Robotic-assisted total hip arthroplasty: an economic analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate 90-day episode-of-care (EOC) resource consumption in robotic-assisted total hip arthroplasty (RATHA) versus manual total hip arthroplasty (mTHA). Methods: THA procedures were identified in Medicare 100% data. After propensity score matching 1:5, 938 RATHA and 4,670 mTHA cases were included. 90-day EOC cost, index costs, length of stay and post-index rehabilitation utilization were assessed. Results: RATHA patients were significantly less likely to have post-index inpatient rehabilitation or skilled nursing facility admissions and used fewer home health agency visits, compared with mTHA patients. Total 90-day EOC costs for RATHA patients were found to be US$785 less than those of mTHA patients (p = 0.0095). Conclusion: RATHA was associated with an overall lower 90-day EOC cost when compared with mTHA. The savings associated with RATHA were driven by reduced utilization and cost of post-index rehabilitation services.
Musculoskeletal conditions represent a major burden on the US health system [1]. In the USA, the prevalence and impact of musculoskeletal conditions is likely to increase over time as the population ages [2]. Among the various conditions, osteoarthritis is the most common type. Aggregate annual direct costs for adults with arthritis and joint pain in the years 2012–2014 were reported at US$88.2 billion. While osteoarthritis can affect any joint in the body, it is most frequently associated with the hip and knee [3].
Total hip arthroplasty (THA) has been shown to deliver meaningful improvements in reducing pain, improving function and restoring quality of life for many patients suffering from end-stage osteoarthritis [4]. THA has also demonstrated cost–effectiveness; however, the volume of procedures still results in significant overall costs to the healthcare system [5,6]. Recent data suggest that over 400,000 total hip replacements are performed annually in the USA [7], leading to an estimated US$30.7 billion in hospital charges [3]. Increase in the economic burden has led payers, both public and private, to explore payment models outside of fee-for-service payments. Bundled payment for a period of time that includes surgery and post-operative care, often for 90 days, has been one such method employed, with a goal to help lower the cost and improve the quality of care. Given the evidence suggesting the number of THA procedures is growing and the projected number of patients in need will continue to rise [3], it is important to document whether innovative treatments are cost-effective and enhance important outcomes.
Robotic technology has been utilized in arthroplasty surgery for over 20 years [8–11]. In its early stages, robotic interventions in arthroplasty were first utilized in THA [9,10,12] but showed mixed results in improving outcomes. Haptic-guided robotic technology was introduced in partial knee arthroplasty around 2008 and has changed the landscape [13–15]. Several papers have shown decreased rates of complications and increased accuracy in component placement with this system [16–18]. Haptic-guided robotic arm-assisted total hip replacement technology combines advanced imaging techniques with a robotic arm. This allows the surgeon to plan the procedure in three dimensions and execute the surgical procedure with the help of a digitally defined haptic boundary. This methodology, combined with the ability to change the plan and execution in real time, provides a unique tool for the performance of total hip replacement [19]. The use of this haptic technology in robotic-assisted total hip arthroplasty (RATHA) has been shown in several centers to reduce variance in the placement of implants, reduce incidence of leg length discrepancy, better recreate the patient’s biomechanics, reduce complications and improve outcomes compared to manual surgery [20–23].
The use of robotic technology, with its ability to help surgeons achieve desired component positions, has the potential to enhance the outcomes of THA [20–23]. This may also have an impact on costs. Analyses of the use of this technology in total knee arthroplasty have shown savings in the 90-day episode-of-care (EOC) cost [24,25]; however, few studies have examined whether this trend extends to THA. Thus the objective of this study is to assess and compare resource consumption in RATHA versus manual THA (mTHA) in a 90-day EOC among Medicare patients.
Patients & methods
Study design & data sources
This analysis evaluated the post-index 90-day EOC costs to Medicare, and utilization for Medicare patients undergoing THA. Costs in this analysis represent payments made by the Center for Medicare and Medicaid Services (CMS). Data originated from the Medicare 100% Standard Analytical Files were compiled by CMS and represent medical services provided to nearly 37 million Medicare Fee-for-Service (FFS) beneficiaries. This retrospective claims analysis provides longitudinal assessments of Medicare FFS beneficiaries who underwent THA between 1 October 2015 and 1 October 2018 (referred to as the index period) and includes the following post-index services: acute inpatient, inpatient rehab, outpatient, emergency room, skilled nursing facility (SNF) and home health agency (HHA).
Study population selection
Medicare beneficiaries who received a primary THA (referred to as the index procedure) were considered for inclusion into the study. Cases were identified by the presence of International Classification of Diseases, Tenth Version (ICD-10) billing codes (Supplementary Table 1), in addition to a diagnosis-related group (DRG) assignment of 469 or 470.
Following the identification of THA claims, two study cohorts were created: RATHA and mTHA. RATHA cases met the following criteria: a preoperative CT scan (Supplementary Table 1) that occurred within 60 days prior to the RATHA procedure, and an ICD-10 code indicative of a robotic-arm assisted procedure. The mTHA cohort included the absence of a CT scan in the preoperative period and the absence of the ICD-10 robotic-arm assisted procedure code.
Claims were excluded from the analysis if they met any of the following criteria:
•
Payments associated with the index procedure that were considered erroneous (claims missing payment information).
•
Patient had a bilateral procedure within 90 days of the index procedure (pre or post), identified by the assignment of a DRG indicating major joint replacement or reattachment of lower extremity with major complications or comorbidities (DRG 469) or without major complications or comorbidities (DRG 470).
