Costs, exacerbations and pneumonia after initiating combination tiotropium olodaterol versus triple therapy for chronic obstructive pulmonary disease
This article has been corrected.
VIEW CORRECTIONPublication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare health plan-paid costs, exacerbations and pneumonia outcomes for patients with chronic obstructive pulmonary disease (COPD) initiating combination tiotropium olodaterol (TIO + OLO) versus triple therapy (TT: long-acting muscarinic antagonist + long-acting β2 agonists + inhaled corticosteroid). Patients & methods: COPD patients initiating TIO + OLO or TT between 1 January 2014 and 30 June 2016 were identified from a managed care Medicare database and balanced for baseline characteristics using inverse probability of treatment weighting before assessment of outcomes. Results: Annual COPD-related and all-cause costs were US$4118 (35%) and US$5384 (23%) lower for TIO + OLO versus TT (both p ≤ 0.001). TIO + OLO patients had nearly half the severe exacerbations (8.3 vs 15.5%; p = 0.014) and pneumonia was also less common (18.9 vs 30.9%; p < 0.001). Conclusion: TIO + OLO was associated with improved economic and COPD health outcomes versus TT.
Chronic obstructive pulmonary disease (COPD) affects approximately 24 million adults in USA and is a leading cause of disability and mortality [1–4]. The economic burden is also substantial; the direct medical costs of managing COPD are projected to reach US$49 billion by 2020 [5]. The disease is characterized by chronic airflow limitation, commonly manifesting as shortness of breath, coughing and/or sputum production [6]. COPD exacerbations represent an acute worsening of symptoms that require treatment, ranging from outpatient care to hospitalization, and are the major driver of COPD-related healthcare costs [7–9]. The 2018 Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations provide first and second line pharmacologic treatment algorithms for patients with COPD, grouping them according to their severity, as measured by their exacerbation risk and symptom burden [6]. Groups A and B are characterized by low risk of exacerbation while Groups C and D are at high exacerbation risk [6]. Symptom burden differentiates Group A and C (low) and Groups B and D (high). Accordingly, Group A is the least severe (low exacerbation risk/symptom burden) while Group D represents the most severe (high exacerbation risk/symptom burden).
Inhaled long-acting bronchodilators, namely long-acting muscarinic antagonists (LAMAs) and long-acting β2 agonists (LABAs), are the mainstays of maintenance therapy for patients in Groups B–D [6]. When treatment with a LAMA or LABA, as monotherapy, does not achieve adequate symptom control [10], and symptoms or exacerbations persist, escalation from monotherapy to LAMA + LABA is the preferred treatment pathway for patients in Groups B and C, although escalation to LABA + inhaled corticosteroids (ICS) may also be considered for patients in Group C [6]. Triple therapy (TT; LAMA + LABA + ICS) is recommended only for the most severe patients: those in Group D who experience further exacerbations after escalation to dual therapy [6]. Although the 2018 GOLD recommendations reserved ICS-containing regimens for a select group of patients in Groups C and D, use of these regimens among patients in Groups A and B is reportedly widespread in clinical practice [11–14]. TT specifically has been widely reported among patients with mild or moderate disease [15–20]. However, ICS-containing regimens, including TT, require a risk–benefit assessment given the risk of pneumonia and other potential long-term complications (cataracts, diabetes progression and osteoporosis) associated with regular use of ICS [6,21–25], which in turn results in higher symptom burden, healthcare resource use (HCRU) and costs. Use of ICS-containing regimens early in the patient journey may not only unnecessarily expose patients to an elevated risk of these complications but has also been shown to accelerate the pathway to TT [16].
Overuse of TT has been well documented [15–20]. However, there has been limited comparison of economic and COPD health outcomes for TT versus other therapies, particularly LAMA + LABA, in a real-world setting. Researchers in Germany found that patients treated with LAMA + LABA in primary and secondary care experienced exacerbations at roughly half the rate of their counterparts on TT [26]. Two recent claims-based studies in USA compared tiotropium olodaterol (TIO + OLO) [27,28] – a fixed-dose combination of LAMA (TIO) plus LABA (OLO) in a single inhaler – with TT and found that patients initiating TIO + OLO incurred 27–53% lower COPD-related costs than patients initiating TT in the first year of therapy [29,30]. Besides being conducted in populations with mixed forms of insurance, both these studies employed traditional regression modeling methods to evaluate these treatments. These methodological limitations therefore necessitate additional research to corroborate their findings. Further still, no study to date has accounted for the impact of pneumonia burden. Therefore, the primary objective of this study was to compare HCRU, associated costs (all-cause, COPD-related and non-COPD pneumonia-related), as well as incident COPD exacerbations and occurrences of pneumonia among patients initiating TIO + OLO versus TT in a real-world setting. A secondary analysis compared patients initiating any LAMA + LABA regimen (including TIO + OLO) with TT for the same outcomes. Since Medicare is the primary payer for COPD-related costs in USA [31–33], this study was conducted among a population of managed Medicare beneficiaries with prescription drug coverage, who were diagnosed with COPD.
Methods
Design & data source
This retrospective, observational study used an administrative claims database from the Optum Research Database (ORD). The ORD contains enrollment information and administrative claims for all medical and pharmacy services submitted to each patient’s health plan(s) for reimbursement. Medical claims include International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis and procedure codes and site of service codes. Pharmacy claims include National Drug Codes for medications dispensed with quantity, dose and days’ supply. The ORD is geographically diverse in coverage and represented approximately 17% (∼3.2 million individuals) of the US population with Medicare Advantage with Part D prescription drug coverage (MAPD) benefits in 2016.
No identifiable protected health information was extracted or accessed during the course of the study. All data were accessed in compliance with the Health Insurance Portability and Accountability Act’s rules so Institutional Review Board approval or waiver of authorization was not required.
Patient selection & cohort assignment
The initial population comprised patients diagnosed with COPD as confirmed by the presence of ICD-9-CM (491.xx, 492.xx, 493.2x and 496.xx) and/or ICD-10-CM (J41-J44) codes on ≥2 medical claims on separate dates of service between 1 January 2013 and 30 June 2017 (study period). The first observed long-acting bronchodilator-containing regimen (LAMA, LABA + ICS, LAMA + LABA or TT) with ≥30 consecutive days of therapy between 1 January 2014 and 30 June 2016 (identification period) was defined as the index regimen. The start date of the regimen was set as the index date. For example, for patients initiating TIO + OLO, the index date was the first pharmacy claim for TIO + OLO. For regimens comprised of multiple inhalers, the index date was the fill date for the pharmacy claim commencing ≥30 consecutive days of concurrent therapy for all medications in the regimen. Patients were excluded if they were <40 years on their index date, had incomplete demographic information or had ≥2 medical claims on separate dates of service with a diagnosis of asthma, lung cancer or cystic fibrosis during the study period (Supplementary Table 1 for diagnostic codes). All remaining patients were required to have continuous medical and pharmacy enrollment in a MAPD health plan during the 12-month pre-index (baseline) and 12-month postindex (follow-up) periods; this criterion ensured that all patients had full data for both the 12-month baseline and follow-up periods. The sample was limited to patients who were naive to the index regimen as of the index date. Patients initiating treatment with TIO + OLO or TT, the main therapies of interest, were retained as the final study population for the primary analysis and all other regimens (i.e., LAMA, LABA + ICS and LAMA + LABA other than TIO + OLO) were excluded. The secondary analysis retained the TT cohort and patients initiating any LAMA + LABA regimen (free or fixed-dose combinations, including TIO + OLO). This study used an intent-to-treat approach, with all outcomes during follow-up attributed to the index regimen.
Measures
Patient characteristics
Demographic and clinical characteristics were determined during the baseline period. Comorbidity burden was determined by the Quan–Charlson Comorbidity Index score [34] and the Elixhauser score [35]. Baseline COPD medication use was captured along with any occurrence of severe or moderate COPD exacerbations. Severe exacerbations were defined as an inpatient admission with a COPD diagnosis code in the primary position. Moderate exacerbations were defined as either an emergency department (ED) visit with a COPD diagnosis in the primary position, or an office visit with a COPD diagnosis code in any position plus a pharmacy claim for an oral corticosteroid or COPD-guideline recommended antibiotic prescription within 7 days of the ED or office visit. Exacerbations occurring within 14 days of each other were considered a single exacerbation episode and classified according to the highest severity contributing event.
