Gene therapy: evidence, value and affordability in the US health care system
Abstract
Aims: To explore the challenges presented by gene therapies, discuss potential solutions, and present policy recommendations. Methods: A review of the literature and series of expert interviews were conducted and discussed at a Policy Forum convened by The Institute for Clinical and Economic Review (ICER). The Policy Forum was attended by independent experts and senior representatives from 20 payer organizations and life sciences companies. Results: Three categories of challenges are identified: evidence generation, assessing value and affordability. Possible solutions and policy recommendations are presented for each of the three main categories of challenges. Conclusions: Gene therapies present exciting opportunities, but also pose major challenges. Dialogue between manufacturers and payers around the issues and possible solutions is crucial.
Gene therapy is coming to the US health care system; the first gene therapy is likely to receive regulatory approval in early 2018. Some gene therapies offer the potential for short ‘one-off’ treatments leading to lifelong benefits. The American Medical Association reports that around 4000 diseases have been linked to gene disorders (including cancers, AIDS, cystic fibrosis, and Parkinson's and Alzheimer's diseases) [1]. The promise of successful treatment with gene therapy could therefore positively affect millions of lives.
However, there are many challenges to be overcome: the science is complex, treatment is technically difficult, and the regulatory approval process is necessarily different to that for ‘conventional’ therapies. Gene therapies are also expected to be costly, particularly if they are administered as single or short-term treatments, and are likely to pose major affordability challenges. This raises concerns about the sustainability of the traditional model for the adoption of innovation if patients are to get access to these treatments. What challenges do these therapies give rise to, and how should payers and manufacturers address them?
What is gene therapy?
The American Medical Association describes gene therapy as “a novel approach to treat, cure, or ultimately prevent disease by changing the expression of a person's genes” [1]. Some gene mutations result in proteins not being made correctly (or not being made at all) and can lead to genetic disorders. Gene therapy works by repairing, dis-activating (‘turning-off’) or replacing dysfunctional genes that cause disease with the aim of (re)establishing normal function [1–3].
The gene therapy pipeline
The first commercially available gene therapy, alipogene tiparvovec (Glybera®, UniQure, Amsterdam, The Netherlands) for the treatment of lipoprotein lipase deficiency, was approved for use in the EU in 2012, but has not been approved by the US FDA (UniQure abandoned plans to gain FDA approval for Glybera in 2015 when additional trials were requested). Furthermore, in Europe it has to date only been paid for use in one patient, partly due to its notional US$1.4 million price tag [4]. The company did not renew the marketing authorization when it expired in October 2017 [5]. A second gene therapy, Strimvelis™ (GlaxoSmithKline, Middlesex, UK) for severe combined immune deficiency in children, is also approved in Europe (as of 2016), but not yet in the USA. The FDA has yet to approve a gene therapy. The process by which it reviews gene therapies is summarized in Box 1.
A report from Pharmaprojects [6] suggests that the number of gene therapies in development has increased rapidly in the last 2–3 years. Boliter reports that there are currently 23 gene therapies in active Phase III development. If one can assume the same success rates as for conventional therapies at Phase III [7], then up to 12–14 of the gene therapies that are currently in active Phase III development (around 5–6 non-cancer therapies and 7–8 cancer therapies) may submit a new license application in the next couple of years.
The current front-runner for approval is Spark Therapeutics’ voretigene neparvovec for the treatment of vision loss due to biallelic RPE65-mediated inherited retinal disorder. Results from a Phase III study indicate that this one-time treatment has the potential to provide clinically meaningful and long-lasting improvements in retinal sensitivity. Spark Therapeutics completed submission of a Biologics Licensing Application with the FDA in May 2017, setting up a potential approval decision by January 2018 [8].
To explore the opportunities and challenges presented by the advent of gene therapies, the Institute for Clinical and Economic Review (ICER) convened a Policy Summit in December 2016 with a group of senior medical policy figures. In this paper, we provide a synthesis of insights collected from the literature, pre-meeting conversations with experts, and discussions held during the Policy Summit. Based on these materials we present a range of policy recommendations to promote innovation and achieve sustainable access to gene therapies within the US health care system.
Methods
The ICER Policy Summit was held in December 2016 with leading experts and representatives from 20 leading insurers, pharmacy benefit management firms and drug manufacturers that compose the ICER membership group. Supplementary Table 1 lists all the attendees. Senior researchers at the Office of Health Economics led the development of a background paper based on a review of the literature and interviews with experts. This was shared with participants prior to the meeting to give them a common foundation in some of the key scientific, conceptual and practical issues. The Policy Summit was conducted under Chatham House rules, whereby participants are able to share comments and perspectives heard at the meeting, but commit to not identify the person or organization making the statement.
This White Paper describes the challenges and potential solutions identified in the literature review and interviews, and includes additional insights from the ICER Policy Summit meeting. The policy recommendations summarize the authors’ views on the key thoughts and suggestions emerging from the discussion at the meeting. They should not be interpreted as a consensus statement from the meeting, nor should they be taken to represent the views of any of the people attending (or organizations represented at) the meeting.
Results & Discussion
The challenges
We identified three key categories of challenges: evidence generation; assessing value; and affordability. Two other key challenges outside of these categories (manufacturing and distribution; ethical dilemmas) also arose – for a short discussion of these issues, see Marsden et al. [9].
Assessing comparative clinical effectiveness
Distinctive evidence challenges that increase uncertainty
Conducting randomized controlled trials (RCTs) can be problematic for gene therapy due to the characteristics of these therapies and the intended patient populations [10,11]. Innovators developing therapies targeting ultra-rare populations defined by a specific biomarker or genetic mutation may find it infeasible to recruit enough patients for an adequately sized RCT. In addition, for those gene therapies that require invasive methods of administration (for example, Glybera requires up to 60 intramuscular injections in the thigh while under sedation or anesthetic), even if a placebo or comparator arm is possible, fully blinded placebo-controlled trial designs would require potentially unethical sham procedures [12]. Gene therapy trials, therefore, will often likely be single-arm trials using historical cohorts for comparison, or ‘waitlist’ trials in which untreated patients cross over to the treatment arm after a relatively short duration of time. A literature review of biases likely to affect non-randomized studies conducted by Hettle et al. [11] found that, unless historical control data are available, single arm trials are likely to produce optimistic estimates of benefit.
It can also be difficult to identify the appropriate comparator for the gene therapy to be assessed against, particularly where the therapy leads to marked changes in clinical practice or where there is no existing treatment. In addition, for some therapies there will be no easily measured patient-centered outcome that can be used in short-term trials to evaluate effectiveness. Surrogate outcomes will therefore be used, some of which may need to be developed and validated with limited data.