•
Patient experienced in-hospital mortality during the study period.
Figure 1 is a flow chart illustrating the retention process for our sample population. The analysis included 945 RATHAs and 393,447 mTHAs for propensity score matching (PSM).
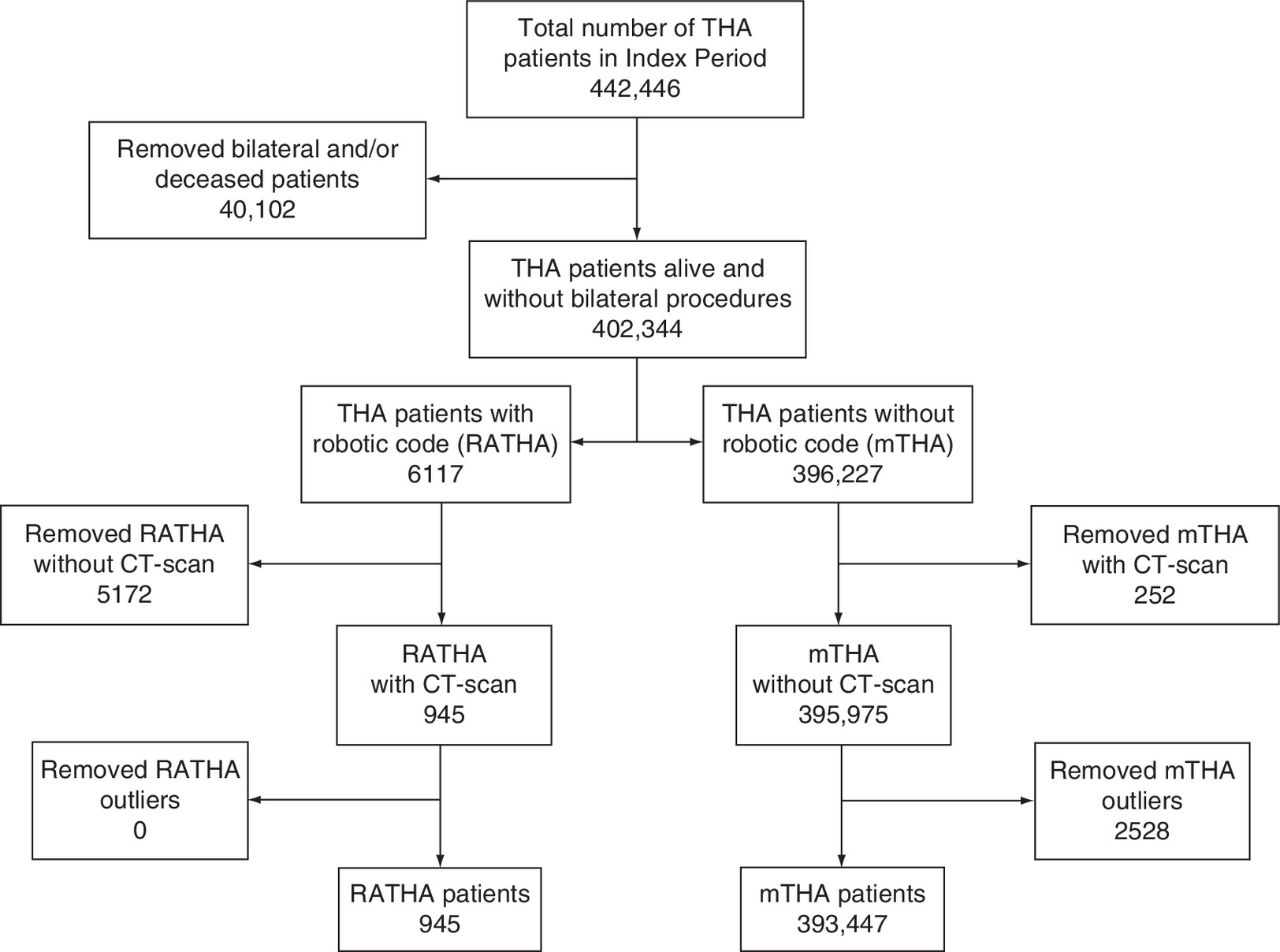
Figure 1. Flow chart of inclusion criteria for sample selection.
mTHA: Manual total hip arthroplasty; RATHA: Robotic-assisted total hip arthroplasty; THA: Total hip arthroplasty.
Propensity score matching
PSM was used to account for index difference, a 1:5 ratio of RATHA patients to mTHA patients, based on the following criteria: age, sex, race (as defined by CMS), geographical division (based on US Census Bureau divisions), academic center designation, physician experience (identified by the volume of procedures performed during the study timeframe) and high-cost comorbidities (chronic obstructive pulmonary disease, hypertension, diabetes, coronary artery disease, smoking, pneumonia, cancer or obesity) [26–29]. After PSM, 942 RATHA and 4710 mTHA cases were identified. Post-matching, patients not flagged by the exclusion criteria were removed from the analysis. Following the removal, the cohorts remained well balanced on the matching criteria (all p-values > 0.05). In all, 938 RATHA and 4670 mTHA were included for analysis.
90-day EOC costs
The overall 90-day EOC costs, including the index procedures and lengths of stay (LOS), were calculated. EOC costs to Medicare were identified through the presence of claims billed in an inpatient, outpatient, emergency room, SNF or HHA setting. For patients who experienced an in-hospital readmission during the 90-day period immediately following their index procedure (known as the 90-day post-index period), readmission rates and inpatient costs were evaluated. LOS was collected at index as well as in the 90-day post-index period for SNF and inpatient settings.
