Intravitreal aflibercept versus intravitreal ranibizumab in patients with age-related macular degeneration: a comparative effectiveness study
Abstract
Aim: A hospital-wide, unselected switch of ranibizumab to aflibercept in treatment of age-related macular degeneration (AMD) allowed us to compare the clinical effectiveness of these agents. Method: In a single-center before–after, observational study design new AMD-patients started with aflibercept treatment in 2013–2014 were compared with a control group of AMD-patients on ranibizumab before the switch. Results: The mean difference in visual acuity (in logMAR units) after 1 year was comparable (+0.012 [aflibercept, n = 37] vs +0.17 [ranibizumab, n = 30], p = 0.154). However, the aflibercept-group did receive more intravitreal injections (5.8 vs 4.7 injections, p = 0.004) and were treated longer (265.7 vs 197.7 days; p = 0.011). Conclusion: With no difference in clinical effectiveness, longer treatment intervals for aflibercept should be investigated.
Comparative effectiveness research (CER) is a vital strategy in translating the efficacy of a new clinical intervention as established in clinical trials to its effectiveness in ‘real world’ patients. The purpose of CER is to inform clinicians and policy makers in making decisions based on real-world data that improve health at both the population and individual level [1].
In the recent years, treatment of age-related macular degeneration (AMD), a disease that is characterized by VEGF-mediated neovascularization that can lead to small bleedings and scar formation under the retina, has evolved majorly with the introduction of several anti-VEGF agents [2,3]. At first, monthly intravitreal injections with ranibizumab and bevacizumab were extensively used, although the use of bevacizumab was off-label. Clinical trials have shown that these agents not only prevent further loss of vision, but also could recuperate some vision in AMD [4]. No significant differences between bevacizumab and ranibizumab have been observed regarding these effects [4]. A few years ago, aflibercept has also been approved by the US FDA and the EMA for the treatment of exudative AMD. A difference with the standard anti-VEGF therapy (ranibizumab and bevacizumab) is the fact that after three monthly injections aflibercept can be injected bimonthly instead of monthly [5]. First clinical efficacy studies confirmed that bimonthly aflibercept is equivalent to monthly ranibizumab and even could be an option for patients with persistent fluid while on ranibizumab and/or bevacizumab therapy [5,6]. As of 1 April 2013, aflibercept was introduced in our large teaching hospital (St. Antonius Hospital, Nieuwegein/Utrecht, the Netherlands). From that time, all patients newly diagnosed with AMD started with aflibercept and current patients were switched from ranibizumab to aflibercept. This full and unselected switch of our treatment policy provided us with an unique opportunity to compare the clinical effectiveness of aflibercept and ranibizumab in a before–after, observational study in a real world setting.
