Patient and provider perspectives on shared decision making: a systematic review of the peer-reviewed literature
Abstract
For comparative effectiveness research to be effective, patients and providers must collaborate in shared decision making (SDM) to make evidence-based clinical decisions that align with patient preferences. We conducted a systematic review to examine patient and provider attitudes toward and engagement in SDM in the USA. Searches in PubMed and PsycINFO identified 1585 articles published between July 2006 and December 2016, of which 290 were screened in for coding and analysis. We found that patients and providers have generally positive attitudes toward SDM, but actual engagement in SDM behavior is lagging. Translation of positive attitudes into behavior could be achieved through policies that support key SDM processes of sharing evidence, considering patient preferences and discussing the relative advantages of different clinical options.
Comparative effectiveness research (CER) or patient-centered outcomes research (PCOR) is intended to give patients and providers the information they need to make evidence-based, patient-centered clinical decisions at the point of care [1–3]. Absent patient engagement in these decisions, however the information itself, cannot help patients make an informed decision that would, from their perspective, improve their health [4,5]. Only if patients join providers in the process via shared decision making (SDM) – a process involving active engagement of patients and presentation by providers of information associated with viable care options, where applicable – can CER/PCOR lead to better healthcare quality and efficiency [6]. SDM can also ensure that clinical decisions align with patient preferences and values, increase patient knowledge and reduce patient anxiety [6]. Alignment of clinical decisions with patient preferences is particularly important, given that most decisions involve consideration of options that vary as to benefits and risks, and patients have different preferences regarding those benefits and risks [5].
Patients are more likely to engage if they know that providers will consider their feelings and opinions, especially regarding more serious clinical decisions [5,7]. Patients are also more likely to participate in SDM if they feel they have the information and support they need to make an informed decision [5]. For instance, patient decision aids are tools that support SDM by providing patients with evidence regarding clinical options and clarifying the preference-sensitive nature of the decision [5].
Providers are more likely to facilitate SDM when they feel a patient takes an interest in his or her care, and when they are comfortable discussing emotionally charged issues with a patient, acknowledging their own uncertainty and relinquishing their role as sole decision makers [5,7]. Provider attitudes regarding SDM in a given context also vary based on the specific clinical condition and treatment decision [8].
For this reason, and because to our knowledge there is only one review on this topic which focuses only on providers and is narrow in focus [8], we conducted a systematic review of the peer-reviewed literature to describe current patient and provider perspectives regarding the SDM process. We examined attitudes toward and engagement in SDM, changes in attitudes or engagement due to an intervention with a patient decision aid intended to promote SDM, and treatment-related patient preferences and information addressed during clinical encounters.
Methods
Search methodology
We conducted a systematic review of the peer-reviewed literature on patients’ and providers’ perspectives on SDM. Table 1 summarizes our search strategy for PubMed and PsycINFO. A potential limitation to our search is that we did not search the CINAHL database, which may have included relevant studies not included in PubMed or PsycINFO.
| Category | ID | Search terms |
|---|---|---|
| Patients and providers | 1 | Consumer* OR patient OR patients OR physician* OR provider* OR doctor* OR nurse* OR practitioner* OR public [‘All Fields’ for PubMed; ‘Abstract Only’ for PsycINFO] |
| Data collection | 2 | Survey* OR interview* OR focus group* OR questionnaire* OR poll OR polls [‘All Fields’ for PubMed; ‘Abstract Only’ for PsycINFO] |
| Shared/informed decision making | 3 | Informed decision making OR shared decision making [‘All Fields’] |
| Perspectives | 4 | Opinion(s) OR attitude(s) OR perception(s) OR reaction(s) OR concern(s) OR belief(s) OR value(s) OR feeling(s) [‘All Fields’ for PubMed; ‘Abstract Only’ for PsycINFO] |
| Combination of terms | 5 | (1 AND 2 AND 3 AND 4) |
We designed a targeted search strategy to obtain articles with findings from surveys, interviews, and focus groups with patients and providers (we included only papers that reported results of primary studies carried out by the authors). We limited our search to articles written in English and published within the period from July 2006 through December 2016 (We conducted our original search and analysis for the 5-year period from July 2006 through June 2011, and then extended that period through December 2016 for the final search and analysis we present here). In addition, we limited ourselves to articles about patients and providers in the USA. We imposed this limit because, although considerable research on SDM has been conducted in other countries (especially in the UK and Australia), perspectives likely vary considerably across countries with different policy histories regarding CER use.
