Survival comparison of hepatocellular carcinoma patients treated with radioembolization versus nonoperative/interventional treatment
Abstract
Aim: To compare the overall survival (OS) and liver cancer-specific survival of advanced-stage hepatocellular carcinoma (HCC) patients who received transarterial radioembolization (TARE) with those who received nonoperative/interventional treatment (NOT). Materials & methods: A total of 12,520 HCC patients from the Surveillance, Epidemiology and End Results database were categorized by treatment with either radioembolization or NOT. Kaplan–Meier and multivariate Cox regression were conducted. Results: The TARE group had both a significantly longer median overall survival than the NOT group (TARE = 9 months; NOT = 2 months; p < 0.0001) and a significantly higher probability of liver cancer-specific survival (hazard ratio = 0.474). Conclusion: TARE appears to provide a significant survival advantage over the NOT population in advanced HCC patients.
Treatment options for hepatocellular carcinoma (HCC) vary widely depending on the size and number of liver lesions, the extent of disease and liver function scores determined by the Child–Pugh classification. For patients fortunate enough to have smaller and localized disease, minimally invasive treatment methods such as the percutaneous injection of ethanol (PEI) or ablation by locoregional delivery of radiofrequency radiation (RFA) are effective, possible options for complete disease removal [1]. For those patients with more extensive early stage HCC, transplantation or surgical resection remains the only chance for a cure [2–4]. Unfortunately, a large proportion of patients are not surgical candidates and many patients who undergo successful disease removal develop recurrent disease [5,6]. Therefore, many patients are left with limited treatment options for disease control or effective palliation. For patients with localized HCC who are not surgical candidates, chemoembolization can be offered as it has been shown to improve survival in patients with intermediate stage disease [7,8].
Once the disease has progressed to advanced T3/T4 HCC (disease that is categorized by portal vein thrombosis and nodal or metastatic disease), the standard of therapy is the multi-tyrosine kinase inhibitor sorafenib [9]. Sorafenib has been shown, through randomized controlled clinical trials, to improve survival in advanced HCC patients [9,10]. In addition, there are advanced HCC patients who still prefer the best supportive care route including comfort measures and palliation. These patients collectively may be placed into the nonoperative/interventional treatment (NOT) route of care group where complete disease removal is unlikely and interventional procedures are no longer considered. Within the recent past, however, some centers have advocated for the use of transarterial radioembolization (TARE) in this patient population because it may improve local disease control and is well tolerated in patients with portal vein thrombosis [11]. Further, it has been reasoned that local disease control may improve survival given that liver tumor burden sometimes dictates the prognosis independent of background liver synthetic function [12].
While the use of TARE is fairly commonplace in the advanced HCC population [13–16], randomized controlled trials (RCTs) such as the SARAH [17] and SIRveNIB trial [18] continue to show that TARE provides similar efficacy to sorafenib with a lower toxicity profile [19]. Nevertheless, there are few studies that have compared the efficacy of TARE with NOT in the advanced HCC patient population. Drawing from the available literature, we reason that TARE may provide a net survival benefit over NOT in patients with advanced HCC. We hope that this study will provide further support for those patients looking for guidance in navigating the many treatment options for advanced HCC.
Accordingly, we utilized the Surveillance, Epidemiology and End results (SEER) database to assess the overall survival (OS) and liver cancer-specific survival (LCSS) in advanced stage (AJCC III/IV) HCC patients treated with TARE versus those electing for the NOT.
Materials & methods
SEER database
This study was exempt from Institutional Review Board approval and was completed in accordance with the National Cancer Institute SEER user agreement. The SEER database provides information on cancer statistics with the goal of reducing the cancer burden in the USA. Data is collected from 18 registries from various locations throughout the country that covers approximately 28% of the American population. Collected data include patient demographics, primary tumor site, tumor morphology, stage at diagnosis, first course of treatment and survival. Care is taken to ensure that individual state registry data are acceptable for subsequent data pooling [20].
Study population
Advanced HCC was defined as American Joint Committee on Cancer (AJCC) stage III and IV disease since these patients have nodal or distant metastases and are not typically candidates either for surgical or locoregional therapy (per Barcelona clinic liver cancer [BCLC] criteria). Advanced HCC cases from 2004 to 2013 were identified. The search was limited to 2004–2013, given that the database contained very few TARE cases prior to 2004, and 2013 was the last year included in the 2016 release. Subjects with other primary cancers and those treated with surgery, transplantation, prior ablative therapies and external beam radiation were excluded to avoid confounding variables. Thus, the composition of the NOT group for this study included those patients who had palliative therapy or unspecified chemotherapy/immunomodulator treatment (sorafenib or otherwise).
Subjects treated with TARE were identified as any subjects with treatment code ‘radioactive implants’ (including brachytherapy) or ‘radioisotopes’ [21]. According to the SEER program coding and staging manual 2016, TARE should be coded as ‘radioactive implants’; however, previous cases have also been coded as ‘radioisotopes’ as per confirmation from the SEER registrar [21]. Of note, an additional analysis comparing patients coded as ‘radioactive implants’ compared with those patients coded as ‘radioisotopes’ was performed to ensure that no differences existed between these groups. For the purposes of this study, patients who are not treated with surgery, radiation or radioembolization were classified as NOT. We do concede that there may be some treatment regiments that were given to patients that were not recorded in the database. Nonetheless, patients without recorded treatments were still classified as NOT.
Demographic, clinical & outcomes data
Demographic and clinical variables obtained from the SEER database included age at diagnosis, race, sex, tumor histology, tumor grade, tumor size, fibrosis score and α-fetoprotein (AFP)-level classification (as continuous variable information for AFP was not provided by the SEER database). The primary outcome was OS, and the secondary outcome was LCSS, which censors patients who died from a cause other than cancer. SEER cause of death data are classified as either attributable to cancer or secondary to another cause. Outcomes were calculated using total months survived, a variable provided by the database. For OS, patients were censored if they were alive at the end of the study period.
Statistics
Baseline demographics and clinical characteristics were compared with a χ2 test for categorical variables and nonparametric Wilcoxon sum rank test for continuous variables. A Kaplan–Meier survival curve was carried out for OS, and a competing risk analysis of cumulative incidence of liver cancer-specific death with a competing risk event of death due to a cause other than cancer was employed for evaluation of LCSS in patients who underwent TARE or NOT. The log-rank test was used to examine the statistical significance of the differences observed between the groups. A multivariate Cox proportional hazards model was also applied to compute hazard ratios (HRs) and 95% CI, adjusting for known prognostic variables (age, gender, AJCC stage, histologic grade, tumor node metastasis [TNM] stage, AFP and fibrosis scores).
