Effectiveness of using an extensively hydrolyzed casein formula supplemented with Lactobacillus rhamnosus GG compared with an extensively hydrolysed whey formula in managing cow’s milk protein allergic infants
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the comparative effectiveness of two hypoallergenic formulae in managing cow’s milk allergic infants. Materials & methods: This study retrospectively analyzed the case records of 940 formula-fed cow’s milk allergic infants in the UK extracted from The Health Improvement Network database. Results: At 24 months after starting a formula, 77% of infants fed an extensively hydrolyzed casein formula supplemented with Lactobacillus rhamnosus GG (eHCF LGG; n = 470) were estimated to have been successfully managed compared with 63% of matched infants who were fed an extensively hydrolyzed whey formula (eHWF; n = 470; p < 0.001). Additionally, significantly more eHWF-fed infants were estimated to be experiencing gastrointestinal symptoms, eczema and asthma (7.1 vs 3.1%; p < 0.02) at 24 months. Conclusion: First-line management of newly diagnosed cow’s milk allergic infants with eHCF LGG may slow down the allergic march seen in cow’s milk allergic children.
Cow’s milk protein allergy (CMPA) is one of the most common food allergies in early childhood, with an estimated prevalence of 2–3% in the first year of life in developed countries [1,2]. CMPA can develop in both exclusively or partially breast-fed children when introduced to cow’s milk. However, the incidence of CMPA is lower among exclusively breast-fed children than formula-fed or mixed-fed children [3].
The only proven treatment for CMPA consists of a cow’s milk protein elimination diet for breast-feeding mothers and/or the use of a hypoallergenic formula [4,5]. Such formulae include extensively hydrolyzed formulae (eHF) and amino acid formulae. eHF contain casein-based milk proteins or whey-based milk proteins, which have been predigested [6], whereas amino acid formulae contain 100% free amino acids. These formulae are considered effective in the dietary management of CMPA [7].
Cow’s milk allergic children fed an extensively hydrolyzed casein formula (eHCF) supplemented with the probiotic Lactobacillus rhamnosus GG (LGG) experience higher tolerance rates to cow’s milk protein compared with those fed an eHCF without LGG or other formulae [8–10]. Results from a recent randomized controlled trial found that the relative risk for the occurrence of at least one allergic manifestation (eczema, urticaria, asthma and rhinoconjunctivitis) was reduced by 49% at 36 months among those children with CMPA, who were fed eHCF LGG compared with those fed eHCF alone [11]. However, there are no published studies comparing tolerance acquisition to cow’s milk protein or the development of allergic manifestations among infants fed with an extensively hydrolyzed whey formula (eHWF) compared with any other hypoallergenic formula. Hence, the aim of this study was to assess the comparative effectiveness and occurrence of allergic manifestations in clinical practice among children with CMPA, who were fed eHCF LGG (Nutramigen LGG) compared with those fed an eHWF (Aptamil Pepti) over a period of 24 months from the start of formula.
Materials & methods
Study design
This was a retrospective cohort analysis of the case records of cow’s milk allergic infants extracted from The Health Improvement Network (THIN) database.
The Health Improvement Network database
The THIN database contains electronic records on >11 million anonymized patients entered by general practitioners (GPs) from >560 practices across the UK. The patient composition within the THIN database has been shown to be representative of the UK population [12], and the database theoretically contains patients’ entire medical history as previously described [13]. Hence, the information contained in the THIN database reflects actual clinical practice in the UK.
(THIN is a registered trademark of Cegedim SA in the UK and other countries. Reference made to the THIN database is intended to be descriptive of the data asset licensed by IQVIA).
Study population
The study population comprised the anonymized case records of a randomly selected cohort of 470 cow’s milk allergic infants from the THIN database, who were initially fed eHWF. These infants were matched with 470 cow’s milk allergic infants from the database, who were initially fed eHCF LGG. The infants were matched according to age, gender, weight, presenting symptoms and interval between presenting symptoms and starting a formula.
Infants were included in the dataset if they:
•
Had a diagnosis of CMPA;
•
Received a prescription for eHCF LGG (Nutramigen LGG) or eHWF (Aptamil Pepti) as their initial formula;
•
Were <1 year of age at the time of starting their first formula;
•
Had at least 12 months medical history in their case record from the time of starting their initial formula.
Infants were excluded from the dataset if they:
•
Did not receive eHCF LGG or eHWF as their first formula;
•
Were >1 year of age at the time of starting their first formula;
•
Did not have at least 12 months medical history in their case record from the time of starting their initial formula.
Ethics approval
The authors obtained ethics approval to use the complete patients’ records from the THIN database from the SRC research ethics committee that appraises studies using the THIN database (reference number 18THIN086).
Study variables & clinical outcomes
Patients’ characteristics, symptoms, clinical outcomes and prescriptions for both clinical nutrition and drugs were systematically extracted from their electronic records and quantified for each group.
The THIN database does not define successful treatment. Hence, infants were considered to be successfully treated if they were no longer using a formula and documented as being symptom-free or no longer cow’s milk allergic, or stopped receiving a prescription for a formula for at least 3 months and there was no other evidence of them being managed for CMPA.