Materials & methods
In this before–after, cross-sectional observational study, the clinical effectiveness after 12 months was compared between a group of patients with exudative AMD that started with aflibercept (April 2013–April 2014) and a control group of patients with the same diagnosis who have been treated with ranibizumab in the years before the switch (2007–2013). Since the number of patients treated with ranibizumab was substantially larger, a smaller subset of patients was randomly sampled to match the sample size of the aflibercept cohort. To be eligible for analysis, patients had to have a new diagnosis of AMD and have a visual acuity score available at maximum 60 days before treatment start. Subsequently, we excluded patients that received only one injection or had no follow-up visual acuity score between 9 and 12 months after start of anti-VEGF treatment. The specific treatment regimen (dosage, frequency and number of injections, visits) was determined by the treating ophthalmologist and patient and thereby fully representative for real-world practice. In general, patients were treated with ranibizumab according to a treat-and-extend regime, or an ‘as-needed’ (Pro Re Nata, PRN) regime. Aflibercept was applied according to the Summary of Product Characteristics (SmPC) recommendations. The study protocol adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of St. Antonius Hospital (R&D/Z-13.27). Because of the observational nature of the study, the need for informed consent was waived by the IRB. For all patients, the data on visual acuity and dates of injections were obtained from our hospital’s ophthalmologic medical record system (Ifa® version 6.0.81). During the entire study period (2007–2014), visual acuity scores have been measured as best corrected distance visual acuity, captured using a Snellens chart and recorded on a decimal scale by ophthalmic technicians. For comparative analyses purposes, these visual acuity scores were converted to LogMAR units by calculating the negative logarithm as published before [7]. The primary study parameter was the difference in mean visual acuity at start (VAstart) and 12 months after start of anti-VEGF treatment (VAend, with a margin of 9–15 months, using the visual acuity score closest to 12 months). To correct for differences in visual acuity at start, we also assessed the difference in relative visual acuity (RVA) after 1 year. RVA was calculated as follows: RVA (%) = VAend (LogMAR units)/Vstart (LogMAR units) × 100%. Secondary study parameters included: progression of disease (defined