Burden of recurrent syncope and injuries and the usefulness of implantable cardiac monitors: insights from a nationwide longitudinal cohort analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The study assesses the burden and costs of recurring unexplained syncope and injuries and the effectiveness of implantable loop recorders. Methods: The English national hospital database (Hospital Episode Statistics) was retrospectively analyzed. Results: 12,002 patients were identified with repeated syncope hospitalizations. 25% of patients were hospitalized at least once again for syncope, 9% of the patients were hospitalized at least once for an injury, causing substantial costs. In the second analysis: 10,902 patients implanted with an implantable cardiac monitor were tracked. By year 3, hospitalizations due to syncope had dropped by 60% versus pre-implantable cardiac monitor (ICM) levels. Conclusion: This study shows a high rate of recurrent syncope admissions and a parallel burden of hospitalizations for injuries. Use of an ICM appears to reduce syncope hospitalizations.
Syncope is a transient loss of consciousness due to cerebral hypoperfusion. The prognosis ranges from benign to life threatening, depending on the underlying cause. Its incidence increases with age, with a sharp rise after the age of 70 years [1]. Since many countries are undergoing major demographic changes with more and more people aged over 70, there is a pressing need to analyze current care pathways and healthcare delivery in order to monitor and reduce healthcare costs, which will otherwise be unaffordable.
Diagnosis of the underlying cause of syncope can be challenging as patients generally do not have symptoms when they seek medical care and diagnostic tests undertaken when they are asymptomatic may be normal. In the elderly, syncope may also masquerade as falls [2]. Syncope remains undiagnosed in up to a third of patients after initial clinical investigations. Irrespective of the cause of syncope, when it remains undiagnosed and untreated, it is likely to recur, putting a strain on patients and their carers [3]. Patients' quality of life of syncope patients has been shown to be as severly afftected as for patients with chronic diseases such as end-stage kidney disease or structural heart disease [4–6].
Even more importantly, studies have also shown an association between syncopal events in otherwise healthy individuals and increased morbidity and mortality [7,8]. Cardiac syncope is estimated to double the risk of death [1]. Recurrent syncope also carries a substantial risk of falls and related injuries; 29% of syncope patients present with injury and trauma in the ED, with 5% of patients being severe cases [9].
Recurrent syncope is likely to be a burden for healthcare systems due to emergency care, injuries and repeated hospitalizations. The costs of evaluating syncope are further increased as diagnostic assessment has been shown to be unstructured in many hospitals irrespective of guidelines [2,10,11]. Patients can be seen by three different specialists and undergo 13 tests without receiving a diagnosis. Standard tests tend to be repeated many times, including various expensive diagnostic tests which have a low diagnostic yield in unexplained syncope patients [10,11].
In order to improve the diagnostic yield of syncope investigations, the Transient Loss of Consciousness (T-LOC) Guidelines by the National Institute for Health and Care Excellence (NICE) as well as the Syncope Guidelines by the European Society of Cardiology (ESC) and by the American College of Cardiology/American Heart Association/Heart Rhythm Society present evidence and recommendations regarding which investigations are most relevant and likely to lead to a diagnosis [2,12,13].
If the underlying cause of recurrent unexplained syncope is suspected to be cardiac, diagnostic clarification of the underlying rhythm with an implantable loop recorder (ILR) is recommended: The 2018 ESC Syncope guidelines recommend ILRs in these patients with class IA. Moreover ILRs are also recommended in patients with suspected or certain reflex syncope (class IIa), in patients in whom epilepsy was suspected but the treatment has proven ineffective and last, in patients with unexplained falls (class IIb) [2].
Syncope might be a first sign of an underlying cardiovascular disease which could carry an increased risk of death if untreated [7,8]. Some of these patients may need treatment with cardiac implantable devices, for example, permanent pacemakers or defibrillators. These cardiac implantable devices have been shown to favorably alter prognosis [14,15]. ILRs enable the recording of an electrocardiogram during a syncopal event, which is considered the gold standard to diagnose arrhythmic or cardiac syncope. Based on a recent meta-analysis, ILR are three- to six-times more likely to reach a diagnosis than conventional testing [2].
The study assesses the burden and costs of recurring unexplained syncope by retrospectively analyzing claims data over a period of 9 years. Separate hospitalizations for injuries that could be the result of a syncope are also analyzed. A syncope is a well-recognized cause of injuries. However, syncope might not be properly coded in claims data if the main reason for the hospitalization was the treatment of an injury. We therefore checked whether patients with recurrent hospitalizations for syncope are also separately hospitalized for injuries which could have been caused by a syncope. Analyzing the correlation between syncope and injury might help to understand the true burden of syncope for patients. ICMs are recommended in Guidelines as a tool to support the diagnosis of patients with unexplained syncope [2,12]. This study analyzes whether implantable loop recorders help to reduce syncope admissions in practise and lead to treatment.
