End-of-life cost for lung cancer patients in Greece: a hospital-based retrospective study
Publication: Journal of Comparative Effectiveness Research
Abstract
Objective: The aim of the present study was to estimate the cost of treating patients with lung cancer at their end-of-life (EOL) phase of care in Greece. Materials & methods: A hospital-based retrospective study was conducted in the Oncology Unit of ‘Sotiria’ Hospital, in Athens, Greece. All lung cancer patients who died between 1 January 2015 and 31 December 2018 with at least 6 months follow-up were enrolled in the study. Healthcare resource utilization data, including inpatient and outpatient ones, during the last 6 months before death was extracted from a registry kept in the unit. This data were combined with the corresponding local unit costs to calculate the 6, 3 and 1-month EOL cost in €2019 values. Results: A total of 122 patients met the inclusion criteria. The mean (standard deviation) age at diagnosis was 67.8 (8.9) years with 78.7% of patients being male and 55.0% diagnosed at stage IV. About 52.5% of patients had been diagnosed with adenocarcinoma, 28.7% with squamous non-small-cell lung cancer types and 18.9% with small-cell-lung cancer. The median overall survival of these patients was 10.8 months. During the EOL periods, the mean cost/patient in the last 6, 3 and 1 month were €7665, €3351 and €1009, respectively. Pharmaceutical cost was the key driver of the total cost (75% of the total 6-month) followed by radiation therapy (16.2%). The median EOL 6-month cost was marginally statistically significantly higher among patients with adenocarcinoma (€9031) compared with squamous (€6606) and to small-cell-lung cancer (€5474). Conclusion: The findings of the present study indicate that lung cancer treatment incurs high costs in Greece, mainly attributed to pharmaceutical expenses, even at the EOL phase.
Lung cancer is a major public health problem worldwide, the most recent global estimations indicate that 2.1 million new cases were diagnosed worldwide in 2018, with 1.8 million death in the same year [1]. Greece is one of the European countries in which lung cancer is a leading cause of death with almost 8300 people having died from lung cancer in 2018 [1]. Apart from the humanistic burden, lung cancer may incur great economic consequences for the healthcare systems, patients and society overall. More specifically, the direct cost of care for lung cancer patients amounts to more than €3 billion per year in Europe [2], while after considering costs related to disability and premature mortality, as well, the total cost amount to more than €100 billion [2]. Moreover, in Greece, a nationwide study that calculated annual hospital costs for the treatment of smoking-attributable diseases, demonstrated that lung cancer-related costs for that year were approximately €38.2 million [3].
However, cancer care costs vary by clinical care phase, with the highest costs observed in the initial period following diagnosis and in the last year of life (end-of-life [EOL] period) [4–7]. The increased EOL care cost is attributed to the aggressive cancer care over the past decade [8]. There is a growing body of literature revealing the overuse of chemotherapy, radiotherapy and monoclonal antibodies/immunotherapy during the last weeks of death [9–11] especially in advanced stage cancer patients [9–11] with limited data to be available for lung cancer patients [9]. Moreover, the existing literature declare that the EOL care depends on a wide range of characteristics such as patients’ age, sex and other sociodemographic characteristics, cancer type and geographical location [11]. However, more aggressive medical care is associated with not only increased cost but worst patients’ quality of life, as well [12–14]. Therefore, estimating EOL care cost and how it varies depending on patient characteristics is critical for healthcare policy makers in order to guide effective interventions for minimizing the impact of EOL care on both patients and society. In Greece, limited data are available regarding the EOL cost of lung cancer patients [15]. In this retrospective study, although the total EOL cost and its cost components are presented, no data are provided regarding the factors that might affect this. In this context, the objective of the current study was to estimate the EOL care cost for patients with lung cancer in Greece and to identify patient characteristics that might affect this cost.
Materials & methods
Study design & population
A retrospective study was conducted based on data extracted from a hospital-based registry kept in the Oncology Unit of ‘Sotiria’ Hospital, in Athens, Greece with all new lung cancer cases who took care in this unit from 2015 onwards. The population of the present study consisted of patients diagnosed with non-small-cell lung cancer, specifically adenocarcinoma and squamous, or small-cell-lung cancer (SCLC) and died between 1 January 2015 and 31 December 2018, with at least 6 months of follow-up before death occurred. All patients died in this time interval were accounted, irrespectively of the place of death. The information maintained in this cancer registry was extracted from patients’ medical records.
Data collected
For the purposes of the present study the following data were extracted: patients’ demographic characteristics such as gender and age and lifestyle characteristics such as smoking status at the time of diagnosis (i.e., current, former or nonsmoker). Moreover, cancer related characteristics at the time of diagnosis like the histological type, the stage and the performance status were also extracted. As for staging, the 7th edition of TNM classification for patients diagnosed earlier than 1 January 2017 was used, while for those with a diagnosis after the mentioned date, 8th edition was used. Patients were classified into those diagnosed at an early stage (stage I or II), those diagnosed at locally advanced (stage III) and metastatic stage (stage IV).
