Economic and organizational impact of the changing hospital funding practices of erythropoiesis-stimulating agents on the management of care of dialysis patients in France
Abstract
Aim: Erythropoiesis-stimulating agents (ESAs) are particularly used to treat dialysis patients suffering from anemia due to renal failure. Since March 2014, ESAs have no longer been funded on top-of-diagnosis-related groups (DRGs) in French hospitals and are funded via DRGs. There are two ways to fund dialysis in French hospitals: the ‘DRG for dialysis in session’ and the ‘off-dialysis DRG’, which is not a DRG and consists in a supplement tariff specific to dialysis for patients hospitalized for another main reason than dialysis. The aim of this study is to assess the impact of this funding change on the dialysis activity and on the budget of the 37 University Public University Hospitals in Paris (10% of the hospitalizations in France). Materials & methods: A before–after study (March–September 2013 vs March–September 2014) was conducted. Medical activity data (and ESAs consumption data) were used to assess the number and costs of DRGs associated with ESAs use. As we do not have access to the whole dialysis activity over the period studied, two hypotheses were considered: the proportion of the dialysis activity was constant between the two periods (Hypothesis A); the dialysis activity was correlated to ESA consumptions delivered by hospital pharmacies to healthcare units (Hypothesis B). A budget impact analysis was also conducted taking into account the evolution of DRG costs and ESA prices. Results: The number of dialysis ‘DRG for dialysis in session’ with ESA consumption have increased by 5% (Hypothesis A) and decreased by 9% (Hypothesis B) between the two periods while the volume of ‘off-dialysis DRG’ with ESA consumption increased by 2% (Hypothesis A) and by 9% (Hypothesis B). The budget impact was -€1.02 million (Hypothesis A) and -€0.7 million (Hypothesis B) leading to a loss for our hospitals. Conclusion: There is no significant impact of the change of funding of ESAs on the hospital activity. The DRG-based payment is negative for the budget of our hospitals but is positive for the French National Health Insurance. Indeed, with the price decrease, the ESAs are more costly for hospitals (not funded on top-of-DRG), but less costly for the society.
French hospitals are funded by the activity-based payment, a prospective payment based on each hospital's casemix evaluated through diagnosis-related groups (DRGs). The National Health Insurance (NHI) reimburses a fixed amount for each DRG. These tariffs cover both medical and pharmacy costs, including drugs [1]. Nevertheless, an additional payment is available for high costs and innovative drugs; on presentation of bills, hospitals receive funding from the NHI for expensive drugs on the list developed at the national level by the French Ministry of Health (115 drugs in December 2014), commonly referred to as the ‘top-of-DRG list’ [2]. It is limited and subjected to regular updates (listing and delisting). The purpose is to ensure access to innovative drugs without creating significant heterogeneity in the cost per stay. The financial traceability of products on the list is mandatory for billing. The criteria defined by the authorities for the listing and the delisting include the expected use of the drug, the medical benefit and its improvement, the frequency and costs of the drug in hospital stays and the equal treatment of comparable products [2]. All public and privately managed hospitals providing services in the area of medicine, surgery or obstetrics (MSO) in France are eligible for this supplementary financing. The NHI reimburses for medications on the out-of-DRG list up to a price agreed upon by the French Healthcare Products Pricing Committee and the pharmaceutical companies, named ‘responsibility tariff’ (RT). The French Government does not regulate the purchasing price of drugs in hospitals; it is up to hospitals to negotiate with the pharmaceutical companies a price that is within the reimbursement price cap. Moreover, as an incentive from the NHI, if the purchase price is less than the RT, hospitals shall receive half of the difference between the actual purchase price and the RT, an amount referred to as profit margin (PM). Besides, hospitals have to respect an agreement of ‘appropriate use of healthcare’ with the NHI in order for their services to be fully reimbursed.
Hospitalizations for inpatient or daycare within MSO hospitals are billed on a DRG while hospitalizations for outpatient are billed as a ‘medical procedure’ or as a ‘consultation’. Otherwise, some medical activities (dialysis, abortion, palliative care, etc.) are funded as add-on payment on top-of-DRG, called supplements. Dialysis can be funded in two ways in French hospitals (Figure 1): in a DRG ‘for dialysis in sessions’ when a patient is hospitalized only for dialysis (daycare); in an ‘off-dialysis DRG’ with a dialysis supplement tariff when a patient is hospitalized for another main reason than dialysis but when a dialysis occur during the stay. Tariffs of dialysis supplements are the same as DRG tariff for dialysis in sessions for each type of dialysis [3,4]. Erythropoiesis-stimulating agents (ESAs) were on the top-of-DRG list until March 2014, when the Minister of Health delisted them, considering their low purchasing prices by hospitals and that they no longer correspond to innovative products [5,6]. Since then, the amount of ESAs has been integrated in DRG, with a slight increase of DRG for dialysis in sessions only (particularly the DRG hemodialysis in sessions, +4.7% for adults, +2.4% for children and the DRG ‘renal failure with dialysis, as outpatient’, +1.6%). However, this slight increase does not cover entirely the price of ESA. Considering that ESAs are available both in hospital pharmacies and in community pharmacies and that all medical personnel are aware of the delisting, physicians may be less likely to prescribe ESAs during hospitalizations or hospitals could make patients purchase ESAs in community pharmacies in order to limit their budget impact (BI) following the delisting decision. Then ESAs would no longer be administered during dialysis. This raised many concerns related to the fact that a decrease of quality and equity of hospital care could occur due to the potential BI especially for severe patients. This is a main stake for the Public University Hospitals in Paris – the largest public hospital group across Europe – given that, as a university-affiliated hospital center, its mission is to ensure the care of patients for severe dialysis patients [7].
