The cost–effectiveness of low-dose budesonide as a Step 2 treatment for pediatric asthma in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the cost–effectiveness of low-dose budesonide versus montelukast among patients aged 1–5 years from a Chinese patient and healthcare payer perspective. Materials & methods: A Markov model based on exacerbation states was developed. Exacerbation was defined as the need for rescue therapy (mild exacerbation) or hoscopitalization (moderate-to-severe exacerbation). Inputs including efficacy (i.e., exacerbation rates), mortality, utilities, costs and treatment adherence were obtained from literature. Results: Compared with montelukast, low-dose budesonide led to fewer exacerbation events (1.44 vs 2.15), lower costs (¥3675 vs 4130) and slightly more quality-adjusted life years (0.974 vs 0.967) over 1 year. Conclusion: These findings may improve the use of low-dose budesonide, an economically and clinically preferable treatment to montelukast in pediatric patients.
Lay abstract
In this study, low-dose budesonide was compared with montelukast as a Step 2 treatment among pediatric patients (aged 1–5 years) for costs and clinical outcomes in China. Over 1 year, patients receiving low-dose budesonide had fewer exacerbation events, incurred lower costs for treatment and exacerbation management and had slightly better quality of life, compared with patients receiving montelukast. The clinical benefits and cost savings suggest that the use of low-dose budesonide may help reduce the burden of persistent pediatric asthma in China.
Asthma is a chronic, heterogeneous respiratory disease that is characterized by lung inflammation and variable expiratory airflow obstruction [1]. Asthma-related symptoms include wheezing, breathlessness, chest tightness and cough [2,3]. Although asthma affects people of all ages, the disease commonly manifests during childhood; according to the Global Initiative for Asthma (GINA), most children experience their first asthma attack (i.e., the initial presentation of asthma) before the age of 6 years [3]. In China, the prevalence of pediatric asthma has been on the rise from 0.9 to 3.0% over the last 30 years [4,5]. The continual rapid industrialization may increase the prevalence of pediatric asthma as children are particularly susceptible to environmental triggers (e.g., pollution, high humidity) [6–8].
Adequate symptom control among patients with asthma is critical to the clinical management of the disease and minimizing the risk of exacerbation and other adverse health outcomes. However, noncompliance to the GINA guidelines has been observed in China, which was associated with uncontrolled disease symptoms, increased exacerbation frequency and compromised patients’ quality of life [9–11]. The 2015 Respiratory Disease Specific Program reported that less than 15% of patients with mild asthma in China were well controlled according to the GINA criteria and treatment intensification with inhaled corticosteroids (ICS) was suggested as an essential strategy to improve patient outcomes [11].
With the increased prevalence of asthma and inadequate symptom control, actions should be taken to ensure effective disease control following the stepwise approach for pharmacotherapy management [12]. In the presence of frequent symptoms, long-term maintenance with low-dose ICS is the preferred front-line treatment option for persistent asthma in pediatric patients according to the GINA guidelines [12]. Treatment guidelines in China also recommend that pediatric patients with mild persistent asthma-related symptoms receive Step 2 maintenance treatment, preferably with low-dose ICS, or alternatively with leukotriene receptor antagonists (LTRA) [13]. Regular use of low-dose ICS or LTRA improves asthma-related symptoms and lung function and decreases the need for additional medication and hospital admission [14,15]. Comparative studies demonstrated the low-dose ICS was associated with clinical benefits compared with LTRA, such as faster improvement in lung function and lower exacerbation rates [16–18].
Despite the demonstrated clinical benefits, the use of ICS remains limited in current real-world clinical practice in China [9–11]. A nationwide survey revealed that, among patients with mild asthma receiving Step 2 treatment, less than one fourth received low-dose ICS while over half received LTRA [11]. The asthma control outcome of these patients was disappointing, with less than 15% achieving asthma control [11]. The observed discrepancy between real-world practice and theoretical guidelines suggested the need of evidence to support informed treatment selection. In informed treatment selection, not only drug acquisition costs, but also disease management costs and clinical outcomes should be considered [19,20]. Therefore, in this study a cost–effectiveness analysis was conducted to compare two guideline-recommended Step 2 maintenance treatments for patients aged 1–5 years old in China with mild persistent asthma: the ICS, low-dose budesonide inhalation suspension, versus the LTRA, montelukast. In the cost–effectiveness analysis, clinical outcomes were balanced against costs to provide evidence to patients and healthcare payers for their treatment selection.
Materials & methods
Model structure
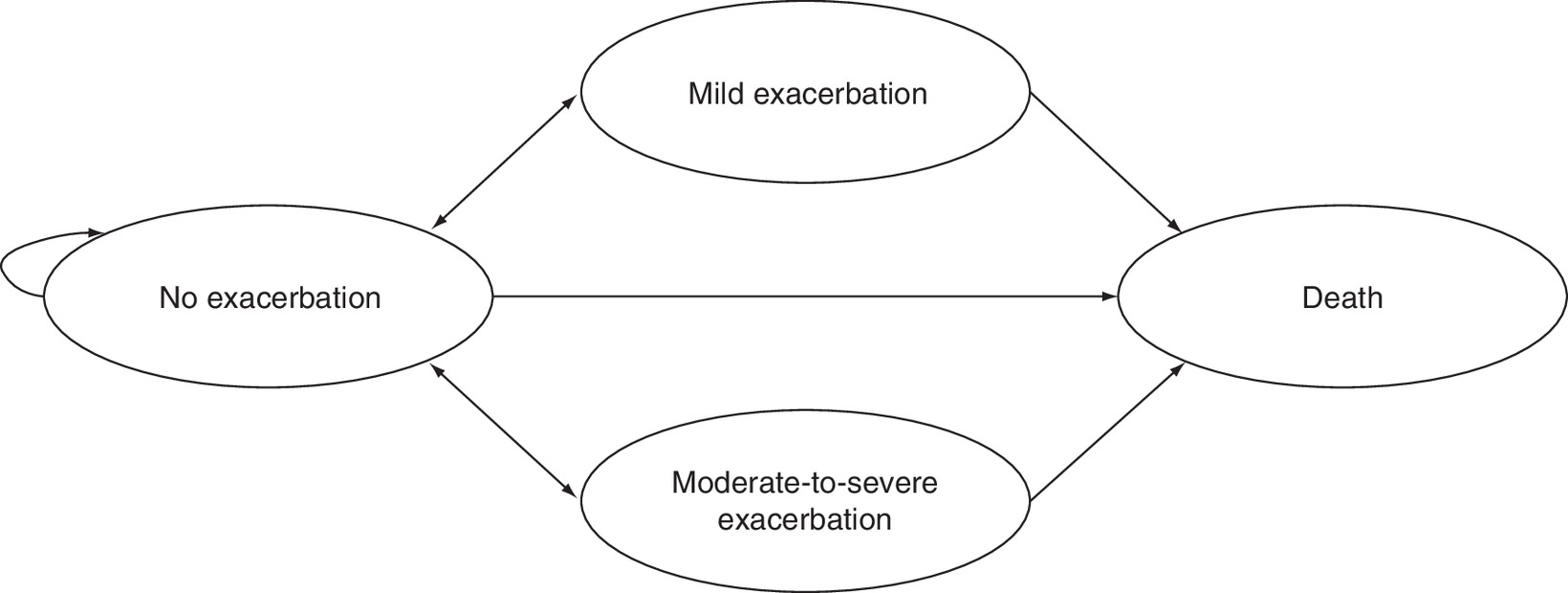