Infants were considered to be suffering from eczema if it was documented in their case records or if they were receiving prescriptions for emollients, topical steroids, anti-infective creams or topical calcineurin inhibitors. Infants were considered to be suffering from gastrointestinal symptoms if it was documented in their case records or if they were receiving prescriptions for H2 antagonists, proton pump inhibitors, antacids, laxatives or antidiarrheals. Infants were considered to be suffering from urticaria if it was documented in their case records or if they were receiving prescriptions for oral antihistamines. Infants were considered to be suffering from rhinitis if it was documented in their case records or if they were receiving prescriptions for nasal spray antihistamines. Infants were considered to be suffering from asthma if it was documented in their case records or if they were receiving prescriptions for inhaled bronchodilators, inhaled steroids, oral prednisolone, oral leukotriene receptor antagonists or inhaled β2 adrenergic receptor agonists. Infants were considered to be suffering from non-asthmatic respiratory symptoms if it was documented in their case records or if they had respiratory symptoms but did not receive a prescription for asthma-relieving medication. Infants were considered to be suffering from anaphylaxis or faltering growth (failure to thrive) if it was documented in their records. These symptoms were not analysed if the infants switched from their initial formula.
Statistical analyses
Analysis of covariance (ANCOVA) was performed to enable differences in infants’ outcomes between the two groups to be adjusted for any heterogeneity in the following covariates: age, gender and interval between symptom presentation and start of a formula. Differences between the two groups were tested for statistical significance using either a Mann–Whitney U-test or a χ2 test. Binary logistic regression investigated relationships between baseline variables and clinical outcomes. Kaplan–Meier analyses were undertaken to compare the probability distributions of being symptomatic between the two groups. The p-values <0.05 were considered statistically significant and have been reported. All p-values ≥0.05 were not considered to be statistically significant, and numerical values >0.05 have not been reported. All statistical analyses were performed using IBM SPSS Statistics (IBM, UK).
Results
The infants in this study initially presented with symptoms of CMPA between 2013 and 2017. However, there was no difference in baseline characteristics or outcomes irrespective of when they presented. A description of the patients’ characteristics is summarized in Table 1.
| eHCF LGG | eHWF | p-value | |
|---|---|---|---|
| Mean age per infant (months) | 4.2 ± 2.7 | 5.4 ± 2.9 | ns |
| Mean weight per infant (kg) | 3.6 ± 0.7 | 3.2 ± 0.7 | ns |
| Percentage male | 55.1% | 58.1% | ns |
| Mean duration between initial presentation and starting a formula per infant (months) | 1.9 ± 2.4 | 1.9 ± 2.3 | ns |
| Mean length of time on initial formula per infant (months) | 8.3 ± 6.7 | 10.2 ± 8.9 | 0.001 |
| Percentage of infants who switched from their initial formula | 24.0% | 31.1% | <0.02 |
| Percentage with eczema at presentation | 24.8% | 26.7% | ns |
| Percentage with gastrointestinal symptoms at presentation – Bloody stools – Reflux – Constipation – Vomiting and/or diarrhoea – Colic – Uncategorized symptoms – Mucus in stools | 24.0% 46.0% 23.0% 14.0% 18.9% 8.9% 1.1% 0.2% | 25.8% 38.1% 18.9% 13.0% 13.0% 7.0% 0.0% 0.2% | ns <0.02 ns ns <0.02 ns ns ns |
| Percentage with rhinitis at presentation | 1.6% | 1.8% | ns |
| Percentage with urticaria at presentation | 9.1% | 11.1% | ns |
| Percentage with respiratory symptoms at presentation | 5.3% | 2.6% | ns |
eHCF: Extensively hydrolyzed casein formula; eHWF: Extensively hydrolyzed whey formulae; LGG: Lactobacillus rhamnosus GG; ns: Nonsignificant.
Infant management of CMPA
Significantly more eHCF LGG-fed infants remained on their initial formula than eHWF-fed infants (76 vs 69%; p < 0.02). Additionally, eHCF LGG-fed infants continued feeding with their initial formula for a significantly shorter duration than eHWF-fed infants (8.3 ± 6.7 vs 10.2 ± 8.9 months; p = 0.001).
A total 16% of the eHCF LGG-fed infants switched to an amino acid formula, 3% to an eHWF, 3% to a soy formula and 2% to an eHCF. A total 18% of the eHWF-fed infants switched to an amino acid formula, 8% to an eHCF, 4% to a soy formula and 1% to eHCF LGG.
At 3 months after starting a formula, significantly more infants fed eHCF LGG were estimated to have been successfully managed than those fed eHWF. This difference continued to increase and by 24 months after starting a formula, 77% of infants fed eHCF LGG were estimated to have been successfully managed compared with 63% of those fed eHWF (p < 0.001; Figure 1A).

Figure 1. (A) Infants who were successfully treated with a formula. (B) Infants estimated to have gastrointestinal symptoms among those who did not switch from their initial formula.
*p < 0.001; **p < 0.02; ***p < 0.03; ****p < 0.05.
eHCF: Extensively hydrolyzed casein formula; eHWF: Extensively hydrolyzed whey formulae; LGG: Lactobacillus rhamnosus GG.
