High-concentration nonavian high-molecular weight hyaluronan injections and time-to-total knee replacement surgery
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To examine the time-to-total knee replacement (TKR) surgery among patients with high-concentration nonavian high-molecular-weight hyaluronan injection (HMW-HA) compared with those without HA injections. Materials & methods: Using MarketScan® Commercial claims all patients aged 18–64 who underwent TKR surgery between 2008 and 2017 were identified. Time-to-TKR surgery was compared between patients receiving Orthovisc® (Anika Therapeutics Inc. Bedford MA, USA, referred to as nonavian HMW-HA) injections and patients who did not receive an HA injection. Results: The median time-to-TKR surgery was 893 days in the nonavian HMW-HA cohort and 399 days in the non-HA cohort (p < 0.001), a difference of 494 days (16.2 months). Conclusion: This study demonstrates that the time-to-TKR surgery is 16.2 months longer in patients who received treatment with nonavian HMW-HA injections.
Osteoarthritis (OA) is a chronic condition of the joints, impacting more than 30 million Americans [1]. The knee joint is the most commonly affected joint by OA andpatients with knee OA may encounter severe pain, aching and functional loss leading to disability-related productivity losses, reduced quality of life and increased financial burden [2,3]. There are an estimated 14 million individuals in the USA who have symptomatic knee OA [2]. The economic burden of knee OA in the USA is substantial, with an estimated 660,000 discharges for total knee replacement (TKR) and corresponding annual hospital charges of US$36.5 billion in 2014 [4]. Knee OA is expected to pose a considerable clinical and economic burden on the US healthcare system in the coming years due to the increasing utilization of TKR, growing obesity epidemic and aging population [5–9].
Several treatment options are available for controlling pain, improving function and potentially delaying the progression of knee OA. Treatment for pain management in knee OA includes oral analgesics, anti-inflammatories, intra-articular corticosteroid injections, platelet-rich plasma, stem cells and visco supplementation with hyaluronic acid (HA) injections [7]. Surgery, such as TKR, is usually reserved as the final treatment option for severe joint damage. Several preparations of intra-articular HAs have been approved by the US FDA for the treatment of pain in knee OA patients who have failed to respond adequately to conservative nonpharmacologic therapy and simple analgesics [10]. These HAs differ in physical composition (purified hyaluronan vs cross-linked hylans), molecular weight (high vs low), source (avian vs derived from bacterial cells), volume, HA concentration andfrequency of injection (multi-injection series vs single injection) [6]. Orthovisc® (DePuy Synthes) is high molecular weight (1.0–2.9 million Da), ultrapure natural (nonavian) hyaluronan derived from bacterial cells. It is administered in a series of 3–4 injections. Clinical efficacy and safety studies have demonstrated that Orthovisc provides significant improvements in pain for up to 6 months and have safety profiles similar to saline injection [11].
Most of the published clinical studies evaluating the efficacy of HAs in reducing pain have had observation periods in the range of 6 months [12]. Consequently, these studies were unable to examine the potential role of HAs in delaying the progression of disease over longer periods of time [12]. Given the limitations of these clinical studies, a number of real-world administrative claims database analyses were recently undertaken to determine whether HA use can delay TKR under longer time horizons [5,6,12,13]. These studies found that HA use does indeed delay TKR surgery. For example, results of a retrospective claims database analysis by Altman and colleagues found that patients receiving HA injections had a longer time-to-TKR surgery versus those who did not receive HA injections and the time-to-TKR increased with additional courses of HA injections [5].
However, little evidence exists about the specific impact of high concentration nonavian high-molecular weight hyaluronan (HMW-HA) on time-to-TKR surgery for patients with knee OA in the real-world setting. Per the authors knowledge, this paper marks the first in several publications looking at time-to-TKR surgery, utilizing a single-source HA. This study tests the hypothesis that patients receiving HMW-HA had a longer time-to-TKR surgery versus those who did not receive HA injections. The primary objective of this study was to retrospectively examine the time-to-TKR surgery of patients who had nonavian HMW-HA injection courses prior to TKR surgery compared with those who had no HA injections. The secondary objective was to examine the relationship between the number of nonavian HMW-HA courses and time-to-TKR.
Materials & methods
Study design & database
This retrospective study utilized the IBM MarketScan Commercial claims database. This database contains administrative claims and eligibility records for approximately 40 million enrollees in distinct sets of files for commercially insured individuals (i.e., working-age adults and their dependents). A standard extract from the database consists of three files: an enrollment file, a medical file and a drug file. The files are linkable based on an encrypted patient identification number. A prior retrospective commercial claims analysis study by Altman and colleagues explored the association between HA injections, using all types of HAs (2006–2011) and time-to-TKR surgery [5]. The present study updates the results of the prior study using recent data from 1 January 2008 to 31 December 2017 and subsets the HA cohort to patients only receiving Orthovisc (referred to as HMW-HA).
Study population
All commercially insured patients who underwent TKR surgery in inpatient settings throughout 1 January 2008 and 31 December 2017 and had a diagnosis for knee OA by an orthopedic surgeon prior to TKR were determined through claims with an International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) procedure code of 81.54 and associated ICD-10-CM procedure codes. The first entry of knee OA diagnosis in the data was identified as the index date. This criterion was used based on the clinical consideration that the diagnosis by someone other than an orthopedic surgeon would not clearly indicate knee problems related to TKR surgery. Patients’ time-to-TKR was defined as the time interval between the baseline date and that of TKR surgery. Patients were subjected to two additional screenings (Figure 1) and were required to have no other knee OA diagnosis visits to an orthopedic surgeon prior to initial knee OA diagnosis, defined as the ‘minimum clean period’ (MCP). The length of the MCP of the study population (90th percentile) was about 14 months (420 days) and spanned from the time between patients' first and second visits to the orthopedic surgeon. Patients were additionally required to demonstrate a minimum continuous enrollment (MCE) period of 7 years. This was derived from the sum of the MCP of 420 days and the time from initial diagnosis of knee OA to the date of TKR surgery or 2188 days (95th percentile), which totaled to 2608 days (or about 7.1 years). A MCE period was required to make sure all claims were available to record time to TKR accurately from initial OA diagnosis.