A Markov model was constructed based on the following health states: no exacerbation, mild exacerbation, moderate-to-severe exacerbation and death (Figure 1). Patients aged 1–5 years old with persistent asthma receiving Step 2 maintenance treatment entered the model and all started from the ‘no exacerbation’ state. Patients in the ‘no exacerbation’ state were at risk of exacerbations and the risk of exacerbations would be informed by clinical evidence. Once patients experienced an exacerbation, healthcare resource use (HRU) in addition to maintenance treatment was required. To reflect the extent of HRU for exacerbation events of different severities, mild and moderate-to-severe exacerbations were considered separately as two model states. Mild exacerbation was defined as the need for rescue therapy (e.g., short-acting beta-agonists, oral corticosteroids) in addition to the maintenance therapy and moderate-to-severe exacerbation was defined as the need for an increased dose of rescue therapy in a short period of time (e.g., 6 doses of a short-acting beta-agonist in a 24-hour period) or hospitalization for worsening symptoms [18].
The model compared the cost–effectiveness of low-dose budesonide inhalation suspension, representing guideline-preferred Step 2 maintenance treatment, with montelukast, representing the alternative treatment. A patient and healthcare payer perspective was adopted, with all direct medical costs considered. Early childhood asthma management is of significant clinical importance (e.g., influencing lung function development) and may increase or decrease patients’ disease severity [21]. To capture the outcomes in early childhood asthma management, costs and effectiveness were compared over a 1-year time horizon. Considering the cyclical exacerbation and recovery characteristics of asthma, a 1-week cycle length was used.
The model was validated with a health economics expert (BW) over the course of two in-depth interviews, one during the design and construction of the model and the other prior to finalizing the model.
Model assumptions
The following key assumptions were incorporated into the model:
•
Patients were assumed to receive the maintenance treatment throughout the modeled time horizon, regardless of their exacerbation status.
•
Treatment adherence was considered and assumed to impact both drug costs and exacerbation rates.
•
Patients experiencing exacerbations were assumed to leave the exacerbation state at the end of a model cycle and transition back to the ‘no exacerbation’ state or to death.
Model inputs
Model inputs included efficacy and mortality, utilities, costs and treatment adherence (Table 1). Inputs and assumptions related to clinical practice (i.e., treatment efficacy, proportions of patients hospitalized during exacerbations, costs used in exacerbation management and treatment adherence rates) were verified with a clinical expert (WZ) in an in-depth interview. The implications of adverse events on cost–effectiveness were trivial and therefore not explicitly considered in the model [18].
| Model input | Base case value | Sources and notes | Ref. |
|---|---|---|---|
| Exacerbation rates | |||
| Low-dose budesonide | |||
| – Mild exacerbation | 0.91 | Szefler et al. | [18] |
| – Moderate-to-severe exacerbation | 0.44 | ||
| Montelukast | |||
| – Mild exacerbation | 1.42 | Szefler et al. | [18] |
| – Moderate-to-severe exacerbation | 0.88 | ||
| Case-fatality rate | |||
| – Hospitalized patients | 0.25% | Lin et al. | [22] |
| Hospitalization rate | |||
| – Moderate-to-severe exacerbation | 24.3% | KAP Project Team | [23] |
| Utilities | |||
| – No exacerbation | 0.99 | Rodriguez-Martinez et al. | [24] |
| – Mild exacerbation | 0.71 | ||
| – Moderate-to-severe exacerbation | 0.28 | ||
| Drug and device costs | |||
| – Budesonide per 0.5 mg vial | ¥10.25 | Provincial/municipal drug procurement databases | [25] |
| – Montelukast per 4.0 mg chewable tablet | ¥5.91 | ||
| – Montelukast per 4.0 mg granules | ¥6.73 | ||
| – Nebulizer annual cost | ¥73.78 | Market data | [26] |
| Exacerbation management costs | |||
| – Outpatient visit per event | ¥180.70 | Du et al., Lin et al., Zhou et al. | [22,27,28] |
| – Hospitalization per event | ¥9044.75 | ||
| Treatment adherence rates | |||
| – Budesonide | 62.3% | Hu et al., expert opinion | [29] |
| – Montelukast | 85.0% | ||
Efficacy & mortality
A targeted literature review identified a randomized clinical trial comparing low-dose budesonide inhalation suspension versus montelukast in children with mild persistent asthma within the age range of interest [18]. This trial followed patients for 1 year to compare their asthma exacerbation outcomes; in this trial, exacerbation events were categorized into two severity levels based on the need for HRU, which corresponded to the defined model states [18]. The exacerbation rates obtained from this trial were used to estimate the transition probabilities from no exacerbation to each severity of exacerbations in the model.
For the risk of death, a case-fatality rate for hospitalized patients with asthma were identified from a nationwide survey in China [22]. No additional risk of death was found for patients who were not hospitalized and therefore the natural mortality rate was applied [30]. The case-fatality rate and natural mortality rate were used to estimate the transition probabilities from all other states to death.