At 24 months after starting a formula significantly more eHWF-fed infants were experiencing gastrointestinal symptoms (Figure 1B). In the eHCF LGG group (n = 357), these symptoms comprised bloody stools (32%), vomiting and diarrhoea (16%), constipation (14%), reflux (8%), colic (2%) and mucus in stools (0%). In the eHWF group (n = 324), these symptoms comprised bloody stools (22%), vomiting and diarrhoea (28%), constipation (11%), reflux (5%), colic (2%) and mucus in stools (<1%).
Over 24 months from the start of formula <1% of infants in both groups were documented as having experienced anaphylaxis or faltering growth (or failure to thrive) at some point.
Allergic manifestations of CMPA
The estimates of allergic manifestations pertains to those patients who did not switch from their initial formula (i.e. n = 357 eHCF LGG-fed infants and n = 324 eHWF-fed infants. At 24 months after starting a formula, significantly more eHWF-fed infants were estimated to be experiencing eczema (Figure 2A). There were no significant differences between the two groups in the percentage of patients presenting with rhinitis (Figure 2B), urticaria (Figure 2C) and non-asthmatic respiratory symptoms (Figure 2D). Significantly more infants fed eHWF were estimated to be experiencing asthma (Figure 3) by 24 months after starting formula compared with those fed eHCF LGG (7.1 vs 3.1%; p < 0.02). In the subgroup of infants who had urticaria at initial presentation, 15.1% of eHWF-fed infants were considered to be experiencing asthma by 24 months compared with 5.1% of eHCF LGG-fed infants (p = 0.05). In comparison, in the subgroup of infants who had no urticaria at presentation, 5.5% of eHWF-fed infants were considered to be experiencing asthma by 24 months compared with 2.5% of eHCF LGG-fed infants (p < 0.03).
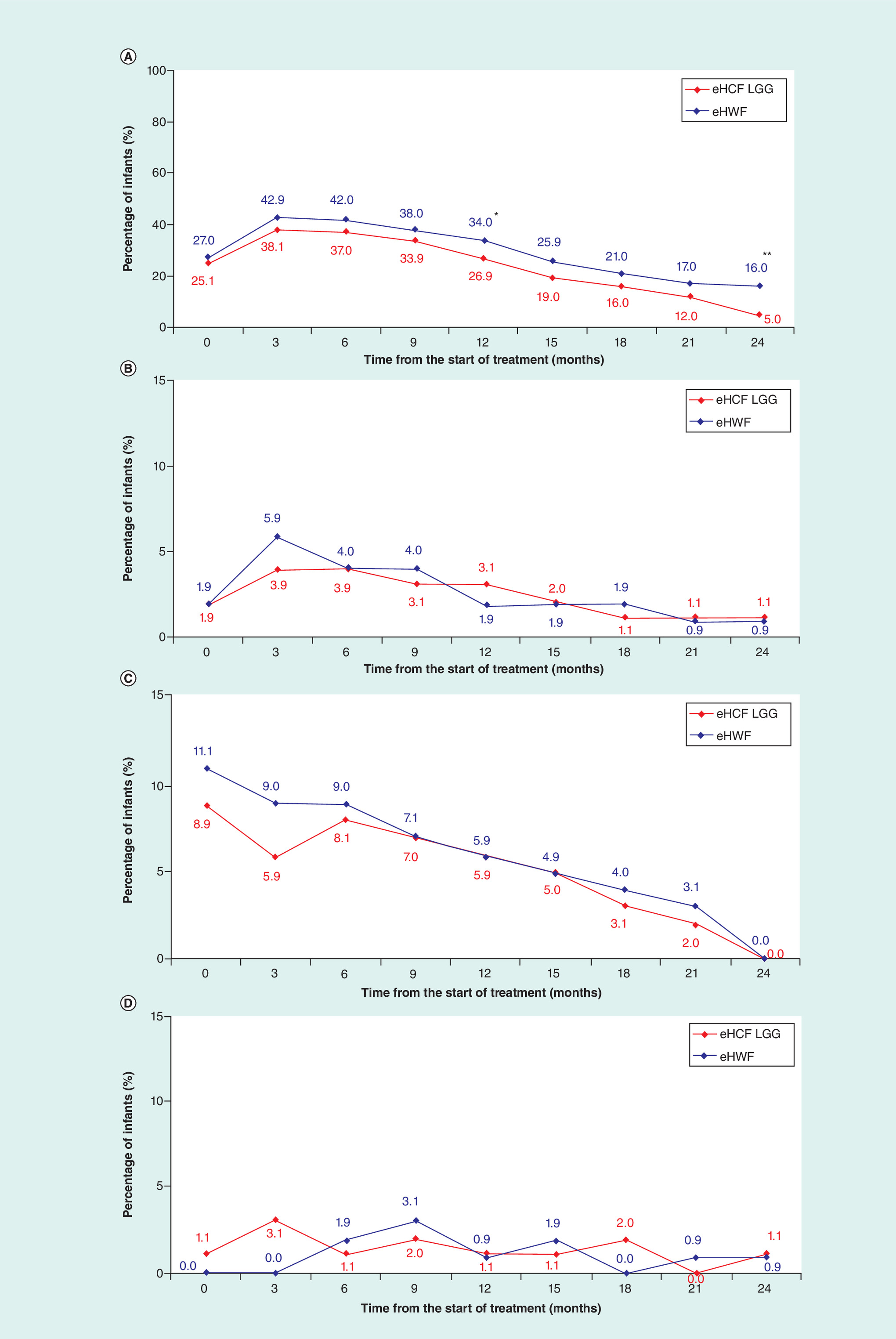
Figure 2. Percentage of infants with an allergic manifestation.
