US database study: burden and healthcare resource utilization in adults with systemic endemic mycoses and aspergillosis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study evaluated burden of illness in immunocompromised patients with systemic mycoses (SM) eligible for itraconazole treatment, specifically, histoplasmosis, blastomycosis and aspergillosis. Methods: A cross-sectional study used an electronic medical record network integrating information from 30 US hospitals, including >34 million patients, to evaluate burden and healthcare resource utilization over 6 months following initiation of antifungal therapy. Results: Symptomatic burden experienced by each of the otherwise healthy or age >65 or immunosuppressed cohorts receiving antifungal therapy for SM was comparable but significantly greater in cancer or HIV patients and transplant recipients. Across groups, there was substantially higher healthcare resource utilization in patients with SM versus matched controls without SM. Conclusion: The total impact of SM is particularly severe in high-risk or vulnerable populations.
Systemic mycoses (SM) are a result of fungi entering the body via the lungs, gastrointestinal tract, paranasal sinuses or skin, leading to considerable morbidity and mortality [1]. Despite advances in antifungal therapy, mortality rates for invasive fungal diseases remain high [2]. Immunocompromised patients are at risk for SM, but these infections also can develop in otherwise healthy patients [2]. SM can be categorized between two main types: endemic mycoses and opportunistic infections.
Endemic mycoses are systemic infections caused by fungi including Histoplasma spp (causing histoplasmosis), Coccidioides spp (causing coccidioidomycosis); Blastomyces spp (causing blastomycosis), Sporothrix spp (causing sporotrichosis), Paracoccidioides spp (causing paracoccidiodomycosis) and Talaromyces marneffei (formerly Penicillium) (causing talaromycosis) [3]. These fungi are found in soil, wood debris, bat guano and other environmental niches. Histoplasma is prevalent in southern USA, central America, South America, Africa and Asia; Coccidioides is prevalent throughout western USA and central and South America; Sporothrix is prevalent worldwide in tropical and sub-tropical regions and Blastomyces is most often found in north America [3].
Opportunistic fungal infections primarily occur in immunocompromised patients [1,3]. The specific fungi are ubiquitous and include Candida species (causing candidiasis, the most frequent invasive mycosis in the healthcare setting), Aspergillus species (causing aspergillosis), Cryptococcus (causing cryptococcosis), the Mucorales (causing mucormycosis) and the agents responsible for chromoblastomycosis and phaeohyphomycosis [1,3]. People at highest risk for SM include those with uncontrolled HIV, systemic malignancy, or neutropenia (low white blood cell count), organ transplant recipients, postoperative patients (major surgery), those with poorly controlled diabetes mellitus and those at the extremes of age [2].
The incidence of systemic fungal infections is rising [3–5] and changes in the epidemiology and burden of infection have been recognized in oncology patients and transplant recipients [6]. This trend has been evident for close to 40 years in the USA; between 1980 and 1997, the annual number of deaths in which an invasive mycosis was listed on the death certificate increased from 1557 to 6534 ― a 320% increase over 17 years attributable in large part at that time to HIV infection [7]. More recent increased incidence has been attributed to various changes leading to an increase in the pool of immunocompromised patients, including an increased number of solid organ and hematopoietic stem cell transplants. Together with acute leukemia, transplants now represent the most common risk factors for opportunistic fungal infections [6,8]. In 2008, over 23,000 organs were transplanted in the USA – twice the amount transplanted 10 years previously [9]. The use of newer and more potent chemotherapeutic agents and regimens, along with continued advances in the treatment of neurologic and rheumatologic diseases, has placed upward pressure on numbers of immunocompromised patients [10,11]. Despite the increasing prevalence of SM, there have been no new classes of antifungal therapy introduced since the azoles in the early 1980s and the echinocandins in 2000 [12]. There have, however, been some advances with new formulations of antifungals to improve bioavailability and tissue distribution.
To better understand the clinical burden of systemic mycoses in the USA, we queried an electronic medical records (EMRs) system from hospital institutions to evaluate the burden of illness, healthcare resource utilization and real-world outcomes in these patients treated with antifungal medications. Our focus was patients with histoplasmosis, blastomycosis and aspergillosis, as we were particularly interested in patients eligible for itraconazole treatment according to its approved usage in the USA.
Methods
Study setting & data
This study used a federated EMR network (TriNetX) containing information on more than 34 million patients from 30 US hospital institutions at the time the network was accessed. The healthcare organizations (HCOs) contributing to the TriNetX data consisted at that time mostly of large academic health centers comprised of main and satellite hospitals and outpatient clinics. Aggregated results from de-identified EMRs can be queried in real-time with an average of 5–6 years of data available from the time of query. The de-identified, health insurance portability and accountability act (HIPAA)-compliant EMR network provides information on patient demographics, ICD-10 codes, Clinical Modification (ICD-10-CM), procedure codes (ICD-10-Procedure Coding systems, Current Procedural Terminology), medications, labs, oncology data, genomics and vital signs. Various and disparate data from numerous healthcare organizations are mapped to control terminologies within the network to simplify the data extraction process. Strong coverage is available for diagnoses, procedures, medications and lab results, while genomics and oncology data are less supported.
Design & study population
This study was a cross-sectional observational study which queried the EMR network during November 2017; hence, the average data available span the period 2012–2017. Patients aged ≥18 years old with SM were included in an initial data capture using different pathogenic fungal organisms using ICD-10-CM diagnosis codes of B38–B44: coccidioidomycosis (B38), histoplasmosis (B39), blastomycosis (B40), paracoccidioidomycosis (B41), sporotrichosis (B42), chromoblastomycosis and phaeohyphomycosis (B43) and aspergillosis (B44). This study focused on symptoms, clinical burden, resource use and treatment in patients diagnosed with histoplasmosis, blastomycosis and aspergillosis. These three organisms were selected as we were seeking to understand the clinical burden specifically in patients who would be eligible for itraconazole treatment according to its approved uses in the USA. To further refine the adult systemic mycoses patient population, medication data was used to identify antifungal medications (fluconazole, itraconazole, voriconazole, posaconazole, amphotericin B, liposomal amphotericin B, terbinafine, micafungin and caspofungin) from patients with fungal infection diagnoses. It should be noted that, although different lipid formulations of amphotericin B are available, distinguishing between them was not possible using the data extraction tools from this EMR network; however, this data extraction tool was able to distinguish between liposomal amphotericin B and amphotericin (i.e., nonliposomal amphotericin B).