Statistical analysis
A generalized linear model was selected to test for statistical significance due to the data not being normally distributed. We ran statistical comparisons via a two-part model. Binomial regressions were used in the first part of the model to test cohort differences in the probability of having costs in the 90-day post-index period. The second part of the model ran a γ distribution to analyze cohort differences in cost among members with costs in the 90-day post-index period. For analyses of post-index number of readmissions, we used negative binomial distributions if the variance of the outcome exceeded the mean; otherwise, a Poisson distribution was utilized. Differences among dichotomous and categorical variables were analyzed using Pearson’s χ2 test and those among continuous variables were analyzed using the Mann–Whitney U test. These analyses were performed using SAS Enterprise Guide 7.1 software (SAS Institute, Inc., NC, USA).
Multiple imputation
Because patients may seek post-index outpatient procedures not captured within the Medicare FFS databases – for example, at ambulatory care centers or imaging/radiology centers – we ran multiple imputation modeling to replace missing post-index outpatient visits and cost data. A robust method to impute missing values while minimizing bias in the resulting values, multiple imputation borrows data from randomly selected, non-missing patients that match most closely to the profile of a patient with missing data, and uses the borrowed data to fill in the latter patient’s missing values in many iterations. These iterations are then analyzed and their results pooled.
Results
Population demographics
No statistical differences were observed between the two cohorts in age, gender, race, geographical location, physician experience or high-cost comorbidities. However, both cohorts had similarly high rates of Caucasians (according to CMS classification; 91% RATHA vs 89% mTHA), as well as similar rates of members from the New England (31% RATHA vs 30% mTHA) and West South Central (22% RATHA vs 21% mTHA) regions. Both cohorts had a high proportion of people with high-cost comorbidities (62% RATHA vs 64% mTHA). Table 1 highlights the demographic and comorbidity profiles of the matched study cohorts.
| Demographics | RATHA (n = 938) | mTHA (n = 4670) | p-value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age group | |||||
| – 2 | 314 | 33.48 | 1662 | 35.59 | 0.1455 |
| – 3 | 270 | 28.78 | 1352 | 28.95 | |
| – 4 | 195 | 20.79 | 1013 | 21.69 | |
| – 5 | 103 | 10.98 | 417 | 8.93 | |
| – 6 | 56 | 5.97 | 226 | 4.84 | |
| Male | 367 | 39.13 | 1963 | 42.03 | 0.0991 |
| Caucasian | 853 | 90.94 | 4169 | 89.27 | 0.1279 |
| Geographical division | |||||
| – East North Central | 187 | 19.94 | 966 | 20.69 | 0.9645 |
| – East South Central | 33 | 3.52 | 147 | 3.15 | |
| – Mid-Atlantic | 26 | 2.77 | 143 | 3.06 | |
| – Mountain | 48 | 5.12 | 244 | 5.22 | |
| – New England | 288 | 30.70 | 1422 | 30.45 | |
| – Pacific | 17 | 1.81 | 78 | 1.67 | |
| – South Atlantic | 74 | 7.89 | 340 | 7.28 | |
| – West North Central | 61 | 6.50 | 348 | 7.45 | |
| – West South Central | 204 | 21.75 | 982 | 21.03 | |
| Number of high-cost comorbidities | |||||
| – 0 | 352 | 37.53 | 1699 | 36.38 | 0.3279 |
| – 1 | 227 | 24.20 | 1064 | 22.78 | |
| – 2+ | 359 | 38.27 | 1907 | 40.84 | |
mTHA: Manual total hip arthroplasty; RATHA: Robotic-assisted total hip arthroplasty.
EOC costs
Total 90-day EOC costs for RATHA patients were found to be US$785 (3.8%) less than those for mTHA patients (US$19,734 vs US$20,519; p = 0.0095). In addition, the average index LOS for RATHA patients was 8% less than that of mTHA patients (2.3 vs 2.5 days; p = 0.0137; Table 2).
| RATHA | mTHA | Mean difference | % difference | p-value | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| Index LOS | 2.29 | 1.11 | 2.49 | 1.53 | -0.20 | -8.0% | 0.0137* |
| Index costs | US$12,827 | US$4174 | US$12,665 | US$3353 | US$173 | 1.3% | 0.0487* |
| Total episode costs | US$19,734 | US$11,221 | US$20,519 | US$12,798 | -US$785 | -3.8% | 0.0095* |
*p < 0.05.
LOS: Length of stay; mTHA: Manual total hip arthroplasty; RATHA: Robotic-assisted total hip arthroplasty; SD: Standard deviation.
Index facility costs
Overall index facility costs to the payer for RATHA patients were found to be higher than those for mTHA patients (US$12,827 vs US$12,665; p = 0.0487). These amounts for RATHA patients demonstrate a 1.3% (US$162) higher cost associated with their index facility costs (Table 2).
