Translating stakeholder-driven comparative effectiveness research into practice: the PCORnet Bariatric Study
Publication: Journal of Comparative Effectiveness Research
It is often said that it can take up to 17 years to translate comparative effectiveness research into practice [1]. Stakeholder-driven research may hold promise for shortening that time-frame [2] – for example, by enhancing study recruitment, promoting greater uptake of research findings, facilitating decision making in participatory design and helping to ensure that the proposed interventions are feasible in the clinical setting [3]. Stakeholder-driven research might also improve the fidelity and sustainability of comparative effectiveness research translation.
The engagement of stakeholders throughout the research process has been named as a key tenet of patient-centered outcomes research [2] and is increasingly emphasized in translational research [4,5]. Indeed, stakeholders can contribute throughout the research process, including research question development and study design, data collection, analysis and interpretation, and dissemination of findings [6]. The goal of this editorial is to describe a recent example of stakeholder-driven comparative effectiveness research with the goal of improving the health outcomes of patients with severe obesity.
Severe obesity is very common (14.5% of US adults have a BMI ≥35) [7] and linked with substantial morbidity, mortality and reduced quality of life [8,9]. Considerable data support the safety and effectiveness of bariatric surgery for promoting weight loss and improved health outcomes, particularly among adults with Type 2 diabetes mellitus [10–15]. But there has been a dramatic shift in use of bariatric procedures over the past decade where the newest procedure, the sleeve gastrectomy (SG), is now the most commonly performed despite a lack of long-term evidence comparing its outcomes with the Roux-en-y gastric bypass (RYGB) and adjustable gastric band (AGB). Also, the utilization of bariatric surgical procedures remains low in the eligible population, and reasons for this include low provider and patient knowledge about the risks and benefits and lack of high-quality comparative studies between bariatric procedures [16].
The PCORnet Bariatric Study
At the inception of PCORnet®, the National Patient-Centered Clinical Research Network, the Patient-Centered Outcomes Research Institute (PCORI) invited each network to identify one stakeholder on a multidisciplinary Obesity Task Force, which was charged with identifying and prioritizing research topics that would both contribute important scientific knowledge related to obesity and demonstrate the utility of PCORnet for promoting evidence-based and patient-centered healthcare. One of the highest-priority topics was determined to be the comparison of safety and effectiveness of the most common bariatric procedures, and preliminary topic specification was undertaken by a work group including four patients, eight obesity medicine specialists, one bariatric surgeon and twelve researchers with expertise in topics related to obesity. Following a proposal development process that involved an expanded team of researchers and stakeholders from across PCORnet, PCORI went on to fund this research project as the PCORnet Bariatric Study (PBS) [17] using data from 41 health systems. PBS is the largest and longest multisite longitudinal cohort of bariatric patients ever assembled to examine weight loss, diabetes and safety outcomes, including 46,510 adults and 544 adolescents.
The PBS was guided by a 15-member Executive Stakeholder Advisory Group that included patients, advocacy group leaders, adult and pediatric surgeons, and obesity medicine providers who helped identify relevant outcomes, prioritize analyses, advise on study design and plan for dissemination of findings. Stakeholders attended the study’s in-person meetings and met twice monthly by teleconference over the course of the project. As the study evolved, stakeholders were also invited to work on smaller workgroups that were focused on research activities they were more passionate about.
The key research findings from PBS to date include statistically significant and clinically meaningful differences in all study end points across procedure groups. Specifically, at five years follow-up, the PBS found [17–20]: significantly greater percent total weight loss for RYGB (26%) than either SG (19%) or AGB (12%) [19]; similar cumulative incidence of diabetes remission for RYGB (86%) and SG (84%) – both significantly greater than AGB (59%); lower rates of diabetes relapse with RYGB (33%) compared with SG (42%) and AGB (73%) [21]; and finally, higher rates of abdominal operation or intervention with RYGB (12%) and AGB (41%) compared with SG (9%); as well as higher rates of hospitalization for AGB (42%), followed by RYGB (38%) and SG (33%) [20]. Figure 1 summarizes these results.
