Effects of mindfulness-based interventions on quality of life of women with breast cancer: a systematic review
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The systematic review assessed the effect of mindfulness-based interventions on the quality of life among women with breast cancer. Methods: PubMed, Cochrane library, EMBASE, Web of Science and CINAHL databases were searched for studies published. Our review assessed the effect of mindfulness-based interventions (Mindfulness-Based Stress Reduction [MBSR] intervention and Mindfulness-Based Cognitive Therapy [MBCT]) on quality of life for women with breast cancer. Two authors independently assessed the quality of all included studies using the Downs and Black Quality Index. Results: The search finally identified 15 studies. The MBSR intervention showed a significant effect between groups. The MBCT intervention also showed good effect on quality of life. Adverse events were inadequately reported. Conclusion: The MBSR intervention on quality of life among women with breast cancer was effective and safe. The effect of MBCT intervention on quality of life still needs more research.
Breast cancer is the most common cancer among women worldwide, with an estimated 1.67 million new cases each year [1]. Recently, owing to continuous advances in early detection, medical care and improved diagnosis and treatment, the 5-year survival rate of breast cancer has reached 85% or higher [2,3]. However, for many breast cancer survivors, health related quality of life including psychological, physical and social quality of life is affected by cancer diagnosis and treatment [4]. Patients not only experience physical symptoms such as fatigue, pain, tingling and numbness [5], and sleep disturbances, but must also cope with survival and its associated psychological and social difficulties [6,7]. This may seriously affect health related quality of life among women with breast cancer, and contribute to even higher levels of mortality [8,9].
To improve quality of life and negate the associated disease risks and burdens, nonpharmacological mindfulness-based interventions have been reported to be effective among women with breast cancer [10,11]. A mindfulness-based intervention is a clinical application of principles found in Buddhism and other spiritual practices, based on the thought processes of nonjudgmental acceptance of physical pain or psychological pain. The subjects disengage themselves from painful thoughts by diverting attention to the present moment. thus reducing the tendency to catastrophize their experiences [12]. Two of the main mindfulness-based methods include Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT) [13]. MBSR is a structured 8-week group program of weekly sessions taking an average of 2.5 h/per session with an additional silent day retreat; participants are further instructed to practice the intervention at home. It includes body scans, sitting meditation, walking meditation, hatha yoga and mindful relaxation techniques [12]. MBCT combines MBSR intervention with cognitive–behavioral methods. It retains the 8-week group structure, the silent day retreat, mindfulness training and home practice, but has more explicit psychoeducation components on the relationship between cognition, and mood and functioning. MBCT emphasizes rumination of thoughts to consider negative experience without taking action to remedy the situation [14].
One meta-analysis of randomized trials on MBSR compared with usual care in women with breast cancer from 2012 [15] revealed significant small to moderate effects on physical function, depression, anxiety, stress and quality of life. However, due to the low number of eligible studies, the evidence was limited by incomplete reporting and defects in the methodology of the included trials. In 2016, another meta-analysis of randomized controlled trials of patients with breast cancer was published [16]. However, only two studies evaluated the impact of mindfulness-based intervention on quality of life, and there was only limited evidence from a narrative synthesis. Moreover, safety issues have not been examined by previous reviews. A recent systematic review and meta-analysis in 2017 revealed evidence for only short-term improved health-related quality of life from mindfulness-based intervention in comparison to usual care; in that analysis, the long-term impact was not significant in women with breast cancer. Therefore, the aim of the present systematic review is to analyze results of all clinical trials regarding the effects of mindfulness-based intervention on quality of life among women diagnosed with breast cancer, in order to inform decisions about recommendations for overall treatment.
Material & methods
This present systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [17].
Inclusion criteria
Types of studies: all clinical trials were included in this review.
Types of participants: participants included adult women with a clinical diagnosis of breast cancer (Stage 0–IV).
Types of interventions: only studies that assessed MBSR or MBCT as the major intervention were eligible for inclusion. However, certain differences in MBSR or MBCT interventions, such as session length, frequency or duration did not hinder inclusion. Studies of mindfulness-based interventions that were different from the original MBSR or MBCT programs, such as acceptance and commitment therapy, mindfulness-based exercise, or art therapy were excluded. Acceptable control interventions were usual care, wait list or any other active treatments.
Types of outcomes: the studies were required to report quality of life as one outcome measure.
Search strategy
In October 2018, the electronic literature was systematically searched via PubMed, Cochrane library, EMBASE, Web of Science and CINAHL, limited to English language articles. The searches were based on the following strategy: ‘mindfulness’ OR ‘insight meditation’ OR ‘MBSR’ OR ‘MBCT’ AND ‘breast cancer’ OR ‘breast neoplasm’ OR ‘breast oncology’ OR ‘breast carcinoma’ OR ‘breast tumor’ OR ‘mammary tumor’ AND ‘quality of life.’ We also identified related systematic reviews and meta-analyses and checked their reference lists.