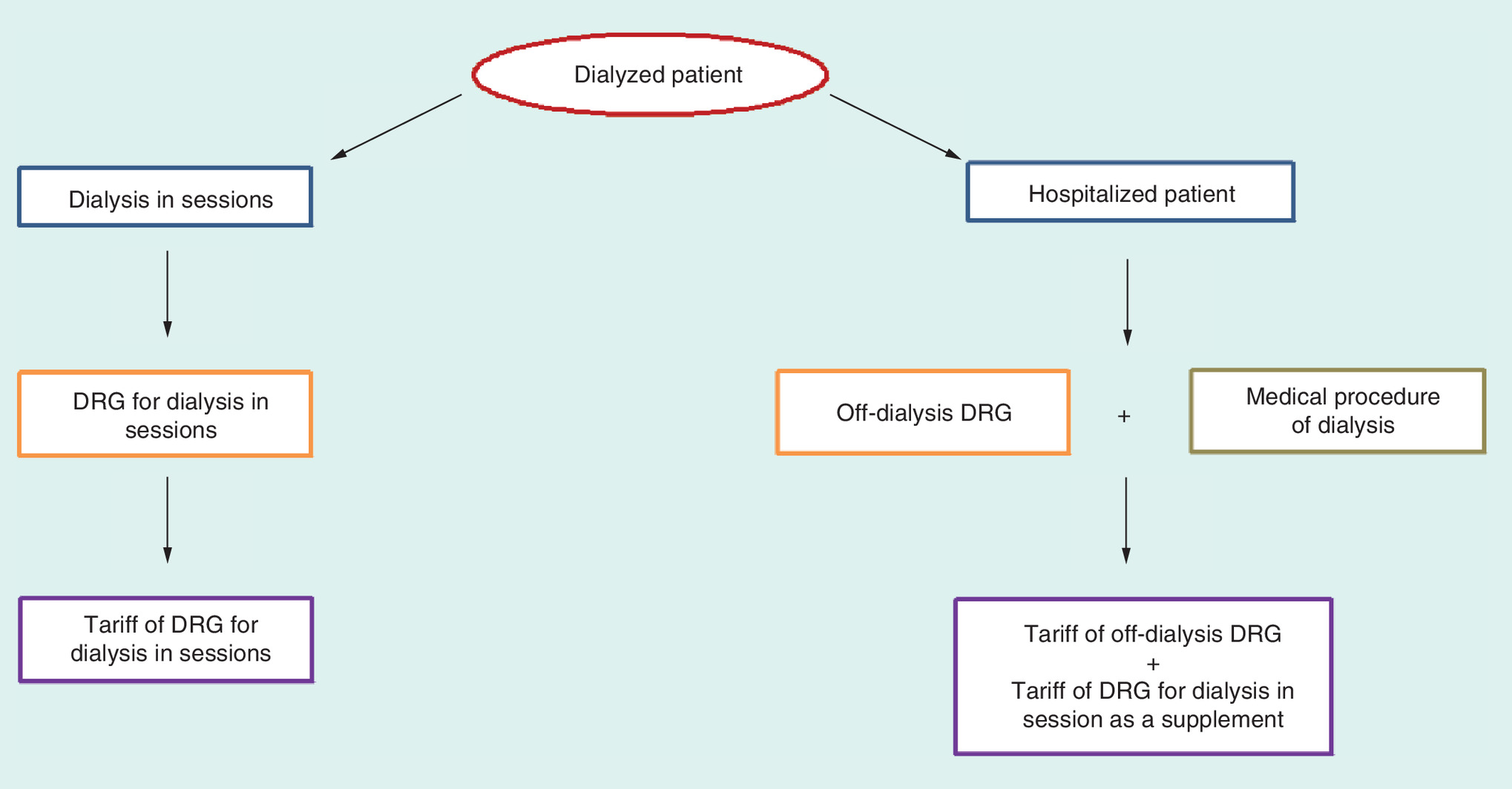
Figure 1. Modalities for the financing of dialysis in hospitals.
Dialysis can be funded in two ways: in a DRG ‘dialysis in sessions’ when a patient is hospitalized only for dialysis (daycare) or in an ‘off-dialysis DRG’ with a dialysis supplement tariff when a patient is hospitalized for another main reason than dialysis but when a dialysis occurs during the hospital stay. Tariffs of dialysis supplements are the same as DRG tariff for ‘dialysis in sessions’ for each type of dialysis.
DRG: Diagnostic-related group.
The aim of this study was to assess the impact of this funding change on the dialysis activity (evaluation of the shift of ESA prescribing for dialysis patients from inpatient to outpatient) and on the budget of the 37 Public University Hospitals in Paris.
Materials & methods
A before–after study was conducted in public hospitals of Paris (Assistance Publique-Hôpitaux de Paris [AP-HP]) MSO hospitals from March to September 2013 versus the same period in 2014. We compared the consumptions of ESAs, the number of hospital stays during which ESAs were given and the costs for both (Figure 2).
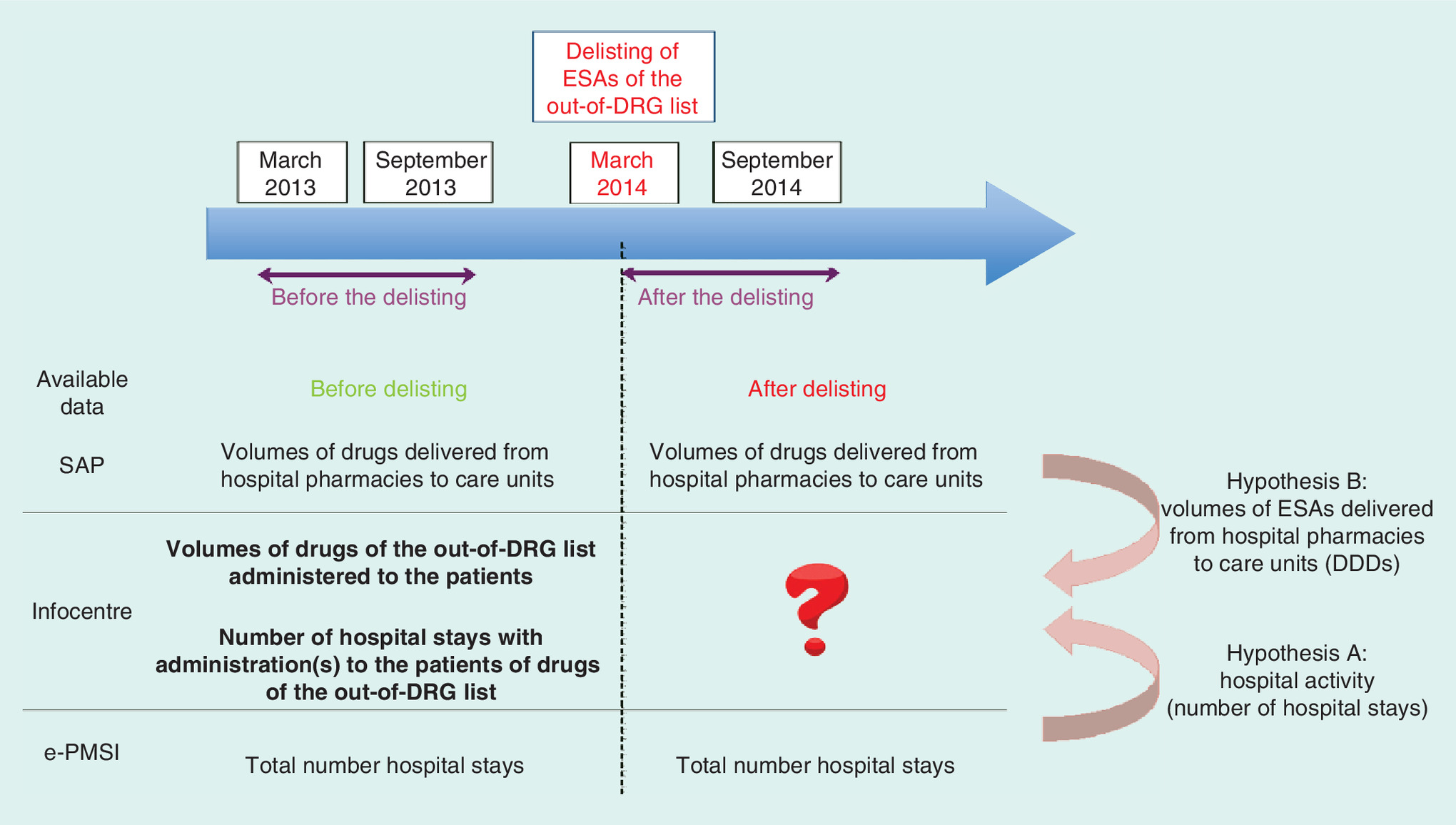
Figure 2. Hypothesis to estimate the number of hospital stays with administration of erythropoiesis-stimulating agents in 2014.