as >0.3 LogMAR units increase in visual acuity after 12 months, equivalent to a loss of >15 letters on the Early Treatment Diabetic Retinopathy Study charts), total number of injections, mean time between injections (in days) and mean time between the first and last injection (in days). Statistical analyses were performed with the commercial software package SPSS Statistics for Windows (version 22). Categorical data were analyzed by χ2 test and continuous data by independent sample t-test (if normally distributed) or rank test (if not normally distributed) where appropriate. Differences with a p-value of <0.05 were considered significant. To assess potential bias from differential drop out of patients between the two groups, a sensitivity analysis was conducted in which all patients with at least one injection were included irrespective of whether that they had a follow-up visual acuity score between 9–15 months from start. In this analysis, the last available visual acuity was used as end point (sort of intention-to-treat analysis).
Results
Overall, a total of 89 eyes (from 80 patients) could be identified of which 75% (ranibizumab) to 76% (aflibercept) (30 and 37 eyes, respectively) had follow-up visual acuity data available, yielding a total of 67 treated eyes available for analysis (see Figure 1 for a flowchart of inclusion). Baseline characteristics of the two groups are provided in Table 1.
| Baseline characteristic | Aflibercept (n = 37) | Ranibizumab (n = 30) | p-value |
|---|---|---|---|
| Age (mean ± SD, years) | 81.2 ( ± 7.4) | 79.9 ( ± 6.7) | 0.466 |
| Male (%) | 38 | 50 | 0.318 |
| Affected eye (% left) | 46 | 53 | 0.548 |
| Visual acuity at start (mean ± SD, LogMAR units) | 0.59 ± 0.48 | 0.74 ± 0.41 | 0.183 |
SD: Standard deviation.
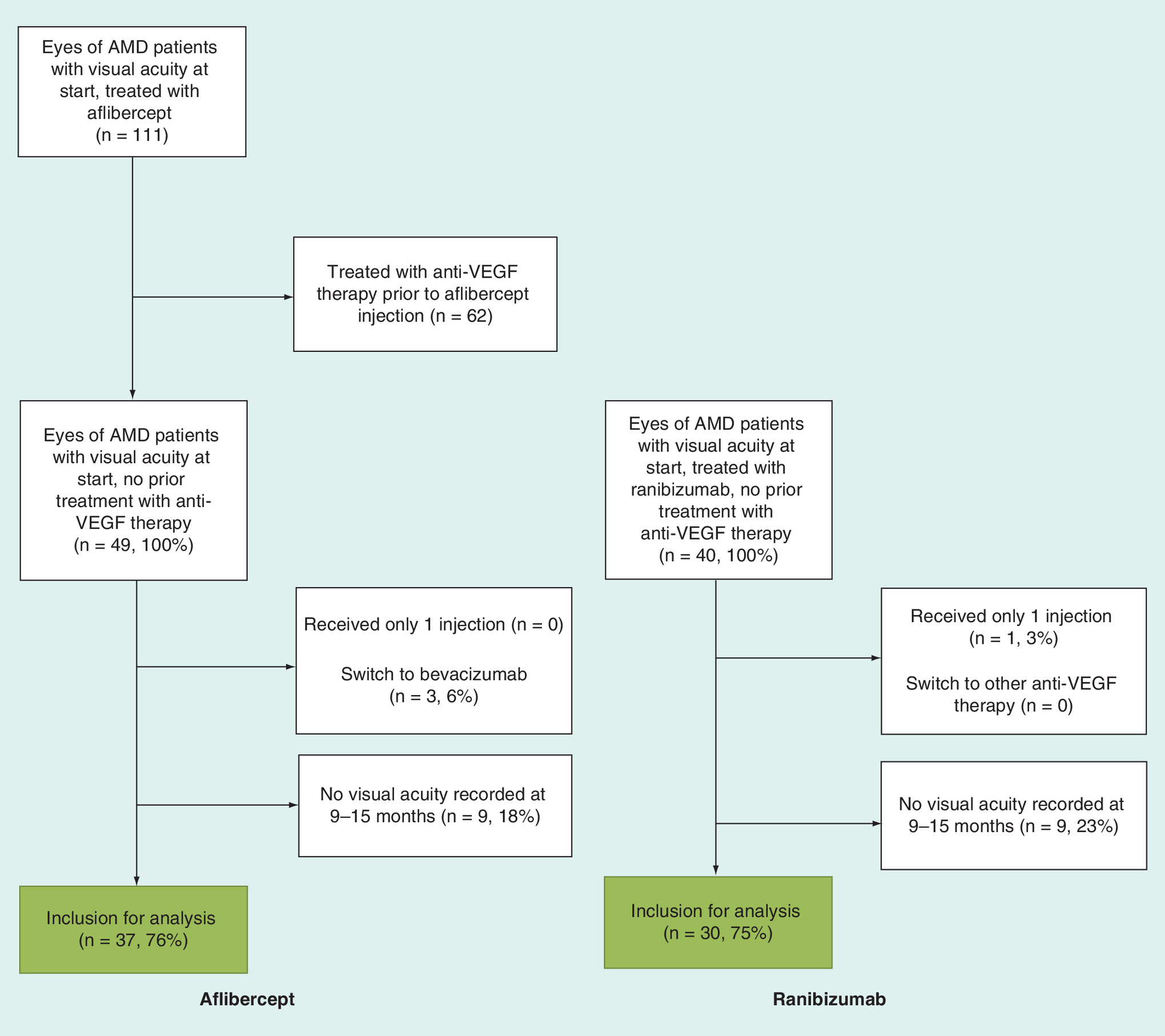
Figure 1. Flowcharts describing patient inclusion for the aflibercept and ranibizumab cohort.
AMD: Age-related macular degeneration.
The development of normalized visual acuity scores (per group) in the first year after start of treatment is shown in Figure 2. The mean and relative difference in visual acuity at 1 year of treatment did not differ between the aflibercept and ranibizumab group (0.012 vs 0.17; p = 0.154 and 122 vs 120%; p = 0.946, respectively), as shown in Table 2. In both groups, there was also no statistically significant difference in the number of patients with progressive disease after 1 year (five [14%] in the aflibercept vs nine [30%] in the ranibizumab group, p = 0.099). Eyes treated with aflibercept did receive more intravitreal injections (5.8 vs 4.7 injections, p = 0.004) and were treated for a longer period (265.7 vs 197.7 days; p = 0.011) during the study period in comparison with ranibizumab-treated eyes. No differences were found in number of days between injections (mean 53.8 vs 53.2 days).