Methods
Data source
England has a National Health Service (NHS) through which medical care is accessible to all residents in England by healthcare providers. Healthcare providers in turn, submit coded claims to the NHS to be reimbursed. The NHS tracks healthcare resource utilization and costs of services delivered to patients through the Hospital Episode Statistics (HES) database which contains all coded hospital claims. Longitudinal data for each individual patient in the entire NHS can be tracked. Limitations of the HES database are that primary care, social care and secondary care visits delivered in private clinics (∼10% of patients have access to private healthcare in addition to the NHS) are not included. This affects the reporting of certain types of treatment delivered, for example, medications prescribed as outpatients, sick pay, remedies and medical aids. The claims submitted by the healthcare providers include three categories of data via coding systems: the disease, the procedures performed and the discharge code which determine the associated lumpsum payment. More specifically, the codes are ICD-10 (International Statistical Classification of Diseases and Related Health Problems), the Classification of Interventions and Procedures (OPCS-4), as well as Hospital Related Group (HRG) codes.
•
Recurrent syncope analysis:
Patients with two syncope hospitalizations were retrospectively identified from the HES database using the ICD-10 diagnosis code R55X – ‘Syncope and collapse’ in the primary diagnosis code position between 2008 and 2014. To select a group of patients with a high burden of syncope, we identified patients who had at least two hospitalizations for syncope within two consecutive years between 1 April 2008 and 31 March 2014. As the total data available was from 2008 to 2016, such an analysis allowed us to follow individual patients longitudinally for at least 2 years after the first two hospitalizations for syncope. As there is no ICD-10 diagnosis code for ‘unexplained’ syncope, patients with recurrent syncope hospitalizations were identified through the ICD-10 code R55 – ‘‘Syncope and collapse’. Patients were excluded if they had a documented ICD-10 diagnosis code in the baseline period which could be the cause of syncope; such codes are for example epilepsy or orthostatic hypotension (Supplementary Table 1). The most common ICD-10 diagnosis code used with R55-X Syncope and Collapse are shown in Supplementary Table 2. In addition, patients who received a cardiac therapeutic device, for example, a permanent pacemaker, implantable cardioverter defibrillator or a cardiac resynchronization therapy device at any time during the study period (1 April 2008 and 31 March 2016) were excluded from the analysis as it was assumed that their cause of syncope had been identified and treated. Also, patients implanted with an ICM were excluded from the analysis as an estimated 70% of patients with ICM receive a diagnosis if they have another event [13]. To assess the long-term burden of recurrent syncope and the costs to the healthcare system, the following outcomes were assessed:
Number of subsequent hospital admissions for syncope
Length of stay
Number of outpatient cardiology visits
Number of separate hospital admissions due to injuries which could have been caused by a syncope.
HRG codes and tariff for the healthcare utilizations above.
Costs were approximated by the HRG tariff which are a lump-sum reimbursement. While acknowledging they will not exactly cover the actual incurred costs for treating a patient, they do provide the best estimate available. Injuries which could have been caused by a syncope were identified using ICD-10 codes S00-S99, T07, T14 (Supplementary Table 3).
•
ILR analysis:
For this separate analysis, a cohort of patients who received an ILR between 1 April 2009 and 31 March 2012 were identified. An ICM implant was identified through the procedure code U191. These patients were then longitudinally tracked from 1 April 2008 to 31 March 2014, thus allowing a minimum follow-up period of 1 year before and 2 years after the ILR implant. The number of syncope hospitalization post-implant were compared with the pre-ILR period.
Patients in the ILR analysis were not directly compared with patients from the recurrent syncope analysis. Comparing the two groups (e.g., through matching) would have had limitations because the HES data only includes hospital records. It cannot be ensured that patients are comparable in other respects as data from primary care is not included in the HES database. We thus decided to keep the two analyses distinct. Patients with an ICM were excluded from Analysis 1 to prevent any patient overlap between the two analyses.
Statistics
The analysis was performed on aggregated data. Continuous data are summarized with a mean ± standard deviation, categorical data as counts and percentages. The risk of recurrence was calculated as number of patients experiencing the specific number of hospitalizations for syncope and the 95% CIs of the binomial distribution are reported. Comparison of the risks were undertaken by means of Chi-square tests.
Results
During the period 2008–2014, the average rate of hospital admissions for syncope was 1.02 per 1000 person-years. This results is consistent with other epidemiological data [14].