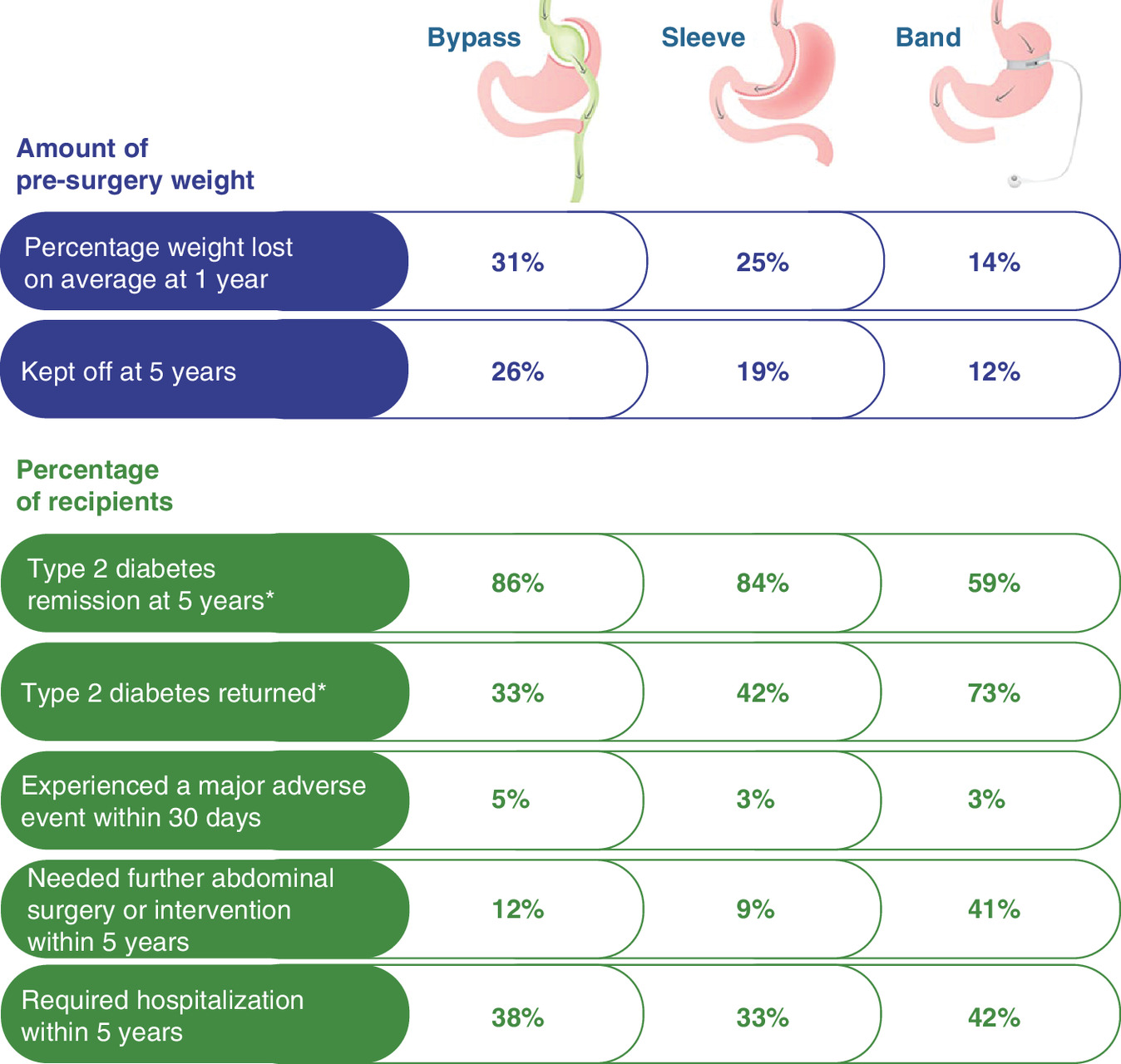
Figure 1. The PCORnet Bariatric Study key findings related to weight loss, diabetes outcomes and safety of bariatric procedures at 5 years follow-up.