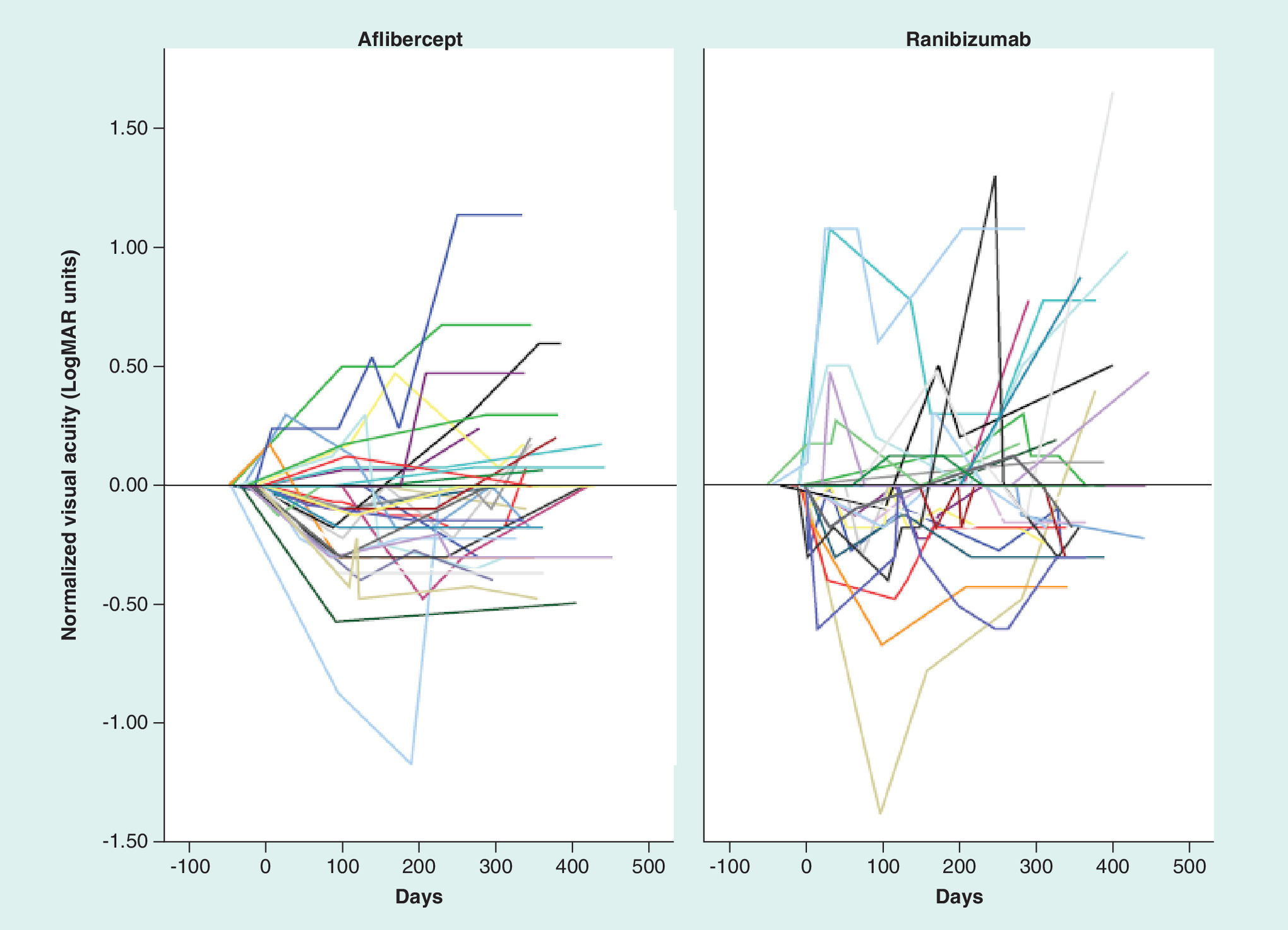
Figure 2. Development of the normalized visual acuity in eyes that were treated with aflibercept for 1 year (n = 37) compared to eyes treated with ranibizumab for 1 year (n = 30).
