Hospitalization risk factors in antipsychotic-treated schizophrenia, bipolar I disorder or major depressive disorder
Abstract
Aim: To examine hospitalization risk factors in antipsychotic-treated patients with schizophrenia, bipolar I disorder (BD-I) or major depressive disorder (MDD). Patients & methods: Using Truven Health MarketScan® Commercial, Medicaid and Medicare Supplemental data (01/01/2012–06/30/2016), logistic regression models were performed to identify risk factors for both psychiatric and all-cause hospitalization in three separate analyses. Results: Significant risk factors included prior hospitalization (schizophrenia: odds ratio [95% CI]: 2.83 [2.50–3.21; psychiatric]; 2.58 [2.31–2.87; all-cause]; BD-I: 2.42 [2.23–2.63]; 2.09 [1.96–2.23]; MDD: 2.81 [2.49–3.16]; 2.21 [2.03–2.40]), previous antipsychotic treatment (schizophrenia: 1.71 [1.52–1.93]; 1.31 [1.18–1.46]; BD-I: 1.33 [1.23–1.44]; 1.22 [1.14–1.30]; MDD: 1.31 (1.11–1.54); 1.17 (1.04–1.32) and substance abuse (schizophrenia: 1.42 [1.27–1.60]; 1.37 [1.23–1.53]; BD-I: 1.72 [1.58–1.86]; 1.61 [1.50–1.72]; MDD: 1.90 [1.68–2.15] and 1.55 [1.41–1.71]). Conclusion: Prior hospitalization, previous antipsychotic treatment and substance abuse were associated with increased hospitalization risk in schizophrenia, BD-I or MDD.
In 2016, it was estimated that 18.3% of adults in the USA (44.7 million adults) suffered from a mental illness [1]. Schizophrenia, bipolar disorder (BD) and major depressive disorder (MDD) are among the most severe mental illnesses, resulting in significant morbidity. Antipsychotics are the cornerstone of pharmacologic treatment for schizophrenia, and have been increasingly used to treat patients with severe BD and MDD [2–6]. Even with treatment (i.e., antipsychotic treatment in any form), relapse rates are high [7–9]. Relapses can be devastating, potentially reducing quality of life, worsening disease prognosis and increasing caregiver burden, and healthcare costs [6,10–12].
Exploration of factors related to treatment response and relapse among patients with severe mental illness is required for improving outcomes and reducing healthcare and societal costs in schizophrenia, BD and MDD. Hospitalization, which has been used as a proxy for relapse, is common among patients with schizophrenia, BD or MDD [6,13]. Several known risk factors may predict hospitalization [14] and/or re-hospitalization, including younger age [15], male gender [16] antipsychotic drug formulation (e.g., oral vs long-acting injectable) and nonadherence [17–21], medication nonresponse [18], substance abuse [7,14,15,19,22–26], a longer duration of hospitalization [16,27], prior hospitalization [13,28–31], multiple and more recent (vs distant) hospitalizations [32], being discharged against medical advice [30] and living in a supervised setting [31].
Most of the existing studies about risk factors of hospitalizations did not target patients who were treated with antipsychotics. These patients tend to be more severe than those without such treatments [33]. And no such data is available among patients with severe MDD treated with antipsychotics, based on our PubMed search. Therefore, in this study, we used more recent, nationally representative data to conduct three separate retrospective analyses examining factors associated with increased risk for both all-cause and psychiatric hospitalizations after initiating a new antipsychotic treatment in a group of commercially, Medicaid or Medicare-insured patients with severe schizophrenia, bipolar I disorder (BD-I) or MDD. Such information may allow for better identification (ID) of at-risk patients and more efficient allocation of limited healthcare resources targeting this patient population.
Patients & methods
Data sources
Data from the Truven Health MarketScan® commercial, Medicaid and Medicare Supplemental databases (MarketScan is a registered trademark of Truven Health Analytics, part of the IBM Watson Health business) were used for analyses, all of which are Health Insurance Portability and Accountability Act (HIPAA)-compliant administrative claims databases.
The Medicaid database contains the pooled healthcare experience of approximately 40 million Medicaid enrollees from multiple states. It includes inpatient and outpatient services and outpatient prescription drug claims, as well as information on enrollment, long-term care and other medical care. In addition to standard demographic variables such as age and sex, the database includes variables of particular value to researchers investigating Medicaid populations (such as ethnicity, maintenance assistance status and Medicare eligibility).
The commercial data included medical encounters from approximately 65 million individuals and their dependents insured by employer-sponsored plans (i.e., non-Medicare eligible). Coverage was provided under a variety of fee-for-service, fully capitated and partially capitated health plans, including preferred provider organizations, point of service plans, indemnity plans and health maintenance organizations.
The Medicare supplemental data included about 5.3 million Medicare-eligible retired employees and their spouses with employer-sponsored Medicare supplemental plans.
The data used for all analyses were from 1 January 2012 to 30 June 2016. Given the de-identified nature of the data used in the present study, informed consent was not required by Health Insurance Portability and Accountability Act (HIPAA) rules.
Study population & measures
To be included in the schizophrenia cohort, adult patients ≥18 years of age were required to have at least one inpatient claim or at least two outpatient claims for schizophrenia disorders (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM] code: 295.xx, excluding 295.4x and 295.7x; or 10th Revision [ICD-10-CM] code: F20x, excluding F20.81) in any diagnosis field of a claim during the study period and received a prescription for an antipsychotic treatment during the ID period from 1 January 2013 to 30 June 2015. In this study, we use the term ‘diagnosis’ when a patient received at least one inpatient claim or at least two outpatient claims for the disease of interest (i.e., the claims-based criteria for that disease were met). Patients with both existing and newly diagnosed schizophrenia were included. The index date was the start date of the antipsychotic treatment in the ID period. The antipsychotics prescribed on the index date included both first-generation (i.e., chlorpromazine, fluphenazine, haloperidol, loxapine, perphenazine, pimozide, prochlorperazine, thioridazine, thiothixene and trifluoperazine) and second-generation (i.e., aripiprazole, asenapine, iloperidone, lurasidone, olanzapine, paliperidone, quetiapine, risperidone, and ziprasidone) ones. Patients were allowed to have nonindex antipsychotic treatment during the 12 months prior to the index date (baseline period).
Analogous ID and selection criteria were applied to patients with BD-I (ICD-9-CM code: 296.0x, 296.1x, 296.4x, 296.5x, 296.6x, 296.7x, 296.8x, excluding 296.82; ICD-10-CM code: F30.x, F31.x, excluding F31.81) or MDD (ICD-9-CM code: 296.2x, 296.3x; ICD-10-CM: F32.0-F32.5, F32.9, F33.0x-F33.4x, F33.9x). Patients with MDD were required to have antipsychotics as an adjunctive treatment with antidepressant medications during the ID period (Figure 1).