Outcomes
HCRU and costs were assessed during the follow-up period and further stratified by setting, in other words, acute inpatient stays, ED visits, ambulatory (office and outpatient) visits and other services (e.g., durable medical equipment, home health visits, independent laboratory tests, long-term care). All-cause resource use included all claims for medical services and all-cause total costs were the sum of all medical costs plus outpatient pharmacy costs. COPD-related resource use was defined as medical claims with a diagnosis of COPD in any position and COPD-related total costs comprised COPD-related medical costs and outpatient pharmacy claims for COPD medications. COPD-attributable resource use was defined as medical claims with a diagnosis of COPD in the primary position on the claim and their corresponding costs together with outpatient COPD pharmacy claims were considered as COPD-attributable costs. Similarly, pneumonia-related resource use included medical claims with a diagnosis code for pneumonia and/or acute bronchitis/bronchiolitis in any position (codes shown in Supplementary Table 1). Since it was possible for COPD and pneumonia/acute bronchitis/bronchiolitis diagnoses to occur on the same claim, non-COPD pneumonia-related costs, in other words, pneumonia-related claims without a concurrent COPD diagnosis on the same claim, were computed. COPD/pneumonia total costs were then calculated by summing total COPD-related costs and the non-COPD pneumonia-related medical costs. All costs measures were computed from a payer perspective and defined as health-plan paid costs, with inflation adjustment to 2017 US dollars [36]. Additional outcomes including occurrence and time to exacerbations (as defined above) and pneumonia diagnosis were assessed starting on the day after the index date.
Statistical analysis
Prior to assessing the outcomes between the TIO + OLO versus TT (primary) and LAMA + LABA versus TT (secondary) cohorts, the cohorts were balanced using inverse probability of treatment weighting (IPTW). IPTW is an established method to minimize or eliminate potential confounding factors in observational studies before assessment of treatment effect [37]. Given the large number of clinically relevant patient baseline characteristics that could potentially influence outcomes, an iterative process was used to identify the logistic regression model that provided the best balance in characteristics (i.e., model covariates) between cohorts. For each potential model, the propensity score (PS) – the conditional probability that the patient would receive TIO + OLO (or LAMA + LABA) treatment, given the observed covariates (defined below) – for each patient was estimated. The weights were computed as the inverse of the conditional probability that the patient would receive the treatment they actually received (i.e., for the TIO + OLO cohort, 1/PS and for the TT cohort, 1/([1-PS]). The distribution of these scores was reviewed to assess the amount of overlap between cohorts, and patients with extreme weights (i.e. >10) [38]) were removed. Several candidate models were evaluated by adding/removing covariates until a model that provided the best balance between cohorts across the maximum number of covariates was identified. Balance was assessed postweighting by examining standardized differences between cohorts for each covariate. Standardized differences of less than 20% were considered adequate [39]. The weights were then normalized within each cohort to sum to the total sample size for the cohort.
Covariates selected for the final IPTW model included health plan type, US census region, index regimen prescriber specialty and baseline characteristics including pneumonia and/or acute bronchitis/bronchiolitis diagnosis, severe COPD exacerbation, COPD medication use, resource use and COPD-related medical cost quartiles. Cohort differences in unweighted baseline characteristics were analyzed by Pearson χ2 test (categorical variables) and two-sample t-test (continuous measures); when comparing cohorts after weighting, statistical testing was done using a Z-test with robust standard errors. The weighted difference in time to first COPD (any, severe) exacerbation was estimated by the Kaplan–Meier method and analyzed by the log-rank test. Weighted COPD-related and weighted all-cause cost outcomes were modeled using Manning and Mullahy’s formulation [40], using a generalized linear model with a γ-distribution and log link and adjusted for any residual imbalances between cohorts. Covariates selected for inclusion in the cost models were based on clinical relevance with an emphasis on characteristics with a standardized difference ≥10% after weighting. Separate models were constructed for total costs, medical costs and pharmacy costs. After adjustment, predicted costs were computed for each cohort using recycled predictions [41]. A secondary analysis was also conducted to compare LAMA + LABA and TT cohorts using the same primary analysis methodology.
Results
Patient identification & baseline characteristics
Among 844,551 patients diagnosed with COPD during the study period, 179,790 were ≥40 years of age and initiating a long-acting bronchodilator-containing regimen during the identification period (Figure 1). Of these patients, 3580 met all remaining inclusion criteria and were assigned to the TIO + OLO (n = 348) or TT (n = 3232) cohort. After examination of the PS distribution between study cohorts, one patient in the TIO + OLO cohort with an extreme weight was removed, leaving 347 patients in the final TIO + OLO cohort.

Figure 1. Patient selection and study cohorts.
†LAMA, LABA + ICS, LAMA + LABA or TT.
‡The first long-acting bronchodilator-containing regimen during the identification period with ≥30 consecutive days of therapy was considered the index regimen.
§≥2 medical claims for any of these conditions during 1 January 2013 to 30 June 2017.
COPD: Chronic obstructive pulmonary disease; ICS: Inhaled corticosteroid; LABA: Long-acting β2 agonist; LAMA: Long-acting muscarinic antagonist; TIO + OLO: Tiotropium olodaterol; TT: Triple therapy.
Baseline demographic and clinical characteristics before and after IPTW are shown in Table 1. Prior to IPTW, the TIO + OLO cohort was similar to the TT cohort with respect to mean age (72.6 vs 72.2 years), the proportion of men (52.9 vs 48.8%) and mean Quan–Charlson Comorbidity Index score (2.1 vs 2.3). However, there were differences in other characteristics between cohorts including a smaller percentage of TIO + OLO patients with severe exacerbations (5.5 vs 23.9%), pneumonia (13.5 vs 24.4%), controller and rescue medication usage and a larger proportion of maintenance naive patients prior to index (80.2 vs 55.0%). After IPTW, the standardized mean difference for nearly all baseline characteristics was below 20%, a cutoff considered to represent small imbalances [39]. Only four baseline characteristics had standardized mean differences that were marginally higher than 20% (21.09–22.89%) after IPTW.
| Characteristic | Before IPTW | After IPTW | ||||||
|---|---|---|---|---|---|---|---|---|
| TIO + OLO (n = 348) | TT (n = 3232) | STD DIFF % | p-value | TIO + OLO (n = 347) | TT (n = 3232) | STD DIFF % | p-value | |
| Age, years, mean (SD)‡ | 72.6 (8.6) | 72.2 (8.4) | −4.10 | 0.463 | 72.5 (8.4) | 72.2 (8.4) | −4.61 | 0.549 |
| Age group, years, n (%) | ||||||||
| − 40–64 | 56 (16.1) | 498 (15.4) | -1.88 | 0.738 | 59 (17.1) | 506 (15.6) | -3.90 | 0.637 |
| − 65–74 | 146 (42.0) | 1486 (46.0) | 8.11 | 0.152 | 145 (41.8) | 1488 (46.0) | 8.55 | 0.299 |
| − ≥75 | 146 (42.0) | 1248 (38.6) | -6.81 | 0.225 | 143 (41.3) | 1239 (38.3) | -5.72 | 0.485 |
| Male, n (%) | 184 (52.9) | 1577 (48.8) | -8.17 | 0.148 | 180 (52.0) | 1593 (49.3) | -5.41 | 0.510 |
| US Census region, n (%) | ||||||||
| − Northeast | 60 (17.2) | 733 (22.7) | 13.64 | 0.020 | 68 (19.5) | 716 (22.1) | 6.50 | 0.427 |