Propensity score & subgroup analyses
Given that both treatment populations were not homogeneous, selection bias was deemed inevitable. Therefore, propensity matching was performed to combat inherent bias. This strategy has been shown to be the most aggressive statistical method to control for background factors in a cohort study and it ensures that known prognostic factors in each group are similarly distributed. This strategy has also been shown to observationally mimic RCTs [22]. Propensity scores were generated using logistic regression, with treatment as the dependent variable and background factors as independent variables. Independent variables that were utilized were those that were reported in the SEER database and included age, gender, race, tumor grade, tumor size, AJCC stage, fibrosis score and AFP level classification. In the SEER database AFP is reported as ‘elevated’, ‘normal’ or ‘unknown’. Fibrosis score is provided as a binary value, with ‘yes’ indicating cirrhosis or severe fibrosis and ‘no’ indicating no or mild fibrosis. No distinction is provided for hepatitis or mild fibrosis. Patients were matched in a 1:1 ratio using the nearest neighbor method outlined in the local and global optimal propensity score matching [23]. Propensity score matched groups were analyzed, where matched pairs Cox regression models were used to estimate differences in OS and LCSS between treatment groups. Two-sided p < 0.05 is considered statistically significant. All analyses were performed within SAS (version 9.4; SAS, NC, USA).
Results
Overall population characteristics
AJCC stage III and stage IV patients were identified for inclusion into the study. Exclusion criteria and their effects on population size are summarized in Figure 1. The number of cases that were identified with histologic or radiographically confirmed HCC was 78,058. After our pretreatment and demographic exclusion criteria were applied, the remaining number of patients was 30,228. Further excluding stages I, II and unknown resulted in 367 patients treated with TARE and 12,153 NOT therapies (Figure 1).

Figure 1. Study population formation from SEER confirmed HCC cases from 2004 to 2013.
AJCC: American Joint Committee on Cancer; HCC: Hepatocellular carcinoma; SEER: Surveillance, Epidemiology and End Results; TARE: Transarterial radioembolization.
Background variables & survival analysis: unmatched group
The unmatched study population consisted of 367 in the TARE group and 12,153 in the NOT group. There was no significant difference in gender distribution or age. However, there were significant differences in AJCC stage, tumor grade, TNM staging, AFP and fibrosis scores between the groups. The NOT group had a higher proportion of AJCC stage IV cases, a higher ratio of poorly differentiated tumors, unknown TNM staging, unknown AFP and unknown fibrosis scores (Table 1).
| Characteristic | Overall, % (n) | NOT, % (n) | Radioembolization (TARE), % (n) | p-value |
|---|---|---|---|---|
| Gender: | 0.9654 | |||
| – Female | 19 (2377) | 19 (2307) | 19.1 (70) | |
| – Male | 81 (1141) | 81 (9846) | 81 (297) | |
| Cancer stage: | < 0.0001 | |||
| – Stage III | 56.9 (7128) | 56.1 (6819) | 84.2 (309) | |
| – Stage IV | 43.1 (5392) | 43.9 (5334) | 15.8 (58) | |
| Tumor grade: | 0.0003 | |||
| – I (well) | 26.8 (1034) | 26.4 (982) | 37.1 (52) | |
| – II (moderately) | 38.1 (1470) | 37.9 (1409) | 43.6 (61) | |
| – III (poorly) | 31.9 (1231) | 32.4 (1205) | 18.6 (26) | |
| – IV (undifferentiated) | 3.2 (125) | 3.3 (124) | 0.7 (1) | |
| Tumor (T) stage: | < 0.0001 | |||
| – T0 | 0.2 (22) | 0.2 (22) | 0 | |
| – T1 | 10.7 (1343) | 11 (1333) | 2.7 (10) | |
| – T2 | 5.7 (718) | 5.8 (704) | 3.8 (14) | |
| – T3 | 61 (7633) | 60.3 (7327) | 83.4 (306) | |
| – T4 | 10.4 (1302) | 10.5 (1275) | 7.4 (27) | |
| – Tx | 12 (1502) | 12.3 (1492) | 0.7 (10) | |
| Node (N) stage: | < 0.0001 | |||
| – N0 | 65.9 (8249) | 65.6 (7968) | 76.6 (281) | |
| – N1 | 19.2 (2401) | 19.2 (2331) | 19.1 (70) | |
| – Nx | 14.9 (1870) | 15.2 (1854) | 4.3 (16) | |
| Metastasis (M) stage: | < 0.0001 | |||
| – M0 | 56.9 (7128) | 56.1 (6819) | 84.2 (309) | |
| – M1 | 43.1 (5392) | 43.9 (5334) | 15.8 (58) | |
| AFP: | 0.0052 | |||
| – Borderline | 0.2 (22) | 0.2 (21) | 0.3 (1) | |
| – Elevated | 68.6 (8591) | 68.5 (8323) | 73 (268) | |
| – Normal | 11.4 (1425) | 11.3 (1374) | 13.9 (51) | |
| – Unknown | 19.8 (2482) | 20 (2435) | 12.8 (47) | |
| Fibrosis: | < 0.0001 | |||
| – Fibrotic | 16.3 (2045) | 16 (1949) | 26.2 (96) | |
| – None | 3.7 (466) | 3.8 (454) | 3.3 (12) | |
| – Unknown | 80 (10009) | 80.2 (9750) | 70.5 (259) | |
| Age, mean (SD) | 62.3 (11.8) | 62.3 (11.8) | 62.9 (10.8) | 0.253 |
AFP: α-fetoprotein; NOT: Nonoperative/interventional treatment; Nx: Node metastases unknown; SD: Standard deviation; TARE: Transarterial radioembolization; Tx: Treatment.
The TARE group had a significantly (p < 0.0001) longer median OS of 9 months (95% CI: 8–11 months) compared with the NOT group of 2 months (95% CI: 2–3 months; Figure 2). Similarly, there was a lower probability of LCSS in the NOT group, with an HR of 1.79 (95% CI: 1.63–1.96; Figure 3). Furthermore, treatment type showed independent prognostic significance for both OS and LCSS. TARE showed a protective effect with an HR of 0.474 (95% CI: 0.285–0.786; Table 2). Other covariates that showed significant OS and LCSS prognostic value included tumor stage, tumor grade and tumor size (Tables 2 & 3).