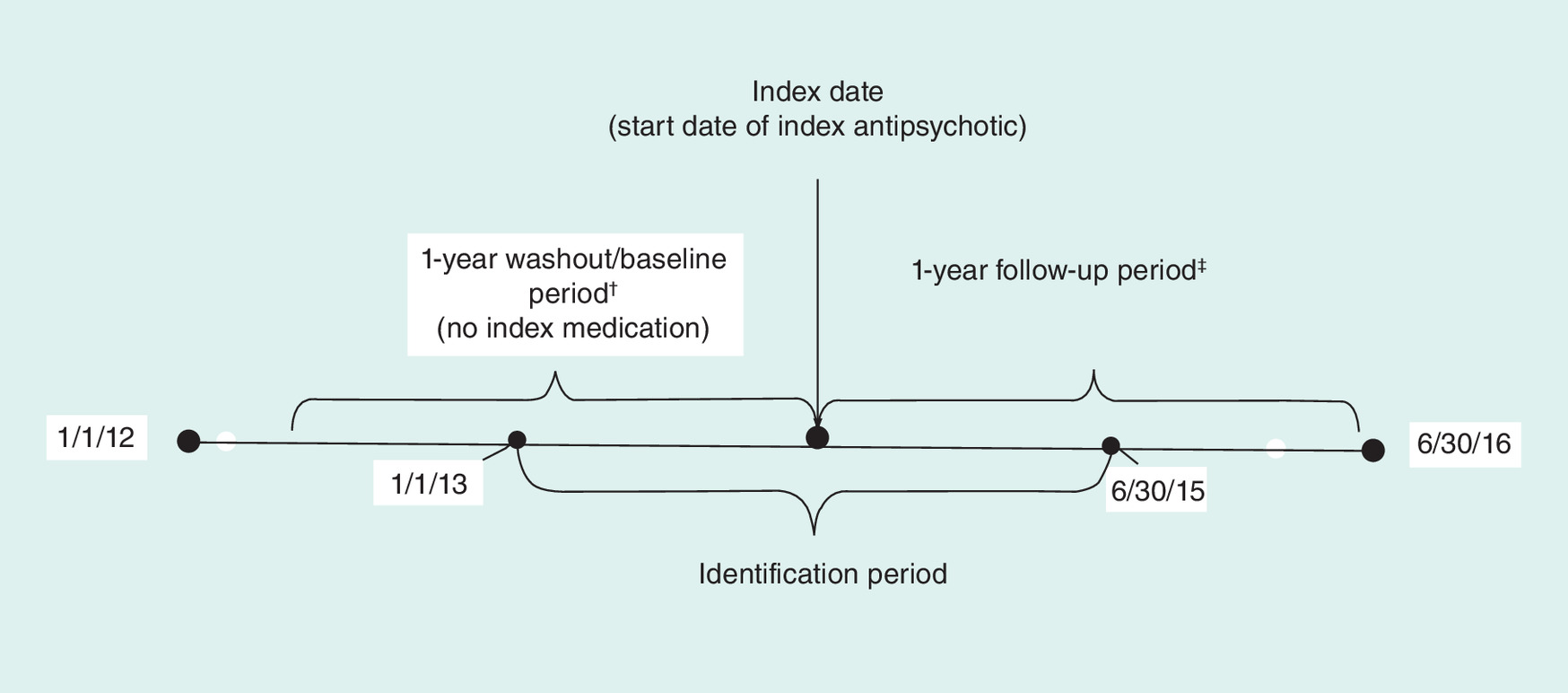
Figure 1. Study timeline for patients with schizophrenia, bipolar I disorder or major depressive disorder.
†12 months before (baseline) the index date.
‡12 months after the index date.
Patients in all cohorts were required to be ≥18 years of age on the index date and have continuous enrollment in a health plan for the 12 months before (baseline) and after (follow-up) the index date. The first diagnosis date for each disease of interest occurred prior to or on the index date. To ensure complete medication claims histories, patients with Medicare dual eligibility and those without mental health coverage were excluded. Patients hospitalized within 7 days of the index date were excluded because we aimed to include only community-dwelling patients in this study and patients who had a prescription for clozapine any time during the study period were excluded since clozapine is indicated for treatment of patients who fail to respond adequately to standard antipsychotic treatment. Additionally, we excluded patients with concomitant schizophrenia diagnosis from the BD-I cohort and patients with concomitant schizophrenia and/or BD-I from the MDD cohort.
Potential baseline risk factors
Guided by literature review and availability of variables in our datasets, we identified the potential baseline risk factors which could contribute to all-cause or psychiatric hospitalization during the 1-year follow-up period. Sociodemographic variables included age, gender and insurance type. General disease burden was measured using Charlson Comorbidity Index (CCI) [34] and number of Healthcare Cost and Utilization Project (HCUP) chronic condition indicators [35]; somatic comorbidities included obesity and diabetes mellitus, and were identified by the presence of a single code for the relevant condition. Somatic medication use included antidiabetic medications, lipid lowering medications and antihypertensive medications. Psychiatric comorbidities included BD (in the cohort of patients with schizophrenia), MDD (in the cohorts of patients with schizophrenia or BD-I), personality disorder, anxiety and substance abuse. BD and MDD were identified based on having at least one inpatient or two outpatient claims for the specific disease, while personality disorder, anxiety and substance abuse were identified by the presence of a single code for the relevant condition. Psychiatric medication use included antidepressants (in the group of patients with schizophrenia or BD-I), anti-anxiety medications, mood stabilizers, sedatives or hypnotics and nonindex antipsychotics. Presence of any hospitalizations was also included as a potential baseline risk factor.
All-cause & psychiatric hospitalization
All-cause hospitalization was defined as having any hospitalization during the 1-year follow-up period. Psychiatric hospitalization was defined as having a primary diagnosis of any mental disorder (ICD-9-CM code: 209.xx-311.xx; ICD-10-CM code: F01.xx-F99.xx) during the 1-year follow-up period.
Statistical analysis
Descriptive statistics including means, standard deviations and relative frequencies, and percentages for continuous and categorical data, respectively, were reported for all cohorts.
Multivariate logistic regression models were conducted to identify potential risk factors for all-cause and psychiatric hospitalizations during the 1-year follow-up period. All data transformations and statistical analyses were performed using SAS© version 9.4.
