadly known and not considered as an important method of existing contemporary clinical research. Nevertheless, they regard it as an important method for future clinical research.
A second finding of our study is a group difference in the perception of advantageous effects of stakeholder engagement in clinical research. Participants from DACH countries rated the beneficial effects of stakeholder engagement like increased transparency, patient empowerment, or facilitation of recruitment and implementation, lower when compared with participants from North America and China.
Overall, researchers from the DACH countries use stakeholder engagement less than researchers from the comparison regions. They also indicate less willing to make joint decisions regarding their research. Furthermore, they have lower expectations when it comes to applying technology-based methods for stakeholder engagement than participants from North America and China. Surprisingly, participants across all groups gave low scores for possible high financial cost of the stakeholder engagement process and the overrepresentation of individual stakeholder opinions.
The main strength of this study is its global approach with participants from different world regions. Furthermore, the questionnaire is profound, built on an intensive literature review and hence on previous works and findings [1,11,26–29]. Conceptualization of different sections, extensive discussion and pretesting lead to a well-elaborated survey. We used a modern online survey technique, which is economic, safe, anonymous, user-friendly and allows reaching an international sample without risk of interviewer bias. We aimed to answer a research question that has high relevance for usual care practice and reflects an international setting. Our sample groups showed notable varieties in characteristics. We controlled for the possible confounder age in an ANCOVA and obtained results that were consistent with our primary findings.
Nevertheless, our study has several limitations. The complexity of the survey could have led to frustration and dropout of study participants, reflected in the participation rate of 36.9% and the completion rate of roundly 50%. The overall view rate from links to the survey homepage was <4%. However, these rates are commonly observed in web-based surveys and do not necessarily lead to nonresponse bias [30,31]. More likely, results underly a social desirability bias and nonresponse was caused by the inability to send out personal reminders, due to the anonymity of the study [32]. Additionally, the sample is a convenience sample with volunteer bias, including solely researchers who are member of mailing lists with limited reach [33]. This resulted in a small sample size which limits the representativeness of the data. Future studies should consider using incentives and aim for bigger samples. Low response could also have been affected by noninterest in newsletters content in the first place. We endeavored to address diverse mailing lists, but yet conclusions on the population are only allowed to a limited extent. Furthermore, we were facing the challenge of transferring information between different languages, cultures and systems. First, a certain term or expression may not have the same significance in all languages. Second, addressed health systems, research infrastructures and cultures may vary significantly. Even so, we used the same questionnaire in all target samples, aiming for high comparability.
The grouping of participants intends to recognize possible differences in mindsets by world region, assuming that there exist different research cultures across the world. Nonetheless a categorization by their country of residence does not guarantee relation between world region (or more broadly defined: research culture) and the participants’ opinion. Moreover, a participant residing in China could have been trained in North America, and afterward finding herself applying what she has learned in a Chinese research context. To conclude, in our globalized world clear relationship between place of residence and stakeholder practice is not necessarily given, but could result out of different framework conditions and research cultures. It would also be of great interest to consider the influence of the researcher’s particular field of research, as existing experiences and practices differ across research fields. Data on these were not collected in our survey and should be part of future research.
Consistent with previous work, this study points out that researchers are not assigning a leading role to stakeholders, but prefer a consulting or collaborating level of engagement [14]. Our findings show that especially researchers in DACH countries favor to engage patients, clinicians and researchers, although other actors like payers, policy makers and training institutions are also promoted by the stakeholder approach [11].
Conclusion
Clinical researchers in North America are more familiar with the method and definition of stakeholder engagement and regard institutional infrastructure and funding essential to foster stakeholder engagement in clinical research. In comparison, stakeholder engagement is not broadly known among researchers from DACH countries and not considered as an important method of existing contemporary clinical research but of future research. The reasons for lack of implementation of stakeholder engagement remain unclear.
Future perspective
For a broader acceptance and implementation of stakeholder engagement in clinical researches, institutional support and motivational conditions might be needed.
More data are needed to find out what prevents researchers in DACH countries from implementing stakeholder engagement. As a first step, information and training on stakeholder engagement should be provided to inform researchers about the concept.
•
Stakeholder engagement is defined as the active inclusion and participation of different individuals or groups in a research process. Stakeholders are characterized by holding an interest in or being affected by the conducted research.