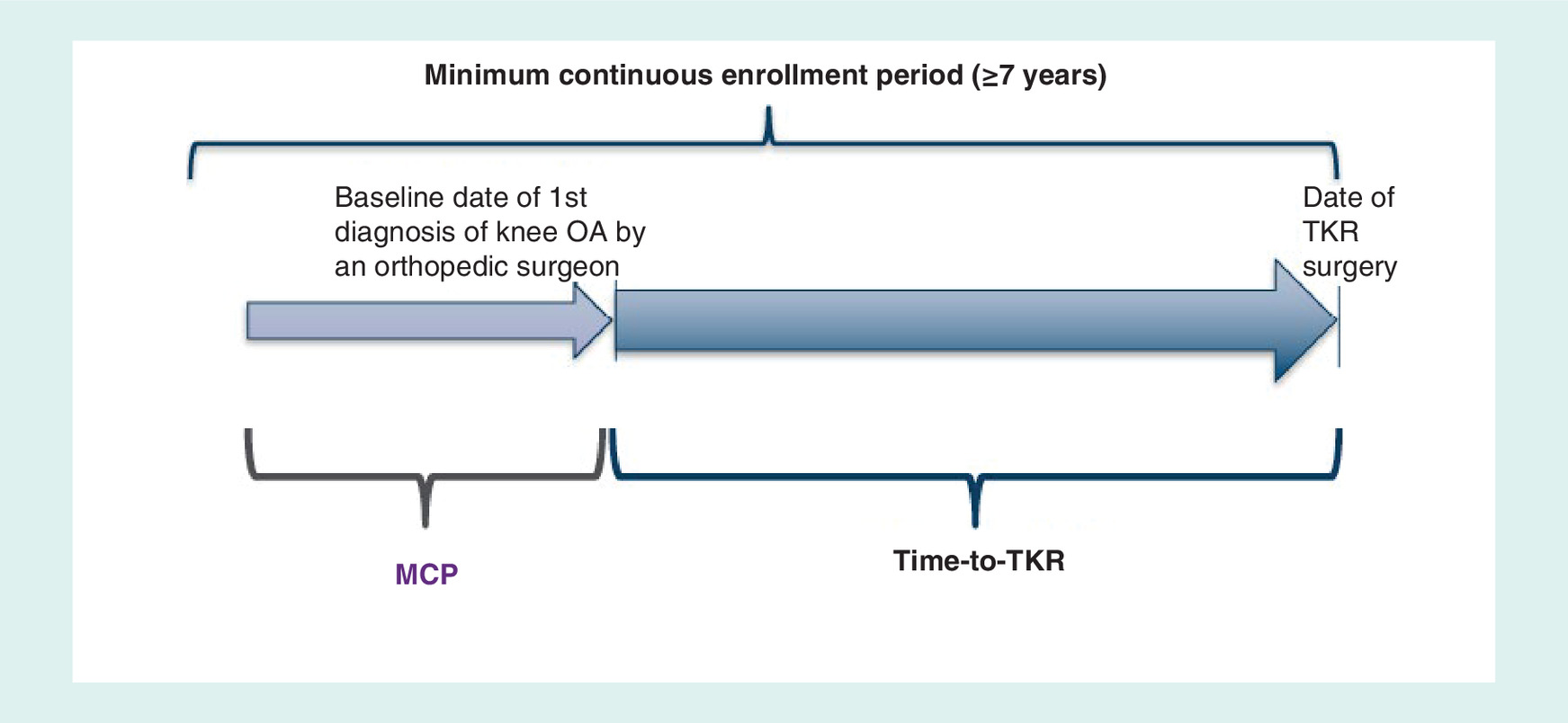
Figure 1. Minimum clean period and minimum continuous enrollment screenings for study population.
MCP with no other knee OA diagnosis visits to an orthopedic surgeon = 14 months.
MCE: Minimum continuous enrollment; MCP: Minimum clean period; OA: Osteoarthritis; TKR: Total knee replacement.
Study cohorts
The study population was grouped into two cohorts, one comprised of patients who had nonavian HMW-HA injections and the other of patients who did not have nonavian HMW-HA injections (or any other HA injection). Nonavian HMW-HA is administered as a series of 3–4 weekly injections within a 6-month period. The age group, gender and US geographic region of resident patients were determined for each study cohort.
Inclusion & exclusion criteria
Patients were included in the study if they were between 18 and 64 years of age at time of diagnosis for knee OA (as the database did not cover Medicare-eligible patients). Patients were excluded from the study if they met any of the following exclusion criteria: had other knee OA diagnosis visits to an orthopedic surgeon prior to the initial diagnosis date of knee OA, designated as MCP. This was to remove prevalent cases of knee OA; had prior HA injections (including nonavian HMW-HA) in the MCP and other HA injections from index date to TKR. This was to remove any prevalent users of HA and to restrict the cohort to only new users; had continuous enrollment below the MCE period. This was to remove patients that may have missing TKR claims due to loss of enrollment; had a TKR surgery in any setting any time prior to the first TKR surgery in inpatient settings identified between 1 January 2008 and 31 December 2017. This was to remove bilateral TKR cases and; had a diagnosis for revision TKR any time prior to the first TKR surgery in inpatient settings between 1 January 2008 and 31 December 2017. Revision TKR would indicate a prior TKR and hence this was to remove bilateral TKR cases.
Study end points
Time-to-TKR surgery was defined by the total number of days between the date of initial knee OA diagnosis and the date of the TKR surgery. For both the nonavian HME-HA and non-HA cohorts, the median and mean times-to-TKR surgery were evaluated, as was time-to-TKR surgery associated with repeat nonavian HMW-HA courses. One course of nonavian HMW-HA was defined as three injections within 6 months or, alternatively, the end of a 6-month period from the first injection.
Statistical analyses
p-values where calculated to evaluate baseline differences in patient characteristics. Kaplan–Meier curves were developed. The t-test and log-rank test were used independently to estimate the differences in mean and median times to TKR surgery for the two cohorts, respectively. Furthermore, the impact that the number of courses of nonavian HMW-HA injections had on mean and median times to TKR surgery were evaluated using a one-way analysis of variance (ANOVA) and log-rank test, respectively. Statistical significance was set at 0.05 (two sided). Finally, Cox regression models were used to evaluate the effect of nonavian HMW-HA injections (yes/no) and number of courses of nonavian HMW-HA injections on time to TKR surgery adjusting for baseline demographic (age, gender [reference – male], region [reference – west] and insurance type [reference – preferred provider organization]) and clinical characteristics (functional comorbidity score derived from 18 different comorbid conditions). Cox models were run separately for cohorts with and without continuous enrollment restrictions.