Results
The final study sample included 8574 patients with schizophrenia, 29,621 patients with BD-I and 20,020 patients with MDD (Table 1).
| Demographics | Schizophrenia | BD-I | MDD |
|---|---|---|---|
| n (%) | 8574 (100.0) | 29,621 (100.0) | 20,020 (100.0) |
| Age (years): | |||
| – Mean (SD) | 43.7 (15.5) | 41.4 (15.3) | 48.2 (16.8) |
| – Median | 45 | 42 | 50 |
| Age (years) no. (%): | |||
| – 18–34 | 2844 (33.2) | 10,648 (35.9) | 4389 (21.9) |
| – 35–44 | 1408 (16.4) | 6125 (20.7) | 3446 (17.2) |
| – 45–54 | 1952 (22.8) | 6495 (21.9) | 4801 (24.0) |
| – 55–64 | 1804 (21.0) | 4862 (16.4) | 4875 (24.4) |
| – 65+ | 566 (6.6) | 1491 (5.0) | 2509 (12.5) |
| Female, no. (%) | 4067 (47.4) | 19,981 (67.5) | 13547 (67.7) |
| Region, no. (%): | |||
| – Midwest | 596 (7.0) | 4885 (16.5) | 4236 (21.2) |
| – Northeast | 426 (5.0) | 4421 (14.9) | 3862 (19.3) |
| – South | 735 (8.6) | 9218 (31.1) | 7426 (37.1) |
| – West | 216 (2.5) | 2719 (9.2) | 1993 (10.0) |
| – Unknown (Medicaid) | 6601 (77.0) | 8378 (28.3) | 2503 (12.5) |
| Race, no. (%): | |||
| – White | 2031 (23.7) | 5636 (19.0) | 1498 (7.5) |
| – Black | 3392 (39.6) | 1475 (5.0) | 577 (2.9) |
| – Other | 1178 (13.7) | 1267 (4.3) | 428 (2.1) |
| – Unknown (Commercial/Medicare supplemental) | 1973 (23.0) | 21,243 (71.7) | 17,517 (87.5) |
| Insurance type, no. (%): | |||
| – Medicaid | 6601 (77.0) | 8378 (28.3) | 2503 (12.5) |
| – Commercial | 1456 (17.0) | 19,349 (65.3) | 14,788 (73.9) |
| – Medicare supplemental | 517 (6.0) | 1894 (6.4) | 2729 (13.6) |
BD-I: Bipolar I disorder; MDD: Major depressive disorder; SD: Standard deviation.
Schizophrenia, BD-I and MDD patients had substantial comorbidities. For example, 16.7, 13.6 and 11.7% had obesity, respectively; and 23.2, 13.6 and 15.5% had Type II diabetes mellitus, respectively (Table 2).
| Comorbidities and medications | Schizophrenia | BD-I | MDD |
|---|---|---|---|
| n | 8574 | 29,621 | 20,020 |
| Psychiatric comorbidities, no. (%) | 5745 (67.0) | 19,820 (66.9) | 12,127 (60.6) |
| BD-I | 3139 (36.6) | – | – |
| MDD | 1831 (21.4) | 9091 (30.7) | – |
| Anxiety | 2874 (33.5) | 14,382 (48.6) | 10,941 (54.7) |
| Personality disorder | 801 (9.3) | 1824 (6.2) | 559 (2.8) |
| Substance abuse | 2767 (32.3) | 7004 (23.6) | 3241 (16.2) |
| Obesity, no. (%) | 1434 (16.7) | 4038 (13.6) | 2344 (11.7) |
| Diabetes mellitus Type II, no. (%) | 1987 (23.2) | 4040 (13.6) | 3108 (15.5) |
| Psychiatric medications, no. (%) | 5493 (64.1) | 25,322 (85.5) | 19,035 (95.1) |
| Somatic medications, no. (%) | 3915 (45.7) | 13,391 (45.2) | 10,755 (53.7) |
| Any baseline inpatient hospitalization, no. (%) | 4039 (47.1) | 10,013 (33.8) | 6495 (32.4) |
| Nonindex antipsychotics, no. (%) | 4710 (54.9) | 8232 (27.8) | 1987 (9.9) |
BD-I: Bipolar I disorder; MDD: Major depressive disorder.
Among patients with schizophrenia, in the follow-up period, 33.7% had at least one all-cause hospitalization and 23.6% had at least one psychiatric hospitalization (not shown in table). In risk-adjusted models, factors predicting both psychiatric and all-cause hospitalization included: having a prior hospitalization (odds ratio [OR; 95% CI]: 2.83 [2.50–3.21; psychiatric]; 2.58 [2.31–2.87; all-cause]); previous treatment with nonindex antipsychotics (1.71 [1.52–1.93]; 1.31 [1.18–1.46]); substance abuse (1.42 [1.27–1.60]; 1.37 [1.23–1.53]); and having at least one inpatient claim or two outpatient claims for psychiatric comorbidities, including BD-I (1.30 [1.16–1.46]; 1.19 [1.07–1.33]), personality disorders (1.38 [1.17–1.63]; 1.21 [1.03–1.42]), MDD (1.22 [1.07–1.38]; 1.27 [1.13–1.43]), and anxiety (1.20 [1.07–1.35]; 1.12 [1.01–1.25]). Also, younger age (18–34 vs 55+) predicted psychiatric hospitalization (OR; 95% CI): 1.30 (1.1–1.55; Table 3).
| Effect | All-cause inpatient hospitalization in post 1 year | Psychiatric inpatient hospitalization in post 1 year | ||
|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |
| Schizophrenia | ||||
| Age group: | ||||
| – 18–34 vs 55+ | 1.06 (0.90–1.23) | 0.495 | 1.30 (1.10–1.55) | 0.002 |
| – 35–44 vs 55+ | 0.88 (0.75–1.04) | 0.138 | 1.05 (0.87–1.26) | 0.612 |
| – 45–54 vs 55+ | 1.00 (0.87–1.16) | 0.980 | 1.11 (0.94–1.30) | 0.232 |
| Female vs male | 1.00 (0.90–1.11) | 0.981 | 0.97 (0.87–1.09) | 0.609 |
| Insurance type: | ||||
| – MCD vs COM | 1.09 (0.95–1.25) | 0.219 | 0.89 (0.77–1.03) | 0.125 |
| –MCR vs COM | 1.28 (1.01–1.63) | 0.044 | 0.75 (0.56–1.00) | 0.046 |
| Modified CCI without DM | 1.08 (1.04–1.12) | <.001 | 0.99 (0.96–1.04) | 0.787 |
| No. HCUP chronic conditions | 1.07 (1.03–1.10) | <.001 | 1.00 (0.96–1.03) | 0.792 |
| BD (y vs n) | 1.19 (1.07–1.33) | 0.001 | 1.30 (1.16–1.46) | <0.001 |
| MDD (y vs n) | 1.27 (1.12–1.43) | <.001 | 1.22 (1.07–1.38) | 0.003 |
| Anxiety (y vs n) | 1.12 (1.01–1.25) | 0.038 | 1.20 (1.07–1.35) | 0.003 |
| Personality disorder (y vs n) | 1.21 (1.03–1.42) | 0.020 | 1.38 (1.17–1.63) | <0.001 |
