Efficacy of immunotherapy with PD-1 inhibitor in colorectal cancer: a meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: PD-1 inhibitors have a leading role among immunotherapy while its efficacy on colorectal cancer (CRC) patients did not reach consensus and the small sample size remains as a limitation. Therefore, we undertook a meta-analysis on the effects of the monotherapy anti-PD-1 inhibitors in treating metastatic colorectal cancer (mCRC). Materials & methods: We searched databases to identify studies on efficacy of anti-PD-1 inhibitor on CRC. Objectives were objective response rate, progression-free survival rate, disease control rate and overall survival rate with their 95% CI. Results: The overall survival rate at 1-year was 64.2% (95% CI: 0.46–0.83). Disease control rate was 56.5% (CI: 0.27–0.86) and the objective response rate as 19.7% (CI: 0.08–0.32). The 1-year-progression-free survival rate was 38.4% (CI: 0.12–0.66). Sensitivity analysis and subgroup analysis were also conducted. Conclusion: The monotherapy anti-PD-1 inhibitors are effective in treating mCRC and could be a new option for dMMR mCRC patient in first-line treatment.
Colorectal cancer (CRC) is the most common cancer in men and the second in women worldwide making it the world’s fourth deadliest cancer (after lung, liver and stomach cancer) with almost 700,000 people dying as a result of CRC in 2012 [1,2]. Like other malignancies, the pathogenesis is not very clear and whether an abnormal microbiome, a cause of CRC is in mystery. Recently, immunotherapy with PD-1 inhibition changed the treatment paradigm and its respective outcomes in many advanced cancer like melanoma, renal, bladder and lung cancer [3].
In 2018, the Noble Prize in Physiology or Medicine was awarded for the discovery of cancer therapy by the inhibition of negative immune regulation [4]. The recipient Professor Honjo successfully identified PD-1 as a component of inhibition of the immune system that PD-1 is a cell receptor found on the surface of activated T cells, pro-B cells and macrophages with at least two ligands – programmed death-ligand 1 (PD-L1) and programmed death-ligand 2 (PD-L2). Binding of PD-L1 or PD-L2 to the PD-1 receptor leads to the deactivation of T-cell function, which allow tumor cell to evade from immune attack for the binding accomplishes a counter-inhibitory negative feedback loop, of which this mechanism can prevent a host from an attack by its own immune system [5,6].
Moreover, molecular phenotypes of CRC are defined by the mutational status of genes encoding mismatch repair (MMR) proteins, KRAS and BRAS. Mismatch repair deficient (dMMR) will result in microsatellite instability (MSI), whereas KRAS and BRAF mutations are considered to cause or at least favor the development of disease [7]. However, we still get limited information of monotherapy anti-PD-1 inhibitor’s efficacy in CRC and the sample size of its clinical test is small. For all these reasons, this meta-analysis aimed to evaluate the immunotherapy using monotherapy anti-PD-1 inhibitors in treating metastatic colorectal cancer (mCRC) and subgroup analysis was conducted to evaluate respective efficacy between dMMR and DNA mismatch repair proficient (pMMR) patients via the analysis of all available data.
Materials & methods
Literature search
Eligible studies were identified by electronic search of databases and cross-checking references of related papers before 22 May 2020. The databases of PubMed, Web of science, Elsevier, Cochrane Library, Embase and CNKI (China National Knowledge Infrastructure) were systematically searched using the following search terms: ‘programmed cell death protein 1’, 'immunotherapy’, ‘colorectal cancer’, ‘nivolumab’ and ‘pembrolizumab’. Two independent authors first retrieved potentially relevant papers according to titles and abstracts, and then further screened the articles by reading full texts. Any disagreements were resolved by discussion.
Inclusion & exclusion criteria
Two reviewers independently extracted data from eligible papers into a standardized data collection form. Inclusion criteria were as follows: patients with diagnostic CRC receiving monotherapy anti-PD-1 inhibitors: pembrolizumab or nivolumab; studies that demonstrated detailed clinical data: overall survival rate (OS), progression-free survival rate (PFS), disease control rate (DCR) and objective response rate (ORR) should be provided in detail or can be calculated; full-text articles written in English or Chinese are available. Except for original articles, other publications like letters, reviews, case reports or editorial articles were rejected. The two reviewers reached consensus on each items through discussion.
Data extraction quality assessment
Two reviewers independently extracted data from eligible papers into a standardized data collection form. The following data were collected: the first author’s name, year of publication, study design, subjects’ inclusion and exclusion criteria, number of participants, age, gender, CRC types, ORR, PFS, DCR and OS rate with their 95% CIs. Methodological quality of included studies were assessed with the Cochrane Collaboration tool [8]. Risk of bias for each item was graded as ‘low’, ‘unclear’ and ‘high’. Two investigators appraised the study quality independently, and discrepancies were resolved by discussion.