Patients, who included those treated in the inpatient or outpatient setting were further categorized into six nonmutually exclusive cohorts using diagnosis codes and medication data: otherwise healthy controls; elderly aged ≥65 years old; those receiving immunosuppressant medication (including biologicals, e.g., infliximab and adrenal corticosteroids, e.g., prednisone); cancer patients; transplant recipients (solid organ transplant or hematopoietic stem cell transplant recipients); and HIV-positive patients. Patients could be included in more than one cohort as the cohorts were not mutually exclusive. The inclusion and exclusion criteria were built into the data extraction parameters. For example, group 1 excluded all criteria defining groups 2–5 and so on for the other groups. Inclusion criteria were: mycoses diagnosis (histoplasmosis, blastomycosis or aspergillosis); and treatment with systemic antifungal therapy. Further inclusion criteria were based on defining characteristic as described for groups 2–5.
All patients in the six cohorts were initially identified by their EMR denoting a systemic mycosis (as defined above with a diagnosis code for a pathogenic fungal organism) and having been prescribed at least one antifungal agent. The otherwise healthy cohort (group 1) EMRs showed a fungal diagnosis and also included treatment with one or more of the antifungal medications only. The otherwise healthy (group 1) and elderly patient (group 2) cohorts did not include patients whose records described the use of immunosuppressant or antineoplastic therapies, receipt of transplants or diagnosis of HIV/AIDS. Similarly, immunosuppressed patients (group 3) were defined as those being treated with an immunosuppressant therapy, but excluded if also treated with an antineoplastic agent, were a receipt of a transplant (solid organ transplant or hematopoietic stem cell transplant recipients) or had a diagnosis of HIV/AIDS. The same inclusion logic was applied for fungal patients in the cancer cohort (group 4) as showing treatment with antineoplastic therapy; the transplant cohort (group 5) had received a transplant; lastly, HIV/AIDS patients (group 6) were defined as those a diagnosis of HIV infection and could be at any stage of their disease.
Patients were not mutually exclusive because some fell into multiple cohorts, for example, the elderly cohort was a sub-population of the healthy cohort; patients in the cancer, transplant or HIV/AIDS cohorts could be overlapping as well. To facilitate comparisons between outcomes in this study, control cohorts were created of patients without a history of systemic mycoses and antifungal treatment but were comprised of the analogous disease profile of immunosuppressed or cancer patients, transplant recipients and HIV/AIDS patients.
Outcomes
Study outcomes to assess the burden of illness in patients with systemic mycoses were identified within 6 months after initiation of a patient’s first antifungal agent. The study outcomes for the control cohorts were assessed 6 months from the start of immunosuppression therapy for the immunosuppressed patients without SM; the start of antineoplastic therapy for cancer patients without SM; the time of a transplant procedure for transplant recipients without SM; and time of diagnosis for the HIV/AIDS patients without SM. Therefore, all patient cohorts had a common denominator as a follow-up of 6 months so that outcomes could be compared.
Symptom burden
The prevalence of symptoms arising from the systemic mycoses infections (whether constitutional, respiratory, metabolic, gastrointestinal or other signs of infection) were identified within 6 months of starting an antifungal medication. Initially, SM cohorts (groups 2–5) were compared with the otherwise healthy cohort (group 1) as a reference. Systemic mycoses cohorts were further compared with the analogous control cohorts of similar categories (i.e., immunosuppressed, with cancer/transplants/HIV-positive). The rate of symptoms for each cohort was defined from the start of therapy for the primary disease (whether immunosuppressant medication [group 3], antineoplastic therapy [group 4]), completion of a transplant procedure (group 5) or the time of HIV/AIDS diagnosis (group 6).
Treatment utilization
The proportion of patients prescribed each antifungal treatment of interest (itraconazole, fluconazole, liposomal amphotericin B, voriconazole, terbinafine, micafungin, posaconazole, caspofungin, amphotericin B, flucytosine) was summarized among the six SM patient cohorts.
Healthcare resource utilization