Post-acute services
Differences in post-acute utilization were most notable in the inpatient rehab, SNF and HHA settings. RATHA patients were 76.1% less likely to have an inpatient rehab post-index admission and 16.8% less likely to have a SNF post-index stay (p < 0.0001 and p = 0.0041, respectively). For post-index HHA services, RATHA patients were 12.4% more likely to have HHA (72.9 vs 64.9%; p < 0.0001; Table 3).
| RATHA (n = 938) | mTHA (n = 4670) | Difference | % difference | p-value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||
| Acute inpatient | 59 | 6.3 | 369 | 7.9 | -1.6% | -20.4 | 0.1261 |
| Inpatient rehab | <11 | <11 | 125 | 2.7 | <11 | <11 | <0.0001* |
| Outpatient | 938 | 100 | 4670 | 100 | 0.0% | 0.0 | >0.9999 |
| ER | 128 | 13.6 | 631 | 13.5 | 0.1% | 1.0 | 0.8373 |
| SNF | 195 | 20.8 | 1167 | 25.0 | -4.2% | -16.8 | 0.0041** |
| HHA | 684 | 72.9 | 3029 | 64.9 | 8.1% | 12.4 | <0.0001* |
| Any post-index services | 938 | 100 | 4670 | 100 | 0% | 0 | >0.9999 |
*p < 0.0001; **p < 0.05.
ER: Emergency room; HHA: Home health agency; mTHA: Manual total hip arthroplasty; RATHA: Robotic-assisted total hip arthroplasty; SNF: Skilled nursing facility.
RATHA patients had a 12.1% (US$948) lower average cost than mTHA patients (p = 0.0004) during the post-index 90-day EOC. Among members utilizing post-acute services, RATHA patients had 21.7% (or US$3184) lower inpatient rehab costs than mTHA patients (US$11,490 vs US$14,674; p = 0.0470; Table 4). Although the difference was not statistically significant, RATHA patients utilized fewer days in inpatient and SNF care (7.2 vs 7.9; p = 0.8029 and 18.0 vs 19.6; p = 0.5080, respectively). Of patients using HHA services, RATHA patients utilized 6% fewer HHA visits compared with mTHA patients (14.1 vs 15.0; p = 0.0006).
| RATHA | mTHA | Difference | % difference | p-value | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| Acute inpatient | US$19,132 | US$14,266 | US$17,413 | US$15,232 | US$1718 | 9.9 | 0.2820 |
| Inpatient rehab | US$11,490 | US$8659 | US$14,674 | US$7183 | -US$3184 | -21.7 | 0.0470* |
| Outpatient | US$1179 | US$2006 | US$1111 | US$1520 | US$68 | 6.1 | 0.1473 |
| ER | US$715 | US$837 | US$786 | US$846 | -US$71 | -9.1 | 0.8201 |
| SNF | US$9184 | US$6820 | US$10,408 | US$10,159 | -US$1224 | -11.8 | 0.0598 |
| HHA | US$3352 | US$2325 | US$3496 | US$1891 | -US$144 | -4.1 | 0.0133* |
| All post-index costs | US$6907 | US$9710 | US$7854 | US$11,732 | -US$948 | -12.1 | 0.0004** |
*p < 0.05; **p < 0.001.
ER: Emergency room; HHA: Home health agency; mTHA: Manual total hip arthroplasty; RATHA: Robotic-assisted total hip arthroplasty; SD: Standard deviation; SNF: Skilled nursing facility.
The aforementioned reduction in utilization among patients using HHA care resulted in significantly decreased costs for the RATHA cohort (US$3352 vs US$3496; p = 0.0133). The HHA setting results for costs and number of visits run counter to the significantly higher proportion of RATHA patients utilizing HHA care (72.9 vs 64.9%; p < 0.0001), indicating higher costs in the mTHA cohort that may be due to a higher amount of post-index visits per patient.
Discussion
Our PSM allowed us to identify 938 cases treated with robotic technology and compare them with 4670 treated manually, all within the Medicare population. The resulting groups were statistically equivalent in terms of age, race, geographical location of the patients and comorbid conditions (Table 1).
In the mTHA group, the surgery was performed utilizing conventional x-rays to plan the procedure and standard instrumentation to perform the procedure. This included mechanical targeting devices and a manual oscillating saw and reamer, where the reaming process includes multiple stages before the final sized reamer is used. Surgery for the robotic-assisted group was performed utilizing CT scanning to plan the surgery in three dimensions and the surgeon executing the surgical procedure with a haptically guided robotic arm that kept the surgeon within a defined boundary when performing the surgery. Utilizing the robotic technology also allowed them to modify placement of the implants in real time. This technology, which uses a single-ream process, has been associated with more accurate and reproducible positioning of the acetabular component to plan and more accurate restoration of the center of rotation of the hip as well as vertical and horizontal offsets. In addition, the technology allows the surgeon to see in real time the change in leg length with the trial components in place. This process allows the modification of the biomechanical variables with the trial components until the surgeon's preoperative plan is satisfied and before the surgeon places the actual implants.
Our data showed that RATHA patients were discharged home sooner and utilized acute inpatient rehabilitation less often than mTHA patients (Table 3). This is in agreement with the data on total knee replacement reported by Cool et al. [24] in the Medicare population as well as the data reported by Pierce et al. in a commercial cohort [25]. The Pierce et al. cohort was selected from a commercial database and included younger patients. In our population, the index procedure LOS in RATHA cases was 0.25 days lower in the robotic cases when compared with the manual cases (Table 2); this difference was statistically significant. The average index payment was US$173 higher for the RATHA group; however, when looking at the overall 90-day EOC, the costs were lower for RATHA when compared with mTHA.