Statistical analysis
Our objectives: ORR, PFS rate, DCR and the OS rate with their 95% CIs were estimated for the included studies in this meta-analysis. We pooled the effective size in cancer treated with anti-PD1 agents. Heterogeneity of each group was tested using the χ2 test and the in consistency index (I2). An I2 greater than 50% and p-value of χ2 less than .05 confirmed the existence of significant heterogeneity, and a random effect model was chosen to pool the data. Otherwise, a fixed effect model was used. As a possible source of heterogeneity in the analysis, sensitivity analysis and subgroup analysis were also conducted to determine if certain variance could affect the heterogeneity and overall diagnostic effect.
Results
Study evaluation
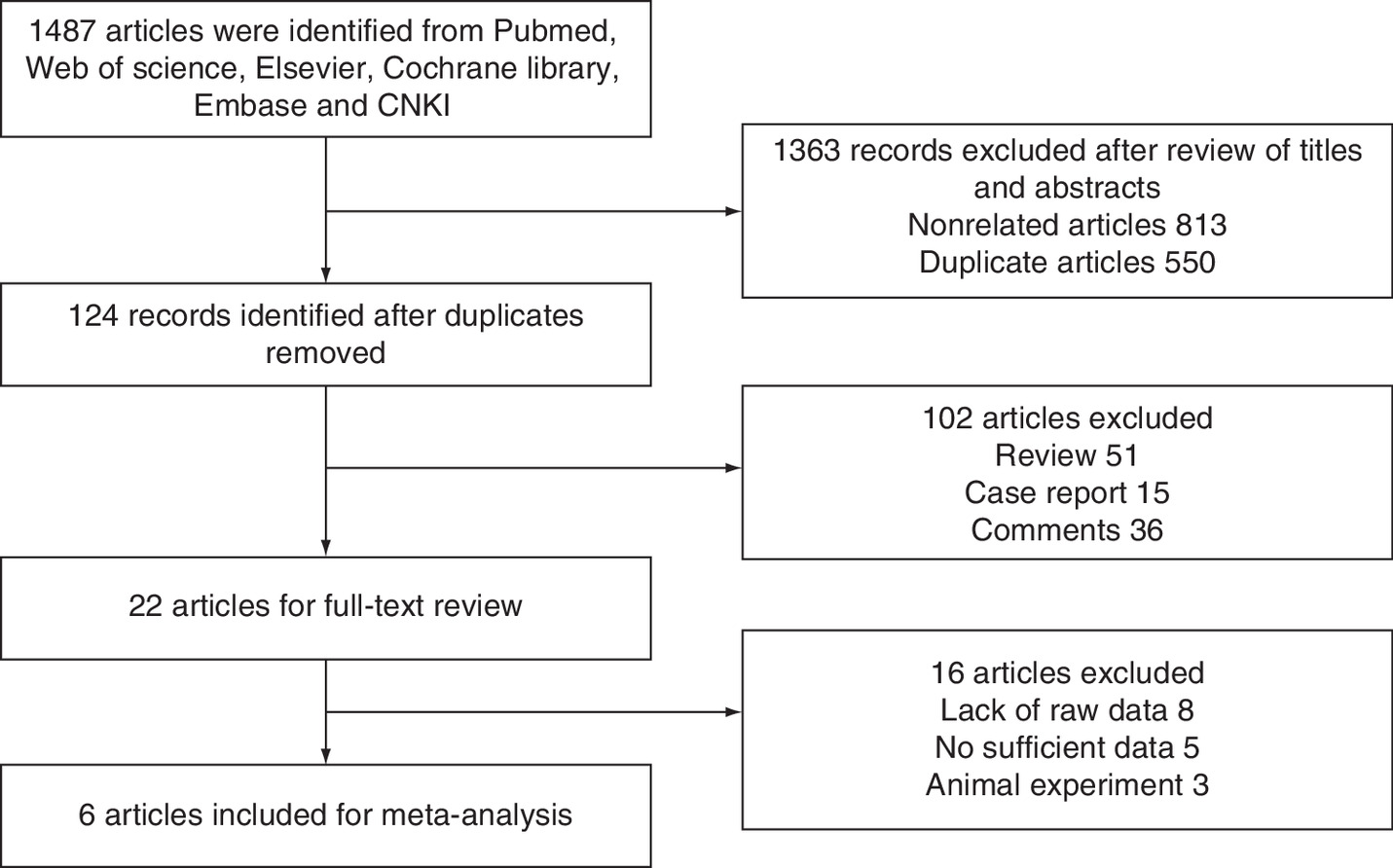
A total of 1487 potential citations were identified for inclusion into the study via multiple database searches and cross-checking of reference lists. After reviewing all the titles and abstracts, studies were excluded due to nonrelated topic and duplication, and 124 remained as potential candidates for our meta-analysis. We further excluded 98 studies since they did not meet our eligibility. Twenty-two were under full-text reviews and data extraction, of which eight studies lacked raw data and five studies were excluded for combining immune checkpoint inhibitor with other standard cancer therapies. Thus, the final six studies were included in our meta-analysis. Figure 1 presented the flowchart of a literature search.