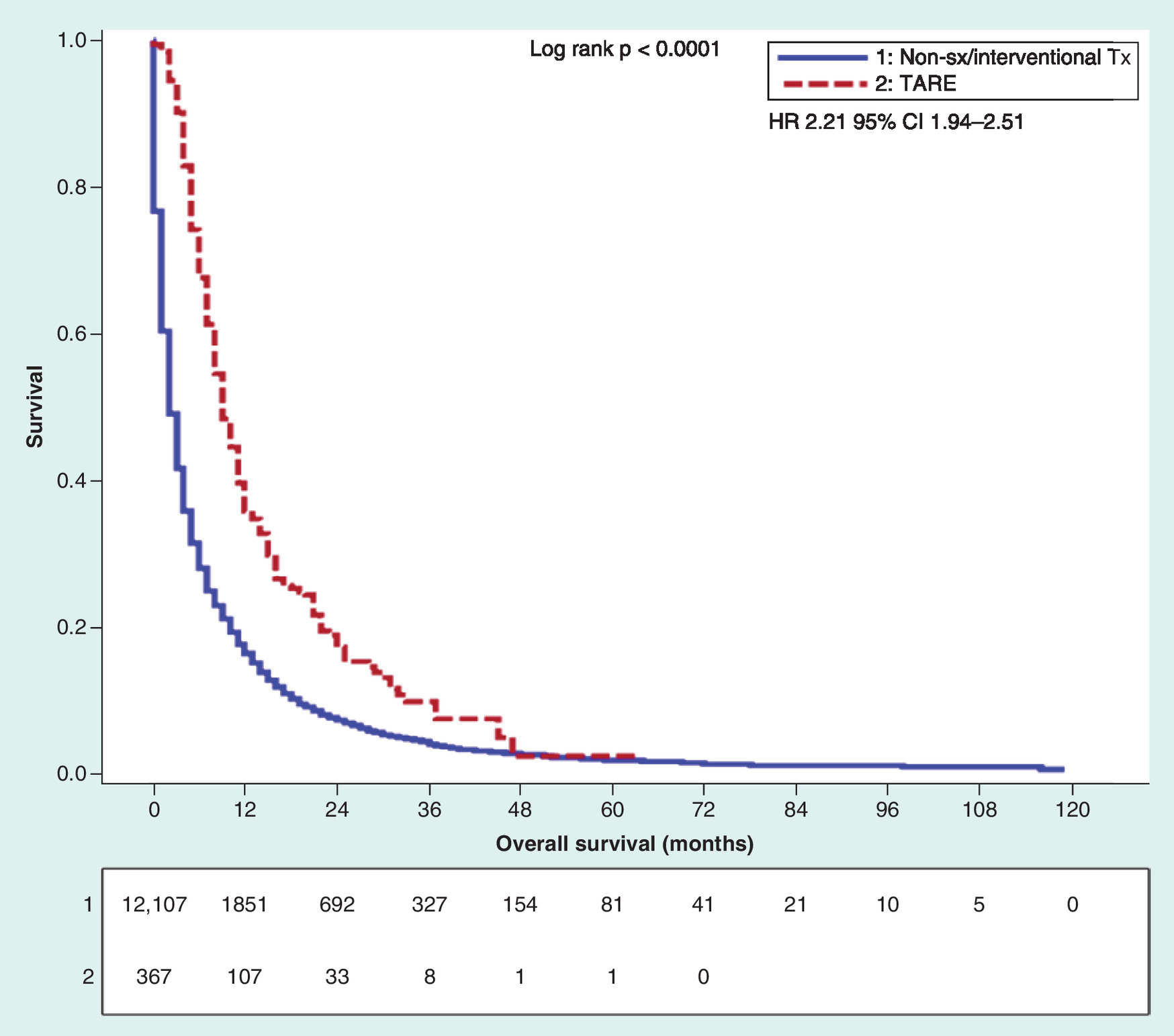
Figure 2. Kaplan–Meier overall survival analysis of advanced hepatocellular carcinoma patients treated with TARE compared to non-Sx/interventional Tx in the unmatched patient population.
HR: Hazard ratio; Sx: Surgical; TARE: Transarterial radioembolization; Tx: Treatment.
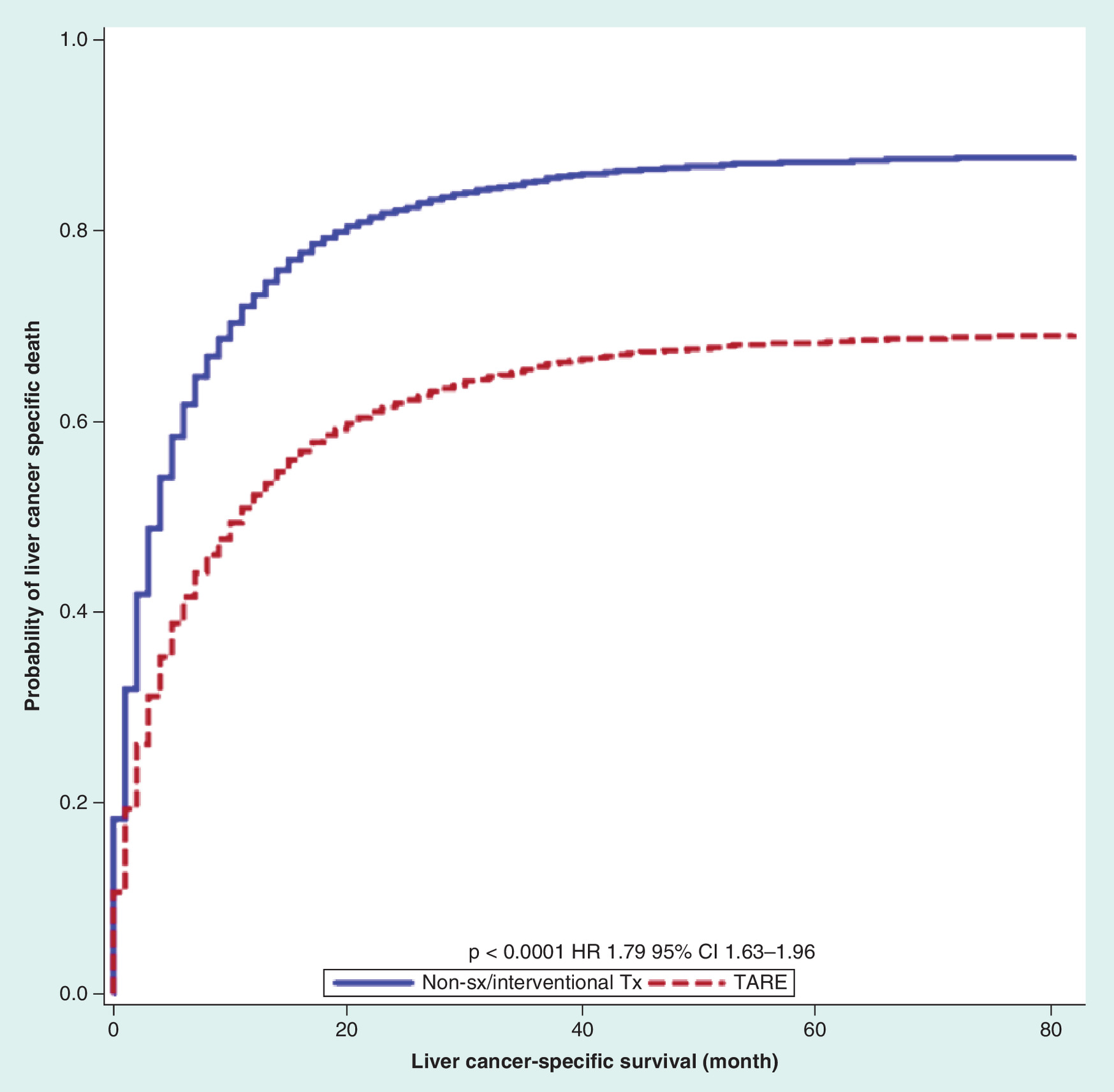
Figure 3. Liver cancer-specific survival analysis of advanced hepatocellular carcinoma patients treated with TARE compared to non-Sx/interventional Tx in the unmatched patient population.
