Comparative effectiveness of first-line nab-paclitaxel versus paclitaxel monotherapy in triple-negative breast cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This observational study evaluated the effectiveness of nab-paclitaxel versus paclitaxel monotherapy as first-line (1L) treatment for metastatic triple-negative breast cancer (mTNBC). Materials & methods: 200 patients from the US Flatiron Health electronic health record-derived database (mTNBC diagnosis, January 2011–October 2016) who received 1L nab-paclitaxel (n = 105) or paclitaxel (n = 95) monotherapy were included. Overall survival and time to next treatment were evaluated. Results: The adjusted overall survival hazard ratio was 0.98 (95% CI: 0.67–1.44), indicating a similar risk of death between groups. Adjusted time to next treatment hazard ratio was 0.89 (95% confidence interval: 0.62–1.29). Conclusion: Nab-paclitaxel and paclitaxel monotherapy showed similar efficacy, suggesting their interchangeability as 1L treatments for mTNBC.
Triple-negative breast cancer (TNBC) is a subtype of breast cancer characterized by the lack of expression of estrogen and progesterone receptors (ER and PR) and no amplification of the gene encoding HER2. TNBC represents approximately 15–20% of breast cancer cases and has the poorest prognosis of breast cancer subtypes [1]. Published median overall survival (OS) estimates for metastatic (m)TNBC range from 7 to 18 months, depending on study design and patient population [2–6]. Approved targeted agents that can be used for mTNBC, such as bevacizumab or PARP inhibitors, have not demonstrated definitive OS benefit for patients with mTNBC [7,8], while checkpoint inhibitor therapy in combination with chemotherapy has shown promise [9,10]. As a result, the standard of care for patients with mTNBC has historically been chemotherapy. Taxanes, including paclitaxel, nab-paclitaxel and docetaxel, have been shown to be efficacious for the treatment of TNBC and are commonly used in first-line (1L) treatment of metastatic disease [11–13]. In March 2019, atezolizumab plus nab-paclitaxel was granted accelerated approval by the US FDA for the treatment of PD-L1–positive locally advanced or mTNBC [10].
Nab-paclitaxel, an albumin-bound formulation of paclitaxel, was developed to address the toxicity issues related to the solvents used for both paclitaxel and docetaxel [13] and to potentially improve the therapeutic index. Based on results from head-to-head Phase II and III trials, nab-paclitaxel received approval for treatment of HER2-negative metastatic breast cancer (mBC) in Europe and the USA [13–15]. To date, however, few studies have directly compared the effectiveness of nab-paclitaxel and paclitaxel as monotherapies in the way they are used in routine clinical practice, which includes a broader patient population than what is included in clinical trials. Furthermore, the 1L-treated patients with mTNBC are rarely evaluated separately from the broader HER2-negative population, and thus, information on the effectiveness of these two drugs in this specific population is largely lacking. In a recent study by Mahtani et al., patients with HER2-negative mBC treated with nab-paclitaxel in the first or second-line (2L) had significantly longer time to treatment discontinuation and time to next treatment (TTNT) than patients treated with paclitaxel [11]. However, in a subgroup analysis among the mTNBC population, the clinical effectiveness of the two taxanes appeared similar (median 1L/2L TTNT, 6.2 vs 5.4 months, respectively; adjusted p = 0.7323). The current study aimed to further evaluate the mTNBC population, comparing the effectiveness of 1L nab-paclitaxel with paclitaxel monotherapy in patients treated in routine US clinical practice.
Materials & methods
Data source
This retrospective, observational study used the Flatiron Health electronic health record (EHR)-derived database, which comprises longitudinal, demographically and geographically diverse EHR data from across the USA from over 265 cancer clinics (approximately 800 sites of care) that include more than 2 million active records for patients with cancer. The patient-level data in EHRs include structured data (e.g., laboratory values and prescribed drugs) in addition to unstructured data collected via technology-enabled chart abstraction from physician’s notes and other unstructured documents (e.g., biomarker reports, physician notes, pathology reports).
Cohort identification
The following criteria were used to identify patients (Figure 1) for inclusion in a broad cohort, from which the analytic cohort was drawn: confirmed diagnosis of mBC on or after 1 January 2011, ≥18 years of age at metastatic diagnosis, ≥2 Flatiron network clinic visits on or after 1 January 2011, ≥1 negative result for ER and PR and ≥1 negative or equivocal result for HER2 in the patient’s record, and confirmed treatment with nab-paclitaxel or paclitaxel monotherapy in the 1L setting.

Figure 1. Analytic cohort selection.
Flowchart for the broad and analytic cohort selection is displayed.
†Described in methods section.
‡Windows to identify negative tests for all three biomarkers (ER, PR, HER2) were defined (see methods section).
§A patient was considered to have received monotherapy if there was no evidence of other anticancer agents (using order and administration records) within the first 30 days following their index treatment, except if the patient received another taxane during this time (in which case, patients were considered to have switched treatments and were classified based on the first treatment received).
¶14 patients switched treatments from paclitaxel to nab-paclitaxel and were classified based on the first treatment received.
EHR: Electronic health record; ER: Estrogen receptor; ICD: International Classification of Disease; mBC: Metastatic breast cancer; mTNBC: Metastatic triple-negative breast cancer; nab-pac: Nab-paclitaxel; pac: Paclitaxel; PR: Progesterone receptor.
In order to ensure proper classification of 1L treatment, patients were excluded if there was a gap of >90 days between their confirmed metastatic diagnosis date and the date of their first structured activity in the EHR, if there was evidence of other concurrent active cancers within the 3 years prior to the date of metastatic diagnosis, if they received prior hormonal therapies (as defined by the presence of at least two orders for the same hormonal therapy drug in the patient’s record), or if they did not receive taxane monotherapy for 1L treatment. Patients meeting both the criteria of receiving taxanes for ≤90 days and taxane treatment within 60 days of receiving combination chemotherapy, were excluded, as this treatment pattern is more consistent with adjuvant taxane treatment or possible 2L treatment.
Further criteria were used to define the analytic cohort for this study. Patients were included if their metastatic diagnosis date was between 1 January 2011 and 31 October 2016, and if they received ≥1 administration of nab-paclitaxel or paclitaxel within 90 days of their diagnosis date. For a patient’s cancer to be considered mTNBC, a patient had to have a specimen collected, a negative test result for ER and PR and a negative or equivocal result for HER2 within 60 days of the diagnosis of metastatic disease. If the patient did not have a biomarker specimen collected within this time frame, biomarker results from their initial breast cancer diagnosis were used. Patients were followed up until death, loss to follow-up or study end date (30 June 2017), whichever occurred first.
Institutional review board approval of the study protocol was obtained prior to study conduct and included a waiver of informed consent. Data provided to third parties were de-identified, and provisions were in place to prevent re-identification in order to protect patients’ confidentiality.