Healthcare resource utilization data, such as hospitalization, therapy (i.e., chemotherapy/immunotherapy, radiotherapy and surgery), and laboratory/imaging tests during the last 6 months before death were also extracted. More specifically, the data extracted regarding medication therapy (i.e., chemotherapy, targeted therapy, immunotherapy, supportive therapy like zoledronic acid, denosumab, granulocyte colony-stimulating factors (G-CSFs) and erythropoietin) included the name of the active substance, the total dose per administration, the route of administration, the number of days of administrations per cycle, and the number of cycles per line. Hospitalization data included the reason of hospitalization, and the duration of hospitalization, while the type of surgery (if any) was recorded, as well. The type of radiotherapy along with the number of fractions were recorded, and the number of laboratory and imaging tests to which patients were subjected were recorded. Finally, the date of diagnosis along with the date of death was used to estimate the overall survival.
Cost estimation
To estimate EOL care cost from payer perspective, healthcare resource utilization data were combined with the corresponding local unit costs (in €, 2019), as reimbursed by the public payer (National Organization for Healthcare Services Provision [EOPYY]). To be more specific, to estimate systematic therapy cost and the supportive care cost during the EOL period, the total dose per regimen per cycle was combined with the reimbursed unit costs and the number of cycles per line of therapy administered during the last 6 months. The cost of administration of intravenous agents was included to the cost of drug therapy; this cost was extracted from the Official Government Gazette, law 2150/B/2011. The reimbursed drug cost was calculated on the grounds of the ex-factory prices, as they were published in the drug bulletin issued by the Greek Ministry of Health [16] after applying the relevant discounts provided in the corresponding legislation (Official Government Gazette, law 115/7 August 2017). The type of radiotherapy along with the number of fractions and the corresponding unit costs as extracted from the official website of EOPYY was used to estimate the radiotherapy cost. Similarly, the laboratory/imaging cost was calculated, combining the frequency of laboratory/imaging tests used during the EOL period with the corresponding unit costs as obtained from the official website of EOPYY under the assumption that all tests were performed privately (Supplementary Table 1). The cost for inpatient services including hospitalization for reasons relevant to the disease setting as well as surgeries was calculated using the corresponding Diagnostic Related Groups tariff issued by the Greek Ministry of Health [17] (Supplementary Table 2). Similarly, the 3 and 1-month EOL was calculated, as well.
Statistical analysis
All continuous variables were summarized with median, 1st and 3rd qualtiles as their distributions were skewed, while all categorical variables were summarized with frequencies (n) and percentages (%).
Cost data are presented as mean and 95% CI using the bias-corrected and accelerated CI (adjusted for ties) as obtained from 5000 nonparametric bootstrapped resamples. To determine factors associated with EOL cost we applied generalized linear models with gamma family and a log link function, which best fit the expenditure data according to the Box-Cox test and the modified Park test [18]. Cost data were additionally checked if they fit the gamma distribution using Villasenor and Gonzalez-Estrada parameter estimators [19]. Robust standard errors were computed to account for the fact that clinicians treating patients in the same hospital may share the same clinical practices. Gamma co-efficients generated by the regression model were exponentiated to retransform them into relative cost estimates. As potential risk factors the number of comorbidities, the number of metastases, the histological type, the duration from diagnosis to death, the cancer stage, the gender and the age during diagnosis were tested using univariate models. Factors which had a p-value < 0.2 in the univariate analyses were included in the multivariate model. The significance level was set to a = 0.05. Statistical analysis was performed using STATA software (version 13.0, STATA Corp, College Station, TX, USA) while gamma distribution fitness was checked using R version 3.6.1.
Results
Patients’ characteristics
A total of 122 patients met the inclusion criteria, almost half of whom were diagnosed with adenocarcinoma. The place of death was reported for the 44% of the patients. Among them, the 59% had died in a hospital, while the rest in their home. The mean age at diagnosis was 68 years with 78.7% of patients being male and 55.0% diagnosed at stage IV. Only 9.0% of patients had no comorbidities, while more than 50.0% were current smokers at the time of cancer diagnosis. Almost all patients except for two had metastases at the time of diagnosis (Table 1). The median (1st–3rd quartile) overall survival of these patients was 10.8 (8–13) months. Almost 60.0% had died within 12 months since diagnosis.
| Demographic and diagnostic characteristics | n = 122 |
|---|---|
| Gender, n (%) | |
| – Female | 26 (21.3) |
| – Male | 96 (78.7) |
| Age at the time of diagnosis, years | |
| – Median (1st, 3rd quartile) | 68.2 (63.7, 74.3) |
| Smoking status, n (%) | |
| – Current smoker | 60 (51.3) |
| – Former smoker | 51 (43.6) |
| – Nonsmoker | 6 (5.1) |
| Histological or cytological diagnosis | |
| – Adenocarcinoma | 64 (52.5) |
| – Squamous | 35 (28.7) |
| – Small-cell-lung cancer | 23 (18.9) |
| Stage of cancer at diagnosis, n (%) | |
| – Early disease (stages I & II) | 9 (7.4) |
| – III | 45 (37.6) |
| – IV | 66 (55.0) |
| Number of comorbidities, n (%) | |
| – 0 | 11 (9.02) |
| – 1 | 28 (22.95) |
| – 2 | 36 (29.51) |
| – ≥3 | 47 (38.52) |
| Performance status at baseline, n (%) | |
| – Normal activity | 23 (29.5) |
| – Restricted but light work | 36 (46.2) |
| – Selfcaring. Unable to work. Mobile >50% working hours | 16 (20.5) |
| – Limited self-care only. Mobile <50% working hours | 3 (3.9) |
Smoking status data were missing for four patients; stage data were missing for one patient, performance status at baseline data were missing for 44 patients.