Other distinctive features of gene therapies also increase uncertainty. Gene therapies use novel mechanisms to introduce the genetic material, raising questions about long-term safety that cannot be addressed with short-term trials. And, similarly, although gene therapies may appear to provide a ‘cure’, the durability of benefit may remain open to question. All these limitations on study design, outcome measures and ability to determine long-term benefits will mean that the evidence on gene therapies at launch will be notable for vulnerabilities to selection bias and other potential biases, reducing the certainty in estimates of efficacy and comparative effectiveness.
Safety evidence
As gene therapies are relatively new to medicine, there is little long-term experience with which to gauge the potential for serious safety consequences that might emerge years after the initial treatment phase. Although many of the pipeline gene therapies augment or supplement existing genes rather than editing germ line DNA sequences, gene therapies will arrive with their own set of safety concerns. For example, when delivered through viral mechanisms they can be tumorigenic and can give rise to proliferation in tissues that have not been intentionally targeted [12]. They can also stimulate immune reactions, requiring immunotherapy, adding to overall risks [13].
Assessing value
The challenges noted above around evidence generation and uncertainty make it difficult to produce the robust estimates of health and economic impact that are the core of any assessment of value.
Four additional types of questions arise in assessing the value of, and agreeing on a price for, a gene therapy:
Whether extra value should be attached to potentially curative therapies (compared with more incremental benefits)
Curative therapies may be valued more highly by society than treatments that offer the same ‘total’ health gains through marginal gains over many years and/or patients, as curative therapies have the potential to put an end to the need for long-term chronic treatments and provide longer term increases in quality of life. Early cures or substantial benefits at a young age could help produce significant gains in work productivity for patients compared with treatments that bring marginal gains over many years. Little evidence is available to suggest whether or not this preference does indeed exist, and no health technology assessment system currently includes such a weighting. Long-lasting treatment effects may, however, reduce ongoing costs of patient support and of managing chronic comorbidities, thereby offsetting high upfront costs [14]. Note that this ‘offsetting’ of future costs may appear less relevant in private insurance-based systems such as the USA where patients can move from one insurer to another.
Whether there are elements of value to patients, the health care system, or society, that are not captured in the usual payer value assessment
Payers typically focus primarily on health gain for the patient and net direct costs to the health system when looking at their willingness to pay for a therapy in particular circumstances. However, other elements of value may be considered relevant in general or in specific circumstances [15–17]. Additional elements or modifiers of value that have special relevance for gene therapy could include: disease severity, age of onset (there is evidence, for example, that society expects priority to be given to children), lifetime burden of illness, the potential to return to work or study, and reductions in burden of care for family members (‘informal’ care).
Whether small patient numbers mean that manufacturers must seek prices far beyond usual standards for cost-per-QALY thresholds or other similar decision rules in order to make an adequate return on investment
As with other ‘ultra-orphan’ treatments, manufacturers of gene therapies targeting very rare conditions face high per-patient development costs. In the case of gene therapies, there may be additional costs driven by the personalized nature of the medicines, which may mean that products cannot be prepared, tested and manufactured in bulk, and may involve higher costs for clinical delivery.
But it is not clear whether or not payers should therefore include consideration of R&D and manufacturing costs in their assessments of value and/or decisions on reimbursement in an implicit ‘cost plus’ approach. A similar debate has arisen in the context of orphan drugs more generally. Some argue that the same value assessment or willingness-to-pay criteria should be used, with no special considerations given for small patient numbers or the attributes of the technology. Others have noted that without high per-patient prices, and/or longer-term market exclusivity, these therapies may not be developed. Incentives to promote innovations sought by patients and society should be recognized as part of a problem requiring long-term solutions.
Affordability
More than any other challenge that may be presented by the emergence of gene therapies, that of affordability looms the largest in the minds of payers and policymakers. The health budgets of public insurers (Medicaid and Medicare), and payers in the private insurance system (employers, health plans), are already constrained, and pressures to control costs are expected to increase in future years. Estimates suggest that 25–30 million Americans (around 10%) have a rare condition related to a genetic defect [18]. Based on the initial pricing experience with gene therapy in Europe, should a growing number of gene therapies come into use at costs of US$1–2 million, the cumulative budget impact would be very substantial, and perhaps unsustainable. Even if gene therapies are developed to treat only one in ten patients with a genetic condition – approximately 1% of the total US population – the cumulative budget impact at that price could rise to US$3 trillion, as much as is currently spent in a year on all health care in the USA. Of course, a genetic therapy will not be found for every rare condition (although, conversely, some may not be for rare conditions, pushing up budget impact), prices may vary, and the rate at which successful gene therapies are likely to reach the market is such that these levels of budget impact would not be seen for many years, if at all.
In addition, some gene therapies may produce significant cost offsets by replacing expensive existing long-term treatments (such as enzyme replacement therapy), reducing hospitalizations and preventing further (potentially expensive) adverse clinical events. In order to assess the full financial impact, these long-term savings should be included in affordability considerations. But still, the general expectation that the health system will be confronted with the challenge of absorbing upfront treatment prices over US$1 million per patient for even a relatively small number of patients has raised significant concerns among payers and policymakers, even if cost savings will be realized over time in some cases. Manufacturers also recognize that existing payment mechanisms and other strategies to manage affordability may not be adequate to support the introduction of a growing number of gene therapies, highlighting the need for collaboration on further policy development to create a stable pricing, financing and health insurance structure for these technologies.
Possible solutions
Possible solutions to the evidence challenges
Use of early dialogue
The FDA provides opportunities for scientific dialogue and the provision of advice to help companies design trials that will address the FDA's concerns as a regulator. The benefits of early scientific dialogue that includes payers could be:
Ensuring that manufacturers take care to make the best use of the small available population, using appropriate trial designs (possibly including adaptive trial designs and cross-over studies) and methods of statistical analysis that are likely to maximize the usefulness of the evidence to payers and providers;
Discussion about whether surrogate end points are adequate for decision-making, and how surrogate end points can best be validated and evaluated;
Choice of comparator and understanding of current standards of care;
Consideration of follow-up periods for tracking patients and collecting and analyzing post-launch evidence on effectiveness and safety.
Attendees at the ICER Policy Summit meeting considered that early dialogue is typically an extremely useful exercise, but also noted that it is resource intensive and should only be carried out when there is value to be gained.
Sustained efforts to perform RCTs or adaptive trial designs
Whenever possible, manufacturers should seek ways to perform at least one RCT comparing the new therapy to best existing care, considering the use of adaptive trial designs, weighted randomization and cross-over to meet ethical requirements. In cases where RCTs are not possible, manufacturers should work with payers and regulators to establish the most appropriate feasible method of clinical evidence generation.
Collection of post-launch real-world evidence
Collection of real-world evidence via post launch registries tracking treated patients will usually be a safety requirement accompanying regulatory approval. It can also be used to mitigate the ‘leap of faith’ that short-term evidence of improvements in surrogate indicators is proof of long-term health benefits.