Treatment, line-of-therapy & variable definitions
To identify 1L monotherapy treatment, the date of the first administration of nab-paclitaxel or paclitaxel was considered the index treatment date. A patient was considered to have received monotherapy if there was no evidence of other anticancer agents (using order and administration records) within the first 30 days following their index treatment, except if the patient received another taxane during this time (in which case, patients were considered to have switched treatments and were classified based on the first treatment received). The end of 1L treatment was defined as any addition of a new anticancer agent or switch to another therapy that occurred more than 30 days after the patient’s index treatment date.
The relative dose (mg/m2) documented on a patient’s medication order was used to determine which dose of taxane they had received. If a patient’s relative dose information was missing, the dose for the first administration and a patient’s closest height and weight information (obtained any time prior to or after the start of 1L therapy or first dose received) were used to calculate a relative dose. The schedule of taxane was based on the ordered relative dose (when available) or calculated relative dose (when not) and were classified as either weekly (80 and 90 mg/m2 for paclitaxel; 100, 125 and 150 mg/m2 for nab-paclitaxel) or every 3 weeks (q3w; 175 and 260 mg/m2 for paclitaxel and nab-paclitaxel, respectively). If a patient’s ordered or calculated relative dose did not fall into these categories, we classified the patient as having received another dose or having received a dose reduction based on the dose received.
Covariates included variables from structured and unstructured data. Eastern Cooperative Group (ECOG) performance status, insurance status, race, sex and practice type were determined using the structured data from the EHR. The ECOG performance status assessment that occurred closest and prior to the start of 1L treatment was used. For a patient’s primary payer, we used the insurance payer that had a start date prior to and overlapping with the diagnosis of metastatic disease. If a patient had more than one payer that met the criteria, the following hierarchy was used to classify a patient: commercial health plan > Medicare > Medicaid > other government plan > patient assistance program > workers compensation > self pay.
Other covariates were abstracted from unstructured data using Flatiron’s technology-enabled platform. A patient was considered to have had a diagnosis of metastasis to a given site (bone, lung, liver, brain/central nervous system, distant lymph nodes, other) if their abstracted date of diagnosis (to a given site) occurred during the same month as their metastatic diagnosis (only month and year for each site provided in data set). Evidence of treatment of bone metastases (administration of denosumab or zoledronic acid during 1L treatment) and the abstracted diagnosis were included to determine whether a patient had metastases to the bone. Each independent site of metastasis was used as a separate incident; therefore, a patient could have >1 site of metastasis. The number of metastatic sites was the sum of all incidences of metastatic sites identified in the patient’s record. Visceral disease was defined as disease with lung, liver or brain metastases and classified as ‘yes’ or ‘no’.
A patient was considered to have a diagnosis of prior neuropathy if a physician’s note explicitly mentioned neuropathy or paresthesia (symptom description was not sufficient to indicate neuropathy diagnosis) prior to the start of 1L therapy. This could include episodic and/or chronic instances. Treatment-free interval (TFI) was defined as the duration of time between the end of premetastatic therapy (including systemic therapy, surgery and radiation) and the date of metastatic disease diagnosis. Information from both the structured and unstructured parts of the EHR were used to determine whether a patient used any taxane (paclitaxel, nab-paclitaxel or docetaxel) during their premetastatic treatment, including adjuvant or neoadjuvant treatment of early-stage breast cancer.
The individual components of the Charlson Comorbidity Index (CCI) [16,17], with the exception of metastatic cancer, were abstracted for each patient. A patient was considered to have a diagnosis of a given comorbidity if there was documentation of the diagnosis any time prior to the patient’s metastatic diagnosis date, inclusive. A modified CCI score was created for each patient as previously described [16].
Outcomes & statistical analyses
In this study, OS was evaluated as the primary outcome, and TTNT was evaluated as a secondary outcome. For each cohort, OS was calculated from the initiation of 1L treatment with paclitaxel or nab-paclitaxel to death from any cause. The exact date of death was determined for each patient. Patients without a death date were censored at the latest available drug administration date or visit date (lab, office, radiology, treatment or nonfacility visits) that occurred on or before the study end date (30 June 2017). TTNT was defined as the time from the initiation of 1L treatment with paclitaxel or nab-paclitaxel until either the day before the start of 2L treatment, for patients with evidence of 2L treatment in the Flatiron network, or death if the death occurred within 45 days following the patient’s last administration of 1L treatment. If a patient did not have evidence of 2L treatment in the Flatiron network and did not die within the 45 days following the last 1L administration, the patient was censored at the latest available date that occurred on or before the end of study date of either drug administration plus the number of days in a treatment cycle (+7 or +21 days for weekly and q3w regimens, respectively) or visit date. Patient demographics and clinical characteristics at baseline were described using frequency distributions. We used χ2 tests of independence and Kruskal–Wallis tests to assess differences between the two patient groups (paclitaxel or nab-paclitaxel treatment) for categorical and continuous variables.
Time-to-event Kaplan–Meier analyses were used to estimate median survival and TTNT and corresponding 95% confidence intervals (CIs). Log-rank tests were used to compare differences between treatment groups for each end point. Cox proportional hazards models were used to determine the association of treatment choice with outcomes (OS and TTNT), adjusting for key prognostic variables. The following variables were included in the model: age at treatment initiation, stage at initial diagnosis, race, TFI, ECOG performance status at 1L initiation, visceral disease, prior taxane use, prior neuropathy, number of metastatic sites, insurance status and CCI. Adjusted hazard ratios (HRs) and corresponding 95% CIs were reported.
The primary analysis for this study was the evaluation of all patients who met the criteria outlined above. Additional sensitivity analyses were conducted to test the robustness of the models: analysis of the intent-to-treat population, defined as patients who received 80 mg/m2 of paclitaxel or 100 mg/m2 of nab-paclitaxel based on ordered dose when available, or calculated dose when not; analysis of a dose-administered population, defined as patients who received 80 mg/m2 of paclitaxel or 100 mg/m2 of nab-paclitaxel according to EHR administration records (not including the information from orders); analysis of patients in the overall population with a TFI >12 months; propensity score analyses using inverse probability treatment weights with various top/bottom trimming thresholds (1, 2.5 and 5%) and propensity score matching [18,19] as alternative methods to adjust for confounding factors and analysis of TTNT using a longer window in which death was considered an event: 60 days from the last administration of a taxane in 1L.