Resource utilization
Table 2 presents the resource utilization during the EOL periods. During the last 6 months before death, 88.5% of patients received medication therapy, while this percentage reduced to 74.6% at 3 months and 41% at 1 month before death. Almost two-third of patients that received medication therapy over the last 6 months of their life, received only chemotherapy while almost 20% of drug treated patients received immunotherapy even the last month before death. Platinum-based therapies were the most frequently prescribed treatment as first-line therapy (∼75% of those received chemotherapy as first-line), and nivolumab was the most frequently prescribed immunotherapy as second-line treatment (data not shown). Moreover, during the last 6 months of patients’ life, more than a third was subjected to radiotherapy, while this figure was estimated to be about 10% the last month before death. Only 16% of patients were hospitalized for reason other than drug administration during the last 6 months before death, with this percentage falling to 3% in the last month of patient life. Patients required hospitalization mainly due to respiratory system disorders (in 60% of patients during the last 6 months of life; data not shown).
| 6-months before death | 3-months before death | 1-month before death | |
|---|---|---|---|
| Resource utilization | N (%) | N (%) | N (%) |
| Drug therapy | 108 (88.5) | 91 (74.6) | 50 (41.0) |
| – Chemotherapy + immunotherapy + targeted therapy | 2 (1.8) | 0 (0.0) | 0 (0.0) |
| – Chemotherapy + immunotherapy | 18 (16.7) | 8 (8.7) | 1 (2.0) |
| – Chemotherapy | 70 (64.8) | 60 (65.9) | 34 (68.0) |
| – Chemotherapy + targeted therapy | 11 (10.2) | 9 (9.9) | 2 (4.0) |
| – Immunotherapy | 3 (2.8) | 10 (11.0) | 9 (18.0) |
| – Targeted therapy | 4 (3.7) | 4 (4.4) | 4 (8.0) |
| – G-CSF | 81 (75.0) | 53 (75.0) | 26 (52.0) |
| – Epoetin | 32 (29.6) | 19 (20.9) | 7 (14.0) |
| – Supportive care (other than above) | 8 (7.4) | 5 (5.5) | 1 (2.0) |
| Radiotherapy | 42 (34.4) | 24 (19.7) | 12 (9.8) |
| – Prior to radiotherapy, n (%) patients received | |||
| – G-CSF | 19 (45.2) | 3 (12.5) | 1 (8.3) |
| – Epoetin | 10 (23.8) | 2 (8.3) | 0 (0) |
| – Supportive care (other than above) | 1 (2.4) | 0 (0) | 0 (0) |
| Surgery | 2 (1.6) | 0 (0) | 0 (0) |
| Hospitalization | 20 (16.4) | 17 (13.9) | 4 (3.3) |
| Laboratory/imaging tests | 121 (99.2) | 119 (97.5) | 80 (65.6) |
G-CSF: Granulocyte colony stimulating factor.
Cost estimations
The mean total cost per patient from payer perspective were €7665, €3351 and €1009 in the last 6, 3 and 1 month before death, respectively. Pharmaceutical cost was the key driver of the total 6, 3 and 1-month EOL cost (75, 65 and 58%, respectively) followed by radiation therapy (16.2, 22.8 and 31.1%, respectively; Table 3). The key drivers for the 6, 3 and 1-month pharmaceutical cost were the cost of G-CSFs (31, 28 and 30%, respectively), the immunotherapy cost (25, 30 and 32%, respectively) and the chemotherapy cost (23, 20 and 20%, respectively).
| Cost components | 6-month Mean (95% CI) | 3-month Mean (95% CI) | 1-month Mean (95% CI) |
|---|---|---|---|
| Overall cost per patient | 7665 (6733–8943) | 3351 (2860–4080) | 1009 (757–1428) |
| Cost of therapy | |||
| – Drug therapy | 5727 (4878–6853) | 2170 (1821–2652) | 586 (443–817) |
| – Chemotherapy | 1306 (1050–1713) | 437 (338–592) | 119 (79–188) |
| – Targeted therapy | 881 (480–1589) | 339 (170–691) | 63 (22–138) |
| – Immunotherapy | 1426 (907–2352) | 644 (401–1028) | 190 (96–386) |
| – Administration | 248 (210–282) | 101 (82–121) | 30 (23–38) |
| – Epoetin | 71 (50–107) | 34 (20–55) | 9 (4–18) |
| – G-CSF | 1777 (1458–2153) | 609 (453–760) | 174 (120–247) |
| – Supportive care (other than above) | 18 (7–37) | 6 (2–15) | 1 (0–4) |
| – Radiotherapy | 1244 (815–1750) | 763 (457–1268) | 314 (129–664) |
| – Surgery | 55 (0–138) | 0 (0–0) | 0 (0–0) |
| Laboratory/imaging tests | 330 (298–368) | 170 (146–205) | 66 (48–100) |
| Hospitalizations | 309 (178–507) | 247 (135–434) | 43 (8–193) |
G-CSF: Granulocyte colony stimulating factor.