Results
Patient selection & demographics
Table 1 describes the process through which patients were selected for the study population. A total of 412,430 adult patients who had a TKR surgery between 1 January 2008 and 31 December 2017 were identified overall, 30,028 of which met the study inclusion criteria and were therefore included in the overall study population. There were 1978 patients in the nonavian HMW-HA cohort and 28,050 patients in the non-HA cohort.
| Inclusion and exclusion criteria | Excluded | Remaining |
|---|---|---|
| Include patients with a claim for TKR surgery in inpatient setting, between 1 January 2008–31 December 2017 = index TKR | 412,430 | |
| Exclude patients with TKR surgery in any setting prior to index TKR | 9468 | 402,962 |
| Exclude patients with no diagnosis of knee OA by orthopedic surgeon prior to index TKR | 84,718 | 318,244 |
| Exclude patients who had other knee OA diagnosis visits to an orthopedic surgeon during MCP period, prior to the initial diagnosis date of knee OA | 1 | 318,243 |
| Exclude patients with procedure for revision TKR (any setting) prior to and inclusive of index TKR | 30,859 | 287,384 |
| Exclude patients with no enrollment information | 68 | 287,384 |
| Exclude patients with noncontinuous enrollment in MCP + ‘baseline to index TKR’ period | 135,319 | 151,997 |
| Exclude patients who had any HA injection prior to initial diagnosis date of knee OA as far back as MCP start. | 8679 | 143,318 |
| Exclude patients with any HA injection on day of index TKR | 18 | 143,300 |
| Exclude patients with any HA (other than nonavian HMW-HA) injections from initial diagnosis date of knee OA to index TKR | 36,816 | 106,484 |
| Exclude patients that do not meet the MCE period of 7 years | 76,456 | 30,028 |
| – Nonavian HMW-HA cohort | 1978 | |
| – Non-HA cohort | 28,050 |
MCE = 7 years; MCP = 13 months.
HA: Hyaluronic acid; HMW-HA: High-concentration high-molecular weight hyaluronan; MCE: Minimum continuous enrollment; MCP: Minimum clean period; OA: Osteoarthritis; TKR: Total knee replacement.
Patient characteristics of the overall study population and patient cohort are presented in Table 2. Of the overall study population, 58.2% were women and 66.5% were aged 55–64 years old. The majority of patients were from the south (47.2%) and north central (29.8%) of the USA. Both cohorts were similar in baseline characteristics.
| Characteristics | All (n = 30,028) | Nonavian HMW-HA cohort (n = 1978) | Non-HA cohort (n = 28,050) | p-value |
|---|---|---|---|---|
| Gender, n (%) – Female – Male | 17,479 (58.2) 12,549 (41.8) | 1247 (63) 731 (37) | 16,232 (57.9) 11,818 (42.1) | <0.0001 |
| Age group, n (%) – 18–44 – 45–54 – 55–64 | 992 (3.3) 9078 (30.2) 19,958 (66.5) | 111 (5.6) 750 (37.9) 1117 (56.5) | 881 (3.1) 8328 (29.7) 18,841 (67.2) | <0.0001 |
| Region, n (%) – South – North central – Northeast – West – Unknown | 14,175 (47.2) 8938 (29.8) 2643 (8.8) 4222 (14.1) 50 (0.2) | 999 (50.5) 544 (27.5) 198 (10) 235 (11.9) 2 (0.1) | 13,176 (47) 8394 (29.9) 2445 (8.7) 3987 (14.2) 48 (0.2) | 0.0005 |
| Insurance plan type, n (%) – CDHP – Comprehensive – EPO – HDHP – HMO – POS – POS with capitation – PPO – Unknown | 2450 (8.2) 2663 (8.9) 167 (0.6) 527 (1.8) 3848 (12.8) 3530 (11.8) 240 (0.8) 16,395 (54.6) 208 (0.7) | 189 (9.6) 119 (6.0) 15 (0.8) 42 (2.1) 207 (10.5) 285 (14.4) 16 (0.8) 1096 (55.4) 9 (0.5) | 2261 (8.1) 2544 (9.1) 152 (0.5) 485 (1.7) 3641 (13.0) 3245 (11.6) 224 (0.8) 15,299 (54.5) 199 (0.7) | <0.0001 |
CDHP: Consumer-driven health plan; EPO: Exclusive provider organization; HA: Hyaluronic acid; HDHP: High-deductible health plan; HMO: Health maintenance organization; HMW-HA: High-concentration high-molecular-weight hyaluronan; POS: Point of service; PPO: Preferred provider organization.
A total of 18 different comorbid conditions were used to develop a functional comorbidity score, along with mean functional comorbidity score [14]. Patient comorbid conditions of the overall study population and patient cohorts by use of nonavian HMW-HA are presented in Table 3. Of the overall study population, the mean value for the Functional Comorbidity Index was 2.8 overall. The nonavian HMW-HA cohort index was 2.7 and the non-HA cohort was 2.8. The highest individual comorbidity was congestive heart failure or heart disease with 53.8% overall, 50.9% for nonavian HMW-HA cohort Index and 54.0% for the non-HA cohort.