Recurrent syncope analysis
12,002 patients (mean age: 73 ± 28 years, 53% females, were identified with ≥2 syncope hospitalizations within two consecutive years between 1 April 2008 and 31 March 2014.
Recurrent hospitalizations for syncope & associated costs
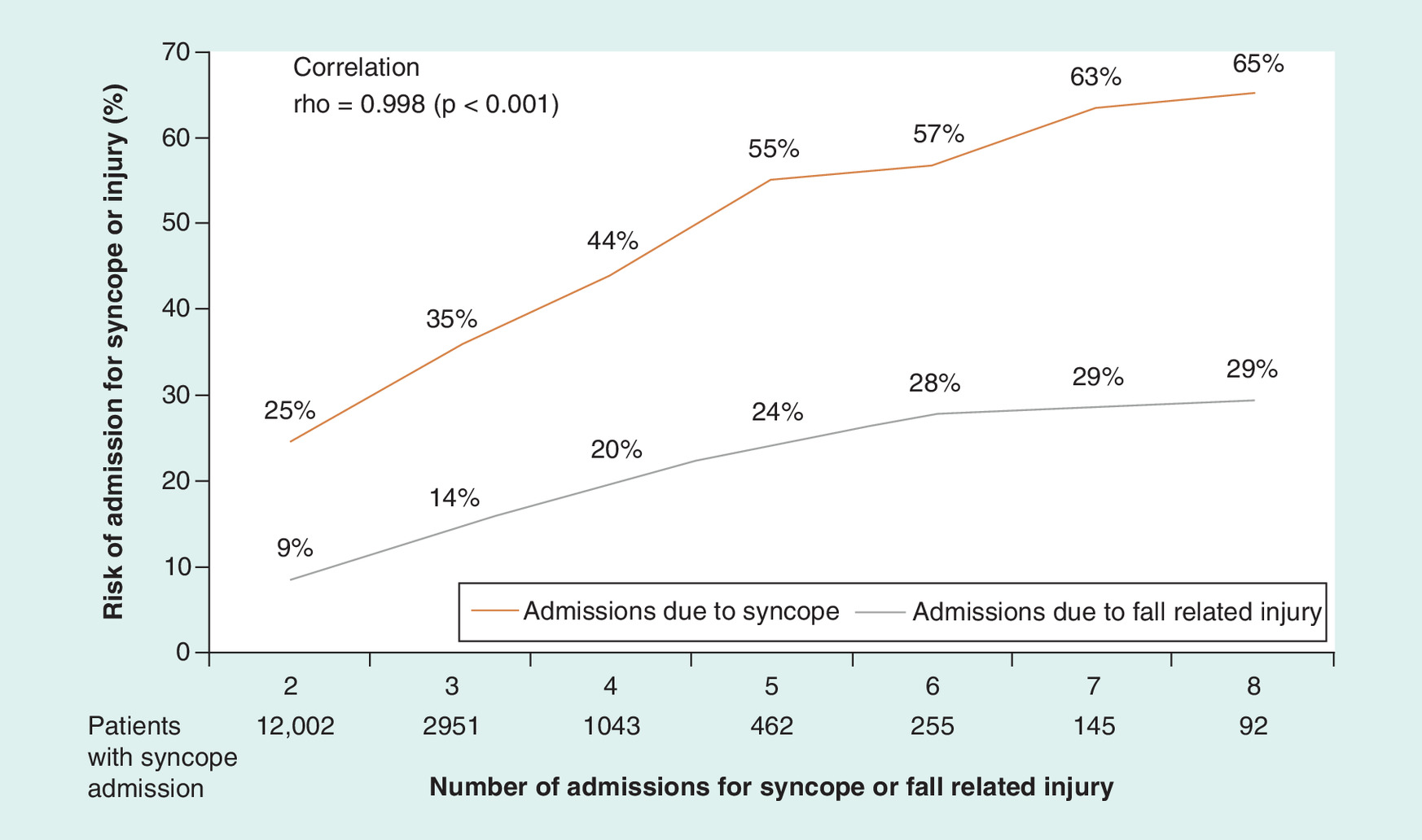
There were a total of 6548 hospitalizations for recurrent syncope over the follow-up period, with 55% (95% CI: 52.3–57.9) of patients experiencing at least one recurrent hospitalization. One quarter (24–25%) of patients were re-hospitalized at least once in the next few months. Considering the subset of patients with at least one hospitalization for recurrence of syncope, the mean number of recurrences per patient was 2.4 (95% CI: 2.3–2.6). As shown in Figure 1, the more syncope admissions a patient had experienced, the higher the risk of subsequent recurrences. This same group of patients also had frequent admissions due to injuries which could have been caused by a syncope; however, they were not coded together with an episode of syncope. A patient with two prior syncope admissions, for example, has a risk of 25% to be hospitalized at least once again for syncope. In addition, patients with two prior syncope hospitalizations have a 9% risk to be hospitalized separately for an injury. There is a remarkably high correlation (0.998) between being hospitalized for syncope and to incur additional hospitalizations for injuries. Of note, due to shrinking sample sizes with increasing number of recurrences, the estimated risk for recurrences 4 and 5 have a large CIs and the values need to be interpreted with caution.