| − Midwest | 85 (24.4) | 1,022 (31.0) | 14.73 | 0.011 | 101 (29.0) | 981 (30.3) | 2.95 | 0.731 |
| − South | 184 (52.9) | 1221 (37.8) | -30.68 | <0.001 | 145 (41.7) | 1270 (39.3) | -4.95 | 0.534 |
| − West | 19 (5.5) | 276 (8.5) | 12.09 | 0.047 | 34 (9.8) | 266 (8.2) | -5.43 | 0.582 |
| Quan–Charlson comorbidity Index score, mean (SD) | 2.1 (1.7) | 2.3 (1.7) | 8.41 | 0.141 | 2.2 (1.6) | 2.3 (1.7) | 4.88 | 0.500 |
| Quan–Charlson Comorbidity Index score categories, n (%) | ||||||||
| − 0–1 | 173 (49.7) | 1600 (49.5) | -0.42 | 0.941 | 170 (48.9) | 1681 (50.1) | 2.30 | 0.780 |
| − 2–3 | 118 (33.9) | 981(30.4) | -7.62 | 0.172 | 118 (34.0) | 973 (30.1) | -8.32 | 0.306 |
| − 4–5 | 39 (11.2) | 510 (15.8) | 13.41 | 0.024 | 44 (12.6) | 503 (15.6) | 8.69 | 0.280 |
| − ≥6 | 18 (5.2) | 141 (4.4) | -3.80 | 0.486 | 16 (4.6) | 138 (4.3) | -1.41 | 0.852 |
| Elixhauser comorbidity score, mean (SD) | 8.0 (7.8) | 9.4 (8.6) | 17.72 | 0.001 | 8.2 (7.6) | 9.2 (8.5) | 13.13 | 0.070 |
| Pneumonia diagnosis, n (%) | 47 (13.5) | 787 (24.4) | 27.95 | <0.001 | 50 (14.5) | 755 (23.4) | 22.89 | 0.013 |
| Pneumonia and/or acute bronchitis/bronchiolitis diagnosis, n (%) | 96 (27.6) | 1178 (36.5) | 19.08 | 0.001 | 98 (28.3) | 1147 (35.5) | 15.43 | 0.076 |
| COPD medications, n (%) | ||||||||
| − Naive to LAMA or LABA§ | 279 (80.2) | 1776 (55.0) | -55.94 | <0.001 | 210 (60.5) | 1857 (57.5) | -6.12 | 0.492 |
| − Any LAMA¶ | 48 (13.8) | 746 (23.1) | 24.13 | <0.001 | 91 (26.1) | 717 (22.2) | -9.15 | 0.314 |
| − Any LABA¶ | 22 (6.3) | 779 (24.1) | 51.10 | <0.001 | 59 (16.9) | 721 (22.3) | 13.68 | 0.222 |
| − Any ICS¶ | 24 (6.9) | 928 (28.7) | 59.50 | <0.001 | 62 (17.7) | 872 (27.0) | 22.34 | 0.048 |
| − LABA + ICS# | 17 (4.9) | 745 (23.1) | 54.30 | <0.001 | 56 (16.0) | 687 (21.3) | 13.49 | 0.240 |
| − Any SABA¶ | 189 (54.3) | 1890 (58.5) | 8.41 | 0.134 | 214 (61.6) | 1870 (57.9) | -7.64 | 0.334 |
| − Any SAMA¶ | 49 (14.1) | 667 (20.6) | 17.38 | 0.004 | 59 (17.1) | 654 (20.3) | 8.21 | 0.416 |
| − SABA + SAMA# | 45 (12.9) | 596 (18.4) | 15.19 | 0.011 | 52 (15.1) | 584 (18.1) | 8.00 | 0.439 |
| − Methlyxanthines | 2 (0.6) | 50 (1.6) | 9.50 | 0.150 | 5 (1.4) | 49 (1.5) | 1.25 | 0.910 |
| − Phosphodiesterase-4 inhibitors | 2 (0.6) | 26 (0.8) | 2.78 | 0.644 | 11 (3.2) | 26 (0.8) | -17.43 | 0.062 |
| − Oral corticosteroids | 131 (37.6) | 1427 (44.2) | 13.27 | 0.020 | 165 (47.5) | 1413 (43.7) | -7.61 | 0.358 |
| Oxygen therapy, n (%) | 77 (22.1) | 1047 (32.4) | 23.21 | <0.001 | 104 (29.9) | 1014 (31.4) | 3.11 | 0.727 |
| Annual exacerbations | ||||||||
| Severe | ||||||||
| − n (%) | 19 (5.5) | 772 (23.9) | 53.94 | <0.001 | 56 (16.3) | 713 (22.1) | 14.76 | 0.185 |
| − Count, mean (SD) | 0.06 (0.28) | 0.28 (0.57) | 49.37 | <0.001 | 0.19 (0.46) | 0.26 (0.55) | 14.10 | 0.174 |
| Moderate | ||||||||
| − n (%) | 130 (37.4) | 1376 (42.6) | 10.67 | 0.061 | 162 (46.6) | 1362 (42.1) | -9.09 | 0.271 |
| − Count, mean (SD) | 0.55 (0.90) | 0.70 (1.07) | 14.41 | 0.006 | 0.77 (1.06) | 0.69 (1.06) | -7.67 | 0.443 |
| GOLD high risk group classification, n (%)†† | 58 (16.7) | 1162 (36.0) | 44.89 | <0.001 | 107 (30.7) | 1101 (34.1) | 7.18 | 0.444 |
| Annual acute inpatient utilization, n (%) | ||||||||
| − COPD-related | 53 (15.2) | 1196 (37.0) | 51.17 | <0.001 | 99 (28.5) | 1125 (34.8) | 13.58 | 0.156 |
| − Pneumonia-related | 23 (6.6) | 613 (19.0) | 37.65 | <0.001 | 45 (12.9) | 579 (17.9) | 14.06 | 0.195 |
| − All-cause | 74 (21.3) | 1340 (41.5) | 44.60 | <0.001 | 112 (32.2) | 1278 (40.0) | 15.29 | 0.095 |
| Annual health plan-paid costs, US$, mean (SD) | ||||||||
| − COPD-related total cost | 3603 (7890) | 9693 (17,939) | 43.95 | <0.001 | 6108 (10,070) | 9157 (17,451) | 21.41 | <0.001 |
| − Pneumonia-related medical cost | 1011 (5437) | 3593 (13,506) | 25.09 | <0.001 | 1331 (4,508) | 3395 (13,090) | 21.09 | <0.001 |
| − All-cause total cost | 14,215 (20,470) | 18,802 (26,440) | 19.40 | <0.001 | 14,674 (17,214) | 18,330 (26,062) | 16.55 | 0.003 |
†
Weighted results were computed from propensity scores derived from a logistic regression model adjusted for health plan type (health maintenance organization, preferred provider organization, other, missing), US census region (northeast, midwest, south, west), index regimen prescriber specialty (pulmonology, all others) and baseline characteristics including pneumonia and/or acute bronchitis/bronchiolitis diagnosis, severe COPD exacerbation, COPD medication use (any LAMA [free dose or combination inhaler], LABA/ICS [single combination inhaler]), HCRU (COPD-attributable ED visit, number of COPD-related ambulatory visits, other COPD-related medical resource use, pneumonia-related ambulatory visit) and COPD-related medical cost quartile group (<US$1450; US$1450 – <US$8700; US$8700 – <US$21,000; ≥US$21,000).
‡
As of index date.
§
Based on medical and pharmacy claims.
¶
Free dose or combination inhaler.
#
Single combination inhaler.
††
≥2 moderate exacerbations or ≥1 severe exacerbation.
COPD: Chronic obstructive pulmonary disease; ED: Emergency department; GOLD: Global initiative for chronic obstructive lung disease; HCRU: Healthcare resource use; ICS: Inhaled corticosteroid; IPTW: Inverse probability of treatment weighting; LABA: Long-acting β2 agonist; LAMA: Long-acting muscarinic antagonist; SABA: Short-acting β2 agonist; SAMA: Short-acting muscarinic antagonist; SD: Standard deviation; STD DIFF: Standardized difference; TIO + OLO: Tiotropium olodaterol; TT: Triple therapy.
Outcomes
COPD-related & all-cause HCRU & costs
Annual medical resource use during follow-up is shown in Table 2. Compared with the TT cohort, significantly lower percentage of TIO + OLO patients had ≥1 COPD-related acute inpatient stays (16.8 vs 28.7%; p < 0.001), ED visits (22.0 vs 30.0%; p = 0.045) and/or outpatient visits (36.1 vs 54.0%; p < 0.001). The TIO + OLO cohort also had fewer mean acute inpatient stays (0.3 vs 0.5; p = 0.006), inpatient days (1.9 vs 3.2 days; p = 0.018) and ED visits (0.3 vs 0.6; p = 0.002). This pattern observed for COPD-related HCRU was also evident for all-cause HCRU: mean counts of acute inpatient stays, ED visits and outpatient visits were lower in the TIO + OLO cohort and a smaller share of TIO + OLO patients utilized these services.
| Medical resource use category | TIO + OLO (n = 347) | TT (n = 3232) | p-value |
|---|---|---|---|
| COPD-related | |||
| Acute inpatient stay | |||
| − n (%) | 58 (16.8) | 927 (28.7) | <0.001 |
| − Count, mean (SD) | 0.28 (0.77) | 0.46 (0.92) | 0.006 |
| − Length of stay, days, mean (SD) | 1.9 (6.7) | 3.2 (8.8) | 0.018 |
| Emergency department visit | |||
| − n (%) | 76 (22.0) | 968 (30.0) | 0.045 |
| − Count, mean (SD) | 0.33 (0.73) | 0.57 (1.34) | 0.002 |
| Office visit | |||
| − n (%) | 310 (89.4) | 2692 (83.3) | 0.052 |
| − Count, mean (SD) | 4.09 (3.23) | 3.85 (3.86) | 0.440 |
| Outpatient visit | |||
| − n (%) | 125 (36.1) | 1746 (54.0) | <0.001 |
| − Count, mean (SD) | 1.66 (3.69) | 2.55 (4.63) | 0.008 |
| Other | |||
| − n (%) | 164 (47.2) | 1805 (55.8) | 0.037 |
| − Count, mean (SD) | 4.36 (7.82) | 6.75 (13.80) | <0.001 |
| All-cause | |||
| Acute inpatient stay | |||
| − n (%) | 80 (22.9) | 1042 (32.2) | 0.009 |
| − Count, mean (SD) | 0.35 (0.81) | 0.55 (1.05) | 0.003 |
| − Length of stay, days, mean (SD) | 2.4 (8.9) | 3.8 (9.7) | 0.018 |
| Emergency department visit | |||
| − n (%) | 139 (40.0) | 1559 (48.2) | 0.043 |
| − Count, mean (SD) | 0.88 (1.62) | 1.38 (2.84) | <0.001 |
| Office visit | |||
| − n (%) | 338 (97.4) | 3106 (96.1) | 0.571 |
| − Count, mean (SD) | 16.49 (13.98) | 14.98 (12.35) | 0.205 |
| Outpatient visit | |||
| − n (%) | 246 (70.9) | 2648 (81.9) | 0.001 |
| − Count, mean (SD) | 7.29 (11.23) | 9.90 (12.69) | 0.001 |
| Other | |||
| − n (%) | 297 (85.5) | 2853 (88.3) | 0.334 |
| − Count, mean (SD) | 9.84 (11.10) | 13.93 (20.87) | <0.001 |
COPD: Chronic obstructive pulmonary disease; SD: Standard deviation; TIO + OLO: Tiotropium olodaterol; TT: Triple therapy.