This decrease in length of stay observed with haptic-guided robotic technology has been noted in several papers [24,25]. There may be several reasons for this finding. Previous studies have reported decreased soft tissue damage associated with robotic arm-assisted total knee arthroplasty and have observed that less exposure is needed for robotic arm-assisted cases to achieve desired placement of implants, compared with manual techniques [16]. The RATHA technique uses single-stage reaming, which reduces the number of times the instruments pass through the soft tissues. It has also demonstrated more accurate placement of the acetabular cup, improved restoration of the head center of rotation and improved native bone preservation, as well as enhanced outcomes such as reduced blood loss and higher Harris Hip Scores [20,21,23,30,31]. A supratentorial effect could also be present when patients are receiving procedures with advanced technology.
We were unable to identify any statistically significant difference between the groups in dislocation, infection and revision cases. In general, the prevalence of these problems is very low in total hip cases. Overall, as expected, the volumes of these complications were quite low in both groups during the 90-day follow-up in this population. At longer-term follow-up, differences in dislocation rates between mTHAs and RATHAs have been observed. Illgen et al. compared three groups of THAs: the first 100 mTHAs in practice, the last 100 mTHAs in practice and the first 100 RATHAs in practice. At 2 years of follow-up, they found statistically significant reduction in dislocation between the first 100 mTHAs and the first 100 RATHAs (5 vs 0%; p < 0.05) [20].
After discharge, RATHA patients in our analysis were less likely to go to an acute inpatient rehabilitation facility or SNF when compared with the mTHA cohort. Both of these parameters were statistically significant. The average length of stay in a SNF following a RATHA in this population was 3.74 days, while the average stay in a SNF for the mTHA group was 4.91 days (p < 0.005). The average post-index stay in an inpatient facility was 0.5 days for a RATHA, while the average length of stay for a mTHA patient in an inpatient rehabilitation facility was 0.82 days (p < 0.0015). Two potential factors contributing to lower utilization of services after discharge could be the supratentorial effect and the potential for more accurate reproduction of the biomechanics of the reconstructed hip in RATHA cases. RATHA has been shown to more accurately reproduce a patient’s center of hip rotation and native combined offset when compared with mTHA [21]. Proper biomechanical reconstruction of the hip has been shown to have a significant impact on clinical outcomes, including increased hip abductor strength and improved function [32,33]. The use of robotic arm assistance is designed to allow the surgeon to accurately place the implants with less exposure. The haptic boundaries defined by the robotic system are independent of the visualization of anatomical landmarks usually required to guide the surgeon’s placement of the implants. In addition, more accurate restoration of the hip mechanics, including the vertical and horizontal offset as well as leg length, may result in a ‘more normal hip’ and therefore faster recovery [23]. Clinical studies of RATHA have reported significant improvement in outcomes such as higher Harris Hip Scores, Forgotten Joint Scores and SF-12 scores out to 5 years post-operatively [22,23].
Overall, RATHA patients in this study had lower resource consumption in the 90-day EOC when compared with mTHA patients. This was mostly due to reduced post-discharge resource utilization and an early discharge for RATHA patients. The total expenses associated with post-discharge rehabilitation were nearly US$1000 less using robotic arm-assisted technology compared with manual procedures (Table 4). Allowable reimbursement for the index procedures in the Medicare population is standard and the same for all cases, regardless of the use of robotic assistance. The post-discharge expenses are reimbursed based on a FFS system. Early discharge from a SNF produced over US$1000 of average case savings. With over 20% of the total hip replacement patients in this analysis going to a SNF, the use of robotic technology has the potential to impact the total expenditures in the 90-day EOC.
Total joint arthroplasty has been a target of bundled payments for some time. Bundled payment programs started with the Ace projects in the early 1990s and have evolved into national Medicare and commercial pilot projects that involve many healthcare markets in the USA [34–38]. With these programs, a single payment is made for an arthroplasty that includes all expenses in a period of 90 days (the EOC). Publications evaluating bundled costs have shown that post-discharge rehabilitation makes up a substantial portion of costs in the episode [1].
Our results are in agreement with several papers that have shown that the costs of an EOC for a primary arthroplasty are significantly less when the robotic arm assistance is used [24,25]. This may represent an opportunity for cost savings not only by payers, but also by providers participating in bundled payments that have invested in implementing a robotic technology program. While this data is based on US costs, the global burden of osteoarthritis continues to increase. It is possible that other healthcare systems may have the potential to see savings with the use of robotic assistance in hip replacement surgery in areas where the surgery is performed.
Our study has significant limitations which have been delineated in the past by Cool et al., who used similar methodology for their paper [24]. In a large administrative claims database study, it can be difficult to precisely identify the population of interest as well as their clinical progressions. Clinical factors such as case complexity, type and duration of anesthesia, the anticoagulation prescribed and other risk factors were not assessed. We performed PSM in order to account for age, sex, race, geographical region, high-cost comorbidities and teaching institution status in order to temper potential bias in the data. Although our cost analysis did not include the capital expenditures and the maintenance cost of robotic technology in the hospital, our objective was to analyze the economic impact of the use of the robotic system to the payer of the procedure and therefore did not account for these costs. Despite these limitations, as a large, propensity matched analysis of cost and health resource utilization of RATHA versus mTHA over a 90-EOC, this study makes an important contribution to the evidence on the potential value of robotic assistance in total joint arthroplasty.