Selection of literature
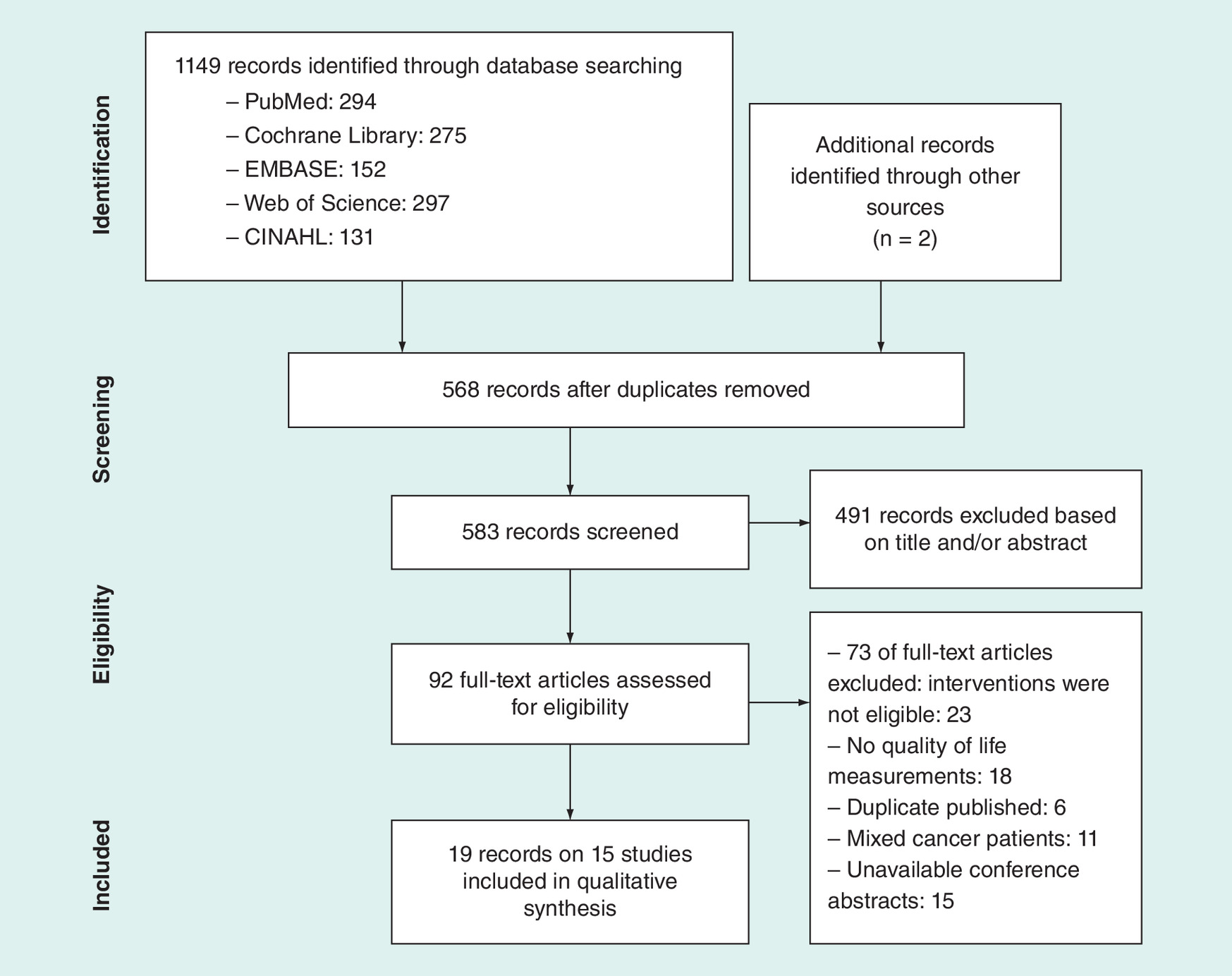
The study selection process is outlined in Figure 1. Eligibility was assessed by two independent raters in a standardized manner. Study titles and abstracts were independently assessed twice to confirm relevance to the topic of this review. If there was inadequate information to include or exclude an article, the full-text version was sought. Full-text versions of all the relevant studies were obtained and read by two independent reviewers to ensure eligible inclusion criteria.
Quality assessment
Two reviewers independently assessed the quality of all selected studies using the Downs and Black Quality Index (QI), which assesses the quality of articles for both nonrandomized and randomized trials [18]. The scale includes reporting, external validity, bias, confounding and power; the maximum possible scores are 11, 3, 7, 6 and 5, respectively and the maximum total score is 32. The quality scores were estimated and ranked on a four-category scale: poor (<18), moderate (18–23), good (24–29) and excellent (>30). Scoring differences were rechecked between the two reviewers and discussed until consensus was reached.
Data extraction
Two reviewers used a standard data extraction checklist to independently extract the following data from each study: study characteristics, sample population characteristics, characteristics of the intervention and control groups, and outcomes. One investigator conducted the data extraction, which was checked by a second investigator. The results from different study designs should be considered systematically to avoid increased heterogeneity of results [19]. Therefore, no meta-analysis was performed due to the heterogeneity of study designs and outcomes.
Results
Search results
Figure 1 shows the literature search flow chart of the 1149 records identified. Two additional studies were retrieved via a manual search of the reference lists of the full-text versions collected during the initial search. Of these, 568 records were excluded as they represented duplicate records, and the initial sifting based on the title and abstract through Endnote X9 resulted in the exclusion of a further 491 records. The full-text version of 92 studies were investigated, and 73 studies were excluded because the intervention was not eligible, they were duplicate publications, subjects included other cancers, they were unavailable conference abstracts, or they did not report quality of life as an outcome measurement. Finally, 19 records [20–38] of 15 study samples with 1518 participants were included in our systematic review.