HR: Hazard ratio; Sx: Surgical; TARE: Transarterial radioembolization; Tx: Treatment.
| Treatment | OS median (months) | Lower 95% confidence limit | Upper 95% confidence limit |
|---|---|---|---|
| Unmatched group | |||
| Nonsurgical/interventional treatment | 2.000 | 2.000 | 3.000 |
| Radioembolization | 9.000 | 8.000 | 11.000 |
| Matched group | |||
| Nonsurgical/interventional treatment | 4.000 | 3.000 | 4.000 |
| Radioembolization | 9.000 | 8.000 | 11.000 |
OS: Overall survival.
| Characteristic | Overall, % (n) | NOT, % (n) | Radioembolization (TARE), % (n) | p-value |
|---|---|---|---|---|
| Gender: | 0.7039 | |||
| – Female | 18.5 (136) | 18 (66) | 19.1 (70) | |
| – Male | 81.5 (598) | 82 (301) | 80.9 (297) | |
| Cancer stage: | 0.535 | |||
| – Stage III | 85 (624) | 85.8 (315) | 84.2 (309) | |
| – Stage IV | 15 (110) | 14.2 (52) | 15.8 (58) | |
| Tumor grade: | 0.8499 | |||
| – I (well) | 37.7 (103) | 38.3 (51) | 37.1 (52) | |
| – II (moderately) | 44.7 (122) | 45.9 (61) | 43.6 (61) | |
| – III (poorly) | 17.2 (47) | 15.8 (21) | 18.6 (26) | |
| – IV (undifferentiated) | 0.4 (1) | 0 | 0.7 (1) | |
| Tumor (T) stage: | 0.5504 | |||
| – T1 | 3 (22) | 3.3 (12) | 2.7 (10) | |
| – T2 | 3.1 (23) | 2.4 (9) | 3.8 (14) | |
| – T3 | 83.9 (616) | 84.5 (310) | 83.4 (306) | |
| – T4 | 6.6 (48) | 5.7 (21) | 7.4 (27) | |
| – Tx | 3.4 (25) | 4.1 (15) | 2.7 (10) | |
| Node (N) stage: | 0.755 | |||
| – N0 | 76.6 (562) | 76.6 (281) | 76.6 (281) | |
| – N1 | 18.5 (136) | 18 (66) | 19.1 (70) | |
| – Nx | 4.9 (36) | 5.5 (20) | 4.3 (16) | |
| Metastasis (M) stage: | 0.535 | |||
| – M0 | 85 (624) | 85.8 (315) | 84.2 (309) | |
| – M1 | 15 (110) | 14.2 (52) | 15.8 (58) | |
| AFP: | 0.1702 | |||
| – Borderline | 0.3 (2) | 0.3 (1) | 0.3 (1) | |
| – Elevated | 75.2 (552) | 77.4 (284) | 73 (268) | |
| – Normal | 11.4 (84) | 9 (33) | 13.9 (51) | |
| – Unknown | 13.1 (96) | 13.3 (49) | 12.8 (47) | |
| Fibrosis: | 0.0684 | |||
| – Fibrotic | 26.6 (195) | 27 (99) | 26.2 (96) | |
| – None | 2 (15) | 0.8 (3) | 3.3 (12) | |
| – Unknown | 71.4 (524) | 72.2 (265) | 70.6 (259) | |
| Age, mean (SD) | 63 (10.8) | 63 (10.8) | 62.9 (10.8) | 0.9291 |
AFP: α-fetoprotein; NOT: Nonoperative/interventional treatment; SD: Standard deviation; TARE: Transarterial radioembolization.
Background variables & survival analysis: matched group
In the propensity-matched comparison, there were 367 TARE cases matched to 367 NOT cases, for a total of 734 cases. There was no significant difference between groups with regards to gender ratio, age, AJCC cancer stage, tumor grade, TNM stage, AFP or fibrosis score (Table 3).
The TARE group had a significantly longer overall median survival of 9 months (95% CI: 8–11 months) compared with the NOT group of 4 months (95% CI: 3–4; p < 0.0001; Figure 4). This result is further supported by a lower probability of LCSS in the NOT group with a HR of 1.64 (95% CI: 1.4–1.93; Figure 5).
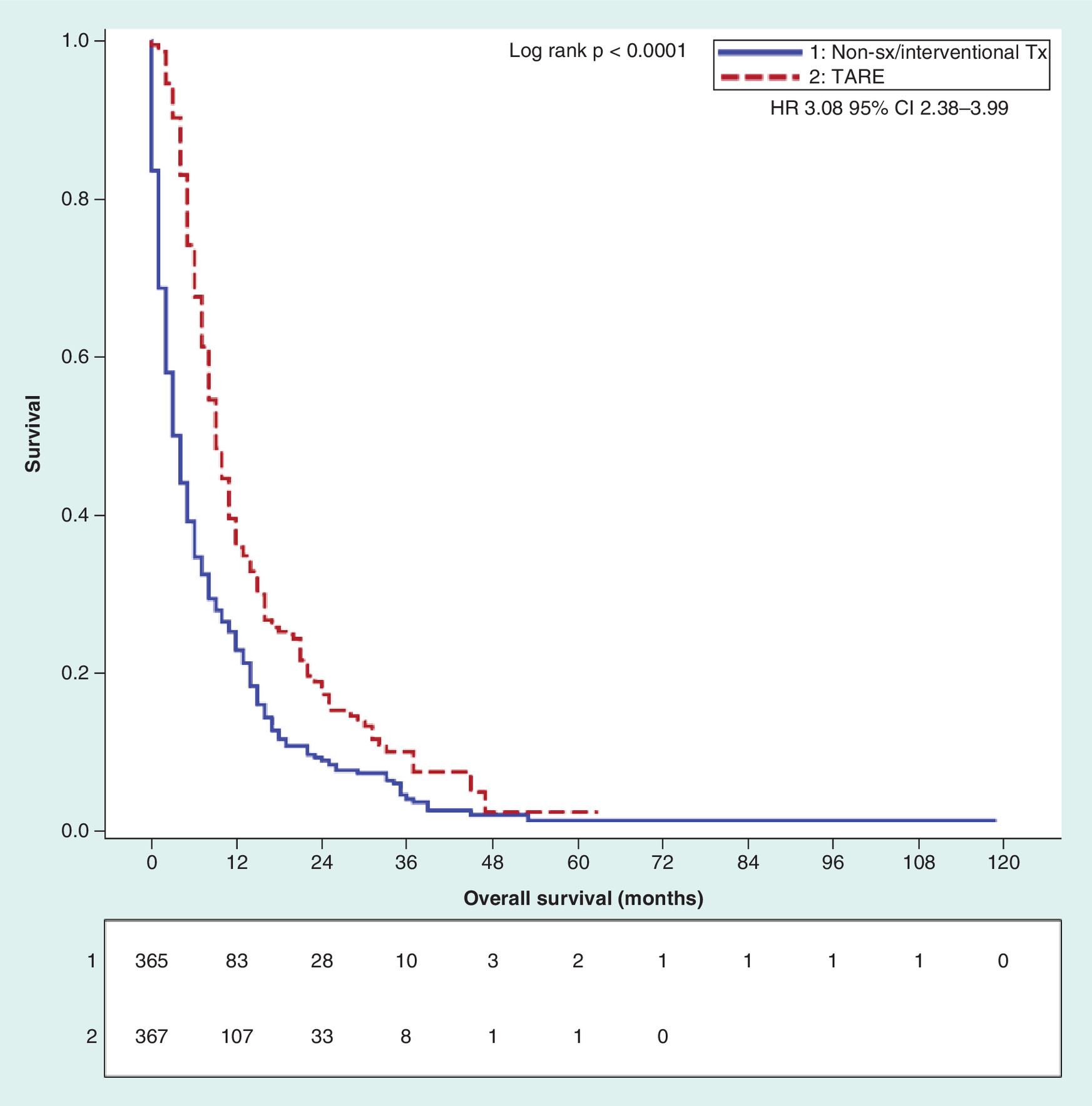
Figure 4. Kaplan–Meier overall survival analysis of advanced hepatocellular carcinoma patients treated with TARE compared to non-Sx/interventional Tx in the matched patient population.