Visual acuity scores are shown in LogMAR units and normalized to visual acuity score at start (first injection with anti-VEGF drug). Each line represents one eye.
| Outcome measure | Aflibercept (n = 37) | Ranibizumab (n = 30) | Mean difference (95% CI) |
|---|---|---|---|
| Difference in mean visual acuity after 1 year (LogMAR units ± SD) | 0.012 ± 0.34 | 0.17 ± 0.51 | -0.16 (-0.37–0.06) |
| Relative mean visual acuity at 1 year (% of start ± SD) | 122 ± 136 | 120 ± 82 | 2.8 (-0.5–5.8) |
| Number of injections ( ± SD) | 5.8 ± 1.5 | 4.7 ± 1.5 | 1.1 (0.4–1.8) |
| Mean period between injections (days ± SD) | 53.8 ± 12.0 | 53.2 ± 28.0 | 0.7 (-10.4–11.8) |
| Duration of active treatment (days between first and last injection ± SD) | 265.7 ± 103.6 | 197.7 ( ± 108.3) | 25.9 (16.1–119.9) |
SD: Standard deviation.
Discussion
Our results show that in our real world setting, clinical effectiveness was comparable between aflibercept and ranibizumab. Visual acuity scores after 1 year did not differ between patients with AMD who were treated with aflibercept compared with ranibizumab. In both groups, the vision scores remained stable during the 1-year observation period. Interestingly, we observed that during the study period, patients who were treated with aflibercept received, on average, one injection more in comparison with the ranibizumab-patients (5.8 and 4.7 injections/year, respectively). In addition, the patients who were treated with aflibercept were treated for a longer period of time (almost 70 days longer). The average time between injections did not differ between the two groups.
The observed differences in dosing regimens contrast with the VIEW trials [5], in which monthly ranibizumab was compared with bimonthly aflibercept (after three monthly injections), but do align with other recent observational studies that also found similar dosing frequencies for ranibizumab and aflibercept [8–11]. In our study, aflibercept treatment was applied in compliance with SmPC recommendations of bimonthly injections, while a similar bimonthly regimen was already employed for ranibizumab (an ‘as needed’ or treat-and-extend regimen). With these regimens, aflibercept and ranibizumab seem to provide similar visual acuity outcomes after 1 year.
The major strength of our study is that we were able to obtain information on the clinical effectiveness of aflibercept versus ranibizumab in a real-world setting. In our study, both treatment and outcome data were recorded as part of routine clinical care. For the visual acuity outcome, a validated method based on the Snellens chart was employed. Also, our study has a low risk of selection bias because ranibizumab was replaced by aflibercept for both new and existing patients without exception (April 2013), and our analysis was restricted to patients who started anti-VEGF treatment (new users). Furthermore, other possible confounding factors, such as different logistics or method for measurement of visual acuity remained unaltered over the years further adding to a low risk of bias.
However, as with most observational studies, there are also limitations that need to be addressed. First, in the control group of patients, there was a relatively higher percentage of patients with no visual acuity score at 9–15 months (23 vs 18%). It is possible that some of these patients seized treatment due to ineffectiveness, in which case this could bias our results and conclusions. On the other hand, our sensitivity analysis, in which patients excluded for this reason were reintroduced, did result in similar findings (data not shown). Second, we observed a higher visual acuity score at baseline in the aflibercept group (although this was not statistically significant). A higher visual acuity at baseline could mean a more aggressive approach in treating AMD in the recent years. A better visual acuity score at start might result in a lower absolute effect of the anti-VEGF treatment. Even though, we observed no difference in relative visual acuity after 1 year. This implies that the effect of visual acuity at start could be considered as limited. In hindsight, the difference in entry level visual acuity could have been absent if only ranibizumab patients would have been selected from the last years before switching to aflibercept. Another option could have been to match patients based on entry level visual acuity. However, we considered matching not necessary beforehand because of the very low risk of confounding (by indication) bias since all patients received aflibercept without exception from April 2013. Finally, we chose visual acuity scores as our end point since this was also employed in the VIEW trials [5]. In the future, it would be interesting to obtain data in daily clinical practice on vision-related quality of life, as was recently done in trial-context in the VIEW 1 and 2 groups [12].