| Substance abuse disorders (y vs n) | 1.37 (1.23–1.53) | <.001 | 1.42 (1.27–1.60) | <.001 |
| Obesity (y vs n) | 0.97 (0.85–1.12) | 0.696 | 1.03 (0.89–1.20) | 0.665 |
| Diabetes mellitus Type II (y vs n) | 1.19 (1.05–1.36) | 0.007 | 1.10 (0.95–1.27) | 0.198 |
| Any baseline inpatient hospitalization (y vs n) | 2.58 (2.31–2.87) | <.001 | 2.83 (2.50–3.21) | <.001 |
| Psychiatric medications (y vs n) | 1.18 (1.04–1.33) | 0.008 | 1.10 (0.96–1.26) | 0.161 |
| Somatic medications (y vs n) | 0.92 (0.82–1.04) | 0.208 | 0.85 (0.74–0.97) | 0.016 |
| Nonindex antipsychotic use (y vs n) | 1.31 (1.18–1.46) | <.001 | 1.71 (1.52–1.93) | <.001 |
| BD-I | ||||
| Age group: | ||||
| – 18–34 vs 55+ | 1.10 (1.00–1.21) | 0.052 | 1.50 (1.33–1.70) | <0.001 |
| – 35–44 vs 55+ | 0.87 (0.78–0.96) | 0.006 | 1.11 (0.97–1.27) | 0.114 |
| – 45–54 vs 55+ | 0.93 (0.84–1.02) | 0.109 | 1.13 (0.99–1.27) | 0.060 |
| Female vs male | 1.06 (0.99–1.13) | 0.073 | 0.95 (0.88–1.03) | 0.184 |
| Insurance type: | ||||
| – MCD vs COM | 0.98 (0.92–1.05) | 0.602 | 0.65 (0.59–0.71) | <0.001 |
| – MCR vs COM | 1.35 (1.19–1.53) | <.001 | 0.81 (0.68–0.97) | 0.021 |
| Modified CCI without DM | 1.09 (1.07–1.11) | <.001 | 1.01 (0.99–1.04) | 0.368 |
| No. HCUP chronic conditions | 1.11 (1.09–1.13) | <.001 | 1.01 (0.99–1.04) | 0.224 |
| MDDs (y vs n) | 1.13 (1.06–1.20) | <.001 | 1.32 (1.22–1.42) | <0.001 |
| Anxiety (y vs n) | 1.07 (1.00–1.14) | 0.040 | 1.13 (1.05–1.22) | 0.002 |
| Personality disorder (y vs n) | 1.15 (1.03–1.28) | 0.015 | 1.50 (1.33–1.70) | <0.001 |
| Substance abuse disorders (y vs n) | 1.61 (1.50–1.72) | <.001 | 1.72 (1.58–1.86) | <0.001 |
| Obesity (y vs n) | 1.01 (0.93–1.10) | 0.858 | 0.94 (0.84–1.05) | 0.294 |
| Diabetes mellitus Type II (y vs n) | 1.23 (1.13–1.34) | <.001 | 1.26 (1.13–1.41) | <0.001 |
| Any baseline inpatient hospitalization (y vs n) | 2.09 (1.96–2.23) | <.001 | 2.42 (2.23–2.63) | <0.001 |
| Psychiatric medications (y vs n) | 1.17 (1.07–1.29) | 0.001 | 1.17 (1.04–1.31) | 0.010 |
| Somatic medications (y vs n) | 1.05 (0.98–1.13) | 0.153 | 1.09 (1.00–1.19) | 0.056 |
| Nonindex antipsychotics use (y vs n) | 1.22 (1.14–1.30) | <.001 | 1.33 (1.23–1.44) | <0.001 |
| MDD | ||||
| Age group: | ||||
| – 18–34 vs 55+ | 1.23 (1.08–1.40) | 0.002 | 1.58 (1.33–1.89) | <.001 |
| – 35–44 vs 55+ | 0.90 (0.79–1.03) | 0.134 | 1.12 (0.94–1.35) | 0.214 |
| – 45–54 vs 55+ | 0.94 (0.84–1.05) | 0.287 | 1.06 (0.90–1.24) | 0.506 |
| Female vs male | 1.00 (0.92–1.08) | 0.904 | 0.84 (0.76–0.94) | 0.003 |
| Insurance type: | ||||
| – MCD vs COM | 1.30 (1.16–1.45) | <.001 | 0.71 (0.60–0.85) | <.001 |
| – MCR vs COM | 1.53 (1.36–1.73) | <.001 | 0.79 (0.65–0.96) | 0.018 |
| Modified CCI without DM | 1.09 (1.06–1.12) | <.001 | 1.00 (0.97–1.04) | 0.892 |
| No. HCUP chronic conditions | 1.12 (1.09–1.15) | <.001 | 1.01 (0.98–1.05) | 0.540 |
| Anxiety (y vs n) | 1.06 (0.98–1.15) | 0.136 | 1.26 (1.12–1.41) | <.001 |
| Personality disorder (y vs n) | 0.97 (0.79–1.20) | 0.796 | 1.21 (0.94–1.57) | 0.136 |
| Substance abuse disorders (y vs n) | 1.55 (1.41–1.71) | <.001 | 1.90 (1.68–2.15) | <.001 |
| Obesity (y vs n) | 1.00 (0.89–1.12) | 0.969 | 0.85 (0.71–1.02) | 0.073 |
| Diabetes mellitus Type II (y vs n) | 1.21 (1.09–1.34) | <.001 | 1.13 (0.97–1.32) | 0.123 |
| Any baseline inpatient hospitalization (y vs n) | 2.21 (2.03–2.40) | <.001 | 2.81 (2.49–3.16) | <.001 |
| Psychiatric medications (y vs n) | 1.09 (0.91–1.31) | 0.358 | 1.21 (0.95–1.56) | 0.125 |
| Somatic medications (y vs n) | 1.18 (1.07–1.30) | <.001 | 1.12 (0.98–1.27) | 0.101 |
| Nonindex antipsychotics use (y vs n) | 1.17 (1.04–1.32) | 0.009 | 1.31 (1.11–1.54) | 0.001 |
BD: Bipolar disorder; CCI: Charlson Comorbidity Index; COM: Commercial; DM: Diabetes mellitus; HCUP: Healthcare Cost and Utilization Project; MCD: Medicaid; MCR: Medicare Supplemental; MDD: Major depressive disorder; OR: Odds ratio.
Among patients with BD-I, in the follow-up period, 21.6% of patients had at least one all-cause hospitalization and 12.3% had at least one psychiatric hospitalization (not shown in table). In logistic regression models, factors associated with both psychiatric and all-cause hospitalization included: having a prior hospitalization (OR [95% C]): 2.42 [2.23–2.63; psychiatric]); 2.09 [1.96–2.23; all-cause]); previous treatment with nonindex antipsychotics (1.33 [1.23–1.44]; 1.22 [1.14–1.30]); previous treatment with psychiatric medications (1.17 [1.04–1.31]; 1.17 [1.07–1.29]); substance abuse (1.72 [1.58–1.86]; 1.61 [1.50–1.72]); having at least one inpatient or two outpatient claims for psychiatric comorbidities, including personality disorder (1.50 [1.33–1.70]; 1.15 [1.03–1.28]), MDD (1.32 [1.22–1.42); 1.13 [1.06–1.20]) and anxiety (1.13 [1.05–1.22]; 1.07 [1.00–1.14]); and having Type II diabetes (1.26 [1.13–1.41]; 1.23 [1.13–1.34]). Also, younger age (18–34 vs 55+) predicted psychiatric hospitalization (OR; 95% CI): 1.50 (1.33–1.70) (Table 3).