Annual weighted mean COPD-related costs, before and after multivariable adjustment for baseline characteristics, are shown in Figure 2. Pre-adjustment, total mean weighted COPD-related costs were US$4834 lower for TIO + OLO versus TT (US$7076 vs US$11,910; p < 0.001). Acute inpatient costs were the largest contributor (43.5–45.6%) to the total costs in both cohorts and were also the driver (−US$2353) behind the observed weighted difference. Multivariable adjustment of residual baseline imbalances provided a more conservative estimate of the weighted cohort difference: adjusted total costs averaged US$7794 for TIO + OLO versus US$11,912 for TT and were 35% lower (US$4118) for TIO + OLO (cost ratio [CR] = 0.65; 95% CI = 0.54–0.80). This difference was primarily driven by medical cost differences for TIO + OLO versus TT (US$3103). Specifically, the adjusted COPD-related medical and pharmacy costs were lower for TIO + OLO by approximately 36 and 39%, respectively.

Figure 2. Annual weighted and adjusted† weighted chronic obstructive pulmonary disease-related costs‡ postinitiation of tiotropium olodaterol versus triple therapy.
†COPD-related total, medical and pharmacy adjusted costs were computed using a generalized linear model adjusted for age (<65, 65–<75, 75+), gender, US census region (northeast, midwest, south, west, other), index season (winter, spring, summer, fall), index prescribing provider specialty (pulmonology, internal medicine, cardiology, other), baseline comorbidities (arrhythmia, pneumonia or acute bronchitis/bronchiolitis, pneumonia) and the following baseline characteristics: total days’ supply of any LABA [free dose or combination]), ICS (free dose or combination) use, count of oral corticosteroids fills, oxygen therapy, all-cause utilization (count of ambulatory visits, ≥1 office visit, count of office visits, ≥1 ED visit, count of ED visits, ≥1 acute inpatient stay, count of acute inpatient stays, count of other medical visits), all-cause costs (other medical, medical), COPD-attributable count of ED visits and costs, COPD-related utilization (acute inpatient stays [days], ≥1 ambulatory visit), COPD-related costs (ED, other medical visits, pharmacy) and pneumonia-related count of other medical visits. Park test estimate for model = 1.498.
‡Values are health plan-paid costs.
§Mean costs for TIO + OLO cohort minus mean costs for TT cohort.
COPD: Chronic obstructive pulmonary disease; ED: Emergency department; ICS: Inhaled corticosteroid; LABA: Long-acting bronchodilator agents; TIO + OLO: Tiotropium olodaterol; TT: Triple therapy.
A similar pattern of cost savings for the TIO + OLO cohort was documented for all-cause costs (Figure 3). Annual weighted all-cause total costs were US$6274 lower for TIO + OLO versus TT (US$15,758 vs US$22,031; p < 0.001); after adjustment, weighted costs were 23% lower (US$5384) for TIO + OLO versus TT (US$17,504 vs US$22,887; CR: 0.77; 95% CI: 0.65–0.90). Consistent with the COPD-related cost results, the TIO + OLO cohort’s lower costs were driven primarily by lower (US$4652) adjusted all-cause medical costs (US$11,130 vs US$15,782; p < 0.001).

Figure 3. Annual weighted and adjusted† weighted all-cause costs‡ postinitiation of tiotropium olodaterol versus triple therapy.
†All-cause total, medical and pharmacy adjusted costs were computed using a generalized linear model adjusted for age (<65, 65–<75, 75+), gender, US census region (northeast, midwest, south, west, other), index season (winter, spring, summer, fall), index prescribing provider specialty (pulmonology, internal medicine, cardiology, other), baseline comorbidities (arrhythmia, pneumonia or acute bronchitis/bronchiolitis, pneumonia) and the following baseline characteristics: total days’ supply of any LABA [free dose or combination]), ICS (free dose or combination) use, count of oral corticosteroids fills, oxygen therapy, all-cause utilization (count of ambulatory visits, ≥1 office visit, count of office visits, ≥1 ED visit, count of ED visits, ≥1 acute inpatient stay, count of acute inpatient stays, count of other medical visits), all-cause costs (other medical, medical), COPD-attributable count of ED visits and costs, COPD-related utilization (acute inpatient stays [days], ≥1 ambulatory visit), COPD-related costs (ED, other medical visits, pharmacy) and pneumonia-related count of other medical visits. Park test estimate for model = 1.536.
‡Values are health plan-paid costs.
§Mean costs for TIO + OLO cohort minus mean costs for TT cohort.
COPD: Chronic obstructive pulmonary disease; ED: Emergency department; ICS: Inhaled corticosteroid; LABA: Long-acting bronchodilator agent; TIO + OLO: Tiotropium olodaterol; TT: Triple therapy.
COPD exacerbations
Severe exacerbations were significantly less common during follow-up in the TIO + OLO cohort, with 8.3% experiencing them compared with 15.5% of TT patients (p = 0.014; Table 3). Kaplan–Meier estimates of the distribution of severe exacerbations over time were consistent with these results (p = 0.018; Figure 4A). The percentage of patients with any exacerbation (i.e., moderate or severe) and the corresponding Kaplan–Meier distribution (Figure 4B) did not differ significantly between cohorts.
| COPD exacerbation | TIO + OLO (n = 347) | TT (n = 3232) | p-value |
|---|---|---|---|
| Severe | |||
| – n (%) | 29 (8.3) | 502 (15.5) | 0.014 |
| – Count, mean (SD) | 0.13 (0.49) | 0.20 (0.54) | 0.109 |
| Moderate | |||
| – n (%) | 143 (41.3) | 1331 (41.2) | 0.986 |
| – Count, mean (SD) | 0.75 (1.31) | 0.74 (1.16) | 0.903 |
| Any (moderate or severe) | |||
| – n (%) | 162 (46.8) | 1549 (47.9) | 0.776 |
| – Count, mean (SD) | 0.89 (1.38) | 0.94 (1.37) | 0.736 |
COPD: Chronic obstructive pulmonary disease; SD: Standard deviation; TIO + OLO: Tiotropium olodaterol; TT: Triple therapy.
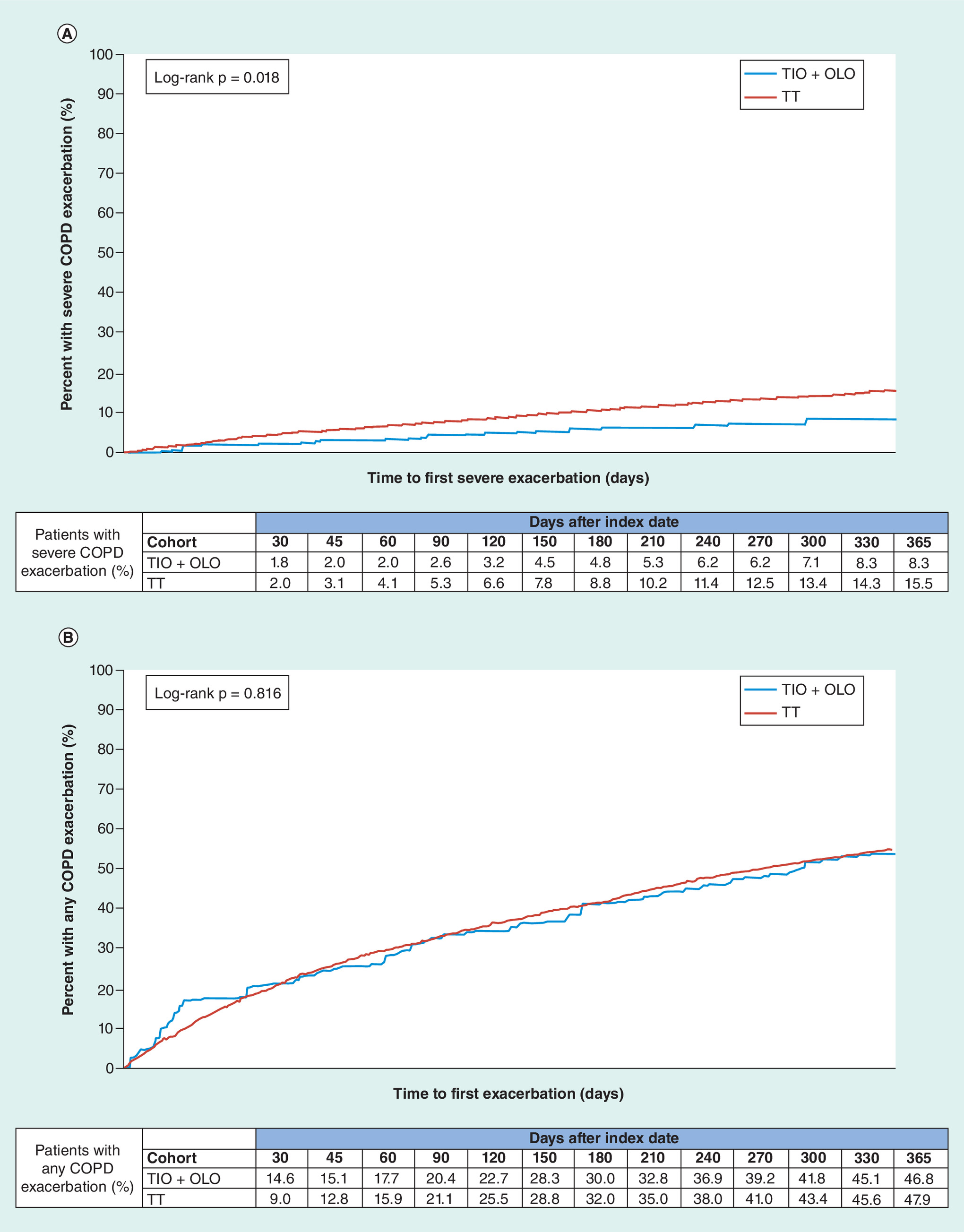
Figure 4. Kaplan–Meier probability of time to first weighted chronic obstructive pulmonary disease exacerbation postinitiation of tiotropium olodaterol versus triple therapy.