HR: Hazard ratio; Sx: Surgical; TARE: Transarterial radioembolization; Tx: Treatment.
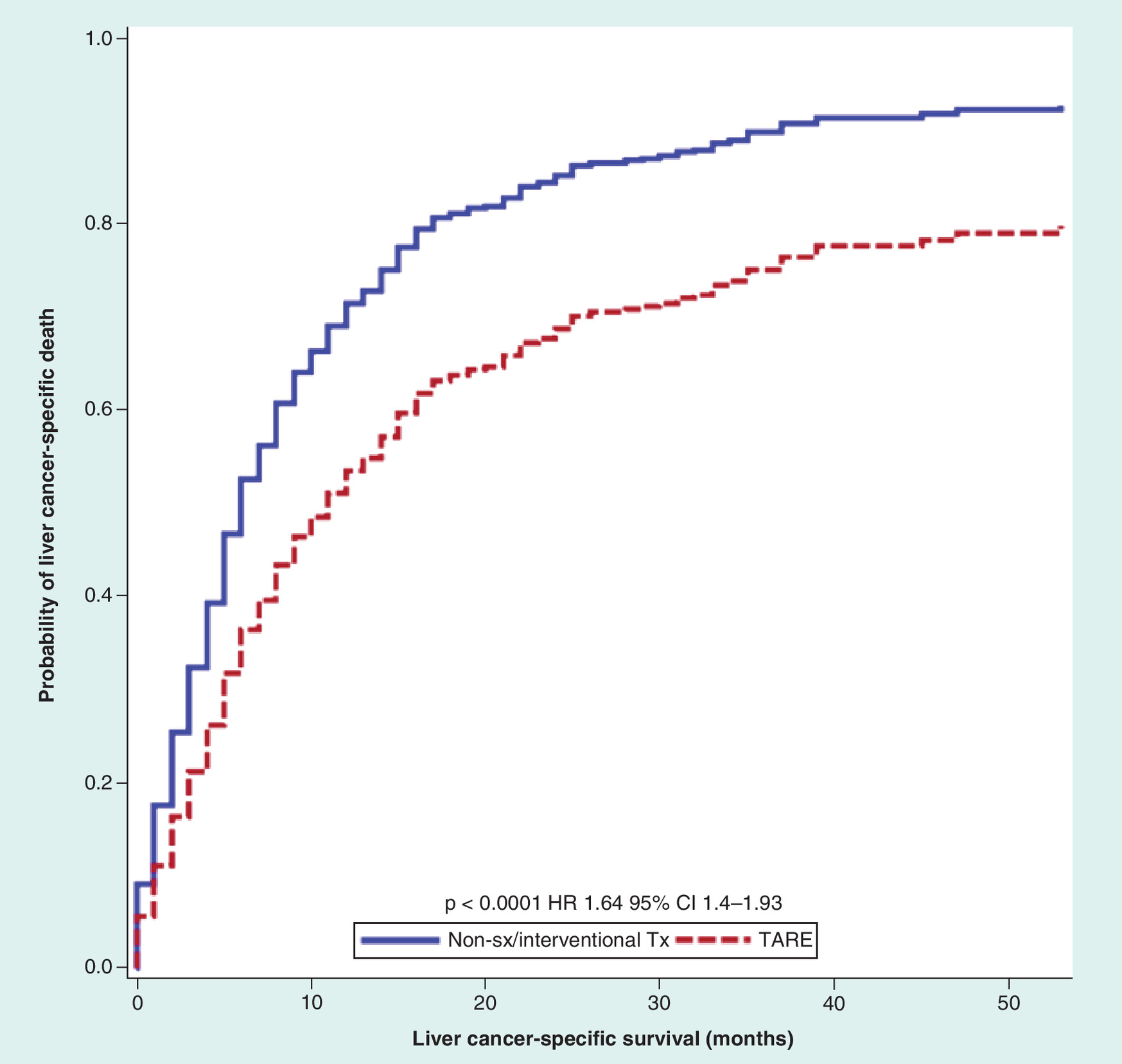
Figure 5. Liver cancer-specific survival analysis of advanced hepatocellular carcinoma patients treated with TARE compared to non-Sx/interventional Tx in the matched patient population.
HR: Hazard ratio; Sx: Surgical; TARE: Transarterial radioembolization; Tx: Treatment.
Radioactive implants versus radioisotopes
Comparisons were made between these two International Classification of Disease (ICD) codes to confirm that the study populations could be equally considered. Baseline demographics and clinical patient characteristics comparing the two different ICD distinctions revealed only fibrosis score as a differing variable between the two groups with a higher proportion of fibrotic patients in the radioisotopes group (Table 4). All other metrics were considered to be statistically nonsignificant. OS was 10 months for the radioactive implants group (95% CI: 8–12 months) and 9 months for the radioisotopes group (95% CI: 8–10 months; Table 5 & Figure 6). Log-rank test between the two groups was not statistically significant with p = 0.0815 (Figures 6 & 7). These two groups were subsequently combined in our study.