| Characteristics | All (n = 30,028) | Nonavian HMW-HA cohort (n = 1978) | Non-HA cohort (n = 28,050) | p-value |
|---|---|---|---|---|
| Comorbidity, n (%) – Arthritis – Osteoporosis – Asthma – COPD/ARDS – Angina – CHF or heart disease – Heart attack – Neurological disease – Stroke or TIA – Diabetes – PVD – Upper gastrointestinal disease – Depression – Anxiety or panic disorders – Visual impairment – Hearing impairment – Degenerative disc disease – Obesity | 30,028 (100.0) 7630 (2.5) 1871 (6.2) 886 (3.0) 474 (1.6) 16,143 (53.8) 276 (0.9) 10,513 (35.0) 180 (0.6) 5549 (18.5) 399 (1.3) 4384 (14.6) 2501 (8.3) 1661 (5.5) 393 (1.3) 673 (2.2) 3315 (11.0) 3243 (0.1) | 1978 (100.0) 52 (2.6) 148 (7.5) 59 (3.0) 26 (1.3) 1006 (50.9) 15 (0.8) 735 (37.2) 4 (0.2) 306 (15.5) 22 (1.1) 298 (15.1) 171 (8.7) 110 (5.6) 36 (1.8) 39 (2.0) 239 (12.1) 181 (0.1) | 28,050 (100.0) 710 (2.5) 1725 (6.2) 827 (3.0) 446 (1.6) 15,136 (54.0) 261 (0.9) 9778 (34.9) 177 (0.6) 5245 (18.7) 376 (1.3) 4084 (14.6) 2331 (8.3) 1551 (5.5) 356 (1.3) 634 (2.3) 3077 (11.0) 3060 (0.1) | 0.789 0.0175 0.937 0.335 0.008 0.447 0.038 0.0172 0.0004 0.391 0.541 0.598 0.958 0.037 0.408 0.127 0.015 |
ARDS: Acute respiratory distress syndrome; CHF: Congestive heart failure; COPD: Chronic obstructive pulmonary disease; HMW-HA: High-concentration high-molecular weight hyaluronan; PVD: Peripheral vascular disease; TIA: Transient ischemic attack.
Time-to-TKR surgery
The median time-to-TKR surgery was 893 days for the nonavian HMW-HA cohort and 399 days for the non-HA, with a difference of 494 days (or 16.2 months; p < 0.001) between them (Figure 2). The mean time-to-TKR surgery was 1201 days (or 39.4 months) for the nonavian HMW-HA cohort, which differed from the timespan of 837 days (or 27.4 months) for the non-HA cohort by 364 days (12 months; p < 0.001).
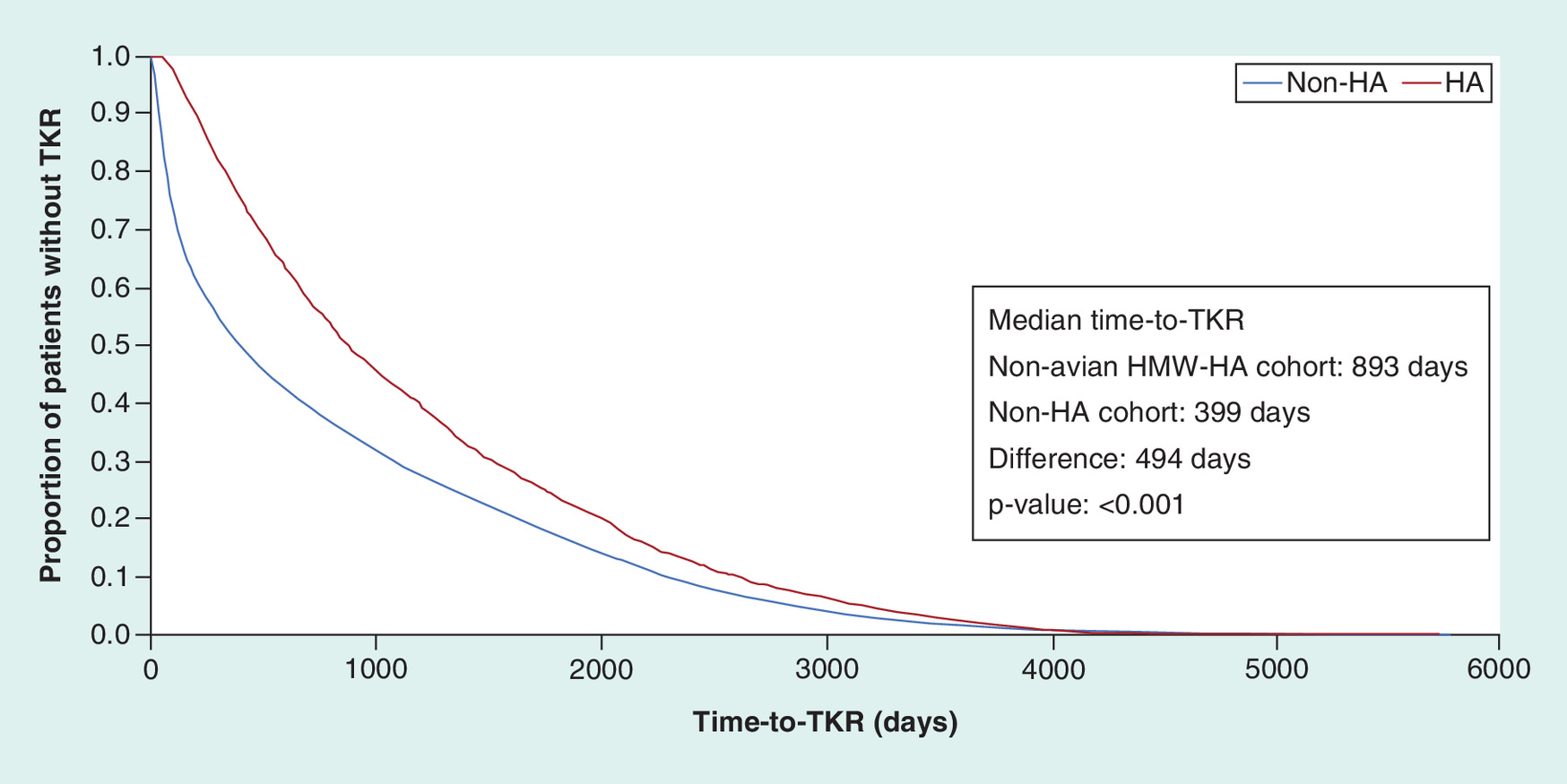
Figure 2. Median time-to-total knee replacement surgery for nonavian HMW-HA and nonhyaluronic acid cohort.
HA: Hyaluronic acid; HMW-HA: High-concentration high-molecular-weight hyaluronan; TKR: Total knee replacement.