Healthcare resource utilization was defined as the number of visits to a healthcare provider (clinic or emergency room) and/or the number of hospitalizations. Healthcare resource use was assessed in the 6 months following treatment with antifungals for the SM patient cohorts or study control cohorts without SM: immunosuppressed (treatment with immunosuppressants), cancer (time of antineoplastic therapy), transplant (time of transplant) or HIV/AIDS (time of diagnosis).
Statistical analysis
Unadjusted descriptive statistics were conducted to summarize characteristics of patients within each of the six study cohorts. Percentages and means, with standard deviations, were calculated. The percentage of patients in each cohort affected by each symptom burden was calculated. The percent difference in symptom prevalence was also determined for comparisons of interest. Two-tailed t-tests were calculated for p-values to indicate the significance of each difference. Differences in healthcare resource utilization were similarly calculated. Treatment utilization was assessed by considering the proportion of systemic mycoses patients on each treatment, within each cohort. A p-value of <0.05 was defined to be statistically significant.
Results
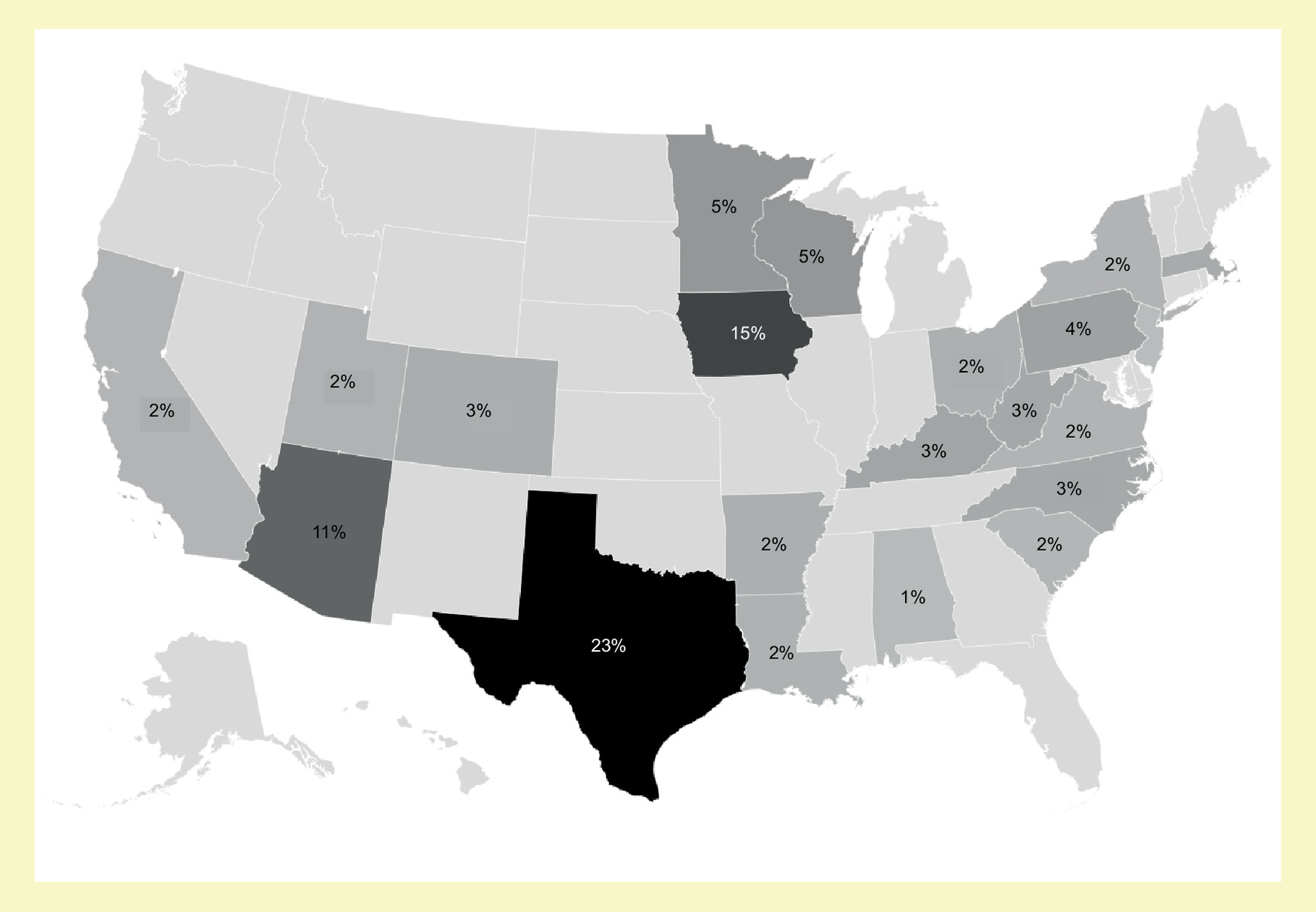
A total of 34,751,020 patients were queried across the 30 US sites. The annual prevalence of SM was relatively constant: 2012 (n = 6120), 2013 (n = 6080), 2014 (n = 5430), 2015 (n = 5550), 2016 (n = 5600) and the projected data for 2017 (n = 5265). The most prominent fungal infections were histoplasmosis (43.8%), aspergillosis (37.7%) and coccidioidomycosis (14.0%) (Table 1). In total, data from 33,230 patients with SM were available for initial analysis (Table 1); 39% showed treatment with antifungal medications in their EMRs (n = 13,181). Geographically, patients received care in 30 sites, with three sites accounting for over half of all cases: University of Texas Southwestern Medical Center (23%), University of Iowa Hospitals and Clinics (15%) and University of Arizona (11%) (Figure 1.)
| Disease | n | % | ICD-10 code |
|---|---|---|---|
| Aspergillosis | 12,530 | 37.7 | B44 |
| Blastomycosis | 1080 | 3.2 | B40 |
| Chromomycosis and pheomycotic abscess | 190 | 0.6 | B43 |
| Coccidioidomycosis | 4650 | 14.0 | B38 |
| Histoplasmosis | 14,560 | 43.8 | B39 |
| Paracoccidioidomycosis | 80 | 0.2 | B41 |
| Sporotrichosis | 310 | 0.9 | B42 |
| Systemic mycoses (total) | 33,230 | 100.4† |
EMR sampled 26 October 2017.
†
Total >100% due to a small number of patients with more than one infection.
EMR: Electronic medical record.
Patients with specified SM (histoplasmosis, aspergillosis and blastomycosis) with at least one prescription for one of 11 specific antifungal agents were further categorized: otherwise healthy cohort (n = 2321; 17.2%), aged ≥65 years (n = 769; 5.7%), immunosuppressant medication (n = 5513; 40.7%), cancer (n = 3284; 24.3%), transplant recipients (n = 1099; 8.1%) and HIV/AIDS (n = 532; 3.9%) (Table 2). Patient characteristics for the SM study cohorts are provided in Table 2. The mean ages across the study cohorts were consistent, (50–57 years), excluding the elderly cohort. The HIV/AIDS cohort was notable for three characteristics, youngest mean age (50 years), mainly male (highest proportion, 79%) and lowest proportion of white race (44%). Patients with SM were far more likely to be immunocompromised (77.0%) (cancer [24.3%], transplant recipients [8.1%], HIV/AIDS [3.9%] or receiving systemic immunosuppressant therapy [40.7%]) than not immunocompromised (22.9%) (otherwise healthy [17.2%] or age >65 [5.7%]).
| Patient cohorts | Otherwise healthy | Age ≥ 65 | Immunosuppressant medication | Cancer | Transplant recipient | HIV |
|---|---|---|---|---|---|---|
| n, (%) | 2321 (17.2) | 769 (5.7) | 5513 (40.7) | 3284 (24.3) | 1099 (8.1) | 532 (3.9) |
| Age, mean (SD), years | 52 (21) | 74 (7) | 55 (20) | 57 (19) | 55 (16) | 50 (12) |
| Male, % | 51 | 54 | 50 | 53 | 62 | 79 |
| White, % | 65 | 71 | 77 | 78 | 76 | 44 |
| African–American, % | 16 | 11 | 13 | 12 | 13 | 39 |
No specific data were available on age ranges or on racial breakdown of remaining patients.
SD: Standard deviation.
Table 3 compares symptom burden in SM patients who were aged over 65 years (elderly) or immunocompromised versus the otherwise healthy patients (reference cohort) with systemic mycoses. The symptom burden experienced by elderly SM patients for almost all symptoms and symptom classes was broadly similar to the reference cohort, exceptions were the higher prevalence of malaise and fatigue, edema and metabolic symptoms (hypertension, hyperlipidemia and diabetes mellitus) in elderly patients.