| Characteristic | Overall, % (n) | Radioactive implants, % (n) | Radioisotopes, % (n) | p-value |
|---|---|---|---|---|
| Gender: | 0.8894 | |||
| – Female | 19.1 (70) | 19.4 (36) | 18.8 (34) | |
| – Male | 80.9 (297) | 80.6 (150) | 81.2 (147) | |
| Cancer stage: | 0.6897 | |||
| – Stage III | 84.2 (309) | 84.9 (158) | 83.4 (151) | |
| – Stage IV | 15.8 (58) | 15.1 (28) | 16.6 (30) | |
| Tumor grade: | 0.8471 | |||
| – I (well) | 37.1 (52) | 36.7 (29) | 37.7 (23) | |
| – II (moderately) | 43.6 (61) | 43 (34) | 44.3 (27) | |
| – III (poorly) | 18.6 (26) | 19 (15) | 18 (11) | |
| – IV (undifferentiated) | 0.7 (1) | 1.3 (1) | 0 | |
| Tumor (T) stage: | 0.0531 | |||
| – T1 | 2.7 (10) | 0.5 (1) | 5 (9) | |
| – T2 | 3.8 (14) | 4.3 (8) | 3.3 (6) | |
| – T3 | 83.4 (306) | 87.1 (162) | 79.6 (144) | |
| – T4 | 7.4 (27) | 5.9 (11) | 8.8 (16) | |
| – Tx | 2.7 (10) | 2.2 (4) | 3.3 (6) | |
| Node (N) stage: | 0.2092 | |||
| – N0 | 76.6 (281) | 76.3 (142) | 76.8 (139) | |
| – N1 | 19.1 (70) | 21 (39) | 17.1 (31) | |
| – Nx | 4.3 (16) | 2.7 (5) | 6.1 (11) | |
| Metastasis (M) stage: | 0.6897 | |||
| – M0 | 84.2 (309) | 84.9 (158) | 84.3 (151) | |
| – M1 | 15.8 (58) | 15.1 (28) | 16.6 (30) | |
| AFP: | 0.686 | |||
| – Borderline | 0.3 (1) | 0.5 (1) | 0 | |
| – Elevated | 73 (268) | 73.7 (137) | 72.4 (131) | |
| – Normal | 13.9 (51) | 14.5 (27) | 13.3 (24) | |
| – Unknown | 12.8 (47) | 11.3 (21) | 14.4 (26) | |
| Fibrosis: | 0.0048 | |||
| – Fibrotic | 26.2 (96) | 18.8 (35) | 33.7 (61) | |
| – None | 3.3 (12) | 3.2 (6) | 3.3 (6) | |
| – Unknown | 70.6 (259) | 78 (145) | 63 (114) | |
| Age, mean (SD) | 62.9 (10.8) | 63.1 (9.9) | 62.7 (11.6) | 0.7272 |
AFP: α-fetoprotein; SD: Standard deviation.
| Treatment | OS median (months) | Lower 95% confidence limit | Upper 95% confidence limit |
|---|---|---|---|
| ‘Radioactive implants’ | 10.0 | 8.0 | 12.0 |
| ‘Radioisotopes’ | 9.0 | 8.0 | 10.0 |
OS: Overall survival.
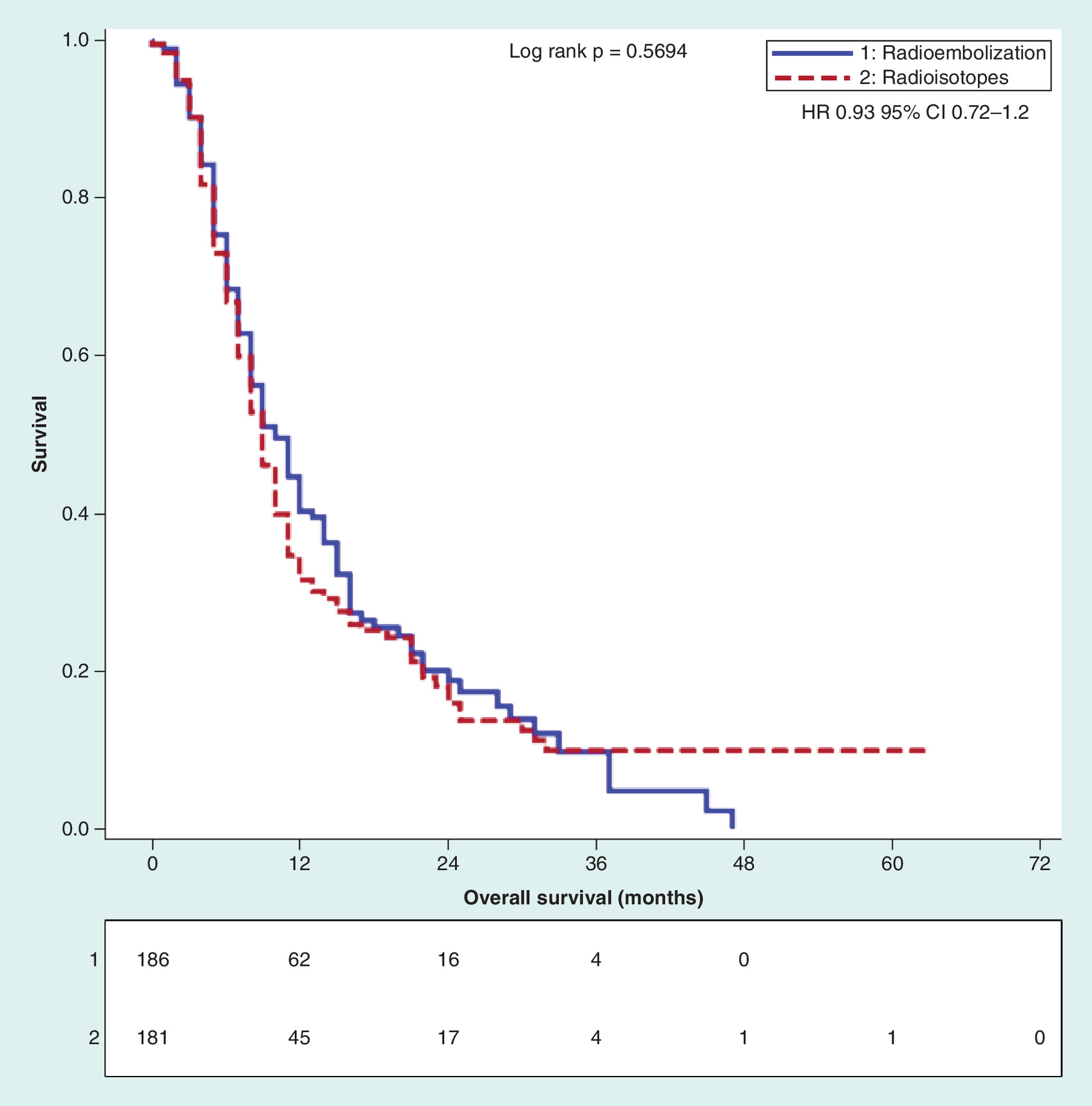
Figure 6. Kaplan–Meier overall survival analysis of combined ‘radioisotope' labeled and ‘radioactive implants' labeled radioembolization patients.
HR: Hazard ratio.

Figure 7. Liver cancer-specific survival analysis of combined ‘radioisotope' labeled and ‘radioactive implants' labeled radioembolization patients.
HR: Hazard ratio.
Discussion
The utility of TARE for advanced HCC is fairly commonplace with several papers reporting good efficacy in this treatment population [11,15,19,24,25]. A review published by Rognoni et al. [16] investigated 26 papers evaluating studies relating to the efficacy of TARE for the treatment of advanced HCC. Through their work, they found that the average OS for advanced HCC patients receiving TARE is approximately 12–24 months with this range cut in half when there is main portal vein involvement (one indication of AJCC stage IV HCC). Other studies have also supported a prognosis in this range [15,25,26].
