Twelve-month healthcare utilization and expenditures in Medicare fee-for-service patients with clinically significant mitral regurgitation
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study sought to quantify the healthcare burden of Medicare patients with clinically significant mitral regurgitation (sMR). Materials & methods: Proxy definitions were used for sMR, including MR surgery, atrial fibrillation, pulmonary hypertension or >2 echocardiograms. Results: In this study, 11,173 patients had significant degenerative MR (sDMR); 25,402 had significant functional MR (sFMR); and 12,232 had significant uncharacterized MR (sUMR). Patients with sFMR (18,880) were more likely to be hospitalized and present to the emergency department compared with patients with sDMR (9,795) or sUMR (10,587). Annual healthcare expenditures for sMR patients were: US$29,328 for sFMR; US$17,112 for sUMR; and US$12,870 for sDMR. Conclusion: Novel therapeutic interventions merit further evaluation to reduce the substantial healthcare burden of sMR in the Medicare population.
Moderate-to-severe valvular heart disease is present in 2.5% of the USA population and increases with age, affecting 4–9% of people aged 65–75 years and 12–13% of those aged 75 years and older [1–3]. Mitral regurgitation (MR), defined as the backward flow of blood from the left ventricle into the left atrium, is the most common form of valvular heart disease in the USA (two- to three-times more common than aortic stenosis) [2,3]. Moderate or severe MR was estimated to affect between 2 and 2.5 million people in the USA in 2000. Because the prevalence of the disease increases with age (MR affects 9.3% of people aged 75 years and older compared with 1% of people aged 55–64 years) [2,3], that number is expected to nearly double by 2030 as the population grows and ages [3].
When assessing patients with MR, it is necessary to distinguish between two clinically recognized etiologies: primary, or degenerative MR (DMR) and secondary, or functional MR (FMR). In patients with DMR, at least one of the valve components (leaflets, chordae tendineae, papillary muscles or mitral valve [MV] annulus) is physically dysfunctional, which causes MV incompetence and systolic regurgitation of blood from the left ventricle back to the left atrium. Therefore, DMR is the result of a structural abnormality. It is most commonly related to MV prolapse [4], which has a prevalence of 2–3% in the population [5]. Chronic, severe DMR (sDMR) results in left ventricular dysfunction and volume overload, which eventually leads to heart failure (HF) and death [1,6,7]. In patients with FMR, the MV leaflets and chords are structurally normal (typically) and lack any degenerative deformities. Instead, FMR is associated with severe left ventricular dysfunction that causes inadequate leaflet coaptation, resulting in MR [8,9]. FMR is more common than DMR [10] and is associated with a worse prognosis [8].
Treatment of MR depends on several factors: etiology, symptomatology, effects on cardiac function and severity [9]. Currently, guidelines established by the American College of Cardiology and the American Heart Association [1] recommend that most patients with symptomatic DMR and/or left ventricular dysfunction be treated with surgical MV repair or replacement. However, the most effective interventions for chronic, severe FMR (sFMR) are not as well-defined. FMR is secondary in nature, and any process or pathology that affects left ventricular function (coronary, myocardial, other) can worsen the prognosis [1,7,8,11]. The dynamic nature of this disease makes treatment difficult, and variations in the diagnostic criteria and treatment for FMR are widespread [1,6,7].
The variability and inconsistency in optimal treatment pathways contribute to the substantial healthcare cost-burden associated with clinically significant MR (sMR). A 2016 study by Moore et al. [12] reported substantial overall valvular heart disease costs, with the greatest direct annual healthcare costs associated with MV disease. When aggregated to the USA population, the study found that patients with symptomatic MV disease and aortic valve disease had annual costs of US$7.6 and 5.6 billion, respectively. Patients with asymptomatic MV disease and aortic valve disease had annual costs of US$5.6 and 4.6 billion, respectively, yielding a total annual cost of US$23.4 billion for patients with valvular heart disease. Previous studies [3,12,13] have shown that MR is the most frequent type of valve disease in USA with prevalence increasing with age; most patients with MR are aged over 65 years. With the highest prevalence and increasing per-hospitalization costs, MV disease is considered the costliest valve disease in USA at US$13.2 billion annually. As the baby-boomer population ages, it will become increasingly important to understand MV disease and its impact on the elderly population from both a clinical and economic standpoint.
This study aims to build upon the Moore et al. [12] study by focusing on the healthcare burden of sMR in the Medicare population, which is not currently well-understood, and by sMR etiology. This study is a retrospective database analysis designed to describe the characteristics of all Medicare patients diagnosed with sMR and to quantify the healthcare burden of sMR.
Materials & methods
Data for this study were derived from the Medicare 5% Limited Dataset Standard Analytic Files for beneficiaries enrolled in fee-for-service Medicare from 1 January 2011 to 31 December 2016. These data contain detailed information from claims submitted by providers.