Results
Patient & treatment characteristics
Of the 344,460 potentially eligible patients with breast cancer in the Flatiron network, 200 met all study criteria and were included in the current mTNBC analysis (Figure 1): 105 who received nab-paclitaxel monotherapy and 95 who received paclitaxel monotherapy for 1L treatment (Figure 1). 14 patients who were classified as receiving paclitaxel subsequently switched to nab-paclitaxel during 1L, whereas there were no patients who were classified as receiving nab-paclitaxel for 1L treatment who subsequently switched to paclitaxel. The majority of patients in the study (>95%) were treated in community practice (data not shown). Compared with patients who received paclitaxel, those who received nab-paclitaxel were more likely to have earlier stage disease at initial diagnosis and have recurrent disease; among those with recurrent disease, patients who received nab-paclitaxel were more likely to have a TFI from adjuvant to metastatic disease of ≤12 months, have received a taxane in adjuvant treatment and have a prior diagnosis of neuropathy (Table 1). Other characteristics were balanced between groups.
| nab-Paclitaxel (n = 105) | Paclitaxel (n = 95) | p-value | |
|---|---|---|---|
| Age at 1L initiation, median (IQR), years | 66 (53–73) | 65 (58–75) | 0.22 |
| – <55, n (%) | 28 (26.7) | 19 (20.0) | |
| – 55–64, n (%) | 22 (21.0) | 25 (26.3) | 0.21 |
| – 65–74, n (%) | 38 (36.2) | 27 (28.4) | |
| – ≥75, n (%) | 17 (16.2) | 24 (25.3) | |
| Year of diagnosis of metastatic disease, n (%) | |||
| – 2011 | 17 (16.2) | 10 (10.5) | |
| – 2012 | 15 (14.3) | 9 (9.5) | |
| – 2013 | 14 (13.3) | 17 (17.9) | 0.43 |
| – 2014 | 17 (16.2) | 23 (24.2) | |
| – 2015 | 18 (17.1) | 18 (19.0) | |
| – 2016 | 24 (22.9) | 18 (19.0) | |
| Stage at diagnosis, n (%) | |||
| – I | 9 (8.6) | 13 (13.7) | |
| – II | 28 (26.7) | 18 (19.0) | 0.001 |
| – III | 31 (29.5) | 10 (10.5) | |
| – IV | 28 (26.7) | 48 (50.5) | |
| – Unknown | 9 (8.6) | 6 (6.3) | |
| Recurrent vs de novo, n (%) | |||
| – Recurrent | 77 (73.3) | 46 (48.4) | |
| – TFI ≤12 months | 32 (41.6)† | 11 (23.9)† | <0.001‡ |
| – TFI >12 months | 43 (55.8)† | 33 (71.7)† | |
| – De novo, n (%) | 28 (26.7) | 49 (51.6) | |
| Race/ethnicity, n (%) | |||
| – White | 67 (63.8) | 57 (60.0) | |
| – African–American | 15 (14.3) | 18 (19.0) | |
| – Other | 13 (12.4) | 10 (10.5) | 0.81 |
| – Missing | 10 (9.5) | 10 (10.5) | |
| Insurance status, n (%) | |||
| – Commercial | 52 (49.5) | 36 (37.9) | |
| – Medicare | 13 (12.4) | 14 (14.7) | 0.43 |
| – Other | 10 (9.5) | 11 (11.6) | |
| – Missing/unknown | 30 (28.6) | 34 (35.8) | |
| ECOG at/prior to 1L treatment initiation, n (%) | |||
| – 0 | 26 (24.8) | 19 (20.0) | |
| – 1 | 20 (19.1) | 20 (21.1) | 0.46§ |
| ≥– 2 | 6 (5.7) | <4 (<4)§ | |
| –Missing | 53 (50.5) | >50 (>53.0)§ | |
| Site of metastases, n (%) ¶ | |||
| – Bone | 49 (46.7) | 54 (56.8) | 0.15 |
| – Liver | 25 (23.8) | 22 (23.2) | 0.91 |
| – Lung | 61 (58.1) | 54 (56.8) | 0.86 |
| – Brain/central nervous system | 7 (6.7) | 14 (14.7) | 0.06 |
| – Distant lymph node(s) | 42 (40.0) | 31 (32.6) | 0.28 |
| – Other | 13 (12.4) | 15 (15.8) | 0.49 |
| Median number of metastatic sites (IQR) | 2 (1, 2) | 2 (1, 3) | 0.58 |
| Patients with indicated number of metastatic sites, n (%) | |||
| – 1 | 44 (41.9) | 37 (39.0) | |
| – 2 | 36 (34.3) | 34 (35.8) | 0.91 |
| – ≥3 | 25 (23.8) | 24 (25.3) | |
| Visceral disease, n (%) | |||
| – Yes | 78 (74.3) | 67 (70.5) | 0.55 |
| – No | 27 (25.7) | 28 (29.5) | |
| Prior (neo) adjuvant taxane use, n (%) ¶ | |||
| – Yes | 57 (74.0)† | 18 (39.1)† | 0.0001 |
| – No/unknown | 20 (26.0)† | 28 (60.9)† | |
| Prior neuropathy, n (%) ¶ | |||
| Yes | 28 (26.7) | 12 (12.6) | |
| No/Unknown | 77 (73.3) | 83 (87.4) | 0.01 |
| Charlson comorbidities, n (%) | |||
| – Chronic pulmonary disease | 11 (10.5) | 12 (12.6) | 0.63 |
| – Congestive heart failure | 6 (5.7) | 4 (4.2) | 0.63 |
| – Diabetes (no complications) | 20 (19.1) | 20 (21.1) | 0.72 |
| – Diabetes (with complications) | <4 (<4)§ | <4 (<4)§ | 0.50 |
| – Peptic ulcer disease | <4 (<4)§ | <4 (<4)§ | 0.27 |
| – HIV/AIDS | <4 (<4)§ | 0 | 0.34 |
| – Liver disease (mild or moderate/severe) | <4 (<4)§ | <4 (<4)§ | 0.62 |
| – Dementia | 0 | <4 (<4)§ | 0.29 |
| – Peripheral vascular disease | <4 (<4)§ | <4 (<4)§ | 0.92 |
| – Paralysis | 0 | <4 (<4)§ | 0.14 |
| – Cerebrovascular disease | 5 (4.8) | 7 (7.4) | 0.44 |
| – Renal disease | 7 (6.7) | 10 (10.5) | 0.33 |
| – Myocardial infarction | 4 (3.8) | 0 | 0.05 |
| – Connective tissue disease | 6 (5.7) | <4 (<4)§ | 0.19 |
| Charlson Comorbidity Index, median (IQR) | 0 (0, 1) | 0 (0, 1) | 0.79 |
| – 0, n (%) | 80 (76.2) | 69 (72.6) | |
| – 1, n (%) | 13 (12.4) | 17 (17.9) | 0.72 |
| – 2, n (%) | 6 (5.7) | 4 (4.2) | |
| – ≥3, n (%) | 6 (5.7) | 5 (5.3) | |
†
Percentages based on patients with recurrent disease only. Percentages do not equal 100% due to rounding or patients with unknown/missing values.
‡
p-value reported tested for differences between recurrent vs de novo disease and TFI distribution; other variables evaluated (year of diagnosis, practice type, visceral disease and individual components of the Charlson Comorbidity Index) were not different between treatment groups.
§
Exact numbers were removed in order to prevent back calculation (i.e., minimize de-identification risk). p-value was calculated using all values.
¶
Patients without these characteristics or with unknown information are not included in the table.
1L: First line; ECOG: Eastern Cooperative Oncology Group; IQR: Interquartile range; mTNBC: Metastatic triple-negative breast cancer; TFI: Treatment-free interval.
