Intramedullary versus extramedullary alignment guides on total knee arthroplasty: a meta-analysis
Abstract
Aim: A meta-analysis concentrated on the effect of intramedullary and extramedullary systems on total knee arthroplasty. Method: Potential academic articles were identified from Cochrane Library, Medline, PubMed, Embase, ScienceDirect, CNKI, WanFang, VIP and other databases. The STATA version was used to analyze the pooled data. Results: There are obvious significant differences in drainage volume and transfusion rate. There was no significant difference in lower limb coronal alignment, coronal and sagittal alignment of the femoral component, operation time, postoperative knee score and complications. Conclusion: Our meta-analysis shows that the alignment of the extramedullary distal femur osteotomy is as accurate as intramedullary systems. Furthermore, extramedullary distal femur osteotomy without invading the femoral medullary cavity could reduce postoperative bleeding and the transfusion rate. Furthermore, research is required to test the robustness of our findings when more data is available and by undertaking both Bayesian and frequentist methods. When more data are available, the heterogeneity can be further explored through sensitivity analysis, and the available data can be combined to verify the hypothesis.
Total knee arthroplasty (TKA) has been considered one of the most successful surgical procedures for eradicating advanced knee pain, restoring knee joint function and improving the quality of life of patients [1]. Limb alignment, selection of prostheses, accurate surgical techniques and perioperative management are all critical to the success of the procedure. Limb alignment is crucial for reconstructing normal knee function, reducing liner wear and improving prosthesis survival [2–4]. The TKAs require reconstruction of the mechanical axis of the lower limb, which is based on the right osteotomy and the precise balance of the soft tissue [5]. Some authors favor that intramedullary alignment produces more accurate and reproducible placement and can reach 85 to 96% in the normal range [6–8]. A retrospective study of 6726 cases of TKAs revealed that the angle of the tibial and femoral anatomical axis of the coronal alignment in the intramedullary group was more accurate than that of the extramedullary alignment group (4.6 ± 2.2°; 5.1 ± 3.3°) [9]. However, postoperative x-ray images for 201 patients with intramedullary femoral alignment systems showed that up to 8.5% of patients had an unsatisfactory mechanical axis [10]. Furthermore, the accuracy of the coronal alignment was 98.2% when using the apex of the anterior superior iliac spine and the trochanter of the femur [11]. In recent years, the advanced extramedullary alignment system has been more accurate in femoral osteotomy with coronal and sagittal alignments by means of the interfemoral head center distance and the mechanical axis marker systems in TKAs [11,12].
A distal femur osteotomy usually requires opening the medullary cavity and the placement of an intramedullary positioning rod. Intramedullary alignment could result in prosthesis placement error due to various factors such as anatomy and technology. Osteotomy error with intramedullary femoral alignment systems exists mainly in the following aspects: the location of the needle point of the intramedullary positioning rod is inaccurate; the positioning rod is not located in the center of the large femoral medullary cavity; the error caused by the difference between the diameter of the positioning rod and the insertion length; and apparent extra-articular deformity [13–15]. Additionally, reaming or inserting an intramedullary rod may cause damage to the intramedullary microvasculature, leading to the extrusion of bone marrow cells and fat particles into the injured blood vessels, which is one of the bases of thrombosis and fat embolism. Accompanied by massive blood loss, platelet and coagulation factors are lost in blood, which leads to an imbalance of the coagulation and fibrinolysis system and increases the risk of thrombosis or bleeding [16].
A meta-analysis concentrating on the intramedullary and extramedullary femoral alignment systems recently pooled the results from studies with finite sample sizes. Consequently, we performed a more comprehensive meta-analysis concerning whether the intramedullary system is more accurate in reproducing a neutral distal femoral resection compared with an extramedullary alignment system on the coronal and sagittal alignments during TKAs. Simultaneously, we extracted data regarding drainage volume, operation time and the number of complications to provide further evidence for clinical decisions.
Materials & methods
Literature & search strategy
The electronic databases, including Cochrane Library, Medline, PubMed, Embase, ScienceDirect, CNKI, WanFang and VIP were retrieved to identify the publications (RCTs and non-RCTs) exploring the effect of extramedullary or intramedullary femoral alignment guide systems for TKAs from the inception of electronic databases to November 2017. Structured search strategies were used in combination, according to Boolean logic: total knee replacement, TKA, intramedullary, extramedullary and femoral. In addition, the research on the appraisal reference list was manually reviewed for other potential trials that should be included. The process was iterated until no further articles could be determined. The meta-analysis was based on acknowledged prioritized reported items for systematic review and meta-analysis guidelines.
Inclusion & exclusion criteria
If the literature met the following criteria in accordance with PICOS, the article is considered to be included in the current meta-analysis: population: patients who received TKAs were similar in demographics; intervention: extramedullary and intramedullary femoral alignment system TKAs; comparison intervention: extramedullary or intramedullary alignment system; outcome measures, one or more of the following outcomes were reported: lower limb coronal alignment, coronal alignment of femoral component, sagittal alignment of femoral component, drainage volume, transfusion rate, complications, postoperative knee score and operation time; and study design: randomized controlled trial (RCTs) and non-RCTs, in vitro animal experiments and clinical trial with adequate data are excluded.
Data extraction & outcome measures
Two of the reviewers independently extracted data from the included studies. The following essential information was captured: first author name, publication year, sample size, study design and outcomes. Other relevant data such as patient characteristics and literature quality score were also extracted from individual studies. The extracted data – median, range and size of the trial – and mean difference (MD) and standard deviation (SD) were inputted into the designed standardized table. When there were differences in opinion, another author had the final decision. The primary outcome measurements were lower limb coronal alignment, coronal alignment of the femoral component and sagittal alignment of the femoral component. Secondary outcomes included the drainage volume, transfusion rate, complications, operation time and postoperative knee score at different follow-up times. Complications included incidence of infection, fracture, nerve and vascular injury and thrombosis.