| Study cohorts | Healthy (reference) n = 2321 (%) | Age >65 years n = 769 | Immunosuppressant medication n = 5513 | Cancer n = 3284 | Transplant recipient n = 1099 | HIV-positive n = 532 | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| List of symptoms | % | Δ%† | % | Δ%† | % | Δ%† | % | Δ%† | % | Δ%† | |
| Constitutional symptoms | |||||||||||
| Malaise and fatigue | 11.10 | 15.70 | 41 | 12.86 | 16 | 56.97 | 413 | 34.68 | 213 | 46.80 | 322 |
| Depression, other mood disorders | 10.34 | 11.65 | 13 | 13.79 | 33 | 35.72 | 246 | 22.12 | 114 | 44.17 | 327 |
| Headache | 5.15 | 4.43 | -14 | 6.55 | 27 | 36.51 | 609 | 18.70 | 263 | 36.28 | 605 |
| Vision disturbances | 3.04 | 3.42 | 13 | 3.25 | 7 | 20.86 | 587 | 7.02 | 131 | 25.75 | 748 |
| Sleep disorder | 7.59 | 10.25 | 35 | 13.21 | 74 | 41.08 | 441 | 21.16 | 179 | 27.82 | 266 |
| Fever | 8.86 | 7.85 | -11 | 10.24 | 16 | 65.41 | 638 | 46.97 | 430 | 52.26 | 490 |
| Pain | 6.37 | 5.32 | -17 | 9.39 | 47 | 36.57 | 474 | 15.19 | 138 | 29.51 | 363 |
| Dizziness | 2.78 | 3.92 | 41 | 3.42 | 23 | 21.59 | 675 | 9.66 | 247 | 21.99 | 690 |
| Edema | 5.82 | 9.37 | 61 | 9.77 | 68 | 39.25 | 574 | 21.95 | 277 | 24.44 | 320 |
| Rash | 3.80 | 3.42 | -10 | 4.62 | 22 | 38.92 | 925 | 21.77 | 473 | 33.27 | 776 |
| Abnormal weight loss | 4.22 | 4.94 | 17 | 5.12 | 21 | 22.14 | 425 | 6.85 | 62 | 28.01 | 564 |
| Respiratory symptoms | |||||||||||
| Dyspnea | 19.58 | 23.16 | 18 | 24.20 | 24 | 63.61 | 225 | 38.81 | 98 | 56.58 | 189 |
| Pain in throat & chest | 12.36 | 12.91 | 4 | 12.75 | 3 | 48.87 | 295 | 22.39 | 81 | 51.13 | 314 |
| Cough | 13.76 | 14.18 | 3 | 16.40 | 19 | 55.05 | 300 | 23.79 | 73 | 55.45 | 303 |
| Metabolic symptoms | |||||||||||
| Hypertension | 26.37 | 41.01 | 56 | 34.87 | 32 | 68.54 | 160 | 54.96 | 108 | 53.38 | 102 |
| Hyperlipidemia | 12.11 | 21.77 | 80 | 16.92 | 40 | 37.52 | 210 | 21.33 | 76 | 32.14 | 165 |
| Diabetes mellitus | 18.57 | 23.04 | 24 | 24.65 | 33 | 37.52 | 102 | 29.32 | 58 | 19.36 | 4 |
| Hypokalemia | 6.84 | 7.47 | 9 | 9.12 | 33 | 52.07 | 662 | 34.50 | 405 | 35.71 | 422 |
| Gastrointestinal symptoms | |||||||||||
| Abdominal/ pelvic pain | 10.46 | 9.87 | -6 | 12.46 | 19 | 53.7 | 414 | 30.47 | 191 | 52.82 | 405 |
| Gastroesophageal reflux disease | 13.88 | 15.32 | 10 | 26.60 | 92 | 54.93 | 296 | 28.80 | 107 | 30.26 | 118 |
| Nausea and vomiting | 7.93 | 7.34 | -7 | 11.34 | 43 | 61.48 | 675 | 43.28 | 446 | 45.86 | 478 |
| Diarrhea | 6.50 | 7.34 | 13 | 10.16 | 56 | 57.64 | 787 | 43.55 | 570 | 49.44 | 661 |
| Infections | |||||||||||
| Influenza/ pneumonia | 20.08 | 21.39 | 7 | 24.69 | 23 | 72.53 | 261 | 41.62 | 107 | 61.09 | 204 |
| Acute upper respiratory | 5.91 | 4.94 | -16 | 7.40 | 25 | 42.63 | 622 | 16.24 | 175 | 32.89 | 457 |
| Severe sepsis | 3.21 | 5.06 | 58 | 5.64 | 76 | 30.05 | 837 | 11.50 | 259 | 18.98 | 492 |
As the queries were performed in real-time, the number of patients in each population may vary slightly.
†
Δ% = percent difference compared with healthy controls; unbolded values correspond to p-values >0.01; bold values correspond to p-values <0.01.
All metabolic symptoms, including hypokalemia, were significantly more prevalent in patients on immunosuppressants. Among patients on immunosuppressants, symptom burden was significantly higher among those with SM compared with the control cohort, but the difference in symptom burden for the SM versus control cohort was even more pronounced in the cohorts with cancer, transplant recipients and patients with a history of HIV infection. In those three cohorts, virtually all symptoms were significantly more prevalent in the SM cohort than in the reference cohort, with the exceptions of diabetes mellitus in the HIV/AIDS cohort and abdominal/pelvic pain and acute upper respiratory tract infection in the immunosuppressant cohort (Table 3).
Symptom burden in immunocompromised patients with SM (on immunosuppressants, with cancer, transplant recipients or HIVAIDS) was also compared with patients with the same immunocompromising feature or condition, but without systemic mycoses (control cohorts). The control cohorts (matched non-systemic mycoses) had substantially larger samples sizes: immunosuppressants (n = 4,166,383), cancer (n = 774,313), transplant recipients (n = 37,913) and HIV/AIDS patients (n = 91,275). Patient cohorts with SM and cancer or HIV/AIDS show a uniformly consistent higher prevalence for all symptoms listed (Table 4). Furthermore, when compared with control cohorts of comparable patients without SM (measured as Δ%), SM patients with cancer or HIV/AIDS had much higher rates of constitutional symptoms (cancer 999%; HIV/AIDS 760%), respiratory symptoms (1190%; 624%), metabolic symptoms (630%; 450%), gastrointestinal symptoms (844%; 576%) and infections (i.e., influenza and pneumonia, acute upper respiratory infection and severe sepsis) (2265%; 955%) (Table 4).