Multiple courses of nonavian HMW-HA & time-to-TKR surgery
A total of 32.3% of the patients in the nonavian HMW-HA cohort had two or more courses during the evaluation period, with 20.8% having two courses, 5.7% having three courses and 5.8% having four or more courses of nonavian HMW-HA (Table 4).
| Nonavian HMW-HA courses, n | 1 (n = 1340) | (n = 411) | 3 (n = 113) | 4+ (n = 114) |
|---|---|---|---|---|
| Cohort (%) | 67.7% | 20.8% | 5.7% | 5.8% |
| Median time-to-TKR in days (IQR) | 773 (333–1644) | 995 (538–1914) | 1399 (859–2099) | 1612 (995–2359) |
| Mean time-to-TKR in days (SD) | 1090 (953) | 1295 (987) | 1613 (951) | 1763 (937) |
HMW-HA: High-concentration high-molecular weight hyaluronan; IQR: Interquartile range; SD: Standard deviation; TKR: Total knee replacement.
The median time-to-TKR increased with each additional course of nonavian HMW-HA, ranging from 773 days among patients with one course of nonavian HMW-HA to 1612 days among patients with 4+ nonavian HMW-HA courses (Table 2). The time-to-TKR stratified by number of courses of nonavian HMW-HA injections is presented in Figure 3.
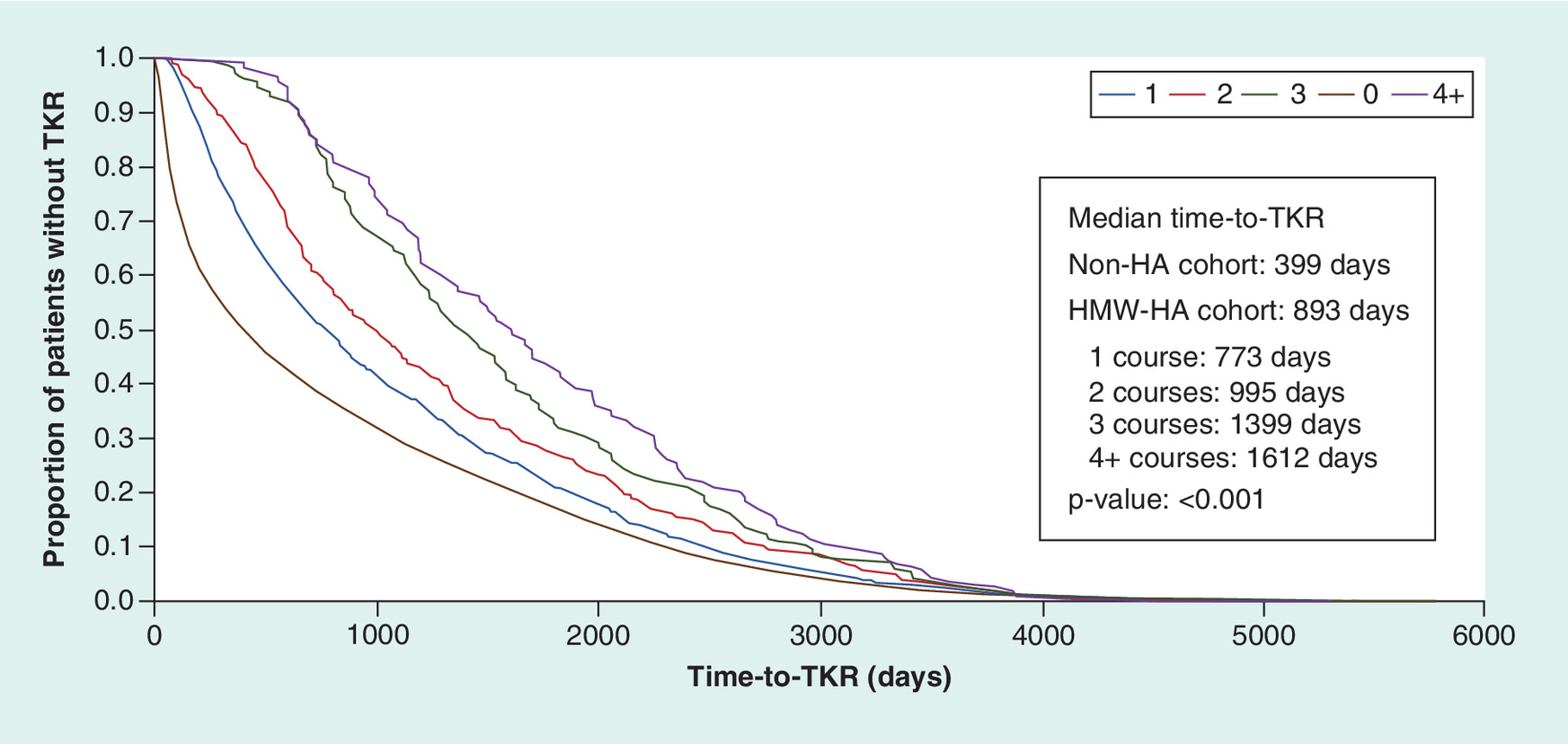
Figure 3. Time-to-total knee replacement surgery stratified by number of courses of nonavian HMW-HA Injections.
HA: Hyaluronic acid; HMW-HA: High-concentration high-molecular-weight hyaluronan; TKR: Total knee replacement.
These results show that treatment with an increasing number of courses of nonavian HMW-HA injections was associated with a stepwise increase in time-to-TKR surgery (p < 0.001).
Cox regression among patients with & without at least 7 years continuous enrollment
For patients with at least 7 years continuous enrollment, two multivariable Cox regression models adjusting for baseline demographic and clinical factors were conducted; one with any use of nonavian HMW-HA and the other evaluating the effect of number of courses for nonavian HMW-HA. Any use of nonavian HMW-HA model showed that the risk for TKR was 24.3% lower with receipt of nonavian HMW-HA as compared with no HA at any given time (Table 5). The model for number of courses for nonavian HMW-HA showed that the risk of TKR reduced as the courses of nonavian HMW-HA increased as compared with no HA: 18.2% lower risk with one course, 30.3% lower risk with two courses, 38.5% lower risk with three courses and 43.8% lower risk with four or more courses of nonavian HMW-HA (Table 6).