Quality assessment & statistical analysis
Tools from Cochrane Bone, the Joint and Muscle Trauma Group and methodological index for nonrandomized studies were conducted to evaluate the quality of the included studies. The literature quality evaluation was conducted separately by two reviewers. Consensus was reached through consultation for divergence. We used STATA version 11.0 (Stata Corporation, TX, USA) for statistical analyses. When I2 > 50%, we consider that the data have obvious heterogeneity and we conduct a meta-analysis using a random-effect model according to the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0). Otherwise, the fixed-effect model was performed. The results of continuous outcomes (drainage volume, postoperative knee score and operation time) were expressed as the MD with 95% confidence intervals (CIs). For discontinuous variable outcomes (lower limb coronal alignment, coronal alignment, sagittal alignment, transfusion rate, complications), a risk difference (RD) or relative risk (RR) with 95% CIs was applied for the assessment.
Results
Search results
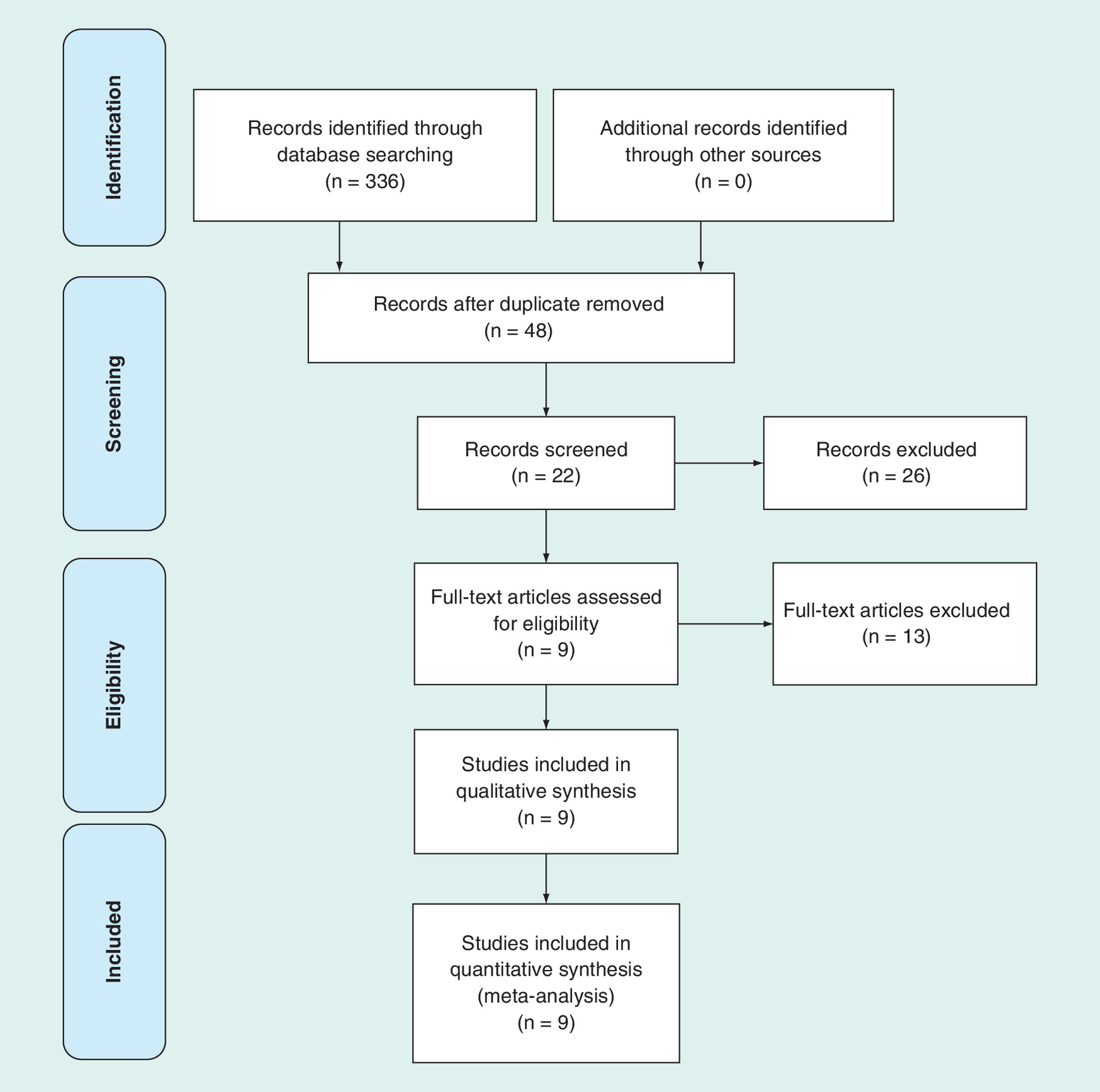
The selection process is illustrated in Figure 1; the original database (Cochrane Library, Medline, PubMed, Embase, ScienceDirect, CNKI, WanFang, and VIP) search yielded 336 records. Of them, 314 were excluded for various reasons (unavailable data, case report, reviews, and irrelevant articles). In addition, the remaining 22 articles were reviewed through the whole text. We excluded 13 articles, because they did not compare extramedullary and intramedullary guides on femoral component geometry treatment. Finally, nine studies [7,9,11–13,16–19] were included in the present meta-analysis.