However, such observational level evidence is generally less well received by payers as it typically has greater risk of bias. Indeed, Hettle et al. comment that use of retrospective studies and historical control studies carry a risk of biased estimates of effect [11]. Potential partnership between payers and manufacturers, with agreement on the outcomes to be collected, might mitigate some of these concerns. The design of post-launch evidence collection is likely to be crucial for establishing medium-to-long-term evidence of effectiveness and comparative effectiveness.
Use of Centers of Excellence for diagnosis & treatment
The potential for problems with accurate diagnosis of patients, combined with uncertainty about whether the delivery of the treatment itself will reap the benefits seen in the trial data, may require centralization of diagnostic processes and follow up at Centers of Excellence. Centers of Excellence could also be used to manage provider payments in a way that eliminates payer concerns about large provider margins being added to therapy delivery costs. This option was viewed favorably by many attendees at the ICER Policy Summit meeting. For example, Spark Therapeutics is proposing to limit administration of voretigene neparvovec to Centers of Excellence that specialize in treating inherited retinal disorders that meet strict capabilities and training requirements to support appropriate patient care [19].
Possible solutions to the value assessment challenge
A shared value framework
A number of value frameworks have been proposed in the USA, combining descriptions of the elements of value with an algorithm for how they should be assessed and combined (for review see [20,21]). None of the frameworks have been developed to address the specific challenges that may arise in valuing a gene therapy. There is a case for stakeholders to: seek consensus on the elements of value relevant to gene therapy; identify relevant evidence for each of these; and consider how this information can be used in a decision-making process.
Understanding how budget impact will be assessed & addressed
Where budget impact is included in value frameworks or coverage decisions, it will be important to carefully consider the appropriate time horizon for these estimates. Typically payers consider 1–2 year time horizons, but this will not capture the true budget impact of many of these therapies where substantial savings are expected to be realized over the patient's lifetime. In order to accurately assess the budget impact, payers will need to consider these longer term benefits.
Once the potential net budget impact has been assessed there are various options that can be explored: (i) a direct adjustment to the calculation of value (as was proposed in a draft ICER value framework [16]); (ii) negotiations leading to discounts and revenue caps; (iii) exploration of alternative payment and funding arrangements. Options (ii) and (iii) are explored in more detail below.
Potential solutions to the affordability challenge
We have already noted that the affordability challenge is not unique to gene therapies. We look at methods that have been used or proposed to date, noting the strengths and weaknesses of each approach where appropriate.
Discounts & revenue caps
These have been used to control spending, for example, on high-cost hepatitis C virus (HCV) treatments around the world. They are designed to reduce the initial price or to set a total budget restriction or cap within the payers’ ability to pay. However, using this type of mechanism will send signals to industry about the extent to which health systems value (or do not value) gene therapies. If efforts to develop cures are not rewarded appropriately, researchers may choose to focus on incremental rather than breakthrough therapies. The choice of cap is also important. To date this has been rather ad hoc. Using the same caps across different therapy areas or types of treatment would send the signal that payers are indifferent between these, which may not be the case.
Targeting the highest value patient groups
One route long favored by payers is to prioritize and target expensive therapies at those patient groups who are most at risk and/or who get the most health gain. But it is important to note that, because the trials supporting registration for gene therapies may be smaller than typical development programs, it may be more difficult to perform meaningful subgroup analyses to assist in identifying, with any degree of certainty, these potential high-value groups.
Risk-sharing agreements & outcomes-based payments
Agreements can be developed that offer money-back guarantees if the expected outcomes are not achieved. This will still require payers to fund the upfront costs of the therapy. In the case of the HCV drugs, agreements were established in Spain and France such that health care payers would only pay for the HCV drugs for cured patients. Another approach would be to pay the manufacturer per unit of health delivered, for example, per year that a patient remains free of disease. Such agreements mean that the risk of non-performance is shared between the health care payer and the manufacturer.
The challenges of reaching and managing these agreements have been well documented [22,23]. The biggest obstacle is the difficulty and cost of collecting evidence on outcomes. This said, the regulatory requirement to track patients receiving gene therapy is likely to make this easier to organize. The second biggest obstacle is agreeing on contractual terms – what constitutes ‘success’ and ‘failure’ and what will be paid for or not paid for. Associated with this, there is the potential difficulty of withdrawing treatment from patients for whom the response may not justify the high cost, but for whom there may still be some beneficial effect. The inherent nature of a cure may make these issues easier to address, but careful delineation of how to measure success and how to handle “failure” will still be needed. Risk-sharing agreements and outcomes-based payments were generally perceived favorably by attendees at the ICER Policy Summit meeting.
Reinsurance
Reinsurance is where insurers seek insurance of their own to cover catastrophic pay-outs. Reinsurance could theoretically offer a short-term option for the first few gene therapies, but concerns were raised at the Policy Forum that commercial reinsurers may look to exclude such high-cost therapies. In addition, stakeholders believe that the reinsurance model will not work well over the long term given how quickly future risk will be priced into the premium.
Amortization
Amortization refers to some mechanism for paying for a large upfront cost by making a number of smaller payments over a period of time. Home mortgages are the most commonly known example, but stakeholders at the ICER Policy Summit objected to this comparison as being overly simplistic given the many differences between the choices involved in home ownership and those related to payment for a novel gene therapy (differences noted included the lack of choice for patients, no equity or ability to re-sell, and the fragmentation of insurance markets versus a single residential housing market – albeit with differentiated products). An example of an amortization mechanism in health care can be found in Spain, where the national government announced low-interest loans for regional payers to fund high-cost HCV therapies [24]. Gottlieb and Carino suggest that mechanisms such as these help to align the cost of the cure with its long-term economic benefits, thereby allowing payers to fund the treatments whilst balancing their budgets within a single year [25].