•
Infrastructure for stakeholder engagement and its evaluation is continuously growing in North America and the UK. However, very little attention has been paid to understand practices in DACH countries (country codes for Germany, Austria and Switzerland) and China in a worldwide scope.
•
This well-elaborated survey was built based on intensive literature review and pretesting, and ensured feasible access with three different languages (English, German and Chinese).
•
The sample was a convenience sample based on researcher newsletters and mailing lists; the resulted small sample size might limit the representativeness of the data; participants may yield substantial volunteer bias.
•
Almost all participants from North America stated knowing the term “stakeholder engagement” (96.30%), while it was 65% among participants from DACH and 56% among those from China.
•
For researchers from DACH countries, stakeholder engagement is not broadly known and not considered as an important method of existing contemporary clinical research. However, they regard it important for future clinical research.
•
Results should be carefully interpreted, as health systems, research infrastructures, term expressions and cultures may vary significantly.
•
Our study results suggested that, for a broader acceptance and implementation of stakeholder engagement in clinical studies, institutional support and motivational conditions might be needed.
Author contributions
A Heiß, CM Witt and D Pach conceived and designed the study. A Heiß, J Wang and Y Fei performed the study. A Heiß, K Icke, CM Witt and D Pach analyzed and discussed the data. A Heiß and D Pach wrote the first draft of the paper. All authors revised the paper and approved the final.
Acknowledgments
The authors thanked I Bartsch for data management support, S Roll for statistical advice during the planning of the study, B Eden for support of the team and all researchers for their participation in this study. Special credits go to all developers of R and R packages, as well as to D Beiter and E Steirou for personal and statistical support.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The study received approval from the Charité – Universitätsmedizin Berlin Ethic Committee on 3 May 2016 (Approval Number EA1/128/16) and data protection committee on 15 June 2016 (AZ 293/16).
All participants were informed about the objectives of the study and could provide their informed consent by initiating the online survey.
Data sharing statement
The anonymized survey datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest
1.
Concannon TW, Meissner P, Grunbaum JA et al. A new taxonomy for stakeholder engagement in patient-centered outcomes research. J. Gen. Intern. Med. 27(8), 985–991 (2012).
• Reports the definition, practices and implementations of stakeholder engagement.
2.
Kim KK, Khodyakov D, Marie K et al. A novel stakeholder engagement approach for patient-centered outcomes research. Med. Care 10(Suppl. 1), S41–S47 (2018).
3.
Lavallee DC, Wicks P, Alfonso Cristancho R, Mullins CD. Stakeholder engagement in patient-centered outcomes research: high-touch or high-tech? Expert Rev. Pharmacoecon. Outcomes Res. 14(3), 335–344 (2014).
4.
Esmail L, Moore E, Rein A. Evaluating patient and stakeholder engagement in research: moving from theory to practice. J. Comp. Eff. Res. 4(2), 133–145 (2015).
• Reports the definition, practices and implementations of stakeholder engagement.
5.
Van Der Scheer L, Garcia E, Van Der Laan AL, Van Der Burg S, Boenink M. The benefits of patient involvement for translational research. Health Care Anal. 25(3), 225–241 (2017).
6.
Goodman MS, Sanders Thompson VL. The science of stakeholder engagement in research: classification, implementation, and evaluation. Transl. Behav. Med. 7(3), 486–491 (2017).
• Reports the definition, practices and implementations of stakeholder engagement.
7.
Hansen SL, Holetzek T, Heyder C, Wiesemann C. Stakeholder-Beteiligung in der klinischen Forschung: eine ethische analyse. Ethik in der Medizin.30(4), 289–305 (2018).
8.
Freeman RE. Strategic Management: A Stakeholder Approach. Cambridge University Press, MA, USA (1984).
9.
PCORI. Patient-centered outcomes research institute: about us (2014). www.pcori.org/about-us/our-story
10.
PCORI. Patient-centered outcomes research institute: funding opportunities (2012). www.pcori.org/funding-opportunities/research-support-funding-opportunities
11.
Forsythe LP, Ellis LE, Edmundson L et al. Patient and stakeholder engagement in the PCORI pilot projects: description and lessons learned. J. Gen. Intern. Med. 31(1), 13–21 (2016).
12.
Selby JV, Forsythe L, Sox HC. Stakeholder-driven comparative effectiveness research: an update from PCORI. JAMA 314(21), 2235–2236 (2015).
• Reports the definition, practices and implementations of stakeholder engagement.