Risk of bias assessment
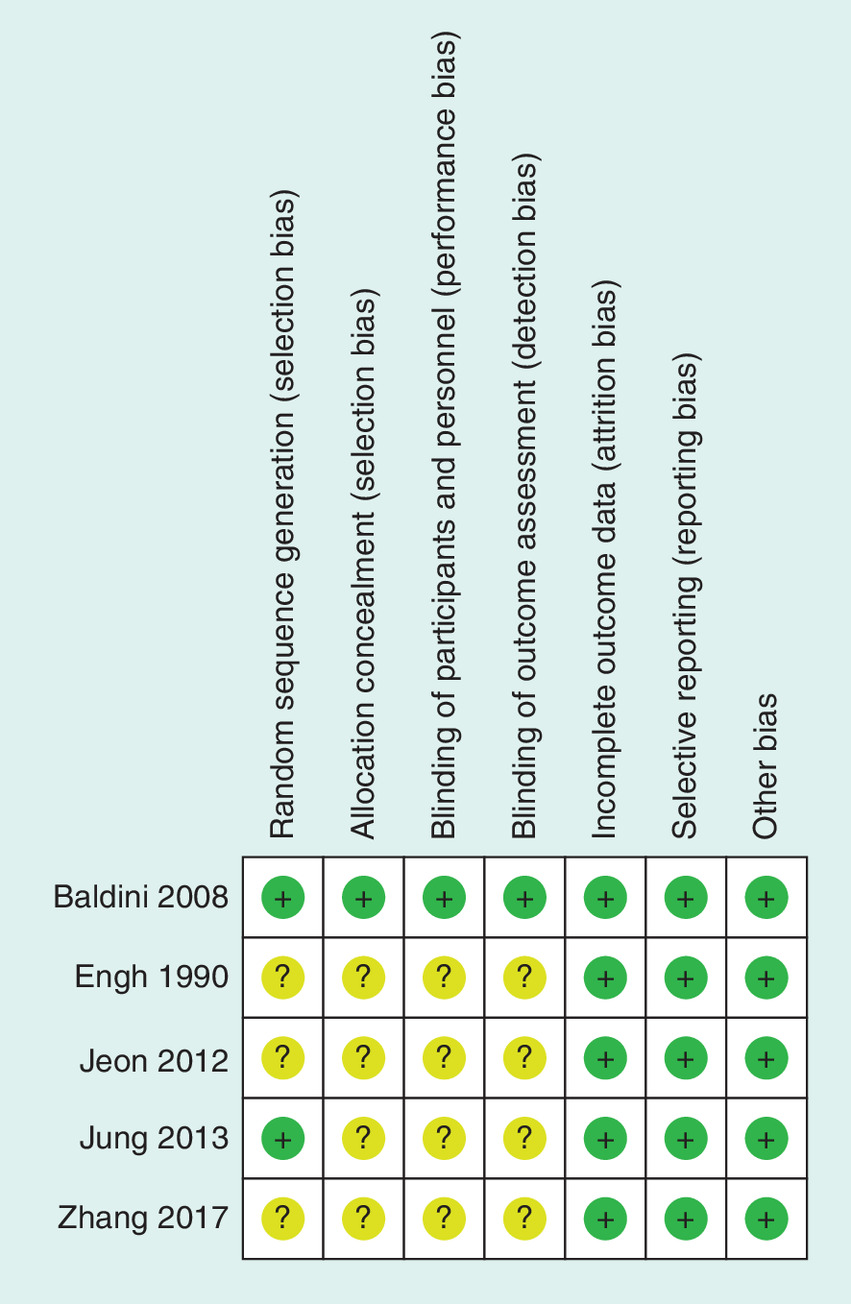
Tools from Cochrane Bone, the Joint and Muscle Trauma Group were conducted to evaluate the quality of the included studies of RCTs. We present the details in Figure 2. The scores of non-RCTs evaluated by the methodological index for nonrandomized studies quality assessment ranged from 18 to 20. Table 2 summarizes more details of the quality assessment for non-RCTs.
| Study (year) | Country | Simple size EM/IM | Age EM/IM | Type | Total knee system | EM system |
|---|---|---|---|---|---|---|
| Zhang (2017) [19] | China | 30/30 | 68.80/65.00 | RCT | Gemini prosthesis (link) | Markers attached to skin |
| Tillete (1998) [20] | America | 25/25 | 69(38-88) | RCS | Depuy | An extramedullary device with preoperative templated data |
| Li (2017) [18] | China | 20/20 | 65.1/65.7 | RCS | Gemini prosthesis (link) | Markers attached to skin |
| Meding (2011) [9] | Indiana | 1733/4993 | NS | RCS | NS | NS |
| Kandle (2010) [16] | Australia | 45/45 | 71/72 | RCS | Insight, osteonics | NS |
| Jung (2013) [11] | South Korea | 56/50 | 70.4/68.5 | RCT | PS prosthesis (Stryker) | Mechanical axis marker with IFD measurement |
| Baldini (2008) [12] | Italy | 50/50 | 70/71 | RCT | Posterior stabilized flex fixed-bearing prosthesis (Zimmer) | An extramedullary device with preoperative templated data |
| Engh (1990) [17] | America | 32/40 | 70.9/67.5 | RCT | Depuy | HDisc–peg taped to skin for intraoperative location |
| Jeon (2012) [13] | South Korea | 39/40 | 70.1/69.2 | RCT | PS prosthesis (Stryker) | Markers attached to skin |
EM: Extramedullary group; IFD: Interfemoral head center; IM: Intramedullary group; NS: Not specified; PS: Posterior – stabilized; RCT: Randomized controlled trial.
| Quality assessment for nonrandomized trials | Meding (2011) [9] | Tillett (1988) [20] | Li (2017) [18] | Kandle (2010) [16] |
|---|---|---|---|---|
| A clearly stated aim | 2 | 2 | 2 | 2 |
| Inclusion of consecutive patients | 2 | 2 | 2 | 2 |
| Prospective data collection | 0 | 0 | 0 | 0 |
| End points appropriate to the aim of the study | 2 | 2 | 2 | 2 |
| Unbiased assessment of the study end point | 2 | 2 | 2 | 2 |
| A follow-up period appropriate to the aims of study | 2 | 2 | 0 | 2 |
| Less than 5% loss to follow-up | 2 | 2 | 2 | 2 |
| Prospective calculation of the sample size | 0 | 0 | 0 | 0 |
| An adequate control group | 2 | 2 | 2 | 2 |
| Contemporary groups | 2 | 2 | 2 | 2 |
| Baseline equivalence of groups | 2 | 2 | 2 | 2 |
| Adequate statistical analyses | 2 | 2 | 2 | 2 |
Study characteristics
Demographic characteristics and details concerning the literature type of the included studies are summarized in Table 1. The studies included in the meta-analysis were conducted in six countries (China, America, Indiana, Australia, South Korea and Italy) from 1988 to 2017 and involved 7323 patients (2030 patients treated with extramedullary systems and 5293 patients treated with intramedullary systems).