Quality assessment
Table 2 shows the quality assessment of the 15 studies in this systematic review. Most of the studies demonstrated good reporting quality; however, most of the studies had a high risk of bias in terms of study design. Five studies were of poor quality, with a mean score of 13; of the remaining ten studies, six were deemed to be of high quality and four were deemed to be of moderate quality.
| Study (year), [Ref.] | Location | Sample characteristics | Intervention characteristics | Outcomes | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean age, years | Participants | Sample size (n) | Treatment group | Control group | Frequency and Duration | Quality of life measurements | Findings | Dropout | ||
| Henderson et al. (2012), [20] Henderson 2013 [21] | USA | 49.8 | Breast cancer, Stage I–II. undergoing adjuvant treatment. | TG = 53 CG1 = 52 CG2 = 58 | An original MBSR program | CG1 = NEP program CG2 = usual care | Weekly 2.5- to 3.5-h sessions, with an additional 7.5-h intensive retreat session, 8 weeks | FACT-B | Marginally significant between-group differences for spirituality, social-family and emotional well-being (All p < 0.1) | 17 |
| Lengacher et al. (2009), [25] Lengacher 2012 [22] Lengacher 2014 [23] | USA | 57.5 | Breast cancer, Stage 0–III, ≤18 month post-surgery/adjuvant treatment. | TG = 41 CG = 43 | A modified MBSR program | Usual care | Weekly 2-h sessions, 6 weeks | SF-36 | Significant between-group differences for physical functioning (p = 0.01), physical health (p = 0.03) and energy (p = 0.02) | TG = 1 CG = 1 |
| Lengacher et al. (2016), [26] | USA | TG = 56.5 CG = 57.6 | Breast cancer, Stage 0–III, ≥2 months and ≤2 years post-surgery/adjuvant treatment | TG = 167 CG = 155 | A modified MBSR program | Usual care | Weekly 2-h sessions, 6 weeks | SF-36 | No significant between-group difference | TG = 15 CG = 8 |
| Hoffman et al. (2012), [27] | UK | TG = 49 CG = 50.1 | Breast cancer, Stage 0–III, ≥2 months and ≤2 years post-adjuvant treatment | TG = 114 CG = 115 | An original MBSR program | Wait list | Weekly 2-h sessions, plus one 6-h day of mindfulness, 8 weeks | FACT-B | Significant between-group differences (p < 0.01) | TG = 11 CG = 4 |
| Lee et al. (2017), [28] | Korea | 53.5 | Metastatic breast cancer, undergoing adjuvant treatment | TG = 20 CG = 12 | An original MBSR Program, yoga part was excluded | Wait list | Weekly 2-h sessions, 8 weeks | FACT-B | No significant between-group difference | TG = 11 CG = 3 |
| Lengacher et al. (2011), [29] | USA | 56.8 | Breast cancer, Stage 0–III, ≥1 year post-surgery/adjuvant treatment | 19 | An original MBSR Program | None | Weekly 2-h sessions, 8 weeks | SF-36 | Significant improvements in emotional well-being (p = 0.003) and general health (p =0.03) | 2 |
| Eyles et al. (2015), [30] | UK | NR | Metastatic breast cancer | 20 | A modified MBSR Program,the day of mindfulness was 4.5 h, home practice was 30 min/day | None | Sessions were 2 h except the first and last, which were 2.5 h, 8-weeks | EORTC QLQ C30 | Significant improvements in global health scale (p = 0.005), physical functioning (p = 0.037), cognitive functioning (p = 0.015) and insomnia (p = 0.007) | 1 |
| Carlson et al. (2013), [31] Carlson 2016 [24] | Canada | TG = 55.12 CG = 54.14 | Breast cancer, Stage I –III, ≥3 months post-adjuvant treatment | TG = 113 CG1 = 104 CG2 = 54 | A modified MBSR Program, plus a 6-h workshop | CG1: 12-week SET program CG2: Usual care | Weekly 90 min sessions, 8-weeks | FACT-B | Significant between-group difference for functional well-being (p = 0.01) | 87 |
| Bisseling et al. (2017), [32] | The Netherlands | 52.3 | Breast cancer | 64 | An original MBSR program | None | Weekly 2.5-h sessions, 6 weeks | EORTC QLQ-C30 | No significant improvement | 12 |
| Rahmani et al. (2014), [33] | Iran | TG = 44.92 CG1 = 43.25 CG2 = 44.08 | Breast cancer, Stage I –III. | TG = 12 CG1 = 12 CG2 = 12 | An original MBSR program | CG1: Metacognition group therapy CG2: Usual care | Weekly 2-h sessions 8 weeks | EORTC QLQ-C30 and EORTC QLQ-BR23 | Significant between-group differences for functions, roles, fatigue, pain, future perspective and treatment side effects symptoms (all p < 0.05) | NR |
| Johannsen et al. (2016), [34] | Denmark | TG = 56.8 CG = 56.7 | Primary breast cancer, ≥3 months post-surgery/adjuvant treatment | TG = 67 CG = 62 | A modified MBCT Program, meditation exercises≤ 30 min, the whole-day session was omitted | Wait list | Weekly 2 h sessions, 8 weeks | WHO-5 | Significant between-group differences (p = 0.028) | TG = 28 CG = 5 |
| Lengacher et al. (2017), [35] | USA | 57 | Breast cancer, Stage 0–III,≥2 weeks and ≤2 years post-surgery/adjuvant treatment | 15 | A modified MBSR Program via iPad | None | Weekly 2 h sessions, 6 weeks | SF‐36 | Significant improvements in energy (p = 0.02), emotional well-being (p = 0.03), general health (p = 0.01) and physical health (p = 0.03) | 0 |
| Lerman et al. (2012), [36] | USA | TG = 57.5 CG = 56.4 | Breast cancer subsample. under/post-surgery/adjuvant treatment | TG = 34 CG = 14 | An original MBSR program | Wait list | Weekly 2 h sessions, a 4-h retreat, 8 weeks | EORTC QLQ-BR23 | Significant between-group differences (p = 0.001) | TG = 2 CG = 2 |
| Witek-Janusek et al. (2008), [37] | USA | TG = 55 CG = 54 | Breast cancer, Stage 0–II | TG = 44 CG = 31 | An original MBSR program, plus one full day session held | Usual care | Weekly 2.5 h sessions, 8 weeks | Quality of Life Index Cancer Version III | Significant between-group differences for spiritual (p = 0.001) and life satisfaction (p = 0.046) | TG = 6 CG = 3 |
| Park et al. (2018), [38] | Japan | 50.1 | Breast cancer, Stage I–II, under/post- adjuvant treatment | 12 | A modified MBCT program, retreat was omitted | None | Weekly 2 h sessions, 8 weeks | FACT-B | Significant improvements in global QOL, emotional and functional well-being (all p < 0.05) | 0 |
CG: Control group; EORTC QLQ-BR23: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire – Breast Cancer Module; EORTC QLQ C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire -Core 30; FACT-B: Functional Assessment of Cancer Therapy-Breast; MBCT: Mindfulness-based cognitive therapy; MBSR: Mindfulness-based stress reduction; NEP: Nutrition education program; NR: Not reported; QOL: Quality of life; SET: Supportive expressive therapy; SF-36: Short Form-36; TG: Treatment group; WHO-5: WHO-Five Well-Being Index.
