Type I collagen matrix plus polyhexamethylene biguanide antimicrobial for the treatment of cutaneous wounds
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Determine the effectiveness of purified native type I collagen matrix plus polyhexamethylene biguanide antimicrobial (PCMP) on cutaneous wounds. Materials & methods: A prospective cohort study of 307 patients (67 venous leg ulcers, 62 diabetic foot ulcers, 45 pressure ulcers, 54 post-surgical wounds and 79 other wounds) was conducted. Results: Cox wound closure for PCMP was 73% at week 32. The median time to wound closure was 17 weeks (Kaplan–Meier). The incidence of PCMP-treated wounds showing >60% reductions in areas, depths and volumes were 81, 71 and 85%, respectively. Conclusion: PCMP demonstrated clinically meaningful benefits to patients with various types of cutaneous wounds.
Clinical Trial registration number: NCT03286452.
This is the first prospective, noninterventional, multicenter study to examine the ‘real-world’ effectiveness of purified native cross-linked extracellular matrix (ECM) plus polyhexamethylene biguanide (PHMB) antimicrobial (PCMP) barrier on cutaneous wounds including acute and chronic wounds. Effectiveness results demonstrated at 28 US wound care facilities and in 307 PCMP (PuraPly AM®; Organogenesis Inc., MA, USA) patients treated in the PCMP registry (Real-World Effectiveness Study of PuraPly AM on Wounds) are reported. The PCMP registry was a postmarketing, prospective, cohort study (ClinicalTrials.gov; registration no. NCT03286452) conducted from 2017 to 2019. PCMP wounds were assessed for: frequency of wound closure, time to wound closure and reductions from baseline in wound measurements. Retrospective analyses of chronic wound care costs are taken under consideration and discussed. Though anecdotal, observational and interim data have supported the use of PCMP as a useful adjunct in the management of various cutaneous wounds, collection of additional real-world data from a larger patient population with several types of wounds treated in multiple clinical practice settings was warranted [1–3]. The results of the PCMP registry cohort study are presented in this report.
PCMP is a US FDA class II medical device, 510(k)-cleared #K051647 [4]. In the USA, PCMP is marketed and classified as for reimbursement by the Centers for Medicare and Medicaid Services as a skin substitute [5,6]. PCMP is intended for the management of wounds, acts as an effective barrier to resist microbial colonization and reduces the number of microbes penetrating to the wound bed. PCMP may be used for the management of: partial and full-thickness wounds, pressure ulcers (PRUs), venous leg ulcers (VLUs), diabetic foot ulcers (DFUs), chronic vascular ulcers, tunneled/undermined wounds, post-surgical wounds (PSWs; e.g., donor sites/grafts, post-Moh’s surgery, postlaser surgery and wound dehiscence), trauma wounds (abrasions, lacerations, second-degree bums and skin tears) and draining wounds [7]. PCMP consists of a collagen sheet coated with 0.1% PHMB. It is supplied in the form of dry sheets and packaged in sterile, sealed single pouches.
Even with good wound care practiced according to recognized guideline therapy recommendations, high proportions of chronic wounds fail to heal by 6 months postinitiation of wound care therapy [8–10]. For example, in VLUs, up to 75% of patients fail to achieve healing with the use of standard compression therapy [11]. Longer term follow-up of VLU patients showed that up to 50% of ulcers remain unhealed at 6 months, 20% at 2 years, and approximately 8% at 5 years [12]. In DFUs, up to 70% of ulcers have been reported as nonhealed by 6 months [13]. All chronic wounds are associated with greater risks of infections, osteomyelitis, amputations and death [9,14,15]. There is a 150-fold greater risk of amputation in patients with foot infections [16]. The 5-year mortality rate for amputated patients has been reported as up to 50%. Postamputation, the 50%, 5-year mortality rate is higher than the most commonly occurring cancers [17]. Chronic wounds of all types result in serious clinical consequences, poor quality of life for patients and impose burdensome healthcare costs that affect society as a whole [17–21]. Claims data show that 15% of Medicare beneficiaries are affected by chronic wounds with an estimated annual cost of over US$30 billion [17,19,22,23].
Key considerations regarding the activity of PCMP (purified native type I collagen matrix plus PHMB antimicrobial) at the site of the wound bed are: collagen and ECM proteins, biofilms and bioburden, and PHMB as a broad spectrum antimicrobial that disrupts the formation of biofilm. First, the effects of collagen on the wound environment are critical to the process of wound repair. Although collagen was originally believed to simply provide structural support for the wound healing process, collagen and collagen-derived fragments have been shown to control a variety of cellular functions, including cell shape and differentiation, cell migration, and the synthesis of a number of proteins. Collagen-based wound dressings have also been reported to have the ability to absorb wound exudates and maintain a moist wound environment [24]. Second, the pathogenesis of chronic nonhealing wounds involves multiple and interrelated variables including increased bioburden and the formation of biofilm [25,26]. Biofilm occurs when bacteria adhere to tissue, proliferate and extrude ECM proteins to form a polymer matrix enclosing the bacteria themselves [27,28]. The prevalence of biofilms in chronic wounds has been reported to be 78% in in a meta-analysis of nine studies and 185 chronic wounds [29]. There is considerable evidence that shows that biofilm impairs wound healing [25,30]. Living bacteria encased within biofilm are difficult to eliminate using topical or systemic antibiotics alone [28,31,32]. Biofilm can impair wound healing by prolonging the inflammatory phase of the wound healing cascade thereby stalling the wound healing process. The normal progression of the phases of wound healing becomes disrupted, and a chronic inflammatory state follows. The persistence of an ineffective inflammatory state is a defining characteristic of chronic wounds. Third, PHMB is a cationic topical antimicrobial that strongly binds to bacterial cell walls and membranes. PHMB has demonstrated broad spectrum, potent antimicrobial activity against both Gram-positive and Gram-negative bacteria, and in particular against bacteria that form biofilm [33]. Studies have shown high binding of PHMB to biofilm matrix and a strong dose–response effect [34]. PHMB has not been demonstrated to be systemically absorbed when applied topically on intact skin or cutaneous wounds [33,35]. Importantly, PHMB has been used for the treatment of infections of chronic wounds including localized infections associated with VLUs [36].
Analysis of Medicare beneficiaries in calendar year 2018 showed that approximately 8.2 million people had wounds with or without infections [37,38]. With rates as high as 50–75% of chronic wounds remaining unhealed after 6 months of using existing therapies, new chronic wound treatment regimens are needed to improve heal rates and decrease wound-related complications [11–13,39]. The authors hypothesized that PCMP may affect fundamental wound repair processes in ways that may benefit patients with chronic wounds.
Materials & methods
Study design
This was a postapproval, open-label, prospective, multisite registry examining the real-world effectiveness of PCMP on various types of wounds. The purpose of this prospective, cohort study was to investigate the effectiveness of PCMP in the treatment of skin wounds over a 32-week study period. The primary analyses were frequency of and time to wound closure by 32 weeks. The key secondary analyses were determination of the incidence of wounds that demonstrated >60% reduction in wound area and depth from baseline, and the incidence of wounds that demonstrated >75% reduction in wound volume from baseline. Male and female patients, 18 years or older, with target wounds suitable for the use of PCMP as defined by inclusion/exclusion criteria were eligible for participation in the PCMP registry. Approximately 300 patients from approximately 30 US sites were to be enrolled. The choice to initiate treatment of PCMP was made by the treating physicians independent of and prior to any decision to participate in the PCMP registry. Since the PCMP registry employed a prospective, noninterventional study design to collect information regarding the use of PCMP, no experimental intervention control group was involved.