13.
Woolf SH, Zimmerman E, Haley A, Krist AH. Authentic engagement of patients and communities can transform research, practice, and policy. Health Affairs 35(4), 590–594 (2016).
14.
Concannon TW, Fuster M, Saunders T et al. A systematic review of stakeholder engagement in comparative effectiveness and patient-centered outcomes research. J. Gen. Intern. Med. 29(12), 1692–1701 (2014).
• Reports the definition, practices and implementations of stakeholder engagement.
15.
Lavery JV. Building an evidence base for stakeholder engagement. Science 361(6402), 554 (2018).
16.
Jackson T, Pinnock H, Liew SM et al. Patient and public involvement in research: from tokenistic box ticking to valued team members. BMC Med. 18(1), 79 (2020).
17.
National Institute for Health Research. NIHR: about INVOLVE (2021). www.invo.org.uk/about-involve/
18.
National Institute for Health and Care Excellence. Developing NICE guidelines: a guide for stakeholders and the public (2014). www.nice.org.uk/Media/Default/About/what-we-do/our-programmes/developing-NICE-guidelines-information-for-stakeholders.pdf
19.
Brereton L, Ingleton C, Gardiner C et al. Lay and professional stakeholder involvement in scoping palliative care issues: methods used in seven European countries. Palliat. Med. 31(2), 181–192 (2017).
20.
Liu C, Meyers K. Beyond clinical trials: social outcomes of structured stakeholder engagement in biomedical HIV prevention trials in China. Cult. Health Sex 1–17 (2019).
21.
Wratil P, Helbing G, Wiens O. Research report I. Results of the legacy study - a first overview (2017). https://bibliothek.wzb.eu/pdf/2017/p17-006.pdf
22.
Leiner DJ. SoSci Survey. Informationen über SoSci survey (2016). www.soscisurvey.de/de/about
23.
Leiner DJ. SoSci survey (2016). www.soscisurvey.de
24.
Rstudio Team. RStudio: integrated development environment for R (Version 1.1.419). MA, USA (2018). www.rstudio.com/
25.
R Core Team. R: a language and environment for statistical computing (2017). R Foundation for Statistical Computing, Vienna, Austria. www.R-project.org/
26.
Deverka PA, Lavallee DC, Desai PJ et al. Stakeholder participation in comparative effectiveness research: defining a framework for effective engagement. J. Comp. Eff. Res. 1(2), 181–194 (2012).
27.
Mallery C, Ganachair D, Fernandez J, Smeeding L, Robinson S, Moon M. Innovative methods in stakeholder engagement: an environmental scan. AHRQ Publication NO. 12-EHC097-EF (2012). https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/stakeholders-engagement-others_research-2012-1.pdf
28.
Guise JM, O'Haire C, McPheeters M et al. A practice-based tool for engaging stakeholders in future research: a synthesis of current practices. J. Clin. Epidemiol. 66(6), 666–674 (2013).
• Reports the definition, practices and implementations of stakeholder engagement.
29.
Thariani R, Wong W, Carlson JJ et al. Prioritization in comparative effectiveness research: the CANCERGEN experience. Med. Care 50(5), 388–393 (2012).
30.
Sebo P, Maisonneuve H, Cerutti B, Fournier JP, Senn N, Haller DM. Rates, delays, and completeness of general practitioners' responses to a postal versus web-based survey: a randomized trial. J. Med. Internet Res. 19(3), e83–e83 (2017).
31.
Af Wåhlberg AE, Poom L. An empirical test of nonresponse bias in internet surveys. Basic Appl. Social Psychol. 37(6), 336–347 (2015).
32.
Cook DA, Wittich CM, Daniels WL, West CP, Harris AM, Beebe TJ. Incentive and reminder strategies to improve response rate for internet-based physician surveys: a randomized experiment. J. Med. Internet Res. 18(9), e244 (2016).
33.
Eysenbach G, Wyatt J. Using the internet for surveys and health research. J. Med. Internet Res. 4(2), e13 (2002).
Information & Authors
Information
Published In
Pages: 751 - 761
PubMed: 33955232
Copyright
© 2021 Heiß et al. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 10 December 2020
Accepted: 26 March 2021
Published online: 6 May 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Current practice of stakeholder engagement: researchers’ experiences in North America, DACH countries and China. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0279
Export citation
Select the citation format you wish to export for this article or chapter.