Study characteristics
The included six studies consisted of a total of 297 participants. The PD-1 inhibitor were nivolumab and pembrolizumab. Among the five studies evaluating immunotherapy with PD-1 inhibition, two studies were conducted to evaluate the performance of nivolumab [9,10] and four studies described the performance of pembrolizumab [11–14]. All the eligible patients had progressed on or after, at least one previous line of treatment, including chemotherapy, monoclonal antibody or targeted therapy. Table 1 shows the detailed characteristics of the included studies.
| Study | Year | n | Age (years) | M/F | Anti-PD-1 inhibitor | OS rate at 1 year (%) | DCR | PFS rate 1 year (%) | ORR (%) | Dose | Molecular phenotypes | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Keynote 164 | 2018 | 63 | 59 (23–83) | 33/30 | Pembrolizumab | 76 | 95% | 41 | 33 | 200 mg every 3 weeks | dMMR | [11] |
| Le et al. | 2015 | 11 | 46 (24–65) | 6/5 | Pembrolizumab | - | 90% | - | 40 | 10 mg/kg | dMMR | [13] |
| 21 | 61 (32–79) | 13/8 | Pembrolizumab | - | 11% | - | 0 | 10 mg/kg | pMMR | |||
| O’Neil et al. | 2017 | 23 | 57 (40–78) | 13/10 | Pembrolizumab | 29.8 | - | 4.3 | 4 | 10 mg/kg | pMMR | [14] |
| Overman et al. | 2017 | 74 | 52.5 (44–64) | 44/30 | Nivolumab | 73 | 69% | 50 | 31.1 | 3 mg/kg | dMMR | [9] |
| T. Le et al. | 2017 | 86 | 57 (24–92) | 44/42 | Pembrolizumab | 76 | - | 64 | 52 | - | dMMR | [12] |
| Topalian et al. | 2012 | 19 | 63 (29–85) | - | Nivolumab | - | - | - | 0 | 0.3 mg/kg | pMMR | [10] |