Among patients with MDD, in the follow-up period, 18.7% patients had at least one all-cause hospitalization and 7.9% had at least one psychiatric hospitalization (not shown in table). In risk-adjusted models, factors associated with both psychiatric and all-cause hospitalization included: having a prior hospitalization (OR [95% CI]: 2.81 [2.49–3.16; psychiatric]); 2.21 [2.03–2.40; all-cause]); previous treatment with nonindex antipsychotics (1.31 [1.11–1.54]; 1.17 [1.04–1.32]); and having a substance abuse disorder (1.90 [1.68–2.15]; 1.55 [1.41–1.71]). Also, younger age (18–34 vs 55+) predicted psychiatric and all-cause hospitalization (OR [95% CI]: 1.58 [1.33–1.89; psychiatric]; 1.23 [1.08–1.40; all-cause]) (Table 3).
Discussion
We found risk factors that predicted hospitalization in patients with severe schizophrenia, BD-I or MDD 1 year after initiating a new antipsychotic treatment were nearly identical to those seen in other populations, such as hospitalized mentally ill patients. Specifically, prior hospitalization, previous treatment with antipsychotics and substance abuse disorder were associated with significantly increased risk for all-cause and psychiatric hospitalization 1 year after starting a new antipsychotic medication. This was true not only for schizophrenia and BD-I, but also for MDD, which is novel. It is important to note that prior hospitalization, substance abuse disorder and previous treatment with antipsychotics may be indicators of disease severity and any causal attribution should be made with caution in this study. Among schizophrenia and BD-I patients, having at least one inpatient or two outpatient claims for another psychiatric illness predicted an increased risk for psychiatric and all-cause hospitalization, signifying the additional illness severity and burden these patients face.
The hospitalization rates found in our study were similar to those reported in the literature [13,15,36–38]. For example, in our study, 33.7% of patients with schizophrenia had at least one all-cause hospitalization in the 1-year follow-up period; Lang et al. found that 29% of Medicaid and commercially insured patients with schizophrenia had an all-cause hospitalization within 1 year after antipsychotic treatment [13].
Prior hospitalization was associated with a significantly increased risk of hospitalization in the 1 year following antipsychotic treatment among patients with schizophrenia, BD-I or MDD in our analyses, and these findings are similar to those from earlier studies [13,28–31,39]. For example, in a study that aimed to identify key factors that correlated with readmission to a military psychiatric hospital in Washington, DC over a 13-month period, Bobo et al. found that previous psychiatric hospitalization was associated with readmission in risk-adjusted models [31]. Similarly, Hamilton et al. found that patients with BD who were admitted consecutively to a psychiatric hospital in the US in 2013 and had three or more prior psychiatric hospitalizations were significantly more likely to be readmitted within 1 year of discharge [36].
Our finding that previous treatment with at least one nonindex antipsychotic drug was associated with an increased risk of hospitalization is similar to findings from previous studies [40]. Severely ill patients who are more difficult to treat due to nonresponse may cycle through several different antipsychotics in an attempt to properly control symptoms. Therefore, in our study, previous nonindex antipsychotic treatment may indicate a group of patients who are less responsive to treatment [15].
We found that younger age was associated with increased risk of psychiatric hospitalization among patients with schizophrenia and BD-I, and both psychiatric and all-cause hospitalization among patients with MDD. The onset of schizophrenia, BD-I or MDD usually spikes in younger age [41–43]. Younger age has been reported to be a risk factor for psychiatric readmissions [44].
Our finding that substance abuse was associated with increased risk of hospitalization among these three patient populations – schizophrenia, BD-I and MDD – is supported by several previous studies showing that re-hospitalization rates increased among mentally ill patients as a function of substance abuse problems [7,14,19,22–26,45]. For example, analyses by Haywood et al. with data collected on patients with schizophrenia, schizoaffective disorder, unipolar major depression and BD, indicated that substance abuse was associated with significantly higher rates of hospitalization [19].
Reducing hospitalizations in patients with severe mental illness is essential in lowering the burden of mental disorders placed on individuals and the society. The transition period from inpatient to outpatient settings is recognized as a critical period in a patient's illness. Mental health interventions and strategies employed during this period can effectively reduce physical health readmissions [46]. Unfortunately, the majority of hospital readmission reduction programs have been tested and implemented in general medical and surgical elderly and/or chronic condition populations. Little research has been devoted to approaches to transition seriously mentally ill patients from inpatient to outpatient settings, especially among those with comorbid substance abuse (the only modifiable risk factor that predicted increased hospitalization rates in all three psychiatric patient populations in our study) [47]. In fact, systematic searches of the literature have failed to identify any transitional care models that specifically apply to patients with severe mental illness [48]. However, there have been local collaborative initiatives, such as Amerigroup in Florida, Colorado Access and RARE in Minnesota, that aim to organize hospitals, outpatient providers and/or health plans to reduce psychiatric rehospitalization [48]. Expanding these initiatives to the broader population may be beneficial. More efforts are needed in developing and delivering efficient and effective interventions to patients with severe mental illness and substance abuse.
Study limitations
This study is not without limitations. First, claims data used for these analyses are generated for reimbursement, not research, so coding errors, misclassification, diagnostic uncertainty and/or omissions could affect the reliability of the results. Specifically, we could not clinically validate any diagnoses in this study. Nevertheless, health insurance claims data are a valuable source of information, as they contain a valid and large sample of real-world patient characteristics. Second, the list of predictors assessed in this study was limited to those available in the claims database. Other potential predictors of hospitalization such as disease severity (current and lifetime) [49], length of the illness [50], socioeconomic factors (e.g., educational level) [16,51], psychosocial factors [52,53] and medication side effects [54] were not available in the database, thereby limiting generalizability of the findings. Third, our study population focused on a select group of patients who were treated with antipsychotics. MDD patients treated with antipsychotics may represent those who failed to respond to antidepressants eventually ending with an antipsychotic augmentation treatment. Last, we did not include patients who were Medicare and Medicaid dual-eligible, which may explain the smaller ratio of patients with schizophrenia to patients with BD-I we found compared with the national rate, as a larger percentage of patients with schizophrenia have dual eligibility than the US general population [55].