This study illustrates the promising value of CER in ophthalmology. For expensive treatments, such as anti-VEGF for AMD, a cost-driven decision to switch from monthly ranibizumab to bimonthly aflibercept should, in our opinion, always be accompanied with a suitable follow-up analysis of effects. CER could help to examine how the effectiveness of the new standard treatment matches the former first choice treatment and the results from clinical trials. Besides this, CER could provide information on whether the new treatment does yield the expected lower healthcare costs in a real-life setting. Concerning this last aspect, our study shows that the amount of anti-VEGF injections did not decrease after the introduction of aflibercept, since an ‘as needed’ or ‘treat-and-extend’ regimen was already employed for ranibizumab in our clinical practice.
Our finding that visual acuity outcomes of bimonthly aflibercept were similar to a lower ranibizumab injection frequency than studied in the VIEW trials, suggests that the dosing frequency of aflibercept might also be reducible. A mathematical model showed that intravitreal VEGF-binding activity could remain up to 10–12 weeks after a single injection with aflibercept [13]. It would be interesting to investigate the possibility of longer intervals between injections with aflibercept. Otherwise the advantage of aflibercept’s lower injection frequencies as investigated in the clinical trial setting will not be realized in clinical practice. So far, the first studies regarding this aspect showed inconsistent results [14–16].
Conclusion
This comparative effectiveness study showed no difference in clinical effectiveness between bimonthly aflibercept and ranibizumab being applied in a reduced dosing intensity. The latter supports the need to further investigate the possibilities of longer time intervals between injections with aflibercept as well.
In 2013, all patients in our large teaching hospital who were newly diagnosed with age-related macular degeneration (AMD) were treated with aflibercept as primary anti-VEGF agent.
This full and unselected switch of our treatment policy provided us with a unique opportunity to compare the clinical effectiveness of aflibercept and ranibizumab in a before–after, observational study in a real world setting.
The mean difference in visual acuity after 1 year was comparable between both groups (+0.012 [aflibercept, n = 37] vs +0.17 (ranibizumab, n = 30; p = 0.154). However, patients in the aflibercept group did receive more intravitreal injections (5.8 vs 4.7 injections; p = 0.004) and were treated longer (265.7 vs 197.7 days; p = 0.011). No differences were found in number of days between injections (mean 53.8 vs 53.2 days).
In our population, aflibercept treatment was applied in compliance with Summary of Product Characteristics recommendations of bimonthly injections, while a similar bimonthly regimen was already employed for ranibizumab (an ‘as needed’ or treat-and-extend regimen). With these regimens, aflibercept and ranibizumab seem to provide similar visual acuity outcomes after 1 year.
It would be interesting to investigate the possibility of longer intervals between injections with aflibercept. Otherwise, the advantage of aflibercept’s lower injection frequencies as investigated in the clinical trial setting will not be realized in clinical practice.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The study protocol adhered to the tenets of the Declaration of Helsinki and was approved by the IRB of St. Antonius Hospital (R&D/Z-13.27). Because of the retrospective nature of the study, the need for informed consent was waived by the IRB.
References
Papers of special note have been highlighted as: • of interest
1.
Sox HC, Greenfield S. Comparative effectiveness research: a report from the Institute of Medicine. Ann. Intern. Med. 151(3), 203–205 (2009).
2.
Jager RD, Mieler WF, Miller JW. Age-related macular degeneration. N. Engl. J. Med. 358(24), 2606–2617 (2008).
• Elaborate overview of the pathophysiology and management of age-related macular degeneration.
3.
Yancopoulos GD. Clinical application of therapies targeting VEGF. Cell 143(1), 13–16 (2010).
4.
Group CR, Martin DF, Maguire MG et al. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 364(20), 1897–1908 (2011).
5.
Heier JS, Brown DM, Chong V et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 119(12), 2537–2548 (2012).
• The VIEW trials, large, multicenter studies that prospectively compared monthly ranibizumab with several aflibercept dosing regimens, demonstrated that bimonthly aflibercept had comparable efficacy to monthly ranibizumab in a prospective trial setting.