-: Non declared; DCR: Disease control rate; dMMR: DNA mismatch repair deficient; mCRC: Metastatic colorectal cancer; MSI-H: Microsatellite instability-high; MSS: Microsatellite-stable; ORR: Objective respose rate; OS: Overall survival; PD-1: Programmed cell death protein-1; PFS: Progression-free survival; pMMR: DNA mismatch repair proficient.
Data analysis
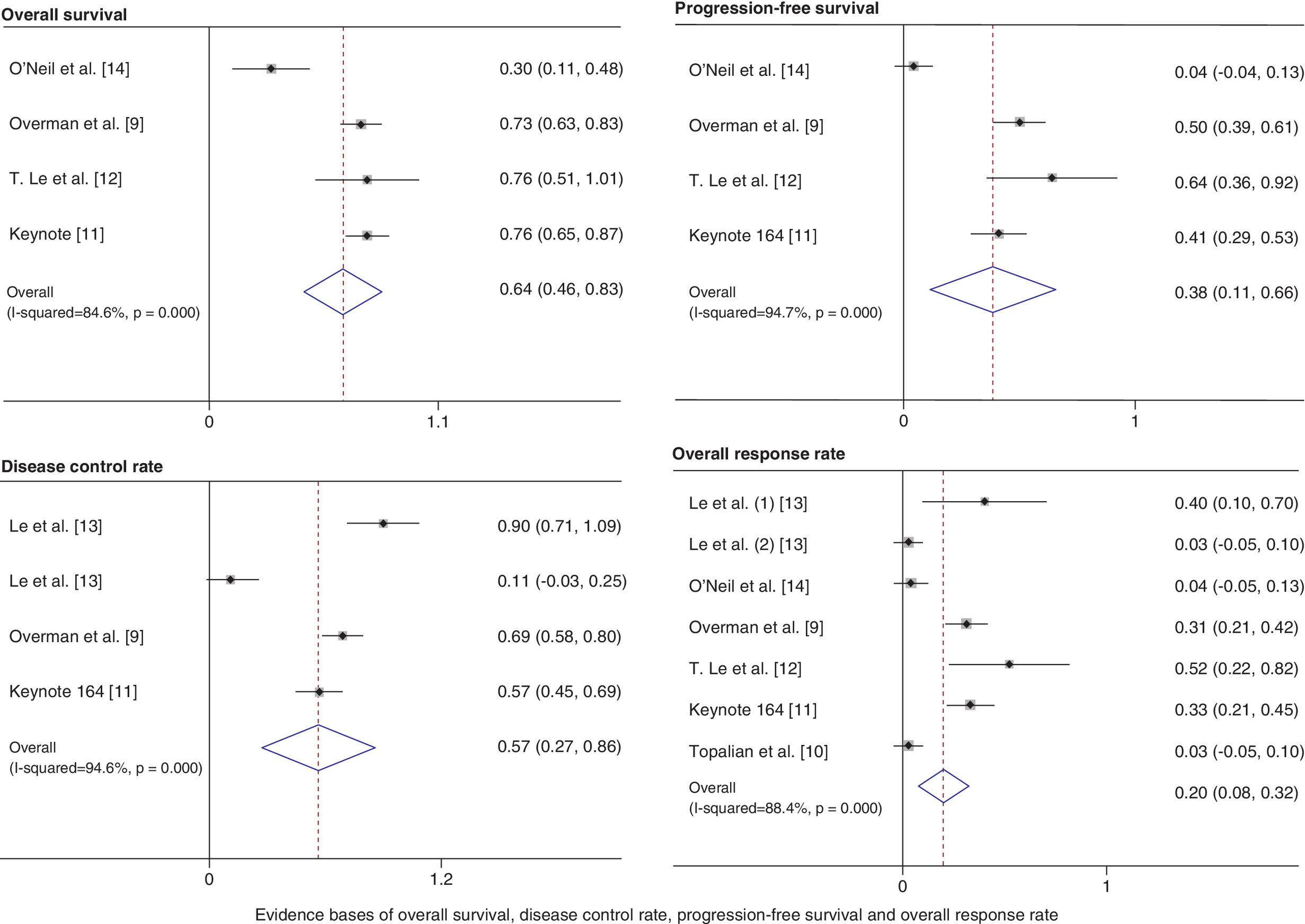
We identified four studies on the data analysis of OS at 1 year. The OS rate at 1 year was 64.2% (95% CI: 0.46–0.83; I2 = 84.6%; p = 0.000). The estimation of the DCR indicated a result of 56.5% (95% CI: 0.27–0.86; I2 = 94.6%) and four studies were included. The ORR was 19.7% (95% CI: 0.08–0.32; I2 = 85.9%) and six studies were included. The results of meta-analysis of random effect model show that the PFS rate was 38.4% (95% CI: 0.12–0.66; I2 = 94.7%) and four studies were included. Details of data analysis are presented in Figure 3.
An I2 above 50% shows the existence of significant heterogeneity, and a random effects model was chosen to pool the data. We performed a sensitivity analysis to eliminate factors that influence heterogeneity. In the analysis of OS, sensitive analysis revealed that data of O’Neil et al. [14] is the source of statistical heterogeneity in the meta-analysis. When this outlier study is removed, there was no evidence of heterogeneity in three remaining studies (p = 0.00, 95% CI: 0.67–0.82; I2 = 0%). Also, when removed, the study of O’Neil, the heterogeneity of the four remaining studies changed significantly from 94.7 to 22.5% (p = 0.00, 95% CI: 0.38–0.57) in the analysis of PFS. In the interpretation of heterogeneity of DCR of anti-PD-1 inhibitors, sensitive analysis revealed that cohort