Outcomes of meta-analysis
Lower limb coronal alignment
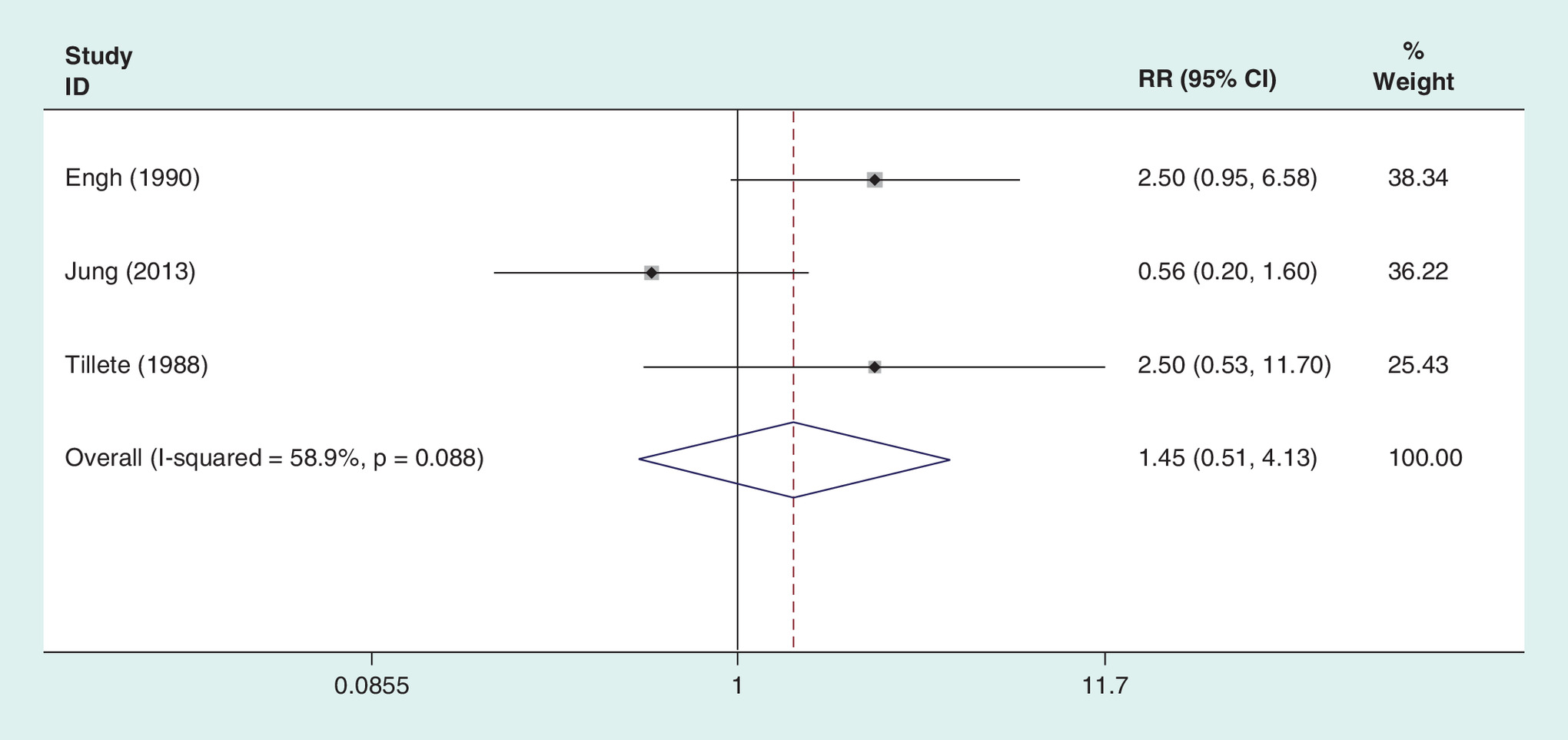
An accuracy comparison of lower limb coronal alignment between the two groups was conducted among three of the included studies. The results show that there were no significant differences between patients treated with extramedullary and intramedullary systems (heterogeneity p = 0.088; I2 = 58.9%; RD = 0.00, 95% CI: -0.05 to 0.06; p = 0.90; Figure 3).