*Cumulative incidence of remission and relapse at 5 years. The cumulative incidence of relapse is the percentage among those whose diabetes had remitted.
Shared decision making & the translation of bariatric surgery research into practice
Only 1% of eligible patients choose to undergo bariatric surgery each year. Whether this is the ‘right rate’, based on the preferences of well-informed patients, is unknown, but a recent national survey of adults with severe obesity found that only 1 in 10 report that their primary care provider (PCP) had recommended bariatric surgery [22]. There is also a wide geographical variation in bariatric surgery use in the USA [17,23,24], and this variation in care is likely driven by a variety of factors, including, low patient understanding of the benefits and risks, lack of insurance coverage, and surgeon preference and skill (e.g., not all surgeons have been trained or feel comfortable with all procedures) [25]. For true shared decision making (SDM) to occur, it is important for surgeons to have a balanced discussion of the risks and benefits of all available options, not just the ones for which he or she has preference, expertise or special training. And PCPs should know how to identify appropriate bariatric surgical candidates, be broadly familiar with the available bariatric procedures and outcomes, and be able to engage patients in a SDM conversation that identifies their preferences for treatment [26].
Despite research demonstrating the effectiveness of SDM, uptake of SDM in clinical practice remains slow, and most clinicians and care settings have little or no experience with SDM [27]. Some of the systemic barriers to the use of SDM include perceived time constraints associated with SDM; perceptions that SDM does not work well with certain patient groups; lack of training to equip clinicians with requisite education and skills necessary to facilitate SDM; and the perception among providers that they already do SDM with their patients, despite evidence to the contrary [28]. In recognition of these challenges, PCORI requested applications for dissemination and implementation projects applying multicomponent implementation strategies to translate comparative effectiveness research into routine clinical practice through SDM [27], and the PBS team was awarded funding.
The primary objectives of our project are to refine, deploy and rigorously evaluate a multicomponent strategy to implement a SDM approach to improve decisions around bariatric surgery among patients with severe obesity in primary and specialty care settings. We have incorporated the comparative effectiveness research evidence from PBS into an existing decision aid (DA) and SDM approach, which has a demonstrated impact on patient knowledge, decisional conflict, satisfaction and care decisions [29–34]. The updated strategy will be implemented into two healthcare systems: Kaiser Permanente Washington (KPWA) and UPMC in Pennsylvania. These sites also contributed data to PBS, so their involvement in this phase of implementation work represent excellent examples of ‘learning health systems’ in action.
The EPIS – Exploration, Preparation, Implementation and Sustainment – conceptual model was used to guide our project design, implementation process, evaluation plan (e.g., timing and constructs of interest) and outcomes [35,36]. We are also using the Dynamic Adaptation Process to guide stakeholder-driven adaptations that are contextually responsive over time to inform our SDM approach for bariatric surgery in our healthcare systems (Figure 2) [35]. The process involves identifying the core elements and adaptable characteristics [37] of a SDM approach for bariatric surgery, then supporting SDM implementation in each health system with specific guidance on allowable adaptations that are planned and executed by a site-specific, multi-stakeholder Implementation Resource Team (IRT). The IRT members offer their expertise to prospectively identify multilevel factors of influence (system, organization, provider and consumer) that require implementation strategies, such as provider stigma related to obesity and obesity treatment that may act as a barrier to SDM. Additional implementation strategies will address known barriers to SDM from the published literature (Table 1) using approaches that have been successfully applied in our prior work [29–34].

Figure 2. Conceptual model guiding the Dynamic Adaptation Process to support effective implementation of a shared decision making approach representing the four main phases of the EPIS model: Exploration, Preparation, Implementation and Sustainment.