Conclusion
In this real-world study, we found that prior hospitalization, previous treatment with antipsychotics, and substance abuse disorder were significantly associated with both all-cause and psychiatric hospitalization within 1 year of initiating a new antipsychotic treatment in patients with severe schizophrenia and BD-I. This is also true for patients with severe MDD treated with antipsychotics. Continued careful assessment of these risk factors is essential and interventions that target them, especially substance abuse, may be helpful in reducing hospitalizations in these patients with severe mental illness.
Schizophrenia, bipolar disorder (BD), and major depressive disorder (MDD) are among the most severe mental illnesses, resulting in significant morbidity.
While antipsychotics are frequently used to treat schizophrenia and are increasingly used in severe BD and MDD, relapse rates are still high.
Hospitalization, which has been used as a proxy for relapse, is common among patients with schizophrenia or BD.
Exploration of factors related to treatment response and relapse among patients with severe mental illness is a prerequisite for improving outcomes and reducing healthcare and societal costs in schizophrenia, BD and MDD.
Current literature has identified several known risk factors that may predict hospitalization, but rarely focuses on patients who were treated with antipsychotics and tended to be more severe than those without such treatments; no such data exists among patients with severe MDD treated with antipsychotics.
Using 2012–2016 data from the Truven Health Analytics MarketScan® (Commercial, Medicaid and Medicare Supplemental) databases, the final sample of patients included: 8575 with schizophrenia, 29,621 with bipolar I disorder (BD-I) and 20,020 with MDD.
Prior hospitalization, previous treatment with nonindex antipsychotics and substance abuse were associated with statistically significant increased risk of both psychiatric and all-cause hospitalization in patients with schizophrenia and BD-I. This is also true for patients with severe MDD treated with antipsychotics.
Careful assessment and interventions that target the modifiable risk factor – substance abuse – should continue to be implemented in patients with severe mental illness to reduce hospitalizations.
Author's contributions
All authors were equally involved in the design of the study. E Chang conducted the statistical analyses and all authors contributed equally in the interpretation of results and writing of the manuscript.
Financial & competing interests disclosure
Funding for the study was received from Otsuka Pharmaceutical Development and Commercialization, Inc., and Lundbeck. J Munday was a past employee, and MS Broder, E Chang and T Yan are present employees, of PHAR, LLC, who were paid by Otsuka and Lundbeck to perform the research described in this manuscript. M Greene is an employee of Otsuka. M Touya and A Hartry are employees of Lundbeck. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
The National Institute of Mental Health. Mental Illness [Internet]. Health Inf. - Stat (2017). www.nimh.nih.gov/health/statistics/mental-illness.shtml.
2.
Stovall J. Bipolar disorder in adults: epidemiology and pathogenesis [Internet] (2016). www.uptodate.com/contents/bipolar%C2%ADdisorder%C2%ADin%C2%ADadults%C2%ADepidemiology%C2%ADand%C2%ADpathogenesis/print?source=search_result&search=bipolar%20stovall&select%E2%80%A6.
3.
Naudet F, Maria AS, Falissard B. Antidepressant response in major depressive disorder: a meta-regression comparison of randomized controlled trials and observational studies. PLoS ONE 6(6), e20811 (2011).
4.
Wright BM, Eiland EH, Lorenz R. Augmentation with atypical antipsychotics for depression: a review of evidence-based support from the medical literature. Pharmacotherapy 33(3), 344–359 (2013).
5.
Bergeson JG, Kalsekar I, Jing Y, You M, Forbes RA, Hebden T. Medical care costs and hospitalization in patients with bipolar disorder treated with atypical antipsychotics. Am. Health Drug Benefits 5(6), 379–386 (2012).
6.
Yan T, Greene M, Chang E, Hartry A, Touya M, Broder MS. All-cause hospitalization and associated costs in patients with schizophrenia or bipolar disorder initiating long-acting injectable antipsychotics. Curr. Med. Res. Opin. 34(1), 41–47 (2018).
• In this head-to-head comparison that included recently approved long-acting injectables (LAIs), aripiprazole once-monthly was more effective than haloperidol- and risperidone-LAIs in reducing all-cause hospitalization.
7.
Porcelli S, Bianchini O, De Girolamo G, Aguglia E, Crea L, Serretti A. Clinical factors related to schizophrenia relapse. Int. J. Psychiatry Clin. Pract. 20(2), 54–69 (2016).
8.
Sartorius N, Gulbinat W, Harrison G, Laska E, Siegel C. Long-term follow-up of schizophrenia in 16 countries. A description of the International Study of Schizophrenia conducted by the World Health Organization. Soc. Psychiatry Psychiatr. Epidemiol. 31(5), 249–258 (1996).
9.
Wiersma D, Nienhuis FJ, Slooff CJ, Giel R. Natural course of schizophrenic disorders: a 15-year follow-up of a Dutch incidence cohort. Schizophr. Bull. 24(1), 75–85 (1998).
10.
Almond S, Knapp M, Francois C, Toumi M, Brugha T. Relapse in schizophrenia: costs, clinical outcomes and quality of life. Br. J. Psychiatry J. Ment. Sci. 184, 346–351 (2004).
11.
Awad AG, Voruganti LNP. The burden of schizophrenia on caregivers: a review. PharmacoEconomics 26(2), 149–162 (2008).
12.
Suzuki T. A further consideration on long-acting injectable versus oral antipsychotics in the treatment of schizophrenia: a narrative review and critical appraisal. Expert Opin. Drug Deliv. 13(2), 253–264 (2016).
13.
Lang K, Federico V, Muser E, Menzin J, Menzin J. Rates and predictors of antipsychotic non-adherence and hospitalization in Medicaid and commercially-insured patients with schizophrenia. J. Med. Econ. 16(8), 997–1006 (2013).
• This study of Medicaid and Commercial insurance patients with schizophrenia reported that previous nonadherence, newly starting antipsychotic therapy and previous hospitalization were significant predictors of nonadherence and hospitalization in these patient populations.
14.
van Dijk D, Koeter MWJ, Hijman R, Kahn RS, van den Brink W. Effect of cannabis use on the course of schizophrenia in male patients: a prospective cohort study. Schizophr. Res. 137(1–3), 50–57 (2012).
15.
Innes H, Lewsey J, Smith DJ. Predictors of admission and readmission to hospital for major depression: a community cohort study of 52,990 individuals. J. Affect. Disord. 183, 10–14 (2015).
• This study found a number of factors increased the risk of a first admission (e.g., gender, income, being a heavy drinker, etc.); whereas, only older age (70+ years) and previous psychiatric-related (other than major depression) admission were statistically significant risk factors for readmission.
16.
Lin C-H, Chen W-L, Lin C-M, Lee M-D, Ko M-C, Li C-Y. Predictors of psychiatric readmissions in the short- and long-term: a population-based study in Taiwan. Clinics 65(5), 481–489 (2010).
• This study compared predictors of readmission during varying follow-up times with only two factors (patient age and hospital accreditation level) associated with different risk levels depending on time period after discharge.
17.