The delisting of ESAs from the out-of-DRG list occurred in March 2014. The impacts of the delisting of ESAs from the out-of-DRG list in the public hospitals of Paris (AP-HP) were assessed by a before–after study from March to September in 2013 (before the delisting) and in 2014 (after the delisting). As there were no longer data on ESAs’ uses after the delisting occurred, two hypotheses were used to calculate an estimation of the data for 2014. SAP enables knowing the volumes of a drug delivered from hospital pharmacies to care units. Infocentre (AP-HP database) mainly contains hospital activity and data on the administration of out-of-DRG drugs as coded data. e-PMSI (database available on the internet) gives a feedback on French hospitals activity, included DRGs produced in each hospital.
Hypothesis A: the repartition of the hospital activity is constant, in other words, the proportion of stays during which ESAs were administered is the same in 2013 and in 2014. The number of stays with ESAs in 2014 was calculated from 2013 data in proportion to the total number of stays in 2014 filled in the e-PMSI.
Hypothesis B: the number of hospital stays during which ESAs are administered is linked with consumptions of ESAs by care units; the number of stays during which ESAs were administered in 2014 was calculated in proportion to quantities of ESAs transferred by each hospital pharmacy to each care unit (dialysis care units and off-dialysis care units and adults and children were separated).
AP-HP: Public hospitals of Paris (Assistance Publique-Hôpitaux de Paris); DRG: Diagnostic-related group; ESA: Erythropoiesis-stimulating agent; SAP: Financial and logistics software shared between all AP-HP care facilities.
Time horizon
The study was conducted over the same months before and after the delisting in order to ensure greater uniformity of hospital activity. At the beginning of the study, the data were available up to and including September 2014. This is the reason why the study compared data from March to September in 2013 and in 2014.
Data
In order to receive reimbursement for their hospital stays and drugs expenditures, hospitals report monthly to the French Health Authorities the information about hospital stays and usage of drugs on the top-of-DRG list, as coded data, including the ‘Anonymous summary file’ (RSA: Résumé de sortie anonymisé – in French) containing descriptive data about hospital stays and data on the administration of top-of-DRG drugs. The French Technical Agency of Information on Hospitals collects this information and implements a database available on the internet through the program for the medicalization of information systems platform (e-PMSI) which gives a feedback on French hospitals activity, included DRGs produced in each hospital [8].
These data were no longer available after the delisting of ESAs. This is the reason why two databases were created using data gathered from two administrative and medical databases which are available for the General Agency of Equipments and Health Products of AP-HP (the central drug purchasing structure also responsible for implementing a scientific and pharmacoeconomic evaluation of medicines, and for referencing them in the AP-HP's formulary or not).
Database 1 was created gathering SAP (Engineered Resource Planner) software data. SAP is a financial and logistics software shared between all AP-HP care facilities. It enables knowing the volumes of a drug delivered from hospital pharmacies to care units. Database 1 associated each transfer of ESAs from hospital pharmacies to care units with the name of the hospital, the medical discipline of the care unit, the quantities of ESAs in DDDs (defined daily doses, defined by the WHO), the month and the year.
Database 2 was created gathering data from Infocenter. Infocenter is an AP-HP database, which mainly contains hospital activity and data on the administration of top-of-DRG drugs as coded data. Database 2 associated each ESA administered from March to September 2013 with the data about the drug (hospital, volume administered in DDDs, month and year, therapeutic indication); about the patient (age, weight, geographical distribution) and about the hospital stay (month of leaving, DRG, number and names of supplement payments, associated comorbidities).
Inclusion & noninclusion criteria
Only AP-HP hospitals were included. The inclusion criteria were the deployment of SAP software; the consumptions of ESAs in the year 2013 in more than 50% of care units carrying out MSO activities (as other activities and home care facility are not funded in the same way). The care units, which do not carry out MSO activities were not included in the study.
Outcome measures
The impact on ESA consumptions was assessed by calculating the evolution rates, before and after the delisting, of quantities of ESAs (quantities were always expressed in DDDs) transferred from hospital pharmacies to care units.
The impact on the hospital activity (number of hospital stays equal to number of DRGs) was assessed by estimating the evolution of the number of stays during which ESAs were administered. Considering the lack of data after the delisting of ESAs, two hypotheses were performed to estimate the number of stays for 2014. Hypothesis A: the repartition of the hospital activity is constant from 2013 to 2014, in other words, the proportion of stays during which ESAs were given is the same in 2013 and in 2014. The number of DRGs with administration of ESAs in 2014 was calculated from 2013 data in proportion to the total number of stays in 2014 filled on the e-PMSI. Hypothesis B: the number of hospital stays during which ESAs are given is linked with consumptions of ESAs by care units, the number of stays during which ESAs were given in 2014 was calculated in proportion to quantities of ESAs transferred by each hospital pharmacy to each care unit (dialysis care units and off-dialysis care units; adults and children were separated).