Registry plan
Patients’ wounds were assessed and received standard of care therapies as determined by the physician investigators. Standard of care treatments administered were defined as wound therapy regimens consistent with recognized wound care guidance documents and investigators’ institutional treatment algorithms [40–42]. One wound treatment regimen practiced at many participating clinical sites follows: wounds were cleansed and debrided at the initial visit. After wound bed preparation, PCMP was applied, wetted with normal saline and immobilized using steri-strips. Next, a moist dressing (e.g., hydrogels, hydrocolloids and alginates) and a nonstick layer were applied. Each PCMP sheet remained on the study wound for 1 week. Low evaporative dressings (e.g., adaptic or xeroform) were used as secondary dressings. The greatest proportion of patients participating in the registry suffered from one of three types of chronic wounds. VLU patients were placed in compression wraps, DFU patients used fixed ankle walker boots for off-loading and PRU patients used alternating pressure surfaces/low-air-loss beds. PCMP would then be applied weekly or until wound closure. Wound dressings were applied at the clinical sites through week to the end of study (EOS; week 32).
Patients
Sterling Institutional Review Board (registration no. IRB00001790) reviewed and approved the registry protocol, and the study complied with current International Council for Harmonization Good Clinical Practice guidelines and 21 CFR parts 11, 50, 56 and applicable regulations. Written informed consent to participate in the registry was obtained for all patients prior to any study procedures being performed. One target wound per patient was identified for study inclusion and was followed for up to 32 weeks. Patients were at least 18 years of age with a cutaneous wound appropriate for receiving PCMP as defined by registry entry criteria and who had not had PCMP applied previously to the target wound. The PCMP registry was designed to assess the effectiveness of PCMP across a wide range of wound types in a real-world clinical setting. Physician investigators were not limited by the type of wound to include in the study. The study population included patients ≥18 years of age having a partial or full-thickness wounds appropriate for receiving PCMP. Appropriate wounds included: pressure ulcers, venous ulcers, diabetic ulcers, chronic vascular ulcers, tunneled/undermined wounds, surgical wounds (e.g., donor site/grafts, post-Mohs’ surgery, postlaser surgery, podiatric surgery wound and wound dehiscence), trauma wounds with tissue damage (e.g., abrasion, laceration, second-degree burn and skin tear) and draining wounds. Key exclusion criteria included patients with: third-degree burns, known sensitivity to PHMB, known sensitivity to porcine materials and whose target wound was previously treated with PCMP.
The criteria used to categorize ulcers and PSWs into different categories relied upon clinical assessments of patients’ signs and symptoms. Diagnostic testing was used to supplement clinical evaluations of patient histories and physical examinations. VLUs were defined by: presence of clinical signs and symptoms of venous ulceration, such as hyperpigmentation of the surrounding skin, edema, varicosities, lipodermatosclerosis and dermatitis; absence of significant arterial insufficiency as determined by ankle-brachial index (e.g., ABI >0.65); and evidence of venous insufficiency by venous duplex assessment, air plethysmography or photoplethysmography with venous refilling time being less than 20 s. The key criteria for DFUs were patients with type 1 or 2 diabetes with partial or full-thickness neuropathic ulcers as determined by physical examination (e.g., monofilament test to assess peripheral neuropathy). Dorsalis pedis and posterior tibial pulses as assessed by palpation or audible by doppler were required to establish a pathophysiology consistent with DFUs and not ischemic ulcers or an ulcers of mixed etiology. The main DFU exclusion criteria was the presence of an infection at the ulcer site. PRUs were defined as localized injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear [43]. Categorization of an ulcer as a PRU was based on staging on type of tissue visualized or palpated. PRUs over anatomical locations including sacrum, coccyx, greater trochanter, ischial tuberosity, calcaneus and lateral malleolus were included. PRU stages II–IV were included that were defined by involvement of skin layers extending from the papillary and reticular dermis (partial and full-thickness), subcutaneous fat (full thickness), to exposed tendon, muscle or bone (full thickness). PSWs were categorized as surgical incisions sutured together by a margin approximation dressing or device after an operative procedure that fail to heal. PSWs that failed to heal primarily due to dehiscence were defined by the separation of the incision line prior to complete healing resulting in an open wound. Partial dehiscence of a surgical wounds presented as superficial layers of tissue being reopened. Complete dehiscence presented as all tissue layers being separated with underlying tissue and organs being exposed and sometimes protruding through the wound opening. Other symptoms that characterized PSW dehiscence included broken sutures before the wound had healed, renewed pain, bleeding and drainage from the surgical wound site. Wounds types assessed as being of mixed etiologies (e.g., both venous and atrial insufficiency; diabetes and pressure characteristics), or wound types present in a few patients carrying diagnoses other than VLU, DFU, PRU or PSW were categorized as, ‘other’.
Data collection
Physician investigators were responsible for collecting and recording the data for the registry in standardized electronic case report forms. The data collection system, MedNet® (NJ, USA) was the interface that allowed sites to enter data electronically and was built with data quality checks and prompts programmed into respective electronic case report forms to ensure data quality. Periodic data cleaning, data reviews and data reconciliation were performed by Worldwide Clinical Trials, Inc. (NC, USA). Data queries were issued for site clarification for any discrepancies noted during data review. Accurate records of the clinical data generated from this study were maintained according to Good Clinical Practices requirements. No interim analyses were completed during the course of the registry.
Digital photography was used to image index wounds both pre- and post-PCMP treatment at each study visit. Wound measurements were also collected for all patients at each study visit in the PCMP registry. The maximum length, maximum width and maximum depth of the index wound was measured before use of PCMP at each study visit through to the EOS. Investigators were instructed to measure the greatest length of the open wound end-to-end perpendicular (90○ angle) to width. The width was measured at the widest width of the open wound side to side perpendicular to the length. Maximum depth was measured by moistening a cotton-tipped applicator with normal saline. The applicator tip was placed in the deepest aspect of the wound and the distance to the skin level was measured. Cross-sectional area (cm2) was electronic data collection calculated by computerized algorithms if length and width were entered. Wound volume: (cm3) was electronic data collection calculated by computerized algorithms if length, width and depth were entered.
Statistical analysis
All statistical analyses were performed with the understanding that the PCMP registry was a prospective, cohort, noninterventional study design, where no treatment randomization was involved. Continuous data were summarized using descriptive statistics: count (n), mean, standard deviation and median. Categorical data were described using frequencies and percentages. All statistical analyses were performed using SAS® 9.4 (SAS Institute, NC, USA).
To assess the effectiveness of PuraPly AM in real-world clinical settings, the following were measured: actual and percent change in wound area from baseline through the EOS using wound details (wound length [cm], wound width [cm], maximum wound depth [mm], cross-sectional area [cm2] and wound volume [cm3]), and time to wound closure for each individual patient, if wound closure occurred, using dates and wound variables (baseline wound dates, wound characteristics, follow-up dates and/or EOS date).