| Parameter | Hazard ratio | 95% hazard ratio confidence limits | p-value | |
|---|---|---|---|---|
| Age | 1.127 | 1.124 | 1.131 | <0.0001 |
| FCI | 1.086 | 1.078 | 1.095 | <0.0001 |
| Female vs male | 0.970 | 0.948 | 0.992 | 0.009 |
| North central vs west | 1.014 | 0.976 | 1.053 | 0.482 |
| Northeast vs west | 0.907 | 0.862 | 0.953 | 0.0001 |
| South vs west | 0.905 | 0.874 | 0.938 | <0.0001 |
| Unknown vs west | 0.771 | 0.583 | 1.019 | 0.068 |
| CDHP vs PPO | 1.507 | 1.443 | 1.573 | <0.0001 |
| Comprehensive vs PPO | 0.911 | 0.873 | 0.950 | <0.0001 |
| EPO vs PPO | 0.890 | 0.763 | 1.038 | 0.138 |
| HDHP vs PPO | 1.575 | 1.444 | 1.718 | <0.0001 |
| HMO vs PPO | 0.909 | 0.877 | 0.943 | <0.0001 |
| POS vs PPO | 0.873 | 0.841 | 0.906 | <0.0001 |
| POS with capitation vs PPO | 0.620 | 0.545 | 0.705 | <0.0001 |
| Unknown vs PPO | 0.826 | 0.720 | 0.947 | 0.0063 |
| Nonavian HMW-HA vs no HA† | 0.757 | 0.723 | 0.792 | <0.0001 |
†
Main variable of interest.
CDHP: Consumer-driven health plan; EPO: Exclusive provider organization; FCI: Functional comorbidity index; HA: Hyaluronic acid; HDHP: High-deductible health plan; HMO: Health maintenance organization; HMW-HA: High-concentration high-molecular weight hyaluronan; POS: Point of service; PPO: Preferred provider organization.
| Parameter | Hazard ratio | 95% hazard ratio confidence limits | p-value | |
|---|---|---|---|---|
| Age | 1.127 | 1.124 | 1.131 | <0.0001 |
| FCI | 1.087 | 1.078 | 1.095 | <0.0001 |
| Female vs male | 0.970 | 0.948 | 0.993 | 0.0104 |
| North central vs west | 1.016 | 0.978 | 1.055 | 0.4202 |
| Northeast vs west | 0.908 | 0.864 | 0.955 | 0.0002 |
| South vs west | 0.906 | 0.875 | 0.939 | <.0001 |
| Unknown vs west | 0.771 | 0.583 | 1.019 | 0.0673 |
| CDHP vs PPO | 1.507 | 1.443 | 1.573 | <0.0001 |
| Comprehensive vs PPO | 0.910 | 0.873 | 0.949 | <0.0001 |
| EPO vs PPO | 0.889 | 0.762 | 1.037 | 0.1347 |
| HDHP vs PPO | 1.571 | 1.440 | 1.713 | <0.0001 |
| HMO vs PPO | 0.910 | 0.877 | 0.943 | <0.0001 |
| POS vs PPO | 0.873 | 0.841 | 0.906 | <0.0001 |
| POS with capitation vs PPO | 0.620 | 0.545 | 0.706 | <0.0001 |
| Unknown vs PPO | 0.825 | 0.720 | 0.947 | 0.0061 |
| 1 course of HMW-HA vs no HA† | 0.818 | 0.774 | 0.864 | <0.0001 |
| 2 courses of HMW-HA vs no HA† | 0.697 | 0.632 | 0.769 | <0.0001 |
| 3 courses of HMW-HA vs no HA† | 0.615 | 0.511 | 0.740 | <0.0001 |
| 4+ courses of HMW-HA vs no HA† | 0.562 | 0.467 | 0.675 | <0.0001 |
†
Main variable of interest.
CDHP: Consumer-driven health plan; EPO: Exclusive provider organization; FCI: Functional comorbidity index; HA: Hyaluronic acid; HDHP: High-deductible health plan; HMO: Health maintenance organization; HMW-HA: High-concentration high-molecular weight hyaluronan; POS: Point of service; PPO: Preferred provider organization.
For patients with no continuous enrollment restriction, similar results were obtained from the multivariable cox regression models. Any use of nonavian HMW-HA model showed that the risk for TKR was 39.1% lower with receipt of nonavian HMW-HA as compared with no HA at any given time. Additionally, the risk of TKR reduced as the courses of nonavian HMW-HA increased as compared with no HA: 34.3% lower risk with one course, 44.8% lower risk with two courses, 56.2% lower risk with three courses and 59.6% lower risk with four or more courses of nonavian HMW-HA.
Discussion
The results of this retrospective analysis of a healthcare claims database demonstrates that the time from the initial diagnosis of knee osteoarthritis by an orthopedic surgeon to TKR surgery is 16.2 months longer in patients who received treatment with nonavian HMW-HA injections versus patients who did not receive HA injections. Additionally, among knee osteoarthritis patients who received nonavian HMW-HA injections, the time to TKR is longer with each additional course of treatment.
The ability to postpone or potentially avoid TKR may be advantageous for patients who do not prefer immediate surgical interventions due to personal reasons and it allows the patient a chance to reduce risks by weight loss and strength building. It also potentially avoids the risk associated with TKR, such as patellar fracture, implant loosening, vascular injury, etc. and future revision surgery (especially in younger populations) [15–17]. Persistent pain following TKR surgery is a prevalent but under-acknowledged condition with approximately 15% of TKR recipients experiencing persistent pain for up to 4 years after surgery [17]. Additionally, of the 4 million adults in the USA currently living with a TKR, it is estimated that more than 500,000 (about 12%) have undergone revision of their primary TKR [16]. The annual rates of revision are higher among younger TKR recipients due to the higher levels of physical activity in this population after surgery and the subsequent wear and tear on the knee implant [18,19]. There are other patients for whom surgery may not be medically appropriate due to conditions such as heart disease, diabetes, obesity or generalized medical debilitation who may prefer other therapeutic options for treating their knee OA while they manage their comorbidities [15,20].
The findings from the present analysis are generally consistent with other recently published retrospective database and chart review studies evaluating the impact of HAs on the time-to-TKR in the real-world setting [5,6,12,13,21–24]. One prospective study by Turajane and colleagues examined the impact of repeat injections of HA on time to TKR in 183 patients with knee OA over a 54 month follow-up period and reported a mean time to TKR of 15.4 months following HA injections [22].