The analysis of the BI was divided into three parts: IB = α-β-γ, where α is the difference between the amount of dialysis (DRG for sessions and supplement payments, valued with the official tariffs of the year) over the March–September 2014 period compared with the March–September 2013 period; β is the amount of PM from March to September 2013; γ is the amount of ESA uses included in DRG, after delisting, and calculated using the purchasing prices before tax.
Results
Products & hospitals included in the study
During the two study periods, four ESA products were included in the AP-HP's drug formulary: two first-generation ESAs: Eprex® (Janssen, NJ, USA; epoetin alfa) and Neorecormon® (Roche, Basel, Switzerland; epoetin beta), one second-generation ESA: Aranesp® (Amgen, CA, USA; darbepoetin alfa) and one third-generation ESA: Mircera® (Roche; methoxy-polyethylene-glycol-epoetin beta). After the delisting of the ESAs from the top-of-DRG list, purchasing prices of first-generation ESAs were not changed while that of second- and third-generation fell (-2.6% for Aranesp and -10.2% for Mircera).
A total of 20 hospitals were included in the study (Figure 3). Among the 37 care facilities of the AP-HP, the structure of home care facility was excluded; 1 hospital was excluded because the SAP software was not deployed at the period of the study and 1 hospital was excluded because it had not consumed any ESA in 2013. The 14 hospitals in which more than 50% of ESA consumptions in 2013 concerned non-MSO services were also excluded. Among the 20 hospitals included in the study, 10 hospitals have dialysis care units. From March to September 2013, ESAs were mostly used for anemia related to renal failure (63.5% of Eprex uses, 89.7% of Aranesp and 98.1% Mircera).
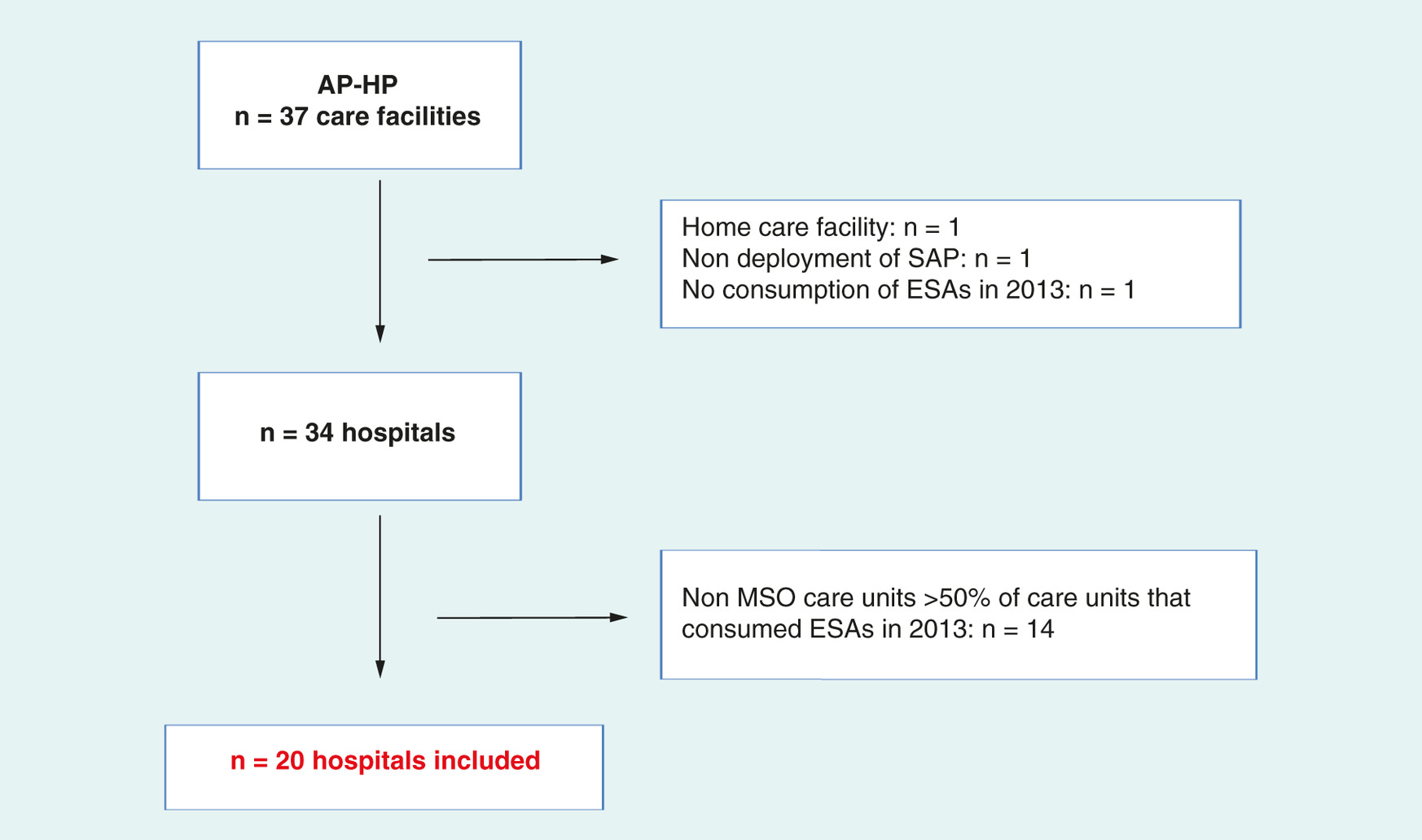
Figure 3. Flowchart of inclusion of hospitals in the study.
Among the 37 care facilities of the AP-HP, the structure of home care facility was excluded; 1 hospital was excluded because the SAP software is not deployed and 1 hospital was excluded because it had not consumed by ESAs in 2013. The 14 hospitals in which more than 50% of consumptions of ESAs in 2013 concerned non-MSO services were also excluded. All in all, a total of 20 hospitals were included in the study.
AP-HP: Public hospitals of Paris (Assistance Publique-Hôpitaux de Paris); ESA: Erythropoiesis-stimulating agent; MSO: Medicine, surgery or obstetrics; SAP: Financial and logistics software shared between all AP-HP care facilities.