The ordered dose and schedule of paclitaxel and nab-paclitaxel for patients who had this information available are presented in Table 2. Over 90% of patients treated with paclitaxel or nab-paclitaxel received weekly doses, with 80 and 100 mg/m2 being the most common doses, respectively. The median duration of 1L treatment was 98 days (95% CI: 42–153) with paclitaxel and 104 days (95% CI: 49–187) with nab-paclitaxel. Patients were followed up for a median of 8.5 months; 77% of patients died during follow-up.
| nab-Paclitaxel (n = 104) | Paclitaxel (n = 91) | |
|---|---|---|
| Dose reductions, n (%) | 7 (6.7) | 9 (9.9) |
| qw, n (%) | ||
| – 80 mg/m2 | 0 | 69 (75.8) |
| – 90 mg/m2 | 0 | 5 (5.5) |
| – 100 mg/m2 | 81 (77.9) | 0 |
| – 125 or 150 mg/m2 | 8 (7.7) | 0 |
| q3w, n (%) | ||
| – 175 mg/m2 | 0 | 8 (8.8) |
| – 260 mg/m2 | 8 (7.7) | 0 |
mTNBC: Metastatic triple-negative breast cancer; q3w: Every 3 weeks; qw: Weekly.
Overall survival & time to next treatment
The cumulative incidence of mortality after start of 1L treatment was similar in both groups, with 76.8% of paclitaxel and 77.1% of nab-paclitaxel patients dying during follow-up. Median survival was 10.8 months (95% CI: 8.1–14.2) and 11.2 months (95% CI: 7.9–12.8) in patients treated with paclitaxel and nab-paclitaxel, respectively. The comparison of OS is presented in Figure 2 (log-rank p = 0.82). After adjustment for covariates, the association of the 1L treatment and OS yielded an HR for OS of 0.98 (95% CI: 0.67–1.44).
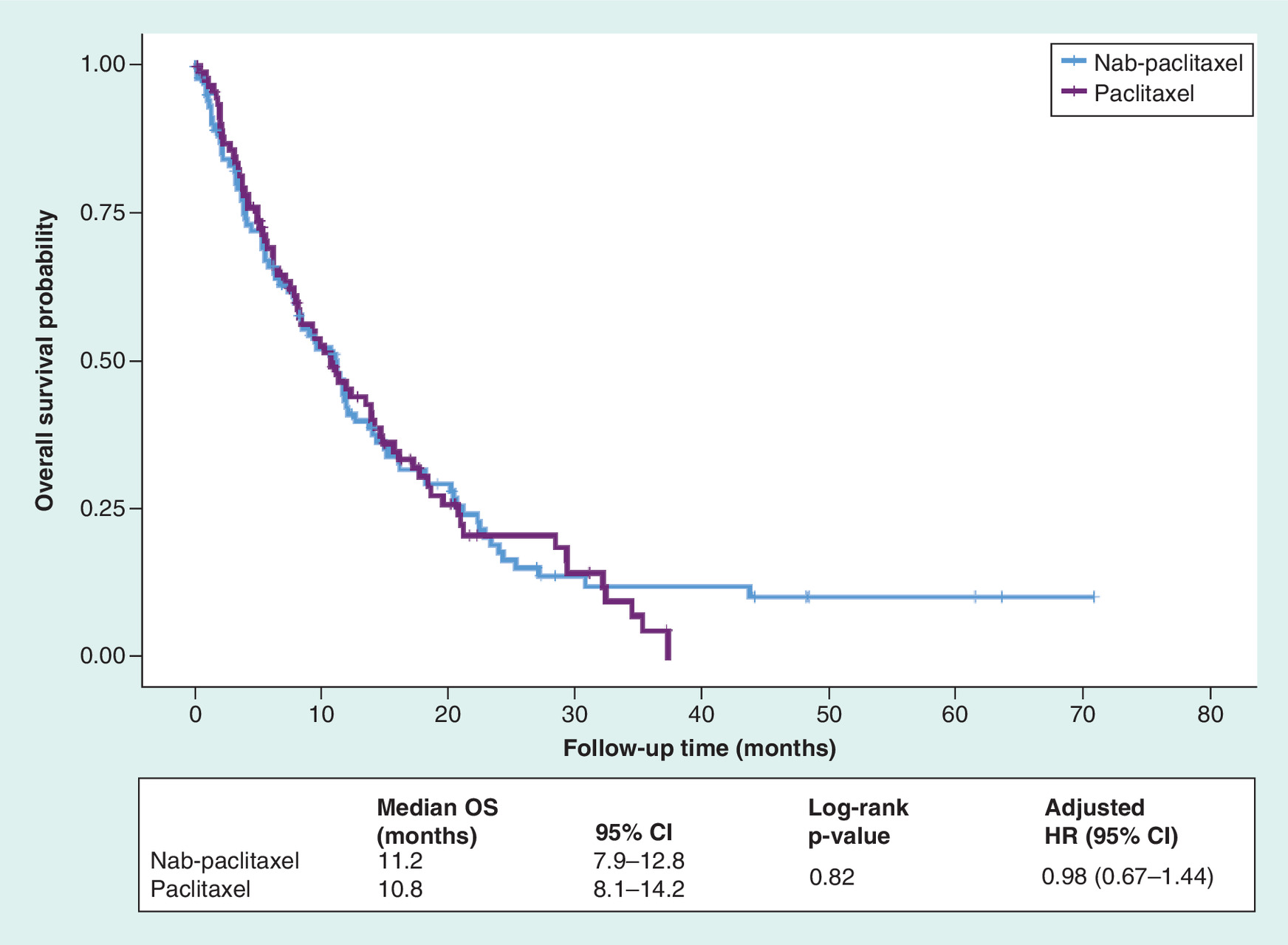
Figure 2. Kaplan–Meier curves for overall survival.
Kaplan–Meier plot of OS is plotted for patients with mTNBC treated with nab-paclitaxel versus paclitaxel. Censored patients are indicated as + marks. Median OS and Cox analyses are reported.
HR: Hazard ratio; mTNBC: Metastatic triple-negative breast cancer; OS: Overall survival.
Median TTNT was 4.3 months (95% CI: 3.4–5.4) and 4.7 months (95% CI: 3.7–6.4) for paclitaxel and nab-paclitaxel, respectively. The comparison of TTNT is presented in Figure 3 (log-rank p = 0.44). After adjustment for differences in baseline characteristics, the HR for TTNT was 0.89 (95% CI: 0.62–1.29).