B’s data of Le et al. [13] had an impact on the heterogeneity; omitting the study of Le et al. decreased the I2 for heterogeneity from 94.6 to 76.5% (p = 0.00, 95% CI: 0.55–0.87). The overall results showed a change from 94.6 to 76.5% while it still remains a high heterogeneity.
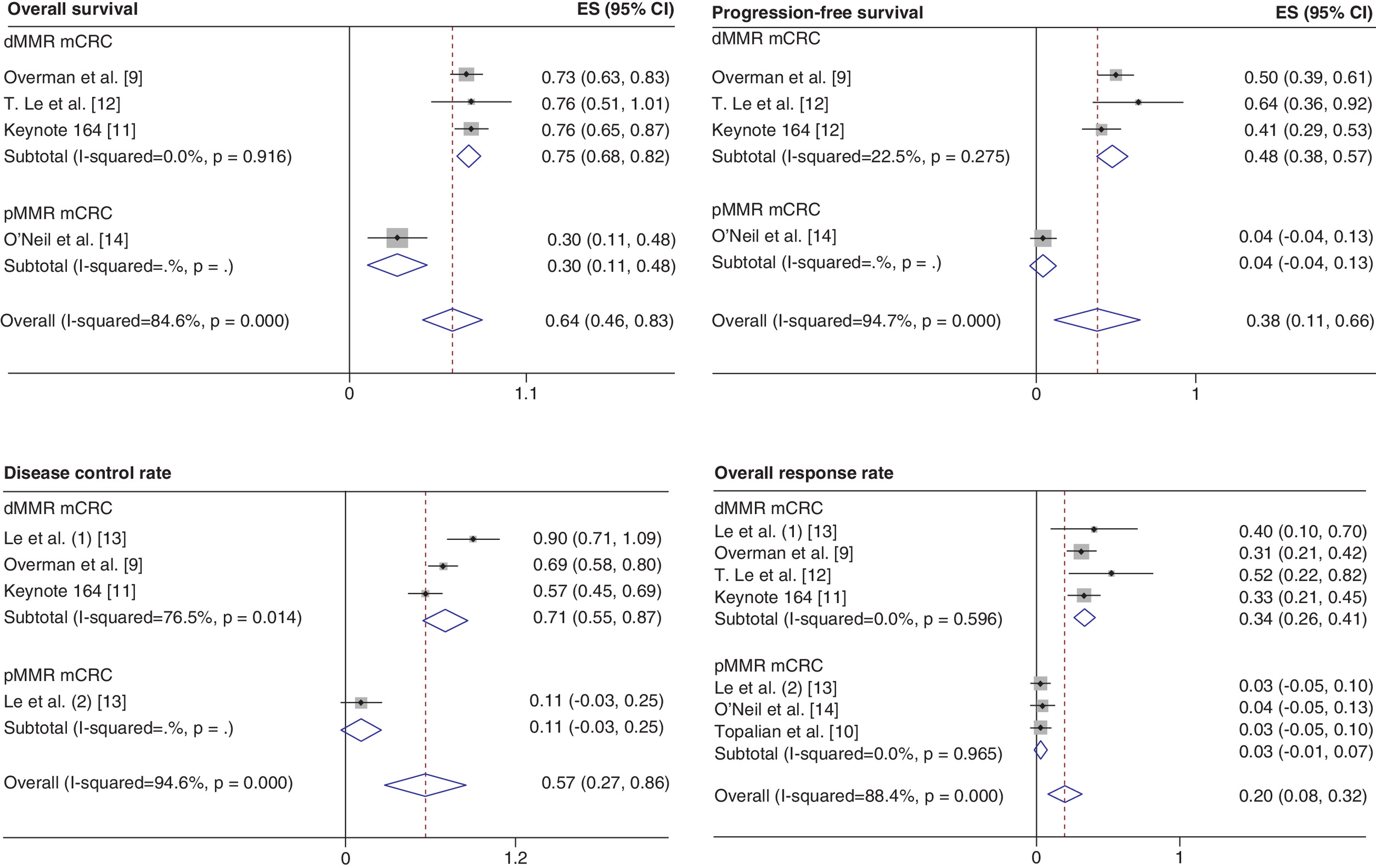
Subgroup analysis stratified by molecular phenotypes of CRC showed that ORR performs better in dMMR/microsatellite instability-high (MSI-H) CRC patients based on its pooled ORR of 34% (95% CI: 0.26 ∼ 0.41) and heterogeneity decreased to 0%, while in the pMMR/microsatellite-stable (MSS) groups, ORR become less significant according to its pooled data of 3% (95% CI: 0.01 ∼ 0.07). Same situation also appeared in the data process of OS and PFS showing that the monotherapy anti-PD-1 inhibitors are ineffectual in those patients (Figure 4).
Quality assessment
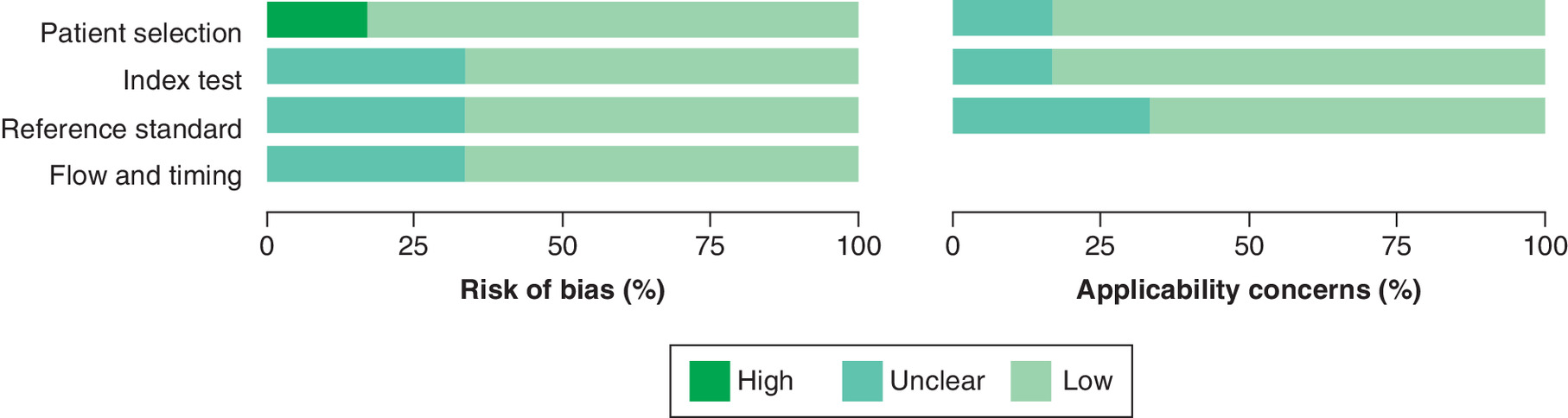
According to the results of the QUADAS-2 items, high risk of bias was observed in the ‘patients’ selection’ category of the study of T. Le et al. because it did not avoid inappropriate exclusions (i.e., one patient with a grade 3 bilirubin level higher than the cut-off specified in the inclusion criteria was enrolled institutional review board eligibility waiver). Unclear risk of bias was mostly observed in the “reference standard” category because the majority of trials did not clarify whether the reference standard results were interpreted without knowledge of the results of the index tests. Detailed information of the included studies and the results of the distribution are presented in Figure 2.