Variation of ESA consumptions
After the delisting, ESA consumptions increased by 1.7%; consumptions of Aranesp and Neorecormon, respectively, decreased by 2.2 and 31.6% while consumptions of Eprex and Mircera, respectively, increased by 2.0 and 34.4% (Table 1). In dialysis care units, ESA consumptions decreased by 4.0%, with a decrease of Eprex, Neorecormon and Aranesp consumptions (respectively, -33.7, -29.1 and -9.9%) and an increase of Mircera (+30.3%) consumptions. In off-dialysis care units, ESA consumptions increased by 7.2%. Aranesp was the most consumed ESA both before (69.8%) and after the delisting (67.2%).
| Product | Quantities of ESAs delivered by hospital pharmacies to healthcare units from March to September, DDDs | Evolution of the consumptions (2014 vs 2013) (%) | |
|---|---|---|---|
| 2013 | 2014 | ||
| All care units | |||
| Total ESAs | 271,181 | 275,708 | 1.7% |
| Aranesp® | 189,349 (69.8%) | 185,142 (67.2%) | -2.2% |
| Eprex® | 39,241 (14.5%) | 40,036 (14.5%) | 2.0% |
| Mircera® | 32,410 (12.0%) | 43,570 (15.8%) | 34.4% |
| Neorecormon® | 10,181 (3.8%) | 6960 (2.5%) | -31.6% |
| Dialysis care units | |||
| Total ESAs | 134,251 | 128,878 | -4.0% |
| Aranesp | 87,216 (65.0%) | 78,604 (61.0%) | -9.9% |
| Eprex | 13,956 (10.4%) | 9255 (7.2%) | -33.7% |
| Mircera | 29,570 (22.0%) | 38,529 (29.9%) | 30.3% |
| Neorecormon | 3510 (2.6%) | 2490 (1.9%) | -29.1% |
| Off-dialysis care units | |||
| Total ESAs | 136,930 | 146,831 | 7.2% |
| Aranesp | 102,133 (74.6%) | 106,538 (72.6%) | 4.3% |
| Eprex | 25,285 (18.5%) | 30,781 (21.0%) | 21.7% |
| Mircera | 2840 (2.1%) | 5041 (3.4%) | 77.5% |
| Neorecormon | 6672 (4.9%) | 4471 (30%) | -33.0% |
This table presents the evolution of the quantities of ESAs (Aranesp, Eprex, Mircera and Neorecormon) consumed in the care units between March–September 2013 and March–September 2014. Results are expressed per product in DDDs and as a percentage of the total quantities of ESAs consumed for each year and presented for all care units, for dialysis care units and for care units that do not practice dialysis activities (off-dialysis care units).
DDD: Defined daily dose; ESA: Erythropoiesis-stimulating agent.
Variation of hospital activity
Dialysis sessions
Under Hypothesis A, after the delisting, the number of dialysis sessions during which ESAs were administered increased by 264 (+5%) (Table 2), linked to an increase of the total number of dialysis sessions in 2014 compared with 2013 and considering that the proportion of DRGs with administration of ESAs was the same in 2014 and in 2013. In order to assess the number of dialysis sessions and of dialysis supplements in 2014 under Hypothesis B, it was considered that each ESA administered during a dialysis session was transferred to a dialysis care unit in each hospital. Thus, for any hospitals, the number of dialysis sessions in 2014 was calculated from the 2013 number in proportion to quantities of ESAs transferred to dialysis care units. Otherwise, as an ESA administered during a dialysis supplement could have been transferred either to a dialysis care unit or to an off-dialysis care unit, we calculated the correlation coefficients between quantities of ESAs in 2013 on the basis of databases 1 and 2 and three types of hospitals were thus identified (Table 3): type 1: hospitals have dialysis care units and ESAs administered during dialysis supplements are delivered to an off-dialysis care unit; type 2: hospitals have dialysis care units and ESAs administered during dialysis supplements are transferred to a dialysis care unit; type 3: hospitals do not have dialysis care units (but it is possible for the hospitals to produce dialysis supplements). The data from H15 was globally correlated as it was not correlated by separating dialysis units. Thus, the number of dialysis supplements in 2014 was calculated from the number of 2013 in proportion to, for type 1, quantities of ESAs transferred to off-dialysis care units; for type 2, quantities of ESAs transferred to dialysis care units; type 3 and H15, quantities of ESAs transferred to all care units.
| Hospital | Number of stays with ESAs in 2013 (March–September) | Number of hospital stays with ESAs in 2014 (March–September) (evolution rate, %) | |
|---|---|---|---|
| Hypothesis A | Hypothesis B | ||
| Dialysis sessions | |||
| Total AP-HP | 5278 | 5542 (+5%) | 4829 (-9%) |
| H2 | 737 | 698 (-5%) | 719 (-2%) |
| H4 | 54 | 101 (+87%) | 114 (+111%) |
| H7 | 696 | 650 (-7%) | 408 (-41%) |
| H8 | 192 | 360 (+87%) | 131 (-32%) |
| H9 | 332 | 314 (-6%) | 387 (+17%) |
| H13 | 913 | 1089 (+19%) | 924 (+1%) |
| H15 | 345 | 360 (+4%) | 418 (+21%) |
| H17 | 417 | 386 (-8%) | 440 (+5%) |
| H19 | 276 | 260 (-6%) | 173 (-37%) |
| H20 | 1316 | 1328 (+1%) | 1117 (-15%) |
| Other stays | |||
| Total AP-HP | 4060 | 4140 (2%) | 4406 (9%) |
| H1 | 314 | 314 (0%) | 272 (-13%) |
| H2 | 153 | 163 (6%) | 157 (3%) |
| H3 | 43 | 45 (4%) | 35 (-18%) |
| H4 | 97 | 99 (2%) | 89 (-8%) |
| H5 | 64 | 65 (1%) | 78 (22%) |
| H6 | 47 | 45 (-5%) | 57 (21%) |
| H7 | 352 | 364 (3%) | 333 (-5%) |
| H8 | 376 | 390 (4%) | 769 (104%) |
| H9 | 330 | 330 (0%) | 285 (-14%) |
| H10 | 13 | 13 (3%) | 21 (60%) |
| H11 | 31 | 33 (7%) | 62 (99%) |
| H12 | 41 | 41 (0%) | 11 (-73%) |
| H13 | 423 | 436 (3%) | 343 (-19%) |
| H14 | 75 | 82 (9%) | 47 (-37%) |
| H15 | 496 | 504 (2%) | 672 (35%) |
| H16 | 15 | 15 (3%) | 23 (54%) |
| H17 | 162 | 191 (18%) | 121 (-25%) |
| H18 | 160 | 174 (9%) | 198 (24%) |
| H19 | 463 | 497 (7%) | 511 (10%) |
| H20 | 405 | 339 (-16%) | 322 (-21%) |
The number of hospital stays during which ESAs were administered from March to September 2013 and number of stays calculated for the same period in 2014 under the two assumptions A and B are presented with the changes under each hypothesis as a percentage. Dialysis in sessions are presented separately from the other stays.