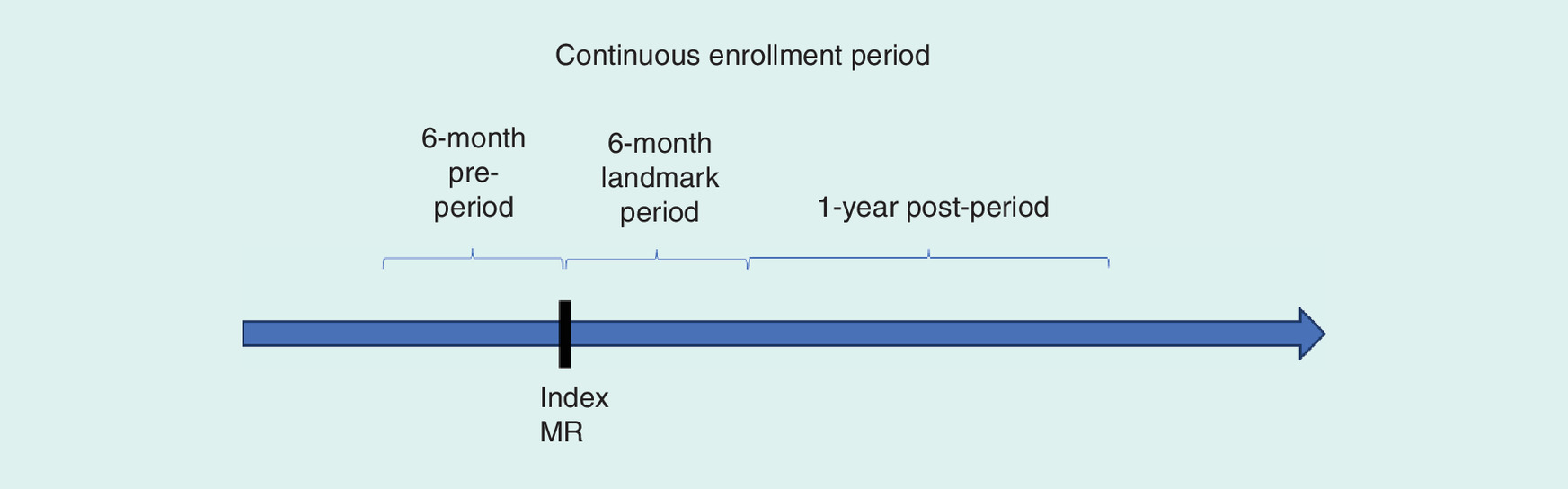
Patients were included in this study if they were enrolled in Medicare part A and B, had at least one inpatient or two outpatient claims with a diagnosis for MR in any position on the claim between 1 January 2011 and 31 December 2016 (see Supplementary Material for diagnosis codes), had at least 6 months of continuous enrollment before the first observed diagnosis of MR (baseline period) and 6 months of continuous enrollment after (landmark period), and were aged 18 years or older at index event (Figure 1). Patients were excluded if, at any time in the database, they had a record of at least one inpatient or two outpatient claims with a diagnosis for mitral stenosis or rheumatic insufficiency (see Supplementary Material for coding detail).
Medicare patients meeting all inclusion criteria were placed into three cohorts based on their disease etiology: FMR, DMR and uncharacterized MR (UMR). In clinical practice, patients are diagnosed with either FMR or DMR; UMR is not a recognized third etiology, and mostly represent lack of specification in the records. However, it is understood that patients with mixed etiologies exist and represent a fraction of that cohort. For this analysis, researchers did not have access to patients’ echocardiogram results – a primary diagnostic tool for determining whether a patient has FMR or DMR [5,8]. Consequently, while there are only two clinically recognized etiologies, three cohorts are used for this study that represent the full population of Medicare patients diagnosed with MR: FMR, DMR and UMR.
The index event was identified with the first inpatient admission or second outpatient visit with a diagnosis of MR. McCullough et al. [14] found this method to be accurate in 83% of patients diagnosed with HF based on a chart review in the claims-database driven REACH Study. The baseline period was defined by the 6-month, pre-index event period and the landmark period by the 6 months following the index event. Baseline and landmark periods were used to define etiology, severity and patient characteristics.
Cohorts were defined by the following algorithm (see Supplementary Tables for coding detail). First, patients with a record of chordal rupture were automatically classified as DMR, regardless of other criteria. Second, patients with a record of at least one inpatient or two outpatient claims for HF during the 6-month baseline or landmark period were classified as FMR. Third, patients with no record of at least one inpatient or two outpatient claims with a diagnosis of HF or ischemia during the baseline or landmark period were classified as DMR. Ischemia was defined as a record of coronary artery disease, acute myocardial infarction, coronary artery bypass grafting or percutaneous coronary intervention (angioplasty). For procedures, one outpatient claim was sufficient to qualify for an ischemia definition. Patients not meeting any of the previous criteria were classified as UMR.
Patients were further classified by clinical significance, which is a proxy for severity traditionally determined by an echocardiogram. Patients were considered to have sMR if they met any of the following criteria during the baseline or landmark period: a record of pulmonary hypertension or a record of atrial fibrillation. Patients were also considered to have sMR if, during the landmark period, any one of the following criteria were met: a record of chordal rupture; a record of MR surgery; or a record of two or more echocardiograms. The justification for two or more echocardiograms is based on the American College of Cardiology and the American Heart Association clinical guidelines [1] for valvular heart disease, which recommend that patients with sMR have an echocardiogram as frequently as every 6 months to 1 year. Patients not meeting the above criteria were considered non-sMR.