| Study cohorts | Immunosuppressant medication | Cancer | Transplant recipient | HIV-positive | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| List of symptoms | Control cohort n = 4,166,383 | SM cohort n = 5513 | Percent difference | Control cohort n = 774,313 | SM cohort n = 3284 | Percent difference | Control cohort n = 37,913 | SM cohort n = 1099 | Percent difference | Control cohort n = 91,275 | SM cohort n = 532 | Percent difference |
| % | % | Δ% | % | % | Δ% | % | % | Δ% | % | % | Δ% | |
| Constitutional symptoms | ||||||||||||
| Malaise and fatigue | 3.72 | 12.86 | 246 | 6.63 | 56.97 | 759 | 20.68 | 34.68 | 68 | 5.47 | 46.80 | 756 |
| Depression, other mood disorders | 5.83 | 13.79 | 137 | 6.47 | 35.72 | 452 | 15.53 | 22.12 | 42 | 15.32 | 44.17 | 188 |
| Headache | 3.48 | 6.55 | 88 | 3.17 | 36.51 | 1050 | 9.59 | 18.70 | 95 | 5.11 | 36.28 | 610 |
| Vision disturbances | 1.62 | 3.25 | 100 | 1.57 | 20.86 | 1230 | 3.29 | 7.02 | 114 | 3.21 | 25.75 | 703 |
| Sleep disorder | 5.31 | 13.21 | 149 | 5.54 | 41.08 | 642 | 17.71 | 21.16 | 19 | 4.64 | 27.82 | 500 |
| Fever | 3.08 | 10.24 | 233 | 4.32 | 65.41 | 1415 | 27.38 | 46.97 | 72 | 4.60 | 52.26 | 1035 |
| Pain | 3.8 | 9.39 | 141 | 4.88 | 36.57 | 650 | 12.76 | 15.19 | 19 | 3.34 | 29.51 | 783 |
| Dizziness | 1.76 | 3.42 | 94 | 1.92 | 21.59 | 1024 | 5.71 | 9.66 | 69 | 1.95 | 21.99 | 1028 |
| Edema | 1.86 | 9.77 | 425 | 2.97 | 39.25 | 1220 | 18.54 | 21.95 | 18 | 1.90 | 24.44 | 1189 |
| Rash | 3.94 | 4.62 | 17 | 2.61 | 38.92 | 1388 | 12.52 | 21.77 | 74 | 4.27 | 33.27 | 680 |
| Abnormal weight loss | 0.79 | 5.12 | 550 | 1.75 | 22.14 | 1161 | 4.72 | 6.85 | 45 | 2.83 | 28.01 | 890 |
| Average | 198 | 999 | 57 | 760 | ||||||||
| Respiratory symptoms | ||||||||||||
| Dyspnea | 5.85 | 24.20 | 314 | 5.33 | 63.61 | 1094 | 21.28 | 38.81 | 82 | 7.87 | 56.58 | 619 |
| Pain in throat and chest | 4.29 | 12.75 | 197 | 4.31 | 48.87 | 1033 | 14.37 | 22.39 | 56 | 7.03 | 51.13 | 627 |
| Cough | 6.34 | 16.40 | 159 | 3.57 | 55.05 | 1444 | 12.35 | 23.79 | 93 | 7.64 | 55.45 | 626 |
| Average | 223 | 1190 | 77 | 624 | ||||||||
| Metabolic symptoms | ||||||||||||
| Hypertension | 17.19 | 34.87 | 103 | 17.90 | 68.54 | 283 | 65.36 | 54.96 | -16 | 19.41 | 53.38 | 175 |
| Hyperlipidemia | 8.70 | 16.92 | 94 | 8.63 | 37.52 | 335 | 29.24 | 21.33 | -27 | 8.05 | 32.14 | 299 |
| Diabetes mellitus | 7.08 | 24.65 | 248 | 7.66 | 37.52 | 390 | 34.88 | 29.32 | -16 | 7.48 | 19.36 | 159 |
| Hypokalemia | 1.43 | 9.12 | 538 | 3.23 | 52.07 | 1511 | 26.35 | 34.50 | 31 | 2.82 | 35.71% | 1168 |
| Average | 246 | 630 | -7 | 450 | ||||||||
| Gastrointestinal symptoms | ||||||||||||
| Abdominal/pelvic pain | 5.51 | 12.46 | 126 | 6.7 | 53.7 | 700 | 22.30 | 30.47 | 37 | 8.74 | 52.82 | 504 |
| Gastroesophageal reflux disease | 7.76 | 26.60 | 243 | 7.97 | 54.93 | 589 | 28.06 | 28.80 | 3 | 6.15 | 30.26 | 392 |
| Nausea and vomiting | 3.66 | 11.34 | 210 | 7.04 | 61.48 | 773 | 33.3 | 43.28 | 30 | 5.61 | 45.86 | 717 |
| Diarrhea | 2.09 | 10.16 | 385 | 4.07 | 57.64 | 1315 | 33.60 | 43.55 | 30 | 6.26 | 49.44 | 690 |
| Average | 241 | 844 | 25 | 576 | ||||||||
| Infections | ||||||||||||
| Influenza and pneumonia | 3.07 | 24.69 | 705 | 3.09 | 72.53 | 2250 | 16.92 | 41.62 | 146 | 7.75 | 61.09 | 689 |
| Acute upper respiratory | 11.59 | 7.40 | -36 | 3.76 | 42.63 | 1035 | 9.02 | 16.24 | 80 | 4.58 | 32.89 | 619 |
| Severe sepsis | 0.46 | 5.64 | 1114 | 0.83 | 30.05 | 3512 | 5.30 | 11.50 | 117 | 1.14 | 18.98 | 1558 |
| Average | 594 | 2266 | 114 | 955 | ||||||||
As the queries were performed in real-time, the number of patients in each population may vary slightly, Δ% = percent difference, unbolded values correspond to p-values >0.01; bold values correspond to p-values <0.01.
SM: Systemic mycoses.
Patients with SM and on immunosuppressants also bore a significantly higher symptom burden compared with their control cohort, albeit with numerically lower percentage differences compared with the cancer or HIV/AIDS patients. Transplant recipients appeared to show the lowest percentage differences in symptom prevalence compared with their respective control cohort, notably, in pain and gastroesophageal reflux disease, the differences were not significant. For three metabolic symptoms, rates were significantly lower in systemic mycoses patients compared with control cohort [hypertension (-16%), hyperlipidemia (-27%) and diabetes mellitus (-16%).
Antifungal treatment utilization among the patients with SM is summarized for the six study cohorts in Table 5. Drug utilization adds up to over 100% because some patients received more than one antifungal agent, either in combination or sequentially, during the data collection period. Fluconazole was the most commonly prescribed treatment when measured across all cohorts, with 56.0% (weighted average) of all patients using this medication, followed by voriconazole (53.5%) and itraconazole (19.5%). Liposomal amphotericin B was prescribed at an intermediate rate (11.6%) (Table 5). Treatment utilization was consistent for the top three antifungals across cohorts; however, more itraconazole was prescribed on a percentage basis than voriconazole for HIV/AIDS patients. Slightly more voriconazole than fluconazole was prescribed for patients on immunosuppressant medication (45.70 vs 41.09%) and patients with cancer (69.86 vs 66.86%). Notably, although itraconazole use was third-most frequent antifungal across all cohorts, its use in transplant recipient patients was lower and it was ranked 7th as antifungal treatment in these patients (Table 5).