The primary efficacy end point of the study was defined as: time to and frequency of complete wound closure (i.e., 100% wound closure) by or on 32 weeks. Complete wound closure (referred to as wound closure in this article) was defined as: full epithelialization of the wound with the absence of drainage. Epithelialization was defined as a layer of epithelium visible on the wound surface.
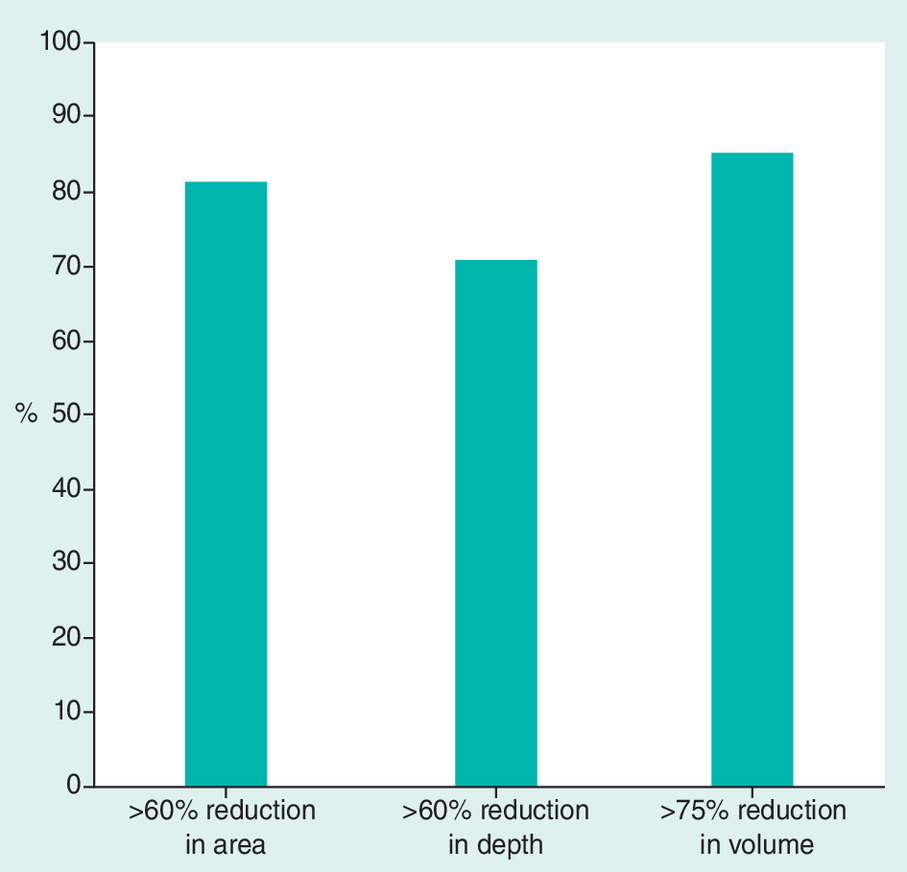
Secondary efficacy end points were defined as: the proportion of subjects achieving >60% reduction in wound area from baseline (i.e., >60% epithelialization defined as a layer of epithelium visible on the wound surface); the proportion of subjects achieving >60% reduction in wound depth from baseline; and the proportion of subjects achieving >75% reduction in wound volume from baseline.
Frequency of wound closure (i.e., wound closure rates) as a function of time (weeks) was determined using the Kaplan–Meier (K–M) time to event analysis (SAS 9.4) through week 32 for: all wounds, and subgroups of wounds treated such as VLUs, DFUs, PRUs, PSWs and other (wounds not meeting the diagnostic criteria for any of the identified wound types occurring in fewer than five patients). K–M time to event analysis was used to determine the median time to wound closure.
A forward selection Cox proportional hazards regression model that adjusted for patient demographics (i.e., age, race, sex and BMI) and wound characteristics (i.e., area, depth, volume and age of the ulcer at baseline) was performed to compute the adjusted wound closure rates for all wounds, VLUs, DFUs, PRUs, PSWs and other wounds from PCMP treatment application day 0 through to week 32. The Cox analyses were used to estimate the frequency of wound closure at every time point that patients were evaluated.
All analyses were intent to treat and included data from all patients who received PCMP in the registry (Figures 1–4).


Results
Each subject had one ulcer identified as the index ulcer for treatment with PCMP. There was a total of 307 PCMP-treated wounds (all wounds [n = 307]). Of these 307 wounds: 67 were VLUs; 62 were DFUs; 45 were PRUs; 54 were PSWs and 79 were other wounds. Baseline patient demographics, wound characteristics and treatment characteristics are shown for all patients in the PCMP registry (Table 1). The majority of patients were males (53.1%) and the median age was 70 years. Seventy-two percent of the PCMP-treated patients were ≥65 years of age. At the first treatment application, the mean wound area was 12.9 cm2, the mean wound depth was 5.2 mm and the mean wound volume was 11.2 cm3 (Table 1).
| Patient, wound and treatment characteristics | PCMP (n = 307) |
|---|---|
| Age (years) Mean ± SD Median | 70.3 ± 14.2 70.0 |
| Age group (years), n (%) <65 ≥65 | 86 (28.0) 221 (72.0) |
| Sex, n (%) Female Male | 144 (46.9) 163 (53.1) |
| Number of ulcers treated per patient Mean ± SD Median | 1.0 ± 0 1.0 |
| Wound duration (days) Mean ± SD Median | 96.2 ± 192.0 60.0 |
| Wound area (cm2) Mean ± SD Median | 12.9 ± 21.3 5.0 |
| Wound depth (mm) Mean ± SD Median | 5.2 ± 9.7 2.0 |
| Wound volume (cm3) Mean ± SD Median | 11.2 ± 36.2 1.7 |
| Number of applications Mean ± SD Median | 5.2 ± 3.1 5.0 |
| Days between applications Mean ± SD Median | 9.7 ± 5.1 7.7 |
PCMP: Type I collagen matrix plus polyhexamethylene biguanide antimicrobial; SD: Standard deviation.
The average number of treatment applications used in the PCMP wounds was 5.2 (Table 1). A total of 21.8% of PCMP patients received one or two applications, and less than 2% received more than ten applications. For patients receiving multiple applications, the median interval between PCMP applications was 9.7 days (Table 1).
The primary end point (Cox) of wound closure for all wounds (n = 307) was 52, 62 and 73% at week 20, 26 and 32, respectively (Figure 1). For all 307 of these PCMP wounds, the incidence of achieving greater than a 60% reduction in baseline area and depth was 81 and 71%, respectively (Figure 2). In addition, the incidence of wounds demonstrating greater than a 75% reduction in baseline volume was 85% (Figure 2).