(A) Infants estimated to have eczema. (B) Infants estimated to have rhinitis. (C) Infants estimated to have urticaria. (D) Infants estimated to have nonasthmatic respiratory symptoms.
*p < 0.05; **p < 0.001.
eHCF: Extensively hydrolyzed casein formula; eHWF: Extensively hydrolyzed whey formulae; LGG: Lactobacillus rhamnosus GG.
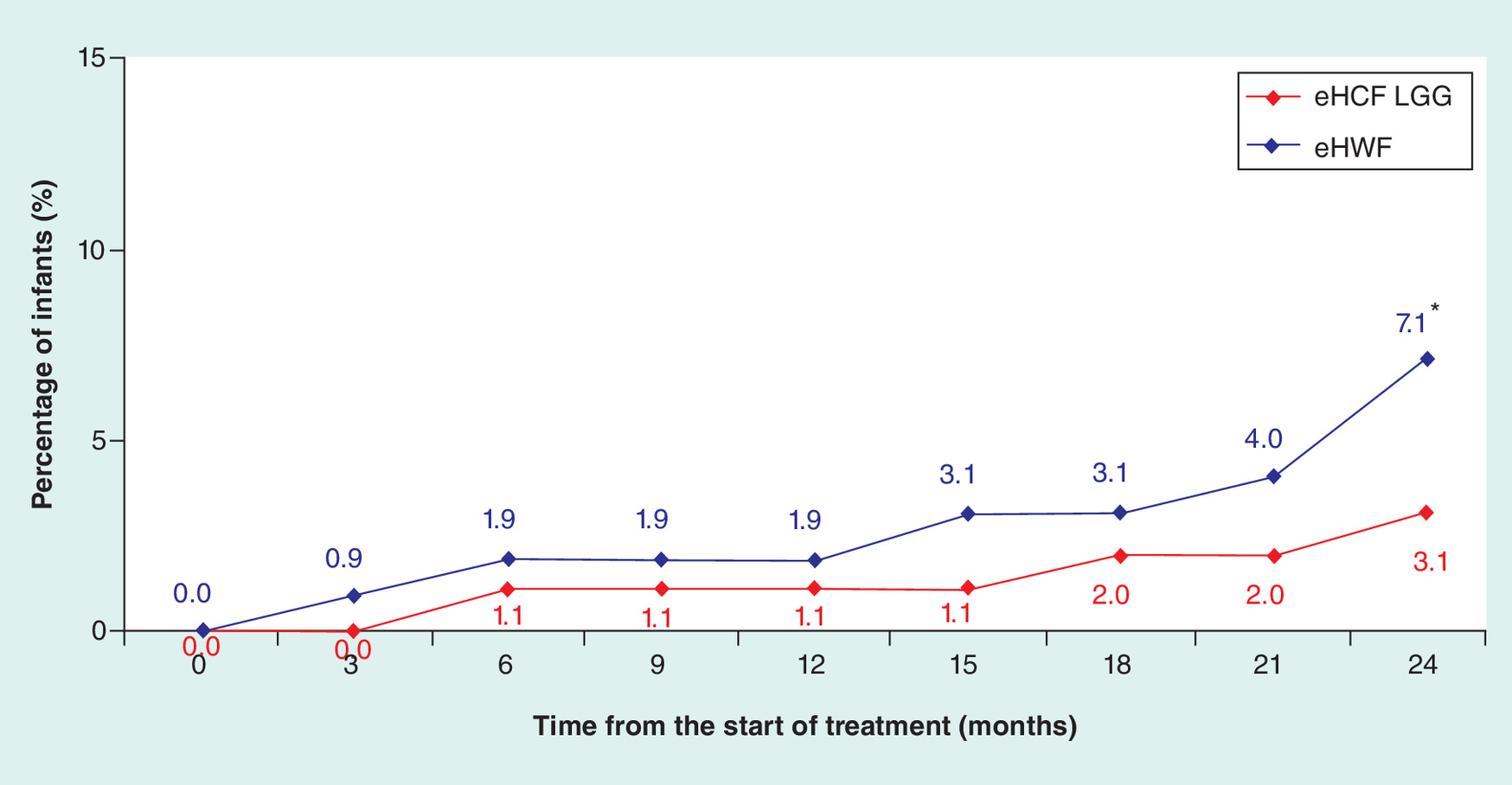
Figure 3. Infants estimated to have asthma.
