Cost-minimization analysis of negative pressure wound therapy technologies for the treatment of moderate-to-severe foot infections
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The objective was to estimate the cost of care associated with two negative pressure wound therapy (NPWT) technologies used to treat patients admitted to the hospital with moderate-to-severe foot infections. Materials & methods: A decision tree simulation model was developed to estimate the hospital costs associated with two different NPWT technologies: Cardinal Health™ PRO (NPWT-C) and V.A.C. ULTA™ (NPWT-K). Clinical data were obtained from a previously completed single-site prospective trial. One-way and probabilistic sensitivity analyses were performed to gauge the robustness of the results. Results: The total expected per-patient costs were US$41,206 (SD: US$8,194) for NPWT-C and US$44,439 (SD: US$8,963) for NPWT-K. Conclusion: This study found that NPWT-C was expected to minimize the total costs over the episode of treatment. Larger and more clinically diverse studies are recommended to confirm these findings.
Negative pressure wound therapy (NPWT) has dramatically changed the care of complex foot wounds. Compared with standard wound care, patients with diabetic foot wounds treated with NPWT are 5.9-times more likely to heal and 4.4-times less likely to require amputation [1,2]. NPWT is performed by delivering subatmospheric pressure through a vacuum pump connected to a specialized dressing that maintains a closed environment. NPWT increases perfusion to the wound, accelerates granulation tissue formation, reduces edema and reduces bioburden [1–3].
The USA spends more than US$33 billion annually on chronic wound treatment, including diabetic foot ulcers [4]. Health economic studies have found NPWT to be a cost-effective and cost-saving treatment in several clinical contexts; however, the impact of variations in operational costs associated with different NPWT systems on the total treatment cost is not well understood [5–8].
A recently published study (conducted by authors KED and LAL) that compared the efficacy of NPWT systems when treating patients admitted to hospital with moderate and severe foot infections found no significant differences in clinical outcomes or adverse events among the NPWT technologies [9]. Given equivalent clinical performance, providers should also consider the total cost of care for the course of treatment. Unlike many acute in-patient procedures, a single episode of chronic wound treatment with NPWT may span weeks or months, which may result in capital and disposable costs being more pronounced in the total cost of care. Pricing for commercially available NPWT components varies greatly across brands and may be heavily influenced by contractual relationships (e.g., group purchasing organization membership) [10]. Therefore, the secondary aim of the study was to estimate the total cost associated with each NPWT brand for patients admitted to the hospital with moderate to severe foot infections over the episode of care from the health system perspective. The NWPT with saline irrigation treatment arm was excluded from the analysis because there was not a statistically significant difference in clinical outcomes and data for other automated irrigation products were not collected for comparison.
Materials & methods
A cost-minimization analysis (CMA) was performed to estimate the expected episodic costs of treating moderate to severe foot infections with two different NPWT systems: NPWT-C (Cardinal Health™ PRO, OH, USA) and NPWT-K (KCI V.A.C. ULTA™, TX, USA). A CMA was chosen because the outcomes of the NPWT systems were similar and there were no significant differences in health-related quality of life [9]. A decision tree simulation model was developed to estimate the expected costs for each system. This method was chosen due to the short time horizon, population-level analysis and nature of the outcomes [11].
The model followed a hypothetical patient across the episode of care from initiation of NPWT to the conclusion of a 12-week evaluation period. A visual representation of the decision model is shown in Figure 1. The clinical utilization of interest were: duration of NPWT, length of stay (LOS), time to heal, incision and drainage procedure, antibiotic usage and amputation (foot and leg). All modeling was performed using TreeAge Pro 2019 (TreeAge Software, Inc., MA, USA) and validated using Microsoft Excel 2016 (Microsoft, Inc., WA, USA). All analysis were performed with publicly available data. Therefore, this study was exempt from institutional board review board approval.