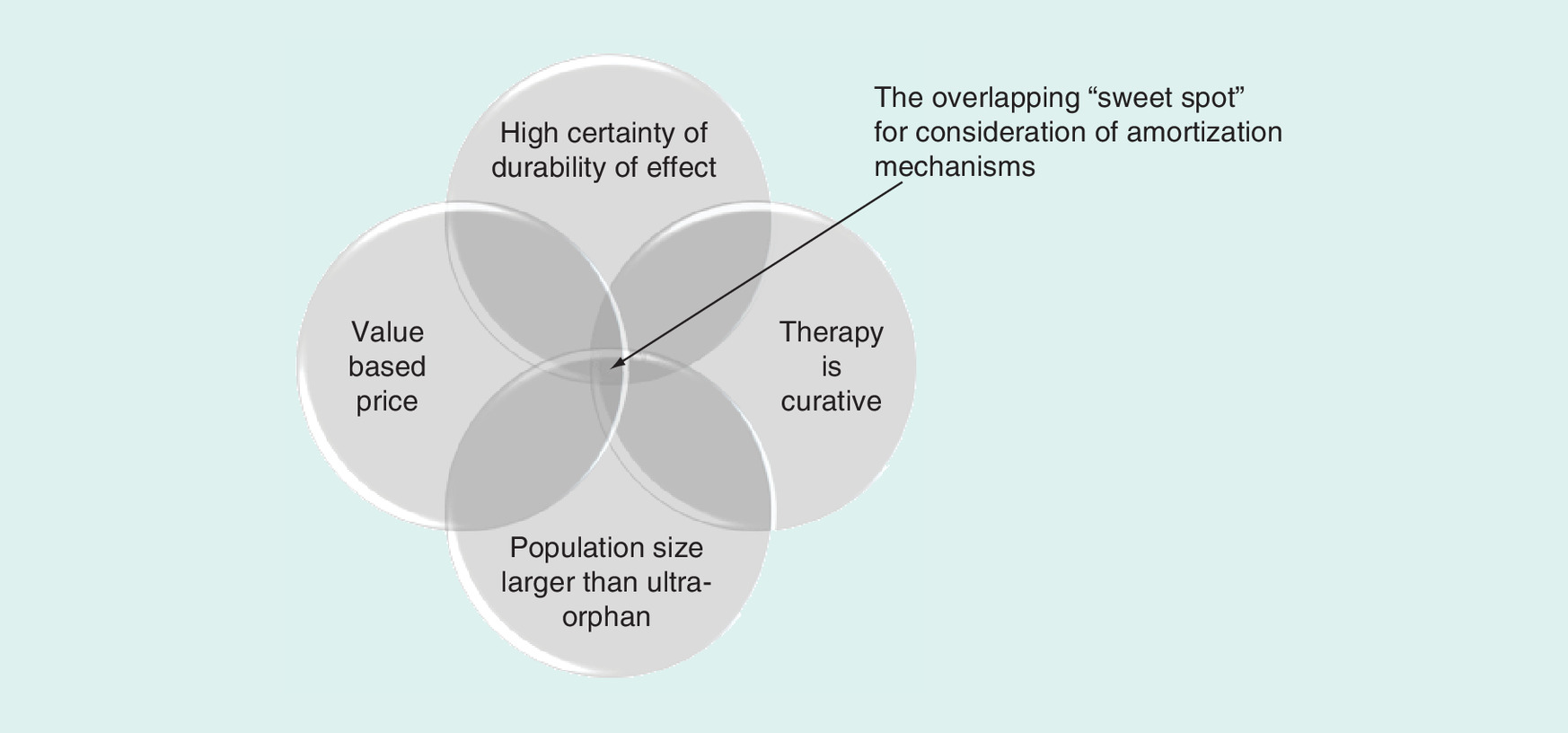
It is not currently clear whether some form of amortization will emerge as a viable option for managing the affordability of gene therapies. Some payers at the Summit expressed concerns that the introduction of any such arrangements would lead to higher prices and so threaten the future sustainability of the health care system. There do, however, appear to be certain characteristics that would make some gene therapies better candidates than others for consideration for an amortization approach. These characteristics include:
A one-time or very short-term treatment regimen with a ‘curative’ clinical impact, meaning that benefits accrue over a long period of time. In such circumstances, spreading costs over a longer duration means that these can be paid alongside the realization of benefits;
A durability of clinical benefit that is well established or that can be monitored through a linked outcomes-based mechanism. This means that data can be collected to facilitate an ongoing payment schedule. This is particularly important where amortization is used in combination with a outcomes-based payment approach;
A population size that is big enough to create concerns that upfront payment would not prove easily manageable. If this is not the case amortization may not be necessary;
A method by which the overall regimen price is fairly set to reflect the added value for patients and underlying development costs.
This set of circumstances is shown in Figure 1.
Options for the amortization of gene therapy payment
The options for amortization can be divided into categories dependent on who bears the financial risk and who provides the financing. The major categories are: (1) consumer loans to pay large upfront prices to manufacturers; (2) third-party financial institution financing for payers to obtain financing for large upfront prices to manufacturers; (3) government financing for payers to pay large upfront prices to manufacturers; and (4) manufacturer-managed financing, in which long-term payment plans are negotiated with payers and probably linked to outcomes-based agreements.
Each option is discussed in turn, and we summarize the thinking of the various mechanisms in Table 1.
| Outcomes-based agreements | Reinsurance | Consumer loan | Third-party financing | Manufacturer-managed financing | Government financing | |
|---|---|---|---|---|---|---|
| Features | Payment for results | Payer purchases reinsurance to reduce financial risk of having to pay extremely high costs for individual patients | Patient obtains a personal loan to enable upfront payment for the treatment outside of regular health insurance and repays the loan in periodic instalments Payments stop if the patient dies or the treatment fails | Payer receives a loan from a financial institution to enable upfront payment to the manufacturer, with loan repayment in periodic instalments Payments stop if the patient dies or the treatment fails | Manufacturer offers an instalment payment option allowing the payer to pay the cost of treatment in periodic instalments Payments stop if the patient dies or the treatment fails | Payer receives a loan from the government to enable upfront payment and repays the loan in annual instalments Payments stop if the patient dies or the treatment fails |
| Strengths | Addresses uncertainty about clinical benefits Can be combined with amortization methods | Relieves short-term budget pressure | Addresses uncertainty about clinical benefits Moves upfront payment to annual fee for performance | Addresses payer uncertainty about clinical benefits Moves upfront payment to annual fee for performance | Addresses payer uncertainty about clinical benefits Moves upfront payment to annual fee for performance | Addresses payer uncertainty about clinical benefits Moves upfront payment to annual fee for performance |
| Weaknesses | Difficulty of measuring outcomes Difficulty of agreeing criteria for ‘success’ | May be substantial premiums to pay Spreads the risk, but does not address long-term sustainability | Untested mechanism; Many people unable to afford payments Patient is taking on financing costs unless manufacturer offers a lower price | Untested mechanism; Need to address patient switch of health insurer Payer is taking on financing costs | Untested mechanism Needs to address patient switch of health insurer Negotiation of responsibility for financing costs | Untested mechanism Need to address patient switch of health insurer Payer is taking on financing costs |
Consumer loans
In this scenario patients are able to take out loans themselves to finance the cost of the therapy. Costs would be amortized over time, repayable with interest. Not all patients would be able to afford these treatments and so get access, even if loans were to be available. A US$1 million treatment could easily require payments of more than US$10,000 per month. Montazerhodjat et al. suggest that whilst patients taking on substantial debts in return for health care is not equitable, it is preferable to them not having access at all [26]. Still, attendees at the Summit viewed consumer mortgages as inconsistent with the basic understanding of the purpose of health insurance in the USA and therefore a poor option for amortizing payment.
Third-party amortization for payers
In some instances, amortization could be combined with a third party absorbing the risk. For example, Montazerhodjat et al. propose that hedge funds or other financial institutions are well placed to provide loans for high-cost therapies [26]. On the assumption that third parties bear the risk, they can build a risk related premium into the interest rate included in the repayment schedule. Such transactions are common in many industries outside of health care. This scenario would require the outstanding balance to move with the patient (i.e., it would need to become part of a patient's pre-existing condition), which would require a change to existing legislation (the pre-existing conditions clause in the Affordable Care Act) to extend to pre-existing financial ‘conditions’.