Coronal alignment of femoral component
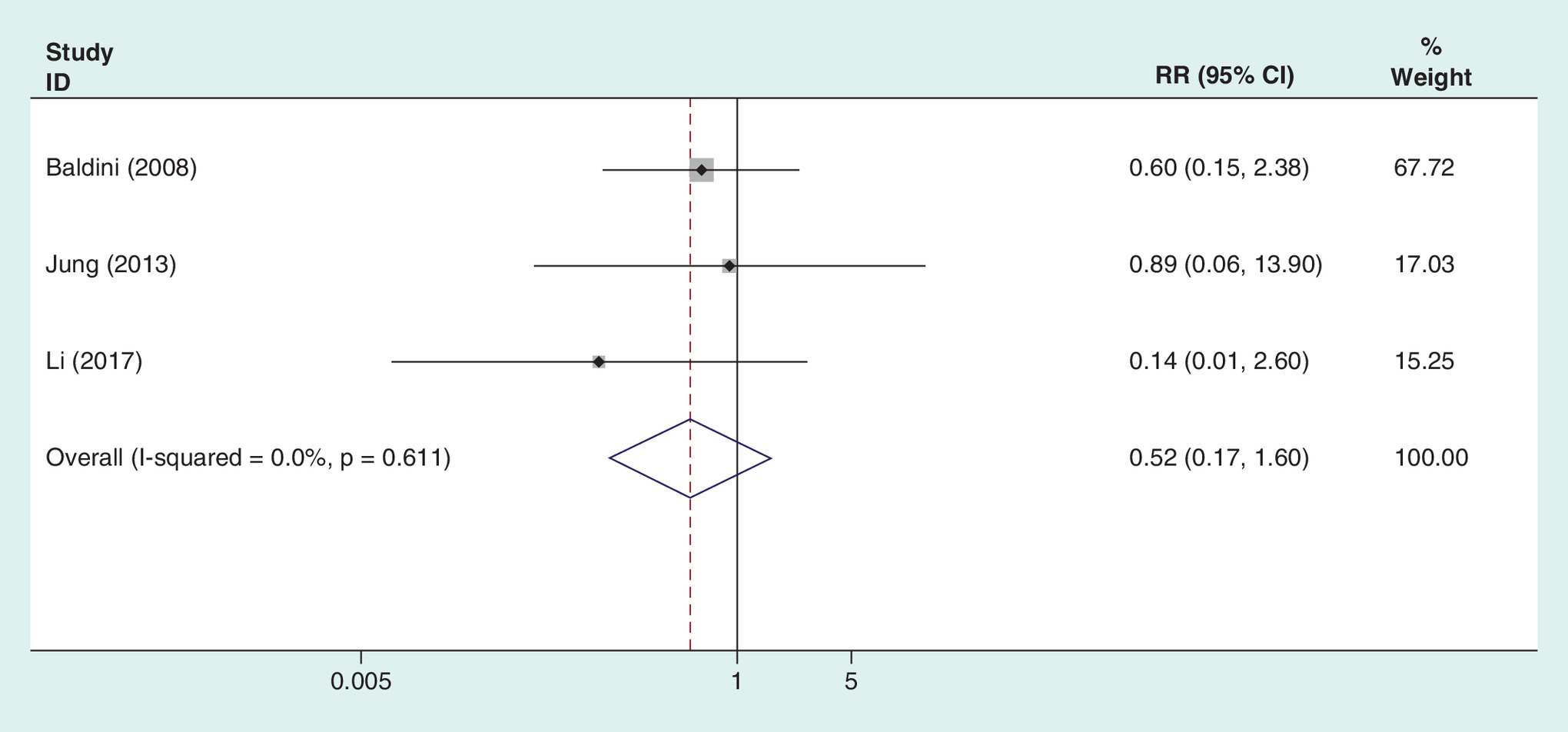
Three articles have been published on the coronal alignment of the femoral component. There is no heterogeneity in the statistical results of the pooled literature (I2 = 0.0%; p = 0.611). The result of the fixed effect model showed that an extramedullary system could achieve the same accuracy as an intramedullary system on coronal alignment of the femoral component (RR = 0.516; 95% CI: 0.166–1.601; p = 0.252; Figure 4).
Sagittal alignment of femoral component
Three publications reported sagittal alignment of the femoral component among 246 patients. Similar to the results described above, the result of sagittal alignment of the femoral component also showed that an extramedullary system could produce the same clinical effect as the intramedullary system on sagittal alignment of the femoral component (heterogeneity p = 0.303; I2 = 16.3%; RR = 0.662; 95% CI: 0.365 –1. 200; p = 0.174; Figure 5).

Drainage volume
Figure 6 shows the results of the postoperative volume of drainage. In five publications, 210 and 205 patients were enrolled in extramedullary or intramedullary groups, respectively. There was a significant difference between the extramedullary group and the intramedullary group (heterogeneity p = 0.223; I2 = 29.8%; MD = -96.933; 95% CI: -134.652 to -59.214; p = 0.000). The drainage volume in the extramedullary group was significantly lower than that in the intramedullary group.

Transfusion rate
The number of postoperative blood transfusion patients was counted by two authors among 169 patients. In total, 27 patients received blood transfusions in the intramedullary group and 43 patients received blood transfusions in the intramedullary group. The results of the meta-analysis showed that a postoperative blood transfusion was less common in patients in the extramedullary group (heterogeneity p = 0.217; I2 = 34.3%; RR = 0.634; 95% CI: 0.437–0.918; p = 0.016; Figure 7).

Total complications
Complications, including embolism, fracture, vascular nerve injury, or infection, were evaluated in two studies. No significant differences were observed between the extramedullary and intramedullary groups (RD = -0.058; 95% CI: -0.275 to 0.160; p = 0.604; Figure 8) with obvious heterogeneity (heterogeneity p = 0.012; I2 = 84.1%).

Postoperative knee score
The postoperative knee score was reported in two included studies. A fixed-effects model was performed with no heterogeneity (I2 = 0.0%; p = 0.896). The postoperative knee score in the intramedullary group was not significantly higher than that in the extramedullary group (MD = -0.187; 95% CI: -0.918 to 0.543; p = 0.615; Figure 9).

Operation time
Five studies reported the operation time. There was obvious heterogeneity (I2 = 81.6%; p = 0.000); therefore, a random-effects model was applied. Pooling the results demonstrated that the incidence of operation time in the intramedullary group was not significantly lower than that in the extramedullary group (MD = -0.299; 95% CI: -5.192 to 4.594; p = 0.905; Figure 10).

Discussion
The current meta-analysis demonstrated that extramedullary distal femur osteotomy without invading the femoral medullary cavity could significantly reduce postoperative bleeding and the transfusion rate. Furthermore, there are no differences in terms of lower limb coronal alignment or the coronal and sagittal alignment of the femoral component between the extramedullary and intramedullary groups. The alignment of the extramedullary distal femur osteotomy is as accurate as that of the intramedullary systems in TKA patients, with satisfactory long-term safety.