*p < 0.02.
eHCF: Extensively hydrolyzed casein formula; eHWF: Extensively hydrolyzed whey formulae; LGG: Lactobacillus rhamnosus GG.
Kaplan–Meier analysis (Figure 4) showed the distribution of being symptomatic between the two groups was significantly different (Log Rank [Mantel-Cox]: p = 0.001). This difference is reflected in the significant difference in the number of drugs prescribed for symptomatic relief of CMPA and its allergic manifestations (Table 2).
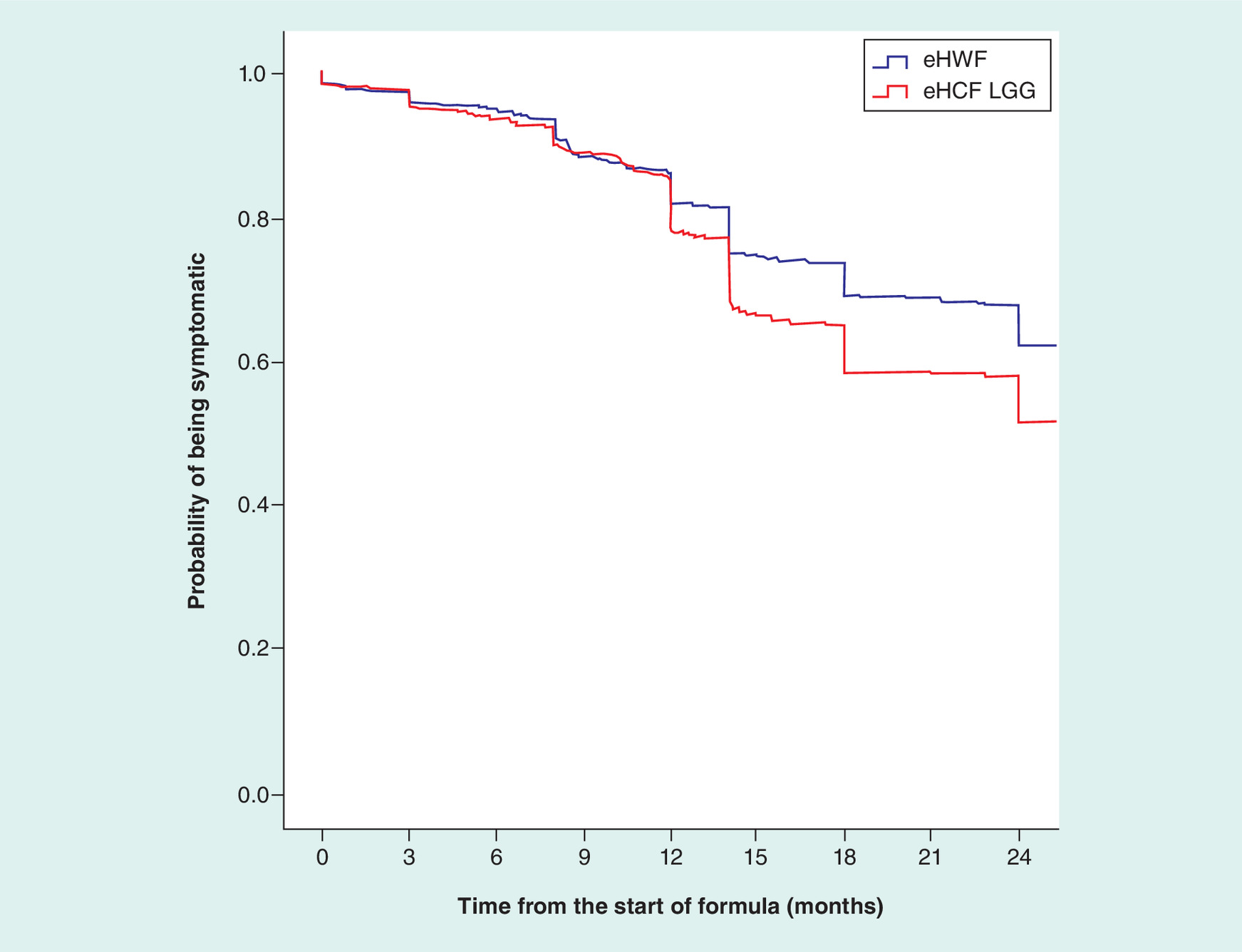
Figure 4. Kaplan–Meier analysis of the probability of being symptomatic over 24 months of follow-up (Log Rank [Mantel-Cox]: p = 0.001).
eHCF: Extensively hydrolyzed casein formula; eHWF: Extensively hydrolyzed whey formulae; LGG: Lactobacillus rhamnosus GG.
| Mean number of prescriptions per patient | p-value | ||
|---|---|---|---|
| eHCF LGG | eHWF | ||
| Oral antihistamines | 0.4 ± 1.2 | 0.7 ± 1.8 | 0.005 |
| Gastrointestinal drugs | 3.8 ± 6.4 | 4.4 ± 9.5 | <0.03 |
| Emollients, anti-infective creams and topical calcineurin inhibitors | 3.3 ± 7.2 | 6.8 ± 12.4 | <0.001 |
| Topical steroids | 1.1 ± 2.6 | 1.9 ± 5.1 | 0.005 |
| Asthma drugs | 0.9 ± 2.5 | 1.9 ± 6.4 | <0.04 |
| Inhaled antihistamines | 0.2 ± 0.2 | 0.3 ± 0.3 | ns |
eHCF: Extensively hydrolyzed casein formula; eHWF: Extensively hydrolyzed whey formulae; LGG: Lactobacillus rhamnosus GG.