| Study [Ref.] | Reporting (11) | External validity (3) | Bias (7) | Confounding (6) | Power (5) | Total (32) | Quality as per cut-off described |
|---|---|---|---|---|---|---|---|
| Henderson et al. [20] Henderson [21] | 9 | 2 | 5 | 4 | 5 | 25 | Good |
| Lengacher et al. [25] Lengacher [22] Lengacher [23] | 10 | 1 | 6 | 4 | 5 | 26 | Good |
| Lengacher et al. [26] | 10 | 2 | 5 | 4 | 5 | 26 | Good |
| Hoffman et al. [27] | 10 | 1 | 7 | 4 | 5 | 27 | Good |
| Chung Eun et al. [28] | 7 | 1 | 3 | 3 | 0 | 14 | Poor |
| Lengacher et al. [29] | 8 | 1 | 3 | 1 | 0 | 13 | Poor |
| Eyles et al. [30] | 9 | 2 | 4 | 2 | 5 | 22 | Moderate |
| Carlson et al. [31] Carlson [24] | 10 | 2 | 7 | 4 | 5 | 28 | Good |
| Bisseling et al. [32] | 8 | 3 | 4 | 3 | 0 | 18 | Moderate |
| Rahmani et al. [33] | 8 | 0 | 4 | 2 | 0 | 14 | Poor |
| Johannsen et al. [34] | 10 | 2 | 3 | 5 | 5 | 25 | Good |
| Lengacher et al. [35] | 6 | 1 | 4 | 2 | 0 | 13 | Poor |
| Lerman et al. [36] | 10 | 3 | 4 | 4 | 0 | 21 | Moderate |
| Witek-Janusek et al. [37] | 8 | 1 | 5 | 1 | 5 | 20 | Moderate |
| Park et al. [38] | 5 | 1 | 3 | 2 | 0 | 11 | Poor |
Study characteristics
The characteristics of the included articles are listed in Table 1. In the 15 selected studies, the sample size ranged from 15 [35] to 322 [26] participants. Mean age ranged from 43.25 [33] to 57.6 [26] years. Of these included studies, seven were performed in the United States [20,25,26,29,35–37], two in the United Kingdom [27,30], one in Canada [31], one in Japan [15], one in Iran [33], one in The Netherlands [32], one in Korea [28] and one in Denmark [34]. The patient samples ranged from Stage 0 (nonmetastatic breast cancer) to Stage III breast cancer. Cancer treatment status varied among studies, with nine studies including patients who were post-adjuvant or surgery treatment [25–27,29,31,34–36,38] and only two studies including patients who undergoing adjuvant treatment [20,28], excluding four studies that did not report patients cancer treatment status [30,32,33,37]. The interventions included 13 MBSR program studies [20,25–33,35–37], and two MBCT program studies. Control groups included usual care (six studies) [20,25,26,31,33,37], wait list (four studies) [27,28,34,36], supportive expressive group therapy (one study) [31], metacognition group therapy (one study) [33] and group nutrition education program (NEP) (one study) [20]. Five studies did not have a control group [29,30,32,35,38].
Outcomes
MBSR interventions
Thirteen studies containing 1377 participants reported the effect of MBSR interventions on the quality of life in patients with breast cancer [20,25–33,35–37]. The interventions included eight studies of the original MBSR program [20,27–29,32,33,36,37], and five studies that assessed modified MBSR interventions [25,26,30,31,35]. Of these five, three studies were mainly modifications of the original MBSR program in terms of duration period [25,26,35], and two studies were mainly modifications of the original MBSR program in terms of session time [30,31]. The duration of the training sessions varied from at least 90 min [31] to 2.5 h [20,32,37] weekly, the duration of the total training period only including 6 weeks [25,26,32,35] and 8 weeks [20,27–31,33,36,37]. Among the included studies, three studies compared intervention type with two control groups [20,31,33]. Quality of life was assessed using three breast cancer-specific measures: four studies used the Functional Assessment of Cancer Therapy-Breast quality-of-life instrument (FACT-B) [20,27,28,31]; three studies used the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core-30 (EORTC QLQ C30) [30,32,33]; and two studies used the European Organization of Research and Treatment of Cancer Quality of Life Questionnaire – Breast Cancer Module (EORTC QLQ-BR23) [33,36]. Furthermore, two generic quality of life tools were used: four studies used the Medical Outcomes Study Short Form Health Survey (SF-36) [25,26,29,35]; and one study used Quality of Life Index Cancer Version III [37]. Among the included studies, one study used two quality of life measures [33].
Among 13 studies, three studies reported no significant impact of MBSR interventions on quality of life in patients with breast cancer. Lee et al. investigated Korean patients with metastatic breast cancer undergoing adjuvant treatment [28]. A randomized trial by Lengacher et al. studied the large sample; their patients underwent a 6-week modified MBSR intervention for breast cancer survivors [26].