Hypothesis A: the repartition of the hospital activity is constant; the proportion of stays during which ESAs were administered is the same in 2013 and in 2014. It was calculated from the 2013 data in proportion to the total number of stays in 2014 filled on the e-PMSI (program for the medicalization of information systems) online platform, giving a feedback on French hospitals activity).
Hypothesis B: the number of stays with administration of ESAs in 2014 is linked with consumptions of ESAs by care units; the number of stays during which ESAs were administered in 2014 was calculated in proportion to quantities of ESAs transferred by each hospital pharmacy to each care unit (dialysis care units and off-dialysis care units and adults and children were separated).
AP-HP: Public hospitals of Paris (Assistance Publique-Hôpitaux de Paris); ESA: Erythropoiesis-stimulating agents; H: Hospital (hospitals were anonymized in H1–H20).
| Type of hospital | Hospitals | Correlation coefficient (p-value) | |
|---|---|---|---|
| Dialysis | Off-dialysis | ||
| Type 1 | H2, H4, H8, H9, H19 | 0.9666 (<0.0005) | 0.9544 (<0.0005) |
| Type 2 | H7, H13, H17, H20 | 0.9820 (<0.0005) | 0.9959 (<0.0005) |
| Type 3 | H1, H3, H5, H6, H10, H11, H12, H14, H16, H18 | Not applicable | 0.9111 (<0.0005) |
| Not applicable | H15 | 0.9955 (<0.001) | |
Coefficients of correlation between ESA volumes dispensed from hospital pharmacies in dialysis units and off-dialysis care units with ESA volumes administered to dialysis patients.
Type 1: hospitals having dialysis care units and in which ESAs administered during dialysis supplements are delivered to an off-dialysis care unit; number of dialysis supplements in 2014 calculated from the number in 2013 in proportion to quantities of ESAs transferred to off-dialysis care units.
Type 2: hospitals having dialysis care units and in which ESAs administered during dialysis supplements are transferred to a dialysis care unit; number of dialysis supplements in 2014 calculated from the number of 2013 in proportion to quantities of ESAs transferred to dialysis care units.
Type 3: hospitals which do not have dialysis care units but can produce dialysis supplements; H15: global correlation as data were not correlated by separating dialysis units; type 3 and H15: number of dialysis supplements in 2014 calculated from the number in 2013 in proportion to quantities of ESAs transferred to all care units.
ESA: Erythropoiesis-stimulating agent; H: Hospital (hospitals were anonymized in H1–H20).
Under Hypothesis B, the number of dialysis sessions during which ESAs were administered decreased after the delisting by 449 (-9%) (Table 2).
Other stays
After the delisting, the number of off-dialysis DRGs in which ESAs were administered increased by 80 (+2%) under Hypothesis A, linked to an increase of the total number of DRGs in 2014 compared with 2013 and considering that under Hypothesis A the proportion of DRGs with administration of ESAs is the same in 2014 and in 2013. The number of off-dialysis DRGs increase by 346 (+9%) under Hypothesis B (Table 2).
Whichever hypothesis is applied, the Wilcoxon test showed no significant difference before and after the delisting neither between the number of dialysis sessions nor between the number of off-dialysis stays during which ESAs were administered. Thus, medical care practices might not have changed during the 7 months following the delisting of ESAs from the out-of-DRG list.
Budget impact
Before the delisting, the amounts of dialysis associated with ESA administrations for the 20 hospitals included in the study corresponded to €4,700,291 with €2,036,894 for dialysis sessions and €2,660,397 for dialysis supplements. The amount of ESAs was €1,257,718 and the amount of PM was €222,035.
After the delisting, under Hypothesis A, the amounts of dialysis with ESA administrations were €5,086,189 with €2,228,909 for dialysis sessions and €2,857,280 for dialysis supplements; the amount of ESAs was €1,185,339. Under Hypothesis B, the amounts were €5,391,897 for dialysis with €1,982,726 for dialysis sessions and €3,409,171 for dialysis supplements and €1,168,265 for ESAs.
All in all, during the 7 months following the delisting of ESAs from the out-of-DRG list, the BI, under Hypothesis A, is estimated at -€1,018,476 with -€365,641 related to dialysis sessions and -€652,834 related to other stays (Table 4); under Hypothesis B it is estimated at -€695,693 with -€592,174 related to dialysis sessions and -€103,518 related to other stays.
| Hypothesis | Hypothesis A | Hypothesis B |
|---|---|---|
| Global BI (BI = α - β - γ) | -€1,018,476 | -€695,693 |
| Difference between number of dialysis sessions in 2014 and in 2013 (α) | €388,898 | €694,606 |
| PM 2013 (β) | -€222,035 | -€222,035 |
| Amount of ESAs included in DRG tariffs in 2014 (γ) | -€1,185,339 | -€1,168,264 |
| Dialysis sessions (BI = α - β - γ) | -€365,641 | -€592,174 |
| Difference between number of dialysis sessions in 2014 and in 2013 (α) | +€192,015 | -€54,168 |
| PM 2013 (β) | -€76,217 | -€76,217 |
| Amount of ESAs included in DRG in 2014 (γ) | -€481,439 | -€461,789 |
| Other stays (BI = α - β - γ) | -€652,834 | -€103,518 |
| Difference between number of dialysis sessions in 2014 and in 2013 (α) | €196,883 | +€748,774 |
| PM 2013 (β) | -€145,818 | -€145,818 |
| Amount of ESAs included in DRG tariffs in 2014 (γ) | -€703,900 | -€706,475 |
The BI for the public hospitals of Paris (AP-HP) during the 7 months following the delisting of erythropoiesis-stimulating agents (ESAs) calculated under each hypothesis is presented. The BI is declined for dialysis in sessions and for the other hospital stays.
Hypothesis A: the repartition of the hospital activity is constant; the proportion of stays during which ESAs were administered is the same in 2013 and in 2014. It was calculated from the 2013 data in proportion to the total number of stays in 2014 filled on the e-PMSI (an online platform giving a feedback on French hospitals activity).
Hypothesis B: the number of stays with administration of ESAs in 2014 is linked with consumptions of ESAs by care units; the number of stays during which ESAs were administered in 2014 was calculated in proportion to quantities of ESAs transferred by each hospital pharmacy to each care unit (dialysis care units and off-dialysis care units and adults and children were separated).
α: difference between amount of dialysis (DRG for sessions and supplement payments, valued with the official tariffs of the year) over the March–September 2014 period compared with the March–September 2013 period. β: amount of PM from March to September 2013. γ: amount of ESA uses included in DRG after delisting calculated using the purchasing prices before tax.