Conclusion
These study results demonstrate that RATHA was associated with an overall lower 90-day episode-of-care cost when compared to mTHA. Savings observed in the RATHA cohort were driven by reduced utilization and cost of post-index rehabilitation services. Overall, the current analysis further supports that robotic assistance in total joint arthroplasty can provide value over the EOC. This is of importance as avenues are explored by payers and providers to offer value in addition to enhanced outcomes. Future studies should continue to evaluate these topics with this technology.
Future perspective
The IEEE Robotics and Automation Society states that surgical robotic systems in the next 25 years promises to be comparable to that of manufacturing robots on industrial production over the past 25 years. Robotic-arm assisted technology that incorporates three dimensional planning and haptics has demonstrated the potential for cost reduction, enhanced patient outcomes, and more efficient healthcare resource utilization. As the population ages and thus the prevalence of patients with osteoarthritis increases, innovative health care solutions continue to be sought to address the challenges patients face. We can expect that the healthcare field will continue to pursue avenues to enhance outcomes while delivering value.
•
The prevalence of hip osteoarthritis has been on the rise, leading to a growing demand and volume for total hip arthroplasty (THA), the gold standard procedure for end-stage hip osteoarthritis.
•
As a result, the overall costs associated with THA contribute to substantial financial burdens on payers.
•
Robotic arm-assisted THA (RATHA), a technological advancement, has been introduced as an alternative to manual THA (mTHA) to help enhance clinical, radiographic and patient-reported outcomes.
•
Clinical evidence for RATHA compared with mTHA has demonstrated accuracy, precision to plan and assistance in restoration of biomechanics, which can largely be attributed to the enhanced preoperative planning and haptic guidance employed during RATHA procedures.
•
THA has already been shown to be cost-effective for patients, but the potential value added by the use of a RATHA device has yet to be determined.
•
This economic analysis showed that the use of RATHA yielded statistically significantly lower costs in the overall 90-day episode-of-care period.
•
Post-acute savings for RATHA were driven by RATHA patients experiencing reduced utilization and cost of post-index rehabilitation services including inpatient rehabilitation, skilled nursing facilities and home health agencies.
•
RATHA patients utilized fewer post-index services overall than mTHA patients, ultimately reducing the costs for the RATHA patients in the 90-day episode.
•
The study results presented herein can assist managed care decision-makers to identify potential for cost savings in the management of patients who need to undergo THA.
Financial & competing interests disclosure
This study was sponsored by Stryker. A Coppolecchia is an employee of Stryker and owns stock in Stryker. C Lavernia is a paid consultant of Stryker. J Pierce, K Needham and C Adams are employees of Baker Tilly LLP, which received consulting fees from the sponsor. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Supplementary Material
File (supplementary table 1.docx)
- Download
- 14.84 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
McLawhorn AS, Buller LT. Bundled payments in total joint replacement: keeping our care affordable and high in quality. Curr. Rev. Musculoskelet. Med. 10(3), 370–377 (2017).
2.
Yelin E, Weinstein S, King T. The burden of musculoskeletal diseases in the United States. Semin. Arthritis Rheum. 46(3), 259–260 (2016).
3.
United States Bone and Joint Initiative: The Burden of Musculoskeletal Diseases in the United States. Osteoarthritis (2014). www.boneandjointburden.org/print/book/export/html/978
4.
Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet 370(9597), 1508–1519 (2007).
5.
Lavernia CJ, Alcerro JC. Quality of life and cost–effectiveness 1 year after total hip arthroplasty. J. Arthroplasty 26(5), 705–709 (2011).
6.
Daigle ME, Weinstein AM, Katz JN, Losina E. The cost–effectiveness of total joint arthroplasty: a systematic review of published literature. Best Pract. Res. Clin. Rheumatol. 26(5), 649–658 (2012).
7.
Singh JA, Yu S, Chen L, Cleveland J. Rates of total joint replacement in the United States: future projections to 2020–2040 using the national inpatient sample. J. Rheumatol. 46(9), 1134–1140 (2019).
8.
Bargar WL, Bauer A, Borner M. Primary and revision total hip replacement using the Robodoc System. Clin. Orthop. Relat. Res. (354), 82–91 (1998).
9.
Bargar WL. Robots in orthopaedic surgery: past, present, and future. Clin. Orthop. Relat. Res. 463, 31–36 (2007).
10.
Lang JE, Mannava S, Floyd AJ et al. Robotic systems in orthopaedic surgery. J. Bone Joint Surg. Br. 93(10), 1296–1299 (2011).
11.
Parsley BS. Robotics in orthopaedics: a brave new world. J. Arthroplasty 33(8), 2355–2357 (2018).
12.
Schulz AP, Seide K, Queitsch C et al. Results of total hip replacement using the Robodoc surgical assistant system: clinical outcome and evaluation of complications for 97 procedures. Int. J. Med. Robot. 3(4), 301–306 (2007).
13.
Jacofsky DJ, Allen M. Robotics in arthroplasty: a comprehensive review. J. Arthroplasty 31(10), 2353–2363 (2016).
14.
Sinha RK. Outcomes of robotic arm-assisted unicompartmental knee arthroplasty. Am. J. Orthop. 38(Suppl. 2), 20–22 (2009).
15.
Pearle AD, O'Loughlin PF, Kendoff DO. Robot-assisted unicompartmental knee arthroplasty. J. Arthroplasty 25(2), 230–237 (2010).
16.
Hampp EL, Sodhi N, Scholl L et al. Less iatrogenic soft-tissue damage utilizing robotic-assisted total knee arthroplasty when comparted with a manual approach. Bone Joint Res. 8(10), 495–501 (2019).