Patient demographics and comorbid conditions were summarized for all Medicare patients with sMR. The Charlson comorbidity index (CCI), a scale from 0 to 6 that predicts 10-year mortality derived from 19 comorbidity categories, was used as a measure of chronic-disease severity. Medicare patients with sMR and 12 months of continuous enrollment following the landmark period were evaluated for healthcare utilization in the form of emergency department (ED) visits, all-cause inpatient hospitalization, MR- or HF-related inpatient hospitalizations, and length of stay. ED visits and inpatient hospitalizations were classified based on the service location from the claim. Cause-specific hospitalizations were classified based on the relevant disease codes in the healthcare encounter of interest. All-cause hospitalizations accounted for all disease codes in the inpatient setting. Differences in baseline characteristics and outcomes were assessed by Pearson χ2 and one-way ANOVA tests, as appropriate, with an α-level of 0.05. To further understand the disease burden of these patients with sMR, annual healthcare expenditures were modeled using the log-γ model, which included patient demographics and the CCI as model covariates.
Results
Of the 3,586,154 patients in the total Medicare 5% sample from 1 January 2011 to 31 December 2016, only 2.8% of patients (99,675) met the initial MR inclusion criteria (Figure 2). Patients with DMR made up 34.5% (34,374) of the initial MR sample, with FMR at 36.4% (36,275) and UMR with the remaining 29.1% (29,026). Clinically significant criteria were applied to each sample size, resulting in the following sMR cohorts: 11,173 (32.5%) patients with sDMR, 25,402 (70.0%) patients with sFMR and 12,232 (42.1%) patients with significant UMR (sUMR). A very small percentage of patients were classified as clinically significant based on having a record of MV surgery in the landmark period. MV surgery rates by etiology were as follows: 0.68% of patients with sDMR (76 of 11,173), 1.13% of patients with sFMR (288 of 25,402) and 0.66% of patients with sUMR (81 of 12,232).
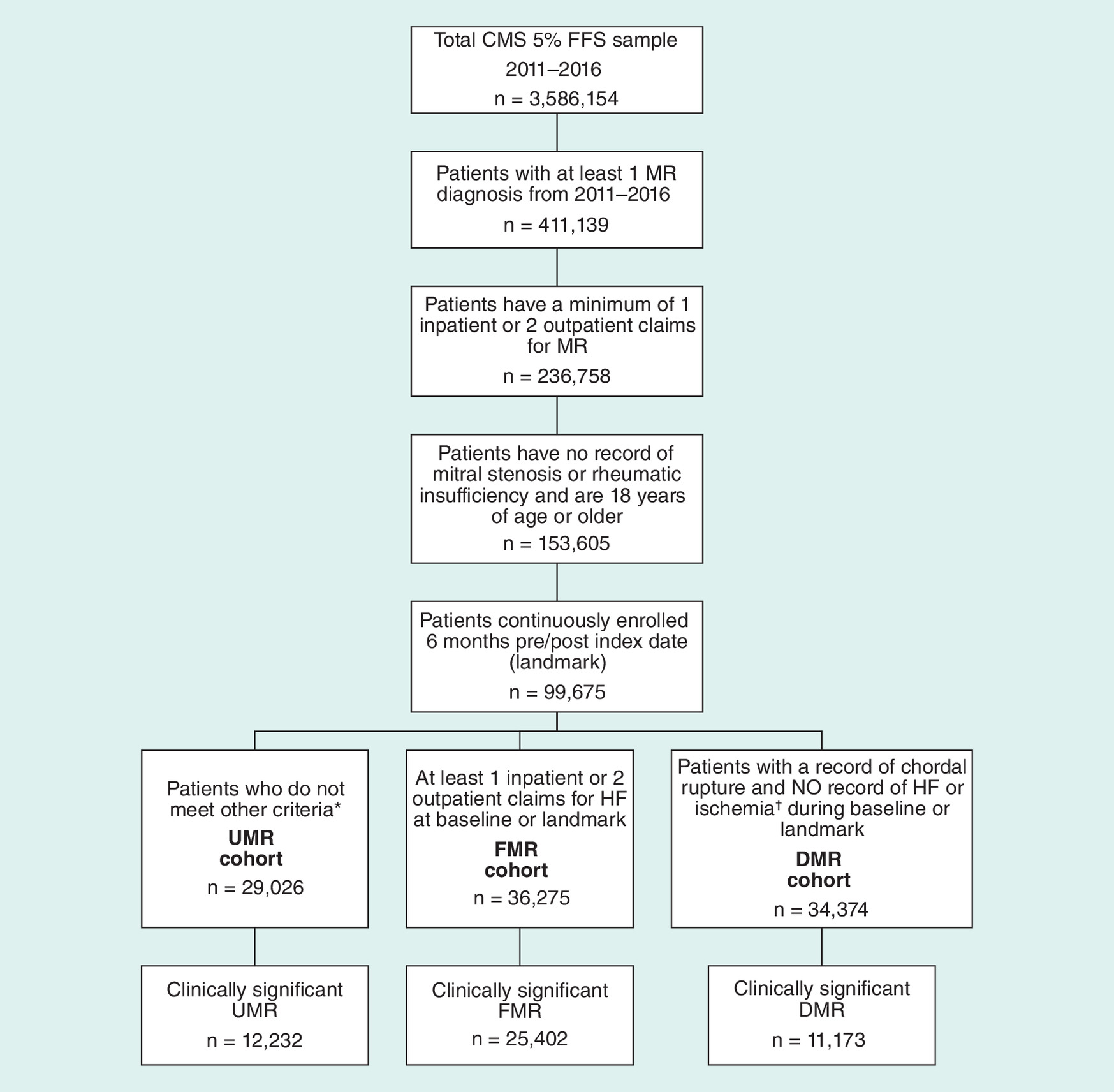
Figure 2. Patient attrition diagram.