Discussion
Immunotherapy with PD-1 inhibition is a promising therapy in cancer treatment in recent year [5]. This is the first meta-analysis that includes evidence from clinical trials on the efficacy of monotherapy anti-PD-1 inhibitors among patients with CRC. The finding of our study provides additional evidence that monotherapy anti-PD-1 inhibitors are associated with a favorable efficacy in treating CRC patients who had received previous treatment. In antitumor analysis, data synthesis revealed a superior outcome of OS and disease control that anti-PD-1 inhibitors are effective on the treatment of mCRC; regarding molecular phenotypes the monotherapy anti-PD-1 inhibitor performs a superior outcome in dMMR/MSI-H mCRC patients, which means that immune checkpoints (ICIs) might be more suitable for those patients to prevent the inhibition of T-cell function and to achieve a better effect.
Considering approximately 70% of CRC are characterized by proficiency in MMR, whether PD-1 inhibitor monotherapy has an effect on pMMR/MSS patients remains a matter of debate. Subgroup analysis based on molecular phenotype was conducted and revealed that PD-1 inhibitor monotherapy is inferior in treating pMMR/MSS patients, which is consistent with clinical trials referred in their respective research by Le et al. [13] and Topalian et al. [10] examining the efficacy of immune checkpoints among pMMR/MSS patients with mCRC. In those patients, the poor antitumor effect might be because of several potential mechanisms that could contribute to the resistance to immunotherapy. On one hand, tumor antigen-specific CD8+ T cell can be enhanced by ICIs which is associated with durable tumor response and efficacy in the treatment of patients with dMMR/MSI-H mCRC. On the other hand, pMMR mCRC tumor cells have relatively low immunogenicity for CD8+ T-cell recognition due to low expression of tumor-specific antigen secondary to low mutation burden that leads to a relatively anergic state of CD8+ T cell [15]. Also, the immunosuppressive status of the tumor microenvironment can lead to anergy of CD8+ T cell. For all these reasons, monotherapy anti-PD-1 inhibitors to pMMR/MSS patients may be ineffective and thus it is necessary to move attention to the combination of anti-PD-1 inhibitors with other therapeutic approaches. Recently, investigators have extended the combination of PD-1/PD-L1 inhibitors with different types of treatment in first-line and early second-line therapy on CRC. Studies on the combination of anti-PD-1/PD-L1 inhibitors with other immunotherapy, targeting drugs and chemotherapy were published and at least three trials have observed favorable objective response and improved PFS in the combination use of anti-PD-1 inhibitors [16–18].
This study has several strengths. Although immunotherapy has showed clinical benefit in many tumor types like melanoma, renal and lung cancer, it is not very clear about its effect on CRC. We believed the current meta-analysis further strengthens the evidence on the efficacy of anti-PD-1 inhibitors on mCRC and encourages a further exploration on it. In the present study, the significant improvement in survival is mostly showed in CRC patients who underwent previous treatment. It is notable that anti-PD-1 inhibitors are mostly used as a second or third choice for CRC at present. It will be important in the future to study immunotherapy in first-line treatment, especially in dMMR/MSI-H mCRC patients who are sensitive to ICI and expand the application of anti-PD-1/PD-L1 inhibitor on other cancer types. Furthermore, mechanisms of resistance to PD-1 blockade is also a promising field to investigate for the pMMR/MSS patients make up a large proportion of the population.
This study has some limitations, which should be taken into consideration while interpreting its findings. First, few studies were included because the research on PD-1 inhibitor on CRC is a new field. Many of the published studies on PD-1 inhibitor are early phase clinical trials with a small amount of patients. Moreover, high heterogeneity performed in the meta-analysis of DCR was a major concern. Although sensitivity analysis had omitted studies that affect heterogeneity, the result only changed slightly and so did the subgroup analysis. At present, studies and trials on the immunotherapy with PD-1 inhibition are less than our expectation and most of the studies on PD-1 inhibitors are reviews, not to mention study like meta-analysis on PD-1 inhibitor on the treatment of CRC [19–23]. Given the fact that the sample size in the analysis was relatively small, this outcome needs to be interpreted with caution and verified by large randomized clinical trials.
Conclusion
The efficacy of monotherapy anti-PD-1 inhibitor is encouraging with prolonged survival related to patients with dMMR/MSI-H mCRC. Still, treatments like surgical operation, radiotherapy or chemotherapy are still the main treatments modality. The result of current study shows a promising future of PD-1 inhibitor on treatment of CRC. We encourage more attention on the exploration of PD-1 inhibitor in the treatment of CRC patients and with the results showing that PD-1 inhibitors are effective in dMMR CRC and MSI-H mCRC, additional information is needed for a further evaluation on it.
•
First meta-analysis of clinical evidence on the efficacy of monotherapy anti-PD-1 inhibitors among patients with metastatic colorectal cancer (mCRC) including evidence from all possible published studies.
•
The combined estimate of effect suggests potential survival improvement associated with immunotherapy with PD-1 inhibitors with a 64.2% pooled estimate on overall survival rate and the pooled disease control rate was 56.6%.