EBP: Evidence-based programs (such as shared decision making); SDM: Shared decision making.
| Barriers to SDM addressed | Implementation strategy | Description of implementation strategy |
|---|---|---|
| Poor leadership buy-in | Engage formally appointed leaders | Formally appointed leaders identified for KPWA and UPMC; co-developed implementation strategy with leadership input |
| Lack of motivation for SDM | Identify clinical champions for SDM | Clinical champions; bariatric and primary care; nominated by clinical leadership or self-nominated; champions formally trained on SDM with a focus on bariatric surgery |
| Low system engagement | Form Implementation Resource Team | An IRT was formed at each site (KPWA and UPMC) and includes representatives from relevant stakeholders, including patients, surgeons, primary care providers, other organizational leaders |
| Understanding of SDM and bariatric surgery evidence | Train providers on SDM process and skills | Separate online CME programs for primary care providers and surgeons; CME credit offered; content: bariatric surgery evidence, SDM steps, DA overview, tools for implementation, audit & feedback plan |
| SDM not a priority clinically | Mandated participation in SDM | IRT leadership communicate clear expectations to bariatric surgeons that SDM is mandatory; primary care leadership set expectation for use of SDM Approach in conversations about treatment options |
| Unclear who is accountable for SDM happening | Develop workflow | Detailed SDM workflows are develop by IRT and adapted to the local clinical setting (e.g., likely different for surgical vs primary care) |
| Lack of time for SDM | IT support tools | EMR ordering and messaging tools facilitate easy delivery of DAs; we will automate DA delivery at referral to bariatric clinic; smart phrases will document SDM conversations |
| Lack of explicit performance monitoring | Audit and feedback | Public reports track DA use, bariatric referral and procedure volume, as well as SDM documentation with feedback to providers about performance |
| Uneven SDM uptake across providers/staff | Ongoing consultation | Follow-up meetings of IRT with care teams discuss DA use and SDM documentation; provide opportunity for feedback on public report; assess barriers, facilitators; check and adjust |
CME: Continuing medical education; DA: Decision aid; EMR: Electronic medical record; IRT: Implementation resource team; KPWA: Kaiser Permanente Washington; SDM: Shared decision making.
The multi-disciplinary project team includes patients, bariatric surgeons, primary care physicians, implementation scientists and experts in shared decision making. There are three primary areas of stakeholder engagement: Development and refinement of the DA: patients, bariatric surgeons, PCPs, nurses, dieticians and psychologists were engaged in the development of the DA, and feedback from patients, bariatric surgeons, primary care physicians, clinical leaders from KPWA and UPMC, and professional society leaders informed the current version. The implementation plan for our SDM approach was also discussed with the PBS Executive Stakeholder Advisory Group. IRT: at each site, the IRTs include two patient members, as well as bariatric surgeons, bariatric medicine specialists, PCPs, quality leaders and administrators, nurse/care managers, administrators, DA developer, researchers and implementation scientists who drive barrier identification and prioritization and subsequent implementation strategy selection and deployment. Executive Stakeholder Advisory Group: modeled after the PBS project, an Executive Stakeholder Advisory Group comprising a diverse, national group of patients, surgeon leaders from the American Society of Metabolic and Bariatric Surgeons, primary care clinicians and leaders of the Obesity Action Coalition advises the IRT on the SDM approach and the revised DA, and will help interpret results.
The proposed SDM strategy will address two preference-sensitive decisions for patients with severe obesity: first, whether or not to undergo bariatric surgery and second, which bariatric procedure to undergo [25]. These preference-sensitive decisions require patients to consider important short- and long-term trade-off in risks and benefits as they decide between bariatric surgery or no surgery (e.g., risk of surgical complications vs long-term chance of weight loss), and the decision about which bariatric procedure to undergo is driven both by patient preferences and other factors (e.g., surgeon preferences, insurance coverage) [38].