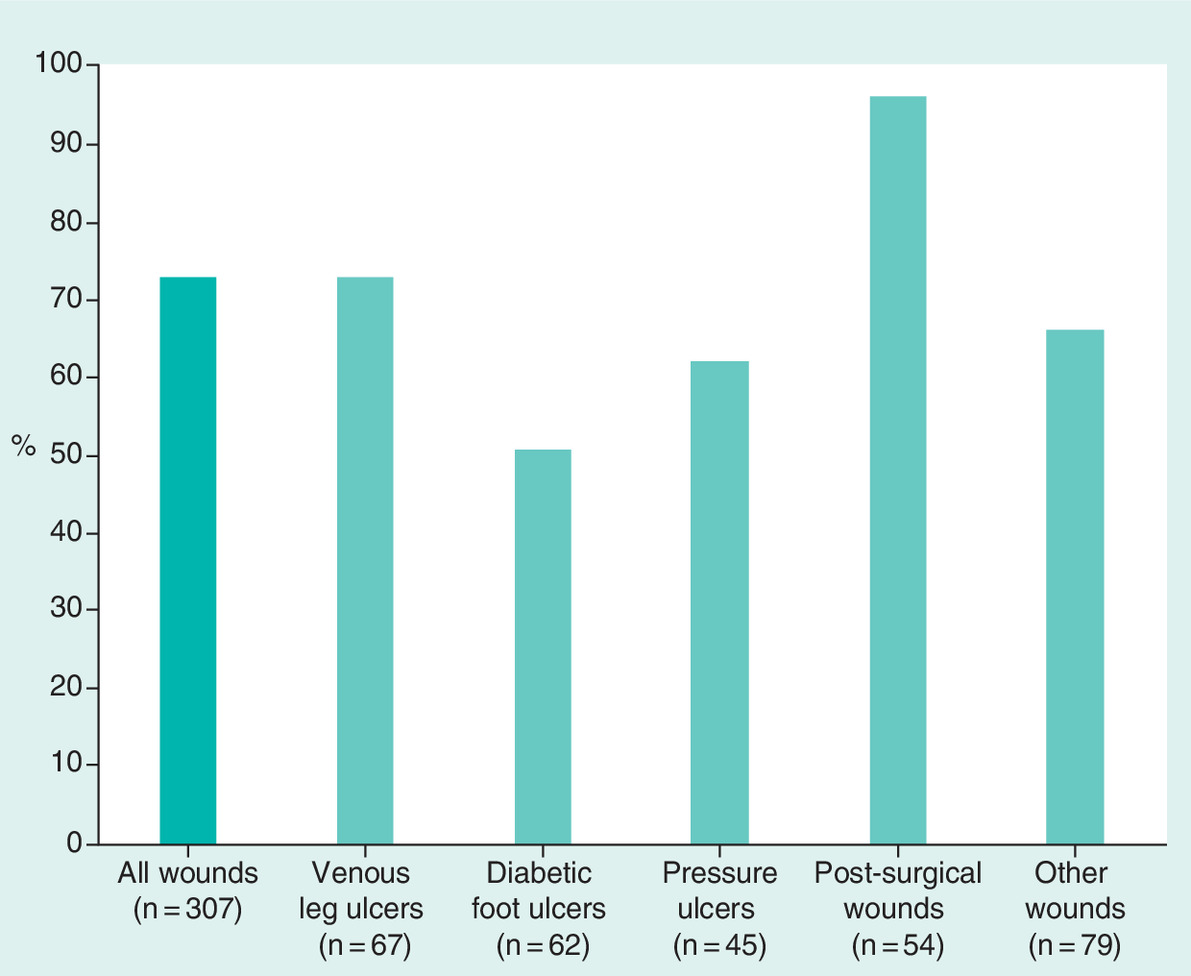
Cox adjusted estimates of frequencies of wound closure at week 32 demonstrated not only the frequency (%) of wound closure for all wounds (73%), but also the frequencies of wound closure for VLUs (73%), DFUs (51%), PRUs (62%), PSWs (96%) and other wounds (67%) (Figure 3). Cox wound closure frequencies at week 26 were also computed for all wounds (62%), VLUs (64%), DFUs (50%), PRUs (51%), PSWs (67%) and other wounds (67%) (Figure 3).
The K–M median time to wound closure for all 307 enrolled in the registry was 17 weeks. Using the same K–M method of analysis, the times to wound closure for VLUs, DFUs, PRUs, PSWs and other wounds were 22, 31, 32, 12 and 14 weeks, respectively (Figure 4).
Safety data were actively collected throughout the 32-week registry study. PCMP appeared to be well tolerated, and there were no adverse events (AEs) or serious AEs that were attributed or related to PCMP.
Discussion
The data show that the use of PCMP demonstrated clinically meaningful benefits to patients with skin wounds. The PCMP registry included all wounds (n = 307) that was comprised of 67 (22%) VLUs; 62 (20%) DFUs; 45 (15%) PRUs; 54 (18%) PSWs; and 79 (26%) other wounds. Given the intended uses for PCMP (wounds with the exception of third-degree burns) defined by FDA’s 510(k) marketing clearance, the wounds analyzed in this cohort study proved to be reflective of a postmarketing patient population and are best examined as an aggregate, single wound population. K–M time to event analysis showed that for all wounds (n = 307), the median time to wound closure was 17 weeks, and the Cox-derived frequency of wound closure was 73%. In addition, a more subjective end point of ‘achieving treatment goals’ was also prospectively identified in the registry protocol. Achieving treatment goals was defined as demonstrating improvements in the wound bed condition such as increased, healthy granulation tissue, reduced exudate and readiness for grafting or treatment with other advanced skin substitutes. Using these criteria, 86% of all PCMP patients met clinicians’ treatment goals. Overall clinical improvements to patients treated with PCMP were demonstrated by the more subjective determination of ‘achieving treatment goals’. Consistent with clinical assessments of ‘achieving treatment goals’, objective wound measurements showed reductions in wound dimensions from baseline. The percentages of PCMP wounds that demonstrated >60% reductions in wound area (cm2) and depth (mm) were 81% (250 of 307) and 71% (221 of 307), respectively. Wound area reductions of >50 and >60% from baseline have previously been proven to be highly predictive surrogate end points for healing [44–46]. In this trial, we used a strict cutoff of >60% partial wound closure and >60% wound depth reduction as surrogates for longer term healing. Large, pooled randomized controlled trial (RCT) databases of over 35 thousand wounds have shown rates of 70% or higher in sensitivity and specificity of predicting wound healing when >40% wound area reductions from baseline were observed at 4 weeks [45]. One retrospective cohort study (39,918 neuropathic wounds on 20,213 individuals) showed correct classification of healed or not healed by 20 weeks of 70% [45]. The wound area reduction data reported in this study are intended to provide clinically meaningful information that may help guide treatment decisions for the management of the most common chronic wounds seen in the community. In addition, we showed reductions in wound volumes consistent with the reductions in area and depth. Objective assessment metrics used in the PCMP registry, support the conduct of formal RCTs to assess beneficial effects on patients’ quality of life, activities of daily living and ability to work.
PCMP registry clinical outcomes were in a primarily elderly population with large, deep wounds, of long durations (age of the wounds prior to treatment with PCMP) (Table 1). Of the general population studied in the registry, 72% (221 of 307 patients) were ≥65 years of age. US Medicare is available for patients age 65 or older, and approximately 15% of the US population (45 million people) were enrolled in medicare as their primary health insurance at the time of initiation of the PCMP registry [47]. Baseline characteristics of wounds treated included those that were of long duration (96 days), large size (12.9 cm2), deep (5.2 mm) and high volume (11.2 cm3). These wound measurement parameters at the first day of treatment application have previously been shown to be negative risk factors for healing (Table 1) [48–50]. It appears that PCMP successfully resulted in wound closure in a patient population who most often present with difficult-to-heal wounds refractory to previous treatments.