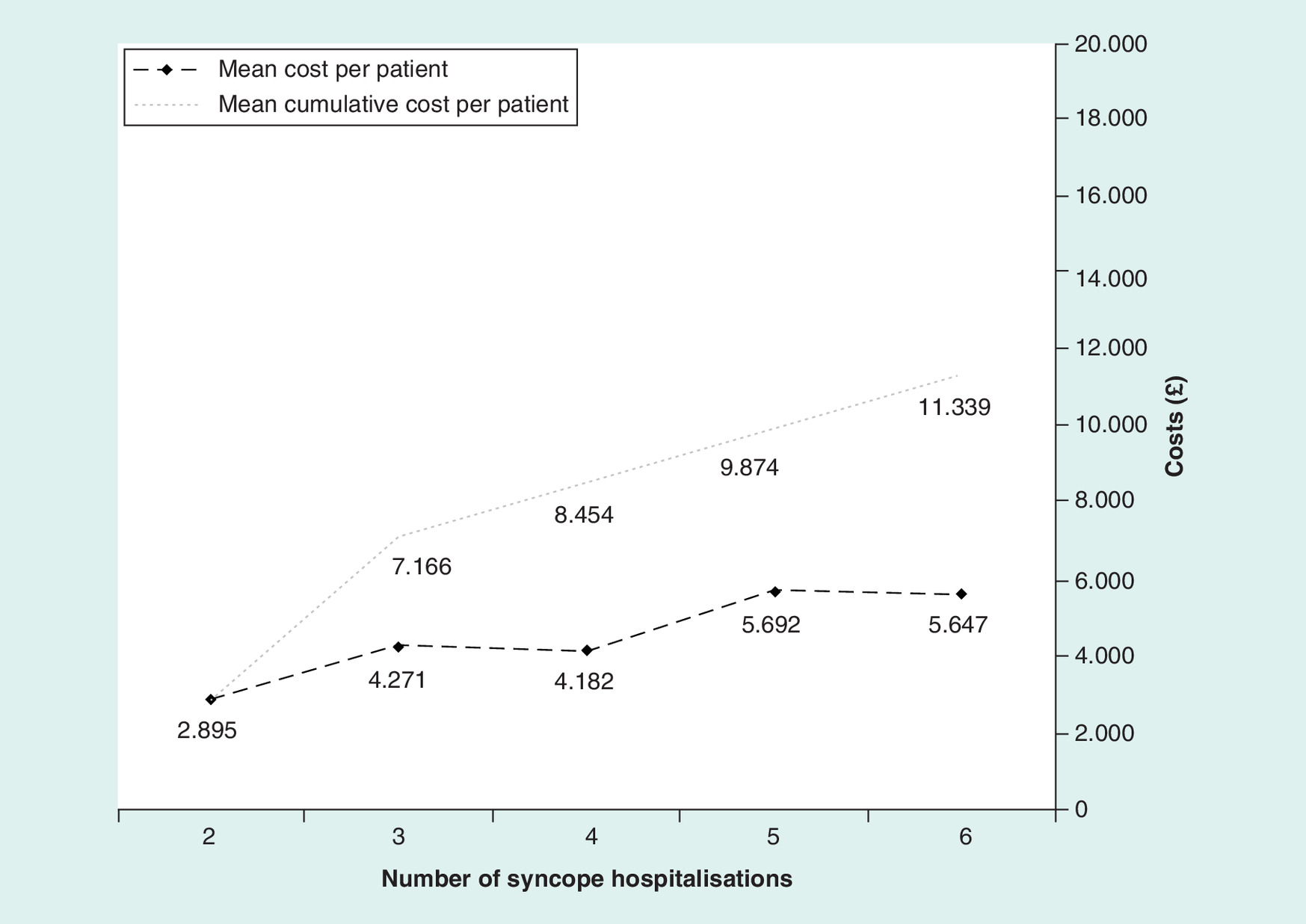
The mean cost per syncope admission was £3406 (range: £2000 – 6000) (£/US$ = 1.24) during follow-up, the total average cost of all syncope hospitalizations was £5713/patient. The more recurrent syncope hospitalizations a patient experienced, the higher the cost of each subsequent admission (Figure 2). The higher costs were not a result of a longer length of stay. There were no specific trends with regard to the number of recurrences and the length of stay. The overall mean length of stay was 1.9 ± 4.1 days.