Utilities
No utility values for Chinese patients with asthma were identified from a literature review. However, a Colombian utility valuation study was found [24]. This study used the standard gamble methodology to elicitate utility values for pediatric patients with persistent asthma. Three health states were measured in the study, and based on the description of HRU in each state, the utility values could be mapped to no exacerbation, and mild and moderate-to-severe exacerbation states in the model. Because of the availability of utility values, the consistency in study population and the relatively similar socioeconomic development status between China and Colombia, utility values from the Colombian study were considered appropriate for the model and therefore used in the base case.
Utility values for children with stable asthma were also assessed in several other studies, but none of them reported the utility changes during exacerbations [31–35]. Another study provided disutility values associated with exacerbations in an adult population [36]. These values were used as alternative utility values in the model and were tested in the sensitivity analyses.
Costs
Because of the patient and payer perspective, all direct medical costs were considered in the model. These included drug costs, inhalation delivery device costs and exacerbation management costs. All cost inputs were inflation-adjusted to 2018 Chinese Yuan (¥) using the medical care component of the Consumer Price Index [37].
Drug unit costs were obtained from the drug procurement database [25]. Montelukast had brand name and generic versions, and dosage forms of chewable tablets and granules. In the base case, the brand name drug cost was used and patients were assumed to receive chewable tablets and granules in a 50–50% split. Budesonide had two package sizes of 1.0 and 0.5 mg per vial. In patients receiving low-dose budesonide, 0.5 mg per vial is often used to avoid drug wastage. Doses and dosing frequencies were obtained from China’s National Medical Product Administration drug labels [38]. Per the approved labels, budesonide inhalation suspension was administered as 0.25 mg twice daily and montelukast was administered as 4 mg once daily.
In addition to drug costs, patients on budesonide also incurred inhalation delivery device costs. The inhalation delivery device costs were calculated as the average of devices at different costs weighted by their market shares while accounting for the product life cycle and were applied to the model [26].
Exacerbation management costs consisted of costs associated with rescue therapies and medical exams received during unscheduled hospital visits due to exacerbations [18]. In collecting the model inputs, the lump-sum costs for exacerbation management in outpatient and inpatient settings were identified using two China studies [22,27]. Generally, patients with mild exacerbations were managed in an outpatient setting, and thus the corresponding lump-sum cost was applied; patients with moderate-to-severe exacerbations may be hospitalized and the proportion from a nationwide survey among children with asthma was used to calculate the weighted average cost applied in the model [23]. According to the clinical expert (WZ), the practice in managing moderate-to-severe exacerbations varied substantially across different regions in China. To evaluate the impact of the variation, a range of proportions for hospitalization were tested in the sensitivity analyses.
Treatment adherence
Nonadherence to treatment is a common obstacle in disease management, particularly among pediatric patients with asthma [39]. To account for nonadherence, an adherence rate of the proportion of the actual dose consumed out of the expected dose was applied to estimate actual drug costs. Nonadherence to treatment may also compromise treatment efficacy, therefore a hazard ratio suggesting a 12% increased exacerbation rate for every 25% reduction in treatment adherence was also applied [40].
The adherence rate for budesonide was based on a Chinese study [29]. In this study, pediatric patients received ICS over 1 year and the actual amount of ICS administered out of the total amount of ICS prescribed during the period was estimated as the adherence rate (62.3%). To account for the uncertainties, the adherence rate of low-dose budesonide was varied from 22 to 63% in sensitivity analyses, based on data from different populations reported in a systematic review [41]. The good treatment adherence profile of montelukast has been demonstrated in various real-world studies [42–44], but the exact adherence rate was not available. Since 85% is a cutoff value for good adherence as per a local Chinese study in pediatric patients with asthma [29], it was applied to montelukast in the base case and varied by 25% (capped by 100%) to reflect the potential variation in patients.
Model outputs
Model outputs included total costs and total effectiveness including the number of exacerbation events and quality-adjusted life years (QALYs). QALYs are estimated as a function of the length of life and the quality of life (measured with utility values) [45].
Sensitivity analyses
Sensitivity analyses were performed to assess the robustness of the model. In the deterministic sensitivity analysis (DSA), one model input or scenario varied while others were held at the base case value. The variation of model inputs was either based on 95% CI obtained from the literature [40] or increasing and decreasing the values by 25%. The scenarios included the drug unit costs of montelukast based on generic drugs (chewable tablets: ¥4.43, granules: ¥6.77) [25]; varying the hospitalization rate during moderate-to-severe exacerbations from 5 to 50% to reflect the regional variation across China and utility values based on alternative data sources (utility for no exacerbation: 0.70 to 0.96, disutility for mild exacerbation: -0.10, disutility for moderate-to-severe exacerbation: -0.20) [31–36].
In the probabilistic sensitivity analysis, key model inputs were varied simultaneously, with input values randomly drawn from prespecified distributions. A beta distribution was assumed for transition probabilities and utilities and a gamma distribution and log-normal distribution for costs and the hazard ratio, respectively. A Monte-Carlo simulation with 1000 iterations was carried out. The simulated incremental cost–effectiveness ratios (ICERs) were compared with the willingness-to-pay threshold in China to estimate the probability of low-dose budesonide being cost-effective in China. An ICER between 1–3-times a country’s annual GDP per capita is defined as cost-effective while an ICER below a country’s annual GDP per capita is considered to be highly cost-effective [46,47]. The GDP per capita from 2018 was applied (¥64,644) [48].
Results
Base case analysis
Over 1 year, patients receiving low-dose budesonide were expected to have 1.44 exacerbation events (mild: 0.97 events, moderate-to-severe: 0.47 events) and to incur a total of ¥3,675. Of the total costs, 65.2% of costs were attributed to the drug and inhalation device and 34.8% to exacerbation management. Comparatively, patients receiving montelukast were expected to have 2.15 exacerbation events (mild: 1.32 events, moderate-to-severe: 1.83 events) and to incur a total of ¥4,130. Drug costs contributed to 47.5% of the total costs and exacerbation management contributed to the remaining 52.5%. Low-dose budesonide was also found to be associated with slightly higher QALYs compared with montelukast (0.974 vs 0.967, difference: 0.007). The base case results are shown in Table 2.
| Low-dose budesonide | Montelukast | Low-dose budesonide vs montelukast | |
|---|---|---|---|
| Costs (2018 CNY) | |||
| – Drug and device costs | ¥2397 | ¥1962 | ¥434 |
| – Exacerbation management costs | ¥1278 | ¥2167 | -¥889 |
| Total costs | ¥3675 | ¥4130 | ¥455 |
| Effectiveness | |||
| – Total QALYs | 0.974 | 0.967 | 0.007 |
| Conclusion | |||
| Dominant | |||
Bold values highlight the relevant results.