Consistent with our prior SDM implementation work at KPWA involving more than a dozen preference-sensitive decisions in six specialty areas (orthopedics, gynecology, urology, neurosurgery, general surgery and cardiology; >50,000 DAs delivered since 2009; >4000 DAs annually) [31–34], the proposed SDM approach has four core components: first, identification of eligible patients, second, delivery of an evidence-based patient DA, third, a structured SDM conversation and fourth, documentation of the SDM conversation in the electronic medical record. Briefly, patients with severe obesity who are eligible for SDM will be identified by their PCPs (or other clinic staff such as medical assistants or nurses) during routine visits or at the point of referral to the bariatric surgeon. Eligible patients will receive the DA, which will be ordered through the electronic medical record at both sites and delivered as a hard copy DVD (with booklet) or viewed online. Patients will be asked to review the DA prior to their next visit, at which the provider will engage the patient in a SDM conversation and document the SDM conversation in the medical record. PCPs conversations will focus primarily on whether the patient is interested enough in bariatric surgery to be referred to the surgeon. The surgical SDM conversations will address whether to have surgery, and if so, which procedure to undergo.
We expect that the implementation of the PBS results and our SDM approach will improve healthcare and outcomes primarily through higher quality decision making. Specifically, patients with severe obesity will report that their providers helped them better understand their options including the risks and benefits, inquired about their preferences, and took their preferences into account when choosing what to do next. Providers will also be more knowledgeable about the available options, feel more confident in their ability to discuss these options with patients, and feel more confident in their patients’ decisions. In terms of decision making, we expect to learn whether the improved dissemination of evidence about the efficacy and safety of bariatric surgery results in changes in the rate of referral to bariatric surgery and the rate of uptake of bariatric surgery among eligible patients (which is currently ∼1% of eligible patients). We expect referrals to bariatric surgery programs and volume of surgery may increase; however, the expected magnitude of the increase is unclear and will be driven by informed patient preferences.
Central to the PBS results, which compare the effectiveness and safety of bariatric procedures, we also expect to learn whether this SDM approach influences decision making about the type of bariatric procedure patients choose to undergo. Currently, many patients in our health systems choose the SG procedure; however, the PBS evidence for the SG is mixed, showing better safety, but less weight loss and less durable improvements in diabetes compared with RYGB. It is unclear whether the proportion of patients choosing SG, RYGB and AGB will change with improved SDM, but our study is well-positioned to track any shifts in procedure choice.
We believe that this SDM approach will be broadly generalizable and scalable for use in other settings. Our stakeholder engagement strategy will also help to ensure that other major professional groups and healthcare organizations can disseminate this SDM approach. It is our hope that implementation of this SDM approach will help to more rapidly translate comparative effectiveness research into clinical practice and improve the quality of decision making around bariatric surgery.
Acknowledgments
The views, statements and opinions presented in this editorial are solely the responsibility of the author(s) and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute® (PCORI®), its Board of Governors or Methodology Committee.
Financial & competing interests disclosure
Research reported in this editorial was funded through two Patient-Centered Outcomes Research Institute® (PCORI®) Awards (SDM-2018C2-13368 and OBS-1505-30683). A Courcoulas reported receiving grants from Allurion Technologies outside the submitted work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
1.
Morris ZS, Wooding S, Grant J. The answer is 17 years, what is the question: understanding time lags in translational research. J. Royal Soc. Med. 104(12), 510–520 (2011).
2.
Selby JV, Forsythe L, Sox HC. Stakeholder-driven comparative effectiveness research: an update from PCORI. JAMA 314(21), 2235–2236 (2015).
3.
Slutsky J, Sheridan S, Selby J. Getting engaged. J. Gen. Intern. Med. 29(12), 1582–1583 (2014).
4.
Leclair AM, Kotzias V, Garlick J et al. Facilitating stakeholder engagement in early stage translational research. PLoS ONE 15(7), e0235400 (2020).
5.