| Study cohort | Weighted average | Otherwise healthy (n = 2321) | Age >65 (n = 769) | Immunosuppressant medication (n = 5513) | Cancer (n = 3284) | Transplant recipient (n = 1099) | HIV (n = 532) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antifungal | % | n | % | n | % | n | % | n | % | n | % | n | % |
| Fluconazole | 56.05 | 1067 | 45.02 | 306 | 38.73 | 2212 | 41.09 | 2259 | 66.68 | 902 | 82.07 | 367 | 68.98 |
| Itraconazole | 19.50 | 594 | 25.06 | 156 | 19.75 | 1386 | 25.75 | 440 | 12.99 | 88 | 8.01 | 200 | 37.59 |
| Voriconazole | 53.51 | 600 | 25.32 | 257 | 32.53 | 2460 | 45.70 | 2367 | 69.86 | 844 | 76.80 | 119 | 22.37 |
| Posaconazole | 13.94 | 135 | 5.70 | 54 | 6.84 | 394 | 7.32 | 714 | 21.07 | 299 | 27.21 | 20 | 3.76 |
| Ketoconazole | 6.90 | 135 | 5.70 | 59 | 7.47 | 359 | 6.67 | 256 | 7.56 | 53 | 4.82 | 68 | 12.78 |
| Amphoterecin B | 3.60 | 58 | 2.45 | 16 | 2.08 | 170 | 3.08 | 145 | 4.72 | 47 | 4.28 | 10 | 1.88 |
| Amphotericin B liposomal | 11.57 | 143 | 6.03 | 46 | 5.82 | 468 | 8.69 | 518 | 15.29 | 166 | 15.10 | 94 | 17.67 |
| Caspofungin | 7.26 | 19 | 0.80 | 12 | 1.52 | 174 | 3.23 | 463 | 13.67 | 123 | 11.19 | 13 | 2.44 |
| Micafungin | 15.10 | 116 | 4.89 | 53 | 6.71 | 424 | 7.88 | 751 | 22.17 | 356 | 32.39 | 32 | 6.02 |
| Flucytosine | 0.23 | 10 | 0.42 | 0 | 0 | 13 | 0 | 10 | 0 | 10 | 0.9 | 10 | 1.88 |
| Terbinafine | 2.81 | 99 | 4.18 | 30 | 3.80 | 162 | 3.01 | 86 | 2.54 | 12 | 1.09 | 18 | 3.38 |
Healthcare resource utilization (HCRU) over a 6-month period was assessed and patients with SM consistently utilized all three HCRU modes (ER [emergency room], hospitalisation or outpatient visits) more frequently than their corresponding control cohorts, with the exception of ER visits for patients on immunosuppressant medications, 20.2% of patients with SM compared with 32.4% of control patients on immunosuppressants presenting to ER (Table 6). Highest hospitalization rates were observed in SM transplant recipients (74.5%), followed by non-SM transplant recipients (65.1%). SM patients who underwent transplant and SM with cancer showed the highest rates of outpatient visits, 82.3 and 67.0%, respectively (Table 6). Generally (with one exception noted above), across all patient cohorts with SM, there was higher HCRU compared with the control study cohorts without systemic mycoses, these differences were statistically significant (p < 0.01) (Table 6).
| Cohorts | Otherwise healthy | Age >65 | Immunosuppressant medication | Cancer | Transplant recipients | HIV/AIDS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of patients | n = 2321 | n = 769 | Control 4,166,383 | SM 5513 | % difference | Control 775,313 | SM 3284 | % difference | Control 37,913 | SM 1099 | % difference | Control 91,275 | SM 532 | % difference |
| % | % | % | % | Δ% | % | % | Δ% | % | % | Δ% | % | % | Δ% | |
| Outpatient | 62.0 | 62.6 | 46.6 | 56.5 | 21.2 | 51.5 | 67.0 | 30.1 | 73.0 | 82.3 | 12.7 | 48.2 | 60.2 | 24.9 |
| ER | 15.9 | 13.9 | 32.4 | 20.2 | -37.7 | 7.61 | 22.5 | 196 | 20.3 | 26.0 | 28.1 | 16.9 | 30.3 | 79.3 |
| Hospitalization | 26.6 | 32.5 | 17.5 | 36.9 | 110.9 | 8.88 | 50.2 | 465 | 65.1 | 74.5 | 14.4 | 13.3 | 39.1 | 194 |
Bold values are statistically significant p < 0.01.
ER: Emergency room; SM: Systemic mycoses.
Discussion
This study evaluated outcomes associated with the burden of illness for patients with SM, focusing on those eligible for itraconazole treatment according to its approved uses in the USA. In this study, a majority of patients were immunocompromised in some manner (77.0%), with the data showing that these patients (whether cancer or HIV patients, those on immunosuppressant therapy or transplant recipients) have a significantly higher overall burden of illness than SM patients that are otherwise healthy or elderly (≥65 years old). Given the magnitude in the frequency of reported symptoms for the immunocompromised cohorts, these patients have a substantially greater burden of illness arising from systemic mycoses. Because the database captures symptoms regardless of cause, it is also possible that these patients had a greater symptom burden due to comorbid conditions and/or adverse effects of treatment, in addition to the effects of SM infection.
The relative percentage of constitutional symptoms which were experienced in both otherwise healthy and elderly SM cohorts may be secondary to comorbidities and age-related physiological changes leading to increased patient symptomatology (Flevari et al.) [13]. This is consistent with our study findings where a higher incidence of constitutional symptoms was observed in the elderly healthy cohort compared with otherwise healthy younger (i.e., < 65 years old) patients. It would be useful to have additional detail beyond what was available in this database in order to better understand the relationship between age and burden of systemic mycoses. It was also noted that SM patients in the immunosuppressed cohort experienced higher rates of constitutional symptoms when compared with both the otherwise healthy SM cohort and the immunosuppressed control groups that did not have SM, findings that suggest the immunosuppressed population may have had a greater burden of disease.
The largest differences in symptom burden in SM immunocompromised patients (i.e., immunosuppressant medication, cancer, transplant or HIV) compared with otherwise healthy SM patients were observed in cancer patients as shown in Table 3. Additionally, in cancer patients with SM compared with cancer without SM, there was commonly 10–20× greater incidence of many reported symptoms, across all symptom classes. As these patients are frequently neutropenic secondary to recent chemotherapy it is not surprising that more severe symptoms were observed in this cohort. This high symptom burden is also likely exacerbated by the documented concomitant mental, physical and emotional distress that accompanies an active cancer diagnosis along with symptom burden for patients with systemic mycoses [14].
Respiratory symptoms were common in patients with SM in this study, reflecting that the predominant site of infection in these patients is the lung [15,16]. The rates of pulmonary symptoms in all immunosuppressed patients with systemic mycoses were higher than the otherwise healthy counterparts that have systemic mycoses. Constitutional symptoms such as fever, malaise, pain, abnormal weight loss, were increasingly prevalent across the spectrum with SM from otherwise healthy patients (4–11%); elderly patients (5–16%) to cancer patients (22–57%) (Table 3). Other sites of infection for the target organisms include the bloodstream, splenic and liver abscess, urinary tract and central nervous systemic sites [17].