The average time between syncopal events was 5.2 ± 4.5 months, with a shorter time between events in patients with more recurrent syncopal events. For a patient with five recurrent events, the average time between events shortened to 3.1 ± 1.3 months.
Separate admissions for injuries
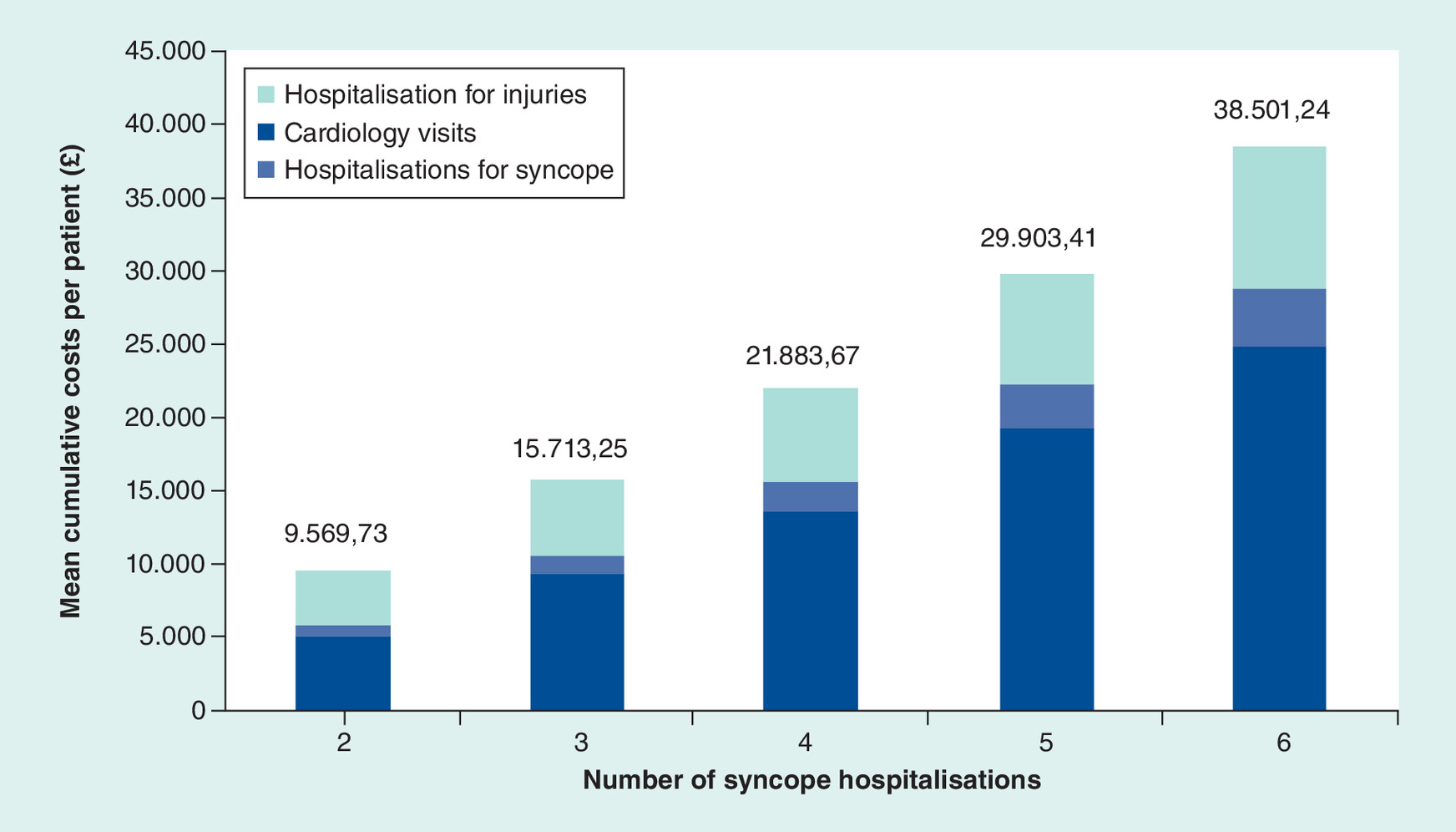
One of the most striking results of the analysis was the high correlation (rho = 0.998) between admissions due to syncope and separate admissions for injuries. Figure 1 shows the risk of experiencing an injury in relation to recurrent hospitalizations for syncope. The burden for these patients was large as they incurred a mean of 2.3 hospitalizations for injuries (95% CI: 2.5–2.7) with an average length of stay of 5.1 ± 8.9 days at a mean cost of £5617 (range: £3267–8949). The most common injury was to the head, followed by injuries to the hip and thigh. The most common HRG codes applied were Orthopaedic Trauma Procedures followed by Mouth Head Neck and Ears Procedures and Disorders. (See Figure 3 & Supplementary Tables 3 & 4for details on diagnosis codes and HRGs used).