Ten studies reported a significant effect of MBSR interventions on the quality of life in patients with breast cancer compared with those in the control group.
Henderson et al. conducted a randomized controlled trial comparing the original MBSR program with NEP for early-stage breast cancer. MBSR intervention was associated with significant improvement on measures of emotional well-being and spirituality subscales of FACT-B versus women in NEP and usual care, and social-family well-being after control for confounding variables [20]. Hoffman et al. examined the relationship between original MBSR intervention and breast cancer-specific quality of life after hospital treatment in women with Stage 0 to III breast cancer. Participants were asked to record the time and amount of home activities on record sheets. They found that there were significant improvements in mood, well-being and breast- and endocrine-related quality of life in the experimental group in women with breast cancer compared with standard care and these results persisted at 3 months [27]. Rahmani et al. found metacognition treatment and the MBSR treatment were effective in improving global and specific quality of life compared with the control group. The MBSR treatment was superior in improving fatigue, pain, future perspective and treatment side effects symptoms at the end of the treatment in comparison to the metacognition treatment, which persisted until the two-month follow-up. The important finding in this study was that the MBSR program had a broader effect range in specific life quality and in reducing pain intensity associated with cancer [33]. Witek-Janusek et al. evaluated women with early-stage breast cancer enrolled in an original 8-week MBSR program and found significantly reduced cortisol levels compared with the non-MBSR group. They suggested that the early provision of original MBSR intervention during the peritreatment period may be conducive to restore immune function, probably mediated by neuroendocrine activation resulting in the production or reduction of proinflammatory cytokines. They also found significant improvements compared with that of usual care on two of four domains of used Quality of Life Index Cancer Version III, in other words, ‘psychological–spiritual’ and ‘family.’ This suggests that MBSR allows individuals facing a potentially life-threatening situation to find more satisfaction in family and psychological–spiritual domains when evaluated using the Quality of Life Index Cancer Version III [37].
Lengacher et al. conducted a randomized controlled trial of a modified 6-week MBSR program with 84 female breast cancer survivors and found that compared with usual care, subjects in the MBSR group had significantly lower mean levels of depression, and anxiety, along with mean quality of life scores including physical functioning, and role limitations related to physical health. They also found that subjects who were more compliant with the MBSR intervention and practiced more tended to have larger reductions in perceived stress and pain of adjusted quality of life scores using SF-36 [25]. Carlson et al. measured the effects of modified MBCR intervention and supportive expressive group therapy (SET) in 252 distressed Stage I–III breast cancer survivors. They reported that patients in the MBCR intervention group reported increased emotional and functional quality of life relative to those in the SET group and control group, with benefits lasting more than 1 year. Improvements in fatigue and depression were noted but not significant [31]. Lengacher et al. tested the impact on delivering a mobile 6-week MBSR program using an iPad for breast cancer survivors on symptom improvement. Using video file modules on an iPad, the MBCR intervention group participants and to record practice time on the iPad. The authors reported significant improvements in energy, emotional well-being, general health and physical health scores of the SF-36, and sleep quality and fatigue from baseline to 6 weeks post MBSR [35].
Therefore, these results indicate a beneficial effect of MBSR interventions on quality of life among patients with breast cancer.
MBCT interventions
The interventions were both modified MBCT programs. Among the included studies, quality of life was assessed using FACT-B [38] and the WHO Well-Being Index (WHO-5) [34] separately.
Johannsen et al. assessed the efficacy of a modified 8-week MBCT for late post-treatment pain in 129 women treated for primary breast cancer. They found that the intervention group reported significantly reduced neuropathic pain, and the present pain intensity and increased quality of life after correction for multiple comparisons, and these effects persisted to the 6-month follow-up [34]. Park et al. examined effect of a modified MBCT intervention on quality of life in patients with breast cancer. They observed that MBCT had a favorable effect on anxiety, trauma-related psychological symptoms, and emotional and functional well-being scores of the FACT-B [38].
These results indicate a beneficial effect of MBCT interventions on quality of life in patients with breast cancer.
Safety
No study formally reported adverse events. In one trial, one patient was lost to follow-up from the MBSR group, and her drop-out was related to recurrence of disease [25]. Another trial reported two patients discontinued MBSR classes in the MBSR group because of breast cancer recurrence when the intervention began [27]. Lee et al. reported one patient experienced a lumbar sprain and cancelled the MBSR session [28]. However, all other trials reported neither absence nor adverse events, with the exception of four studies that did not report detailed reasons for dropping out [20,31,36,37].
Discussion
This is the first review to systematically evaluate the effect of mindfulness-based interventions on the quality of life in patients with breast cancer. In this systematic review, the 15 included studies were heterogeneous in terms of type of the participants, treatment session program and quality of life measurements. Ten of the 13 MBSR studies reported a significant effect of MBSR interventions on quality of life in patients with breast cancer compared with those in the control group. The two MBCT studies reported a significant effect of MBCT programs on quality of life in patients with breast cancer compared with those in the control group.
Various policies were implemented to reduce the dropout rate of patients in the intervention group, such as supervised meditation sessions, provision of practice consultations, having the oncology nurse specialist call patients, home practice with providing audiotapes and discs, encouraging participants to fill out diaries at home, holding group meetings and reminders by the class instructor to attend the next class. Among the included studies, 13 provided supervisory measures [25–29,31–38]. In these 13 studies, attendance ranged from 59.2 to 93%. Ten of these 13 studies reported that the intervention significantly improved the quality of life of breast cancer patients [25,27,29,31,33–38]. The majority of patients was satisfied with the group intervention and said that the supportive interaction among team members to practice meditation yielded stimulative effects.