Strengths & limitations
Strengths of the present study were the large cohort size (n = 30,028), long time horizon (7 years minimum continuous enrollment), the use of real-world patient care data, the multiple institutions and physician practice patterns represented andthe varying geographic locations of patients in the study sample. Another strength included, this study was limited to a single nonavian HMW-HA, which would reduce HA differentiation bias. Additionally, this study used multivariable regression approach to adjust for the baseline differences between the patients receiving nonavian HMW-HA and no HA. The regressions showed similar results with and without 7 years continuous enrollment criteria showing the robustness of the results. the This study was subject to a number of important limitations. First, information potentially impacting study results, including measures of disease severity baseline pain scores or patient willingness in both nonavian HMW-HA injection status cohorts were not available in the claims database. Second, the date of diagnosis by an orthopedic surgeon may not be an accurate reflection of the onset of disease. Furthermore, baseline diagnoses may not necessarily represent the first diagnosis of knee OA. Third, the study population was limited to patients under the age of 65 years, reflecting the patient population included in the database. Therefore, these results may not necessarily be applicable to an elderly population. However, this study is from private payor perspective and thereby Medicare was not analyzed as part of the measured cohort. Fourth, therapy with nonavian HMW-HA injections may have occurred outside of the population included in the claims database or prior to the MCP, excluding such patients from this study. Fifth, medium and small firms were not represented in this study as MarketScan data is primarily supplied by large employers, despite the size of this data source. Sixth, certain plan-specific policies may restrict the usage of nonavian HMW-HA or require patients to try specific therapies prior to undergoing TKR surgery. Due to the inability to identify specific health insurance plans in the claims database, it was not possible to account for such policies. Seventh, the database does not provide information on delays in getting an appointment with an orthopedic surgeon and getting into the operating room. However, this time bias would have affected both the nonavian HMW-HA cohort and non-HA cohort equally. Eighth, no causal inferences can be drawn as this is an observational study and lacks randomization that may cause systematic differences between the groups compared. Finally, as with most retrospective claims analyses, it may be possible that some knee OA diagnoses and nonavian HMW-HA treatments were miscoded. Most of these limitations are inherent to claims database analysis and do not preclude the development of clinically relevant conclusions about the real-world impact of HAs such as nonavian HMW-HA on time-to-TKR in patients with knee OA.
Conclusion
This retrospective study provides real-world insights into the time-to-TKR surgery and a single-sourced, nonavian HMW-HA injection among knee OA patient. The results indicated that the time from initial diagnosis of knee OA to the date of TKR surgery for patients treated with nonavian HMW-HA injections was a median of 16.2 months longer than in patients who did not receive nonavian HMW-HA injections. The findings further indicate that the time-to-TKR was longer with each additional course of nonavian HMW-HA treatment.
•
The primary objective of this study was to examine the time-to-total knee replacement (TKR) surgery of patients who had high-concentration, nonavian, high-molecular-weight hyaluronan injection (HMW-HA) courses prior to TKR surgery with those who did not receive hyaluronic acid (HA) injections.
•
The secondary objective of this study was to examine the relationship between number of nonavian HMW-HA courses and time-to-TKR.
•
A retrospective analysis of the IBM MarketScan Commercial claims database was performed.
•
A total of 30,028 patients who received TKR surgery between 2008 and 2017 were divided into a nonavian HMW-HA cohort (n = 1978) and a non-HA cohort (n = 28,050).
•
The median time-to-TKR surgery was 893 days in the nonavian HMW-HA cohort and 399 days in the non-HA cohort (p < 0.001) for a difference of 494 days.
•
Patients in the nonavian HMW-HA cohort who received 1, 2, 3 or 4+ courses of treatment had median times-to-TKR of 773 days, 995 days, 1399 days and 1612 days, respectively.
•
The time from the diagnosis of knee osteoarthritis to TKR surgery was demonstrated to be 16.2 months longer in patients who received treatment with nonavian HMW-HA injections compared with patients who did not receive HA injections.
•
The time-to-TKR is longer with each additional course of treatment among knee osteoarthritis patients who received nonavian HMW-HA injections.
Author contributions
Concept and design were performed by AS Chitnis, K Etter, CE Holy and SK Bhattacharyya; acquisition of data was performed by AS Chitnis and K Etter; analysis and interpretation of data were performed by AS Chitnis, K Etter, CE Holy, SK Bhattacharyya, FS Gray, FJ Manalac and B Bisson; drafting of the manuscript was performed by AS Chitnis, K Etter, CE Holy and SK Bhattacharyya; critical revision of the manuscript for important intellectual content was performed by AS Chitnis, K Etter, CE Holy, SK Bhattacharyya, FS Gray, FJ Manalac and B Bisson; statistical analysis was performed by AS Chitnis and K Etter. SK Bhattacharyya obtained the funding. Supervision was done by CE Holy, B Bisson and SK Bhattacharyya.
Acknowledgments
The abstract of this paper was presented at the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Europe 2018 conference as a poster presentation with interim findings. The poster’s abstract was published in the journal Value in Health, Volume 21, Page S300: https://doi.org/10.1016/j.jval.2018.09.1786
Financial & competing interests disclosure
Support for this research was provided by DePuy Synthes, Raynham, MA, USA. K Etter, AS Chitnis, CE Holy, B Bisson and SK Bhattacharyya are employees and stockholders of Johnson & Johnson. FJ Manalac and FS Gray presented on Orthovisc/Monovisc and were compensated by Johnson & Johnson. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open Access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Arthritis Foundation. Arthritis by the Numbers: Book of Trusted Facts and Figures. (2017).
2.
Deshpande BR, Katz JN, Solomon DH et al. Number of persons with symptomatic knee osteoarthritis in the US: impact of race and ethnicity, age, sex andobesity. Arthritis Care Res. 68(12), 1743–1750 (2016).
3.
McIntyre LF, Bhattacharyya S, Yadalam S, Bisson B. Impact of hyaluronic acid injections on utilization of pain management medications. Am. J. Pharm. Benefits 9(6), 195–199 (2017).
4.