Outpatient visits
In addition to the costs incurred for treatment of syncope and injuries, patients with recurrent syncope also frequently visited cardiologists as outpatients. Typically, a patient with two prior hospitalizations for syncope saw a cardiologist in the outpatient setting seven-times thereafter. Long-term costs for these multiple visits were substantial (Supplementary Figure 4) with the mean cumulative costs varying from £454 to £4409 (Supplementary Figure 4).
Overall costs to the healthcare system
The overall costs of the resulting healthcare utilizations in these patients were substantial. The cumulative inclusive costs of hospitalizations due to syncope, injuries and outpatient visits during follow-up were £9570 per patient and 14.9 million in total. For patients with more recurrent syncope hospitalizations, the costs were significantly higher as shown in (Supplementary Figure 5).
ICM analysis
In the second separate analysis, 10,902 patients (mean age: 67, females 50%) implanted with an ILR were tracked. Slightly more than half (55%, 95% CI: 53.3–56.1) of these patients had been hospitalized for syncope at least once in the year before their ICM implant. The annual rate of hospitalization due to syncope fell by 41% (95% CI: 38–43%) each year after implant. By year 3, hospitalizations due to syncope were 14% (95% CI: 13.6–15.2) and thus had dropped by 60% (95% CI: 57–61%) as compared with pre-ICM levels. Moreover, 27% (95% CI: 26–28%) of the cohort received a pacemaker after the ICM implant and 5% received an implantable cardiac defibrillator or an ablation.
Discussion
This study is the first nationwide longitudinal study of syncope patients to use the English hospital database HES. The study has shown that patients with a high burden of recurrent hospitalizations due to syncope are at risk of incurring more syncopal events as well as injuries. The resulting hospital admissions cause substantial healthcare costs. The true burden of recurrent syncope is likely to be underestimated in this analysis as recurrences of syncope as healthcare utilization in primary care or the emergency department have not been captured.
Moreover, this study also documents that the incidence of recurrent syncopal events decreases after ILR implant. The aim of implanting an ILR is to provide a diagnosis which identifies the underlying cause of the syncope so that treatment can be initiated and future syncope events prevented. Syncope hospitaliations are expensive and often do not result in a diagnosis. While we cannot see the diagnostic yield of the ILR in this data, the record shows that nearly 32% of patients receive a therapeutic cardiac implantable device after the ILR.
It is key to diagnose and treat patients with recurrent syncope in order to prevent future events and injuries. Syncope care could most likely be improved by following the ESC Syncope Guidelines or the NICE TLOC Guidance. The observational PICTURE registry reported that an apparent lack of structured care pathways leads to significant overinvestigation where tests are repeated many times and patients undergo various expensive diagnostic tests with low diagnostic yield [10,11]. In contrast, standardized syncope care has been shown to lower costs per diagnosis and admission rates [16]. Syncope units/care pathways are also recommended by the NICE TLOC guidance as well as an EHRA position paper [12,17]. This analysis shows that the syncope hospitalization rates are lower after ICM implant than before, and lead to treatment in approximately a third of patients at 3 years of follow-up. Greater adoption of ICMS could possibly lower the costs per diagnosis as has been shown in clinical practice [16].
This analysis has shown that patients with recurrent syncope hospitalizations are also likely to be hospitalized for injuries potentially caused by a syncope. The frequency of separate admissions related to an injury was investigated to estimate the correlation between admissions due to syncope and injuries. A syncope diagnosis code was not documented during the same admission, and thus these injuries may or may not be directly related to a syncopal event. However, syncope is a well-recognized cause of injuries and patients who need urgent care for an injury after a syncope might not be investigated for the precise circumstances of the injury. Thus, careful examination and diagnostic testing in patients with injuries and a history of syncope may improve outcomes.
Limitation
Claims data provide the possibility to follow patients over a long period of time and to document healthcare utilization in the longer term which is generally not possible with clinical studies due to limited follow-up. The main limitation is of course the observational nature of the study and the lack of clinical data, particularly, electrocardiographic data.