(A) Severe COPD exacerbation. (B) COPD exacerbation (any severity).
COPD: Chronic obstructive pulmonary disease; TIO + OLO: Tiotropium olodaterol; TT: Triple therapy.
Pneumonia-related outcomes
Pneumonia or acute bronchitis/bronchiolitis was significantly less common for patients in the TIO + OLO cohort compared with the TT cohort (18.9 vs 30.9%; p < 0.001; Table 4). A smaller percentage of TIO + OLO patients had pneumonia-related acute inpatient stays, and utilization of pneumonia-related ED and outpatient visits was also lower. Total annual pneumonia-related medical costs were lower for TIO + OLO, averaging US$1566 versus US$2897 for TT (p = 0.045). Acute inpatient costs accounted for more than 85% of total pneumonia-related medical costs in both cohorts and the difference between cohorts (US$1138) also appeared to drive the observed medical cost differences. Non-COPD pneumonia-related medical costs averaged US$1223 for the TIO + OLO cohort (78.1% of pneumonia-related medical costs) and US$2058 for the TT cohort (71.0% of pneumonia-related medical costs; p = 0.104). COPD/pneumonia costs were thus calculated to be US$8299 (i.e., US$7076 [COPD] +US$1223 [non-COPD pneumonia]) and US$13,968 (i.e., US$11,910 + US$2058) for the TIO + OLO and TT cohorts respectively, yielding a total difference of US$5669 favoring TIO + OLO.
| Pneumonia outcomes | TIO + OLO (n = 347) | TT (n = 3,232) | p-value |
|---|---|---|---|
| Pneumonia diagnosis, n (%) | 46 (13.3) | 720 (22.3) | 0.007 |
| Pneumonia and/or acute bronchitis/bronchiolitis diagnosis, n (%) | 66 (18.9) | 999 (30.9) | <0.001 |
| Pneumonia-related medical resource use | |||
| Acute inpatient stay | 46 (13.3) | 720 (22.3) | 0.007 |
| – n (%) | 23 (6.6) | 405 (12.5) | 0.014 |
| – Count, mean (SD) | 0.10 (0.46) | 0.16 (0.49) | 0.062 |
| – Length of stay, days, mean (SD) | 0.9 (4.5) | 1.5 (6.5) | 0.105 |
| Emergency department visit | |||
| – n (%) | 23 (6.8) | 338 (10.4) | 0.095 |
| – Count, mean (SD) | 0.08 (0.31) | 0.13 (0.44) | 0.015 |
| Office visit | |||
| – n (%) | 52 (15.0) | 569 (17.6) | 0.367 |
| – Count, mean (SD) | 0.23 (0.71) | 0.31 (0.86) | 0.115 |
| Outpatient visit | |||
| – n (%) | 15 (4.4) | 302 (9.3) | <0.001 |
| – Count, mean (SD) | 0.12 (0.96) | 0.26 (1.20) | 0.002 |
| Other | |||
| – n (%) | 20 (5.8) | 281 (8.7) | 0.152 |
| – Count, mean (SD) | 0.17 (1.11) | 0.41 (2.33) | 0.001 |
| Pneumonia-related medical costs, US$, mean (SD)† | |||
| – Total medical | 1566 (7351) | 2897 (14,202) | 0.045 |
| – Acute inpatient stay | 1360 (6541) | 2498 (13,428) | 0.054 |
| – Emergency department | 28 (175) | 45 (222) | 0.064 |
| – Office | 22 (66) | 27 (80) | 0.258 |
| – Outpatient | 30 (292) | 80 (473) | 0.001 |
| – Other | 126 (1015) | 247 (2064) | 0.154 |
†
Values are health plan-paid costs for medical claims with a diagnosis of pneumonia and/or acute bronchitis/bronchiolitis.
SD: Standard deviation; TIO + OLO: Tiotropium olodaterol; TT: Triple therapy.
Secondary analysis
For the LAMA + LABA versus TT cohort comparison, out of the initial 1368 LAMA + LABA patients, 1366 were well matched to the TT cohort (n = 3232) and retained in the final post-IPTW cohort (Figure 1). COPD-related and all-cause cost outcomes are shown in Supplementary Figures 1 & 2, respectively. Consistent with the primary analysis, adjusted mean annual COPD-related total costs were lower by 25% for LAMA + LABA versus TT (US$8971 vs US$11,985; CR: 0.75; 95% CI: 0.67–0.84; p < 0.001). Total annual all-cause costs followed a similar pattern (US$19,872 vs US$23,055; CR: 0.86; 95% CI: 0.78–0.95; p = 0.002). However, there were no significant differences between cohorts for exacerbation or pneumonia outcomes (complete results shown in the Supplementary Material). Different inhaler combinations within the LAMA + LABA group were not analyzed.
Discussion
To our knowledge, this is the first study comparing resource use, cost, COPD exacerbations and pneumonia after initiating TIO + OLO versus TT within a large real-world MAPD population with COPD. We used IPTW methodology to provide a robust comparison of cohorts [37]. Our findings support economic and COPD health benefit of TIO + OLO versus TT, with lower COPD-related, pneumonia-related and all-cause resource use and costs among patients treated with TIO + OLO, and a smaller percentage of patients experiencing severe exacerbations and pneumonia with TIO + OLO.
Annual COPD-related health plan-paid total costs were 35% lower (−US$4118) for TIO + OLO versus TT, reflecting lower costs in both medical service (−US$3103) and pharmacy (−US$1413) settings. Lower pharmacy costs for TIO + OLO were plausible because TIO + OLO was provided as a single inhaler whereas TT regimens in this study required the use of multiple inhalers. However, cohort differences in COPD-related total costs were primarily driven by medical expenditures, particularly the difference in acute inpatient costs (US$2353). Our results are supported by two previous studies in mixed populations of commercial and managed Medicare enrollees, which found patients initiating TIO + OLO incurred COPD-related costs that were 27–53% lower than their counterparts initiating TT, resulting in annual health plan cost savings of US$3361–US$6765 [29,30]. The COPD-related cost savings observed in the TIO + OLO cohort contributed to lower all-cause costs (23% lower or US$5384 vs TT). The savings in all-cause costs are also consistent with a health and economic modeling study [42] based on efficacy and safety endpoints from the recent IMPACT clinical trial [43] in which total costs were estimated for patients treated with a single LAMA + LABA combination inhaler versus a single combination TT inhaler. In addition, across all phenotypic subgroups examined, annual cost savings with LAMA + LABA ranged from approximately 5–20% [42]. Our secondary analysis comparing treatment with any LAMA + LABA regimen versus the TT cohort found results consistent with the primary analysis; however, the magnitude of the cost savings was lower (US$3013 for COPD-related and US$3183 for all-cause), than what was observed for TIO + OLO versus TT.