Amortization models were discussed in depth at the ICER Policy Summit meeting. Attendees noted the advantages described above, but also raised several concerns including: (i) that such models could have the unwanted effect of increasing prices; (ii) these models do not ‘solve’ the problem, but push it into the future (and possibly exacerbate it if (i) above pertains); (iii) they add another party who will take a cut (thereby increasing the total cost even further).
Manufacturer-managed financing
This is an approach to amortization in which payers (either private insurers or government) pay the manufacturer for the therapy over a number of years. This would continue until the agreed total price is paid, the payer defaults, or, if this approach is tied to an outcomes-based agreement, the benefit from the drug ends. By amortizing the payment over a number of years, the payment for a potential cure acquires the same financial profile as payment for ongoing treatment.
It is important to understand how the manufacturer absorbs the risk of the therapy not working or the patient dying before the agreed term of payments has been reached. The manufacturer can (i) loan the payer the money to pay up front for the drug and receive cash up front, with a pay back on the loan, as long as the drug works and the patient lives; (ii) assume risk but not get an upfront payment in full (matched by a loan) in a risk-sharing, outcomes-based agreement as discussed above; or (iii) see a third party taking on the risk by providing the payer with a loan, but almost certainly the premium interest rate demanded by the third party will be passed back to the manufacturer by the payer who will insist on a lower price for the therapy to offset these financing costs.
Government loans funded by bond issues
Interviewees commented that many patients who will receive gene therapies will be covered by Medicare or Medicaid (i.e., this is the ‘high-risk’ pool) so there will need to be a government response to gene therapies. One interviewee also commented that high-cost issues of life and death are political issues; they are unlikely to be handled sufficiently well by the private sector and are thus likely to become the responsibility of governments. Thus, there are two possible reasons for government to get involved – it is covering gene therapy for Medicare and Medicaid patients, and as a back-stop insurer to the population as a whole.
By issuing bonds for private payers to buy, Government could set repayment terms that took account of – for example – continued achievement of outcomes, the age of the patient (i.e., payments stopped if the patient became eligible for Medicare), or the numbers of patients being handled by a particular insurer, to reduce risk exposure.
Additional considerations
As noted, the Policy Summit discussion did not favor consumer loans, viewing them as being inadequate to provide fair and affordable patient access to these treatments. The focus thus fell upon financing by third parties, such as Wall Street financial institutions, the government or manufacturers. The risk and high costs of gene therapies may prove very difficult to manage within the fragmented private insurance system, and some stakeholders believe that the federal government will need to intervene and take over coverage, much as it did with renal dialysis. It was felt unlikely that Wall Street institutions will of their own volition come forward with a financing option for payers, and payers expressed limited interest in this option. It became clear through the discussion of the Policy Summit that if private insurers were going to consider some kind of payment through amortization, the proposal and the vehicle for doing so would have to come from the manufacturer. Some manufacturers might have the size and financial resources to provide the financing themselves, and offer the payer some form of instalment payment plan; others would most likely need to work with third parties to come up with some kind of financial instrument that they could then either offer to payers or would allow them to offer payers some form of instalment payment plan.
Final policy recommendations
Following discussion of this topic at the Policy Summit, the following policy recommendations reflect a combination of analysis and opinion of multiple stakeholders. For more background on each of the recommendations see Marsden et al. [9].
Recommendations for manufacturers
1. Seek dialogue with payers and regulators as early as possible in the development of new gene therapies in line with recent FDA guidance facilitating dialogue between sponsors and payers on investigational product information. Topics of discussion should include:
a. ways to include or create meaningful patient-centered outcomes or validated surrogate outcomes in developmental trials;
b. options for making the registration studies as robust as possible, especially if RCTs will not be performed;
c. options for partnership on post-approval studies to reduce residual uncertainty about the safety and effectiveness of new therapies (particularly important in the context of possible adaptive licensing);
d. methods of determining patient eligibility that can be feasibly translated into coverage criteria;
e. criteria for designation of potential Centers of Excellence for the delivery of the therapy;
f. size of potential patient population;
g. the role envisioned in therapy within the care pathway;
h. the elements of value that patients, clinicians, manufacturers and payers can agree should be considered in assessing value and judging what price would fairly reflect the added value of the therapy.
There appeared to be general agreement at the ICER Policy Summit meeting that payers, manufacturers and other key stakeholders all need to consider changes to current approaches if significant numbers of these therapies are to reach patients. For example, legislators need to understand the practical limits around evidence generation and create the right structure to promote innovation; manufacturers need to understand financial constraints faced by payers, and payers need to be willing to explore new approaches. The first pathways to coverage and adoption that are explored are unlikely to be perfect, but it is important that all parties are willing to explore new approaches. This will require stakeholders to engage in conversation.
2. Whenever possible, seek ways to perform at least one RCT comparing the new therapy to best existing treatment. Consider the use of adaptive trial designs, weighted randomization, and cross-over to meet ethical requirements. In cases where RCTs are not possible, work with payers and regulators to establish the most appropriate feasible method of clinical evidence generation.
Clearly, typical means of and standards for generating clinical evidence may be problematic for many gene therapies. Yet, evidence is still essential for licensing and reimbursement decisions. RCTs remain the gold standard, but in some cases, the FDA and manufacturers may need to consider alternative means. The pros and cons of new study designs and novel outcome measures to ensure robust evidence generation should be carefully considered by all stakeholders.
3. Work with clinicians, patient groups, regulators and payers to establish robust Patient Registries to facilitate collection of real-world evidence before and after regulatory approval.
Collection of real world evidence could be key to establishing the durability of effect and identifying any unintended consequences over time. Such post-launch data collection may also be useful for (or a requirement of) outcomes-based payments.
4. Be prepared to address concerns about high prices by presenting clear information and evidence on how the price is related to stakeholders’ perceptions of a therapy's value and/or represents a ‘fair’ rate of return given the costs of development, manufacture and administration of the therapy.
Payer representatives at the Policy Summit meeting raised questions about how much it costs to develop gene therapies, and what constitutes a ‘fair price’. They suggested that more transparency and visibility would help both sides to find mutual ground.
5. Where appropriate, collaborate with payers and health technology assessment groups on value assessment reports. Providing input on the scoping parameters of assessments is helpful, and special consideration should be given to sharing patient-level clinical and economic data when possible.
Little is known about the elements of value that stakeholders may agree are specifically relevant to gene therapies. For example, is there agreement that a ‘curative’ effect, or an outcome that halts the progression of a serious disease represents higher value? Should the burden on caregivers or on the disability system be formally considered? And should we be willing to pay higher prices to reward innovation, over and above the patient benefits delivered? Research and discussion is needed to identify the key elements of benefit associated with genetic therapies and the value society attaches to these.