A comparison between the results of three previous PCMP observational studies, one interim analysis of the PCMP registry (n = 63), and the completed RESPOND registry (n = 307) shows comparable clinical outcomes. In one prospective case series of 41 patients treated for various types of wounds (VLUs, DFUs, PRUs and PSWs), heal rates, mean percent wound closure from baseline and time to healing were reported. At 12 weeks, most (73.2%) wounds reduced in area from baseline and many (63.4%) had reached a ≥70% reduction in area. Complete wound closure was reported in 37% of wounds by or on 12 weeks. The duration of study in this 41 patient case series was 20 weeks shorter the PCMP registry here reported. Complete closure was achieved in many types of wounds, including surgical and trauma wounds, PRUs, DFUs and VLUs. The time to complete wound closure was 6.7 weeks whereas the duration of the wounds treated was 103 weeks [2]. A small case series (n = 5) with PCMP demonstrated an average time to complete wound closure of 6.8 weeks [51]. PCMP was reported to be well tolerated with no related systemic or localized AEs. Nine wounds treated with PCMP in another observational case series showed that six (66.7%) of treated wounds healed in an average of ten weeks. The three wounds that failed to heal showed improvements in granulation tissue and reductions in wound area [1]. In an interim analysis of 63 wounds treated in the PCMP registry, the median baseline wound area was 6.5 cm2, and the mean wound duration at baseline was 4 months. Of the 63 wounds, 43 (68.3%) achieved complete wound closure. Mean time to closure for PCMP wounds that healed was 5 weeks [3]. Comparing the heal rates from other PCMP studies with the heal rates here reported shows comparability regardless of the clinical setting and the wound type when duration of the various studies are taken into consideration. It is notable that because of a robust number of patients (n = 307) participating in the RESPOND, the median time to healing for All patients (rather than mean times to healing for only those patients who healed) was able to be computed using intent to treat principles and accepted, recognized K–M methodology. The median time to healing in the completed RESPOND registry of 17 weeks has been shown to compare favorably with other skin substitutes also reporting K–M median times to healing (time in weeks ranging from 20 to 43) [52–55]. The results of these PCMP reports of healing in smaller, observational case series or interim reports are generally consistent with the findings of the completed (n = 307) PCMP noninterventional, prospective registry study.
Regardless of wound type, general local wound management principles exist. The Wound Healing Society has put forth the ‘TIME’ paradigm to address key elements associated with impaired wound healing [56]. Wound treatments administered in the PCMP registry adhered to all elements of TIME. The acronym refers to four considerations in treating cutaneous wounds. ‘T’ refers to recognizing specific tissue deficits as well and using debridement methods to address the presence of devitalized or necrotic tissue. ‘I’ describes management of inflammation or infection within and surrounding the wound site. ‘M’ refers to assessment and management of moisture balance from maceration to desiccation to achieve a moist wound environment. ‘E’ defines evaluations of wound edge quality, observations of undermining of epidermis, identification of devitalized and hyperkeratotic periwound tissue, and assessments of the extent of re-epithelialization [56].
Treating the sequala of nonhealing chronic wounds such as infection, tissue necrosis, gangrene, edema, osteomyelitis and amputation result not only in direct costs that can be quantitated, but also indirect costs that are more difficult to analyze [16,57–59]. In a retrospective analysis of only the direct costs related to wound care, US Medicare data showed that total Medicare spending estimates for all wound types ranged from US$28 to US$97 billion [37]. Using a healthcare economics model for one chronic wound type (VLUs), the potential cost savings of using therapies more effective (demonstrating shorter times to healing) than standard dressings may be addressed. The treatment costs of VLUs alone on the healthcare system was analyzed for 81,000 patients, and the direct costs were calculated as US$18 billion annually [60]. VLU-related costs for nonhealed wounds were over US$500 per patient per week higher when compared with healed VLUs. Of this amount, approximately US$400 per week per patient was for selected services considered directly related to VLU treatment [60]. Applying the figure of US$400 in cost savings per patient per week that a wound is healed, the total cost savings of using a wound care treatment that results in faster healing may be estimated. Using the median time to healing data determined in the PCMP registry (17 weeks) and previously published median times to healing data, the differences in direct wound care treatment costs per patient per week were able to be calculated between PCMP and four other skin substitutes. Estimated times to healing (K–M) in recent comparative effectiveness research studies (CERs) have been reported in weeks as: 20, 26, 30 and 43 for viable cryopreserved placental membrane (vCPM), dehydrated human amniotic membrane, fetal bovine collagen dressing and small intestinal submucosa (SIS), respectively [52–55]. Using the cost model referenced above, a 3 week difference in median time to wound closure (17 weeks for PCMP vs 20 weeks for vCPM) could result in estimated cost savings per patient of US$1200. At the upper range of cost savings (17 weeks for PCMP vs 43 weeks for SIS), a potential cost savings per patient of US$10,400 is calculated. It should also be noted that direct costs of chronic wound treatment shown are indirectly proportional to the frequency of healing with the lowest heal rates associated with the highest costs. Using the skin substitutes listed above, frequencies of wound closure were 46% (vCPM), 47% (dehydrated human amniotic membrane), 46% (fetal bovine collagen dressing) and 46% (SIS) [52–55]. Large sample sizes and direct head-to-head comparisons between the various skin substitutes are needed for accurate healthcare economic analyses.
The PCMP registry shares limitations in common with all postmarketing registry studies. The PCMP cohort registry (RESPOND) was of an open-label, noninterventional design with no comparator treatment group. The main strength of the study is the large group of patients that were enrolled (n = 307), while the main limitation is the lack of control group. Without a comparator, there is no way of being completely certain that treated wounds would not have had similar healing with other skin substitutes or standard of care therapies. Additionally, comparisons of findings with retrospective, nonconcurrent controls or between studies should be interpreted with caution. However, In this PCMP registry there existed practical and other reasons not to include a placebo group. The use of a placebo in clinical research continues to be a topic of debate. Some argue that the use of placebos is often unethical because alternative study designs would produce similar results with less risk to individual research participants [61]. Patients with nonhealing wounds are at risk for infection, cellulitis, osteomyelitis, sepsis and even death if left untreated or poorly treated. Critics of placebo-controlled trials cite article 11.3 of the Declaration of Helsinki: “In any medical study, every patient including those of control group, if any should be assured of the best proven diagnostic and therapeutic methods and no patient should suffer from unnecessary pain” [62]. Given the circumstances that PCMP has been subjected to US FDA premarket evaluation, available by prescription only (i.e., restricted to use by order of a physician or properly licensed practitioner), and marketed in USA for use in the management of cutaneous wounds (with the exception of third-degree burns), comparisons with other wound care products that are not currently approved or cleared for marketing for use in similar wounds proves challenging. Practical reasons for a noninterventional study design included potential, prolonged times to enrollment. While RCTs represent the gold standard in evaluating healthcare interventions, it is common that <40% and as few as 10% of patients screened for a RCT are randomized to receive study treatment [63]. The PCMP registry was intended to provide physicians with real-world clinical outcomes data prospectively collected in a systematic way on a variety of wounds and also to inform future RCTs for the study of specific wound types. By determining heal rates in this single arm study, the treatment effect size between PCMP and comparators may be used more precisely estimate sample sizes in future studies limiting patient exposure to placebo and other controls. Practical considerations of collecting PCMP data on larger numbers of patients with different patient characteristics (age, race and sex), wound types (VLU, DFU, PRU and PSW), and wound characteristics (area, depth and volume) are advantages of using a noninterventional study design. Interventional studies with one or more control arms often necessitate stratification and/or more narrow inclusion/exclusion criteria. The PCMP registry was on open label study that carries risk of investigator bias. We attempted to address potential bias by only relying on wound measurements for our primary and all secondary analyses. Cox modeling that adjusted for multiple common risk factors was used to determine wound closure for all patients as well as chronic wound subgroups. Additional data and more detailed analyses would be needed for valid subgroup comparisons. Notably, the registry included 28 treatment facilities that were evenly distributed geographically across the USA. Treatment center as a variable was not found to be predictive of PCMP effectiveness. It should be noted that PCMP was used as an adjunct to standard of care therapy. Wounds included in this cohort study were unlikely to be considered for surgical interventions. Further specifics on PCMP relative costs would require a dedicated study targeted to healthcare economic outcomes. More cost–effectiveness information is needed than was available from this Registry. Moving forward, both RCTs and CER studies in a real-world setting would greatly contribute to our understanding of PCMP.