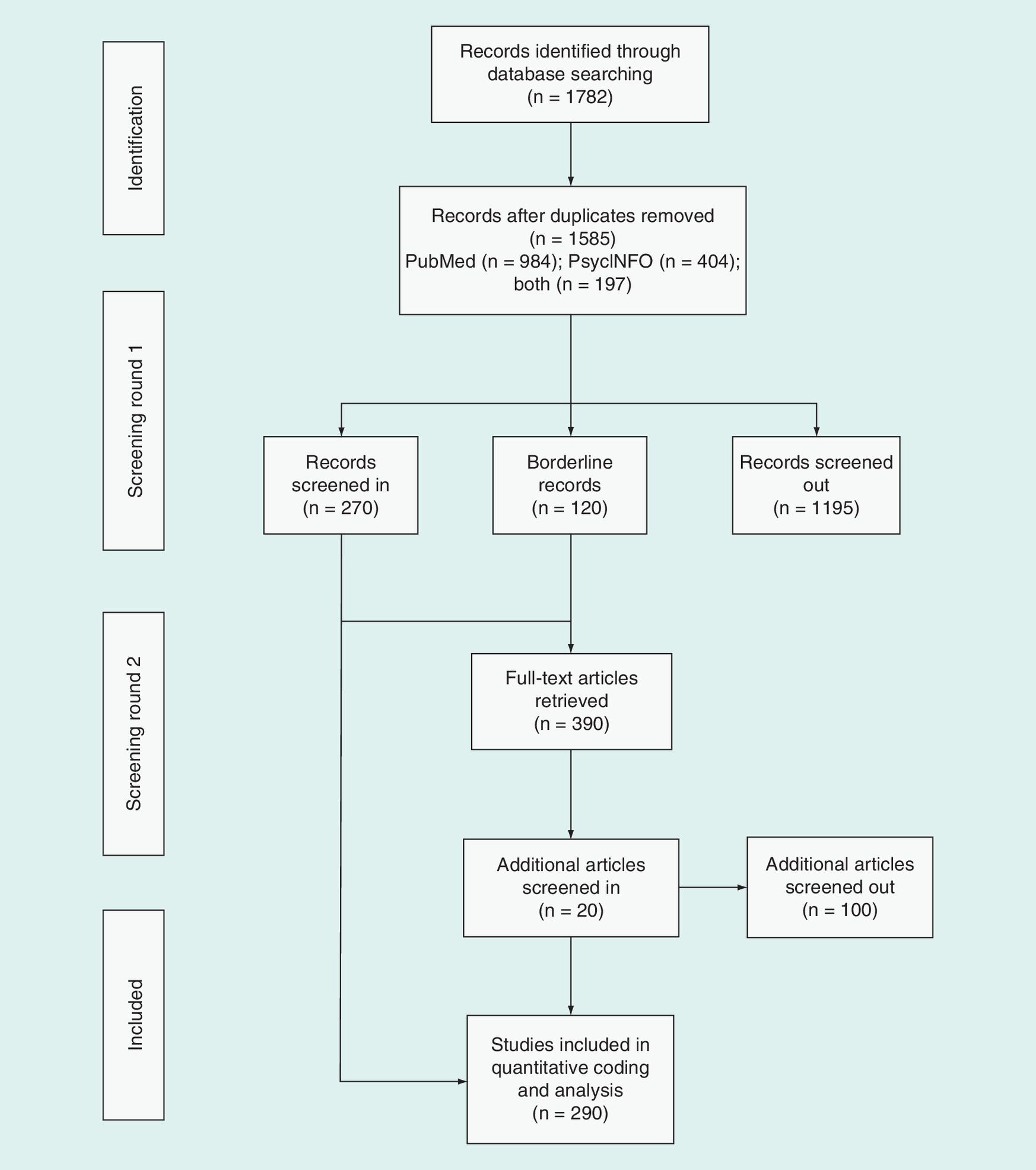
Figure 1 summarizes our screening process, which we conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [9]. Our search returned 1585 articles (984 from PubMed alone, 404 from PsycINFO alone and 197 from both). Because we designed our search strategy to be inclusive, the search returned many articles not relevant to this literature review. For this reason, we screened the abstracts of the returned articles by hand, using a two-stage process to ensure the reliability and accuracy of our screening categories. First, the second author sorted the abstracts into three categories – 270 relevant to the scope (screened in), 1195 not relevant to the scope or for which the article provided insufficient information to determine relevance (screened out) and 120 of borderline relevance. We obtained full-text articles for the 390 screened-in and borderline abstracts. Second, the first author sorted those of borderline relevance into either the screened-in or screened-out categories. Ultimately, we screened in 290 articles for coding and analysis. Please see the online-only Supplementary Appendix document for the full reference list of all studies included in the analysis.