6. For gene therapies whose characteristics make them good candidates for possible amortized payment options, be prepared to come to payers with specific manufacturer-financed mechanism for instalment payments combined with an outcomes- based agreement.
The manufacturer is the party wishing to sell the product, and may also be in the best position to fully understand the risks associated with the product and whether it is appropriate for them to bear the risk themselves, or whether to pass this to a third party, recognizing that if they take the latter approach the third party will require payment.
Recommendations for payers
1. Develop internal understanding of gene therapies, including understanding of the basic scientific techniques and of the usual approach taken by the FDA in assessing the safety and effectiveness of these agents.
Such internal knowledge generation will enable payers to have more productive interactions with stakeholders and contribute to the development of practical solutions.
2. Engage in early dialog with manufacturers of promising new gene therapies. The topics of mutual interest will include those listed above for manufacturers:
a. ways to include or create meaningful patient-centered outcomes or validated surrogate outcomes in developmental trials;
b. options for making the registration studies as robust as possible, especially if RCTs will not be performed;
c. methods of determining patient eligibility that can be feasibly translated into coverage criteria;
d. criteria for designation of potential Centers of Excellence for the delivery of the therapy;
e. size of potential patient population;
f. the role envisioned in therapy within the care pathway;
g. the elements of value that patients, clinicians, manufacturers and payers can agree should be considered in assessing value and judging what price fairly reflects the added value of the therapy.
Early dialogue involving payers as well as regulators allows manufacturers to ensure that they are developing the treatments in line with reimbursement (as well as regulatory) decision requirements. It also gives payers a chance to better understand the new therapies. Finally, early dialogue also provides the FDA and payers with an opportunity to input into the way a treatment is developed.
3. Work with clinicians, patient groups, regulators and manufacturers to establish robust Patient Registries to facilitate collection of real-world evidence following regulatory approval. Individual insurer in-house registries could be pooled with those of other insurers and/or with manufacturers.
Payers will have an interest in collecting real-world evidence to help determine the long-term effectiveness of gene therapies. Registries devoted to evidence collection and monitoring could be an efficient way to approach this. Such post-launch data collection may also be useful for (or a requirement of) outcomes-based payments.
4. Develop categorizations of different types of gene therapies based on their method of delivery, mechanism of action and other key characteristics so that coverage policies can be clearly tailored to meet distinctive therapies.
A key theme that arose from the meeting was this idea of categorizing (or ‘bucketing’) gene therapies. Attendees noted that not all gene therapies are the same, for example: some types use gene augmentation, which boosts production or adds in a functional copy of a gene, whilst others alter the patient's genetic makeup by editing out a genetic mutation; some gene therapies will be curative, but not all of them will be. Some system of categorization that enables a balance between allowing for the differences between gene therapies, whilst grouping them to a level that enables practical steps to be taken for each group, would be useful.
Stakeholders should also be aware that the nature of gene therapies may change over time – the gene therapies we see in the next 5 years are likely to be different from those we see in 10 years. We need to consider that some categories may emerge before others and we may need to think about different solutions over different timelines.
5. Work with plan sponsors to familiarize them with the challenges in this area and to explore options for coverage that will meet their needs for value and affordability while creating a mechanism to help patients gain access to effective new therapies.
Due to the rarity of the diseases affected and the highly specialized nature of the treatments, plan sponsors will look to health plans and pharmacy benefit managers to educate them on gene therapies, guidance in assessing their value, and recommendations on appropriate criteria for coverage policies.
6. Collaborate with manufacturers to explore outcomes-based agreements. Outcomes-based agreements can be combined with different potential methods of amortized payments when health benefits are expected over a long time horizon.
There was broad agreement at the meeting that outcomes-based payments and risk sharing mechanisms that reward effective treatment represent a sensible way forward. However, these types of arrangements are dependent on the feasibility of collecting data on the long-term effect of the treatment. Outcomes-based payments help to increase the overall value of the treatment to payers by reducing costs for those cases where the treatment is not effective. The manufacturer also benefits since they are able to use the outcomes data generated to demonstrate greater effectiveness amongst those who do benefit from the therapy in the long term.
Conclusion
The policy recommendations above are designed to be specific and actionable. They should be used to build upon ongoing dialogue between manufacturers and payers about the challenges of gene therapies and the possible solutions. Once stakeholders are communicating effectively, the recommendations above can be used to develop pilot programs and overcome some of the inevitable inertia in the system. Useful topics to cover as part of these broader conversations include categorization of gene therapies into different groups; elements of value that are specifically relevant for gene therapies and how these can be combined within a value framework; types of evidence generation; approaches to outcomes-based and risk-sharing agreements; and approaches to amortization the first approaches that are explored are unlikely to be perfect, but will still represent progress. Gene therapies will arrive imminently, and it is time to prepare a clear roadmap for evidence generation, assessment, pricing and payment, that will allow current and future patients to benefit from these innovations within an affordable, sustainable framework.
Classification
The US FDA refers to gene therapies as human gene therapy products. They are often considered alongside cell therapies, collectively referred to as “Cellular & Gene Therapy Products”.
Pathway
The Office of Tissue and Advanced Therapies (OTAT), part of the Center for Biologics Evaluation and Research (CBER), regulates gene therapies alongside cell therapy products and related devices. CBER provides management and support to the Cellular, Tissue and Gene Therapies Advisory Committee, who review and evaluate data relating to the safety, effectiveness, and appropriate use of these products.
The regulatory approach for gene therapies is similar to other medical products, but does include flexibility related to the biological and technical complexity of the products. For example, Phase I studies for gene therapies are typically conducted in a population who has the disease being studied (rather than in healthy volunteers). This is mainly due to unknown risks, but also allows sponsors to look for preliminary evidence of bioactivity on the characteristics of the disease.
Gene therapies may also be able to achieve orphan status (which qualifies manufacturers for benefits such as tax credits) and/or be eligible for one of the four available mechanisms for expediting FDA assessment: breakthrough designation, fast-track designation, accelerated approval or priority review. Some gene therapies have already qualified for these mechanisms, for example EB-101 for recessive dystrophic epidermolysis bullosa (Abeona Therapeutics) and AMT-060 for hemophilia B (UniQure), which have both received FDA breakthrough designation.
CBER is also able to provide early scientific and regulatory advice.
Introduction
Gene therapy is coming to the US health care system; the first gene therapy is likely to receive regulatory approval in early 2018.
Some gene therapies offer the potential for short ‘one-off’ treatments leading to lifelong benefits, and could positively affect millions of lives.
However, the distinctive nature of gene therapies presents many challenges that must be addressed in order to assure affordable patient access.
This paper explores the challenges presented by gene therapies, discusses potential solutions, and presents policy recommendations.