Stallings SC, Boyer AP, Joosten YA et al. A taxonomy of impacts on clinical and translational research from community stakeholder engagement. Health Expect. 22(4), 731–742 (2019).
6.
Forsythe LP, Ellis LE, Edmundson L et al. Patient and stakeholder engagement in the pcori pilot projects: description and lessons learned. J. Gen. Intern. Med. 31(1), 13–21 (2016).
7.
Ogden CL, Carroll MD, Fryar CD, Flegal KM. Prevalence of obesity among adults and youth: United States, 2011-2014. NCHS Data Brief 219, 1–8 (2015).
8.
Arterburn DE, Mcdonell MB, Hedrick SC, Diehr P, Fihn SD. Association of body weight with condition-specific quality of life in male veterans. Am. J. Med. 117(10), 738–746 (2004).
9.
Mctigue K, Larson JC, Valoski A et al. Mortality and cardiac and vascular outcomes in extremely obese women. JAMA 296(1), 79–86 (2006).
10.
Sarkhosh K, Switzer NJ, El-Hadi M, Birch DW, Shi X, Karmali S. The impact of bariatric surgery on obstructive sleep apnea: a systematic review. Obes. Surg. 23(3), 414–423 (2013).
11.
Buchwald H, Estok R, Fahrbach K et al. Weight and Type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am. J. Med. 122(3), 248–256 (2009).
12.
Maggard MA, Shugarman LR, Suttorp M et al. Meta-analysis: surgical treatment of obesity. Ann. Intern. Med. 142(7), 547–559 (2005).
13.
Buchwald H, Avidor Y, Braunwald E et al. Bariatric surgery: a systematic review and meta-analysis. JAMA 292(14), 1724–1737 (2004).
14.
Gloy VL, Briel M, Bhatt DL et al. Bariatric surgery versus non-surgical treatment for obesity: a systematic review and meta-analysis of randomised controlled trials. BMJ 347, f5934 (2013).
15.
Puzziferri N, Roshek TB 3rd, Mayo HG, Gallagher R, Belle SH, Livingston EH. Long-term follow-up after bariatric surgery: a systematic review. JAMA 312(9), 934–942 (2014).
16.
Campos GM, Khoraki J, Browning MG, Pessoa BM, Mazzini GS, Wolfe L. Changes in utilization of bariatric surgery in the United States from 1993 to 2016. Ann. Surg. 271(2), 201–209 (2020).
17.
Toh S, Rasmussen-Torvik LJ, Harmata EE et al. The National Patient-Centered Clinical Research Network (PCORnet) Bariatric Study Cohort: rationale, methods, and baseline characteristics. JMIR Res. Protoc. 6(12), e222 (2017).
18.
Inge TH, Coley RY, Bazzano LA et al. Comparative effectiveness of bariatric procedures among adolescents: the PCORnet Bariatric Study. Surg. Obes. Relat. Dis. 14(9), 1374–1386 (2018).
19.
Arterburn D, Wellman R, Emiliano A et al. Comparative effectiveness and safety of bariatric procedures for weight loss: a PCORnet cohort study. Ann. Intern. Med. 169(11), 741–750 (2018).
20.
Courcoulas A, Coley RY, Clark JM et al. Interventions and operations 5 years after bariatric surgery in a cohort from the US National Patient-Centered Clinical Research Network Bariatric Study. JAMA Surg. 155(3), 194–204 (2020).
21.
Mctigue KM, Wellman R, Nauman E et al. Comparing the 5-Year diabetes outcomes of sleeve gastrectomy and gastric bypass: the National Patient-Centered Clinical Research Network (PCORNet) Bariatric Study. JAMA Surg. (2020) (Epub ahead of print).
22.
Still CD. Creating bariatric surgery advocates: why it is critical to educate primary care physicians. Bariatric Times 8(11), 16–18 (2011).
23.