Conclusion
The PCMP registry of over 300 patients showed a 73% frequency of wound closure with a median time of 17 weeks. PCMP appears to be a useful adjunct in the treatment of various types of wounds. Subgroup analyses of wound types and CER studies are warranted.
•
This was the first prospective, large (307 patients), multicenter (28 sites), cohort study to assess the effectiveness of purified native type I collagen matrix plus PHMB, a broad spectrum antimicrobial (PCMP), for use on various types of nonhealing wounds.
•
PCMP was used on 307 wounds.
•
The number and percent in each wound type were: 67 (22%) venous leg ulcers (VLUs), 62 (20%) diabetic foot ulcers (DFUs), 45 (15%) pressure ulcers (PRUs), 54 (18%) post-surgical wounds (PSWs) and 79 (26%) other wounds.
•
Treatment with PCMP showed favorable wound closure rates for all wounds and all subgroups of wounds treated.
•
Wound closure rates (Cox analyses) for All, VLUs, DFUs, PRUs, PSWs and other wounds were computed as 73, 73, 51, 62, 96 and 67%, respectively.
•
Median time to healing (Kaplan–Meier survival analysis) for All, VLUs, DFUs, PRUs, PSWs and other wounds were demonstrated to be 17, 22, 31, 32, 12 and 14 weeks, respectively.
•
PCMP was associated with substantial reductions in wound areas, depths and volumes. PCMP showed a high incidence of >60% reductions in area (81%) and depth (71%), and >75% reductions in volume (85%).
•
PCMP may result in improved rates and times to wound closure than either of its primary components (type I collagen and PHMB) could achieve individually.
•
The RESPOND registry showed that the use of PCMP was associated with substantial reductions in wound area and notable rates of wound closure. PCMP use should be considered when managing chronic or acute wounds of various etiologies.
•
Randomized controlled studies (RCTs) and comparative effectiveness research (CER) studies of real-world data comparing PCMP with other skin substitute products for the management multiple chronic wound types are warranted.
Author contributions
All authors made substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; and drafted the work or revised it critically for important intellectual content; and gave final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The authors wish to acknowledge Virtu Stat, Ltd. (PA, USA) for statistical support.
Financial & competing interests disclosure
This study was funded by Organogenesis, Inc.; ML Sabolinski serves as a consultant for AOBiome, Oppilan, Neumedicines, Organogenesis, Inc. and Allergan. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval and have followed the principles outlined in the Declaration of Helsinki for all human investigations. In addition, for all subjects participating in this prospective cohort study, informed consent has been obtained prior to any study procedures being performed.
Data sharing statement
The manuscript reports original clinical research from a prospective cohort study (registry). Individual subject’s wound assessments will be shared upon request postcompletion of the study and publication of the subjects’ data. ICFs, IRB approvals, the study protocol will be shared as requested.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Lintzeris D, Vernon K, Percise H. Effect of a new purified collagen matrix with polyhexamethylene biguanide on recalcitrant wounds of various etiologies: a case series. Wounds 30(3), 72–78 (2018).
2.
Oropallo AR. Use of native type I collagen matrix plus polyhexamethylene biguanide for chronic wound treatment. Plast. Reconstr. Surg. Glob. Open 7(1), e2047 (2019).
3.
Bain MA, Thibodeaux KT, Speyrer MS, Carlson E, Koullias GJ. Effect of native type I collagen with polyhexamethylene biguanide antimicrobial on wounds. Plast. Reconstr. Surg. Glob. Open 7(6), e2251 (2019).
4.
510(k) Premarket Notification. (2020). https://www.accessdata.fda.gov/SCRIPTS/cdrh/cfdocs/cfPMN/pmn.cfm?ID=18685
5.
AHRQ Technology Assessment Program. Skin substitutes for treating chronic wounds – draft technical brief. (2019). https://www.ahrq.gov/sites/default/files/wysiwyg/research/findings/ta/drafts-for-review/skin-substitutes_draft.pdf
6.
CMS Manual System. Pub 100-04 medicare claims processing. (2020). https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/2019Downloads/R4204CP.pdf
7.
510(K) SUMMARY K051647. (2020). https://www.accessdata.fda.gov/cdrh_docs/pdf5/K051647.pdf
8.
Lavery LA, Davis KE, Berriman SJ et al. WHS guidelines update: diabetic foot ulcer treatment guidelines. Wound Repair Regen. 24(1), 112–126 (2016).
9.
Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv. Wound Care 4(9), 560–582 (2015).
10.
Hingorani A, LaMuraglia GM, Henke P et al. The management of diabetic foot: a clinical practice guideline by the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine. J. Vasc. Surg. 63(Suppl. 2), S3–S21 (2016).
11.
O'Meara S, Cullum NA, Nelson EA. Compression for venous leg ulcers. Cochrane Database Syst. Rev. (1), CD000265 (2009).
12.
Kurz X, Kahn SR, Abenhaim L et al. Chronic venous disorders of the leg: epidemiology, outcomes, diagnosis and management. Summary of an evidence-based report of the VEINES task force. Venous Insufficiency Epidemiologic and Economic Studies. Int. Angiol. 18(2), 83–102 (1999).
13.
Margolis DJ, Kantor J, Berlin JA. Healing of diabetic neuropathic foot ulcers receiving standard treatment. A meta-analysis. Diabetes Care 22(5), 692–695 (1999).
14.
Gordois A, Scuffham P, Shearer A, Oglesby A, Tobian JA. The health care costs of diabetic peripheral neuropathy in the US. Diabetes Care 26(6), 1790–1795 (2003).
15.
Lavery LA, Armstrong DG, Wunderlich RP, Mohler MJ, Wendel CS, Lipsky BA. Risk factors for foot infections in individuals with diabetes. Diabetes Care 29(6), 1288–1293 (2006).