The aim of this analysis was to understand the burden and costs of recurrent syncope. Hospital records can unfortunately only serve as proxy for syncope events and true healthcare costs. Though syncope is a well-defined term, the usage of the code R55X could be broader as the wording also includes ‘collapse' or the coding could simply be inaccurate. Additionally, R55X does not necessarily indicate a recent syncope event. For example, patients could also be re-hospitalized with R55X for continued examinations without having incurred another event. However, hospitals can only claim one hospitalization per patient every 30 days and thus there are at least 30 days between each coded hospitalization. Additionally, the average time between syncope hospitalizations in this study is 5.2 months which appears to be too long for a continued examination. Importantly, a recent validation study has shown that the administrative coding of syncope could accurately be used to identify patients with syncope event with a positive predictive value of 95% [18].
The aim of implanting an ILR is to provide a diagnosis which identifies the underlying cause of the syncope so that the treatment can be initiated and future syncope events prevented. Unfortunately, treatment could only be identified if visible in codes and if provided during a hospitalization, such as the implant of a therapeutic cardiac device. A large ILR registry has shown that patients also receive therapes which are not visible in codes: 11% of syncope patients receive drug therapy and 15% receive counseling, education on counter pressure maneuvers or similar [13]. ILRs are also used to rule out a cardiac cause in patients with recurrent syncope.
In order to evaluate the real-world effectiveness of ILRs to prevent syncope hospitalizations, syncope hospitalizations pre- versus post-implant were also compared. While patients need to have another syncope event in order to establish a diagnosis with an ILR, these patients are generally taken care of in the outpatient setting and further hospitalizations can often be avoided. Moreover, a share of patients can already be diagnosed when having a pre-syncope.
Conclusion
Recurrent syncope in an older population carries a high clinical and financial burden. Patients with repeated hospitalizations for syncope show a high rate of recurrent admissions with syncope and a parallel burden of injuries, imposing a substantial burden on the NHS. Our analysis also shows that ILRs may significantly reduce hospitalization due to syncope. ILRs can help in diagnosing as well as deciding about appropriate treatment and may therefore lead to avoided rehospitalizations, improved patient outcomes and overall cost savings to the NHS. The results of the study may inform clinical practice by emphasizing the need for complete history taking including hospitalizations for injuries. It might also support the implementation of more syncope care pathways, which have been shown to improve care and lower costs.
•
First nationwide longitudinal study of syncope patients to use the English hospital database (Hospital Episode Statistics).
•
The study assesses the burden and costs of recurring unexplained syncope and injuries by following patients over a period of 9 years.
•
The analysis documents that many patients with syncope admissions also have separate hospitalizations for injuries which could have been caused by a syncope.
•
As syncope is a well-recognized cause of injuries, it might be informative to consider the frequency of both for the patient care pathway.
•
Implantable loop recorders are recommended in guidelines as a tool to support the diagnosis of patients with infrequent unexplained syncope.
•
This study analyses whether implantable loop recorders help to reduce syncope events in practice.
•
In the absence of complete data on syncope events, syncope admissions are used as a proxy.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/suppl/10.2144/cer-2020-0059
Financial & competing interests disclosure
C Wolff is an employee of Medtronic, one of the manufacturers of implantable loop recorders. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_file.docx)
- Download
- 37.59 KB
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Soteriades ES, Evans JC, Larson MG et al. Incidence and prognosis of syncope. N. Engl. J. Med. 347(12), 878–885 (2002).
2.
Brignole M, Moya A, de Lange FJ et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. H. J. 39(21), 1883–1948 (2018).
•• The ESC Syncope Guidelines present evidence and recommendations regarding which investigations are most relevant and likely to lead to a diagnosis in syncope patients. They include a meta-analysis showing that implantable loop recorder are 3.6 times more likely to reach a diagnosis than conventional testing.
3.
Sutton R, Benditt DG. Epidemiology and economic impact of cardiac syncope in western countries. Future Cardiol. 8(3), 467–472 (2012).
4.
van Dijk N, Sprangers MA, Colman N, Boer KR, Wieling W, Linzer M. Clinical factors associated with quality of life in patients with transient loss of consciousness. J. Cardiovasc. Electrophysiol. 17, 998–1003 (2006).
5.
Linzer M, Gold DT, Pontinen M, Divine GW, Felder A, Brooks WB. Recurrent syncope as a chronic disease: preliminary validation of a disease-specific measure of functional impairment. J. Gen. Intern. Med. 9(4), 181–186 (1994).
6.
Numé AK, Kragholm K, Carlson N et al. Syncope and its impact on occupational accidents and employment. Circ. Cardiovasc. Qual. Outcomes 10(4), e003202 (2017).
7.