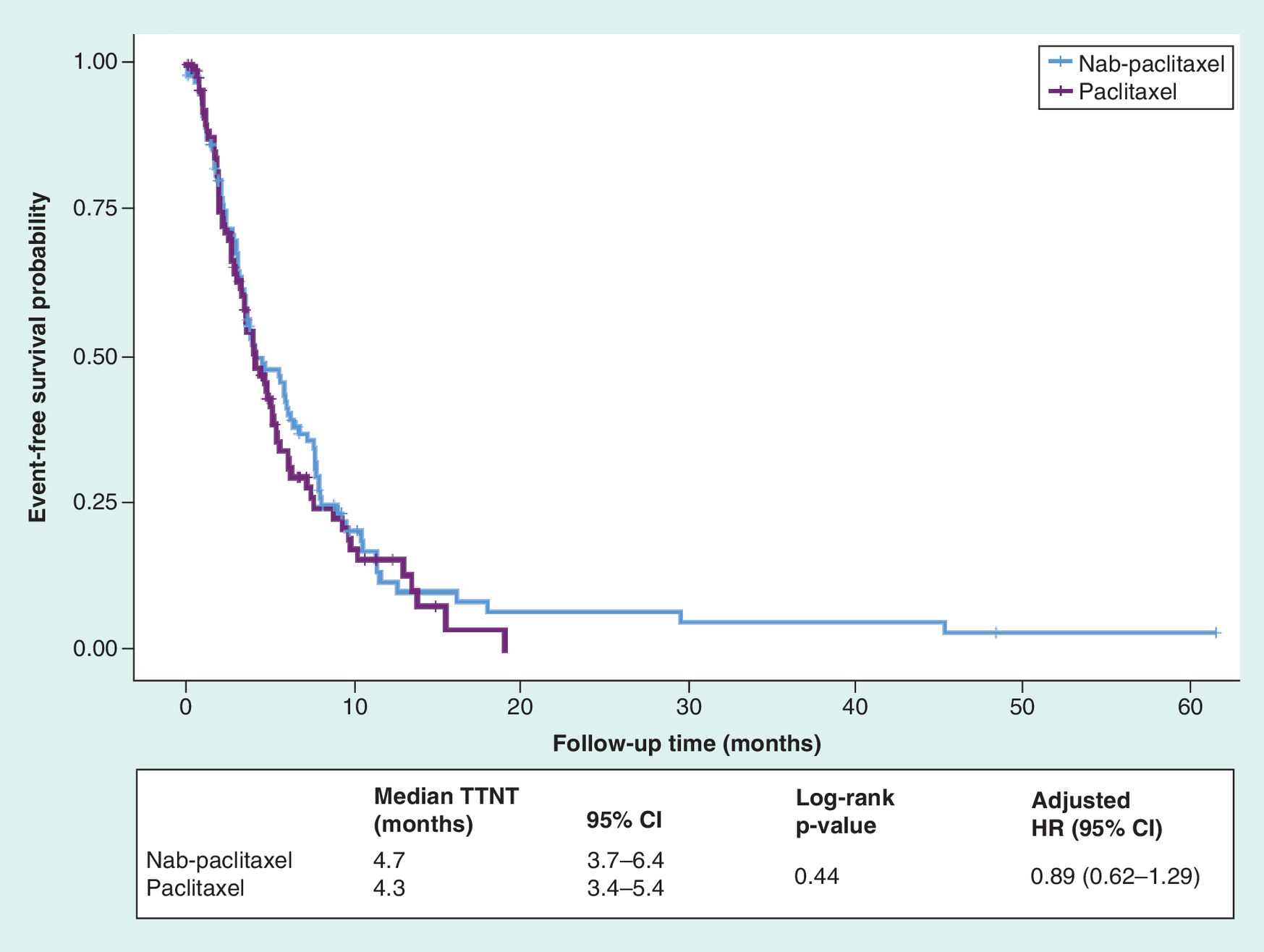
Figure 3. Kaplan–Meier curves for time to next treatment.
Kaplan–Meier plot of TTNT is plotted for patients with mTNBC treated with nab-paclitaxel versus paclitaxel. Censored patients are indicated as + marks. Median TTNT durations and Cox analyses are reported.
HR: Hazard ratio; mTNBC: Metastatic triple-negative breast cancer; TTNT: Time to next treatment.
The estimates observed from the primary analysis of all patients meeting the inclusion criteria for the study were consistent across a number of sensitivity analyses (Figure 4). These included propensity score adjustments and restricting the patient population by either the dose ordered by the physician or the dose received.
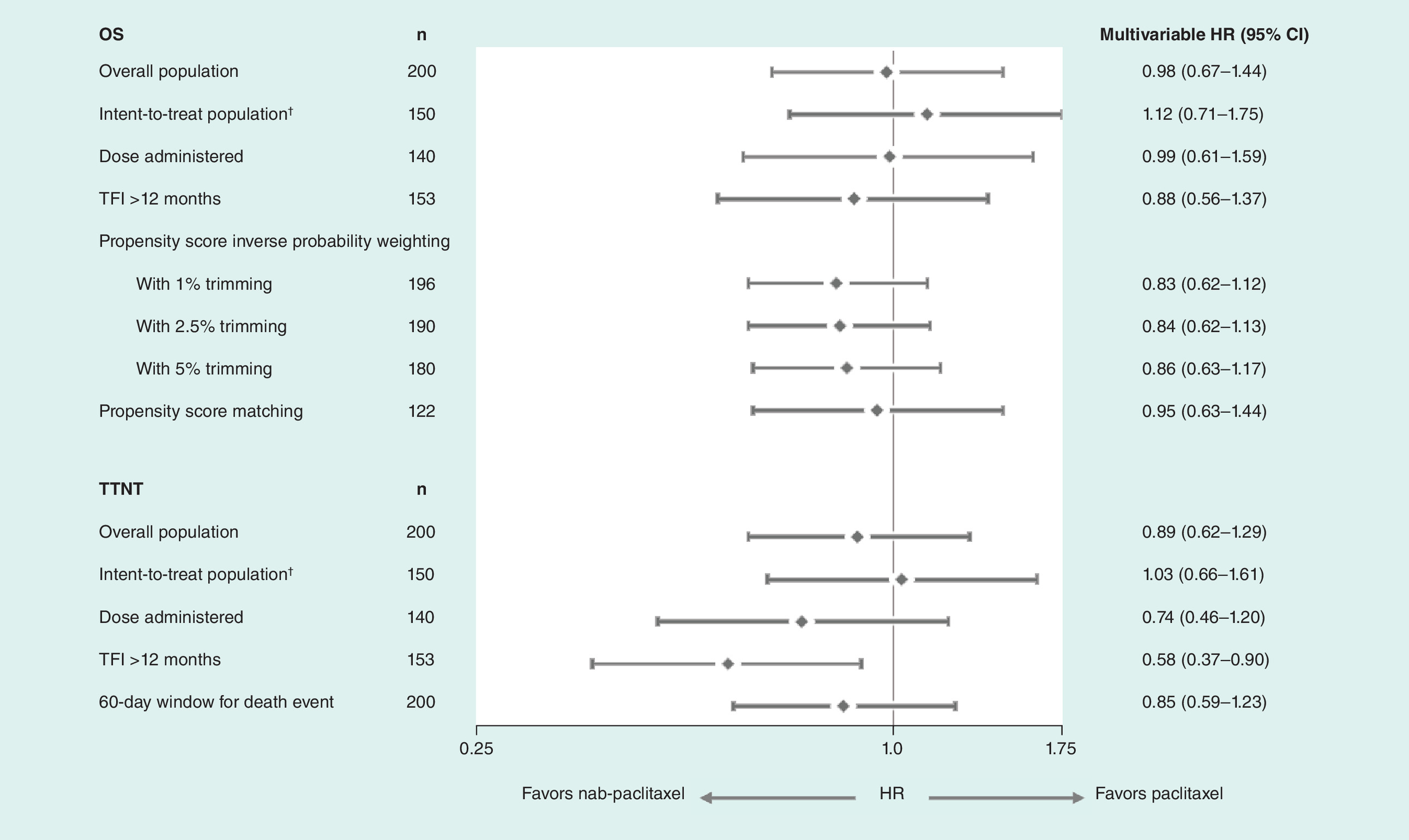
Figure 4. Sensitivity and subgroup analyses for overall survival and time to next treatment.