The SEER database can be a valuable tool to study the net effects of TARE compared with patients receiving NOT in a large patient population. The advantages of using a large population database include having adequate power to reveal differences between therapies, performing regression analysis in a large population, having the ability to perform propensity matched pairs while maintaining adequate power for comparison, and observing a ‘real life’ treatment population without the patient selection that occurs with RCTs [27,28]. Comparing the difference between NOT and TARE would be difficult to do in a RCT setting because of inherent differences in the treatment population. In addition, the NOT strategy is potentially unethical as sorafenib has effectively been established as the standard of AJCC advanced HCC care [9]. In addition locoregional treatments are becoming more commonplace in this clinical setting and are increasingly being shown to provide a survival benefit [15,25,26]. Still, large-scale studies establishing the net benefit of TARE compared with NOT are lacking, which leaves room to further delineate the differences in survival associated with these two treatments for advanced HCC.
Recent trials have compared TARE with sorafenib for the treatment of advanced HCC and found that both treatments had similar efficacy with a better toxicity profile in the TARE group [1,18,19]. These studies imply that TARE may improve survival over NOT given that sorafenib has already been proven to improve survival in patients with advanced HCC. Our study confirmed this finding, showing a clear survival advantage for TARE over the NOT group in the unmatched pooled cohort (9 months 95% CI: 8–11 months vs 2 months 95% CI: 2–3 months); however, this initial analysis was compromised due to inequalities between the comparison groups. Comparing patient characteristics in the unmatched SEER population revealed that patients treated with NOT had worse tumor staging, worse tumor grade and more patients with metastatic disease. In short, this group had more advanced disease than the TARE group. Tumor staging and tumor grade were found to be independent prognostic factors on regression analysis; therefore, the imbalance of the groups would be expected to skew the data favoring TARE independent of the effects of therapy. This necessitated the propensity matching we performed to ensure that the groups are evenly distributed and homogenous. After the matching process, there were no differences in the background variables of each group.
After creating homogenous groups, the survival advantage of TARE persisted with 9 months OS for TARE and 4 months for NOT. Moreover, Cox regression analysis revealed that treatment type was an independent prognostic factor. Given the possibility that the statistical assessment may be vulnerable when there are a high number of noncancer related deaths, we performed an analysis looking at LCSS in the unmatched and matched cohorts. Again, there was clear LCSS advantage for TARE over NOT in both cohorts. The constellation of findings confirms the usefulness of TARE for the treatment of advanced HCC.
Our study performed a propensity match comparing the TARE treatment against NOT and further supports the survival benefit of TARE (HR: 1.79 [95%CI: 1.63–1.96] in the unmatched and 1.64 [95%CI: 1.4–1.93] in the matched pool). Our results somewhat contradict those found by Gramenzi et al. who performed a propensity matched analysis of TARE patients against matched patients who instead received the multi-tyrosine kinase inhibitor drug sorafenib [19]. Through their univariate analysis, they found a nonstatistically significant difference between the survival probabilities of these two treatment modalities [19]. Because our results do not further define the NOT group, further refinement of our propensity matched control will be needed to compare results between these studies.
Naturally, the use of the SEER database has its own limitations. First, specific variables obtained from the SEER database were given in less than ideal formats or missing completely. For example, fibrosis and AFP are important prognostic variables that can be categorized continuously; however, in the SEER database, they are presented as categorical variables. Liver fibrosis is provided only as a binary value, with ‘yes’ indicating cirrhosis or severe fibrosis. In addition, overall performance status and liver function are not only necessary for calculating BCLC liver stage score, but also are known prognostic factors in HCC survival; however, there is no performance status and liver function status in the SEER database, hence the BCLC stage cannot be determined from SEER data. Nevertheless, it is in the realm of possibility that in the advanced stage HCC setting, these variables are distributed at random and are unlikely to be statistically disastrous. Second, there is limited information regarding a patient’s systemic chemotherapy or immunotherapy treatment in the SEER database. Therefore the impact of these therapies, including sorafenib, cannot be quantified. The SEER-Medicare linked data could overcome some of these aforementioned issues, but these introduce additional limitations. These limitations include limited analysis to Medicare-age patients, limiting overall generalizability and the number of subjects. The choice for this study was to aim for generalizability by using the nonlinked data, including as many patients as possible, and providing results more applicable to the general population. Additionally, because of database limitations, this study did not assess differences in patients treated both with TARE and sorafenib or chemotherapy to those treated by TARE alone. Given the previously mentioned data, which show a trend toward improved survival in patients treated with sorafenib versus TARE alone, it would be interesting to determine if the benefit observed in this study could be attributable to sorafenib or chemotherapy, or if TARE with these therapies provides any additional survival benefit.
Conclusion
HCC continues to be a treatment dilemma as the optimal treatment for patients in a variety of stages continues to be studied. The results of this study demonstrate that TARE improves the survival of advanced stage HCC patients compared with those patients who were treated with NOT. This difference was found both in the unmatched and in the propensity-matched patient population, which further supports other studies that are investigating the use of TARE as a treatment option for patients with advanced stage HCC. While these findings are very convincing, studies that are able to quantify the type and amount of chemotherapy administration used in a similar patient population and prospective studies are still needed to confirm these observations.
Advanced hepatocellular carcinoma patients from the Surveillance, Epidemiology and End Results database were compared in regard to overall survival and liver cancer-specific survival (LCSS) to determine the comparative effectiveness of either transarterial radioembolization (TARE) or nonoperative/interventional treatment (NOT).
The TARE cohort showed a significant survival advantage over NOT in the unmatched study population.
The NOT cohort demonstrated a lower probability of LCSS compared with the TARE group.
Propensity score matching, a method used to eliminate differences in the study population, was conducted with the 367 TARE patients.
In the matched cohort, TARE still outperformed NOT in both survival and LCSS.
Comparative analysis of the demographics and survivals of radioactive implants versus radioisotopes was conducted.
Fibrosis was the only metric significantly different between these two study populations.
Survival and LCSS were statistically insignificant between these two study populations.
Financial & competing interests disclosure
This research was supported by institutional funding and not any external grants. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This study was exempt from institutional review board approval and was completed in accordance with the National Cancer Institute SEER user agreement.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Luo W, Zhang Y, He G et al. Effects of radiofrequency ablation versus other ablating techniques on hepatocellular carcinomas: a systematic review and meta-analysis. World J. Surg. Oncol. 15(1), 126 (2017).
•• The Phase III prospective comparisons of transarterial radioembolization (TARE) and sorafenib provide a look into the efficacies of various tumoricidal treatments for advanced hepatocellular carcinoma patients.
2.
Vigano L, Conci S, Cescon M et al. Liver resection for hepatocellular carcinoma in patients with metabolic syndrome: a multicenter matched analysis with HCV-related HCC. J. Hepatol. 63(1), 93–101 (2015).
3.