6.
Cho H, Shah CP, Weber M et al. Aflibercept for exudative AMD with persistent fluid on ranibizumab and/or bevacizumab. Br. J. Ophthalmol. 97(8), 1032–1035 (2013).
7.
Holladay JT. Proper method for calculating average visual acuity. J. Refract. Surg. 13(4), 388–391 (1997).
8.
Johnston SS, Wilson K, Huang A, Smith D, Varker H, Turpcu A. Retrospective analysis of first-line anti-vascular endothelial growth factor treatment patterns in wet age-related macular degeneration. Adv. Ther. 30(12), 1111–1127 (2013).
9.
Reich O, Bachmann LM, Faes L et al. Anti-VEGF treatment patterns and associated health care costs in Switzerland: findings using real-world claims data. Risk Manag. Healthc. Policy 8, 55–62 (2015).
10.
Lotery AJ, Regnier S. Patterns of ranibizumab and aflibercept treatment of central retinal vein occlusion in routine clinical practice in the USA. Eye (Lond.) 29(3), 380–387 (2015).
11.
Böhni SC, Bittner M, Howell JP, Bachmann LM, Faes L, Schmid MK. Comparison of Eylea® with Lucentis® as first-line therapy in patients with treatment-naïve neovascular age-related macular degeneration in real-life clinical practice: retrospective case-series analysis. BMC Ophthalmol. 15, 109 (2015).
12.
Yuzawa M, Fujita K, Wittrup-Jensen KU et al. Improvement in vision-related function with intravitreal aflibercept: data from Phase III studies in wet age-related macular degeneration. Ophthalmology 122(3), 571–578 (2015).
13.
Stewart MW, Rosenfeld PJ. Predicted biological activity of intravitreal VEGF Trap. Br. J. Ophthalmol. 92(5), 667–668 (2008).
14.
Ohnaka M, Nagai Y, Sho K et al. A modified treat-and-extend regimen of aflibercept for treatment-naïve patients with neovascular age-related macular degeneration. Graefe's Arch. Clin. Exp. Ophthalmol. 255(4), 657–664 (2017).
15.
Takayama K, Kaneko H, Sugita T et al. One-year outcomes of 1 + pro re nata versus 3 + pro re nata intravitreal aflibercept injection for neovascular age-related macular degeneration. Ophthalmologica 237(2), 105–110 (2017).
16.
Mori R, Tanaka K, Haruyama M, Kawamura A, Furuya K, Yuzawa M. Comparison of pro re nata versus bimonthly injection of intravitreal aflibercept for typical neovascular age-related macular degeneration. Ophthalmologica 238(1–2), 17–22 (2017).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 12 December 2017
Accepted: 12 January 2018
Published online: 1 June 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Intravitreal aflibercept versus intravitreal ranibizumab in patients with age-related macular degeneration: a comparative effectiveness study. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0099
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Xue Wang, Chaofeng Yu, Jingjing Ding, Comparison of Aflibercept and Ranibizumab on Functional and Morphological Outcome in Exudative Age-Related Macular Degeneration, Journal of Biosciences and Medicines, 10.4236/jbm.2025.132025, 13, 02, (330-347), (2025).
- Daniele Veritti, Valentina Sarao, Valentina Soppelsa, Carla Danese, Jay Chhablani, Paolo Lanzetta, Managing Neovascular Age-Related Macular Degeneration in Clinical Practice: Systematic Review, Meta-Analysis, and Meta-Regression, Journal of Clinical Medicine, 10.3390/jcm11020325, 11, 2, (325), (2022).
- Ozgul Ugurtay, Alev Kockar, Elvan Alper Sengul, Real Life Data of Treat and Extend Intravitreal Ranibizumab and Aflibercept Therapy in Wet Age-related Macular Degeneration Patients: 3-Year Results, Korean Journal of Ophthalmology, 10.3341/kjo.2020.0109, 35, 4, (280-286), (2021).