The accuracy of the lower limb mechanical axis is an essential condition to ensure the longevity of the prosthesis and successful operation after TKAs [21]. An intramedullary positioning is referred to as the anatomical axis of the femur. The accuracy of the mechanical axis relies on the precise interpolation point, which is independent of the preoperative imaging evaluation and the observation of the operation. Hence, the subtlety is not easy to control [22].
The literature demonstrated that the intramedullary femoral alignment guide system had superior accuracy by approximately 10% on the coronal alignment [7,23,24]. Engh [17] found that femoral cuts with an intramedullary alignment guide system could achieve higher acceptable rates compared with extramedullary cuts (87.5 vs 68.8%, respectively). Lotke [25] suggested that an intramedullary alignment system is more accurate with a significant increase in the component position compared with knees relying on extramedullary alignment (85.6 versus 72%, respectively). Most scholars support accuracy of the femoral alignment guide system for distal femoral resection and component position is superior to extramedullary alignment.
However, the accuracy of the coronal alignment was 98.2% on the extramedullary distal femur osteotomy system when using the apex of the anterior superior iliac spine and the trochanter of the femur [11]. Furthermore, the length and diameter of the intramedullary rod will also affect the distal femoral varus–valgus angulation. Additionally, the deviation of the coronal alignment and sagittal alignment will occur when the entry point deviates from the anatomical axis [26]. Deakin [27] found that the valgus angle of the conventional intramedullary alignment guide system was 5° to 7°, which may lead to valgus angulation of the distal femur, and the probability of postoperative mechanical axis deviation on the lower limb is more than 3° in 20–40% of patients [28,29]. Jeffery [30] confirmed that the prosthesis loosening rate was 3% within a 3° deviation of a mechanical axis and the prosthesis loosening rate was 24% when the deviation was more than 3° at the 12-month follow-up in TKA patients. Huang [31] reported that the hospital for special surgery knee score was inferior in patients when the deviation of the lower limb alignment is within 3° compared with patients whose deviation is greater than 3°. The study shows that 30–51% of the patients with TKAs require a valgus angle of less than 5° and more than 6°. However, the fixed valgus angle (5°, 6°, 7°) in the intramedullary femoral alignment guide system will result in improper lower limb alignment in some patients [32].
Traditionally, it is not effective to locate the femoral head center by using the extramedullary femoral cutting guide as a sign of the anterosuperior iliac spine (ASIS) and we found great intraoperative variation of inter-ASIS distances [33]. Recently, a newly designed extramedullary mechanical axis marker system has improved the accuracy of the extramedullary alignment guide system without violating the femoral canal. Baldini [12] redesigned a type of extramedullary instrument that is calibrated using templated data obtained from a preoperative anteroposterior view of the full limb during weight bearing and performed an intraoperative double check using an extramedullary rod that referred to the ASIS. They observed that postoperative femoral component coronal alignment within 0° ± 2° in the extramedullary femoral alignment group was similar with the intramedullary group (86 versus 84%, respectively). Seo et al. identified the femoral head center by a new mechanical axis marker and the location of coronal axis markers with the use of table radiographs. The results show that the coronal alignment within 0° ± 3° is 9.4% of all patients in the extramedullary femoral alignment group. Matsumoto et al. [9,34] believed that coronal localization could be achieved satisfactorily, but the accuracy of the sagittal alignment with the anterior cortex of the distal femur was relatively low. Jung [11] reported that the accuracy of sagittal alignment was 83.9% in the extramedullary femoral alignment group, which was lower than that of coronal alignment. The existence of the femur bow results in an average flexion of 6° relative to the mechanical axis of the distal femur. Studies [35] have confirmed that a short intramedullary positioning rod could avoid the anterior femoral notch, but femoral prosthesis flexion was prone to postoperative knee extension difficulty when the distal femoral flexion angle (DFFA) > 12°. Hsu [36] found that the probability of deviation of the femoral lateral mechanical axis within 3° is 32% when DFFA > 12° preoperatively. A total of 69% of patients had a DFFA < 12°.
Dominant blood loss is as high as 380–800 ml, which is mainly from the osteotomy surface and medullary cavity [37,38]. Some publications reported that a large number of small emboli could be detected through the right atrium and right ventricle by transesophageal echocardiography when inserting the intramedullary pin [39,40]. Bone marrow cells and fat embolism have been identified in the emboli and may be one of the foundations of embolism [40]. Femoral extramedullary osteotomy does not invade the femoral medullary cavity, which theoretically reduces or avoids the occurrence of such embolism. Pooled estimates indicate that an extramedullary distal femur osteotomy without invading the femoral medullary cavity could reduce postoperative bleeding (MD = -96.933; 95% CI: -134.652 to -59.214; p = 0.000) and transfusion rate (RR = 0.634; 95% CI: 0.437–0.918; p = 0.016).
Our research also has some limitations that should be considered. First, the low transplant survival rates, ROM scores, radiographic outcomes and other indicators lead to a lack of long-term follow-up indicators. Second, different administrations of prosthetics, operation methods and dramatically different criteria for transfusion might have a biased impact on our results. Third, we only assemble the result of several studies in a single numerical estimate. A systematic review should be performed to identify further relevant data. Finally, the sample sizes of the included studies are relatively small in the present meta-analysis.
Conclusion
Our meta-analysis shows that the alignment of the extramedullary distal femur osteotomy is as accurate as intramedullary systems in TKA patients with satisfactory long-term safety. Furthermore, an extramedullary distal femur osteotomy without invading the femoral medullary cavity could reduce postoperative bleeding and the transfusion rate. Further research is required to test the robustness of our findings when more data is available and by undertaking both Bayesian and frequentist methods. When more data are available, the heterogeneity can be further explored through sensitivity analysis, and the available data can be combined to verify the hypothesis.
Some authors favor that intramedullary alignment produces more accurate and reproducible placement.
A retrospective study revealed that the angle of the tibial and femoral anatomical axis of the coronal alignment in the intramedullary group was more accurate than that of the extramedullary alignment group.