Forest plot including sensitivity and subgroup analyses is displayed. Error bars denote 95% CIs. In the intent-to-treat population, if a patient did not have an ordered dose available, the first administered dose in the first line setting was used to calculate the relative dose received. Correlation analyses showed that there was a high concordance of ordered dose with first administered dose in patients with both values available (data not shown).
CI: Confidence interval; HR: Hazard ratio; OS: Overall survival; TFI: Treatment-free interval; TTNT: Time to next treatment.
Discussion
This real-world comparative effectiveness study evaluated outcomes in patients with mTNBC treated with 1L nab-paclitaxel or paclitaxel monotherapy in routine clinical practice. Patients in this study most commonly received weekly dosing schedules for either taxane. After accounting for differences in prognostic factors, we found that patients treated with nab-paclitaxel had OS and TTNT similar to patients treated with paclitaxel.
As expected for a study in the real-world setting lacking the randomization of clinical trials, some differences were observed in patient characteristics and prognostic factors between the two groups (Table 1). Patients who received nab-paclitaxel were more likely to have recurrent disease, a TFI from adjuvant therapy of ≤12 months, prior taxane use and prior neuropathy compared with patients who received paclitaxel. These differences are consistent with clinical expectations as they relate to the efficacy of nab-paclitaxel after exposure to paclitaxel [20]. These differences in patient population did not appear to affect the results, as both univariate and multivariate analyses did not reveal a difference in outcomes with nab-paclitaxel versus paclitaxel. Other important prognostic factors such as ECOG performance score at 1L treatment initiation, age at 1L treatment initiation and site of metastases involved at 1L treatment did not differ between the groups.
Nab-paclitaxel and paclitaxel prescribing information does not include weekly schedules for breast cancer [14,21]; however, data from randomized studies have indicated that weekly schedules may result in better response rates, time to progression and OS than q3w schedules in patients with mBC [22]. These data have driven clinical practice to trend toward the use of weekly schedules for nab-paclitaxel and paclitaxel, as evidenced by National Comprehensive Cancer Network guidelines and other clinical data suggesting weekly dosing regimens [23]. In this study, the majority of patients (>90%) received weekly dosing regimens of paclitaxel or nab-paclitaxel, which is consistent with previous literature evaluating real-world use of taxanes [11,24]. We did observe that some patients in both treatment arms received dose reductions; however, because information on adverse events was not collected and the sample size of patients with reductions was limited (less than ten patients per arm), we were unable to evaluate the potential reasons for these reductions.
The OS in patients in this study was approximately 11 months and was similar in both treatment arms in the adjusted multivariate models and across a number of sensitivity analyses (Figure 4). This estimate was lower than what has been reported in other literature [2–6,9]; however, several factors could contribute to the difference. For example, the median age at metastatic diagnosis in this study was 65 years, which is older than what has been reported for other populations of patients with mTNBC [2,4,5,9,11,25]. In addition, data from the study were primarily from community-based practices, which could result in a biased sample because patients seen at academic centers or who enroll in clinical trials may be younger or fitter [26–29].
In observational studies, TTNT is commonly used as a proxy for progression-free survival or time to progression [30,31]. In this study, TTNT included deaths that occurred close to the last administration of a taxane to be a better representation of progression-free survival. It is important to note, however, that TTNT includes reasons other than progression for advancing a treatment sequence – namely toxicity and tolerability issues, physician or patient preference and potential insurance coverage changes. The results from this study suggest that patients treated with nab-paclitaxel have a TTNT similar to that of patients treated with paclitaxel, even after adjustment for differences in prognostic factors between the groups (Figure 3). These results are consistent with a recent publication comparing nab-paclitaxel and paclitaxel in mBC, which did not show a statistically significant difference in TTNT between the two treatment groups in patients with mTNBC receiving 1L treatment [11]. Although the TTNT in the nab-paclitaxel group was numerically higher in Mahtani et al. than what we report (6.3 vs 4.0 months, respectively), differences in study methodology – such as inclusion of death as an outcome and the rules used to advance a line of therapy – and patient populations could have contributed to this discrepancy.
The only subgroup analysis that showed a statistically significant association of treatment with outcomes was in patients with a TFI of >12 months: patients treated with nab-paclitaxel had a significantly longer TTNT than those treated with paclitaxel. It is important to highlight that this may be a spurious observation related to this subgroup’s small size (n = 156). Alternatively, it is possible that the difference in treatment efficacy seen with nab-paclitaxel and paclitaxel depends on the TFI between prior neoadjuvant or adjuvant chemotherapy and subsequent relapse; however, additional supportive studies would be required to test this possibility.
Several limitations to the study should be noted. This was a retrospective study, making causal inferences difficult and confounding by indication possible. Although methods to adjust for differences in patient characteristics between the groups were employed, unmeasured confounding may still exist. We employed abstraction of key covariates to increase completeness; however, covariates such as comorbidities may be underreported, potentially leading to misclassification and unmeasured confounding. The sample size was small, and therefore noninferiority cannot be determined; however, all patients who received nab-paclitaxel or paclitaxel monotherapy within the Flatiron network were identified, thereby limiting selection bias. Furthermore, TTNT was identified based on lack of treatment information from EHR data, which may not fully capture subsequent treatments if a patient received treatment outside of the network. Finally, no information on adverse events was collected in the study; therefore, conclusions regarding the safety or tolerability of either drug cannot be made.
Although we found similar efficacy between paclitaxel and nab-paclitaxel in the real-world setting, it should be noted that there are numerous other factors, which were not captured in the available data set, that determine treatment choice, such as tolerability, cost and healthcare utilization. In the absence of these data, it is not possible to assess the complete pharmacoeconomic impact of treatment choice.
The strengths of this study include the geographic and demographic diversity of the broader Flatiron network, suggesting that the study population is representative of patients with mBC treated in routine clinical practice across the USA. Through Flatiron’s technology-enabled abstraction process, the completeness of key variables was increased to improve the quality of the data over what is available in the structured fields of the EHR. Lastly, previous studies validating the mortality end point in the Flatiron Health EHR–derived database have shown a sensitivity of 87% in breast cancer [32], suggesting a high level of completeness for the primary end point for this study.
Conclusion
In this observational comparative-effectiveness study, OS and TTNT were similar in patients treated with nab-paclitaxel and those treated with paclitaxel. Consistency in estimates across several sensitivity analyses suggests robustness of the results. The similarity of results in clinical practice suggests that nab-paclitaxel and paclitaxel may be considered interchangeable as 1L treatments for patients with mTNBC.