The 6-month EOL cost was found to be statistically significantly higher among patients diagnosed with adenocarcinoma compared with those diagnosed with squamous and SCLC, while 1-month EOL was found to be statistically significantly different only between patients diagnosed with adenocarcinoma and those diagnosed with squamous (Figure 1). Moreover, patients who were from 75 to 85 years old incurred statistically significantly less expenditures during last 6 months of their life compared with those who were from 65 to 75 years old (p =.0014) or younger than 65 years (p =.0036, Table 4).
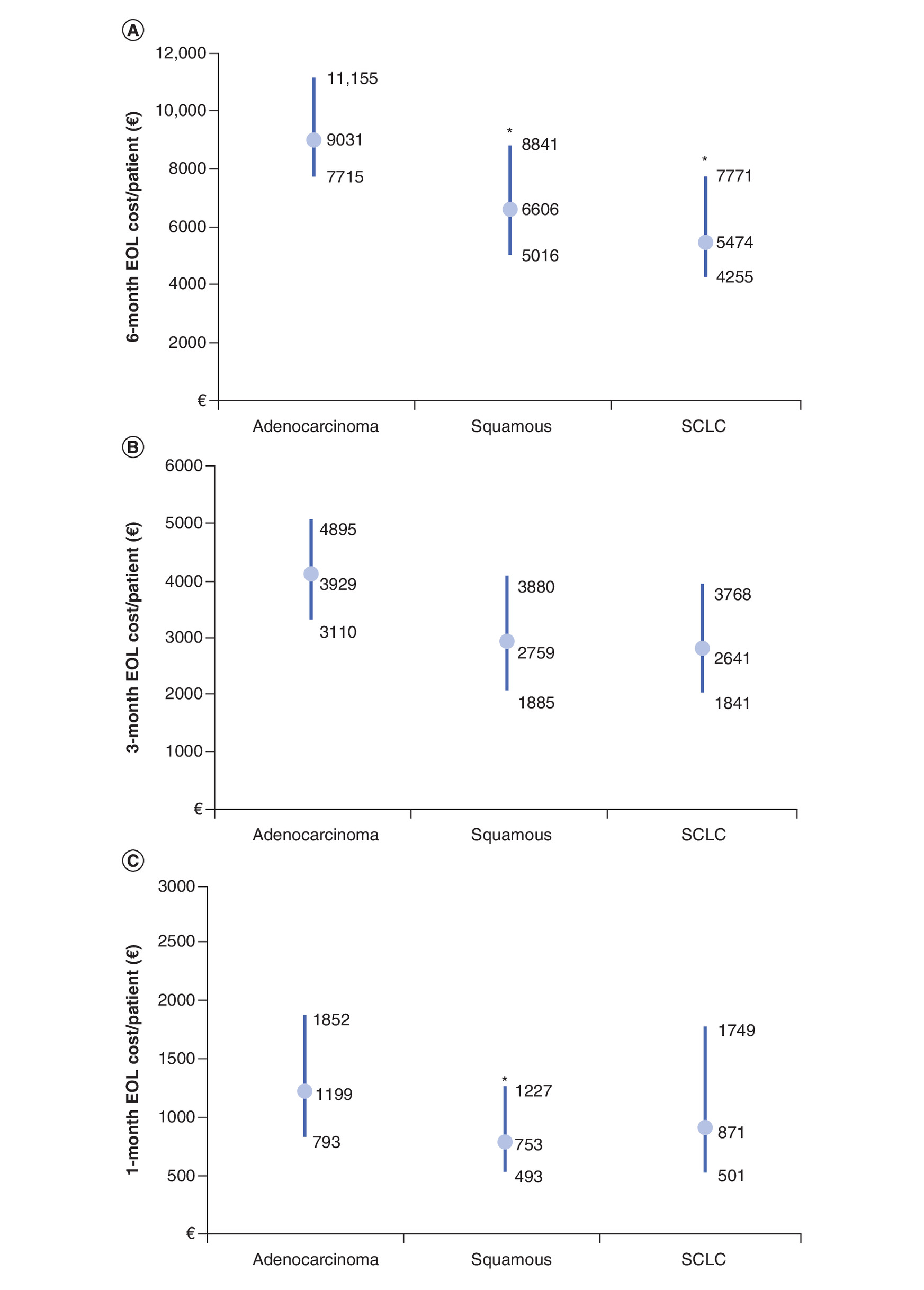
Figure 1. (A) Six, (B) 3 and (C) 1-month EOL cost per lung cancer patient by histological type, in Greece.