Binary logistic regression showed that infants fed eHWF had a higher relative risk of being symptomatic at 24 months after starting a formula compared with those fed eHCF LGG:
•
Eczema: odds ratio (OS) 3.438 (95% CI: 1.975–5.985); p < 0.001
•
Gastrointestinal symptoms: OS 2.275 (95% CI: 1.007–5.137); p < 0.05
•
Asthma: OS 2.651 (95% CI: 1.242–5.660); p < 0.02
Additionally, infants fed eHCF LGG had a higher relative risk of being completely symptom-free at 24 months after starting a formula compared with those fed eHWF: OS 2.988 (95% CI: 1.880–4.748); p < 0.02.
Discussion
To the authors’ knowledge, this is the first study evaluating whether first-line treatment with eHCF LGG is clinically more effective than eHWF in the management of cow’s milk allergic infants in clinical practice. The basis of the analysis was the real world evidence, THIN database. The advantage of using the THIN database is that the patient pathways and clinical outcomes are based on real world evidence derived from clinical practice. Nevertheless, the analyses were based on clinicians’ entries into their patients’ records and inevitably subject to a certain amount of imprecision and lack of detail. In particular, diagnosing asthma in infants is challenging, but the margin of error in such diagnosis would apply equally to both groups. Moreover, the computerized information in the THIN database is collected by GPs and nursing teams for clinical care purposes and not for research. Prescriptions issued by GPs and practice nurses are recorded in the database, but it does not specify whether the prescriptions were dispensed or patient compliance with the product. Despite these limitations, it is the authors’ opinion that the THIN database affords one of the best sources of real world evidence for clinical practice in the UK.
The results of the present study indicate that eHCF LGG is not only more effective than eHWF in managing the symptoms of CMPA, but it also has greater potential to prevent the occurrence of other allergic manifestations. The distribution and severity of symptoms (using the incidence of reflux, faltering growth and anaphylaxis as a proxy), age and bodyweight were all similar between the two groups, and no significant differences were found. Hence, the differences in clinical outcomes cannot be attributed to any differences between the groups. Moreover, the outcomes of infants who were fed eHCF LGG were comparable with those reported in previous studies [9–11]. Additionally, there were no documented adverse reactions to either of the study formulae in the patients’ records.
The term ‘Allergic March’ has been used to describe the natural history of atopic manifestations, which are characterized by IgE-mediated responses and clinical symptoms that may appear early in life and then persist over many years [14]. While the proportion of patients with IgE-mediated CMPA in our study population is likely to be relatively small (<12% had urticaria), the estimated incidence of asthma in the whole population increased over time in parallel with a decline in the estimated percentage of patients experiencing eczema, urticaria and rhinitis. However, fewer infants, who were fed eHCF LGG, were estimated to have developed asthma or experienced these other symptoms at 24 months compared with those fed eHWF. A retrospective power calculation estimated that 435 patients per group would have been required to demonstrate the percentage of infants who were estimated as having developed asthma at 24 months (shown in Figure 3) with 80% power and a Type 1 error of 0.05. Clearly, a longer follow-up time is required to determine the incidence of asthma in this population over the long term. Nevertheless, this is supportive evidence of the potential role that eHCF LGG can play in slowing down the allergic march in infants with CMPA, and which may be due to its potential to modulate the gut microbiota [11] and produce butyrate in infants with CMPA [15]. Further research is required to fully elucidate the mechanism of action of the probiotic, LGG.
The study has several limitations. It was performed on a large cohort of 940 children in the THIN database with suspected CMPA, who were managed in the community by their family practitioner on the basis of presenting symptoms. This is how most patients are diagnosed in the community in the UK and therefore, the diagnosis of CMPA may not be secure in all cases. In particular, the differences in the percentages of infants with bloody stools and vomiting and diarrhoea between the groups suggests that the study might include infants with gastrointestinal symptoms induced by other factors [16]. Nevertheless, there is an increased risk of functional gastrointestinal disorders among infants with CMPA which could be reduced among those fed with eHCF LGG [17]. Consequently, this study’s findings have been derived from actual cases and perceived cases of CMPA. Notwithstanding this, the effect sizes are clinically relevant and a retrospective power calculation estimated that only 272 patients per group would have been required to demonstrate the percentage of infants successfully treated with each formula at 24 months (shown in Figure 1A) with 95% power and a Type 1 error of 0.05. A longer follow-up time is required to test whether this effect persists over the long term.
The THIN database comprises the electronic records of patients who were managed in clinical practice; hence, the analysis does not consider the suitability of infants to receive their respective formula. Furthermore, the THIN database may have under-recorded or miscoded some outcomes in some instances, and the outcomes of infants were excluded once they switched from their initial formula. Additionally, the analysis was truncated at 24 months and does not consider the potential impact of symptomatic infants beyond the study period.