•
Taxanes are a common treatment choice for metastatic triple-negative breast cancer (mTNBC), but few studies have directly evaluated these agents in the real-world setting.
•
The goal of our study was to compare the effectiveness of two taxanes: nab-paclitaxel and paclitaxel.
•
This retrospective observational study evaluated overall survival and time to next treatment in patients with mTNBC treated in clinical practice with first-line nab-paclitaxel versus paclitaxel monotherapy.
•
Data from 200 patients who had received either nab-paclitaxel monotherapy (n = 105) or paclitaxel monotherapy (n = 95) were extracted from the US Flatiron electronic health record–derived database and included in the analysis.
•
The use of paclitaxel and nab-paclitaxel were similar: the majority of patients received weekly dosing schedules, with nab-paclitaxel 100 mg/m2 and paclitaxel 80 mg/m2 being the most common doses.
•
The adjusted overall survival hazard ratio was 0.98 (95% confidence interval: 0.67–1.44), and the adjusted time to next treatment hazard ratio was 0.89 (95% confidence interval: 0.62–1.29), indicating similarity between treatment groups.
•
Consistency in estimates across sensitivity analyses, accounting for differences in characteristics between the populations, suggested robustness of the main results.
•
Our analyses showed similar efficacy for nab-paclitaxel and paclitaxel monotherapy in clinical practice, suggesting their interchangeability as first-line treatments for mTNBC.
Financial & competing interests disclosure
P Luhn, SY Chui, AFC Hsieh, PS Bajaj, W Hasnain, TGN Ton are Genentech/Roche employees and Roche stockholders. In addition, SY Chui has a patent, Diagnostic and Therapeutic Methods for Triple-Negative Breast Cancer (62/734677) pending. A Mecke and A Falgas are F. Hoffmann-La Roche employees and Roche stockholders. J Yi was employed by Genesis Research at the time of the analysis. AW Kurian reports research funding to her institution from Myriad Genetics for an unrelated project. This study was sponsored by F. Hoffmann-La Roche, Ltd. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance for this manuscript was provided by J Men of Health Interactions and funded by F. Hoffmann-La Roche, Ltd.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
The data that support the findings of this study are available from Flatiron Health, but restrictions apply to the availability of these data, which are subject to the de-identification requirements of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and implementing regulations, as amended. Practically speaking, in order to share select data and data elements, it is necessary to first define the methods of storage, transmission, access rights, and the scope of intended use prior to making any such data available, and an agreement memorializing the same and applicable re-identification restrictions are required for the purposes of ensuring compliance with the data license, de-identification, data protection specifications, and requirements under HIPAA. Please refer any questions or requests regarding data used in this manuscript to Patricia Luhn (corresponding author).
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Kohler B, Sherman R, Howlader N et al. Annual report to the nation on the status of cancer, 1975–2011, featuring incidence of breast cancer subtypes by race/ethnicity, poverty, and state. J. Natl Cancer Inst. 107, 1 (2015).
2.
Gobbini E, Ezzalfani M, Dieras V et al. Time trends of overall survival among metastatic breast cancer patients in the real-life ESME cohort. Eur. J. Cancer 96, 17–24 (2018).
3.
Miles DW, Dieras V, Cortes J, Duenne AA, Yi J, O'Shaughnessy J. First-line bevacizumab in combination with chemotherapy for HER2-negative metastatic breast cancer: pooled and subgroup analyses of data from 2447 patients. Ann. Oncol. 24(11), 2773–2780 (2013).
4.
Bajaj P, Latremouille-Viau D, Guerin A et al. What are the treatment patterns and overall survival (OS) in patients with metastatic triple-negative breast cancer (mTNBC) in US clinical practice? Ann. Oncol. 28, mdx365.031, abstract 286P (2017).
5.
Yardley DA, Coleman R, Conte P et al. nab-Paclitaxel plus carboplatin or gemcitabine versus gemcitabine plus carboplatin as first-line treatment of patients with triple-negative metastatic breast cancer: results from the tnAcity trial. Ann. Oncol. 29(8), 1763–1770 (2018).
6.
Aly A, Shah R, Hill K et al. Overall survival, costs and healthcare resource use by number of regimens received in elderly patients with newly diagnosed metastatic triple-negative breast cancer. Future Oncol. 15(9), 1007–1020 (2019).
7.
Roche registration GMBH.Avastin (bevacizumab) summary of product characteristics (2017). www.ema.europa.eu/en/documents/product-information/avastin-epar-product-information_en.pdf
8.
AstraZeneca Pharmaceuticals LP. Lynparza(olaparib) package insert (2018). www.accessdata.fda.gov/drugsatfda_docs/label/2018/208558s001lbl.pdf
9.
Schmid P, Adams S, Rugo HS et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N. Engl. J. Med. 380(10), 986–987 (2019).
10.
Genentech, Inc. Tecentriq (atezolizumab) [package insert] (2019). www.accessdata.fda.gov/drugsatfda_docs/label/2019/761034s018lbl.pdf
11.
Mahtani R, Parisi M, Gluck S et al. Comparative effectiveness of early-line nab-paclitaxel vs. paclitaxel in patients with metastatic breast cancer: a US community-based real-world analysis. Cancer Manag. Res. 10, 249–256 (2018).
•• This observational study compares outcomes of nab-paclitaxel- and paclitaxel-treated patients with metastatic breast cancer.
12.
Cardoso F, Senkus E, Costa A et al. 4th ESO–ESMO international consensus guidelines for advanced breast cancer (ABC 4). Ann. Oncol. 29, 1634–1657 (2018).
13.
Gradishar WJ, Tjulandin S, Davidson N et al. Phase III trial of nanoparticle albumin-bound paclitaxel compared with polyethylated castor oil-based paclitaxel in women with breast cancer. J. Clin. Oncol. 23, 7794–7803 (2005).
•• This randomized Phase III study evaluates nab-paclitaxel versus paclitaxel.
14.
Celgene Corporation, Summit. Abraxane (nab-paclitaxel) package insert (2018). https://media.celgene.com/content/uploads/abraxane-pi.pdf
15.
Gradishar WJ, Krasnojon D, Cheporov S et al. Significantly longer progression-free survival with nab-paclitaxel compared with docetaxel as first-line therapy for metastatic breast cancer. J. Clin. Oncol. 27(22), 3611–3619 (2009).
16.
Quan H, Li B, Couris CM et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173 (6), 676–682 (2011).
17.
Quan H, Sundararajan V, Halfon P et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care. 43(11), 1130–1139 (2005).
• Validates an updated comorbidity index.
18.
Austin P. The performance of different propensity-score methods for estimating relative risks. J. Clin. Epidemiol. 61, 537–545 (2008).
• Evaluates the application of confounding control methods to relative risk estimations.
19.
Rosenbaum P. The central role of the propensity score in observational studies for causal effects. Biometrika 70, 41–55 (1983).
20.
Blum JL, Savin MA, Edelman G et al. Phase II study of weekly albumin-bound paclitaxel for patients with metastatic breast cancer heavily pretreated with taxanes. Clin. Breast Cancer 7(11), 850–856 (2007).
21.