*p < 0.05 compared with adenocarcinoma.
EOL: End-of-life; SCLC: Small-cell-lung cancer.
| Overall cost per patient | 6-month Mean (95% CI) | 3-month Mean (95% CI) | 1-month Mean (95% CI) |
|---|---|---|---|
| Gender | |||
| – Male | 8001 (6672–9450) | 3473 (2823–4230) | 1006 (763–1474) |
| – Female | 6426 (5092–8629) | 2899 (2122–4286) | 1019 (537–2262) |
| Age group | |||
| – Less than 65 years | 8715 (6780–11,551) | 3918 (2917–5295) | 1184 (666–2184) |
| – 65 to 75 years | 8366 (6687–9703) | 3790 (2938–4618) | 1240 (905–1800) |
| – 75 to 85 years | 4838 (3718–7221)† | 1701 (1143–2980)† | 309 (166–538)‡ |
| By year | |||
| – Up to 2016 | 5614 (4256–7542) | 2655 (1892–3,687) | 701 (470–955) |
| – 2017 | 8076 (6526–10,054) | 3364 (2446–4,339) | 862 (561–1489) |
| – 2018 | 8494 (6777–10,627) | 3768 (2,857–4,865) | 1360 (848–2151) |
| Comorbidities | |||
| – 0 or 1 | 8366 (6496–10,478) | 3825 (2754–5072) | 1091 (687–1786) |
| – 2 or more | 7336 (6056–8710) | 3128 (2488–3854) | 970 (642–1424) |
| Smoking status | |||
| – Current smoker | 7868 (6615–9531) | 3697 (2916–4670) | 1017 (674–1526) |
| – Former smoker | 7827 (6155–10,103) | 3135 (2397–4127) | 990 (643–1721) |
| – No smoker | 7063 (5022–9206) | 2622 (1359–4058) | 215 (51–700) |
| Stage during diagnosis | |||
| – I or II | 6013 (4285–7691) | 2948 (1312–5626) | 1965 (89–5427) |
| – III | 7140 (5406–8891) | 3087 (2224–3930) | 940 (643–1452) |
| – IV | 8384 (6951–10,232) | 3618 (2791–4537) | 923 (614–1372) |
| Time of death since diagnosis | |||
| – 6–12 months | 8431 (6968–10,189) | 3569 (2822–4334) | 1002 (673–1480) |
| – >12 months | 6524 (5115–8085) | 3025 (2222–3997) | 1019 (647–1758) |
†
6 and 3-month EOL cost differed for patients from 75 to 85 years old compared with 65 to 75 years old or younger than 65 years (p < 0.005 for all pairwise comparisons; Dunn’s Test).
‡
1-month EOL cost differed for patients from 75 to 85 years old compared with 65 to 75 years old (p = 0.0012). The other two pairwise comparisons had a p-value < 0.10 (Dunn’s Test).
EOL: End-of-life.
The multiple generalized linear model in which patients’ gender, postdiagnosis survival, number of metastases at the time of diagnosis, age, stage and histological type were entered as independent factors, revealed that the 6-month EOL cost was almost 51% higher in males compared with females (p = 0.004) after controlling the rest of independent variables. Moreover, a 10-year increase in patients’ age at diagnosis was found to be associated with an almost 16% lower cost (p = 0.020), and patients diagnosed with SCLC were found to be associated with a 32% lower cost compared with those diagnosed with adenocarcinoma (p = 0.023). The time from diagnosis since death, the number of metastases and the stage of cancer during diagnosis were not associated with the 6-month EOL cost (Table 5). A model that included patients’ gender, number of metastases at the time of diagnosis, age and histological type as independent factors, revealed that a unit increase in the number of metastases was associated with almost 15% higher 3-month EOL cost (p = 0.047), while the rest independent factors were not associated with the 3-month EOL (data not shown). The 1- month EOL cost was not associated with any of the variables tested, as such a multivariate model was not constructed (data not shown).
| Multivariate model | |||
|---|---|---|---|
| Exp(b) | 95% CI | p-value | |
| Time from diagnosis to death, months | |||
| – >6 and <= 12 months | Ref | ||
| – >12 months | 0.838 | 0.614, 1.145 | 0.268 |
| Number of metastases | 1.068 | 0.961, 1.187 | 0.220 |
| Age at diagnosis | 0.981 | 0.967, 0.997 | 0.020 |
| Gender | |||
| – Female | Ref | ||
| – Male | 1.505 | 1.143, 1.981 | 0.004 |
| Stage | |||
| – I or II | Ref | ||
| – III | 1.179 | 0.745, 1.864 | 0.482 |
| – IV | 1.175 | 0.738, 1.873 | 0.497 |
| Histology or cytology type | |||
| – Adenocarcinoma | Ref | ||
| – SCLC | 0.677 | 0.483, 0.949 | 0.023 |
| – Squamous | 0.735 | 0.501, 1.077 | 0.114 |
Bold font indicates statistical significance.