In summary, using real world evidence, the findings from this study indicate a difference in clinical effectiveness between eHCF LGG and eHWF. However, this study does not prove efficacy and a controlled study is required to compare eHCF LGG with eHWF in order to validate the outcomes of this analysis.
Within the study’s limitations, first-line management of newly diagnosed cow’s milk allergic infants with eHCF LGG appears to afford a significantly more clinically effective formula than eHWF, and may slow down the allergic march seen in cow’s milk allergic children.
•
This is the first study to evaluate the patient pathways and associated clinical outcomes, attributable to managing cow’s milk allergic infants over 24 months from the onset of community management in the UK.
•
This study was undertaken using real world evidence derived from the anonymized records of a sample of infants in The Health Improvement Network database (a nationally representative database of clinical practice among >11 million patients registered with general practitioners in the UK).
•
There were no significant differences in duration between initial presentation and starting a formula and in the distribution of presenting symptoms between the two groups.
•
Significantly more extensively hydrolyzed casein formula (eHCF) lactobacillus rhamnosus GG (LGG)-fed infants remained on their initial formula than extensively hydrolyzed whey formulae (eHWF)-fed infants (76 vs 69%; p < 0.02). Additionally, eHCF LGG-fed infants continued feeding with their initial formula for a significantly shorter duration than eHWF-fed infants (8.3 vs 10.2 months; p = 0.001).
•
At 24 months after starting a formula, 77% of eHCF LGG-fed infants were estimated to have been successfully managed compared with 63% of eHWF-fed infants (p < 0.001) and significantly more eHWF-fed infants were estimated to be experiencing gastrointestinal symptoms, eczema and asthma (7.1 vs 3.1%; p < 0.02).
•
The analysis does not consider the potential impact of patients who remained symptomatic beyond 24 months following initial presentation.
•
First-line management of newly diagnosed cow’s milk allergic infants with eHCF LGG appears to afford a significantly more clinically effective formula than eHWF, and it may slow down the allergic march seen in cow’s milk allergic children.
Financial & competing interests disclosure
This analysis was funded by Mead Johnson Nutrition, Warsaw, Poland. The study’s sponsors had no involvement in the study design, the collection, analysis and interpretation of the data, the writing of this manuscript and the decision to submit this article for publication. The views expressed in this article are those of the authors and not necessarily those of the sponsor. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Fiocchi A, Dahdah L, Albarini M, Martelli A. Cow's milk allergy in children and adults. Chem. Immunol. Allergy 101, 114–123 (2015).
2.
Sicherer SH. Epidemiology of food allergy. J. Allergy Clin. Immunol. 127(3), 594–602 (2011).
3.
Niggemann B, Von Berg A, Bollrath C et al. Safety and efficacy of a new extensively hydrolyzed formula for infants with cow's milk protein allergy. Pediatr. Allergy Immunol. 19(4), 348–354 (2008).
4.
Vandenplas Y, Marchand J, Meyns L. Symptoms, diagnosis, and treatment of cow's milk allergy. Curr. Pediatr. Rev. 11(4), 293–297 (2015).
5.
Ludman S, Shah N, Fox AT. Managing cows' milk allergy in children. BMJ 347, f5424 (2013).
6.
Cantani A, Micera M. Immunogenicity of hydrolysate formulas in children (part 1). Analysis of 202 reactions. J. Investig. Allergol. Clin. Immunol. 10(5), 261–276 (2000).
7.
Luyt D, Ball H, Makwana N et al. BSACI guideline for the diagnosis and management of cow's milk allergy. Clin. Exp. Allergy 44(5), 642–672 (2014).
8.
Berni Canani R, Nocerino R, Terrin G et al. Effect of Lactobacillus GG on tolerance acquisition in infants with cow's milk allergy: a randomized trial. J. Allergy Clin. Immunol. 129(2), 580–582 (2012).
9.
Berni Canani R, Nocerino R, Terrin G et al. Formula selection for management of children with cow's milk allergy influences the rate of acquisition of tolerance: a prospective multicenter study. J. Pediatr. 163(3), 771–777 (2013).
10.
Ovcinnikova O, Panca M, Guest JF. Cost-effectiveness of using an extensively hydrolyzed casein formula plus the probiotic Lactobacillus rhamnosus GG compared to an extensively hydrolyzed formula alone or an amino acid formula as first-line dietary management for cow's milk allergy in the US. Clinicoecon. Outcomes Res. 7, 145–152 (2015).
11.
Berni Canani R, Di Costanzo M, Bedogni G et al. Extensively hydrolyzed casein formula containing Lactobacillus rhamnosus GG reduces the occurrence of other allergic manifestations in children with cow's milk allergy: 3-year randomized controlled trial. J. Allergy Clin. Immunol. 139(6), 1906–1913.e4 (2017).
12.
Blak BT, Thompson M, Dattani H, Bourke A. Generalisability of The Health Improvement Network (THIN) database: demographics, chronic disease prevalence and mortality rates. Inform. Prim. Care 19(4), 251–255 (2011).