•
Subgroup analysis showed that monotherapy anti-PD-1 inhibitors contributed a superior effect in treating mCRC among dMMR patients and found the effect inferior among DNA mismatch repair proficient (pMMR) patients.
•
Sensitivity analysis showed that the heterogeneity in each survival data were generally caused by studies focusing on pMMR mCRC patients.
•
The combined estimate of effect suggests that the use of monotherapy anti-PD-1 inhibitors for dMMR mCRC patients could result in a better survival and encourage further use in first-line treatment while for pMMR mCRC patients, the exploration of combination use will be needed.
Author contributions
All the authors contributed to manuscript writing, critical revision and final review of the manuscript. S He, D Hu and X Wang contributed to the conception, design of the study and critical revision of the manuscript. H Feng contributed to the data processing. Y Xue and J Jin were responsible for the study selection, data extraction and quality assessment.
Financial & competing interests disclosure
This study was funded by the China Postdoctoral Science Foundation. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: •• of considerable interest
1.
GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012 v1.0: IARC cancerbase no. 11. International Agency for Research on Cancer, France, https://gco.iarc.fr/
2.
Brody H. Colorectal cancer. Nature 521(7551), S1 (2015).
3.
Oliveira AF, Bretes L, Furtado I. Review of PD-1/PD-L1 inhibitors in metastatic dMMR/MSI-H colorectal cancer. Front. Oncol. 9, 396 (2019).
4.
The Nobel Assembly at Karolinska Institutet. Press release: the nobel prize in physiology or medicine 2018. https://www.nobelprize.org/prizes/medicine/2018/press-release/
5.
Chen L, Han X. Anti–PD-1/PD-L1 therapy of human cancer: past, present, and future. J. Clin. Invest. 125(9), 3384–3391 (2015).
6.
Oiseth SJ, Aziz MS. Cancer immunotherapy: a brief review of the history, possibilities, and challenges ahead. J. Cancer Metastasis Treat. 3(10), 250 (2017).
7.
Kocarnik JM, Shiovitz S, Phipps AI. Molecular phenotypes of colorectal cancer and potential clinical applications. Gastroenterol. Rep. 3(4), 269–276 (2015).
8.
Whiting PF, Rutjes AWS, Westwood ME et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. 155(8), 529–536 (2011).
9.
Overman MJ, McDermott R, Leach JL et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, Phase II study. Lancet Oncol. 18(9), 1182–1191 (2017).
10.
Topalian SL, Hodi FS, Brahmer JR et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 366(26), 2443–2454 (2012).
11.
Le D, Kavan P, Kim TW et al. KEYNOTE-164: pembrolizumab for patients with advanced microsatellite instability high (MSI-H) colorectal cancer. J. Clin. Oncol. 36, 3514–3514 (2018).
12.
Le DT, Durham JN, Smith KN et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 357(6349), 409–413 (2017).
13.
Le DT, Uram JN, Wang H et al. PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 372(26), 2509–2520 (2015).
14.
O'Neil BH, Wallmark JM, Lorente D et al. Safety and antitumor activity of the anti-PD-1 antibody pembrolizumab in patients with advanced colorectal carcinoma. PLoS ONE 12(12), e0189848 (2017).
15.
Lee JJ, Chu E. Recent advances in the clinical development of immune checkpoint blockade therapy for mismatch repair proficient (pMMR)/non-MSI-H metastatic colorectal cancer. Clin. Colorectal Cancer 17(4), 258–273 (2018).
•• The most comprehensive review assessing the potential underlying mechanisms that mediate primary immune resistance of dMMR proficient/nonmicrosatellite instability-high metastatic colorectal cancer to immune checkpoint inhibitor therapy and reporting recent advances in the improvement of combination of programmed cell death protein-1 inhibitors with other therapies.
16.
Diaz LA, Le DT, Yoshino T et al. KEYNOTE-177: Phase III, open-label, randomized study of first-line pembrolizumab (pembro) versus investigator-choice chemotherapy for mismatch repair-deficient (dMMR) or microsatellite instability-high (MSI-H) metastatic colorectal carcinoma (mCRC). J. Clin. Oncol. 36(Suppl. 4), TPS877 (2018).
17.
Lee JJ, Sun W, Bahary N et al. Phase II study of pembrolizumab in combination with azacitidine in subjects with metastatic colorectal cancer. J. Clin. Oncol. 35(Suppl. 15), 3054 (2017).
18.
Lenz HJJ, Van Cutsem E, Limon ML et al. Durable clinical benefit with nivolumab (NIVO) plus low-dose ipilimumab (IPI) as first-line therapy in microsatellite instability-high/mismatch repair deficient (MSI-H/dMMR) metastatic colorectal cancer (mCRC). Ann. Oncol. 29(Suppl. 8), 714, LBA18_PR (2018).
19.
Chen G. Immunotherapy for colorectal cancer: current status and progress. J. Precision Med. 34(1), 1–5 (2019).