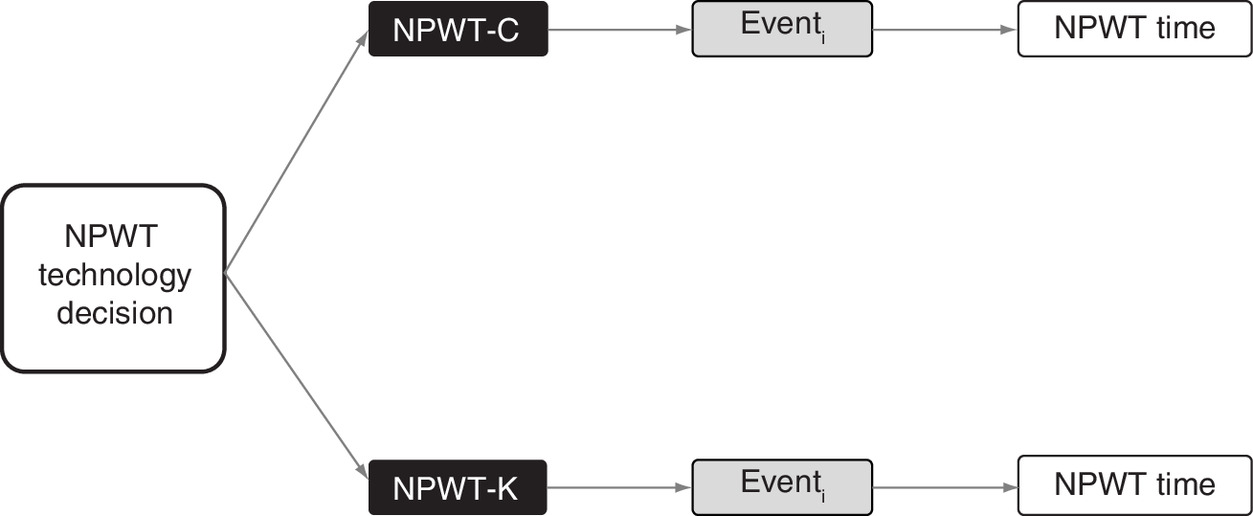
Figure 1. Model diagram.
Event: Utilization Event Rate for parameter i * Cost of i; summed for all events.
NPWT-C: Negative pressure wound therapy Cardinal PRO; NPWT-K: Negative pressure wound therapy KCI VAC ULTA; NPWT-CI: Negative pressure wound therapy Cardinal, PRO with saline irrigation.
Data
Clinical utilization parameters were populated based on a single-site, prospective randomized clinical trial previously published [9]. The study randomized a total of 90 patients in a 1:1:1 ratio across three treatment arms between April 2016 and January 2018. The saline irrigation arm was not modeled in this analysis because it incorporates additional components and data for an equivalent system from alternate manufacturers were not collected. There were no differences in patient characteristics, wound etiology or comorbidities with the exception of race, chronic kidney disease and wound etiology. Similarly, there were no differences in healed wounds, the primary outcome or secondary outcomes including: wound closure, number of surgeries, healed at end of study (12 weeks) and time to heal. The time to heal was reported in days for all study participants who had complete epithelialization with no drainage at end of study follow-up. Additional adverse events including reinfection, hospital readmission and wound dehiscence were similar between the cohorts [9]. The reported average or proportion and 95% CI were used in the model and are shown in Table 1.
| Parameter | NPWT-C | NPWT-K | ||||
|---|---|---|---|---|---|---|
| Base | Low | High | Base | Low | High | |
| NPWT duration, hours | 109.9 | 70.7 | 148.8 | 134.1 | 97.9 | 170.2 |
| Length of stay, index admission | 14.7 | 11.9 | 17.5 | 15.3 | 11.4 | 19.2 |
| Time to heal, days | 40.9 | 30.5 | 51.3 | 45.5 | 27.7 | 63.3 |
| Incision and drainage procedure | 6.7 | 5.0 | 8.4 | 13.3 | 10.0 | 16.6 |
| Amputation foot, % | 13.3 | 10.0 | 16.6 | 3.3 | 0 | 4.1 |
| Amputation leg, % | 0 | 0 | 3.3 | 3.3 | 0 | 4.1 |
| Antibiotic days | 22.4 | 16.26 | 28.6 | 30.2 | 20.9 | 39.5 |
†
Clinical utilization data obtained from Davis et al. (2020) [9].
NPWT: Negative pressure wound therapy.