17.
Chen AF, Kazarian GS, Jessop GW, Makhdom A. Robotic technology in orthopaedic surgery. J. Bone Joint Surg. Am. 100(22), 1984–1992 (2018).
18.
Van der List JP. Current state of computer navigation and robotics in unicompartmental and total knee arthroplasty: a systemic review with meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 24(11), 3482–3495 (2016).
19.
Tarwala R, Dorr LD. Robotic assisted total hip arthroplasty using the MAKO platform. Curr. Rev. Musculoskelet. Med. 4(3), 151–156 (2011).
20.
Illgen RL, Bukowski BR, Abiola R et al. Robotic-assisted total hip arthroplasty: outcomes at minimum two-year follow up. Surg. Technol. Int. 30, 365–372 (2017).
•• Analysis of a single surgeon’s first 100 manual THAs (mTHAs) versus last 100 mTHAs versus first 100 robotic-assisted total hip arthroplasties (RATHAs) at 2-year follow-up, showing more accurate implant placement, reduced blood loss and reduced dislocation rates for RATHA compared to mTHA.
21.
Kayani B, Konan S, Thakrar RR, Huq SS, Haddad FS. Assuring the long-term total joint arthroplasty: a triad of variables. Bone Joint J. 101-B(1 Suppl. A), 11–18 (2019).
22.
Perets I, Walsh JP, Close MR, Mu BH, Yuen LC, Domb BG. Robot-assisted total hip arthroplasty: clinical outcomes and complication rate. Int. J. Med. Robot. 14(4), 1–8 (2018).
23.
Domb BG, Chen JW, Lall AC, Perets I, Maldonado DR. Minimum 5-year outcomes of robotic-assisted primary total hip arthroplasty with a nested comparison against manual primary total hip arthroplasty: a propensity score-matched study. J. Am. Acad. Orthop. Surg. 28(20), 847–856 (2020).
•• Study comparing 66 RATHAs with 66 matched mTHAs at 5-year follow-up, showing higher patient-reported outcome scores and reduced risk of acetabular implant placement outside the designated safe zones.
24.
Cool CL, Jacofsky DJ, Seeger KA, Sodhi N, Mont MA. A 90-day episode-of-care cost analysis of robotic-arm assisted total knee arthroplasty. J. Comp. Eff. Res. 8(5), 327–336 (2019).
• Comparison of Medicare costs for 519 robotic-assisted versus 2595 manual total knee arthroplasties over 90 days, showing reduced lengths of stay, increase in home discharge, reduced readmissions and average savings for the robotic-assisted procedure over a 90-day EOC.
25.
Pierce J, Needham K, Adams C, Coppolecchia A, Lavernia C. Robotic arm-assisted knee surgery: an economic analysis. Am. J. Manag. Care 26(7), e205–e210 (2020).
• Compared 357 robotic-assisted versus 1785 manual total knee arthroplasties, showing reduced lengths of stay, reduced utilization of post-operative services and average savings for the robotic-assisted procedure over a 90-day episode-of-care in commercially insured patients.
26.
Yang JY, Webster-Clark M, Lund JL, Sandler RS, Dellon ES, Stürmer T. Propensity score methods to control for confounding in observational cohort studies: a statistical primer and application to endoscopy research. Gastrointest. Endosc. 90(3), 360–369 (2019).
27.
Pirracchio R, Resche-Rigon M, Chevret S. Evaluation of the propensity score methods for estimating marginal odds ratios in case of small sample size. BMC Med. Res. Methodol. 12, 70 (2012).
28.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46(3), 399–424 (2011).
29.
Staffa SJ, Zurakowski D. Five steps to successfully implement and evaluate propensity score matching in clinical research studies. Anesth. Analg. 127(4), 1066–1073 (2018).
30.
Suarez-Ahedo C, Gui C, Martin TJ, Chandrasekaran S, Lodhi P, Domb BG. Robotic arm-assisted total hip arthroplasty results in smaller acetabular cup size in relation to the femoral head size: a matched-pair controlled study. Hip Int. 27(2), 147–152 (2017).
31.
Heng YY, Gunaratne R, Ironside C, Taheri A. Conventional vs robotic arm assisted total hip arthroplasty (THA) surgical time, transfusion rates, length of stay, complications and learning curve. J. Arthritis 7(4), 1–4 (2018).
32.
McGrory BJ, Morrey BF, Cahalan TD, An KN, Cabanela ME. Effect of femoral offset on range of motion and abductor muscle strength after total hip arthroplasty. J. Bone Joint Surg. Br. 77(6), 865–869 (1995).
33.
Charles MN, Bourne RB, Davey JR, Greenwald AS, Morrey BF, Rorabeck CH. Soft-tissue balancing of the hip: the role of femoral offset restoration. Instr. Course Lect. 54, 131–141 (2005).
34.
Centers for Medicare & Medicaid Services. Comprehensive care for joint replacement model three year extension and changes to episode definition and pricing (2020). www.cms.gov/newsroom/fact-sheets/comprehensive-care-joint-replacement-model-three-year-extension-and-changes-episode-definition-and
35.
Mechanic R. Post-acute care – the next frontier for controlling Medicare spending. N. Engl. J. Med. 370(8), 692–694 (2014).
36.
Feder J. Bundle with care – rethinking Medicare incentives for post-acute care services. N. Engl. J. Med. 369(5), 400–401 (2013).
37.