Coding methodology
We conducted several types of coding in two rounds for the final set of 290 relevant articles.
Table 2 presents our coding categories for the first round of coding. We started by sorting the articles into mutually exclusive categories based on the population targeted by each study – patients, providers, and both patients and providers. Next, we coded the studies based on types of data collection activities (nonmutually exclusive categories), clinical focus (mutually exclusive categories) and demographic focus of the patients (nonmutually exclusive categories). We then tabulated whether the study involved used a patient decision aid as an intervention and, if so, whether the intervention occurred in a clinical setting. To ensure the reliability and accuracy of our coding categories, we used a two-stage process in which the second author conducted the coding, and the first author then reviewed it and reconciled discrepancies (of which there were very few – all minor) with the second author.
| Target population |
| Patients only |
| Providers only |
| Both patients and providers |
| Data collection activities |
| Survey |
| Focus groups |
| Interviews |
| Literature review |
| Clinical focus |
| Screening (especially colon, prostate or breast cancer screening) |
| Treatment (such as cardiac catheterization, lung transplantation, drug treatment or total knee replacement) |
| Other (such as a general study focused on attitudes or behaviors regarding shared decision making) |
| Demographic focus |
| No specific focus (on a demographic group or comparison among demographic groups) |
| Racial, ethnic or socioeconomic focus |
| Gender focus |
| Involved decision aid intervention |
| Involved clinical practice intervention (most typically use of a patient decision aid at the point of care, but also phone counseling with patients at home or mailing decision aid materials to patients at home) |
Next, we created a coding scheme and conducted coding to classify the study outcome variables and findings. This coding was more complex than that for the first round, so we refined it iteratively to ensure the reliability and accuracy of the coding scheme. We did not find adequate code definitions in existing literature; therefore, our codes are empirically driven. The first author developed the initial set of codes based on a sample of 25 patient-focused studies and 25 provider-focused studies; the second author then conducted the initial coding and suggested revisions to the coding scheme, the first author reviewed and finalized the coding scheme, and the second and third authors finalized the coding.
Table 3 presents the final coding definitions for the two outcomes codes – attitudes toward SDM and engagement in SDM behavior (nonmutually exclusive categories). For all studies, we examined attitudes toward SDM (coded as ‘positive’ vs ‘negative’ or ‘passive’) and engagement in SDM behavior (coded as ‘higher’ vs ‘lower’ than typical engagement). For studies that involved a decision aid intervention, we conducted the coding on baseline (preintervention) attitudes and behavior. For those studies, we also examined changes in attitudes (coded as ‘improved’ vs ‘no change’) and engagement (coded as ‘increase’ vs ‘no change’). Table 3 also presents definitions for the two codes used to identify articles reporting on treatment-related patient preferences and information.
| Code | Definition |
|---|---|
| Attitudes toward SDM | Patient or provider preferences regarding the clinical SDM process, including perceived quality of patient–provider communication, desire for patient to engage in SDM vs autonomous decision making or delegation to the provider, satisfaction with the decision-making process, perceived self-efficacy regarding SDM, attitude toward information seeking and preference for information |
| Engagement in SDM behavior | Patient- or provider-reported use of SDM processes, including discussion of treatment options, discussion of patient preferences and goals, and understanding of conditions and relative pros and cons of treatment options |
| Reported on treatment-related patient preferences | Patient or provider reports of patients and providers addressing patient preferences for treatment-related decisions during clinical encounters |
| Reported on treatment-related information | Patient or provider reports of patients and providers addressing information relevant to treatments during clinical encounters |
SDM: Shared decision making.
For those articles that addressed treatment-related patient preferences and information, we conducted a qualitative analysis. The second and third authors reviewed the results and discussion sections of these articles to identify potential trends across study findings, and summarized several themes related to SDM that were commonly reported across several articles. The first author reviewed the summary and finalized it.
Results
Study characteristics
Table 4 shows the study characteristics as well as findings on patient and provider views of SDM. The most common data collection method was a survey (61% of the studies), followed by interviews (34%) and focus groups (14%). The most common clinical focus was treatment (62%), such as cardiac catheterization, lung transplant, drug treatment or total knee replacement. Most of the remaining studies focused on screening (24%), and more specifically on colon, prostate or breast cancer screening.