The observed increases in prevalence of metabolic symptoms in SM patients compared with control cohorts may be due to direct effects of infection on metabolism or exacerbation of comorbidities during active and ongoing infection. Alternatively, infection of endocrine organs, thus adversely affecting regulatory controls on metabolism may contribute to observed rates of metabolic symptoms [18,19]. In addition, current antifungal agents (polyenes, azoles) used for prophylaxis and/or treatment of mycoses also have adverse endocrine and metabolic effects, including hypoadrenalism, hypogonadism, hypoglycemia, dyslipidemia and hyperkalemia or hypokalemia [18,20,21].
Gastrointestinal infection by SM pathogens is uncommon [22]. Gastrointestinal symptoms tend to be nonspecific (e.g., nausea) unless distinct organs such as the liver, bowel, or pancreas are directly invaded. The results reported in this study for the rates of gastrointestinal symptoms arising from SM are consistent with similar findings from prior research, with the highest incidences in the cancer cohort, relatively less of an increase compared with control in the HIV cohort and the transplant cohort mostly resembling the otherwise healthy cohort.
With rising incidence of invasive fungal infections, the burden of symptoms in patients at high-risk of fungal infections is a high priority for healthcare professional and decision-makers. In one large epidemiological study of invasive fungal infections utilizing data from an integrated US health network (Intermountain Healthcare), invasive fungal infections were associated with a high rate of hospital admissions (76.2%) and high 1-year all-cause mortality rate of 28.8% [2]. The conditions or diseases that place patients at higher risk for invasive fungal infections are themselves associated with high symptom burden. This study documented the very high rates of constitutional, respiratory, metabolic, gastrointestinal and infection-related symptoms that are attributable to SM or the accompanying treatment. This study also documented substantially increased HCRU rates attributable to SM.
Given the high burden of SM in terms of symptoms and HCRU, there is a clear impetus for timely diagnosis of SM with identification of the pathogen, which can improve outcomes through prompt initiation of the appropriate antifungal therapy. Currently, many hospitals must send testing off-site for aspergillus and histoplasmosis, which can delay diagnosis and initiation of targeted treatment [23,24]. Of note, 56% of prescriptions in this study were for fluconazole, which is inactive against aspergillosis (38% of diagnoses) and less effective than itraconazole against histoplasmosis and blastomycosis, which together accounted for 47% of diagnoses [8,24,25]. Thus, a substantial number of patients were receiving fluconazole for a disease not optimally treated with this agent. It is possible that fluconazole is sometimes prescribed empirically until fungal testing results are available or fluconazole may be chosen due to limited drug–drug interactions and predictable bioavailability [26].
Future research in larger populations, including among patients with other forms of SM beyond the three pathogens studied here, would be valuable in establishing the burden of SM more broadly. This study was intentionally narrowly focused on pathogens of interest based on our objective of understanding the patient population eligible for itraconazole treatment in the USA, but there would be value in conducting similar analyses on other systemic fungal infections, including candidiasis, cryptococcosis, mucormycosis and pneumocystis infection. It would also be useful to study treatment patterns and outcomes of treatment using real-world evidence, to better understand whether patients are being adequately treated or if there is unmet clinical need in SM.
Limitations
The main limitation in utilizing ‘live’ cross-sectional EMR data relates to the lack of longitudinal data, patients diagnosed with systemic mycoses based on ICD-10 codes were the starting point for data capturing. Capturing EMR data at a fixed point in time precludes re-running the analysis to include or exclude features not accounted for at the time of querying. It is important to note that the EMR database interrogated gives insight into the rate of symptoms experienced per cohort, but not the severity, nor the duration of impact at the patient level or clinical significance of these symptoms (potentially responsible for delays in next chemotherapy cycle etc). In addition, it is acknowledged that there are limitations to the estimates of healthcare resource utilization, as the total HCRU cannot be fully determined from the EMR data available (e.g., supplemental nursing support, at-home care, rehabilitation support, etc.). HCRU was measured as the percentage of total number of patients in the specified group that sought care. This would not account for repeat visits; hence, HCRU would likely be underestimated if there were repeat visits by patients in those groups (i.e., SM patients) shown to use more healthcare resources. HCRU was also not captured at a high level of granularity; for example, hospitalization is not further divided into intensive care unit versus standard unit care. Finally, although different lipid formulations of amphotericin B are available, this level of granularity was not available using the data extraction tools from this EMR network.
Conclusion
To the authors’ knowledge, this is the first study which evaluates the real-world symptom burden and HCRU attributable to systemic mycoses in patients with additional select comorbid conditions. Of note, the observation that the majority of patients who contract a systemic fungal infection are immunocompromised is significant. Given the rising age profile of the US population, associated increases in the rates of serious illnesses including cancers, conditions requiring organ transplants and other chronic conductions that result in long-term compromised immune responses, it is expected that there will be a corresponding increase in high-risk patients vulnerable to invasive fungal infections. The nature of the comorbidities affecting these patients causes substantial symptomatic burden of illness.
This study provides a basis and reference point for further investigation of quality of life in patients with SM, as well as corresponding healthcare resource utilization and economic burden.
•
Despite advances in antifungal therapy, mortality rates for invasive fungal diseases remain high, with immunocompromised patients especially vulnerable to opportunistic infection.
•
This study queried electronic medical records of over 34 million patients from 2012 to 2017 in the USA to evaluate the burden of illness, healthcare resource utilization and real-world outcomes in patients treated with antifungal medications, with a focus on histoplasmosis, blastomycosis and aspergillosis.
•
Symptomatic burden experienced by each of the otherwise healthy or age >65 or immunosuppressed cohorts receiving antifungal therapy for systemic mycoses (SM) was comparable but significantly greater in cancer or HIV patients and transplant recipients.
•
Among the patient cohorts with SM, those in which patients also had cancer or HIV/AIDS showed a consistently higher prevalence for all symptoms listed.
•
The most commonly prescribe treatments were fluconazole (56.0%), voriconazole (53.5%) and itraconazole (19.5%).
•
The highest hospitalization rates were observed in transplant recipients with SM (74.5%), who also had the highest rates of outpatient visits (82.3%).
•
Healthcare resource utilization was higher across all patient cohorts with SM relative to control cohorts without SM infection.
Acknowledgments
Parts of this study were previously published at the International Society for Human and Animal Mycology, Congress of the European Hematology Association and International Immunocompromised Host Society Symposium in 2018.
Financial & competing interests disclosure
G Lewis and R Jordan are employees of Mayne Pharma, which sponsored the research. A Forsythe is an employee of Purple Squirrel Economics, which acted as a consultant to Mayne Pharma. GR Thompson III acted as a consultant to Mayne Pharma. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
K Sandman of Purple Squirrel Economics provided editorial support. This work was sponsored by Mayne Pharma.
References
Papers of special note have been highlighted as: • of interest
1.
De Pauw BE. What are fungal infections? Mediterr. J. Hematol. Infect. Dis. 3(1), e2011001 (2011).
2.