13.
Guest JF, Ayoub N, Mcilwraith T et al. Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5(12), e009283 (2015).
14.
15.
Berni Canani R, Sangwan N, Stefka AT et al. Lactobacillus rhamnosus GG-supplemented formula expands butyrate-producing bacterial strains in food allergic infants. ISME J. 10(3), 742–750 (2016).
16.
Arvola T, Ruuska T, Keranen J, Hyoty H, Salminen S, Isolauri E. Rectal bleeding in infancy: clinical, allergological, and microbiological examination. Pediatrics 117(4), e760–e768 (2006).
17.
Nocerino R, Di Costanzo M, Bedogni G et al. Dietary treatment with extensively hydrolyzed casein formula containing the probiotic Lactobacillus rhamnosus GG prevents the occurrence of functional gastrointestinal disorders in children with cow's milk allergy. J. Pediatr.(2019). (Epub ahead of print).
Information & Authors
Information
Published In
Pages: 1317 - 1326
PubMed: 31526139
Copyright
© 2019 Julian Guest. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 5 July 2019
Accepted: 12 August 2019
Published online: 17 September 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Effectiveness of using an extensively hydrolyzed casein formula supplemented with Lactobacillus rhamnosus GG compared with an extensively hydrolysed whey formula in managing cow’s milk protein allergic infants. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0088
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Zihan Wen, Zhenzhen Zhang, Xiaojing Li, Zhenxing Qiang, Hui Wang, Qiuying Wang, Junying Zhao, Wenxiao Feng, Jingjing Peng, Ling Guo, Lijun Chen, Probiotics in the alleviation of food allergies in infants and young children: research progress, Critical Reviews in Food Science and Nutrition, 10.1080/10408398.2026.2669053, (1-20), (2026).
- Manish Kumar, Shivani Nalla, Jatindra N. Tripathy, Akhilesh Kumar Shakya, Bioengineering Interventions to Enhance the Capacity of the Gut Microbiota in Controlling Food Allergies, Life, 10.3390/life16030433, 16, 3, (433), (2026).
- Gang Yu, Qiaozhi Zhang, Lan Zhao, Ronald van Ree, Linglin Fu, Risk and protective factors for food allergy: an in-depth analysis of dietary patterns and specific dietary components, Allergy Medicine, 10.1016/j.allmed.2025.100076, 6, (100076), (2025).
- Rita Nocerino, Giorgio Bedogni, Laura Carucci, Greta Aquilone, Franca Oglio, Serena Coppola, Antonio Masino, Roberto Berni Canani, Long term impact of formula choice in children with cow milk protein allergy: 6-year follow-up of the Atopic March Cohort Study, Clinical Nutrition, 10.1016/j.clnu.2025.03.026, 48, (134-143), (2025).
- Laura Quintieri, Anna Luparelli, Leonardo Caputo, William Schirinzi, Federica De Bellis, Leonardo Smiriglia, Linda Monaci, Unraveling the Biological Properties of Whey Peptides and Their Role as Emerging Therapeutics in Immune Tolerance, Nutrients, 10.3390/nu17060938, 17, 6, (938), (2025).
- Rita Nocerino, Laura Carucci, Serena Coppola, Franca Oglio, Antonio Masino, Alessandra Agizza, Lorella Paparo, Roberto Berni Canani, The journey toward disease modification in cow milk protein allergy, Immunological Reviews, 10.1111/imr.13372, 326, 1, (191-202), (2024).
- Mao Lin, Cong Yanjun, Research progress on the mechanism of probiotics regulating cow milk allergy in early childhood and its application in hypoallergenic infant formula, Frontiers in Nutrition, 10.3389/fnut.2024.1254979, 11, (2024).
- Margherita Di Costanzo, Adriana Vella, Claudia Infantino, Riccardo Morini, Simone Bruni, Susanna Esposito, Giacomo Biasucci, Probiotics in Infancy and Childhood for Food Allergy Prevention and Treatment, Nutrients, 10.3390/nu16020297, 16, 2, (297), (2024).
- Mengyao Qian, Wei Liu, Xueying Feng, Zhaochuan Yang, Xiaomei Liu, Liang Ma, Yanchun Shan, Ni Ran, Mingji Yi, Changlong Wei, Chenyang Lu, Yanxia Wang, Alterations in the gut microbiota of toddlers with cow milk protein allergy treated with a partially hydrolyzed formula containing synbiotics: A nonrandomized controlled interventional study, Food Science & Nutrition, 10.1002/fsn3.3801, 12, 2, (765-775), (2023).
- Ludovica Cela, Giulia Brindisi, Alessandro Gravina, Francesca Pastore, Antonio Semeraro, Ivana Bringheli, Lavinia Marchetti, Rebecca Morelli, Bianca Cinicola, Martina Capponi, Alessandra Gori, Elia Pignataro, Maria Grazia Piccioni, Anna Maria Zicari, Caterina Anania, Molecular Mechanism and Clinical Effects of Probiotics in the Management of Cow’s Milk Protein Allergy, International Journal of Molecular Sciences, 10.3390/ijms24129781, 24, 12, (9781), (2023).