Reames BN, Birkmeyer NJ, Dimick JB et al. Variation in the care of surgical conditions: obesity. A Dartmouth Atlas of Health Care Series (2014). www.dartmouthatlas.org/downloads/atlases/Surgical_Atlas_2014.pdf
24.
Macht R, Rosen A, Horn G, Carmine B, Hess D. An exploration of system-level factors and the geographic variation in bariatric surgery utilization. Obes. Surg. 26(7), 1635–1638 (2016).
25.
Weinstein AL, Marascalchi BJ, Spiegel MA, Saunders JK, Fagerlin A, Parikh M. Patient preferences and bariatric surgery procedure selection; the need for shared decision-making. Obes. Surg. 24(11), 1933–1939 (2014).
26.
Jensen MD, Ryan DH, Apovian CM et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 129(25 Suppl. 2), S102–S138 (2014).
27.
PCORI the Patient-Centered Outcomes Research Institute. PCORI funding announcement: implementation of effective shared decision-making (SDM) approaches in practice settings. (2020). www.pcori.org/sites/default/files/PCORI-PFA-2018-Cycle-2-Shared-Decision-Making.pdf
28.
Légaré F, Witteman HO. Shared decision making: examining key elements and barriers to adoption into routine clinical practice. Health Aff. (Millwood) 32(2), 276–284 (2013).
29.
Arterburn DE, Westbrook EO, Bogart TA, Sepucha KR, Bock SN, Weppner WG. Randomized trial of a video-based patient decision aid for bariatric surgery. Obesity (Silver Spring) 19(8), 1669–1675 (2011).
30.
Arterburn D, Westbrook EO, Hsu C. Case study: the shared decision making story at group health. In: Shared Decision Making in Health Care. Elwyn G, Edwards A, Thompson R (Eds).Oxford University Press, UK 190–196 (2016).
31.
Arterburn D, Wellman R, Westbrook E et al. Introducing decision aids at Group Health was linked to sharply lower hip and knee surgery rates and costs. Health Aff. (Millwood) 31(9), 2094–2104 (2012).
32.
Arterburn D, Wellman R, Westbrook EO et al. Decision aids for benign prostatic hyperplasia and prostate cancer. Am. J. Manag. Care 21(2), e130–e140 (2015).
33.
Hsu C, Liss DT, Frosch DL, Westbrook EO, Arterburn D. Exploring provider reactions to decision aid distribution and shared decision making: lessons from two specialties. Med. Decis. Making 37(1), 113–126 (2017).
34.
Hsu C, Liss DT, Westbrook EO, Arterburn D. Incorporating patient decision aids into standard clinical practice in an integrated delivery system. Med. Decis. Making 33(1), 85–97 (2013).
35.
Aarons GA, Green AE, Palinkas LA et al. Dynamic adaptation process to implement an evidence-based child maltreatment intervention. Implement. Sci. 7, 32 (2012).
36.
Becan JE, Bartkowski JP, Knight DK et al. A model for rigorously applying the exploration, preparation, implementation, sustainment (EPIS) framework in the design and measurement of a large scale collaborative multi-site study. Health Justice 6(1), 9 (2018).
37.
Chambers DA, Glasgow RE, Stange KC. The dynamic sustainability framework: addressing the paradox of sustainment amid ongoing change. Implement. Sci. 8, 117 (2013).
38.
Opozda M, Wittert G, Chur-Hansen A. Patients' reasons for and against undergoing Roux-en-Y gastric bypass, adjustable gastric banding, and vertical sleeve gastrectomy. Surg. Obes. Relat. Dis. 13(11), 1887–1896 (2017).
Information & Authors
Information
Published In
Pages: 1035 - 1041
PubMed: 33000638
Copyright
© 2020 Future Medicine Ltd.
History
Received: 27 July 2020
Accepted: 30 July 2020
Published online: 1 October 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Translating stakeholder-driven comparative effectiveness research into practice: the PCORnet Bariatric Study. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0156
Export citation
Select the citation format you wish to export for this article or chapter.