20.
Chen JQ, Dong CX, Yuan Y. Progress in colorectal cancer treatment in 2018. J. Prac. Oncol. 34(1), 1–6 (2019).
21.
Chen QX. Progress of PD-1/PD-L1 signaling pathway in immune escape and treatment of colorectal cancer. J. Modern Oncol. 26(13), 2133–2138 (2018).
22.
Chen CX, Lin YH, Zhang M et al. Advances of PD1/PDL1 signaling pathway in immune escape and treatment for colorectal cancer. J. Modern Oncol. 26(13), 2133–2138 (2018).
23.
Cheng Y, Li JH. Progress of PD-1/PD-L1 inhibitors in tumor immunotherapy. Guangdong Med. J. 37(21), 3301–3304 (2016).
Information & Authors
Information
Published In
Pages: 1285 - 1292
PubMed: 33073605
Copyright
© 2020 Future Medicine Ltd.
History
Received: 3 March 2020
Accepted: 28 September 2020
Published online: 19 October 2020
Keywords:
Topics
Authors
Funding Information
China Postdoctoral Science Foundation: 2017M611124
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Efficacy of immunotherapy with PD-1 inhibitor in colorectal cancer: a meta-analysis. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0040
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Liuqing Yang, Zelong Li, Yalin Li, Qi Zhang, Heping Zhang, Synergistic antitumor and immunomodulatory effects of Bifidobacterium animalis subsp. lactis V9 combined with anti–PD-1 therapy, Frontiers in Immunology, 10.3389/fimmu.2026.1791276, 17, (2026).
- Naziba Nuha, Stephen P. Higgins, Ralf-Peter Czekay, Craig E. Higgins, Lynn Guo, Hwajeong Lee, Paul J. Higgins, SERPINE1 drives molecular synergies in colorectal cancer, American Journal of Physiology-Cell Physiology, 10.1152/ajpcell.00759.2025, 330, 1, (C9-C25), (2026).
- Xu Wang, Yuanmin Xu, Rui Sun, Sheng Wang, Xiang Wei, Multi-omics based consensus subtypes, development of prognostic signature, and identification of INHBB as a potential therapeutic target in colorectal cancer, Functional & Integrative Genomics, 10.1007/s10142-025-01691-1, 25, 1, (2025).
- Erfan Rezazadeh‐Gavgani, Reza Majidazar, Parisa Lotfinejad, Tohid Kazemi, Ali Shamekh, Immune Checkpoint Molecules: A Review on Pathways and Immunotherapy Implications, Immunity, Inflammation and Disease, 10.1002/iid3.70196, 13, 4, (2025).
- Xu Wang, Shixin Chan, Jiajie Chen, Yuanmin Xu, Longfei Dai, Qijun Han, Zhenglin Wang, Xiaomin Zuo, Yang Yang, Hu Zhao, Ming Wang, Chen Wang, Zichen Li, Huabing Zhang, Wei Chen, Robust machine−learning based prognostic index using cytotoxic T lymphocyte evasion genes highlights potential therapeutic targets in colorectal cancer, Cancer Cell International, 10.1186/s12935-024-03239-y, 24, 1, (2024).
- Haoran Jin, Bihan Xia, Jin Wang, Shaochong Qi, Weina Jing, Kai Deng, Jinlin Yang, A Novel Lipid Metabolism and Endoplasmic Reticulum Stress-Related Risk Model for Predicting Immune Infiltration and Prognosis in Colorectal Cancer, International Journal of Molecular Sciences, 10.3390/ijms241813854, 24, 18, (13854), (2023).
- Xu Wang, Yuanmin Xu, Longfei Dai, Zhen Yu, Ming Wang, Shixin Chan, Rui Sun, Qijun Han, Jiajie Chen, Xiaomin Zuo, Zhenglin Wang, Xianyu Hu, Yang Yang, Hu Zhao, Kongwang Hu, Huabing Zhang, Wei Chen, A novel oxidative stress- and ferroptosis-related gene prognostic signature for distinguishing cold and hot tumors in colorectal cancer, Frontiers in Immunology, 10.3389/fimmu.2022.1043738, 13, (2022).
- Jun Yuan, Jiarui Li, Ce Gao, Chun Jiang, Ze Xiang, Jian Wu, Immunotherapies catering to the unmet medical need of cold colorectal cancer, Frontiers in Immunology, 10.3389/fimmu.2022.1022190, 13, (2022).
- PelvEx Collaborative PelvEx Collaborative, Contemporary Management of Locally Advanced and Recurrent Rectal Cancer: Views from the PelvEx Collaborative, Cancers, 10.3390/cancers14051161, 14, 5, (1161), (2022).
- Maria Rotundo, Vincenzo Bagnardi, Miryam Rotundo, Mario Comandè, Maria Zampino, PD‑1/PD‑L1 blockade, a novel strategy for targeting metastatic colorectal cancer: A systematic review and meta‑analysis of randomized trials, Oncology Letters, 10.3892/ol.2022.13254, 23, 4, (2022).