SCLC: Small-cell-lung cancer; Ref: reference category.
Discussion
Considering the impact of EOL care on patients’ quality of life and national expenditures, the objective of the present retrospective analysis was to assess the EOL care for lung cancer patients in Greece and to estimate the EOL cost. To the best of our knowledge, this is the second study in Greece [15] aiming to estimate the EOL cost for lung cancer patients and one of the few studies that have been conducted internationally [20–22]. In our study, patients died from 2015 onwards were included as opposed to the previously conducted study in Greece, in which patients died between July 2014 and February 2015 were included. As such, the present study covers the new, innovative therapies approved recently for the management of lung cancer.
Our findings declare that a large proportion of lung cancer patients in Greece continue to receive pharmaceutical therapy (i.e., chemotherapy, targeted therapy and immunotherapy) till the end of their life. Chemotherapy was the most administered therapy till the last month before death, but almost one to five patients received immunotherapy even the last month of their life. These results are in line with those presented in the previously conducted study in Greece aiming to examine the EOL care cost of patients who suffered from terminal stage IIIB/IV lung cancer [15] during the last 6 months of their life. This study revealed that the main inpatient and outpatient cost drivers were chemotherapy and concomitant medication, respectively [15].
However, in other studies conducted in the USA [20,21], Canada [20], English [22] and France [23], it has been found that hospitalization cost was the main cost component of the EOL phase followed by pharmaceutical one. In some studies, it was found that hospitalization cost accounts for more than 70% of the total cost incurred during the terminal phase. These differences among the available studies could be attributed to the treatment patterns, healthcare system, unit costs, type of analysis and study design.
The increased use of pharmacotherapies during the EOL period might be partially explained by the lack of specific treatment guidelines for this phase along with patients’ request to receive further therapy, although they are informed that the expected improvement in terms of survival or quality of life will be probably minimal [24]. Given that the usage of aggressive treatment at EOL stage results in higher healthcare costs without implying improved health outcomes and quality of life for patients [13], health policy interventions are needed to control the unnecessarily aggressive treatment of patients nearing death. Into this line, reduction of unnecessary pharmacotherapy use for patients with advanced cancer who are unlikely to benefit is a goal of the American Society for Clinical Oncology’s Choosing Wisely Campaign [12].
Our study presented that the mean cost per patient from public payer perspective in the last 6, 3 and 1 month before death, was estimated to be €7665, €3351 and €1009, respectively. Therefore, it is understood that, the cost of EOL care has a tremendous financial impact on Greek healthcare system. More specifically, lung cancer is a leading cause of death in Greece with almost 8300 deaths in 2018 [1], combining this number of deaths with the EOL care cost per patient reported in present study, the estimated 1- and 6-month EOL direct cost of these patients for the Greek health system range from €8 million to €64 million per year, respectively. Consequently, it becomes clear that it is of paramount importance to consider the appropriateness of aggressive treatments for EOL patients in Greece to reduce the humanistic and economic burden on patients, their families and the health system.
Moreover, our study found that male gender, younger age and adenocarcinoma were associated with increased EOL care cost. These findings are in line with those provided in the international literature [6,20,25,26]. The association of EOL care cost with age could be partially explained by the tendency of physicians to use all treatment options to prolong the survival of a young patient. The increased EOL care cost for patients diagnosed with adenocarcinoma compared with those diagnosed with SCLC may arise from the fact that there is a growing number of new innovative therapies like immunotherapies approved for the management of non-small-cell lung cancer.
The results of the present study should be interpreted considering several limitations. The main study limitation is that this analysis is based on data extracted from a hospital-based registry and not a national population-based registry. This means that this data might come from a nonrepresentative sample of lung cancer patients in Greece. Second, only direct medical costs were considered in our analysis and not costs incurred by reduced productivity of patients/caregivers, transportation or other intangible costs. Third, although the data were extracted from a registry, the outpatient resource utilization data as well as hospitalization data were collected through interviews with patients or caregivers during the planned visits. This means that outpatient and hospitalization EOL cost is subject to self-reported bias and might hence be underestimated.
Conclusion
To sum up, the findings of the present study indicate that lung cancer treatment incurs high costs in Greece even at the EOL phase, and these costs are mainly attributed to pharmaceutical expenses. Our findings may provide useful insight into the design and implementation of interventions aiming to raise clinicians’ awareness about the importance of not providing aggressive EOL to high-risk care lung cancer patients, in Greece.
•
The objective of the current study was to estimate the end-of-life (EOL) care cost for patients with lung cancer in Greece and to identify patient characteristics that might affect this cost.
•
A hospital-based retrospective study was conducted in the Oncology Unit of ‘Sotiria’ Hospital, in Athens, Greece.
•
Healthcare resource utilization data, including inpatient and outpatient ones, during the last 6 months before death was extracted from a registry kept in the unit.
•
During the EOL periods, the mean cost/patient in the last 6, 3 and 1 month were €7665, €3351 and €1009, respectively.