*For example, a patient with one outpatient visit and a recorded diagnosis of HF or a record of ischemia without HF.
†Ischemia was defined as a record of coronary artery disease, acute myocardial infarction, coronary artery bypass grafting or percutaneous coronary intervention (angioplasty) during baseline or landmark period.
CMS: Centers for Medicare and medicaid service; DMR: Degenerative mitral regurgitation; FFS: Fee-for-service; FMR: Functional mitral regurgitation; HF: Heart failure; MR: Mitral regurgitation; UMR: Uncategorized mitral regurgitation.
The sFMR cohort was slightly older than the other two cohorts. The average age of the sFMR cohort was 76.1 years compared with an average age of 74.8 years for the sDMR cohort and 75.5 years for the sUMR cohort. Females made up more of the sDMR cohort (7077 [63.3%]) compared with sFMR (13,280 [52.3%]) or sUMR (5868 [48.0%]). The distributions of race, region and index year (first diagnosis of MR) were consistent across the three cohorts. Most patients were Caucasian: sDMR (9885 [88.5%]), sFMR (21,488 [84.6%]) and sUMR (10,861 [88.8%]). Geographically, the South had the highest percentage of patients at about 42% across the three cohorts (Table 1). Patients with sFMR were sicker with higher rates of peripheral vascular disease (49.8%), chronic pulmonary disease (69.9%), diabetes (54.1%) and renal disease (51.0%). The CCI for the sFMR cohort was 4.8, more than twice the 2.2 for sDMR and 2.6 for sUMR (Table 2). All baseline characteristics were statistically significantly different by cohort.
| Characteristics, number (%) | sDMR (n = 11,173) | sFMR (n = 25,402) | sUMR (n = 12,232) |
|---|---|---|---|
| Age, y | |||
| Mean (SD) | 74.8 (10.5) | 76.1 (10.8) | 75.5 (9.4) |
| Median | 75 | 77 | 76 |
| Sex | |||
| Female | 7077 (63.3) | 13,280 (52.3) | 5868 (48.0) |
| Male | 4096 (36.7) | 12,122 (47.7) | 6364 (52.0) |
| Race | |||
| Asian | 162 (1.4) | 315 (1.2) | 176 (1.4) |
| Black | 745 (6.7) | 2655 (10.5) | 764 (6.2) |
| Caucasian | 9885 (88.5) | 21,488 (84.6) | 10,861 (88.8) |
| Hispanic | 164 (1.5) | 473 (1.9) | 204 (1.7) |
| Unknown | 217 (1.9) | 471 (1.9) | 227 (1.9) |
| Region | |||
| Midwest | 2192 (19.6) | 5774 (22.7) | 2582 (21.1) |
| Northeast | 2388 (21.4) | 5144 (20.3) | 2628 (21.5) |
| South | 4616 (41.3) | 10,580 (41.7) | 5278 (43.1) |
| West | 1956 (17.5) | 3846 (15.1) | 1702 (13.9) |
| Unknown | 21 (0.2) | 58 (0.2) | 42 (0.3) |
| Index year | |||
| 2011 | 1561 (14.0) | 3806 (15.0) | 1881 (15.4) |
| 2012 | 2816 (25.2) | 6667 (26.3) | 3213 (26.3) |
| 2013 | 2519 (22.6) | 5716 (22.5) | 2684 (21.9) |
| 2014 | 2525 (22.6) | 5352 (21.0) | 2625 (21.5) |
| 2015 | 1752 (15.7) | 3861 (15.2) | 1829 (15.0) |
†
Some percentages may not add up to 100.0% due to rounding.
SD: Standard deviation; sDMR: Significant degenerative mitral regurgitation; sFMR: Significant functional mitral regurgitation; sUMR:Significant uncharacterized mitral regurgitation.