Pesa JA, Doshi D, Wang L, Yuce H, Baser O. Health care resource utilization and costs of California Medicaid patients with schizophrenia treated with paliperidone palmitate once monthly or atypical oral antipsychotic treatment. Curr. Med. Res. Opin. 33(4), 723–731 (2017).
18.
Weiden P, Glazer W. Assessment and treatment selection for ‘revolving door’ inpatients with schizophrenia. Psychiatr. Q. 68(4), 377–392 (1997).
19.
Haywood T, Kravitz H, Grossman L, Cavanaugh JJ, Davis J, Lewis DA. Predicting the ‘revolving door’ phenomenon among patients with schizophrenic, schizoaffective, and affective disorders. Am. J. Psychiatry 152(6), 856–861 (1995).
• Using the schedule for affective disorders and schizophrenia along with a life events history, this study identified substance abuse and medication noncompliance as the most important factors related to hospitalization frequency.
20.
Kane JM, Sanchez R, Zhao J et al. Hospitalisation rates in patients switched from oral anti-psychotics to aripiprazole once-monthly for the management of schizophrenia. J. Med. Econ. 16(7), 917–925 (2013).
21.
Tiihonen J, Mittendorfer-Rutz E, Majak M et al. Real-world effectiveness of antipsychotic treatments in a nationwide cohort of 29/823 patients with schizophrenia. JAMA Psychiatry 74(7), 686–693 (2017).
22.
Di Lorenzo R, Sagona M, Landi G, Martire L, Piemonte C, Del Giovane C. The Revolving Door Phenomenon in an Italian Acute Psychiatric Ward: a 5-year retrospective analysis of the potential risk factors. J. Nerv. Ment. Dis. 204(9), 686–692 (2016).
23.
Frick U, Frick H, Langguth B, Landgrebe M, Hübner-Liebermann B, Hajak G. The revolving door phenomenon revisited: time to readmission in 17′145 [corrected] patients with 37′697 hospitalisations at a German psychiatric hospital. PLoS ONE 8(10), e75612 (2013).
24.
Hoblyn JC, Balt SL, Woodard SA, Brooks JO. Substance use disorders as risk factors for psychiatric hospitalization in bipolar disorder. Psychiatr. Serv. 60(1), 50–55 (2009).
25.
Turkington A, Mulholland CC, Rushe TM et al. Impact of persistent substance misuse on 1-year outcome in first-episode psychosis. Br. J. Psychiatry J. Ment. Sci. 195(3), 242–248 (2009).
26.
Ciudad A, Alvarez E, Bobes J, San L, Polavieja P, Gilaberte I. Remission in schizophrenia: results from a 1-year follow-up observational study. Schizophr. Res. 108(1–3), 214–222 (2009).
27.
Gastal FL, Andreoli SB, Quintana MI, Almeida Gameiro M, Leite SO, McGrath J. Predicting the revolving door phenomenon among patients with schizophrenic, affective disorders and non-organic psychoses. Rev. Saude Publica. 34(3), 280–285 (2000).
28.
Raven MC, Doran KM, Kostrowski S, Gillespie CC, Elbel BD. An intervention to improve care and reduce costs for high-risk patients with frequent hospital admissions: a pilot study. BMC Health Serv. Res. 11, 270 (2011).
29.
Billings J, Mijanovich T. Improving the management of care for high-cost medicaid patients. Health Aff. 26(6), 1643–1654 (2007).
30.
Billings J, Dixon J, Mijanovich T, Wennberg D. Case finding for patients at risk of readmission to hospital: development of algorithm to identify high risk patients. BMJ 333(7563), 327 (2006).
31.
Bobo WV, Hoge CW, Messina MA, Pavlovcic F, Levandowski D, Grieger T. Characteristics of repeat users of an inpatient psychiatry service at a large military tertiary care hospital. Mil. Med. 169(8), 648–653 (2004).
32.
Stein BD, Pangilinan M, Sorbero MJ et al. Using claims data to generate clinical flags predicting short-term risk of continued psychiatric hospitalizations. Psychiatr. Serv. 65(11), 1341–1346 (2014).
33.
Hirschfeld RMA, Bowden CL, Gitlin MJ et al. Practice guideline for the treatment of patients with bipolar disorder (Revision). FOCUS J. Lifelong Learn. Psychiatry 1(1), 64–110 (2003).
34.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40(5), 373–383 (1987).
35.
Agency for Healthcare Research and Quality. HCUP chronic condition indicator. Healthc. Cost Util. Proj. (2015). www.hcup-us.ahrq.gov/toolssoftware/chronic/chronic.jsp.
36.
Hamilton JE, Passos IC, de Azevedo Cardoso T et al. Predictors of psychiatric readmission among patients with bipolar disorder at an academic safety-net hospital. Aust. N. Z. J. Psychiatry 50(6), 584–593 (2016).
• In this study using electronic medical records, factors associated with increased risk of readmission in patients with bipolar disorder included being uninsured, homelessness, having previous psychiatric hospitalizations and male gender.
37.
Woo YS, Bahk W-M, Jung Y-E et al. One-year rehospitalization rates of patients with first-episode bipolar mania receiving lithium or valproate and adjunctive atypical antipsychotics: readmission on lithium versus valproate. Psychiatry Clin. Neurosci. 68(6), 418–424 (2014).
38.
Patel NC, Crismon ML, Pondrom M. Rehospitalization rates of patients with bipolar disorder discharged on a mood stabilizer versus a mood stabilizer plus an atypical or typical antipsychotic. J. Behav. Health Serv. Res. 32(4), 438–445 (2005).
39.
Lang K, Korn J, Muser E, Choi JC, Abouzaid S, Menzin J. Predictors of medication nonadherence and hospitalization in Medicaid patients with bipolar I disorder given long-acting or oral antipsychotics. J. Med. Econ. 14(2), 217–226 (2011).
40.
Jaracz J, Tetera-Rudnicka E, Kujath D et al. The prevalence of antipsychotic polypharmacy in schizophrenic patients discharged from psychiatric units in Poland. Pharmacol. Rep. 66(4), 613–617 (2014).
41.
Mura G. Schizophrenia: from epidemiology to rehabilitation. Clin. Pract. Epidemiol. Ment. Health. 8(1), 52–66 (2012).
42.
Merikangas KR, Akiskal HS, Angst J et al. Lifetime and 12-month prevalence of bipolar spectrum disorder in the national comorbidity survey replication. Arch. Gen. Psychiatry 64(5), 543 (2007).
43.
Hasin DS, Goodwin RD, Stinson FS, Grant BF. Epidemiology of major depressive disorder: results from the national epidemiologic survey on alcoholism and related conditions. Arch. Gen. Psychiatry 62(10), 1097 (2005).
44.
Hung Y-Y, Chan H-Y, Pan Y-J. Risk factors for readmission in schizophrenia patients following involuntary admission. PLoS ONE 12(10), e0186768 (2017).