AP-HP: Public hospitals of Paris (Assistance Publique-Hôpitaux de Paris); BI: Budget impact; DRG: Diagnosis-related group; PM: Profit margin.
According to the data available on the e-PMSI platform, the total budget for ESAs and dialysis during the 7 months of the study period (March–September 2013) in the 20 AP-HP hospitals included in the study corresponds to €17.4 million. The BI after delisting represents 5.8% of the total budget under Hypothesis A and 4.0% under Hypothesis B. The total ESAs and dialysis budget is not assessable for the year 2014, as there is no longer any financial traceability of ESAs since these products were delisted from the top-of-DRG list. For a whole year, the BI would be €1.7 million (8.2% of annual budget) under Hypothesis A and €1.2 million (5.8% of annual budget) under Hypothesis B. Nevertheless, this extrapolation during a year should be interpreted with caution, as it is unlikely that neither the hospital activity nor the quantities of medicines consumed (or the DRGs tariffs or ESAs) prices have changed in the course of the year.
Limitations of the study
This study has several limitations. The first limitation is triggered by the fact that our methodology is a before-and-after study. No external comparison group appears in our analysis, which requires a careful interpretation of our results. We chose this approach as a study of this type was easier to implement and more convenient. The second limitation to put forward is that we do not have an access to the whole dialysis activity over the period studied, and thus two hypotheses were considered: the proportion of the dialysis activity was constant between the two periods (Hypothesis A); the dialysis activity was correlated to ESA consumptions delivered by hospital pharmacies to healthcare units (Hypothesis B). This point may be criticized.
Discussion
The results of this study are based on the use of data from medical and administrative databases, which were not designed for the purpose of conducting such studies. The aim of this work was to make some assessments under specific assumptions. Otherwise, this is an early study, since it only concerns the 7-month period after the delisting of ESAs from the out-of-DRG list. Finally, the purpose was not to establish any causal link between the delisting and the ESA consumptions both for inpatients and outpatients. In this regard, no significant change was shown on the hospital dialysis activity following the delisting of ESAs from the out-of-DRG list. These results correspond to those presented at the second meeting of the ‘French national ESAs monitoring committee’ that showed an increase of ESAs bought by the hospitals, including some presentations that are used to treat chronic renal failure (CRF) [7]. Two central medicines purchasing structures were interrogated. The first (150 members, 71 hospitals, a €295 million healthcare product expenses) reported an average decrease in the ESA purchase prices by 8.5% but no change in medical prescription practices, and the second (first French public buyer, 59 Public University Hospitals and Regional Hospitals, a €1.25 billion healthcare product expenses) reported an average decrease in the purchase prices by 8% and then by 20% without any impact on ESAs uses. Furthermore, according to ESA consumptions in community pharmacies, the NHI reported no change in medical practices after the delisting. Variations of ESA consumptions, globally and in community pharmacies, are consistent with our results related to public hospitals. Another study should assess the impact on private hospitals as the dialysis practices may be different between private and public hospitals [7].
In contrast, in our study, the BI is negative for the hospitals of the AP-HP. This could be explained both by the use of an activity-based payment to value sessions and the fact that AP-HP is a Public University Hospitals that has to support severe patients. In fact, ESAs are mostly used in the AP-HP to treat dialysis patients suffering from CRF. A dialysis activity can be valued in two ways: dialysis sessions (daily hospitalization) and dialysis supplements (in-patient). Dialysis sessions represent a variable part of the dialysis activity, the most likely to be modified by changing the funding of associated drugs; hospitals could encourage patients to obtain ESAs in community pharmacies so that drug administration is separated from the dialysis, in order to decrease the amount of ESAs included in DRG. But, we can underline that the lowest the number of sessions produced by the hospital is, the highest the BI for dialysis sessions gets, even if the amount of ESAs included in the DRG tariffs is also lower. This could be directly attributable to the use of an activity-based payment to value sessions: the more a hospital produces sessions, the more it is paid. If the number of sessions decreases, the remuneration decreases. Given the fact that ESAs are less expensive drugs with negotiable purchase prices, the loss is due to both the decrease of dialysis sessions activity and due to the loss of PM not being compensated by the lower amount included in DRG with the decrease of quantities of ESAs consumed. Dialysis during a complete hospitalization, as a supplement payment, should be considered as an invariable part of the dialysis hospital activity because the patient is hospitalized for another main reason than dialysis. Nevertheless, the BI is also negative, explained by the same mechanisms as those for dialysis in sessions, since the tariffs of dialysis supplements benefited from the same re-evaluation as DRG for dialysis in sessions.
These outcomes and considerations raise the question of whether a payment-based activity is the most appropriate way to fund dialysis in hospitals or whether other funding would be more appropriate for this activity.
Conclusion
The French National Authority for Health (Haute Autorité de Santé [HAS] in French) published, in November 2014, a medico-economic study on the management of patients with end-stage CRF [9]. It was required by the NHI and the French Health Ministry, given the steady growth of patients, increasing the economic burden of CRF on the one hand, and taking into account significant regional disparities in the use of different treatment modalities testifying existing flexibilities on the other hand. The objective was to assess the clinical and economic consequences of changes in patient care pathways between different treatment methods, taking into account the possibilities of evolution compared with the situation observed and without denying the freedom of the patient in choosing his treatment method. The evaluation was based on the ten most common dialysis treatment modalities in France: the hemodialysis center, dialysis in dialysis medicalized unit, in auto-dialysis unit and at home; automated peritoneal dialysis and continuous ambulatory peritoneal dialysis, assisted or not assisted by a nurse at home; and kidney transplantation from deceased or living donor. Several alternative strategies were found efficient by age group. This shows the complexity of the care of dialysis patients, which requires, according to HAS, to improve the match between health needs and healthcare provision.
In line with the work of the HAS and within a regulatory evolution framework [10–12], CRF is among the driver pathologies for experimentation on healthcare patients circuits and new payment schemes (including package-based payment and clinical performance indicators) [13]. According to the French Court of Auditors [14], the development of a 2-year study on a healthcare patient circuit before starting dialysis or kidney transplant is expected to objectify deficiencies in managing a patient's disease and thus determine the more appropriate actions to improve it. More recently, on its 2016 report [7], the French Society of Nephrology, Dialysis and Transplant alerted that a reduction of resources allocated for dialysis by regulatory and economic framework changes may threaten the quality and safety of care. This report also specifies that shifting from a dialysis activity toward private hospitals is not appropriate. Indeed, as dialysis care is of high quality in some areas where dialysis healthcare is mainly carried out by public hospitals and public hospitals are a large part of emergency care of patient without any previous nephrologic monitoring and represent a last resort option of care. Finally, the Public University Hospitals should be responsible for education for all substitution techniques of kidney failure.