Webb BJ, Ferraro JP, Rea S, Kaufusi S, Goodman BE, Spalding J. Epidemiology and clinical features of invasive fungal infection in a US health care network. Open Forum Infect. Dis. 5(8), ofy187 (2018).
• Real-world evidence from a US database on invasive fungal infections.
3.
Pfaller MA, Diekema DJ. Epidemiology of invasive mycoses in North America. Crit. Rev. Microbiol. 36(1), 1–53 (2010).
4.
Pegorie M, Denning DW, Welfare W. Estimating the burden of invasive and serious fungal disease in the United Kingdom. J. Infection 74(1), 60–71 (2017).
5.
Benedict K, Derado G, Mody RK. Histoplasmosis-associated hospitalizations in the United States, 2001–2012. Open Forum Infect. Dis. 3(1), ofv219 (2016).
6.
Low C-Y, Rotstein C. Emerging fungal infections in immunocompromised patients. F1000 Med. Rep. 3, 14 (2011)
7.
McNeil MM, Nash SL, Hajjeh RA et al. Trends in mortality due to invasive mycotic diseases in the United States, 1980–1997. Clin. Infect. Dis. 33(5), 641–647 (2001).
8.
Enoch DA, Yang H, Aliyu SH, Micallef C. The changing epidemiology of invasive fungal infections. In: Human Fungal Pathogen Identification. Methods in Molecular Biology, Vol. 1508. Lion T (Ed.). Humana Press, NY, USA, (2017).
9.
US Department of Health and Human Services. Organ Procurement and Transplantation Network (OPTN). (2020). https://optn.transplant.hrsa.gov/
10.
Garbee DD, Pierce SS, Manning J. Opportunistic fungal infections in critical care units. Crit. Care Nurs. Clin. N. Am. 29(1), 67–79 (2017).
11.
Lockhart SR, Guarner J. Emerging and reemerging fungal infections. Semin. Diag. Pathol. 36(3), 177–181 (2019).
• Comprehensive review of fungal infections with a focus on the Americas.
12.
Miller RA. A case for antifungal stewardship. Curr. Fungal Infect. Rep. 12(1), 33–43 (2018).
13.
Flevari A, Theodorakopoulou M, Velegraki A, Armaganidis A, Dimopoulos G. Treatment of invasive candidiasis in the elderly: a review. Clin. Interv. Aging 8, 1199–1208 (2013).
14.
Meijer A, Roseman M, Delisle VC et al. Effects of screening for psychological distress on patient outcomes in cancer: a systematic review. J. Psychosomat. Res. 75(1), 1–17 (2013).
15.
Razzuk MA, Urschel HC, Paulson DL. Systemic mycoses – primary pathogenic fungi. Ann. Thorac. Surg. 15(6), 644–660 (1973).
16.
Sherif R, Segal BH. Pulmonary aspergillosis: clinical presentation, diagnostic tests, management and complications. Curr. Opin. Pulm. Med. 16(3), 242–250 (2010).
17.
Badiee P, Hashemizadeh Z. Opportunistic invasive fungal infections: diagnosis & clinical management. Indian J. Med. Res. 139(2), 195–204 (2014).
18.
Lionakis MS, Samonis G, Kontoyiannis DP. Endocrine and metabolic manifestations of invasive fungal infections and systemic antifungal treatment. Mayo Clin. Proc. 83(9), 1046–1060 (2008).
19.
Ruhnke M, Schwartz S. Recent developments in the management of invasive fungal infections in patients with oncohematological diseases. Ther. Adv. Hematol. 7(6), 345–359 (2016).
• Review on the diagnosis and treatment of fungal infections in hematologic oncology.
20.
Chang Y-L, Yu S-J, Heitman J, Wellington M, Chen Y-L. New facets of antifungal therapy. Virulence 8(2), 222–236 (2017).
21.
Thompson GR, Chang D, Wittenberg RR, McHardy I, Semrad A. In vivo 11β-hydroxysteroid dehydrogenase inhibition in posaconazole-induced hypertension and hypokalemia. Antimicrob. Agents Chemother. 61(8), (2017).
22.
Avcu G, Karapinar DY, Yazici P et al. Difficult diagnosis of invasive fungal infection predominantly involving the lower gastrointestinal tract in acute lymphoblastic leukaemia. Med. Mycol. Case Rep. 11, 1–4 (2016).
23.
Denning DW, Perlin DS, Muldoon EG et al. Delivering on antimicrobial resistance agenda not possible without improving fungal diagnostic capabilities. Emerg. Infect. Dis. 23(2), 177–183 (2017).
24.
Limper AH, Adenis A, Le T, Harrison TS. Fungal infections in HIV/AIDS. Lancet Infect. Dis. 17(11), e334–e343 (2017).
25.
Salzer HJF, Burchard G, Cornely OA et al. Diagnosis and management of systemic endemic mycoses causing pulmonary disease. Respiration 96(3), 283–301 (2018).
26.
Kriengkauykiat J, Ito JI, Dadwal SS. Epidemiology and treatment approaches in management of invasive fungal infections. Clin. Epidemiol. 3, 175–191 (2011).
Information & Authors
Information
Published In
Pages: 573 - 584
PubMed: 32316748
Copyright
© 2020 Future Medicine Ltd.
History
Received: 4 February 2020
Accepted: 6 April 2020
Published online: 22 April 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
US database study: burden and healthcare resource utilization in adults with systemic endemic mycoses and aspergillosis. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0019
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Juliana G E Bartels, Simon K Camponuri, Theo T Snow, Brittany L Morgan Bustamante, Natalie J Kane, Rose M Reynolds, Aidan Lee, Mark A Hoffman, Theodore C White, Justin V Remais, Jennifer R Head, Updating the Epidemiology of Blastomycosis and Histoplasmosis in the United States, Using National Electronic Health Record Data, 2013–2023, The Journal of Infectious Diseases, 10.1093/infdis/jiaf472, 232, 6, (e1048-e1059), (2025).
- C Orla Morrissey, Hannah Y Kim, Tra-My N Duong, Eric Moran, Ana Alastruey-Izquierdo, David W Denning, John R Perfect, Marcio Nucci, Arunaloke Chakrabarti, Volker Rickerts, Tom M Chiller, Retno Wahyuningsih, Raph L Hamers, Alessandro Cassini, Valeria Gigante, Hatim Sati, Jan-Willem Alffenaar, Justin Beardsley, Aspergillus fumigatus —a systematic review to inform the World Health Organization priority list of fungal pathogens , Medical Mycology, 10.1093/mmy/myad129, 62, 6, (2024).
- Kaitlin Benedict, Hilary K Whitham, Brendan R Jackson, Economic Burden of Fungal Diseases in the United States, Open Forum Infectious Diseases, 10.1093/ofid/ofac097, 9, 4, (2022).