| Patient comorbidities | sDMR (n = 11,173) | sFMR (n = 25,402) | sUMR (n = 12,232) |
|---|---|---|---|
| Charlson comorbidity index | |||
| Mean (SD) | 2.2 (2.2) | 4.8 (2.1) | 2.6 (2.2) |
| Median | 2 | 4 | 2 |
| Comorbid conditions, n (%) | |||
| Acute myocardial infarction | 229 (2.1) | 9739 (38.3) | 3787 (31.0) |
| Congestive heart failure | 1845 (16.5) | 25,402 (100.0) | 3307 (27.0) |
| Peripheral vascular disease | 2963 (26.5) | 12,659 (49.8) | 5339 (43.7) |
| Cerebrovascular disease | 3753 (33.6) | 11,349 (44.7) | 5665 (46.3) |
| Dementia | 1002 (9.0) | 3699 (14.6) | 1318 (10.8) |
| Rheumatic disease | 801 (7.2) | 2100 (8.3) | 910 (7.4) |
| Chronic pulmonary disease | 4414 (39.5) | 17,749 (69.9) | 5632 (46.0) |
| Cancer | 2321 (20.8) | 5082 (20.0) | 2545 (20.8) |
| AIDS | 51 (0.5) | 105 (0.4) | 33 (0.3) |
| Diabetes | 3422 (30.6) | 13,752 (54.1) | 5288 (43.2) |
| Paraplegia and hemiplegia | 524 (4.7) | 1547 (6.1) | 612 (5.0) |
| Metastatic cancer | 449 (4.0) | 952 (3.8) | 418 (3.4) |
| Mild liver disease | 966 (8.7) | 3016 (11.9) | 1091 (8.9) |
| Moderate-severe liver disease | 127 (1.1) | 447 (1.8) | 106 (0.9) |
| Renal disease | 2153 (19.3) | 12,965 (51.0) | 3296 (27.0) |
| Peptic ulcer | 381 (3.4) | 1585 (6.2) | 612 (5.0) |
SD: Standard deviation; sDMR: Significant degenerative mitral regurgitation; sFMR: Significant functional mitral regurgitation; sUMR: Significant uncharacterized mitral regurgitation.
Healthcare utilization outcomes were measured at 12months postlandmark for patients who maintained continuous enrollment through the outcomes period (Table 3). Cohort population size decreased by about 20% at 1-year follow-up due to death or the data-time horizon not being sufficiently long for patients to meet the 1-year follow-up period. Further confirming their complexity, patients with sFMR had the highest utilization patterns in both the inpatient- and ED-setting. Of the 18,880 patients with sFMR with adequate follow-up, 40.8% (7694) visited the ED. The rates of ED visits for patients with sDMR and sUMR were lower than those of sFMR. Patients with sFMR also had higher rates of inpatient hospital admissions (8023 [42.5%]) when compared with patients with sDMR (2380 [24.3%]) or sUMR (3284 [31.0%]). However, average inpatient lengths of stay (in days) were similar across patients with sFMR, sDMR and sUMR (6.1, 5.2 and 5.1, respectively). All outcomes were statistically significantly different by cohort.
| Statistic, number (%)‡ | sDMR (n = 9795) | sFMR (n = 18,880) | sUMR (n = 10,587) |
|---|---|---|---|
| Patients with ED visits§ | |||
| All cause ED visits | 2985 (30.5) | 7694 (40.8) | 3784 (35.7) |
| Patients with INP hospital visits§ | |||
| All cause INP visits | 2380 (24.3) | 8023 (42.5) | 3284 (31.0) |
| All cause INP days | 2380 | 8023 | 3284 |
| LOS, days, mean (SD) | 5.2 (5.9) | 6.1 (8.3) | 5.1 (5.8) |
| LOS, days, median | 4 | 4.5 | 4 |
| HF INP visits | 315 (3.2) | 3464 (18.4) | 509 (4.8) |
| HF INP days | 622 | 5964 | 1000 |
| LOS, days, mean (SD) | 7.5 (10.6) | 6.7 (9.4) | 7.3 (11.4) |
| LOS, days, median | 5 | 5 | 5 |
| MR INP visits | 125 (1.3) | 553 (2.9) | 199 (1.9) |
| MR INP days | 4812 | 15,989 | 6356 |
| LOS, days, mean (SD) | 5.9 (8.9) | 8.4 (13.0) | 6.2 (14.1) |
| LOS, days, median | 4 | 5.5 | 4 |
†
Cohort populations (n-values) for each cohort are significantly less at 1-year follow-up because patients either died or were no longer enrolled.
‡
Statistics reported as number (%) unless otherwise noted.
§
Used to differentiate the categories of analysis.
ED: Emergency department; HF: Heart failure; INP: Inpatient; LOS: Length of stay; MR: Mitral regurgitation; SD: Standard deviation; sDMR: Significant degenerative mitral regurgitation; sFMR: Significant functional mitral regurgitation; sUMR: Significant uncategorized mitral regurgitation.
The results of multivariable expenditure models are displayed in Figure 3. After adjusting for all baseline demographics and the CCI, the annual healthcare expenditures were as follows: US$29,328 for sFMR; US$17,112 for sUMR; and US$12,870 for sDMR. Annual, all-cause healthcare expenditures were highest for patients with sFMR, which were more than double the costs incurred by patients with sDMR.