Resource use and cost results are consistent with COPD exacerbation and pneumonia outcome results. Acute inpatient costs accounted for 48.7% of the difference in mean COPD-related costs between cohorts. COPD exacerbations have historically been a major driver of COPD burden [7–9], particularly severe exacerbations which, by our definition, required an acute inpatient stay with an admission diagnosis of COPD. In our study, we found that the percentage of patients experiencing severe exacerbations in the TIO + OLO cohort was roughly half that of the TT cohort (8.3 vs 15.5%); moderate exacerbations were more common and nearly identical between cohorts (41.3 vs 41.2%). One plausible interpretation is that there was a larger shift from more severe to less severe exacerbations for TIO + OLO versus TT patients, but this hypothesis remains to be confirmed. Respiratory infections such as pneumonia are a frequent trigger of COPD exacerbations [44] and the increased rate of severe exacerbations in the TT cohort can be potentially explained by the higher rate of pneumonia that we observed in this group of patients. Accounting for pneumonia as part of COPD-related burden further widens the gap between TIO + OLO (or LAMA + LABA) and TT. In the TIO + OLO cohort, 18.9% of patients were diagnosed with pneumonia or acute bronchitis/bronchiolitis compared with 30.9% of patients in the TT cohort. The recent IMPACT clinical trial also observed a 53% increased risk of pneumonia with TT compared with LAMA + LABA [43]. However, the results of IMPACT [43], as well as the recent TRIBUTE clinical trial [45] which compared a single LAMA + LABA combination inhaler with a single combination TT inhaler (albeit with different LAMA, LABA and ICS components than IMPACT), did show a lower rate of moderate-to-severe exacerbations among patients with COPD who were treated with TT versus LAMA + LABA. The difference between our results and these two studies likely reflects multiple factors. First, our study population represents patients with COPD treated in a real-world setting rather than the relatively restrictive selection of patients required for clinical trial participation. For example, patients in both the IMPACT and TRIBUTE trials were likely to have more severe COPD than our population because inclusion in the trial required a history of exacerbations [43,45]. Second, neither clinical trial used TIO + OLO as the LAMA + LABA comparator. Last, the IMPACT study did not exclude patients with asthma; and a majority of patients had previous exposure to ICS, which was then abruptly withdrawn from those randomized to the LAMA + LABA treatment arm. This in turn, may have triggered exacerbations, in particular for those patients with comorbid asthma. The inclusion of patients with asthma and abrupt withdrawal of ICS have been widely criticized for the potential to skew results in favor of the TT arm [46–48].
While it is possible that our resource utilization-based definition of exacerbations underestimated the incidence of milder exacerbations (e.g., patients who did not seek medical treatment), our findings corroborate prior reports that TT is commonly prescribed for patients with less severe symptoms and/or exacerbation risk [15–20] thereby indicating that this GOLD inconsistent prescribing pattern is persisting. Although symptom burden could not be measured in this study, a little over a third (34.1%) of patients in the TT cohort would be classified in Groups C or D based on their exacerbation history (≥1 inpatient or ≥2 outpatient exacerbations). Even conservatively assuming that all TT patients with a high baseline risk of exacerbations also had high symptom burden (i.e., Group D), our results are consistent with most study findings that less severe patients are frequently treated with TT [15–20]. Nevertheless, these results contradict a recent study conclusion that overprescribing of TT is limited to roughly 10% of patients in USA [49]. However, that study considered any history of moderate or severe exacerbation or treatment with a COPD maintenance medication (ICS, LAMA or LABA) – not just high risk of future exacerbation – as a criterion for TT appropriateness. While we cannot know the clinical rationale for prescribing either TIO + OLO (or LAMA + LABA) or TT in our study and we excluded patients diagnosed with asthma, in general practice, COPD may be misdiagnosed as asthma, leading to inappropriate use of ICS in COPD [50,51]. It has also been suggested that some clinicians may initiate care with TT to provide maximum treatment for their patients at the outset [52]; however, this approach is incongruent with the preferred GOLD treatment pathway which recommends TT only as an escalation step, and not as an initial therapy [6]. Notably, 57.5% of TT patients in our study had no exposure to a LAMA or a LABA at baseline, suggesting that the recommended escalation pathway to TT per the 2018 GOLD guidelines was uncommon in our study. Shortly after the results of this study were finalized, the 2019 GOLD guidelines were released [53]. The 2019 guidelines maintain the initial approach to therapy for Groups A–D, but follow-up management, while still based on symptoms and exacerbations, are not dependent on GOLD group classification [53]. Nevertheless, the recommendation for TT only as an escalation step after therapy with LAMA + LABA (or LABA + ICS) has been retained. Thus, efforts either through policies or education or both are needed to encourage guideline-compliant prescribing.
Our study provides novel insights into the real-world impact of patients initiating TIO + OLO (or LAMA + LABA) versus TT. While TT is indicated for a subset of patients with severe COPD [6], use of TT in less severe patients may have negative economic, COPD exacerbation and pneumonia consequences. The risk of pneumonia is an important consideration; pneumonia increases the risk of hospitalization and represents an unnecessary and avoidable expense [54]. Careful assessment of the risks and benefits of ICS therapy as well as inhaler type is needed to identify patients for whom TT should be considered.
Limitations
The results of this study should be interpreted in the context of certain limitations. First, the study used administrative claims data which have inherent limitations. The presence of a diagnosis code on a medical claim is not positive proof of disease, but may have been incorrectly coded or included as rule-out criteria. Nevertheless, we required ≥2 diagnosis codes for COPD (on separate dates of service) plus ≥1 claim for a long-acting bronchodilator-containing regimen, strengthening the patient selection process. Also, while pharmacy claims demonstrate that a prescription was filled, whether patients took the medication as prescribed is unknown. Further, although we were able to capture exacerbation risk using GOLD criteria and included the presence of severe exacerbation(s) as an adjustment variable in the IPTW model, symptom burden as measured by the COPD assessment test (CAT™) or modified British Medical Research Council (mMRC) questionnaire [55] scores per GOLD recommendations, were not available and thus, were not accounted for by IPTW, which may have resulted in undetectable, residual imbalances in COPD severity between cohorts. The same limitation applies to other clinically relevant but claims unobservable characteristics (e.g., tobacco history, spirometry results, COPD phenotype, blood eosinophil count and other clinical markers) and residual imbalance in these characteristics may also have influenced outcomes. Second, because no single TT inhaler was available during the study, the TT cohort required use of multiple inhalers (unlike TIO + OLO) which may be less convenient for patients and could potentially impact adherence and ultimately outcomes. However, treatment with TT administered by a single versus two inhalers did not impact exacerbation outcomes in a clinical trial setting [56]. Third, we used an intent-to-treat approach which assigns outcomes to the index treatment and did not control for medication exposures. Although inclusion required ≥30 days of concurrent therapy with the index regimen, it is possible that patients subsequently discontinued or switched their index regimen and differential rates of persistence or adherence to index therapy among cohorts during follow-up may have affected outcomes. An on-treatment analysis is currently being conducted as a follow-up. Fourth, unlike TIO + OLO, TT and LAMA + LABA regimens included in this study contained a mix of different LAMA and LABA (and ICS for TT) components and inhalers and the potential impact of this mix on outcomes is unknown; assessing their differential impact on the outcomes was not the objective of this study. Fifth, all patients in the study were required to have 12 months of follow-up. This may have led to selection of healthier patients into both cohorts, and may limit the generalizability of our results. Further, if a treatment is associated with survival, the requirement of a fixed follow-up period may have increased the bias, and the planned on-treatment analysis will address this limitation. Lastly, the results of this study are based on a population of Medicare Advantage beneficiaries and may not be generalizable to patients with COPD who have other forms of insurance or the uninsured.
Conclusion
This study concluded that health plans can incur annual per patient cost savings for patients initiating TIO + OLO (or LAMA + LABA) versus TT. Consistent with these cost savings, the percentage of patients experiencing severe exacerbations, as well as pneumonia and acute bronchitis/bronchiolitis, was significantly lower for TIO + OLO compared with TT. These findings provide an important economic and clinical real-world perspective to the GOLD recommendations for LAMA + LABA, and specifically TIO + OLO therapy.
•
The Global Initiative for Chronic Obstructive Lung Disease recommends dual therapy with long-acting muscarinic agents/long-acting β2-agonists (LAMA + LABA) for patients who have persistent symptoms and/or exacerbations on LABA or LAMA monotherapy; triple therapy (TT) with LAMA + LABA + inhaled corticosteroids is reserved for the most severe patients such as those experiencing exacerbations after LAMA + LABA treatment.
•
Use of TT must be balanced with the risk/benefit profile given the substantially higher risk of pneumonia and other complications with regular inhaled corticosteroids use; nevertheless, contrary to Global Initiative for Chronic Obstructive Lung Disease recommendations, TT is commonly overprescribed to patients with mild or moderate disease which may impact clinical and economic outcomes.
•
This retrospective claims-based study compared chronic obstructive pulmonary disease (COPD)-related resource use and health plan-paid costs, COPD exacerbations and pneumonia outcomes among patients initiating tiotropium + olodaterol (TIO + OLO) – a LAMA + LABA fixed-dose combination inhaler – versus TT in a real-world US population of managed Medicare insurees; a secondary analysis compared any LAMA + LABA combination (including TIO + OLO) versus TT.
•
The final study cohorts represented patients diagnosed with COPD initiating TIO + OLO or TT between January 2014 and June 2016; cohorts were balanced for baseline characteristics using inverse probability of treatment weighting prior to statistical comparison of outcomes.
•
The TIO + OLO (n = 347) cohort incurred US$4118 (35%) lower annual COPD-related costs and US$5384 (23% lower annual all-cause than the TT cohort (n = 3232) in the first year after therapy initiation.
•
A lesser percentage of patients in the TIO + OLO versus TT cohort experienced severe exacerbations (8.3 vs 15.5%; p = 0.014) and pneumonia diagnoses (18.9 vs 30.9%; p < 0.001).