In conclusion, this study did not show any change in the medical practices of dialysis after the delisting of ESAs from the out-of-DRG list. It can be explained because ESAs are no longer innovative products; they are not expensive and well known by the prescribers. However, the BI of the change in funding is negative for AP-HP. Even if the DRG-based payment for ESA is negative for the budget of our hospitals, it is positive to the French NHI. Indeed, with the price decrease, the ESAs are more costly for the hospital (not funded on top-of-DRG, but less costly for the society). As this is a short-term impact study, over the first 7 months following the delisting, the data should be collected in order to conduct another study to assess the long-term impact of this delisting. Analyses on other therapeutic classes would also be useful in order to show if identical results would be found for other delisted therapeutic classes, notably for some cancer medications. The issue tackled here is first French, but it could also relate to other countries that could make a similar choice in terms of regulation (delisting the drugs funded on top-of-DRG – or outside of a dedicated specified funding – a product that was until then funded in this way may not be neutral regarding the patients’ care and the care organization inside a given country). This study aims at shedding some light on the particular case of ESAs in France. It could indeed be a source of inspiration for other countries.
An additional payment to DRG is available for high costs and innovative drugs in French hospitals: the top-of-DRG list.
Erythropoiesis-stimulating agents (ESAs) used to treat dialysis patients were funded on the top-of-DRG list until March 2014.
Since March 2014, the Minister of Health has decided to delist them, considering their low purchasing prices by hospitals and that they no longer correspond to innovative products.
Following this delisting, there is a risk that physicians may be less likely to prescribe ESAs in hospitals and make patients purchase ESAs in community pharmacies in order to limit the budget impact for their departments.
This raised many concerns related to the fact that a decrease of quality and equity of hospital care could occur due to the potential budget impact especially for severe patients.
The recent experience in the 37 Public University Hospitals in Paris did not show any significant impact on the medical practices of the change of funding of ESAs on the hospital dialysis activity.
This result could be the consequence of the fact that ESAs are no longer innovative products, are low-cost products and well known by the prescribers.
Even if the DRG-based payment for ESA is negative for the budget of Public University Hospitals of Paris, it remains positive for the French National Health Insurance.
Financial & competing interests disclosure
Open Access Option funding was provided by the Paris Descartes University, France. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Degrassat-Théas A, Bensadon M, Rieu C, Angalakuditi M, Le Pen C, Paubel P. Hospital reimbursement price-cap for cancer drugs: the French experience in controlling hospital drug expenditures. Pharmacoeconomics 30(7), 565–573 (2012).
• Explains in detail the system of funding for expensive drugs in hospitals in France.
2.
Financing of Social Security Act for 2004 of 18 December 2003, No. 2003-1199 Law Official Journal of the French Republic of 19 December 2003 [in French]. www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000000249276.
3.
Decree 2016-349 of 24th March 2016 on the procedure and conditions for registration of pharmaceutical products on the list referred to in Article L. 162-22-7 of the Social Security Code. Official Journal of the French Republic of 25 March 2016 [in French]. www.legifrance.gouv.fr/eli/decret/2016/3/24/AFSH1532721D/jo.
4.
Decree of 19th February 2009 on classification and management of hospital benefits for medical, surgery, obstetrics and dentistry activities and made pursuant to Article L. 162-22-6 of the Social Security Code. Official Journal of the French Republic of 26 February 2009 [in French]. www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000020310296&categorieLien=id.
5.
Decree of 14th February 2014 amending the Decree of 19th February 2009 on classification and management of hospital benefits for medical, surgery, obstetrics and dentistry activities and made pursuant to Article L. 162-22-6 of the Social Security Code. Official Journal of the French Republic of 25 February 2014 [in French]. www.legifrance.gouv.fr/eli/arrete/2014/2/13/AFSS1404034A/jo.
• Legal text that deleted the erythropoiesis-stimulating agents from the top-of-DRG list in March 2014.
6.
Decree of 13th February 2014 amending the list of pharmaceutical products funded in addition to the hospital benefits referred to in Article L. 162-22-7 of the Social Security Code. Official Journal of the French Republic of 20 February 2014 [in French]. www.legifrance.gouv.fr/eli/arrete/2014/2/13/AFSS1404034A/jo.
• Legal text that deleted the erythropoiesis-stimulating agents from the top-of-DRG list in March 2014.
7.
French Society of Nephrology Dialysis and Transplantation. Report on chronic dialysis in France in 2016 [in French]. www.centresdedialyse.com/wp-content/uploads/2015/03/rapport_dialyse_chronique_France_2016_SFNDT.pdf.
8.
French Technical Agency of Information on Hospitals. Methodological guide for production of information relating to medical activity and to its billing as medicine, surgery, obstetrics and dentistry (2014). www.atih.sante.fr.
9.
French National Authority for Health. Medico-economic evaluation of the management of strategies of end stage renal disease in France. Report (2014). www.has-sante.fr/portail/jcms/c_1775180/fr/evaluation-medico-economique-des-strategies-de-prise-en-charge-de-l-insuffisance-renale-chronique-terminale-en-france.
• Report serving as a reference for medico-economic evaluation of the management of dialysis patients in France.
10.
Ministry of Social Affairs and Health. National Health Strategy, Roadmap (2013). solidarites-sante.gouv.fr/IMG/pdf/SNS-Feuille_de_route.pdf.
11.
Social Security Financing Act for 2014 NO 2013-1203 of 23th December 2013. Official Journal of the French Republic of 24th December 2013. solidarites-sante.gouv.fr/IMG/pdf/SNS-Feuille_de_route.pdf.
12.
Social Security Financing Act for 2015 NO 2014-1554 of 22th December 2014. Official Journal of the French Republic of 24th December 2013. www.securite-sociale.fr/-LFSS-2015-.
13.
French Health Ministry. Management of chronic renal failure: the ministry is launching experiments in six pilot regions. Formal statement (2015). www.sante.gouv.fr.
14.
Court of Auditors. Report of the Court of Auditors (2015). www.ccomptes.fr/fr.
Information & Authors
Information
Published In
Copyright
© 2018 Pascal Paubel and all co-authors.
History
Received: 28 August 2017
Accepted: 14 February 2018
Published online: 14 March 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Economic and organizational impact of the changing hospital funding practices of erythropoiesis-stimulating agents on the management of care of dialysis patients in France. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0067
Export citation
Select the citation format you wish to export for this article or chapter.