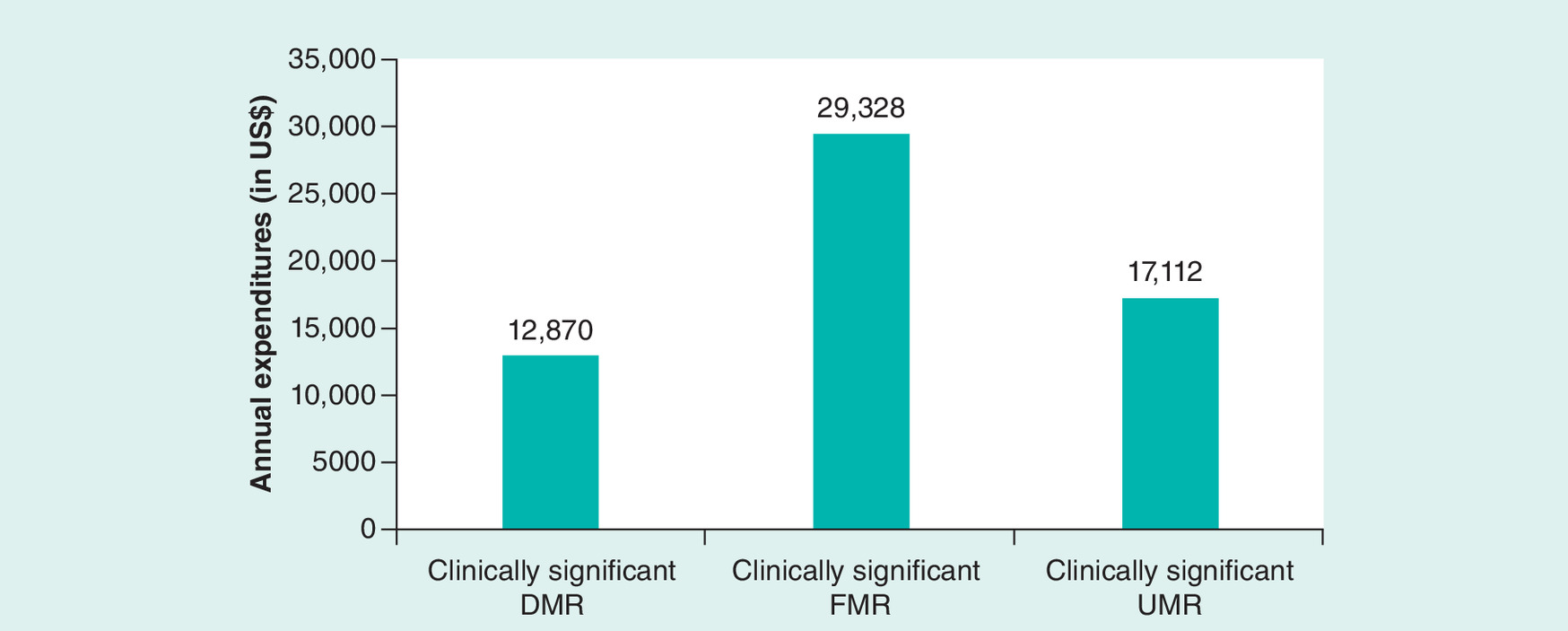
Figure 3. Burden of significant mitral regurgitation: results of multivariable model annual expenditures.
Multivariable model results show all-cause annual healthcare expenditures were highest for clinically significant FMR (US$29,328), followed by UMR (US$17,112) and then DMR with the lowest (US$12,870) expenditures incurred.
DMR: Degenerative mitral regurgitation; FMR: Functional mitral regurgitation; UMR: Uncharacterized mitral regurgitation.
Discussion
Medicare patients with sFMR were older, sicker, presented at the ED and inpatient hospital more frequently, and had higher 12-month healthcare expenditures than patients with sDMR and sUMR. This was expected, given the prevalence, complexity and high incidence of comorbid conditions associated with sFMR. The sUMR cohort had an intermediate risk of patient comorbid conditions and healthcare utilization when compared with the sFMR and sDMR cohort, which could be expected as patients with sUMR could represent a group of patients with sFMR or sDMR, although not specifically stated, and/or a group of patients with mixed characteristics of patients with sFMR and sDMR. In clinical practice where more patient information is available, this subset with UMR is labeled as primarily FMR or DMR, but for this retrospective claims analysis, it was important to separate these patients to better understand the burden of each MR cohort.
Healthcare utilization rates, including ED and inpatient visits, were higher for the sFMR cohort compared with the sDMR and sUMR cohorts. This likely contributed to the greater healthcare costs for patients with sFMR. Annual healthcare expenditures for the sFMR cohort (US$29,328) were significantly higher than both the sUMR (US$17,112) and sDMR (US$12,870) cohorts. These values are higher than those reported by Moore et al. [12], which showed total annual expenditures, including insurer and out-of-pocket costs, for symptomatic MV disease of US$13,550. These results are expected as older patients tend to have higher overall healthcare costs and our study was composed of exclusively Medicare patients, while only 37% of the symptomatic MV disease cohort in the Moore study were Medicare patients. As the baby-boomer population ages, the high clinical and economic burden of patients with sMR will only increase.
The breakdown of expenditures by sMR etiology is as expected due to the increasing complexity of the disease and the greater comorbidity profile of patients with sFMR versus sDMR in this study. Due to constraints of the available Medicare data, we were unable to attribute the higher overall costs of sFMR patients to any specific disease components, for example, HF, MR, interventions, etc. However, we did compare expenditures for patients with clinically sMR versus MR patients without clinically significant disease (nsMR) for all cohorts (DMR, FMR and UMR, respectively) (Figure 3). Those with sMR had a statistically significant increase in expenditure compared with nsMR, suggesting that clinically sMR alone is associated with higher healthcare costs, independent of MR etiology. Patients with both HF and MR are likely to have more severe disease than patients with MR alone. This could explain why patients in the sFMR group had higher healthcare expenditures. Our data further backs this notion, as patients in the UMR cohort (only one outpatient HF code) were seen to have lower healthcare expenditures and less severe HF compared with patients with FMR. Still, patients classified as UMR had higher costs than patients with DMR.