Bristol-Myers Squibb. Taxol (paclitaxel) package insert (2011). www.accessdata.fda.gov/drugsatfda_docs/label/2011/020262s049lbl.pdf
22.
Seidman A, Berry D, Cirrincione C et al. Randomized phase III trial of weekly compared with every-3-weeks paclitaxel for metastatic breast cancer, with trastuzumab for all HER-2 overexpressors and random assignment to trastuzumab or not in HER-2 nonoverexpressors: final results of Cancer and Leukemia Group B protocol 9840. J. Clin. Oncol. 26, 1642–1649 (2008).
• This randomized Phase III study shows that weekly dosing of paclitaxel was superior to every three week dosing.
23.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Breast Cancer (2019). www.nccn.org/professionals/physician_gls/pdf/breast.pdf
24.
Liang C, Li L, Fraser C et al. The treatment patterns, efficacy, and safety of nab-paclitaxel for the treatment of metastatic breast cancer in the United States: results from health insurance claims analysis. BMC Cancer 15, 1019 (2015).
25.
Dirix LY, Takacs I, Jerusalem G et al. Avelumab, an anti-PD-L1 antibody, in patients with locally advanced or metastatic breast cancer: a phase 1b JAVELIN Solid Tumor study. Breast Cancer Res. Treat. 167(3), 671–686 (2018).
26.
Kurian A, Mitani A, Desai M et al. Breast cancer treatment across health care systems: linking electronic medical records and state registry data to enable outcomes research. Cancer 120(1), 103–111 (2014).
27.
Kennedy-Martin T, Curtis S, Faries D, Robinson S, Johnston J. A literature review on the representativeness of randomized controlled trial samples and implications for the external validity of trial results. Trials 16, 495 (2015).
28.
Walsh E, Sheridan A. Factors affecting patient participation in clinical trials in Ireland: a narrative review. Contemp. Clin. Trials Commun. 3, 23–31 (2016).
29.
Baquet C, Commiskey P, Mullins C, Mishra S. Recruitment and participation in clinical trials: socio-demographic, rural/urban, and health care access predictors. Cancer Detect. Prev. 30, 24–33 (2006).
30.
Hari P, Romanus D, Palumbo A et al. Prolonged duration of therapy is associated with improved survival in patients treated for relapsed/refractory multiple myeloma in routine clinical care in the United States. Clin. Lymphoma Myeloma Leuk. 18, 152–160 (2018).
31.
Chen C, Parikh K, Abouzaid S et al. Real-world treatment patterns, time to next treatment, and economic outcomes in relapsed or refractory multiple myeloma patients treated with pomalidomide or carfilzomib. J. Manag. Care Spec. Pharm. 23, 236–246 (2017).
32.
Curtis M, Griffith S, Tucker M et al. Development and validation of a high-quality composite real-world mortality endpoint. Health Serv. Res. 53 (6), 4460–4476 (2018).
• Validates the survival outcome in the Flatiron database.
Information & Authors
Information
Published In
Pages: 1173 - 1185
PubMed: 31394922
Copyright
© 2019 Future Medicine Ltd.
History
Received: 14 June 2019
Accepted: 23 July 2019
Published online: 9 August 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of first-line nab-paclitaxel versus paclitaxel monotherapy in triple-negative breast cancer. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0077
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yuqi Xing, Ruiqi Zhong, Qianchen Li, Xinwei Duan, Moyang Xu, Miao Yu, Chenying Liu, Junming He, Yi Sun, Yunling Wang, Xiaojing Guo, Yunfei Xu, Hongnan Mo, Fei Ma, Hongquan Zhang, Jun Zhan, Paclitaxel drives TREM2+ macrophage expansion underlying its inferior therapeutic efficacy compared to Nab-paclitaxel, Nature Communications, 10.1038/s41467-026-69060-5, (2026).
- Natalia Sadetsky, Patricia Prince, Helen Latimer, Pooja Advani, Demetria Smith-Gaziani, Peter A. Kaufman, Yanina Natanzon, Aliki Taylor, Linda Nguyen, Nick Freemantle, Exploration of real-world outcomes in patients with previously treated HR+/HER2- and triple negative metastatic breast cancer, Scientific Reports, 10.1038/s41598-025-33530-5, 16, 1, (2026).
- Guojun Xiong, Chengwei Jiang, Andreas G. Schätzlein, Ijeoma F. Uchegbu, The colloidal stability of albumin-based drug delivery systems has a profound effect on tumoricidal activity, Drug Delivery, 10.1080/10717544.2026.2614801, 33, 1, (2026).
- Mark S. Shahin, Raina Mathur, Anju Parthan, Prakirthi Yerram, Amanda Kesner-Hays, Rachel Myers, Iulia Cristina Tudor, Darin Dobler, Adrian M. Jubb, Robert L. Coleman, Comparative outcomes of nab-paclitaxel and paclitaxel in platinum-resistant ovarian cancer (COMPASS), Gynecologic Oncology, 10.1016/j.ygyno.2025.11.022, 204, (202-209), (2026).
- S.M. Tolaney, L. Spring, Y.G. Abdou, M.K. Rehnquist, C. Hogea, A. Estrin, N. Sjekloca, C. Lai, K. Kalinsky, Understanding first-line treatment patterns and survival outcomes across sociodemographic groups of women with metastatic triple-negative breast cancer in the United States: a real-world study, ESMO Open, 10.1016/j.esmoop.2025.105841, 10, 10, (105841), (2025).
- Guojun Xiong, Shengxi Li, Andreas G. Schätzlein, Ijeoma F. Uchegbu, Amphiphilic albumin-based nanoparticles designed for the efficient delivery of taxanes, International Journal of Pharmaceutics, 10.1016/j.ijpharm.2025.125965, 682, (125965), (2025).
- Kevin Punie, Allison W Kurian, Ioanna Ntalla, Nikoleta Sjekloca, Adina Estrin, Elizabeth C Dabrowski, Catherine Lai, Sara Hurvitz, Unmet need for previously untreated metastatic triple-negative breast cancer: a real-world study of patients diagnosed from 2011 to 2022 in the United States, The Oncologist, 10.1093/oncolo/oyaf034, 30, 3, (2025).
- Chanchal Tiwari, Jigyasa Tomer, Dharmendra Kumar, Liposomal Drug Delivery: Progress, Clinical Outlook, and Ongoing Challenges, Recent Advances in Drug Delivery and Formulation, 10.2174/0126673878300031240703070511, 18, 3, (157-169), (2024).
- Kennady K. Bullock, Ann Richmond, Beyond Anti-PD-1/PD-L1: Improving Immune Checkpoint Inhibitor Responses in Triple-Negative Breast Cancer, Cancers, 10.3390/cancers16122189, 16, 12, (2189), (2024).
- Ruoding Tan, Lourenia Cassoli, Ying Yan, Vincent Shen, Bann-mo Day, Edith P. Mitchell, Assessing Real-World Racial Differences Among Patients With Metastatic Triple-Negative Breast Cancer in US Community Practices, Frontiers in Public Health, 10.3389/fpubh.2022.859113, 10, (2022).