Sharma P, Balan V, Hernandez JL et al. Liver transplantation for hepatocellular carcinoma: the MELD impact. Liver Transpl. 10(1), 36–41 (2004).
4.
Mazzaferro V, Regalia E, Doci R et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 334(11), 693–699 (1996).
5.
Belghiti J, Kianmanesh R. Surgical treatment of hepatocellular carcinoma. HPB (Oxford) 7(1), 42–49 (2005).
6.
Regimbeau JM, Abdalla EK, Vauthey JN et al. Risk factors for early death due to recurrence after liver resection for hepatocellular carcinoma: results of a multicenter study. J. Surg. Oncol. 85(1), 36–41 (2004).
7.
Eltawil KM, Berry R, Abdolell M, Molinari M. Quality of life and survival analysis of patients undergoing transarterial chemoembolization for primary hepatic malignancies: a prospective cohort study. HPB (Oxford) 14(5), 341–350 (2012).
8.
Llovet JM, Real MI, Montana X et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet 359(9319), 1734–1739 (2002).
9.
Llovet JM, Ricci S, Mazzaferro V et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 359(4), 378–390 (2008).
10.
Abdel-Rahman O, Lamarca A, Valle JW, Hubner RA. Somatostatin receptor expression in hepatocellular carcinoma: prognostic and therapeutic considerations. Endocr. Relat. Cancer 21(6), R485–R493 (2014).
11.
Biederman DM, Titano JJ, Tabori NE et al. Outcomes of radioembolization in the treatment of hepatocellular carcinoma with portal vein invasion: resin versus glass microspheres. J. Vasc. Interv. Radiol. 27(6), 812.e2–821.e2 (2016).
12.
Adhoute X, Penaranda G, Raoul JL et al. Barcelona clinic liver cancer nomogram and others staging/scoring systems in a French hepatocellular carcinoma cohort. World J. Gastroenterol. 23(14), 2545–2555 (2017).
13.
Camma C, Schepis F, Orlando A et al. Transarterial chemoembolization for unresectable hepatocellular carcinoma: meta-analysis of randomized controlled trials. Radiology 224(1), 47–54 (2002).
14.
Sacco R, Conte C, Tumino E et al. Transarterial radioembolization for hepatocellular carcinoma: a review. J. Hepatocell. Carcinoma 3, 25–29 (2016).
15.
Mazzaferro V, Sposito C, Bhoori S et al. Yttrium-90 radioembolization for intermediate-advanced hepatocellular carcinoma: a Phase II study. Hepatology 57(5), 1826–1837 (2013).
16.
Rognoni C, Ciani O, Sommariva S et al. Trans-arterial radioembolization in intermediate-advanced hepatocellular carcinoma: systematic review and meta-analyses. Oncotarget 7(44), 72343–72355 (2016).
• Provides the curious reader with a compilation analysis of survivals from a variety of radioembolization efficacy studies and may help to point to more specific case-based scenarios.
17.
Liver EaFTSOT. SIRT is better tolerated than sorafenib, but doesn't increase overall survival in HCC. Eurekalert! (2017). www.eurekalert.org/pub_releases/2017-04/eaft-sib041217.php
18.
Chow PHW, Gandhi M. Phase III multi-centre open-label randomized controlled trial of selective internal radiation therapy (SIRT) versus sorafenib in locally advanced hepatocellular carcinoma: The SIRveNIB study. J. Clin. Oncol. 35(Suppl. 15), 4002 (2017).
•• The Phase III prospective comparisons of TARE and sorafenib provide a look into the efficacies of various tumoricidal treatments for advanced hepatocellular carcinoma patients.
19.
Gramenzi A, Golfieri R, Mosconi C et al. Yttrium-90 radioembolization vs sorafenib for intermediate-locally advanced hepatocellular carcinoma: a cohort study with propensity score analysis. Liver Int. 35(3), 1036–1047 (2015).
• Introduces a propensity matched investigation of TARE versus sorafenib for those who are curious about a greater separation between nonoperative/interventional treatment and sorafenib receiving patients.
20.
National Cancer Institute. Overview of the SEER program (2017). https://seer.cancer.gov/about/overview.html
21.
Adamo M, Dickie L, Ruhl J. SEER Program Coding and Staging Manual. National Cancer Institute, MD, USA (2016). www.eurekalert.org/pub_releases/2017-04/eaft-sib041217.php
•• Investigation into the Surveillance, Epidemiology and End Results manual for coding will help the curious reader further understand the methodology and aim of this study.
22.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46(3), 399–424 (2011).
•• Propensity matching as an effective tool for mimicking randomized control trials in retrospective analysis studies.
23.
Coca-Perraillon M. Local and global optimal propensity score matching. SAS Global forum paper, 185–2007 (2007). www2.sas.com/proceedings/forum2007/185-2007.pdf
24.
Abdelfattah MR, Al-Sebayel M, Broering D, Alsuhaibani H. Radioembolization using yttrium-90 microspheres as bridging and downstaging treatment for unresectable hepatocellular carcinoma before liver transplantation: initial single-center experience. Transplant Proc. 47(2), 408–411 (2015).
25.
Kulik LM, Carr BI, Mulcahy MF et al. Safety and efficacy of 90Y radiotherapy for hepatocellular carcinoma with and without portal vein thrombosis. Hepatology 47(1), 71–81 (2008).
26.
Sangro B, Carpanese L, Cianni R et al. Survival after yttrium-90 resin microsphere radioembolization of hepatocellular carcinoma across Barcelona clinic liver cancer stages: a European evaluation. Hepatology 54(3), 868–878 (2011).
27.
Oladeru OT, Miccio JA, Yang J, Xue Y, Ryu S, Stessin AM. Conformal external beam radiation or selective internal radiation therapy – a comparison of treatment outcomes for hepatocellular carcinoma. J. Gastrointest. Oncol. 7(3), 433–440 (2016).
28.
Gray SH, White JA, Li P et al. A SEER database analysis of the survival advantage of transarterial chemoembolization for hepatocellular carcinoma: an underutilized therapy. J. Vasc. Interv. Radiol. 28(2), 231.e2–237.e2 (2017).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 14 August 2017
Accepted: 27 October 2017
Published online: 19 March 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Survival comparison of hepatocellular carcinoma patients treated with radioembolization versus nonoperative/interventional treatment. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0064
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yufeng Zhu, Qianru He, Ming Qi, Exosomal circPTPRK promotes angiogenesis after radiofrequency ablation in hepatocellular carcinoma, Experimental Biology and Medicine, 10.3389/ebm.2024.10084, 249, (2024).
- 琪栋 陈, An Analysis of the Factors Influencing Disease-Free and Overall Survival Time after Curative Resection for Hepatocellular Carcinoma, Advances in Clinical Medicine, 10.12677/acm.2024.1441291, 14, 04, (2267-2277), (2024).
- Yufeng Zhang, Xia He, Wenjie Guo, Li Sun, Chang Guo, Yong Feng, CT‐guided liver beacon transponder implantation, Precision Medical Sciences, 10.1002/prm2.12033, 10, 1, (42-50), (2021).