CNY: Chinese Yuan; QALY: Quality-adjusted life year.
Sensitivity analyses
Given that low-dose budesonide was a dominant treatment in the base case, the DSA was conducted for costs and QALYs separately (Figure 2 & Figure 3). Costs were sensitive to the hospitalization rate during moderate-to-severe exacerbations, adherence rate of low-dose budesonide and drug unit cost for budesonide. Low-dose budesonide remained cost-saving or was associated with a cost increase that was less than ¥200. QALYs were sensitive to exacerbation rates and utility values, but none of them would change the base case conclusion.
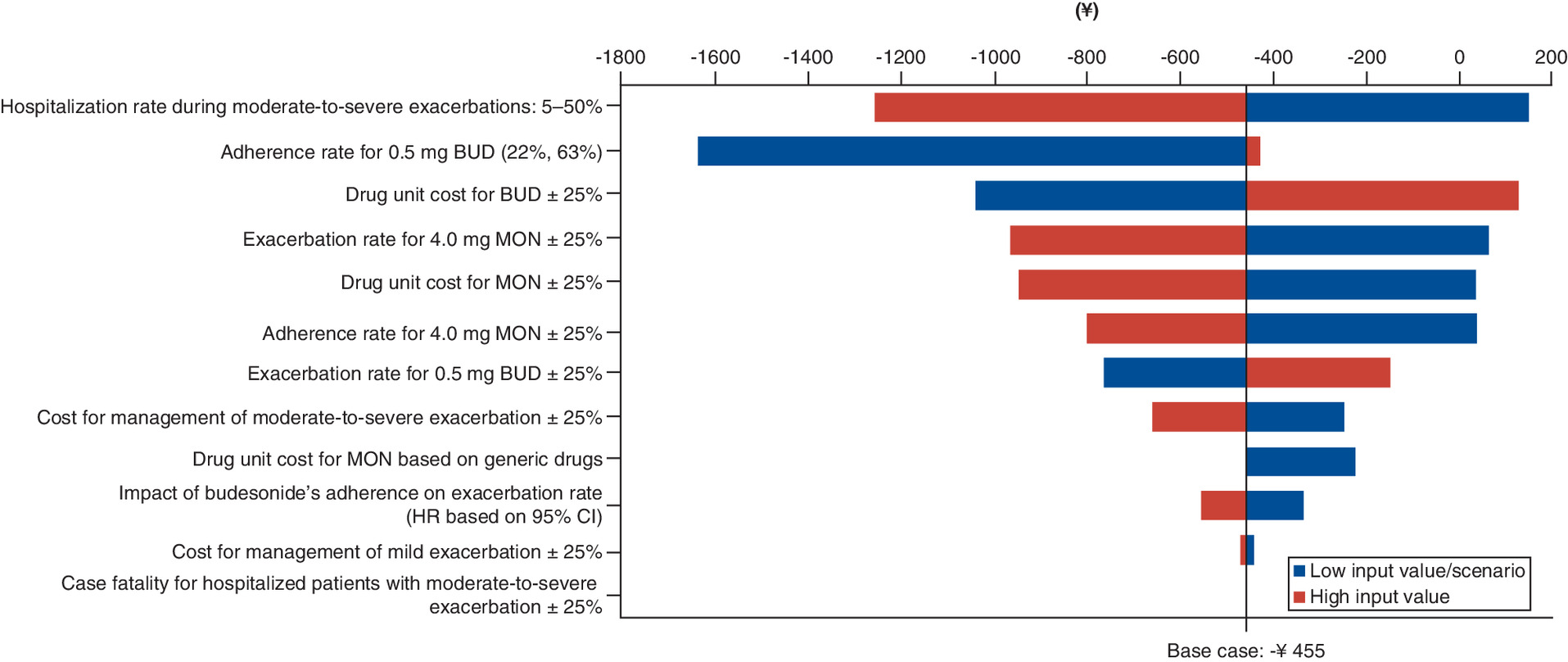
Figure 2. Deterministic sensitivity analysis results on costs.
Only variations/scenarios with impact on the base case result are shown in the chart.
BUD: Budesonide; MON: Montelukast; HR: Hazard ratio.
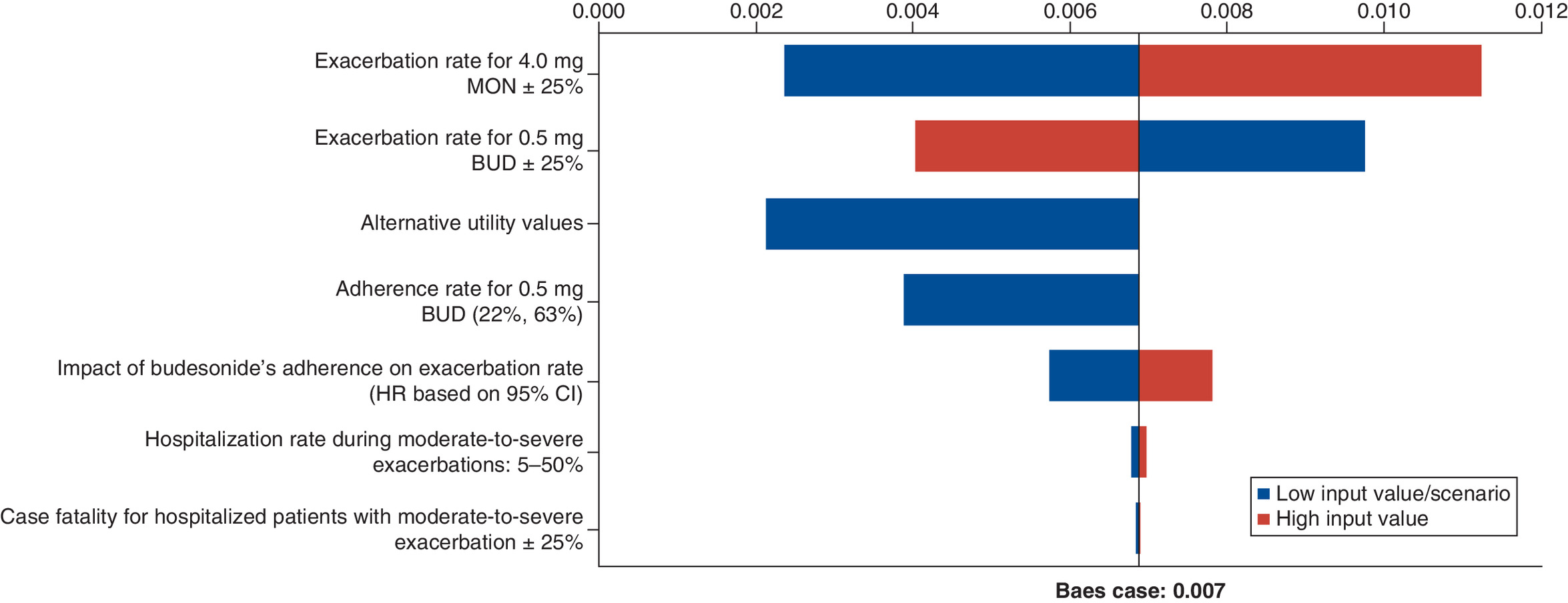
Figure 3. Deterministic sensitivity analysis results on quality-adjusted life years.