The cost data was obtained from a ‘best evidence’ literature review. The literature review evaluated published data based on the applicability to the parameter definition, recency of the data and quality of the study. The midpoint of the identified values from the literature was used as the base value when multiple studies were identified (Table 2). All cost data were adjusted to 2018 US dollars using the medical care inflation rate from the US Bureau of Labor Statistics [12].
| Parameter | NPWT-C | NPWT-K | Ref. | ||||
|---|---|---|---|---|---|---|---|
| Base | Low | High | Base | Low | High | ||
| Technology specific parameters† | |||||||
| NPWT/h | US$1.75 | US$1.32 | US$2.19 | US$2.69 | US$2.01 | US$3.36 | [13] |
| Canister | US$13 | US$10 | US$16 | US$38 | US$29 | US$48 | [13] |
| Initial dressing | US$28 | US$21 | US$35 | US$43 | US$32 | US$54 | [13] |
| Common parameters | |||||||
| Ward/day | US$2,502 | US$1,091 | US$3,670 | [14–17] | |||
| Incision and drainage | US$344 | US$258 | US$430 | [18,19] | |||
| Amputation below knee | US$14,934 | US$14,774 | US$15,094 | [20,21] | |||
| Amputation above knee | US$18,698 | US$17,045 | US$20,753 | [20–22] | |||
| Antibiotic/day‡ | US$1.63 | US$1.22 | US$2.04 | [23] | |||
†
NPWT cost parameters were published Veterans Affairs pricing obtained from the United States General Services (GSA).
‡
Clindamycin 300 mg 3x/day self-administered.
NPWT-C: Negative pressure wound therapy Cardinal PRO; NPWT-K: Negative pressure wound therapy KCI VAC Ulta.
Assumptions
Several assumptions were made and applied equally to the treatment arms. The NPWT cost was obtained from the Veterans Affairs published pricing schedules. All patients were assumed to receive one dressing and canister upon NPWT initiation and one dressing kit every 2 days until surgical closure. Patients requiring incision and drainage were assumed to have this procedure performed in an office setting. Daily antibiotic usage was assumed to be clindamycin 300 mg three-times per day self-administered.
Sensitivity analysis
One-way deterministic and probabilistic sensitivity analyses were performed to assess the uncertainty of the parameter values and gauge the reliability and generalizability of the results [13]. The one-way sensitivity analysis varied each model parameter individually to determine which, if any, parameters would cause the primary finding to change. The probabilistic sensitivity analysis evaluated first- and second-order uncertainty by running 1,000,000 trials. Clinical utilization data were varied within the 95% CI of the base value. Cost data were varied by ± 25% of the base value. The low and high values are shown in (Tables 1 & 2). The sampled distributions were assumed to follow a triangle and gamma distribution for clinical utilization and cost data, respectively. The probabilistic sensitivity analysis was used to estimate the proportion of simulated trials for which NPWT-C or NPWT-K was the cost-saving strategy.
Results
The average expected costs of the episode of care were US$41,206 (standard deviation: US$8,194) and US$44,439 (US$8,963) for NPWT-C and NPWT-K, respectively, for the treatment of moderate to severe foot infections. Therefore, NPWT-C demonstrated a cost savings of US$3,233 per patient treated. Table 3 illustrates the results of the probabilistic sensitivity analysis. The minimum expected cost of care was US$20,036 and US$20,876 (difference US$840) for NPWT-C and NPWT-K, respectively. The maximum expected cost over the episode of care was US$67,460 and US$74,103 (difference US$6,643) for NPWT-C and NPWT-K, respectively. The proportion of trials with NPWT-C as the cost-saving strategy was 74% (Figure 2). The one-way sensitivity analysis revealed that LOS was the only parameter which would cause NPWT-C to not be the cost-saving strategy. An increase in the LOS for NPWT-C of 2 days or a decrease in LOS for NPWT-K of 2 days resulted in NPWT-K becoming the cost-saving technology.
| Results | NPWT-C | NPWT-K |
|---|---|---|
| Mean | US$41,206 | US$44,439 |
| Standard deviation | US$8194 | US$8963 |
| Minimum | US$20,036 | US$20,876 |
| 10th percentile | US$30,251 | US$32,632 |
| 50th percentile | US$41,302 | US$44,263 |
| 90th percentile | US$51,946 | US$56,112 |
| Maximum | US$67,460 | US$74,103 |
Results are based on 1 million trials of hypothetical patients through the model.
NPWT-C: Negative pressure wound therapy Cardinal PRO; NPWT-K: Negative pressure wound therapy KCI VAC ULTA.