Yasa E, Ricci F, Magnusson M, Sutton R, Gallina S, De Caterina R. Cardiovascular risk after hospitalization for unexplained syncope and orthostatic hypotension. Heart 104(6), 487–493 (2018).
•• Shows that a hospitalization for unexplained syncope is associated with a higher risk of cardiovascular death and all-cause mortality. Patients have a higher risk of coronary events, strokes, heart failure and aortic stenosis.
8.
Ricci F, Sutton R, Palermi S et al. Prognostic significance of noncardiac syncope in the general population: a systematic review and meta-analysis. J. Cardiovasc. Electrophysiol. 29(12), 1641–1647 (2018).
•• Shows a higher all-cause mortality in patients with a previous hospitalization for unexplained syncope.
9.
Bartoletti A, Fabiani P, Bagnoli L et al. Physical injuries caused by a transient loss of consciousness: main clinical characteristics of patients and diagnostic contribution of carotid sinus massage. Eur. Heart J. 29(5), 618–624 (2017).
10.
Edvardsson N, Frykman V, van Mechelen R et al. Use of an implantable loop recorder to increase the diagnostic yield in unexplained syncope: results from the PICTURE registry. Europace 13(2), 262–269 (2011).
•• This observational registry showed that syncope evaluations are unstructured which results in low diagnostic yield. Some tests are repeated many times, patients undergo various expensive diagnostic tests with low diagnostic yield and see three specialists without receiving a diagnosis.
11.
Edvardsson N, Wolff C, Tsintzos S, Rieger G, Linker NJ. Costs of unstructured investigation of unexplained syncope: insights from a micro-costing analysis of the observational PICTURE registry. Europace 17(7), 1141–1148 (2015).
12.
Rogers G, O'Flynn N. NICE guideline: transient loss of consciousness (blackouts) in adults and young people. Br. J. Gen. Pract. 61(582), 40–42 (2012).
13.
Shen WK, Sheldon RS, Benditt DG et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. J. Am. Coll. Cardiol. 70(5), e39–e110 (2017).
14.
Shaw DB, Kekwick CA, Veale D, Gowers J, Whistance T. Survival in second degree atrioventricular block. Br. Heart J. 53, 587–593 (1985).
15.
Srinivasan NT, Schilling RJ. Sudden cardiac death and arrhythmias. Arrhythmia Electrophysiol. Rev. 7(2), 111 (2018).
16.
Krahn AD, Klein GJ, Yee R, Hoch JS, Skanes AC. Cost implications of testing strategy in patients with syncope: randomized assessment of syncope trial. JACC 42(3), 495–501 (2003).
17.
Kenny RA, Brignole M, Dan GA et al. Syncope Unit: rationale and requirement-the European Heart Rhythm Association position statement endorsed by the Heart Rhythm Society. Europace 17(9), 1325–1340 (2015).
•• This EHRA position statement explains the benefit and supporting evidence of a syncope unit and provides practical guidance how it is managed and evaluated.
18.
Ruwald MH, Hansen ML, Lamberts M et al. Accuracy of the ICD-10 discharge diagnosis for syncope. Europace 15(4), 595–600 (2012).
Information & Authors
Information
Published In
Pages: 659 - 666
PubMed: 32639168
Copyright
© 2020 Future Medicine Ltd.
History
Received: 17 April 2020
Accepted: 19 May 2020
Published online: 8 July 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Burden of recurrent syncope and injuries and the usefulness of implantable cardiac monitors: insights from a nationwide longitudinal cohort analysis. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0059
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Sandeep A. Saha, Sarah Rosemas, Shantanu Sarkar, Veronica Ramos, Andrew P. Radtke, Shubha Majumder, Mirko De Melis, Jiani Zhou, J. Jason Sims, A Large, Real‐World Cohort Analysis of Arrhythmia Detection and Therapeutic Interventions in Patients With Insertable Cardiac Monitors and Long‐Term Monitoring, Journal of Cardiovascular Electrophysiology, 10.1111/jce.70214, 37, 2, (359-373), (2025).
- Aaron Lau, Minhaz Ahmed, Steve Parry, A Quality Improvement Project to Improve Syncope Care Through Structured Triage and Risk Stratification (STARS), Cureus, 10.7759/cureus.93043, (2025).
- Camille G. Frazier-Mills, Lawrence C. Johnson, Ying Xia, Sarah C. Rosemas, Noreli C. Franco, Sean D. Pokorney, Syncope Recurrence and Downstream Diagnostic Testing after Insertable Cardiac Monitor Placement for Syncope, Diagnostics, 10.3390/diagnostics12081977, 12, 8, (1977), (2022).