•
Pharmaceutical cost was the key driver of the total cost (75% of the total 6-month) followed by radiation therapy (16.2%).
•
The present study indicate that lung cancer treatment incurs high costs in Greece even at the EOL phase, and these costs are mainly attributed to pharmaceutical expenses.
•
Moreover, our findings may provide useful insight into the design and implementation of interventions aiming to raise clinicians’ awareness about the importance of not providing aggressive EOL to high-risk care lung cancer patients, in Greece.
Author contributions
G Kourlaba designed and supervised the study. G Kourlaba and G Stefanou conducted the analyses, interpreted the results and wrote the manuscript. E Kokkotou, E Ntalakou, A Apostolopoulou, A Charpidou and N Syrigos were the medical experts who provided local resource utilization data, contributed to results interpretation and manuscript writing. G Gourzoulidis contributed to results interpretation and manuscript writing. All authors reviewed and approved the final manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
All data used to conduct this study are included in this published article.
Supplementary Material
File (suppl_file.docx)
- Download
- 14.81 KB
References
1.
International Agency for Research on Cancer. Global Cancer Observatory. (2018). https://gco.iarc.fr/
2.
European Respiratory Society. The economic burden of lung disease. In: Gibson GJ LR, Sibille Y, Sheffield LB (Eds). European Lung White Book. European Respiratory Society, UK, 16–27 (2013).
3.
Tsalapati K, Vardavas CI, Athanasakis K et al. Going up in ashes? Smoking-attributable morbidity, hospital admissions and expenditure in Greece. Eur. J. Public Health 24(3), 477–479 (2014).
4.
Chastek B, Harley C, Kallich J, Newcomer L, Paoli CJ, Teitelbaum AH. Health care costs for patients with cancer at the end of life. J. Oncol. Pract. 8(6), 75S–80S (2012).
5.
Kaye DR, Min HS, Herrel LA, Dupree JM, Ellimoottil C, Miller DC. Costs of cancer care across the disease continuum. Oncologist 23(7), 798–805 (2018).
6.
Yabroff KR, Lamont EB, Mariotto A et al. Cost of care for elderly cancer patients in the United States. J. Natl Cancer Inst. 100(9), 630–641 (2008).
7.
Yabroff KR, Warren JL, Brown ML. Costs of cancer care in the USA: a descriptive review. Nat. Clin. Pract. Oncol. 4(11), 643–656 (2007).
8.
Earle CC, Landrum MB, Souza JM, Neville BA, Weeks JC, Ayanian JZ. Aggressiveness of cancer care near the end of life: is it a quality-of-care issue? J. Clin. Oncol. 26(23), 3860–3866 (2008).
9.
Haque W, Verma V, Butler EB, Teh BS. Patterns of end-of-life oncologic care for stage IV non-small cell lung cancer in the United States. Anticancer Res. 39(6), 3137–3140 (2019).
10.
Kovacevic A, Dragojevic-Simic V, Rancic N et al. End-of-life costs of medical care for advanced stage cancer patients. Vojnosanit. Pregl. 72(4), 334–341 (2015).
11.
Langton JM, Blanch B, Drew AK, Haas M, Ingham JM, Pearson SA. Retrospective studies of end-of-life resource utilization and costs in cancer care using health administrative data: a systematic review. Palliat. Med. 28(10), 1167–1196 (2014).
12.
Schnipper LE, Smith TJ, Raghavan D et al. American Society of Clinical Oncology identifies five key opportunities to improve care and reduce costs: the top five list for oncology. J. Clin. Oncol. 30(14), 1715–1724 (2012).
13.
Wright AA, Zhang B, Ray A et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 300(14), 1665–1673 (2008).
14.
Mor V, Wagner TH, Levy C et al. Association of expanded VA hospice care with aggressive care and cost for veterans with advanced lung Cancer. JAMA Oncol. 5(6), 810–816 (2019).
15.
Souliotis K, Kani C, Marioli A et al. End-of-life health-care cost of patients with lung cancer: a retrospective study. Health Serv. Res. Manag. Epidemiol. (2019) (Epub ahead of print).
16.
Greek Ministry of Health. Drug Price Bulletin, February 2019 (2019). www.moh.gov.gr/articles/times-farmakwn/deltia-timwn/6053-epikairopoihsh-deltiwn-timwn-farmakwn-logw-dioikhtikwn-metabolwn-kai-allaghs-f-p-a-12-2-2019
17.
Greek Ministry of Health. Diagnostic Related Groups, A thens (2019). www.yyka.gov.gr/articles/health/domes-kai-draseis-gia-thn-ygeia/kwdikopoihseis/709-kleista-enopoihmena-noshlia-1
18.
Dodd S, Bassi A, Bodger K, Williamson P. A comparison of multivariable regression models to analyze cost data. J. Eval. Clin. Pract. 12(1), 76–86 (2006).
19.
Villaseñor JA, González-Estrada E. A variance ratio test of fit for Gamma distributions. Stat. Probabil. Lett. 96, 281–286 (2015).
20.