Postoperative x-ray images for 201 patients with intramedullary femoral alignment systems showed that up to 8.5% of the patients had an unsatisfactory mechanical axis.
The advanced extramedullary alignment system has been more accurate in femoral osteotomy with coronal and sagittal alignments by means of the inter-femoral head center distance and the mechanical axis marker systems in total knee arthroplasty.
A meta-analysis concentrating on the intramedullary and extramedullary femoral alignment systems recently pooled the results from studies with finite sample sizes.
Our meta-analysis shows that the alignment of the extramedullary distal femur osteotomy is as accurate as intramedullary systems.
Extramedullary distal femur osteotomy without invading the femoral medullary cavity could reduce postoperative bleeding and the transfusion rate.
Further research is required to test the robustness of our findings when more data are available.
By undertaking both Bayesian and frequentist methods when more data are available to further explore and study heterogeneity through sensitivity analysis, we will be able to test the implicit assumptions that the evidence bases are sufficiently homogeneous to be pooled.
Acknowledgments
The authors would like to thank Tianjin Medical University General Hospital for providing the database.
Author contributions
Y Qin designed the study protocol, participated in the data analysis and drafted the manuscript. N Li, W Hu, Z Li, H Li participated in the analysis and revision of the manuscript. All authors have read and approved the final manuscript.
Financial & competing interests disclosure
This work was supported by funding from the National Natural Science Foundation of China (grant number 81501887). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
1.
Saksena J, Platts AD, Dowd GS. Recurrent haemarthrosis following total knee replacement. The Knee 17(1), 7–14 (2010).
2.
Lee SA, Choi SH, Chang MJ. How accurate is anatomic limb alignment in predicting mechanical limb alignment after total knee arthroplasty? BMC Musculoskel. Disord. 16, 323 (2015).
3.
Manjunath KS, Gopalakrishna KG, Vineeth G. Evaluation of alignment in total knee arthroplasty: a prospective study. Eur. J. Orthop. Surg. Traumatol. 25(5), 895–903 (2015).
4.
Schiraldi M, Bonzanini G, Chirillo D, de Tullio V. Mechanical and kinematic alignment in total knee arthroplasty. Ann. Trans. Med. 4(7), 130 (2016).
5.
McConnell J, Dillon J, Kinninmonth A, Sarungi M, Picard F. Blood loss following total knee replacement is reduced when using computer-assisted versus standard methods. Acta Orthop. Belg. 78(1), 75–79 (2012).
6.
Laskin RS. Alignment of total knee components. Orthopedics 7(1), 62–72 (1984).
7.
Maestro A, Harwin SF, Sandoval MG, Vaquero DH, Murcia A. Influence of intramedullary versus extramedullary alignment guides on final total knee arthroplasty component position: a radiographic analysis. J. Arthroplasty 13(5), 552–558 (1988).
8.
Dennis DA, Channer M, Susman MH, Stringer EA. Intramedullary versus extramedullary tibial alignment systems in total knee arthroplasty. J. Arthroplasty 8(1), 43–47 (1993).
9.
Meding JB, Berend ME, Ritter MA, Galley MR, Malinzak RA. Intramedullary versus extramedullary femoral alignment guides: a 15-year follow-up of survivorship. J. Arthroplasty 26(4), 591–595 (2011).
10.
Teter KE, Bregman D, Colwell CW Jr. The efficacy of intramedullary femoral alignment in total knee replacement. Clin. Orthop. Relat. Res. 321, 117–121 (1995).
11.
Jung WH, Chun CW, Lee JH, Ha JH, Jeong JH. The accuracy of the extramedullary and intramedullary femoral alignment system in total knee arthroplasty for varus osteoarthritic knee. Knee Surg. Sports Traumatol. Arthrosc. 21(3), 629–635 (2013).
12.
Baldini A, Adravanti P. Less invasive TKA: extramedullary femoral reference without navigation. Clin. Orthop. Relat. Res. 466(11), 2694–2700 (2008).
13.
Jeon SH, Kim JH, Lee JM, Seo ES. Efficacy of extramedullary femoral component alignment guide system for blood saving after total knee arthroplasty. Knee Surg. Relat. Res. 24(2), 99–103 (2012).
14.
Sparmann M, Wolke B, Czupalla H, Banzer D, Zink A. Positioning of total knee arthroplasty with and without navigation support: a prospective, randomized study. JBJS 85(6), 830–835 (2003).
15.
Mihalko WM, Duquin T, Axelrod JR, Bayers-Thering M, Krackow KA. Effect of one- and two-pin reference anchoring systems on marker stability during total knee arthroplasty computer navigation. Comput. Aided Surg. 11(2), 93–98 (2006).
16.
Kandel L, Vasili C, Kirsh G. Extramedullary femoral alignment instrumentation reduces blood loss after uncemented total knee arthroplasty. J. Knee Surg. 19(4), 256–258 (2006).
17.
Engh GA, Petersen TL. Comparative experience with intramedullary and extramedullary alignment in total knee arthroplasty. J. Arthroplasty 5(1), 1–8 (1990).
18.
Li H, Sun Z, Hu Z, Zhao C, Li Y, Sun C. Clinical application of self-made distal femur alignment cutting template in total knee arthroplasty. Chinese J. Orthop. 37(11), 660–669 (2017).
19.
Zhang H, He M, Shan P et al. Development and application of extramedullary femoral osteotomy module in total knee arthroplasty. Chinese J. Orthopaed. 37(11), 651–659 (2017).
20.
Tillett ED, Engh GA, Petersen T. A comparative study of extramedullary and intramedullary alignment systems in total knee arthroplasty. Clin. Orthop. Rel. Res. 5(230), 176–181 (1988).
21.
Rodricks DJ, Patil S, Pulido P, Colwell CW Jr. Press-fit condylar design total knee arthroplasty: fourteen to seventeen-year follow-up. J. Bone Joint Surg. Am. 89(1), 89–95 (2007).