Six studies indicated that mindfulness-based interventions can significantly reduce symptoms of depression in patients with breast cancer [20,25,27,29,35,38]. Meanwhile, the quality of life in the intervention group was also improved. Nine studies investigated the impact of mindfulness-based intervention on improving anxiety in patients with breast cancer [20,25–27,29–31,35,38]. Among them, one study reported no improvement in quality of life and an improvement only in anxiety. The author hypothesized that the low symptom levels at baseline were inadequate to show clear effects in quality of life. Three studies reported an improvement in pain in the mindfulness-based intervention group in patients with breast cancer [28,33,34]. Of these three studies, one reported significant improvements only in pain and not in quality of life. The author thought that it was likely harder to improve quality of life in women with metastatic breast cancer who received continuous anticancer therapy with a cancer burden. Two other studies both indicated that mindfulness-based intervention significantly improved quality of life and reduced neuropathic pain and the present pain intensity and may have a durable benefits in women treated for breast cancer [33,34].
In our review, nearly one-half of the studies adopted modified interventions [25,26,30,31,34,35,38]. Two studies [30,31] found that many eligible women declined participation during recruitment and particularly when class arrangements clashed with other family commitments, clinic time or treatment. Thus, adapting the class times of a traditional program may be worthwhile and promote the acceptability of MBSR for women with metastatic breast cancer. Lengacher et al. delivered a modified MBSR program for breast cancer using an iPad; the patients reported that practicing the MBSR intervention remotely was convenient and easy to use, and the iPad greatly facilitated content of practice and learning [35]. It seems feasible to adopt technology-based methods such as by the use of mobile devices or video telecommunications instead of in-person sessions. Mindfulness-based interventions can be delivered remotely in an efficacious manner, to improve widespread clinical application and translation of this program. Thus, future studies will be needed to determine the optimal program of mindfulness-based interventions for women with breast cancer.
There are some clear limitations in our included studies. First, only two studies assessed the effects of MBCT intervention. Because of the small number of studies, further randomized controlled trials of MBCT intervention are required for women with breast cancer. Second, only three studies reported definite reasons for drop-out or adverse events, and safety could not be adequately assessed. There was one report of a patient experiencing a lumbar sprain and three cases of breast cancer recurrence during the treatment; although mindfulness-based intervention cannot be excluded as a reason, this seems unlikely. Finally, the purpose of the current systematic review was to assess the effects of mindfulness-based interventions on quality of life; we also need more studies comparing mindfulness-based interventions with other active treatment control groups.
Implications for clinical practice should be drawn in the light of these limitations. This systematic review suggests effectiveness and safety of MBSR/MBCT interventions for women diagnosed with breast cancer during to adjuvant treatment. Therefore, offering MBSR/MBCT programs to such patients could provide an additional option in supportive cancer care.
Conclusion
This systematic review found evidence for the safety and effectiveness of mindfulness-based interventions on quality of life in women with breast cancer. We concluded that an MBSR program is effective and safe to improve the quality of life in patients with breast cancer. The effect of MBCT intervention on quality of life requires further research in people with breast cancer.
•
A mindfulness-based intervention is a clinical application of principles found in Buddhism and other spiritual practices.
•
Mindfulness-based interventions are reported to be effective nonpharmacological interventions to improve quality of life among women with breast cancer.
•
Two of the main mindfulness-based methods include Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT).
•
One meta-analysis on MBSR revealed significant small to moderate effects on physical function and quality of life.
•
The electronic literature was systematically searched via PubMed, Cochrane library, EMBASE, Web of Science and CINAHL, 15 studies were included.
•
Among 13 studies, ten studies reported a significant effect of MBSR interventions on the quality of life.
•
Two studies both reported the effect of MBCT interventions on the quality of life.
•
No study formally reported adverse events.
•
MBSR program is effective and safe to improve the quality of life in patients with breast cancer, the effect of MBCT intervention on quality of life requires further research.
Author contributions
XY Zhang and GJ Wang were involved in the conception and design of the study, DL Liu and BY Zhang were involved in the analysis and interpretation of the data; Y Zhang and XY Zhang were involved in the drafting of the paper or revising it critically for intellectual content; YX Li and XL Wang were involved and in the final approval of thce version to be published. All authors agree to be accountable for all aspects of the work.
Acknowledgments
We thank the authors of all of the included studies.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Ferlay J, Soerjomataram I, Dikshit RC et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 136(5), 359–386 (2015).
2.
Allemani C, Weir HK, Carreira H et al. Global surveillance of cancer survival 1995–2009: analysis of individual data for 25 676 887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 385(9972), 977–1010 (2015).
3.
Belkić K, Belkić D. Possibilities for improved early breast cancer detection by Padé-optimized magnetic resonance spectroscopy. Isr. Med. Assoc. J. 13(4), 236–243 (2011).
4.
Brandão T, Schulz MS, Matos PM. Psychological adjustment after breast cancer: a systematic review of longitudinal studies. Psychooncology 26(7), 917–926 (2017).
5.
Berger AM, Visovsky C, Hertzog M, Holtz S, Loberiza FR Jr. Usual and worst symptom severity and interference with function in breast cancer survivors. J. Support. Oncol. 10(3), 112–118 (2012).
6.
Berger AM, Gerber LH, Mayer DK. Cancer-related fatigue: implications for breast cancer survivors. Cancer 118(8 Suppl.), 2261–2269 (2012).
7.
Colagiuri B, Christensen S, Jensen AB, Price MA, Butow PN, Zachariae R. Prevalence and predictors of sleep difficulty in a national cohort of women with primary breast cancer three to four months postsurgery. J. Pain Symptom Manage. 42(5), 710–720 (2011).
8.