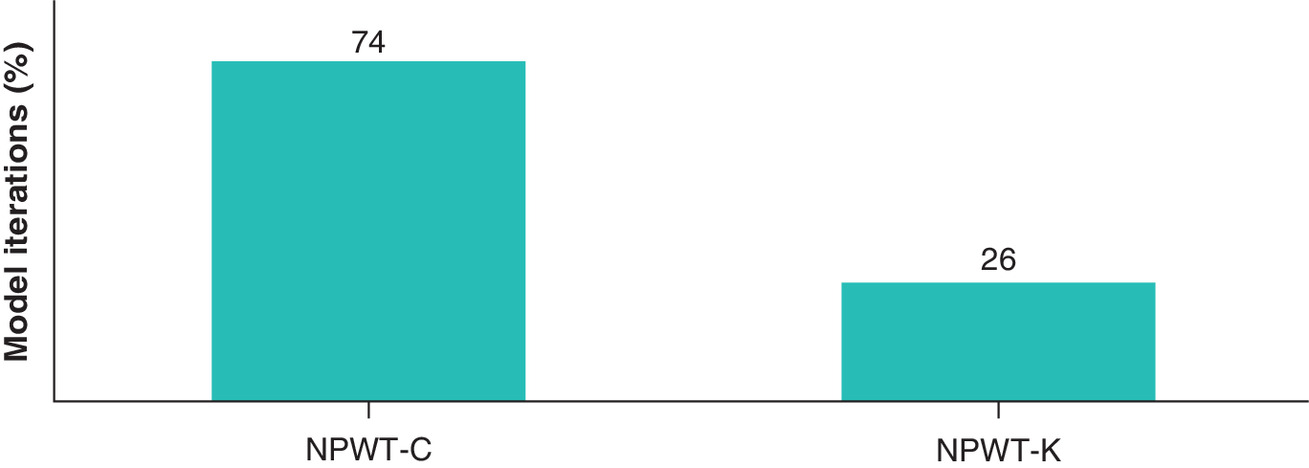
Figure 2. Probabilistic sensitivity results.
NPWT-C was found to be the cost saving technology 74% of the time when compared with NPWT-K after 1 million trials in the Monte Carlo simulation.
NPWT-C: Negative pressure wound therapy Cardinal PRO; NPWT-K: Negative pressure wound therapy KCI VAC ULTA.
Discussion
Limited evidence is available with regard to the cost–effectiveness of NPWT technologies. In capitated payment models such as the acute inpatient, long-term care hospital, and the skilled nursing facility prospective payment systems, such evidence is necessary to maximize the value of an intervention to the patient and provider. The Centers for Medicare and Medicaid Services expects annual price growth between 2.0 and 2.7% while hospital spending is expected to grow nearly 6% per year through 2027 [24]. This discrepancy in expected growth rates will likely place further strain on provider budgets.
It is incumbent upon providers operating under a capitated payment system to continually evaluate the clinical effectiveness and economic effect for any treatment paradigm. The results of our study found that NPWT-C was the cost-minimizing technology with an average expected savings of US$3,233 per patient. Driving these results was a prospective study showing the two technologies, NPWT-C and NPWT-K, have similar clinical outcomes and utilization [9].
Prior clinical studies support the need for robust prospective head to head trials comparing different treatment modalities and techniques in wound care [1,2,25,26]. Combined with the recent prospective study that the results of our economic analysis are based upon, NPWT as a modality is a promising treatment for diabetic foot ulcers [9]. However, there is still uncertainty regarding the optimal devices, pressure, irrigation, dressings and timing. The incorporation of future economic analyses into head-to-head trials may provide the foundational knowledge for clinicians and economic stakeholders to improve decision making.
An examination of the economic parameters that resulted in NPWT-C to be the cost-saving technology showed that LOS, NPWT rental fee and supply costs to have the largest effect in the simulation model. The LOS stay may depend on other unobserved factors, leaving the principal parameters of the NPWT technology and its supplies under the provider’s control. Based on publicly available pricing, NPWT-C was 35% less expensive than NWPT-K, while demonstrating similar clinical and utilization outcomes. In a budget constrained environment, value to the provider and patient can be achieved by choosing the lowest cost option, which provides similar or better clinical outcomes.
Study limitations
The clinical data used in this study are derived from the analysis of the results from a randomized single-site experience. Other health systems may have a different experience based on their own protocols and caution should be taken before generalizing these findings. These data were used because published data from a multi-center or randomized comparative study were not available. However, this study does provide a framework for other health systems to conduct a similar study or a larger multi-site prospective study. Moreover, this study was designed from the perspective of a US health system. Consequently, the findings of this study are likely not generalizable to other countries. Second, data for all relevant parameters may not be available to be included in this CMA. Third, NPWT supply costs were obtained from publicly available US Department of Veterans Affairs price lists. Negotiated prices in other settings may reflect higher component costs and/or a larger proportional difference in system costs. Finally, this study was an investigator-initiated study funded by one of the manufacturers, though the manufacturer did not have any control of the study design or publication of the results.