22.
Ma B, Long W, Rudan JF, Ellis RE. Three-dimensional analysis of alignment error in using femoral intramedullary guides in unicompartmental knee arthroplasty. J. Arthroplasty 21(2), 271–278 (2006).
23.
Blakeney WG, Khan RJ, Palmer JL. Functional outcomes following total knee arthroplasty: a randomised trial comparing computer-assisted surgery with conventional techniques. The Knee 21(2), 364–368 (2014).
24.
Bian YY, Weng XS, Lin J, Jin J, Qian WW, Zhai JL, Zhao LJ. Comparison of clinical influence of intramedullary versus extramedullary alignment guides on total knee arthroplasty. Zhongguo yi xue ke xue yuan xue bao Acta Academiae Medicinae Sinicae. 37(4), 373–377 (2015).
25.
Lotke PA, Ecker ML. Influence of positioning of prosthesis in total knee replacement. J. Bone Joint Surg. Am. 59(1), 77–79 (1977).
26.
Nuno-Siebrecht N, Tanzer M, Bobyn JD. Potential errors in axial alignment using intramedullary instrumentation for total knee arthroplasty. J. Arthroplasty 15(2), 228–230 (2000).
27.
Deakin AH, Sarungi M. A comparison of variable angle versus fixed angle distal femoral resection in primary total knee arthroplasty. J. Arthroplasty 29(6), 1133–1137 (2014).
28.
Nunley RM, Ellison BS, Ruh EL et al. Are patient-specific cutting blocks cost-effective for total knee arthroplasty? Clin. Orthop. Relat. Res. 470(3), 889–894 (2012).
29.
Iorio R, Bolle G, Conteduca F et al. Accuracy of manual instrumentation of tibial cutting guide in total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 21(10), 2296–2300 (2013).
30.
Jeffery RS, Morris RW, Denham RA. Coronal alignment after total knee replacement. J. Bone Joint Surg. Br. 73(5), 709–714 (1991).
31.
Huang NF, Dowsey MM, Ee E, Stoney JD, Babazadeh S, Choong PF. Coronal alignment correlates with outcome after total knee arthroplasty: five-year follow-up of a randomized controlled trial. J. Arthroplasty 27(9), 1737–1741 (2012).
32.
Bardakos N, Cil A, Thompson B, Stocks G. Mechanical axis cannot be restored in total knee arthroplasty with a fixed valgus resection angle: a radiographic study. J. Arthroplasty 22(6 Suppl. 2), 85–89 (2007).
33.
Mullaji A, Shetty GM, Kanna R, Sharma A. Variability in the range of inter-anterior superior iliac spine distance and its correlation with femoral head centre: a prospective computed tomography study of 200 adults. Skeletal Radiol. 39(4), 363–368 (2010).
34.
Matsumoto K, Mori N, Ogawa H, Akiyama H. Accuracy of a novel extramedullary femoral alignment guide system in primary total knee arthroplasty. Arch. Orthop. Trauma Surg. 135(12), 1743–1748 (2015).
35.
Sun Z, Cao J, Tian M et al. Effect of distal femoral flexion angle on sagittal alignment of femoral prosthesis and function recovery after total knee arthroplasty. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 25(1), 38–41 (2011).
36.
Hsu WH, Hsu RW, Weng YJ. Effect of preoperative deformity on postoperative leg axis in total knee arthroplasty: a prospective randomized study. Knee Surg. Sports Traumatol. Arthrosc. 18(10), 1323–1327 (2010).
37.
Yang ZG, Chen WP, Wu LD. Effectiveness and safety of tranexamic acid in reducing blood loss in total knee arthroplasty: a meta-analysis. J. Bone Joint Surg. Am. 94(13), 1153–1159 (2012).
38.
Charoencholvanich K, Siriwattanasakul P. Tranexamic acid reduces blood loss and blood transfusion after TKA: a prospective randomized controlled trial. Clin. Orthop. Relat. Res. 469(10), 2874–2880 (2011).
39.
Wauke K, Nagashima M, Kato N, Ogawa R, Yoshino S. Comparative study between thromboembolism and total knee arthroplasty with or without tourniquet in rheumatoid arthritis patients. Arch. Orthop. Trauma Surg. 122(8), 442–446 (2002).
40.
Kim YH. Incidence of fat embolism syndrome after cemented or cementless bilateral simultaneous and unilateral total knee arthroplasty. J. Arthroplasty 16(6), 730–739 (2001).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 7 July 2018
Accepted: 1 October 2018
Published online: 28 November 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Intramedullary versus extramedullary alignment guides on total knee arthroplasty: a meta-analysis. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0064
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Lars‐Rene Tuecking, Marco Ezechieli, Christoph Barkhausen, Christian Hendrich, Lea Charlotte Wienholt, Christoph Pross, Rüdiger von Eisenhart‐Rothe, Henning Windhagen, Reduced length of stay and improved perioperative outcomes in robotic‐arm‐assisted TKA: A real‐world evidence study of 63,931 cases from German hospitals, Knee Surgery, Sports Traumatology, Arthroscopy, 10.1002/ksa.70437, (2026).
- Gennaro Pipino, Francesco Anzano, Enzo Claudio Moretti, Raffaele Borghi, Davide Corrado Vaccarisi, Patrizio Caldora, Bruno Violante, Nicola Maffulli, Filippo Migliorini, Vincenzo Salini, Clinical outcomes of intramedullary tibial guides in total knee arthroplasty: experience from a single-centre cohort, Journal of Orthopaedic Surgery and Research, 10.1186/s13018-025-06369-9, 20, 1, (2025).
- Ming Li, Jun Li, Shuai Hu, Bingshen Jia, Comparison of intramedullary versus extramedullary alignment technique in total knee arthroplasty: A PRISMA-compliant meta-analysis, Medicine, 10.1097/MD.0000000000032277, 102, 5, (e32277), (2023).