This study found that only a small percentage of patients with sMR underwent MV surgery during the landmark period. These findings support a common narrative in the literature: although MV repair is either indicated or may be reasonable in many cases of sMR (sDMR, sFMR or sUMR), patients rarely receive guideline-recommended interventions in a timely fashion [6,8,15,16]. A study [17] at the Cleveland Clinic from 2000 to 2008 found that only 36% of 814 patients with FMR had MV surgery, while another study [16] at the Mayo Clinic from 2000 to 2010 found that only 5% of 723 patients with FMR had MV surgery. Patients probably do not undergo recommended MV surgeries due to the high risk of complications or fear of prolonged, postoperative rehabilitation.
New treatment options should be evaluated given the clinical and economic burden of Medicare patients with sMR. Minimally-invasive surgical approaches for MV repair [18] may help treat patients who previously were not considered candidates for conventional MV surgery. Minimally-invasive techniques may reduce perioperative complications and mortality without compromising positive outcomes, in addition to potentially reducing the high costs associated with MV disease [12] by shortening recovery times and follow-up visits. A 2016 study by Downs et al. [19] found that, compared with conventional surgical approaches like open sternotomy, patients who underwent minimally-invasive MV surgery had fewer transfusions, shorter overall hospital lengths of stay, similar rates of mortality and stroke and similar costs.
Innovative transcatheter technologies, such as endovascular or percutaneous approaches for MV repair, show promise for improving clinical and economic outcomes for this undertreated population of MR patients. The COAPT study [20] examined the effect of a novel transcatheter MV repair among HF patients with moderate to severe MR (grade 3+ or 4+) on guideline-directed medical therapy (GDMT). The randomized control trial demonstrated important reductions in HF hospitalization rates and all-cause mortality at 24-month follow-up for patients receiving the device and GDMT compared with GDMT alone. The additional effect of the device translated to relative risk reductions of 47% for HF hospitalization and 38% for all-cause mortality. Reduction to MR grade of 2+ or lower (moderate MR) at one-year follow-up was observed in 46.9% of patients on GDMT alone versus 94.8% in the device group plus GDMT, which suggests the inadequacies of current treatment standards of GDMT alone. Treatment with transcatheter MV repair was also shown to reduce Medicare costs one year after intervention compared with pre-MV repair [21]. In addition to improving both clinical and economic outcomes, transcatheter technologies have the potential to increase patient access to therapy as they could treat patients who previously were not surgical candidates or whom decided to forgo surgical intervention due to the high risk. Transcatheter technologies are also promising for the treatment of elderly persons with MR – the population most affected by the disease but seldom offered surgery [4] due to underlying conditions [4,22]. With the potential to reduce the overall burden of MR disease, further studies and clinical trials are necessary to demonstrate the benefits of new, innovative technologies for treatment [1,7,10].
The limitations of this study are consistent with inherent weaknesses in retrospective database analyses, including potential undercoding of nonbillable events. Given its reliance on codes, the risk of coding errors is possible. Additionally, due to the administrative nature of the database, echocardiogram results were not available, and we could not define MR etiology or severity with clinical data. The absence of echocardiograms forced the creation of a third cohort (UMR), which is not a clinical entity in real-world clinical documentation. However, this cohort is believed to exhibit mixed features of FMR and DMR, both as a mixed population (patients with DMR or FMR, unspecified in the records), and as a mixed entity (patients with FMR and DMR). This differentiation was useful in this analysis to allow for more specific DMR and FMR cohorts. Misclassification of patients was also possible due to the proxy algorithms used for cohort criteria. For example, chordal rupture is not the only etiology of DMR, but was the only code available specific enough to include in the clinically significant DMR group. Also, HF could also be secondary to DMR, but our algorithm included all HF patients in the FMR group. The use of serial ECHOs to classify clinically sMR patients is also subject to misclassification as frequency of ECHO may be due to generally poor cardiovascular condition versus severe MR specifically. Utilization and expenditures were likely underestimated due to the continuous enrollment requirement in the 12-month post-landmark, which inherently excluded those who died in that time. Additionally, this survival bias may have been differential based on cohort status as FMR patients were more likely to have severe disease and thus, more likely to die early.
Significant mitral insufficiency is associated with substantial healthcare expenditures. Patients with sFMR were the most medically complex and most costly cohort studied, which is expected given its prevalence and associated comorbidities. Currently, surgical intervention is uncommon. New and innovative interventions should be made available to treat these patients and reduce the significant healthcare burden of MR on the Medicare population.
•
The healthcare burden of clinically significant mitral regurgitation (sMR) is not well understood.
•
We evaluated the burden of sMR in a Medicare population, by etiology of MR disease, using administrative data.
•
Patients were identified as having functional, degenerative or uncharacterized MR.
•
Clinically significant disease was evaluated by proxy variables, including MR surgery, atrial fibrillation, pulmonary hypertension or >2 echocardiograms.
•
In this study, 11,173 patients had significant degenerative MR (sDMR); 25,402 had significant functional MR (sFMR); and 12,232 had significant uncharacterized MR (sUMR).