Conclusion
This study found that NPWT-C was expected to minimize the total costs over the episode of treatment in patients requiring NPWT therapy for moderate to severe foot infections. The findings must be taken in context of the same sample size of the clinical study. Further research is recommended to confirm these findings.
•
Diabetic foot ulcers (DFUs) are a difficult to treat condition with a number of confounding issues faced by clinicians.
•
Negative pressure wound therapy (NPWT) has shown tremendous promise in the treatment of DFUs.
•
There are several commonly employed NPWT devices on the market.
•
Despite substantial differences in cost, it is not clear if there are differences in clinical or economic outcomes with the use of different NPWT devices.
•
A recent head to head conducted at a single site (Davis et al. 2020) compared two different devices and found similar outcomes.
•
This study relied on those results to examine the economic outcomes associated with the use of different NPWT devices for DFUs.
•
Our study found the Cardinal Health™ PRO was the cost-minimizing device compared with KCI V.A.C. ULTA™.
•
Caution should be taken when generalizing these findings due to sample size and single-site of the clinical study relied upon.
Author contributions
PJ Mallow, LA Lavery and KE Davis conceptualized the study design, conducted the analysis, interpreted the results. J Tepsick conducted the analysis and interpreted the results. All authors have contributed substantially to the final version of the manuscript and have approved it in its final form.
Financial & competing interests disclosure
This study received financial support for this research from Cardinal Health, Inc. PJ Mallow is a consultant to Cardinal Health, Inc. KE Davis and LA Lavery have received investigator-initiated grant funding from Cardinal Health, Inc. J Tepsick has no disclosures. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
All data generated or analyzed during this study are available upon request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Armstrong DG, Lavery LA. Negative pressure wound after partial diabetic foot amputation: a multicentre, randomised controlled trial. Lancet 66, 1704–1710 (2005).
2.
Blume PA, Walters J, Payne W, Ayala J, Lantis J. Comparison of negative pressure wound therapy using vacuum-assisted closure with advanced moist wound therapy in the treatment of diabetic foot ulcers: a multicenter randomized controlled trial. Diabetes Care 31(4), 631–636 (2008).
3.
Saxena V, Hwang CW, Huang S, Eichbaum Q, Ingber D, Orgill DP. Vacuum-assisted closure: microdeformations of wounds and cell proliferation. Plast. Reconstr. Surg. 114(5), 1086–1096 (2004).
4.
Rice JB, Desai U, Cummings AK, Birnbaum HG, Skornicki M, Parsons NB. Burden of diabetic foot ulcers for medicare and private insurers. Diabetes Care 37(3), 651–658 (2014).
5.
Philbeck TE, Whittington KT, Millsap MH, Briones RB, Wight DG, Schroeder WJ. The clinical and cost–effectiveness of externally applied negative pressure wound therapy in the treatment of wounds in home healthcare Medicare patients. Ostomy Wound Manage. 45(11), 41–50 (1999).
6.
Apelgvist J, Armstrong DG, Lavery LA, Bouton AJ. Resource utilization and economic costs of care based on a randomized trial of vacuum-assisted closure therapy in the treatment of diabetic foot wounds. Am. J. Surg. 195(6), 782–788 (2008).
7.
Lewis LS, Convery PA, Bolac CS, Valea FA, Lowery WJ, Havrilesky LJ. Cost of care using prophylactic negative pressure wound vacuum on closed laparotomy incisions. Gynecol. Oncol. 132(3), 684–689 (2014).
8.
Yang CK, Alcantara S, Goss S, Lantis JC. Cost analysis of negative-pressure wound therapy with instillation for wound bed preparation preceding split-thickness skin grafts for massive (>100 cm2) chronic venous leg ulcers. J. Vasc. Surg. 61(4), 995–999 (2015).
9.
Davis KE, La Fontaine J, Farrar D et al. Randomized clinical study to compare negative pressure wound therapy with simultaneous saline irrigation and traditional negative pressure wound therapy for complex foot infections. Wound Repair Regen. 28(1), 97–104 (2020).
•• Analysis of negative pressure wound therapy devices from a single site comparing clinical outcomes in diabetic foot ulcer patients.
10.