Methods
Targeted literature reviews and interviews with policy experts were used to identify a list of potential challenges that could arise around the adoption of gene therapies, as well as possible solutions.
These challenges and potential solutions were the subject of discussion at the 2016 Institute for Clinical and Economic Review Policy Summit meeting that brought together experts and leaders from the innovator and payer communities.
Policy recommendations have been developed following the key thoughts and suggestions emerging from the meeting.
Challenges
We identified three key categories of challenges: evidence generation; assessing value; and affordability.
Evidence generation: conducting randomized controlled trials (RCTs) can be problematic due to small population sizes, invasive methods of administration, and a lack of clearly defined existing management approaches for comparison. RCTs that do take place often have short follow up and are based on surrogate outcomes. The long-term effectiveness and safety implications of these emerging therapies are not yet known.
Assessing value: significant uncertainty around estimates of effect makes it difficult to produce robust estimates of health and economic impact. In addition, there is no consensus on whether extra value should be attached to potentially curative therapies (compared with incremental benefits), or whether there are other elements of value specific to gene therapies that are not captured in the usual payer assessments of value.
Affordability: the budget impact of gene therapies is expected to be substantial, raising concerns about affordability and price, and stimulating discussion of possible new mechanisms for managing the costs of curative gene therapy to avoid pushing the US health care system to breaking point.
Possible solutions
Possible solutions are presented for each of the three main categories of challenges:
Evidence generation: early dialogue between the FDA, payers and manufacturers could help manufacturers make the best use of small populations, develop mutually agreed trial designs, and collect relevant outcomes. Collection of post-launch evidence is likely to be crucial for establishing longer term evidence of effectiveness and safety.
Assessing value: a shared value framework would align stakeholders’ views on value. Where budget impact is included in value assessments, it will be important to consider longer time horizons than the period of 1–2 years typically used to adequately capture future benefits and cost offsets.
Affordability: discounts, revenue caps and targeting of patient groups most likely to benefit have been used to control spending on curative treatments to date, but such mechanisms may be harder to justify for some types of gene therapy and risk sending signals that these therapies are not valued.
Risk-sharing agreements could be developed that offer money-back guarantees if the expected outcomes are not achieved.
Risk sharing could be combined with amortization schedules, whereby the upfront cost of the treatment is spread over an extended time frame. We discuss various approaches to amortization of payment for gene therapies: third-party involvement, manufacturer-managed financing, consumer mortgages and government loans.
Recommendations
Manufacturers should: seek dialogue with payers and regulators as early as possible in the development of new gene therapies; seek ways to perform at least one RCT using accepted clinical and patient-centered outcome measures; facilitate collection of real-world evidence; collaborate with payers on value assessment reports; and be prepared to come to payers with proposals for outcomes-based payments, where appropriate combined with manufacturer-financed amortization mechanisms.
Payers should: develop awareness of emerging gene therapies and the issues they raise; engage in early dialog with manufacturers; facilitate collection of real-world evidence; develop categorizations of different types of gene therapies; collaborate with manufacturers to explore outcomes-based agreements; be prepared to respond to proposals for the amortization of payments.
Conclusion
Gene therapies represent an exciting opportunity, but also pose major challenges. The recommendations presented here have been designed to be specific and actionable.
They should be used to inform ongoing dialogue between manufacturers and payers about the challenges of gene therapies and the possible solutions. The first pathways for adoption that are developed are unlikely to be perfect, but will still represent progress and opportunities for improved approaches in the future.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Financial & competing interests disclosure
Funding for the Institute for Clinical and Economic Review (ICER) Policy Summit comes from membership dues contributed by participating organizations representing a broad set of insurers, pharmacy benefit managers, and drug manufacturers. The Office of Health Economics (OHE) received funding from ICER for providing scientific content for the meeting. OHE, a registered charity, receives funding from a variety of sources, including the Association of the British Pharmaceutical Industry. CH is an independent consultant who received funding from ICER for his contributions to the Policy Summit and this paper, and who receives funding from various life sciences companies for work and advice relating to health technology assessment. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_table.docx)
- Download
- 28.45 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
American Medical Association. Gene Therapy. http://www.ama-assn.org/ama/pub/physician-resources/medical-science/genetics-molecular-medicine/current-topics/gene-therapy
2.
Genetics Home Reference. How does gene therapy work? https://ghr.nlm.nih.gov/primer/therapy/procedures
3.
MedlinePlus. Genes and Gene Therapy. https://medlineplus.gov/genesandgenetherapy.html
4.
Ylä-Herttuala S. Glybera's second act: the curtain rises on the high cost of therapy. Mol. Ther. 23(2), 217–218 (2015).
5.
uniQure. uniQure announces it will not seek marketing authorization renewal for Glybera in Europe. http://uniqure.com/GL_PR_Glybera%20withdrawal_FINAL_PDF.pdf
6.
Boliter N. Gene therapies in a bottle – pharma just needs to rub the right way. Pharma intelligence, Informa. September (2016). https://citeline.com/wp-content/uploads/Whitepaper-Report-Gene-Therapy_LR.pdf
7.
Thomas DW, Craighead JL, Economides C, Rosenthal J. Clinical development success rates for investigational drugs. Nat. Biotech. 32(1), 40–51 (2014).
8.
Spark Therapeutics. Spark Therapeutics Completes Rolling Biologics License Application Submission to FDA for Investigational Gene Therapy Voretigene Neparvovec. http://ir.sparktx.com/phoenix.zhtml?c=253900&p=irol-newsArticle&ID=2273905
9.
Marsden G, Towse A, Pearson S, Dreitlein B, Henshall C. Gene therapy: understanding the science, assessing the evidence, and paying for value: a report from the 2016 ICER Membership Policy Summit. Office of Health Economics, London, UK (2017).
•• Full description of the Institute for Clinical and Economic Review Policy Summit on Gene Therapy with greater detail on the challenges around evidence generation, value assessment and affordability, and recommendations for both payers and pharmaceutical manufacturers.
10.
Bubela T, McCabe C, Archibald P et al. Bringing regenerative medicines to the clinic: the future for regulation and reimbursement. Regen. Med. 10(7), 897–911 (2015).
11.
Hettle R, Corbett M, Hinde S et al. Exploring the assessment and appraisal of regenerative medicines and cell therapy products. CRD/CHE University of York, York, UK (2016).
•• Provides a review of previous evaluations of regenerative medicines in the UK, discussions around the use of different types of evidence of informing decision making, and a mock health technology assessment appraisal of chimeric antigen receptor T-cell therapy.
12.
van Schothorst M, Weeda J, Schiffers K et al. Study on the regulation of advanced therapies in selected jurisdictions. European Commission (2014).
13.
Abou-El-Enein M, Bsanhoury A, Reinke P. Overcoming challenges facing advanced therapies in the EU market. Cell Stem Cell 19, 292–297 (2016).
14.