Only variations/scenarios with impact on the base case result are shown in the chart.
BUD: Budesonide; MON: Montelukast; HR: Hazard ratio.
In the probabilistic sensitivity analysis, low-dose budesonide appeared to be a highly cost-effective treatment compared with montelukast. Among 1000 iterations, 83% of simulated results fell below the willingness-to-pay threshold of one-time GDP per capita (Figure 4).
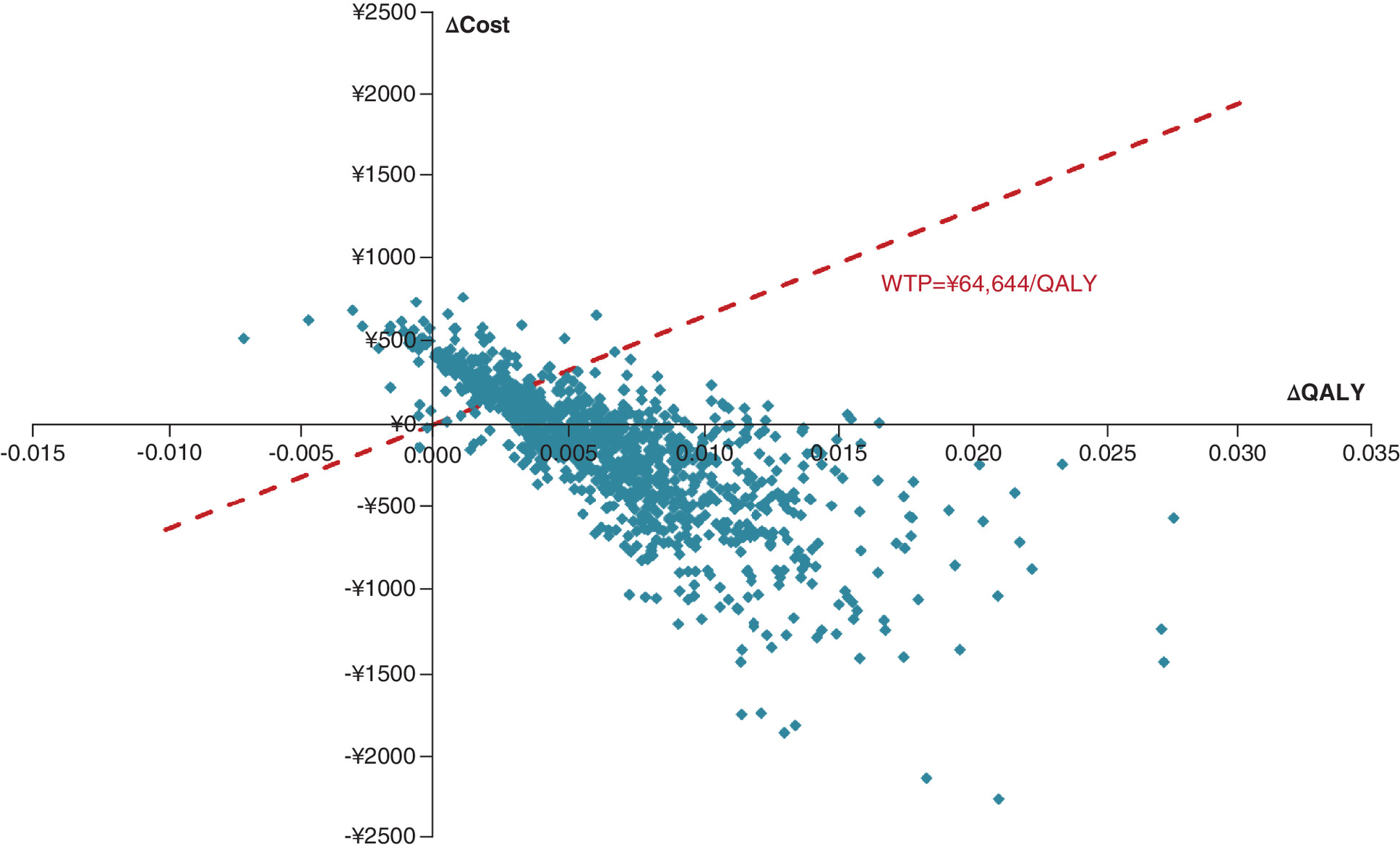
Figure 4. Cost–effectiveness plane.
QALY: Quality-adjusted life year; WTP: Willingness-to-pay.
Discussion
Despite treatment recommendations from GINA and the China guidelines, low-dose ICS, specifically low-dose budesonide, is not adequately used in China [12,13]. By conducting a cost–effectiveness analysis, this study provides evidence that echoes the guideline’s recommendation from an economic perspective. In addition to clinical benefits, low-dose budesonide was demonstrated to be cost-saving when compared with montelukast.
The estimated cost savings were primarily driven by fewer exacerbation events in the low-dose budesonide arm. As low-dose budesonide was associated with better clinical outcomes, use of low-dose budesonide starting at a young age is expected to achieve and maintain effective control of asthma-related symptoms. Overall, the findings of the present study echo the suggestion that introducing treatment with ICS as early as possible has the potential to reduce the disease burden of asthma in China [49]. To our knowledge, this study is the first cost–effectiveness analysis comparing Step 2 treatment options among pediatric patients aged 1–5 years old in China. With such evidence now available, incorporating the usage of low-dose budesonide into the standard of care as a Step 2 treatment for pediatric patients is likely to improve disease management of asthma in China.