•
When the TIO + OLO cohort was expanded to include any LAMA + LABA combination, significant (p < 0.01) but lower cost savings were evident for LAMA + LABA versus TT (COPD-related: 25%; all-cause: 14%).
•
The results of this study support improved economic and COPD health outcomes for TIO + OLO relative to TT in a real-world setting.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2019-0101
Acknowledgments
The authors thank the following study team members of Optum, Inc: S Korrer and L Brekke for analytic support; J Hartje, DV Voorhis, V Peichel and F Cao for programing support; and M Sipper for project management.
Financial & competing interests disclosure
This study was sponsored by Boehringer Ingelheim Pharmaceuticals, Inc., Ridgefield, CT, USA. SR Palli and S Kaila are employees of Boehringer Ingelheim Pharmaceuticals, Inc. T Juday was an employee of Boehringer Ingelheim Pharmaceuticals, Inc at the time of the study. AR Buikema, M Ducharme and M Frazer are employees of Optum, Inc., which was contracted by Boehringer Ingelheim Pharmaceuticals, Inc. to conduct the study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
S Peirce-Sandner provided medical writing assistance and was funded by Boehringer Ingelheim Pharmaceuticals, Inc.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 313.22 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
American Lung Association. Trends in COPD (chronic bronchitis and emphysema): morbidity and mortality (2013). http://www.lung.org/assets/documents/research/copd-trend-report.pdf
2.
Wheaton AG, Cunningham TJ, Ford ES, Croft JB, Centers for Disease Control and Prevention. Employment and activity limitations among adults with chronic obstructive pulmonary disease – United States, 2013. MMWR Morb. Mortal Wkly Rep. 64(11), 289–295 (2015).
3.
James SL, Abate D, Abate KH et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159), 1789–1858 (2018).
4.
Soriano JB, Abajobir AA, Abate KH et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 5(9), 691–706 (2017).
5.
Ford ES, Murphy LB, Khavjou O, Giles WH, Holt JB, Croft JB. Total and state-specific medical and absenteeism costs of COPD among adults aged >/= 18 years in the United States for 2010 and projections through 2020. Chest 147(1), 31–45 (2015).
6.
Global Initiative for Chronic Obstructive Lung Disease, Inc. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2018). https://goldcopd.org/wp-content/uploads/2017/11/GOLD-2018-v6.0-FINAL-revised-20-Nov_WMS.pdf
•• This 2018 international consensus report (Global Initiative for Chronic Obstructive Lung Disease) provides recommendations for management of chronic obstructive pulmonary disease, which include restricting triple therapy (TT) for only the most severe patients.
7.
Dalal AA, Patel J, D'Souza A, Farrelly E, Nagar S, Shah M. Impact of COPD exacerbation frequency on costs for a managed care population. J. Manag. Care Spec. Pharm. 21(7), 575–583 (2015).
8.
Dhamane AD, Moretz C, Zhou Y et al. COPD exacerbation frequency and its association with health care resource utilization and costs. Int. J. Chron. Obstruct. Pulmon. Dis. 10, 2609–2618 (2015).
• The frequency of chronic obstructive pulmonary disease exacerbation was a major driver of real-world healthcare costs.
9.
Patel JG, Coutinho AD, Lunacsek OE, Dalal AA. COPD affects worker productivity and health care costs. Int. J. Chron. Obstruct. Pulmon. Dis. 13, 2301–2311 (2018).
10.
Dransfield MT, Bailey W, Crater G, Emmett A, O'Dell DM, Yawn B. Disease severity and symptoms among patients receiving monotherapy for COPD. Prim. Care. Respir. J. 20(1), 46–53 (2011).
11.
Asche CV, Leader S, Plauschinat C et al. Adherence to current guidelines for chronic obstructive pulmonary disease (COPD) among patients treated with combination of long-acting bronchodilators or inhaled corticosteroids. Int. J. Chron. Obstruct. Pulmon. Dis. 7, 201–209 (2012).
12.
Fitch K, Iwasaki K, Pyenson B, Plauschinat C, Zhang J. Variation in adherence with Global Initiative for Chronic Obstructive Lung Disease (GOLD) drug therapy guidelines: a retrospective actuarial claims data analysis. Curr. Med. Res. Opin. 27(7), 1425–1429 (2011).
13.
Price D, West D, Brusselle G et al. Management of COPD in the UK primary-care setting: an analysis of real-life prescribing patterns. Int. J. Chron. Obstruct. Pulmon. Dis. 9, 889–904 (2014).
14.
White P, Thornton H, Pinnock H, Georgopoulou S, Booth HP. Overtreatment of COPD with inhaled corticosteroids – implications for safety and costs: cross-sectional observational study. PLoS ONE 8(10), e75221 (2013).
15.
Barrecheguren M, Monteagudo M, Ferrer J et al. Treatment patterns in COPD patients newly diagnosed in primary care. A population-based study. Respir. Med. 111, 47–53 (2016).
16.
Brusselle G, Price D, Gruffydd-Jones K et al. The inevitable drift to triple therapy in COPD: an analysis of prescribing pathways in the UK. Int. J. Chron. Obstruct. Pulmon. Dis. 10, 2207–2217 (2015).
• Overuse of inhaled corticosteroid-containing regimens was extensive and ultimately led to overuse of TT in primary care practice.
17.
Burgel PR, Deslee G, Jebrak G et al. Real-life use of inhaled corticosteroids in COPD patients versus the GOLD proposals: a paradigm shift in GOLD 2011? Eur. Respir. J. 43(4), 1201–1203 (2014).
18.
Casas A, Montes de Oca M, Menezes AM et al. Respiratory medication used in COPD patients from seven Latin American countries: the LASSYC study. Int. J. Chron. Obstruct. Pulmon. Dis. 13, 1545–1556 (2018).
19.
Safka KA, Wald J, Wang H, McIvor L, McIvor A. GOLD stage and treatment in COPD: a 500 patient point prevalence study. Chronic Obstr. Pulm. Dis. 4(1), 45–55 (2016).
20.
Simeone JC, Luthra R, Kaila S et al. Initiation of triple therapy maintenance treatment among patients with COPD in the US. Int. J. Chron. Obstruct. Pulmon. Dis. 12, 73–83 (2017).
21.
Yang IA, Clarke MS, Sim EH, Fong KM. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst. Rev.(7), CD002991 (2012).
•• Meta-analysis of randomized controlled trials found that regular use of inhaled corticosteroid-containing regimens increased the risk of pneumonia by 56% over placebo.
22.
Yawn BP, Li Y, Tian H, Zhang J, Arcona S, Kahler KH. Inhaled corticosteroid use in patients with chronic obstructive pulmonary disease and the risk of pneumonia: a retrospective claims data analysis. Int. J. Chron. Obstruct. Pulmon. Dis. 8, 295–304 (2013).
23.
Flynn RW, MacDonald TM, Hapca A, MacKenzie IS, Schembri S. Quantifying the real life risk profile of inhaled corticosteroids in COPD by record linkage analysis. Respir. Res. 15, 141 (2014).
24.
Lee TA, Weiss KB. Fracture risk associated with inhaled corticosteroid use in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 169(7), 855–859 (2004).
25.
Price DB, Russell R, Mares R et al. Metabolic effects associated with ICS in patients with COPD and comorbid type 2 diabetes: a historical matched cohort study. PLoS ONE 11(9), e0162903 (2016).
26.
Buhl R, Criee CP, Kardos P et al. Dual bronchodilation vs triple therapy in the ‘real-life’ COPD DACCORD study. Int. J. Chron. Obstruct. Pulmon. Dis. 13, 2557–2568 (2018).
• Patients treated with long-acting muscarinic antagonist + long-acting β2 agonist in primary and secondary care experienced exacerbations at roughly half the rate of patients treated with TT.
27.
STIOLTO® RESPIMAT® (tiotropium bromide and olodaterol) inhalation spray for oral inhalation use [prescribing information]. Boehringer Ingelheim Pharmaceuticals, Inc., CT, USA (2018). https://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Stiolto%20Respimat/stiolto.pdf
28.
Halpin DMG. The role of tiotropium + olodaterol dual bronchodilator therapy in the management of chronic obstructive pulmonary disease. Tuberc. Respir. Dis. (Seoul) 81(1), 13–18 (2018).
29.
Palli SR, Buikema AR, Korrer S et al. Comparing healthcare costs in COPD patients initiating tiotropium/olodaterol vs. triple therapy. Presented at: Academy of Managed Care Pharmacy (AMCP) Nexus. FL, USA, 22–25 October (2018).
30.
Palli SR, Kaila S, Juday T. Comparing healthcare cost and resource utilization in COPD patients initiating tiotropium/olodaterol (T/O) vs. triple therapy (TT). Presented at: 40th Annual Meeting of the Society for Medical Decision Making (SMDM). Montreal, Canada, 14–17 October (2018).
31.
Ford ES. Hospital discharges, readmissions, and ED visits for COPD or bronchiectasis among US adults: findings from the nationwide inpatient sample 2001–2012 and Nationwide Emergency Department Sample 2006–2011. Chest 147(4), 989–998 (2015).