Abou-El-Enein M, Bauer G, Medcalf N, Volk H, Reinke P. Putting a price tag on novel autologous cellular therapies. Cytotherapy 18, 1056–1061 (2016).
15.
Towse A, Barnsley P. Approaches to identifying, measuring and aggregating elements of value. Int. J. Technol. Assess. Health Care 29(4), 360–364 (2013).
16.
The Institute for Clinical and Economic Review. ICER Value Assessment Framework 1.0 to 2.0. http://icer-review.org/wp-content/uploads/2016/02/Value-Assessment-Framework-slides-for-July-29-webinar-FINAL-corrected-8--22--1.pdf
17.
Oortwijn W, Sampietro-Colom L, Habens F. Developments in value frameworks to inform the allocation of healthcare resources. Int. J. Technol. Assess. Health Care 33(2), 323–329 (2017).
18.
Genetic and Rare Diseases Information Center (GARD). FAQs about rare diseases. https://rarediseases.info.nih.gov/diseases/pages/31/faqs-about-rare-diseases
19.
Spark Therapeutics. 2016 annual report. http://phx.corporate-ir.net/External.File?item=UGFyZW50SUQ9NjY3MTY4fENoaWxkSUQ9Mzc1MDA1fFR5cGU9MQ==&t=1
20.
Neumann P, Cohen J. Measuring the value of prescription drugs. N. Engl. J. Med. 373, 2595–2597 (2015).
21.
Westrich K. Current landscape: value assessment frameworks. National Pharmaceutical Council, Washington, DC, USA (2016).
22.
Garrison LP, Carlson J, Bajaj P et al. Private sector risk-sharing agreements in the United States: trends, barriers, and prospects. Am. J. Manag. Care 21(9), 632–640 (2015).
23.
Garrison LP, Towse A, Briggs A et al. Performance-based risk-sharing – good practices for design, implementation, and evaluation: report of the ISPOR Good Practices for Performance-based Risk-Sharing Task Force. Value Health 16(5), 703–719 (2015).
• Describes different types of performance-based risk sharing arrangements and outlines principles of good practice.
24.
APM Health Europe. Prices of new hepatitis C combinations lower than monotherapy in Spain in six months. www.apmhealtheurope.com/Prices-of-new-hepatitis-C-combinations-lower-than-monotherapy-in-Spain-in-six-months-FS_41696.html
25.
Gottlieb S, Carino T. Establishing new payment provisions for the high cost of curing disease. AEI Research (2014). www.aei.org/wp-content/uploads/2014/07/-establishing-new-payment-provisions-for-the-high-cost-of-curing-disease_154058134931.pdf
• Explores credit and contracting arrangements for amortizing the cost of therapies over a number of years to provide new funding options for high-cost therapies.
26.
Montazerhodjat V, Weinstock D, Lo A. Buying cures versus renting health: financing health care with consumer loan. Sci. Transl. Med. 8(327), 327ps6 (2016).
• Discusses health care loans as a means to improve affordability for large health care expenses, whilst maintaining incentives for manufactures to develop innovative therapies.
27.
US FDA. www.fda.gov
28.
Bailey AM, Arcidiacono J, Benton KA, Taraporewala Z, Winitsky S. United States Food and Drug Administration regulation of gene and cell therapies. Adv. Exp. Med. Biol. 871, 1–29 (2015).
Information & Authors
Information
Published In
Copyright
© 2017 Institute for Clinical and Economic Review.
History
Received: 30 August 2017
Accepted: 11 October 2017
Published online: 16 November 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Gene therapy: evidence, value and affordability in the US health care system. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0068
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Julian Savulescu, Sebastian Porsdam Mann, Christopher Gyngell, G. Owen Schaefer, Ethics of gene therapy, Med, 10.1016/j.medj.2026.101225, (101225), (2026).
- Sumaya Abuloha, Amie Goodin, Tianze Jiao, Manuela Corti, Mikael Svensson, Modeling the Budget Impact of Disease-Modifying Therapies in Infantile-Onset Spinal Muscular Atrophy, Clinical Drug Investigation, 10.1007/s40261-026-01571-x, 46, 8, (883-896), (2026).
- Walter Van Dyck, Sissel Michelsen, David Veredas, Isabelle Huys, Jeroen Luyten, Steven Simoens, When Do Annuity-Based Payments Help to Address the Affordability Challenge of Funding Advanced Therapies? Insights from a Budget Impact Simulation, Journal of Market Access & Health Policy, 10.3390/jmahp14020023, 14, 2, (23), (2026).
- Yi Han, Mattia Andreoletti, Timo Minssen, Effy Vayena, Kelly E. Ormond, The impacts of pricing and reimbursement policies on access to cell and gene therapies across Europe, Journal of Community Genetics, 10.1007/s12687-026-00860-4, 17, 1, (2026).
- Sk Ashif Jan, Abhijit Debnath, Rajesh Kumar Singh, Pankaj Kumar Tyagi, Sachin Singh, Anil Kumar Singh, Targeting Undruggable Proteins: The siRNA Revolution Beyond Small Molecules - Advances, Challenges, and Future Prospects in Therapeutic Innovation, Current Gene Therapy, 10.2174/0115665232357160250123113148, 26, 1, (116-135), (2026).
- Nermina Ferizović, Caroline S. Clarke, Rachael M. Hunter, Ruth Plackett, Nicholas Freemantle, Value attributes of advanced therapy medicinal products: a comprehensive literature review, Discover Medicine, 10.1007/s44337-025-00376-9, 2, 1, (2025).
- Harshini Hariram, Sean P. Gavan, Constraints on delivering cell and gene therapies identified during technology appraisal by the National Institute for Health and Care Excellence, International Journal of Technology Assessment in Health Care, 10.1017/S0266462325100391, 41, 1, (2025).
- L. Evert, T. Potupchik, O. Veselova, I. Svetlakova, B. Panchenko, R. Kudasheva, A. Melnikova, Genome editing in neurodegenerative diseases: risk analysis, technological challenges, and prospects for clinical application, Molekulyarnaya Meditsina (Molecular medicine), 10.29296/24999490-2025-02-03, (21-31), (2025).
- Simona Cosma, Stefano Cosma, Daniela Pennetta, Giuseppe Rimo, Overcoming the “valleys of death” in advanced therapies: The role of finance, Social Science & Medicine, 10.1016/j.socscimed.2024.117639, 366, (117639), (2025).
- Nadezhda A. Pechnikova, Malamati Poimenidou, Ioannis Iliadis, Maria Zafeiriou-Chatziefraimidou, Aleksandra V. Iaremenko, Tamara V. Yaremenko, Kalliopi Domvri, Alexey V. Yaremenko, Pre-Clinical and Clinical Advances in Gene Therapy of X-Linked Retinitis Pigmentosa: Hope on the Horizon, Journal of Clinical Medicine, 10.3390/jcm14030898, 14, 3, (898), (2025).
- See more