Results from the present study are consistent with previous evaluations in other countries [50,51]. A study published in 2018 that systematically reviewed cost–effectiveness analyses comparing ICS and LTRA concluded that in pediatric patients with persistent asthma, ICS, including budesonide or fluticasone propionate, was more likely to be cost-effective than LTRA, including montelukast or zafirlukast [50]. The cost–effectiveness of budesonide for patients with mild persistent asthma was confirmed in another study in which budesonide, added to the usual asthma care regimen, was compared with the standard of asthma care in children 5 to 10 years of age [51]. Results of that study showed that the addition of budesonide was cost-effective from a healthcare payer perspective and cost-saving when taking indirect costs into account [51].
This study has several advantages. The study adopted a commonly used model structure in asthma economic evaluations [28,52–55], in which the model states were defined with patients’ exacerbation states and death. The number of exacerbations is a key measure of clinical outcomes in asthma management and therefore, the exacerbation rates could be obtained from the literature and directly used in the model as state transition probabilities, without assumptions or conversion to control rates. Exacerbation is always associated with substantial HRU, and can influence patients’ quality of life [18], and therefore modeling exacerbation could explicitly capture the implications of clinical outcomes on economic and quality of life outcomes. The model stratified exacerbation into two severity levels, which could capture the levels of the clinical and economic burden associated with exacerbation more accurately. As a chronic disease that requires long-term management, treatment adherence and its impact on costs and treatment outcomes are of high interest to both patients and payers. In this analysis, treatment adherence was considered with well-established input values supporting the model analysis. Regional variation in clinical practices is another key consideration in evaluating cost–effectiveness in China. To account for such variation, the hospitalization rate during moderate-to-severe exacerbations varied remarkably from 5 to 50% in the DSA, and the results supported the generalizability of the study’s findings. Furthermore, the present model accounted for the novel drug procurement scheme and thriving drug market in China by including the generic version of montelukast [56]. Considering the potential trend with generic drugs occupying the market, low-dose budesonide was still associated with cost savings.
The present study should be interpreted within the context of inherent limitations in economic modelling. Model inputs were obtained from different data sources and not necessarily based on a Chinese population. With different baseline characteristics and clinical settings, patients in China may have a different asthma management profile. To address this, model inputs were varied in sensitivity analyses. Several assumptions had been made in this model. To verify the assumptions and account for the associated uncertainties, health economics and clinical experts were consulted and sensitivity and scenario analyses were conducted. The sensitivity and scenario analyses demonstrated the robustness of the model results.
Conclusion
Compared with montelukast, low-dose budesonide is a favorable Step 2 treatment option for pediatric patients (aged 1–5 years) with mild persistent asthma, as it is not only associated with better clinical outcomes but also cost-saving to patients and healthcare payers. These findings may be generalizable to patients residing in different regions of China and remained robust when compared with montelukast generic drugs. This study provides evidence to support informed treatment selection and the study’s findings may improve the use of low-dose budesonide, an economically and clinically preferable treatment to montelukast in pediatric patients.
•
In China, the prevalence of pediatric asthma has risen from 0.9 to 3.0% over the last several decades.
•
Adequate control of asthma-related symptoms is critical in reducing the likelihood of an exacerbation and other adverse events.
•
Clinical guidelines recommend long-term maintenance therapy with low-dose inhaled corticosteroids (ICS) or leukotriene receptor antagonists (LTRA) for persistent asthma in pediatric patients. Although research suggests that low-dose ICS is associated with greater benefits than LTRA, use of ICS in clinical practice is limited, likely due to the perceived burden associated with its costs.
•
In this study, we compared the cost–effectiveness of two recommended Step 2 maintenance treatments for pediatric patients with mild persistent asthma, low-dose budesonide, an ICS, and montelukast, an LTRA, from a patient and healthcare payer perspective in China, to provide evidence supporting informed treatment selection.
•
A Markov model consisting of four health states (no exacerbation, mild exacerbation, moderate-to-severe exacerbation, and death) was constructed to compare treatments over 1 year; inputs included efficacy (i.e., exacerbation rates), mortality, utilities and costs and treatment adherence based on available literature and verified with clinical expert opinion. Deterministic and probabilistic sensitivity analyses were also conducted.
•
Compared with montelukast, low-dose budesonide was associated with fewer exacerbation events, lower costs and slightly more quality-adjusted life years.
•
This study's results echo the guideline’s recommendation from an economic perspective.
•
The better clinical outcomes and cost savings associated with low-dose budesonide may help to reduce the clinical and economic burden of persistent pediatric asthma in China.
Author contributions
X Wang and H Fang contributed equally to the design of the study, drafted the initial manuscript and reviewed and revised the manuscript. All authors contributed to the intellectual content, assisted with revising the manuscript, and have read and approved the final version of the manuscript.
Financial & competing interests disclosure
This study was sponsored by AstraZeneca. T Liu and Y Liu are employees of AstraZeneca. H Fang, J Xie, J Zhong and E Wu are employees of Analysis Group, Inc., which received consultancy fees for the conduct of this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by Gloria DeWalt, PhD, an employee of Analysis Group.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Papi A, Brightling C, Pedersen SE, Reddel HK. Asthma. Lancet 391(10122), 783–800 (2018).
2.
World Health Organization. Asthma (2020). www.who.int/news-room/q-a-detail/asthma
3.
Global Initiative for Asthma. General information about asthma (2020). https://ginasthma.org/about-us/faqs/
4.
Yangzong Y, Shi Z, Nafstad P, Haheim LL, Luobu O, Bjertness E. The prevalence of childhood asthma in China: a systematic review. BMC Public Health 12, 860 (2012).
5.
Institute of Environmental Health and Related Product Safety. Third nationwide survey of childhood asthma in urban areas of China [article in Chinese]. Chin. J. Pediatr. 51(10), 729–735 (2013).
6.
Zhang Q, Qiu Z, Chung KF, Huang SK. Link between environmental air pollution and allergic asthma: east meets west. J. Thorac. Dis. 7(1), 14–22 (2015).