Centers for Medicare & Medicaid Services. Bundled Payments for Care Improvement (BPCI) initiative (2020). https://innovation.cms.gov/innovation-models/bundled-payments
38.
Hackbarth G, Reischauer R, Mutti A. Collective accountability for medical care-toward bundled Medicare payments. N. Engl. J. Med. 359(1), 3–5 (2008).
Information & Authors
Information
Published In
Pages: 1225 - 1234
PubMed: 34581189
Copyright
© 2021 Future Medicine Ltd.
History
Received: 12 November 2020
Accepted: 19 August 2021
Published online: 28 September 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Robotic-assisted total hip arthroplasty: an economic analysis. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0255
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Jenna Bernstein, Jean-Baptiste Trouiller, Mina Kabiri, William G. Hamilton, Cost-Effectiveness of Computer-Assisted Fluoroscopic Navigation in Primary Total Hip Arthroplasty Compared With Robotic or Manual Techniques, JAAOS: Global Research and Reviews, 10.5435/JAAOSGlobal-D-25-00404, 10, 6, (2026).
- Warran Wignadasan, Christos Dragonas, Andreas Fontalis, Marc Jean Berna, Pit Putzeys, Romir Patel, Fares S Haddad, Economic evaluation of robotic-assisted versus manual total hip arthroplasty: a systematic review of cost and clinical outcomes, EFORT Open Reviews, 10.1530/EOR-2025-0179, 11, 6, (553-560), (2026).
- Michael S. Kim, Deeyana Roshanzaer, Melissa R. Romoff, Kylen Soriano, Ryan DiGiovanni, Russell Stitzlein, Steven Yang, Peter Hsiue, Utilization Trends and Surgical Outcomes of Technology-Assisted Total Hip Arthroplasty in the United States From 2014 Through 2024, Arthroplasty Today, 10.1016/j.artd.2026.101983, 39, (101983), (2026).
- Puzhen Wu, Xinrui Liu, Xianyu Zhang, Ziyu Guo, Lawrence Lau, From planning to monitoring: artificial intelligence applications across the total hip arthroplasty continuum, HIP International, 10.1177/11207000261423870, 36, 2, (139-150), (2026).
- Faraz A. Asim, K. Keely Boyle, Antonia F. Chen, Robotic-assisted total hip arthroplasty, Journal of Joint Surgery and Research, 10.1016/j.jjoisr.2025.12.006, 4, 1, (81-86), (2026).
- David Maman, Yaniv Steinfeld, Yaron Berkovich, Robotic-assisted total hip arthroplasty in the United States: a nationwide propensity-matched analysis of adoption, outcomes, and complications, Langenbeck's Archives of Surgery, 10.1007/s00423-025-03963-7, 411, 1, (2026).
- Kazumasa Miyatake, Yasuharu Nakashima, Yutaka Inaba, Naomi Kobayashi, Tetsuya Jinno, Tamon Kabata, Yoshitomo Kajino, Shigeru Mitani, Hirosuke Endo, Satoshi Hamai, Keiichiro Ueshima, Masaki Takao, Takuma Yamasaki, Masanori Fujii, Yasuhiko Takegami, Hyonmin Choe, Yasuhiro Homma, Atsuhiro Fujie, Hiroyuki Ike, Tetsuo Hayama, Gaku Koyano, Naofumi Taniguchi, Kazuo Tomizawa, Keisuke Watarai, Tomohiro Goto, Takaaki Ohmori, Daisuke Inoue, Toru Nishiwaki, Takeyuki Tanaka, Yoshitomo Saiki, Shuro Furuichi, Toyohiro Kawamoto, Tomonori Tetsunaga, Masaru Kadowaki, Yusuke Fujimoto, Ryosuke Yamaguchi, Yusuke Uehara, Daisuke Hara, Tomohiro Shimizu, Tsuguaki Hosoyama, Hironobu Hoshino, Hidetoshi Hamada, Masashi Ishida, Shinya Hayashi, Takashi Imagama, Ryo Sugama, Ryuichi Sato, Yoshinobu Uchihara, Kensuke Fukushima, Ryohei Takada, Kazuki Yamada, Takeshi Shoji, Japanese Orthopaedic Association (JOA) clinical practice guidelines on the management of osteoarthritis of the hip, 2024- the third edition- secondary publication, Journal of Orthopaedic Science, 10.1016/j.jos.2025.10.006, 31, 1, (1-62), (2026).
- Yajing Gao, Yi Yang, Zhuofu Li, Bai Zang, Chengfengyi Yang, Feifei Zhou, Qiaoqin Wan, Systematic review of health economic evaluation of robot-assisted hip and knee arthroplasty, Health Economics Review, 10.1186/s13561-025-00701-z, 16, 1, (2025).
- Duncan E J Whittaker, Gareth Medlock, David W Neilly, Thomas I Diffley, Haroon Rehman, Comparative analysis of CT-based and 2D digital templating in robotic hip arthroplasty, HIP International, 10.1177/11207000251352128, 36, 1, (12-17), (2025).
- Karlos E. Zepeda, Carmelo Burgio, Theofilos Karasavvidis, Tsion M. Yared, Cale Pagan, Edward H. Grabov, Seth A. Jerabek, David J. Mayman, Jonathan M. Vigdorchik, Impact of Robotic Assistance on Total Hip Arthroplasty: Granular Insights Into Surgical Time, The Journal of Arthroplasty, 10.1016/j.arth.2025.03.068, 40, 8, (S172-S178), (2025).
- See more