Lin X, Chen W, Wei F, Ying M, Wei W, Xie X. Night-shift work increases morbidity of breast cancer and all-cause mortality: a meta-analysis of 16 prospective cohort studies. Sleep Med. 16(11), 1381–1387 (2015).
9.
Suppli NP, Johansen C, Kessing LV et al. Survival after early-stage breast cancer of women previously treated for depression: a nationwide danish cohort study. J. Clin. Oncol. 35(3), 334–342 (2017).
• This trial demonstrated the effect of mindfulness-based interventions for insomnia comorbid with cancer.
10.
Garland SN, Carlson LE, Stephens AJ, Antle MC, Samuels C, Campbell TS. Mindfulness-based stress reduction compared with cognitive behavioral therapy for the treatment of insomnia comorbid with cancer: a randomized, partially blinded, noninferiority trial. J. Clin. Oncol. 32(5), 449–457 (2014).
11.
Neuhouser ML, Smith AW, George SM et al. Use of complementary and alternative medicine and breast cancer survival in the Health, Eating, Activity, and Lifestyle Study. Breast Cancer Res. Treat. 160(3), 539–546 (2016).
12.
Keng SL, Smoski MJ, Robins CJ. Effects of mindfulness on psychological health: a review of empirical studies. Clin. Psychol. Rev. 31(6), 1041–1056 (2011).
13.
Abbott RA, Whear R, Rodgers LR et al. Effectiveness of mindfulness-based stress reduction and mindfulness based cognitive therapy in vascular disease: a systematic review and meta-analysis of randomised controlled trials. J. Psychosom. Res. 76(5), 341–351 (2014).
14.
Carlson LE. Mindfulness-based interventions for physical conditions: a narrative review evaluating levels of evidence. ISRN Psychiatry 2012, 651583 (2012).
15.
Cramer H, Lauche R, Paul A, Dobos G. Mindfulness-based stress reduction for breast cancer – a systematic review and meta-analysis. Curr. Oncol. 19(5), e343–e352 (2012).
16.
Zhang J, Xu R, Wang B, Wang J. Effects of mindfulness-based therapy for patients with breast cancer: a systematic review and meta-analysis. Complement. Ther. Med. 26, 1–10 (2016).
17.
Knobloch K, Yoon U, Vogt PM. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and publication bias. J. Craniomaxillofac. Surg. 39(2), 91–92 (2011).
18.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 52(6), 377–384 (1998).
19.
Higgins T, Julian P. Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Book Series[M], Wiley (2008).
20.
Henderson VP, Clemow L, Massion AO, Hurley TG, Druker S, Hébert JR. The effects of mindfulness-based stress reduction on psychosocial outcomes and quality of life in early-stage breast cancer patients: a randomized trial. Breast Cancer Res. Treat. 131(1), 99–109 (2012).
21.
Henderson VP, Massion AO, Clemow L, Hurley TG, Druker S, Hébert JR. A randomized controlled trial of mindfulness-based stress reduction for women with early-stage breast cancer receiving radiotherapy. Integr. Cancer Ther. 12(5), 404–413 (2013).
22.
Lengacher CA, Reich RR, Post-White J et al. Mindfulness based stress reduction in post-treatment breast cancer patients: an examination of symptoms and symptom clusters. J. Behav. Med. 35(1), 86–94 (2012).
23.
Lengacher CA, Shelton MM, Reich RR et al. Mindfulness based stress reduction (MBSR[BC]) in breast cancer: evaluating fear of recurrence (FOR) as a mediator of psychological and physical symptoms in a randomized control trial (RCT). J. Behav. Med. 37(2), 185–195 (2014).
•• This randomized controlled trial (RCT) compared mindfulness-based stress reduction versus supportive expressive group therapy.
24.
Carlson LE, Tamagawa R, Stephen J, Drysdale E, Zhong L, Speca M. Randomized-controlled trial of mindfulness-based cancer recovery versus supportive expressive group therapy among distressed breast cancer survivors (MINDSET): long-term follow-up results. Psychooncology 25(7), 750–759 (2016).
25.
Lengacher CA, Johnson-Mallard V, Post-White J et al. Randomized controlled trial of mindfulness-based stress reduction (MBSR) for survivors of breast cancer. Psychooncology 18(12), 1261–1272 (2009).
26.
Lengacher CA, Reich RR, Paterson CL et al. Examination of broad symptom improvement resulting from mindfulness-based stress reduction in breast cancer survivors: a randomized controlled trial. J. Clin. Oncol. 34(24), 2827–2834 (2016).
27.
Hoffman CJ, Ersser SJ, Hopkinson JB, Nicholls PG, Harrington JE, Thomas PW. Effectiveness of mindfulness-based stress reduction in mood, breast- and endocrine-related quality of life, and well-being in stage 0 to III breast cancer: a randomized, controlled trial. J. Clin. Oncol. 30(12), 1335–1342 (2012).
28.
Lee CE, Kim S, Kim S, Joo HM, Lee S. Effects of a mindfulness-based stress reduction program on the physical and psychological status and quality of life in patients with metastatic breast cancer. Holist. Nurs. Pract. 31(4), 260–269 (2017).
29.
Lengacher CA, Johnson-Mallard V, Barta M et al. Feasibility of a mindfulness-based stress reduction program for early-stage breast cancer survivors. J. Holist Nurs. 29(2), 107–117 (2011).
30.
Eyles C, Leydon GM, Hoffman CJ et al. Mindfulness for the self-management of fatigue, anxiety, and depression in women with metastatic breast cancer. Integr. Cancer Ther. 14(1), 42–56 (2015).
31.