Agency for Healthcare Research and Quality & Nationwide Inpatient Sample (NIS). Costs for year 2014 using ICD-9 procedure codes 81.54 (total knee replacement). (2017). https://www.hcup-us.ahrq.gov/nisoverview.jsp
5.
Altman R, Fredericson M, Bhattacharyya SK et al. Association between hyaluronic acid injections and time-to-total knee replacement surgery. J. Knee Surg. 29(7), 564–570 (2016).
•• Assesses the association between hyaluronic acid (HA) injections and time-to-total knee replacement (TKR) surgery for patients with knee osteoarthritis (OA) who had TKR surgery between 1 January 2006 and 31 December 2011.
6.
Dasa V, Dekoven M, Sun K, Scott A, Lim S. Clinical and cost outcomes from different hyaluronic acid treatments in patients with knee osteoarthritis: evidence from a US health plan claims database. Drugs Context 5, 212296 (2016).
• Compares disease-specific costs and risk of TKR among patients receiving different HA treatments in a commercially insured cohort of patients with knee OA in the USA.
7.
Fibel KH, Hillstrom HJ, Halpern BC. State-of-the-art management of knee osteoarthritis. World J. Clin. Cases 3(2), 89–101 (2015).
8.
Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Joint Surg. Am. 89(4), 780–785 (2007).
9.
Losina E, Weinstein AM, Reichmann WM et al. Lifetime risk and age at diagnosis of symptomatic knee osteoarthritis in the US. Arth. Care Res. 65(5), 703–711 (2013).
10.
Hochberg MC, Altman RD, April KT et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip andknee. Arth. Care Res. 64(4), 465–474 (2012).
11.
ORTHOVISC® (high molecular weight hyaluronan), prescribing information. DePuy Synthes, MA. U.S.A, (2005).
12.
Altman R, Lim S, Steen RG, Dasa V. Hyaluronic acid injections are associated with delay of total knee replacement surgery in patients with knee osteoarthritis: evidence from a large U.S. health claims database. PLoS ONE 10(12), e0145776 (2015).
•• Evaluates records in an administrative claims database of approximately 79 million patients to identify all patients with knee OA who received TKR during a 6-year period and test a hypothesis that HA injection is associated with delay of TKR in a dose-dependent manner.
13.
Delbarre A, Amor B, Bardoulat I, Tetafort A, Pelletier-Fleury N. Do intra-articular hyaluronic acid injections delay total knee replacement in patients with osteoarthritis – a Cox model analysis. PLoS ONE 12(11), e0187227 (2017).
•• Aims to describe patients treated for knee osteoarthritis between 2006 and 2013 in France and to compare the delay from diagnosis to total knee replacement between patients who received intra-articular HA injections and those who did not receive the injections.
14.
Groll DL, To T, Bombardier C, Wright JG. The development of a comorbidity index with physical function as the outcome. J. Clin. Epidemiol. 58(6), 595–602 (2005).
15.
Waddell DD, Bricker DC. Total knee replacement delayed with Hylan G-F 20 use in patients with grade IV osteoarthritis. J. Manag. Care Pharm. 13(2), 113–121 (2007).
• Aims to determine the effect of hylan G-F 20 on patient need for TKR as measured by time from hylan G-F 20 injection to TKR and assess patient factors that might influence time from hylan G-F 20 therapy to TKR
16.
Weinstein AM, Rome BN, Reichmann WM et al. Estimating the burden of total knee replacement in the United States. J. Bone Joint Surg. Am. 95(5), 385–392 (2013).
17.
Wylde V, Hewlett S, Learmonth ID, Dieppe P. Persistent pain after joint replacement: prevalence, sensory qualities andpostoperative determinants. Pain 152(3), 566–572 (2011).
18.
Julin J, Jamsen E, Puolakka T, Konttinen YT, Moilanen T. Younger age increases the risk of early prosthesis failure following primary total knee replacement for osteoarthritis. A follow-up study of 32,019 total knee replacements in the Finnish Arthroplasty Register. Acta Orthopaed. 81(4), 413–419 (2010).
19.
Paxton EW, Namba RS, Maletis GB et al. A prospective study of 80,000 total joint and 5000 anterior cruciate ligament reconstruction procedures in a community-based registry in the United States. J. Bone Joint Surg. Am. 92(Suppl. 2), 117–132 (2010).
20.
Arnold W, Fullerton DS, Holder S, May CS. Viscosupplementation: managed care issues for osteoarthritis of the knee. J. Manag. Care Pharm. 13(Suppl. 4), S3–S19; quiz: S20-S12 (2007).
21.
Shewale AR, Barnes CL, Fischbach LA, Ounpraseuth ST, Painter JT, Martin BC. Comparison of low-, moderate- andhigh-molecular-weight hyaluronic acid injections in delaying time to knee surgery. J. Arthroplasty 32(10), 2952–2957.e2921 (2017).
22.
Turajane T, Amphansap T, Labpiboonpong V, Maungsiri S. Total knee replacement following repeated cycles of intra-articular sodium hyaluronate (500–730 Kda) in failed conservative treatment of knee osteoarthritis: a 54-month follow-up. J. Med. Assoc. Thai. 92(Suppl. 6), S63–S68 (2009).
• Evaluates the incidence of TKR in patients receiving repeated cycles of intra-articular HA during a 54-month follow-up period.
23.
Waddell DD, Joseph B. Delayed total knee replacement with hylan G-F 20. J. Knee Surg. 29(2), 159–168 (2016).
• Examines prospective data on the incidence and time to TKR in patients with grade IV OA treated with hylan G-F 20 from 1997 to 2010 and a patient subset treated from 1997 to 2003 to determine any continued hylan G-F 20 influence on TKR delay.
24.
Whitman C, Allen D, Comadoll JL, Thomason HC, Oweida SJ. A retrospective study of Supartz and repeat treatment for osteoarthritis pain in the knee. J. Manag. Care Med. 13(1), 43–47 (2010).
Information & Authors
Information
Published In
Pages: 795 - 805
PubMed: 32643955
Copyright
© 2020 Abhishek Chitnis. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 22 August 2019
Accepted: 6 June 2020
Published online: 9 July 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
High-concentration nonavian high-molecular weight hyaluronan injections and time-to-total knee replacement surgery. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0128
Export citation
Select the citation format you wish to export for this article or chapter.