•
Patients with sFMR (18,880) were more likely to be hospitalized and present to the emergency department compared with patients with sDMR (9,795) or sUMR (10,587).
•
Annual healthcare expenditures for sMR patients were: US$29,328 for sFMR; US$17,112 for sUMR; and US$12,870 for sDMR.
•
The main limitation of this study was the potential for misclassification due to the use of proxy variables for MR cohort identification and clinically significant disease.
•
Novel therapeutic interventions merit further evaluation to reduce the substantial healthcare burden of sMR in the Medicare population.
Financial & competing interests disclosure
J Van Houten, S Mollenkopf and P Verta are employees of and HS Mehta, DP Cork and C Gunnarsson are consultants to Edwards Lifesciences, the study sponsor. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
References
1.
Nishimura RA, Otto CM, Bonow RO et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation 135(25), e1159–e1195 (2017).
2.
Benjamin EJ, Blaha MJ, Chiuve SE et al. Heart disease and stroke statistics-2017 update: a report from the American Heart Association. Circulation 135(10), e146–e603 (2017).
3.
Nkomo VT, Gardin JM, Skelton TN et al. Burden of valvular heart diseases: a population-based study. Lancet 368(9540), 1005–1011 (2006).
4.
Enriquez-Sarano M, Akins CW, Vahanian A. Mitral regurgitation. Lancet 373(9672), 1382–1394 (2009).
5.
Helms AS, Bach DS. Heart valve disease. Prim. Care 40(1), 91–108 (2013).
6.
Bach DS, Awais M, Gurm HS et al. Failure of guideline adherence for intervention in patients with severe mitral regurgitation. J. Am. Coll. Cardiol. 54(9), 860–865 (2009).
7.
Carabello BA. The current therapy for mitral regurgitation. J. Am. Coll. Cardiol. 52(5), 319–326 (2008).
8.
Asgar AW, Mack MJ, Stone GW. Secondary mitral regurgitation in heart failure: pathophysiology, prognosis, and therapeutic considerations. J. Am. Coll. Cardiol. 65(12), 1231–1248 (2015).
9.
Hussaini A, Kar S. Percutaneous mitral valve repair: potential in heart failure management. Curr. Heart Fail. Rep. 7(1), 22–26 (2010).
10.
de Marchena E, Badiye A, Robalino G et al. Respective prevalence of the different carpentier classes of mitral regurgitation: a stepping stone for future therapeutic research and development. J. Card. Surg. 26(4), 385–392 (2011).
11.
Ahmed MI, McGiffin DC, O'Rourke RA et al. Mitral regurgitation. Curr. Probl. Cardiol. 34(3), 93–136 (2009).
12.
Moore M, Chen J, Mallow PJ et al. The direct health-care burden of valvular heart disease: evidence from US national survey data. Clinicoecon. Outcomes Res. 8, 613–627 (2016).
13.
National Center for Health Statistics (US). Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities. Hyattsville, MD, USA (2016).
14.
McCullough PA, Philbin EF, Spertus JA et al. Confirmation of a heart failure epidemic: findings from the Resource Utilization Among Congestive Heart Failure (REACH) study. J. Am. Coll. Cardiol. 39(1), 60–69 (2002).
15.
Adams DH, Rosenhek R, Falk V. Degenerative mitral valve regurgitation: best practice revolution. Eur. Heart J. 31(16), 1958–1966 (2010).
16.
Dziadzko V, Clavel MA, Dziadzko M et al. Outcome and undertreatment of mitral regurgitation: a community cohort study. Lancet 391(10124), 960–969 (2018).
17.
Goel SS, Bajaj N, Aggarwal B et al. Prevalence and outcomes of unoperated patients with severe symptomatic mitral regurgitation and heart failure: comprehensive analysis to determine the potential role of MitraClip for this unmet need. J. Am. Coll. Cardiol. 63(2), 185–186 (2014).
18.
Welp H, Martens S. Minimally invasive mitral valve repair. Curr. Opin. Anaesthesiol. 27(1), 65–71 (2014).
19.
Downs EA, Johnston LE, LaPar DJ et al. Minimally invasive mitral valve surgery provides excellent outcomes without increased cost: a multi-institutional analysis. Ann. Thorac. Surg. 102(1), 14–21 (2016).
20.
Stone GW, Lindenfeld J, Abraham WT et al. Transcatheter mitral-valve repair in patients with heart failure. N. Engl. J. Med. 379(24), 2307–2318 (2018).
21.
Vemulapalli S, Lippmann SJ, Krucoff M et al. Cardiovascular events and hospital resource utilization pre- and post-transcatheter mitral valve repair in high-surgical risk patients. Am. Heart J. 189, 146–157 (2017).
22.
Iung B, Baron G, Butchart EG et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on valvular heart disease. Eur. Heart J. 24(13), 1231–1243 (2003).
Information & Authors
Information
Published In
Pages: 1089 - 1097
PubMed: 31588786
Copyright
© 2019 Future Medicine Ltd.
History
Received: 15 February 2019
Accepted: 6 August 2019
Published online: 7 October 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Twelve-month healthcare utilization and expenditures in Medicare fee-for-service patients with clinically significant mitral regurgitation. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0026
Export citation
Select the citation format you wish to export for this article or chapter.