7.
Lin J, Wang W, Chen P et al. Prevalence and risk factors of asthma in mainland China: the CARE study. Respir. Med. 137, 48–54 (2018).
8.
Gautier C, Charpin D. Environmental triggers and avoidance in the management of asthma. J. Asthma Allergy 10, 47–56 (2017).
9.
Wang D, Xiao W, Ma D et al. Cross-sectional epidemiological survey of asthma in Jinan, China. Respirology 18(2), 313–322 (2013).
10.
Huang K, Yang T, Xu J et al. Prevalence, risk factors, and management of asthma in China: a national cross-sectional study. Lancet 394(10196), 407–418 (2019).
11.
Ding B, Small M. Disease burden of mild asthma in China. Respirology 23(4), 369–377 (2018).
12.
Global Initiative for Asthma. Global strategy for asthma management and prevention, 2019 (2019). www.ginasthma.org/
•• Treatment guidelines that summarize the stepwise approach for asthma management and prevention with supporting clinical evidence.
13.
The Subspecialty Group of Respiratory Diseases. Guideline for the diagnosis and optimal management of asthma in children [article in Chinese]. Chin. J. Pediatr. (3), 167–180 (2016).
14.
Banov CH. The role of budesonide in adults and children with mild-to-moderate persistent asthma. J. Asthma 41(1), 5–17 (2004).
15.
Dumitru C, Chan SM, Turcanu V. Role of leukotriene receptor antagonists in the management of pediatric asthma: an update. Paediatr. Drugs 14(5), 317–330 (2012).
16.
Kumar V, Ramesh P, Lodha R, Pandey RM, Kabra SK. Montelukast vs. inhaled low-dose budesonide as monotherapy in the treatment of mild persistent asthma: a randomized double blind controlled trial. J. Trop. Pediatr. 53(5), 325–330 (2007).
17.
Shah MB, Gohil J, Khapekar S, Dave J. Montelukast versus budesonide as a first line preventive therapy in mild persistent asthma in 2 to 18 y. Indian J. Pediatr. 81(7), 655–659 (2014).
18.
Szefler SJ, Carlsson LG, Uryniak T, Baker JW. Budesonide inhalation suspension versus montelukast in children aged 2 to 4 years with mild persistent asthma. J. Allergy Clin. Immunol. Pract. 1(1), 58–64 (2013).
•• A clinical study that compared budesonide inhalation suspension versus montelukast in children aged 2–4 years with mild persistent asthma with asthma exacerbation as the primary end point.
19.
Davitkov P, Chandar AK, Hirsch A et al. Treatment selection choices should not be based on benefits or costs alone: a head-to-head randomized controlled trial of antiviral drugs for hepatitis C. PLoS ONE 11(10), e0163945 (2016).
20.
Mark DB. Implications of cost in treatment selection for patients with coronary heart disease. Ann. Thorac. Surg. 61(Suppl. 2), S12–S15; discussion S33–S14 (1996).
21.
Casas M, Den Dekker HT, Kruithof CJ et al. The effect of early growth patterns and lung function on the development of childhood asthma: a population based study. Thorax 73(12), 1137–1145 (2018).
22.
Lin J, Xing B, Tang H et al. A multi-center retrospective study of clinical characteristics and hospitalization costs of patients hospitalized for asthma exacerbation in China during 2013–2014 [article in Chinese]. Chin. J. Tuberculosis Respir. Dis. 40(11), 830–834 (2017).
• This study retrospectively reviewed patients hospitalized for asthma exacerbation in China and reported the case-fatality rate for hospitalized patients.
23.
National Parents of Asthmatic Children Kap Project Team. Asthma control status in children and related factors in 29 cities of China [article in Chinese]. Chin. J. Pediatr. 51(2), 90–95 (2013).
• This study retrospectively analyzed 2690 children with persistent asthma in China, reported the asthma control status, including the hospitalization rate and evaluated related risk factors.
24.
Rodriguez-Martinez CE, Sossa-Briceno MP, Castro-Rodriguez JA. Cost-utility analysis of the inhaled steroids available in a developing country for the management of pediatric patients with persistent asthma. J. Asthma 50(4), 410–418 (2013).
• This study compared different treatment strategies among pediatric patients with persistent asthma in Colombia and conducted a survey to collect utility inputs.
25.
Astrazeneca Analysis. Provincial/municipal drug procurement databases. (2019).
26.
Astrazeneca Analysis. Nebulizer market data. (2019).
27.
Du J, Ying Y. Cost–effectiveness analysis in child asthma treated with GINA inhaled therapeutic regimen and other therapy [article in Chinese]. Mod. J. Integ. Trad. Chin. West. Med. 15(13), 1738–1742 (2006).
28.
Zhou H, Lu Y, Wu B, Che D. Cost–effectiveness of omalizumab for the treatment of inadequately controlled severe allergic asthma in Chinese children. J. Asthma 1(8), 87–94 (2018).
29.
Hu X, Chen Q. Investigation and analysis on glucocorticoid treatment compliance for children in asthma remission phase and strategies. Nurs. Rehab. 9(3), 194–195 (2010).
30.
National Bureau of Statistics in China. Tabulation on the 2010 population census of the people republic of China [content in Chinese] (2010). www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm
31.
Willems DC, Joore MA, Hendriks JJ, Wouters EF, Severens JL. Cost–effectiveness of a nurse-led telemonitoring intervention based on peak expiratory flow measurements in asthmatics: results of a randomised controlled trial. Cost Eff. Resour. Alloc. 5, 10 (2007).
32.
Chiou CF, Weaver MR, Bell MA, Lee TA, Krieger JW. Development of the multi-attribute Pediatric Asthma Health Outcome Measure (PAHOM). Int. J. Qual. Health Care 17(1), 23–30 (2005).
33.
Mittmann N, Trakas K, Risebrough N, Liu BA. Utility scores for chronic conditions in a community-dwelling population. Pharmacoeconomics 15(4), 369–376 (1999).
34.
Juniper EF, Guyatt GH, Feeny DH, Griffith LE, Ferrie PJ. Minimum skills required by children to complete health-related quality of life instruments for asthma: comparison of measurement properties. Eur. Respir. J. 10(10), 2285–2294 (1997).
35.
Carroll AE, Downs SM. Improving decision analyses: parent preferences (utility values) for pediatric health outcomes. J. Pediatr. 155(1), e21–e25 (2009).