45.
Ayano G, Duko B. Relapse and hospitalization in patients with schizophrenia and bipolar disorder at the St Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia: a comparative quantitative cross-sectional study. Neuropsychiatr. Dis. Treat. 13, 1527–1531 (2017).
46.
Benjenk I, Chen J. Effective mental health interventions to reduce hospital readmission rates: a systematic review. J. Hosp. Manag. Health Policy 2, 45 (2018).
47.
Kripalani S, Theobald CN, Anctil B, Vasilevskis EE. Reducing hospital readmission: current strategies and future directions. Annu. Rev. Med. 65, 471–485 (2014).
48.
Pincus HA. Care transition interventions to reduce psychiatric re-hospitalizations. National Association of State Mental Health Program Directors, Alexandria, VA, USA. www.nasmhpd.org/sites/default/files/Assessment%20%233_Care%20Transitions%20Interventions%20toReduce%20Psychiatric%20Rehospitalization.pdf.
49.
Ascher-Svanum H, Zhu B, Faries DE et al. The cost of relapse and the predictors of relapse in the treatment of schizophrenia. BMC Psychiatry 10, 2 (2010).
50.
Lin C-H, Chen M-C, Chou L-S, Lin C-H, Chen C-C, Lane H-Y. Time to rehospitalization in patients with major depression vs. those with schizophrenia or bipolar I disorder in a public psychiatric hospital. Psychiatry Res. 180(2–3), 74–79 (2010).
51.
Aro S, Aro H, Salinto M, Keskimäki I. Educational level and hospital use in mental disorders: a population-based study. Acta Psychiatr. Scand. 91(5), 305–312 (1995).
52.
Hamer M, Stamatakis E, Steptoe A. Psychiatric hospital admissions, behavioral risk factors, and all-cause mortality: The Scottish Health Survey. Arch. Intern. Med. 168(22), 2474 (2008).
53.
Alavi M, Baharlooei O, AdelMehraban M. Do psychosocial factors predict readmission among diabetic elderly patients? Iran. J. Nurs. Midwifery Res. 22(6), 460–464 (2017).
54.
DiBonaventura M, Gabriel S, Dupclay L, Gupta S, Kim E. A patient perspective of the impact of medication side effects on adherence: results of a cross-sectional nationwide survey of patients with schizophrenia. BMC Psychiatry 12(1), (2012). http://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-12-20.
55.
Khaykin E, Eaton WW, Ford DE, Anthony CB, Daumit GL. Health insurance coverage among persons with schizophrenia in the United States. Psychiatr. Serv. 61(8), 830–834 (2010).
Information & Authors
Information
Published In
Copyright
© 2018 Otsuka Pharmaceuticals.
History
Received: 5 September 2018
Accepted: 29 November 2018
Published online: 17 December 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Hospitalization risk factors in antipsychotic-treated schizophrenia, bipolar I disorder or major depressive disorder. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0090
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ana Rabasco, Jihoon Choi, Ilana Ladis, Sarah A. Arias, Lauren M. Weinstock, Ivan Miller, Edwin D. Boudreaux, Carlos A. Camargo, Brandon A. Gaudiano, Who's getting care? Acute treatment utilization following an emergency department visit among adults with major psychiatric disorders and suicidal thoughts and behaviors, Journal of Psychiatric Research, 10.1016/j.jpsychires.2026.03.040, 198, (175-181), (2026).
- Jiseun Lim, KwangHo Mun, BaegJu Na, YuJin Lee, Association of health screening participation with cardiovascular mortality and suicide in patients with schizophrenia and bipolar disorder, Social Psychiatry and Psychiatric Epidemiology, 10.1007/s00127-026-03078-4, 61, 7, (1217-1226), (2026).
- Andrew J. Cutler, Hemangi R. Panchmatia, Alejandro G. Hughes, Noah S. Webb, Michael J. Doane, Rakesh Jain, Healthcare Resource Utilization 6 Months Before and After Olanzapine/Samidorphan Initiation: Real-World Assessment of Patients with Schizophrenia or Bipolar I Disorder, Advances in Therapy, 10.1007/s12325-025-03211-w, 42, 8, (3691-3707), (2025).
- Naomi Launders, Kate Dotsikas, Louise Marston, Gabriele Price, David P. J. Osborn, Joseph F. Hayes, The impact of comorbid severe mental illness and common chronic physical health conditions on hospitalisation: A systematic review and meta-analysis, PLOS ONE, 10.1371/journal.pone.0272498, 17, 8, (e0272498), (2022).
- Ismaeel Yunusa, Chengwen Teng, Ibraheem M. Karaye, Emily Crounse, Saud Alsahali, Nasim Maleki, Comparative Safety Signal Assessment of Hospitalization Associated With the Use of Atypical Antipsychotics, Frontiers in Psychiatry, 10.3389/fpsyt.2022.917351, 13, (2022).
- Mika Kallio, Jyrki Korkeila, Markus Malmberg, Jarmo Gunn, Päivi Rautava, Päivi Korhonen, Ville Kytö, Impaired long-term outcomes of patients with schizophrenia spectrum disorder after coronary artery bypass surgery: nationwide case–control study, BJPsych Open, 10.1192/bjo.2022.10, 8, 2, (2022).
- Xiaoli Niu, Phani Veeranki, Syvart Dennen, Carole Dembek, Kimberly Laubmeier, Yanmei Liu, G. Rhys Williams, Antony Loebel, Hospitalization risk among adults with bipolar I disorder treated with lurasidone versus other oral atypical antipsychotics: a retrospective analysis of Medicaid claims data, Current Medical Research and Opinion, 10.1080/03007995.2021.1897557, 37, 5, (839-846), (2021).
- Xiaoli Niu, Syvart Dennen, Carole Dembek, Kimberly Laubmeier, Yanmei Liu, Phani Veeranki, Michael Tocco, G. Rhys Williams, Hospitalization Risk for Adults with Bipolar I Disorder Treated with Oral Atypical Antipsychotics as Adjunctive Therapy with Mood Stabilizers: A Retrospective Analysis of Medicaid Claims Data, Current Therapeutic Research, 10.1016/j.curtheres.2021.100629, 94, (100629), (2021).
- Yoo Hyun Um, Tae-Won Kim, Ho-Jun Seo, Seung-Chul Hong, Sung-Min Kim, Ji-Hye Oh, Jong-Hyun Jeong, Predictors of 1-year rehospitalization in inpatients with bipolar I disorder treated with atypical antipsychotics, International Clinical Psychopharmacology, 10.1097/YIC.0000000000000318, 35, 5, (263-269), (2020).
- Tania Lecomte, Charles-Édouard Giguère, Briana Cloutier, Stéphane Potvin, Comorbidity Profiles of Psychotic Patients in Emergency Psychiatry, Journal of Dual Diagnosis, 10.1080/15504263.2020.1713425, 16, 2, (260-270), (2020).