Rhee SM, Valle MF, Wilson LM, Lazarus G, Zenilman J, Robinson KA. Negative pressure wound therapy technologies for chronic wound care in the home setting. evidence report/technology assessment. Prepared by the Johns Hopkins University Evidence-based Practice Center under contract no. 290-201-200007-I. Agency for Healthcare Research and Quality, MD, USA (2014). www.ahrq.gov
11.
Roberts M, Russell LB, Paltiel AD, Chambers M, McEwan P, Krahn M. Conceptualizing a model: a report of the ISPOR-SMDM modeling good research practices task force 2. Value Health 15(6), 804–811 (2012).
12.
US Department of Labor BoLS. Consumer price index (2019). www.bls.gov/cpi/
13.
US General Services Administration (GSA). Veteran's Affairs Federal Supply Schedule Service (2019). www.gsaadvantage.gov
14.
Kaiser Family Foundation. State health facts: hospital adjusted expenses per inpatient day (2019). www.kff.org
15.
Halpern NA, Goldman DA, Tan KS, Pastores SM. Trends in critical care beds and use among population groups and Medicare and Medicaid beneficiaries in the United States: 2000–2010. Crit. Care Med. 44(8), 1490–1499 (2016).
16.
Bartsch SM, McKinnell JA, Mueller LE et al. Potential economic burden of carbapenem-resistant Enterobacteriaceae (CRE) in the United States. Clin. Microbiol. Infect. 23(1), 48.e9–48.e16 (2017).
17.
Agency for Healthcare Quality and Research. Healthcare cost and utilization project. HCUP fast stats – trends in inpatient days (2019). www.hcup-us.ahrq.gov
18.
Jones JP, Ellis E. Are office-based oral and maxillofacial surgical procedures profitable? A benefit–cost analysis. J. Oral Maxillofac. Surg. 77(11), 2205–2214 (2019).
19.
Centers for Medicare & Medicaid Services (CMS). Physician fee schedule look-up tool (2019). www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PFSlookup
20.
Rinkel WD, Luiten J, van Dongen J et al. In-hospital costs of diabetic foot disease treated by a multidisciplinary foot team. Diabetes Res. Clin. Pract. 132, 68–78 (2017).
21.
Hicks CW, Selvaraja S, Mathioudakis N et al. Burden of infected diabetic foot ulcers on hospital admissions and costs. Ann. Vasc. Surg. 33, 149–158 (2016).
22.
Locham SS, Paracha N, Dakour-Aridi H et al. Comparison of the cost of drug-eluting stents versus bare metal stents in the treatment of critical limb ischemia in the United States. Ann. Vasc. Surg. 55, 55–62 (2019).
23.
Drugs.com. Price guide (2019). www.drugs.com
24.
Centers for Medicare & Medicaid Services (CMS). National health expenditure data (2020). www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/
25.
Lavery LA, Murdoch DP, Kim PJ et al. Negative pressure wound therapy with low pressure and gauze dressing to treat diabetic foot wounds. J. Diabetes Sci. Technol. 8, 346–349 (2014).
26.
Lavery LA, La Fontaine J, Thakral G et al. Randomized clinical trial to compare negative-pressure wound therapy approaches with low and high pressure, silicone coated dressing, and polyurethane foam dressing. Plast. Reconstr. Surg. 133, 722–726 (2014).
Information & Authors
Information
Published In
Pages: 1027 - 1033
PubMed: 33034531
Copyright
© 2020 Peter J Mallow. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 24 June 2020
Accepted: 19 August 2020
Published online: 9 October 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost-minimization analysis of negative pressure wound therapy technologies for the treatment of moderate-to-severe foot infections. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0127
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Allen Gabriel, Economics of NPWT and Its Variants, Negative Pressure Wound Therapy, 10.1007/978-3-032-13326-7_13, (233-243), (2026).
- Luke Paterson, Interpreting economic evaluations of healthcare interventions: A simple guide, Journal of Wound Care, 10.12968/jowc.2024.33.Sup2b.1, 33, Sup2b, (1-8), (2024).
- Burcu Talu, Ibrahim Isik, Busra Candiri, Yunus Candiri, Remziye Betul Yapalıkan, Effects of Sensor Size, Surface Material, and Contact Area on Pressure Measurements in Thin-Film Pressure Sensors, IEEE Sensors Journal, 10.1109/JSEN.2023.3336460, 24, 2, (1591-1597), (2024).