16.
Järbrink K, Ni G, Sönnergren H et al. Prevalence and incidence of chronic wounds and related complications: a protocol for a systematic review. Syst. Rev. 5(1), 152 (2016).
17.
Rice JB, Desai U, Cummings AKG, Birnbaum HG, Skornicki M, Parsons NB. Burden of diabetic foot ulcers for medicare and private insurers. Diabetes Care 37(3), 651–658 (2014).
•• A clear wound economic model with an analysis of the Medicare database.
18.
Hicks CW, Selvarajah S, Mathioudakis N et al. Trends and determinants of costs associated with the inpatient care of diabetic foot ulcers. J. Vasc. Surg. 60(5), 1247–1254.e2 (2014).
19.
Rice JB, Desai U, Cummings AKG, Birnbaum HG, Skornicki M, Parsons N. Burden of venous leg ulcers in the United States. J. Med. Econ. 17(5), 347–356 (2014).
20.
Lal BK. Venous ulcers of the lower extremity: definition, epidemiology, and economic and social burdens. Semin. Vasc. Surg. 28(1), 3–5 (2015).
21.
van Acker K, Léger P, Hartemann A, Chawla A, Siddiqui MK. Burden of diabetic foot disorders, guidelines for management and disparities in implementation in Europe: a systematic literature review. Diabetes Metab. Res. Rev. 30(8), 635–645 (2014).
22.
Santema TB, Poyck PPC, Ubbink DT. Skin grafting and tissue replacement for treating foot ulcers in people with diabetes. Cochrane Database Syst. Rev. 2(2), CD011255 (2016).
23.
Sen CK, Gordillo GM, Roy S et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 17(6), 763–771 (2009).
24.
Brett D. A review of collagen and collagen-based wound dressings. Wounds 20(12), 347–356 (2008).
25.
Schierle CF, De la Garza M, Mustoe TA, Galiano RD. Staphylococcal biofilms impair wound healing by delaying reepithelialization in a murine cutaneous wound model. Wound Repair Regen. 17(3), 354–359 (2009).
26.
Hurlow J, Couch K, Laforet K, Bolton L, Metcalf D, Bowler P. Clinical biofilms: a challenging frontier in wound care. Adv. Wound Care 4(5), 295–301 (2015).
27.
Lasa I. Towards the identification of the common features of bacterial biofilm development. Int. Microbiol. 9(1), 21–28 (2006).
28.
Mihai M, Holban A, Giurcaneanu C et al. Microbial biofilms: impact on the pathogenesis of periodontitis, cystic fibrosis, chronic wounds and medical device-related infections. Curr. Top. Med. Chem. 15(16), 1552–1576 (2015).
29.
Malone M, Bjarnsholt T, McBain AJ et al. The prevalence of biofilms in chronic wounds: a systematic review and meta-analysis of published data. J. Wound Care 26(1), 20–25 (2017).
30.
Pastar I, Nusbaum AG, Gil J et al. Interactions of methicillin resistant Staphylococcus aureus USA300 and Pseudomonas aeruginosa in polymicrobial wound infection. PLoS ONE 8(2), e56846 (2013).
31.
Stewart PS. Mechanisms of antibiotic resistance in bacterial biofilms. Int. J. Med. Microbiol. 292(2), 107–113 (2002).
32.
Walters MC, Roe F, Bugnicourt A, Franklin MJ, Stewart PS. Contributions of antibiotic penetration, oxygen limitation, and low metabolic activity to tolerance of Pseudomonas aeruginosa biofilms to ciprofloxacin and tobramycin. Antimicrob. Agents Chemother. 47(1), 317–323 (2003).
33.
Hübner N-O, Kramer A. Review on the efficacy, safety and clinical applications of polihexanide, a modern wound antiseptic. Skin Pharmacol. Physiol. 23(1), 17–27 (2010).
34.
Kaehn K. Polihexanide: a safe and highly effective biocide. Skin Pharmacol. Physiol. 23(1), 7–16 (2010).
35.
Muller G, Kramer A. Biocompatibility index of antiseptic agents by parallel assessment of antimicrobial activity and cellular cytotoxicity. J. Antimicrob. Chemother. 61(6), 1281–1287 (2008).
36.
Mancini S, Cuomo R, Poggialini M, D'Aniello C, Botta G. Autolytic debridement and management of bacterial load with an occlusive hydroactive deressing impregnated with polyhexamethylene biguanide. Acta Biomed. 88(4), 409–413 (2018).
37.
Nussbaum SR, Carter MJ, Fife CE et al. An economic evaluation of the impact, cost, and medicare policy implications of chronic nonhealing wounds. Value Health 21(1), 27–32 (2018).
38.
Sen CK. Human wounds and its burden: an updated compendium of estimates. Adv. Wound Care 8(2), 39–48 (2019).
39.
Fife CE, Horn SD, Smout RJ, Barrett RS, Thomson B. A predictive model for diabetic foot ulcer outcome: the wound healing index. Adv. Wound Care 5(7), 279–287 (2016).
40.
Frykberg RG, Zgonis T, Armstrong DG et al. Diabetic foot disorders. A clinical practice guideline (2006 revision). J. Foot Ankle Surg. 45(Suppl. 5), S1–S66 (2006).
41.
Game FL, Apelqvist J, Attinger C et al. Effectiveness of interventions to enhance healing of chronic ulcers of the foot in diabetes: a systematic review. Diabetes Metab. Res. Rev. 32, 154–168 (2016).
42.
US FDA. Guidance for industry chronic cutaneous ulcer and burn wounds – developing products for treatment. (2006). https://www.fda.gov/media/71278/download
43.
Kottner J, Cuddigan J, Carville K et al. Prevention and treatment of pressure ulcers/injuries: the protocol for the second update of the International Clinical Practice Guideline 2019. J. Tissue Viability 28(2), 51–58 (2019).
44.
Sheehan P, Jones P, Caselli A, Giurini JM, Veves A. Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trial. Diabetes Care 26(6), 1879–1882 (2003).
45.
Margolis DJ, Gelfand JM, Hoffstad O, Berlin JA. Surrogate end points for the treatment of diabetic neuropathic foot ulcers. Diabetes Care 26(6), 1696–1700 (2003).
•• Landmark paper for establishing partial wound closure as a surrogate end point for healing.
46.
Snyder RJ, Cardinal M, Dauphinée DM, Stavosky J. A post-hoc analysis of reduction in diabetic foot ulcer size at 4 weeks as a predictor of healing by 12 weeks. Ostomy. Wound Manage. 56(3), 44–50 (2010).
47.
AARP Public Policy Institute. The medicare beneficiary population. (2020). https://assets.aarp.org/rgcenter/health/fs149_medicare.pdf
48.
Sabolinski ML, Gibbons G. Comparative effectiveness of a bilayered living cellular construct and an acellular fetal bovine collagen dressing in the treatment of venous leg ulcers. J. Comp. Eff. Res. 7(8), 797–805 (2018).
49.
Sabolinski ML, Capotorto J V. Comparative effectiveness of a human fibroblast-derived dermal substitute and a viable cryopreserved placental membrane for the treatment of diabetic foot ulcers. J. Comp. Eff. Res. 8(14), 1229–1238 (2019).
50.