32.
Jinjuvadia C, Jinjuvadia R, Mandapakala C, Durairajan N, Liangpunsakul S, Soubani AO. Trends in outcomes, financial burden, and mortality for acute exacerbation of chronic obstructive pulmonary disease (COPD) in the United States from 2002 to 2010. COPD 14(1), 72–79 (2017).
33.
Singh JA, Yu S. Utilization due to chronic obstructive pulmonary disease and its predictors: a study using the U.S. National Emergency Department Sample (NEDS). Respir. Res. 17, 1 (2016).
34.
Quan H, Li B, Couris CM et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173(6), 676–682 (2011).
35.
van Walraven C, Austin PC, Jennings A, Quan H, Forster AJ. A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Med. Care 47(6), 626–633 (2009).
36.
United States, Department of Labor, Bureau of Labor Statistics. Consumer Price Index. Medical Care. Series ID: CUUR0000SAM (2017). http://data.bls.gov/cgi-bin/surveymost?cu
37.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46(3), 399–424 (2011).
38.
Sturmer T, Wyss R, Glynn RJ, Brookhart MA. Propensity scores for confounder adjustment when assessing the effects of medical interventions using nonexperimental study designs. J. Intern. Med. 275(6), 570–580 (2014).
39.
McCaffrey DF, Griffin BA, Almirall D, Slaughter ME, Ramchand R, Burgette LF. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat. Med. 32(19), 3388–3414 (2013).
40.
Manning WG, Mullahy J. Estimating log models: to transform or not to transform? J. Health Econ. 20(4), 461–494 (2001).
41.
Graubard BI, Korn EL. Predictive margins with survey data. Biometrics 55(2), 652–659 (1999).
42.
Langham S, Wright A, Baldwin M. Costs and outcomes of single-inhaler triple therapy compared to dual therapy with a long-acting beta agonist and long-acting muscarinic antagonist for the treatment of patients with chronic obstructive pulmonary disease in the United States. J. Manag. Care Spec. Pharm. 24(Suppl. 10-a), S70 (2018).
43.
Lipson DA, Barnhart F, Brealey N et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N. Engl. J. Med. 378(18), 1671–1680 (2018).
44.
Sapey E, Stockley RA. COPD exacerbations. 2: aetiology. Thorax 61(3), 250–258 (2006).
45.
Papi A, Vestbo J, Fabbri L et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet 391(10125), 1076–1084 (2018).
46.
Suissa S, Drazen JM. Making sense of triple inhaled therapy for COPD. N. Engl. J. Med. 378(18), 1723–1724 (2018).
47.
Petite SE. Single-inhaler triple versus dual therapy in patients with COPD. N. Engl. J. Med. 379(6), 591–592 (2018).
48.
Wedzicha JA, Banerji D, Kostikas K. Single-inhaler triple versus dual therapy in patients with COPD. N. Engl. J. Med. 379(6), 591 (2018).
49.
Bogart M, Stanford RH, Reinsch T, Hull M, Buikema A, Hulbert E. Clinical characteristics and medication patterns in patients with COPD prior to initiation of triple therapy with ICS/LAMA/LABA: a retrospective study. Respir. Med. 142, 73–80 (2018).
50.
Miravitlles M, Andreu I, Romero Y, Sitjar S, Altes A, Anton E. Difficulties in differential diagnosis of COPD and asthma in primary care. Br. J. Gen. Pract. 62(595), e68–e75 (2012).
51.
Price DB, Yawn BP, Jones RC. Improving the differential diagnosis of chronic obstructive pulmonary disease in primary care. Mayo Clin. Proc. 85(12), 1122–1129 (2010).
52.
Cazzola M. The use of triple therapy in chronic obstructive pulmonary disease and outcomes of the IMPACT trial. Eur. Respir. Pulm. Dis. 4(1), 17–18 (2018).
53.
Global Initiative for Chronic Obstructive Lung Disease, Inc. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2019 report) (2019). https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14Nov2018-WMS.pdf
54.
Ernst P, Gonzalez AV, Brassard P, Suissa S. Inhaled corticosteroid use in chronic obstructive pulmonary disease and the risk of hospitalization for pneumonia. Am. J. Respir. Crit. Care Med. 176(2), 162–166 (2007).
55.
Fletcher CM. Standardised questionnaire on respiratory symptoms: a statement prepared and approved by the MRC Committee on the Aetiology of Chronic Bronchitis (MRC breathlessness score). BMJ 2, 1665 (1960).
56.
Vestbo J, Papi A, Corradi M et al. Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (TRINITY): a double-blind, parallel group, randomised controlled trial. Lancet 389(10082), 1919–1929 (2017).
Information & Authors
Information
Published In
Pages: 1299 - 1316
PubMed: 31559852
Copyright
© 2019 Swetha R Palli. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 18 July 2019
Accepted: 12 September 2019
Published online: 27 September 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Costs, exacerbations and pneumonia after initiating combination tiotropium olodaterol versus triple therapy for chronic obstructive pulmonary disease. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0101
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Asif Shaikh, John Ritz, Julian Casciano, Swetha Palli, Brendan Clark, Zenobia Dotiwala, Jennifer Quint, Clinical and Economic Evaluation of Fluticasone Furoate/Umeclidinium/Vilanterol Versus Tiotropium/Olodaterol Therapy in Maintenance Treatment–Naive Patients with COPD in the US, International Journal of Chronic Obstructive Pulmonary Disease, 10.2147/COPD.S479504, Volume 20, (335-348), (2025).
- Wouter H van Geffen, Daniel J Tan, Julia AE Walters, E Haydn Walters, Inhaled corticosteroids with combination inhaled long-acting beta2-agonists and long-acting muscarinic antagonists for chronic obstructive pulmonary disease, Cochrane Database of Systematic Reviews, 10.1002/14651858.CD011600.pub3, 2024, 2, (2023).
- Sanjay Sethi, Swetha R Palli, Lindsay G S Bengtson, Erin K Buysman, Brendan Clark, Andrew Sargent, Asif Shaikh, Gary T Ferguson, Clinical and economic outcomes in patients with chronic obstructive pulmonary disease initiating maintenance therapy with tiotropium bromide/olodaterol or fluticasone furoate/umeclidinium/vilanterol, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2023.22373, 29, 7, (791-806), (2023).
- Sanjay Sethi, Brendan Clark, Lindsay GS Bengtson, Erin K Buysman, Swetha Palli, Andrew Sargent, Asif Shaikh, Gary T Ferguson, Healthcare Resource Utilization, Cost and Clinical Outcomes in Patients Diagnosed with COPD Initiating Tiotropium Bromide/Olodaterol versus Fluticasone Furoate/Umeclidinium/Vilanterol Based on Exacerbation History, International Journal of Chronic Obstructive Pulmonary Disease, 10.2147/COPD.S386962, Volume 18, (625-641), (2023).
- Sanjay Sethi, Antony Wright, Elisabeth Sophia Hartgers-Gubbels, Marlene Hechtner, Brendan Clark, Ciara Wright, Sue Langham, Roland Buhl, Costs and Clinical Consequences of Compliance with COPD GOLD Recommendations or National Guidelines Compared with Current Clinical Practice in Belgium, Germany, Sweden, and the United States, International Journal of Chronic Obstructive Pulmonary Disease, 10.2147/COPD.S371440, Volume 17, (2149-2160), (2022).
- Kostiantyn D. Dmytriiev, Yuriy M. Mostovoy, Oleksandr Dobrovanov, Nataliia S. Slepchenko, EFFICACY OF COMBINATION OF TIOTROPIUM/OLODATEROL IN PATIENTS WITH COPD IN REAL CLINICAL PRACTICE, Wiadomości Lekarskie, 10.36740/WLek202212110, 75, 12, (2953-2957), (2022).
- Swetha R Palli, Bin Xie, Benjamin Chastek, Caitlin A Elliott, Lindsay G S Bengtson, Comparison of COPD health care utilization and associated costs across patients treated with LAMA+LABA fixed-dose therapies, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2021.20514, 27, 7, (810-824), (2021).
- Jennifer Cook, Chloe Bloom, Jen Lewis, Zoe Marjenberg, Jaime Hernando Platz, Sue Langham, Impact of health technology assessment on prescribing patterns of inhaled fixed-dose combination triple therapy in chronic obstructive pulmonary disease, Journal of Market Access & Health Policy, 10.1080/20016689.2021.1929757, 9, 1, (2021).
- Swetha R Palli, Siting Zhou, Asif Shaikh, Vincent J Willey, Effect of compliance with GOLD treatment recommendations on COPD health care resource utilization, cost, and exacerbations among patients with COPD on maintenance therapy, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2021.20390, 27, 5, (625-637), (2021).
- Swetha R. Palli, Monica Frazer, Mary DuCharme, Ami R. Buikema, Amy J. Anderson, Jessica Franchino-Elder, Differences in Real-World Health and Economic Outcomes Among Patients with COPD Treated with Combination Tiotropium/Olodaterol Versus Triple Therapy, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2020.20159, 26, 10, (1363-1374), (2020).