Carlson LE, Doll R, Stephen J et al. Randomized controlled trial of mindfulness-based cancer recovery versus supportive expressive group therapy for distressed survivors of breast cancer. J. Clin. Oncol. 31(25), 3119–3126 (2013).
32.
Bisseling EM, Schellekens MPJ, Jansen ETM, van Laarhoven HWM, Prins JB, Speckens AEM. Mindfulness-based stress reduction for breast cancer patients: a mixed method study on what patients experience as a suitable stage to participate. Support Care Cancer 25(10), 3067–3074 (2017).
33.
Rahmani S, Talepasand S, Ghanbary-Motlagh A. Comparison of effectiveness of the metacognition treatment and the mindfulness-based stress reduction treatment on global and specific life quality of women with breast cancer. Iran J. Cancer Prev. 7(4), 184–196 (2014).
•• This RCT compared mindfulness-based cognitive therapy versus usual care.
34.
Johannsen M, O'Connor M, O'Toole MS, Jensen AB, Højris I, Zachariae R. Efficacy of mindfulness-based cognitive therapy on late post-treatment pain in women treated for primary breast cancer: a randomized controlled trial. J. Clin. Oncol. 34(28), 3390–3399 (2016).
35.
Lengacher CA, Reich RR, Ramesar S et al. Feasibility of the Mobile Mindfulness-Based Stress Reduction for Breast Cancer (mMBSR[BC]) Program for symptom improvement among breast cancer survivors. Psychooncology 27(2), 524–531 (2018).
36.
Lerman R, Jarski R, Rea H, Gellish R, Vicini F. Improving symptoms and quality of life of female cancer survivors: a randomized controlled study. Ann. Surg. Oncol. 19(2), 373–378 (2012).
37.
Witek-Janusek L, Albuquerque K, Chroniak KR, Chroniak C, Durazo-Arvizu R, Mathews HL. Effect of mindfulness based stress reduction on immune function, quality of life and coping in women newly diagnosed with early stage breast cancer. Brain Behav. Immun. 22(6), 969–981 (2008).
38.
Park S, Sado M, Fujisawa D et al. Mindfulness-based cognitive therapy for Japanese breast cancer patients – a feasibility study. Jpn J. Clin. Oncol. 48(1), 68–74 (2018).
Information & Authors
Information
Published In
Pages: 829 - 840
PubMed: 31166120
Copyright
© 2019 Future Medicine Ltd.
History
Received: 3 May 2018
Accepted: 17 May 2019
Published online: 5 June 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Effects of mindfulness-based interventions on quality of life of women with breast cancer: a systematic review. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0053
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Rithika Menon, T. S. Saranya, Impact of mindfulness practices to improve quality of life and mental health of persons diagnosed with breast cancer: a systematic review, Frontiers in Psychology, 10.3389/fpsyg.2025.1641751, 16, (2025).
- Kaina Zhou, Xiao Wang, Yan Wang, Ailan Liu, Effects of WeChat-based EPIC training on health-related quality of life, attribution and life attitude in women newly diagnosed with breast cancer: a clinical randomized controlled trial, Quality of Life Research, 10.1007/s11136-025-03959-2, 34, 7, (1979-1993), (2025).
- Arefeh Ebrahimi, Medi Basiri, Mehdi Mahmoodzadeh, Arezo Hajivosoogh, Moosa Sajadi, Effect of Online Mindfulness-Based Cognitive Therapy on Pain Severity and Life Quality in Women Receiving Treatment for Breast Cancer, Journal of Breast Diseases, 10.61186/ijbd.17.4.96, 17, 4, (96-116), (2025).
- SOMAYEH alinasab, najmeh hamid, Malek Mirhashemy, Comparing the effectiveness of Emotional Awareness and Expression Therapy with Acceptance and Commitment Therapy on Anger and Pain Intensity among Women with Breast Cancer, Journal of Breast Diseases, 10.61186/ijbd.17.4.117, 17, 4, (117-135), (2025).
- Fariba Hosseinzadeghan, Behnam Malkari, Nasim Talebi Azar, THE EFFECT OF MINDFULNESS-BASED COGNITIVE THERAPY (MBCT) ON THE QUALITY OF LIFE OF BURN PATIENTS: A CLINICAL TRIAL, Nursing and Midwifery Journal, 10.61186/unmf.22.9.763, 22, 9, (763-775), (2024).
- Mária Sováriová Soósová, Renáta Suchanová, Valéria Parová, Zdenka Hertelyová, Spiritual and religious interventions as a complementary and supportive therapy in women with breast cancer: an integrative literature review, Kontakt, 10.32725/kont.2024.011, 26, 1, (60-68), (2024).
- Kim Borsky, Fiona Tsang-Wright, Quality of Life and Patient Reported Outcomes in Breast Cancer, Patient Reported Outcomes and Quality of Life in Surgery, 10.1007/978-3-031-27597-5_11, (169-179), (2023).
- Fernando Urcola-Pardo, Incorporating Mindfulness Practice for Better Performance in Work and Daily Life, Brain, Decision Making and Mental Health, 10.1007/978-3-031-15959-6_16, (317-345), (2023).
- Jonathan Ying Ting Fung, Helen Lim, Nopporn Vongsirimas, Piyanee Klainin-Yobas, Effectiveness of eHealth mindfulness-based interventions on cancer-related symptoms among cancer patients and survivors: A systematic review and meta-analysis, Journal of Telemedicine and Telecare, 10.1177/1357633X221078490, 30, 3, (451-465), (2022).
- Chan-Young Kwon, Boram Lee, Sun-Yong Chung, Jong Woo Kim, Do Cochrane reviews reflect the latest evidence on meditation and mindfulness-based interventions? A snapshot of the current evidence, EXPLORE, 10.1016/j.explore.2020.05.016, 17, 6, (557-565), (2021).