Fitzgerald RH, Sabolinski ML, Skornicki M, Parsons NB. Evaluation of wound closure rates using a human fibroblast-derived dermal substitute versus a fetal bovine collagen dressing: a retrospective study. Wound Manag. Prev. 65(9), 26–34 (2019).
51.
Brantley J, Park H, Sanchez PJ, Fitzgerald R. The use of a novel antimicrobial and purified native collagen matrix to manage bioburden and support healing in challenging wounds: a clinical evaluation. Wounds Int. 7(3), 40–45 (2016).
52.
Sabolinski ML, Capotorto J V. Comparative effectiveness of a human fibroblast-derived dermal substitute and a viable cryopreserved placental membrane for the treatment of diabetic foot ulcers. J. Comp. Eff. Res. 8(14), 1229–1238 (2019).
53.
Kirsner RS, Sabolinski ML, Parsons NB, Skornicki M, Marston WA. Comparative effectiveness of a bioengineered living cellular construct vs. a dehydrated human amniotic membrane allograft for the treatment of diabetic foot ulcers in a real world setting. Wound Repair Regen. 23(5), 737–744 (2015).
•• Real-world comparative effectiveness research study for a manufactured, living skin eqivalent US FDA approved as a premarket approval (PMA).
54.
Sabolinski ML, Gibbons G. Comparative effectiveness of a bilayered living cellular construct and an acellular fetal bovine collagen dressing in the treatment of venous leg ulcers. J. Comp. Eff. Res. 7(8), 797–805 (2018).
55.
Marston WA, Sabolinski ML, Parsons NB, Kirsner RS. Comparative effectiveness of a bilayered living cellular construct and a porcine collagen wound dressing in the treatment of venous leg ulcers. Wound Repair Regen. 22(3), 334–340 (2014).
56.
Ayello EA, Dowsett C, Schultz GS et al. TIME heals all wounds. Nursing (Lond.) 34(4), 36–42 (2004).
57.
Sen CK, Gordillo GM, Roy S et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 17(6), 763–771 (2009).
58.
Singer AJ, Clark RAF. Cutaneous wound healing. N. Engl. J. Med. 341(10), 738–746 (1999).
59.
Global Skin and Wound Care Market Is Expected to Reach USD 25.98 Billion by 2025: Fior Markets. (2020). https://www.globenewswire.com/news-release/2020/03/04/1995036/0/en/Global-Skin-and-Wound-Care-Market-Is-Expected-to-Reach-USD-25-98-Billion-by-2025-Fior-Markets.html
60.
Rice JB, Desai U, Cummings AK, Birnbaum HG, Skornicki M, Parsons N. Medical, drug, and work-loss costs of venous leg ulcers. Value Health 16(3), A73 (2013).
61.
Gupta U, Verma M. Placebo in clinical trials. Perspect. Clin. Res. 4(1), 49 (2013).
62.
World Medical Association. Declaration of Helsinki. Medical Research Involving Human Subjects. (2020). https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/
63.
Hare KB, Lohmander LS, Roos EM. The challenge of recruiting patients into a placebo-controlled surgical trial. Trials 15, 167 (2014).
Information & Authors
Information
Published In
Pages: 691 - 703
PubMed: 32476449
Copyright
© 2020 Michael L Sabolinski. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 15 April 2020
Accepted: 14 May 2020
Published online: 1 June 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Type I collagen matrix plus polyhexamethylene biguanide antimicrobial for the treatment of cutaneous wounds. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0058
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Urvi Desai, J Bradford Rice, Serena Kongara, Robert S Kirsner, Lower limb amputation rates among Medicare beneficiaries with diabetic foot ulcers managed with and without native collagen matrix plus PHMB antimicrobial, Journal of Wound Care, 10.12968/jowc.2026.0291, (1-8), (2026).
- Sean Chen, Christopher Bibbo, John Starinski, Xianghua Xu, Chenhong Wang, A PHMB-Functionalized Fully Absorbable Synthetic Matrix as a Novel Alternative to Biologics: Balancing Antibacterial Efficacy, Tissue Repair, and Safety, Bioengineering, 10.3390/bioengineering13030353, 13, 3, (353), (2026).
- J Eduardo Melendez, Karla Chavez, Maribel Henao, Cameron DeShazo, Yeabsera Tamire, Jeyantt Srinivas Sankaran, Gabriel Arevalo, Surgical debridement and type 1 collagen extracellular matrix plus polyhexamethylene biguanide for the management of pressure injuries, Journal of Wound Care, 10.12968/jowc.2025.0164, 34, 9, (740-746), (2025).
- Jiaxing Liu, Ruishuang Sun, Yingxia Luo, Liujie Shi, Yunsong Zhang, Mechanism Exploration of Early Intervention With CO2 Ablative Fractional Laser to Improve Surgical Scars, Dermatologic Surgery, 10.1097/DSS.0000000000004732, 51, 12, (1123-1128), (2025).
- Chun-Kai Chang, Zong-Sheng Wu, Guang-Hao Niu, Yu-Yu Chou, Shih-Hsuan Tang, Mingzi M. Zhang, Chun-Sung Sung, Hsiang-Ting Tung, Lun Kelvin Tsou, Chi-Chieh Tang, Ping-Jyun Sung, Yi-Hao Lo, Zhi-Hong Wen, Marine-derived STING inhibitors, excavatolide B promote wound repair in full-thickness-incision rats, International Immunopharmacology, 10.1016/j.intimp.2025.114593, 155, (114593), (2025).
- Natalie Hickerson, Fiona Gruzmark, Sara Danker, Hadar Lev-Tov, Addressing the Dressings, Dermatologic Clinics, 10.1016/j.det.2024.12.010, 43, 2, (261-272), (2025).
- Van Vo, Hanif Haidari, Allison J. Cowin, Marcus Wagstaff, Bronwyn Dearman, Zlatko Kopecki, Dermal Substitutes for Clinical Management of Severe Burn Injuries: Current and Future Perspectives, Advanced Therapeutics, 10.1002/adtp.202400455, 8, 3, (2025).
- Amirhossein Ahmadieh-Yazdi, Mahdieh Karimi, Elham Afkhami, Fatemeh Hajizadeh-Tafti, Fatemeh Kuchakzadeh, Piao Yang, Mohsen Sheykhhasan, Unveiling therapeutic potential: Adipose tissue-derived mesenchymal stem cells and their exosomes in the management of diabetes mellitus, wound healing, and chronic ulcers, Biochemical Pharmacology, 10.1016/j.bcp.2024.116399, 226, (116399), (2024).
- Katrina A. Harmon, Miranda D. Burnette, Justin T. Avery, Kelly A. Kimmerling, Katie C. Mowry, Varying Properties of Extracellular Matrix Grafts Impact Their Durability and Cell Attachment and Proliferation in an In Vitro Chronic Wound Model, Journal of Tissue Engineering and Regenerative Medicine, 10.1155/2024/6632276, 2024, (1-12), (2024).
- Sunita Chauhan, Monika Gulia, Rahul Pratap Singh, Vikas Jhawat, Diabetic Wound: Pathophysiology, Complications and Treatment Strategies, Current Protein & Peptide Science, 10.2174/0113892037276171231016103320, 25, 3, (200-205), (2024).