Bremner KE, Krahn MD, Warren JL et al. An international comparison of costs of end-of-life care for advanced lung cancer patients using health administrative data. Palliat. Med. 29(10), 918–928 (2015).
21.
Kutikova L, Bowman L, Chang S, Long SR, Obasaju C, Crown WH. The economic burden of lung cancer and the associated costs of treatment failure in the United States. Lung Cancer 50(2), 143–154 (2005).
22.
Oliver E, Killen J, Kiebert G et al. Treatment pathways, resource use and costs in the management of small cell lung cancer. Thorax 56(10), 785–790 (2001).
23.
Bylicki O, Rivière F, Tournier C et al. Factors associated with aggressiveness of end-of-life care for lung cancer patients and associated costs of care. Clin. Lung Cancer (2020) (Epub ahead of print).
24.
Aitini E, Adami F, Cetto GL. End of life in cancer patients: drugs or words? Ann. Oncol. 21(5), 914–915 (2010).
25.
Hung YN, Liu TW, Wen FH, Chou WC, Tang ST. Escalating health care expenditures in cancer decedents' last year of life: a decade of evidence from a retrospective population-based cohort study in Taiwan. Oncologist 22(4), 460–469 (2017).
26.
Zarogoulidou V, Panagopoulou E, Papakosta D et al. Estimating the direct and indirect costs of lung cancer: a prospective analysis in a Greek University Pulmonary Department. J. Thorac. Dis. 7(Suppl. 1), S12–S19 (2015).
Information & Authors
Information
Published In
Pages: 315 - 324
PubMed: 33605788
Copyright
© 2021 Future Medicine Ltd.
History
Received: 8 August 2020
Accepted: 14 December 2020
Published online: 19 February 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
End-of-life cost for lung cancer patients in Greece: a hospital-based retrospective study. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0167
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Nikolaos Papathanasiou, Maria Spiliotopoulou, Eleni Karagkouni, Dimitrios Apostolopoulos, Paraskevi Katsakiori, John Yfantopoulos, Nikolaos Kotsopoulos, Cost-Effectiveness of Positron Emission Tomography/Computed Tomography (PET/CT) in the Initial N-Staging of Head–Neck Cancer and Comparison with CT and Magnetic Resonance Imaging (MRI), Current Oncology, 10.3390/curroncol32120677, 32, 12, (677), (2025).
- Danai Ktena, Panagiota Naoum, Evie Dalakaki, Yiannis Dimitriadis, Grace Mountain, Robert Hughes, Sherneca Clarke-Melville, Alexander Roediger, Kostas Athanasakis, Assessing the impact of anti-PD-1/PD-L1 inhibitors on cancer care health and budget in Greece, Journal of Cancer Policy, 10.1016/j.jcpo.2025.100628, 45, (100628), (2025).
- Xuanqi Pan, Katerina Togka, Hilde ten Berge, Lisa de Jong, Harry Groen, Maarten J. Postma, Eleftherios Zervas, Ioannis Gkiozos, Christoforos Foroulis, Kyriaki Tavernaraki, Sofia Lampaki, Georgia Kourlaba, Antonios Moraris, Sofia Agelaki, Konstantinos Syrigos, Lung cancer screening with volume computed tomography is cost-effective in Greece, PLOS ONE, 10.1371/journal.pone.0316351, 20, 3, (e0316351), (2025).
- George Gourzoulidis, Catherine Kastanioti, George Mavridoglou, Theodore Kotsilieris, Dikaios Voudigaris, Charalampos Tzanetakos, Does Real-World Evidence of the Economic Burden of Lung Cancer in Greece Exist? A Systematic Review of the Literature, Current Oncology, 10.3390/curroncol32030130, 32, 3, (130), (2025).
- Soraya Camargo Ito Süffert, Carlos Eduardo Aliatti Mantese, Felipe Rodrigo de Castro Meira, Katia Flavia Rosso de Oliveira Trindade, Ana Paula Beck da Silva Etges, Rafael José Vargas Alves, Claudia Giuliano Bica, End-of-Life Costs in Cancer Patients: A Systematic Review, American Journal of Hospice and Palliative Medicine®, 10.1177/10499091241285890, 42, 9, (932-961), (2024).
- George Gourzoulidis, Oresteia Zisimopoulou, Andrianos Liavas, Charalampos Tzanetakos, Lorlatinib as a first-line treatment of adult patients with anaplastic lymphoma kinase-positive advanced non-small cell lung cancer: Α cost-effectiveness analysis in Greece, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2023.2288249, 24, 3, (375-385), (2023).
- George Gourzoulidis, Oresteia Zisimopoulou, Nadia Boubouchairopoulou, Christina Michailidi, Chrissy Lowry, Charalampos Tzanetakos, Georgia Kourlaba, Cost-effectiveness Analysis of Lorlatinib in Patients Previously Treated with Anaplastic Lymphoma Kinase Inhibitors for Non-small Cell Lung Cancer in Greece, Journal of Health Economics and Outcomes Research, 10.36469/jheor.2022.32983, 9, 1, (50-57), (2022).