36.
Lloyd A, Price D, Brown R. The impact of asthma exacerbations on health-related quality of life in moderate to severe asthma patients in the UK. Prim. Care Respir. J. 16(1), 22–27 (2007).
37.
National Bureau of Statistics in China. National data: Consumer Price Index Medical Care Component [content in Chinese] (2018). http://data.stats.gov.cn/easyquery.htm?cn=C01
38.
National Medical Product Administration. Drug information [content in Chinese] (2018). http://app1.sfda.gov.cn/datasearchcnda/face3/dir.html?type=yp
39.
Morton RW, Everard ML, Elphick HE. Adherence in childhood asthma: the elephant in the room. Arch. Dis. Child. 99(10), 949–953 (2014).
40.
Williams LK, Peterson EL, Wells K et al. Quantifying the proportion of severe asthma exacerbations attributable to inhaled corticosteroid nonadherence. J. Allergy Clin. Immunol. 128(6), 1185–1191 e1182 (2011).
41.
Barnes CB, Ulrik CS. Asthma and adherence to inhaled corticosteroids: current status and future perspectives. Respir. Care 60(3), 455–468 (2015).
42.
Zhu Y. Clinical outcomes of montelukast in the treatment of asthma in children [article in Chinese]. Chin. J. Mod. Drug 5(1), 91 (2011).
43.
Jin Y, Ma X. Treatment outcomes and treatment adherence in pediatric patients receiving montelukast for asthma [article in Chinese]. J. Chin. Phys. 21(12), 1906–1908 (2019).
44.
Wang J. Observation of 42 children with mild asthma treated with montelukast [article in Chinese]. Chin. J. New Drugs Clin. Rem. (4), 333–335 (2005).
45.
Salomon JA. Quality adjusted life years. In: International Encyclopedia of Public Health (2nd Edition). Quah SR (Ed.). Academic Press, Oxford, UK, 224–228 (2017).
46.
China Guidelines for Pharmacoeconomic Evaluations Working Group. China guidelines for pharmacoeconomic evaluations [content in Chinese]. China Center for Health Economic Research (2011).
• These guidelines provide methodological guidance for pharmacoeconomic evaluations in China, including recommendation on study perspectives, time horizon, data sources and thresholds for decision making, etc.
47.
Marseille E, Larson B, Kazi DS, Kahn JG, Rosen S. Thresholds for the cost–effectiveness of interventions: alternative approaches. Bull. World Health Organ. 93(2), 118–124 (2015).
48.
National Bureau of Statistics in China. National data: GDP per capita [content in Chinese] (2018). http://data.stats.gov.cn/easyquery.htm?cn=C01
49.
Brusselle GG, Ko FW. Prevalence and burden of asthma in China: time to act. Lancet 394(10196), 364–366 (2019).
50.
Rodriguez-Martinez CE, Sossa-Briceno MP, Castro-Rodriguez JA. Cost–effectiveness of pharmacological treatments for asthma: a systematic review. Pharmacoeconomics 36(10), 1165–1200 (2018).
51.
Weiss K, Buxton M, Andersson FL, Lamm CJ, Liljas B, Sullivan SD. Cost–effectiveness of early intervention with once-daily budesonide in children with mild persistent asthma: results from the START study. Pediatr. Allergy Immunol. 17(Suppl. 17), 21–27 (2006).
52.
Zafari Z, Sadatsafavi M, Marra CA, Chen W, Fitzgerald JM. Cost–effectiveness of bronchial thermoplasty, omalizumab, and standard therapy for moderate-to-severe allergic asthma. PLoS ONE 11(1), e0146003 (2016).
53.
Morishima T, Ikai H, Imanaka Y. Cost–effectiveness analysis of omalizumab for the treatment of severe asthma in Japan and the value of responder prediction methods based on a multinational trial. Value Health Reg. Issues 2(1), 29–36 (2013).
54.
Dewilde S, Turk F, Tambour M, Sandstrom T. The economic value of anti-IgE in severe persistent, IgE-mediated (allergic) asthma patients: adaptation of INNOVATE to Sweden. Curr. Med. Res. Opin. 22(9), 1765–1776 (2006).
55.
Campbell JD, Spackman DE, Sullivan SD. The costs and consequences of omalizumab in uncontrolled asthma from a USA payer perspective. Allergy 65(9), 1141–1148 (2010).
56.
Patrick B. 4+7: china's new volume-based purchasing policy (2019). https://pharmaboardroom.com/articles/4-plus-7-chinas-new-volume-based-purchasing-policy/
Information & Authors
Information
Published In
Copyright
© 2020 Future Medicine Ltd.
History
Received: 6 June 2020
Accepted: 14 September 2020
Published online: 6 November 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The cost–effectiveness of low-dose budesonide as a Step 2 treatment for pediatric asthma in China. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0102
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Guohuan Chen, Bizhi Zheng, Jinhe Cui, Proteinase-Activated Receptor 2 Expression and F2RL1 Genetic Variants Are Associated with Asthma: A Case-Control Study in the Chinese Population, Human Heredity, 10.1159/000547925, 90, 1, (51-61), (2025).
- Pingbo Zhang, Yixiao Bao, Xiaojian Zhou, Yanming Lu, Bo Ding, Li Hua, Lili Zhong, Dan Liu, Jing Liu, Deyu Zhao, Zhongping Zhang, Lina Zhen, Suping Tang, Wenhui Jiang, Caifeng Zhang, Zhou Fu, Zehui Ye, Li Dong, Rongfang Zhang, Xuan Liang, Ning Wang, Long Zhao, Ya Luo, Zhaobo Shen, Ping Kang, Mengli Ren, Jie Shao, Comparing the effects of two low-dose budesonide suspension nebulization treatments on asthma among young children: a multicenter study, Journal of Asthma, 10.1080/02770903.2025.2539810, 62, 11, (1960-1969), (2025).
- Keruo Zhou, Min Zhang, Chenyu Zuo, Xiazhen Xie, Jianwei Xuan, Cost-effectiveness analysis of budesonide/formoterol SMART therapy versus salmeterol/fluticasone plus as-needed SABA among patients ≥12 years with moderate asthma from the Chinese societal perspective, Journal of Medical Economics, 10.1080/13696998.2024.2385191, 27, 1, (1018-1026), (2024).