| Coding category | Studies focusing on patients | Studies focusing on providers | Studies focusing jointly on patients and providers |
|---|---|---|---|
| Total number of articles | 186 | 54 | 50 |
| Data collection activities | |||
| Survey | 115 | 33 | 29 |
| Focus groups | 26 | 6 | 10 |
| Interviews | 67 | 20 | 13 |
| Literature review | 0 | 0 | 3 |
| Clinical focus | |||
| Screening | 53 | 11 | 7 |
| Treatment | 122 | 21 | 37 |
| Other | 21 | 6 | 5 |
| Demographic focus (of patients) | |||
| No specific focus | 107 | NA | 38 |
| Racial, ethnic or SES focus | 38 | NA | 2 |
| Gender focus | 51 | NA | 7 |
| Involved patient decision aid intervention | 31 | 13 | 10 |
| Involved clinical practice intervention | 15 | NA | 5 |
| Outcome variable measured | |||
| Attitudes toward SDM | 109 | 34 | 38 |
| Engagement in SDM behavior | 124 | 31 | 33 |
| Findings | |||
| Positive attitudes | 74 | 30 | 34 |
| Negative or passive attitudes | 39 | 17 | 17 |
| Improved attitudes | 11 | 0 | 2 |
| No change in attitudes | 5 | 0 | 2 |
| Higher engagement | 57 | 12 | 19 |
| Lower engagement | 79 | 27 | 23 |
| Increase in engagement | 18 | 2 | 1 |
| No change in engagement | 9 | 0 | 1 |
| Reporting on treatment-related patient preferences and information | |||
| Reported on treatment-related patient preferences | 55 | 12 | 24 |
| Reported on treatment-related information | 63 | 18 | 26 |
Coding categories are not mutually exclusive.
NA: Not applicable; SDM: Shared decision making; SES: Socioeconomic status.
Most of the studies involving patients (58%) did not target a specific demographic group or comparisons between such groups. However, a few focused on race, ethnicity or socioeconomic status (20%), or gender (27%).
41 of the studies that included patients (either exclusively or jointly with providers) used a patient decision aid as an intervention (17%). 20 were conducted in a clinical practice setting in which the aid was typically used at the point of care. In some cases, patients were counseled at home by phone, or patient decision aid materials were mailed to them. The other 21 studies were conducted in a research setting.
Patient & provider perspectives on SDM
The proportions of studies examining attitudes toward SDM (62%) and engagement in SDM behavior (65%) were similar. For all studies, we examined attitudes toward SDM (coded as positive vs negative or passive) and engagement in SDM behavior (coded as higher or lower). For studies that reported findings on the use of a patient decision aid to promote SDM, we also examined changes in attitudes (coded as improved or no change) and changes in engagement (coded as increase or no change). The studies that focused on both patients and providers generally reported synthesized outcomes, such as patient–provider communication or patient–provider agreement in their attitudes toward SDM, the quality of the decision or satisfaction with the decision-making process.
Most of the studies (186; 64%) focused on patients, and more found positive (40%) rather than negative or passive (21%) attitudes toward SDM. However, more of them also found lower (42%) rather than higher engagement (31%) in SDM behavior.
54 studies (19%) focused on providers. Like the patient studies, more of them found a positive (56%) rather than a negative or passive (31%) attitude toward SDM. More also found lower (50%) rather than higher (22%) engagement in SDM behavior.
50 studies (17%) focused on both patients and providers. Again, more of them found positive (68%) rather than negative or passive (34%) attitudes toward SDM, and more found lower (46%) rather than higher engagement (38%) in SDM behavior.
20 studies (7%) examined changes in attitudes toward SDM resulting from an intervention. 13 of them (65%) found improved attitudes. However, these findings should be interpreted with caution because few studies examined changes in attitudes. 31 studies (11%) examined changes in engagement in SDM behavior resulting from an intervention. 21 of them (66%) found increases in engagement.
Treatment-related patient preferences & information
We assessed which studies reported on treatment-related patient preferences and information addressed during clinical encounters. Of the 290 studies screened in for coding and analysis, 91 (31%) reported on treatment-related patient preferences and 107 (37%) reported on treatment-related information. Of the articles that reported on patient preferences, 55 (60%) focused on patients, 12 (13%) reported on providers and 24 (26%) reported on both patients and providers. Of the articles that reported on information, 63 (59%) focused on patients, 18 (17%) on providers and 26 (24%) on both.
We then conducted a qualitative analysis of all of these articles to identify potential trends across study findings, noting commonly reported themes related to SDM. Because 82 studies reported on both treatment-related patient preferences and information, the total pool for the qualitative analysis consisted of 116 articles. We found that the types of treatment-related information exchanged and whether treatment-related patient preferences were addressed were influenced by a variety of factors, including patient condition, tests or procedures being considered and patient demographics. For example, Fowler et al. [10] found that decision-making processes for back or knee replacement surgery included a more balanced discussion of pros and cons compared with discussions about hip or cataract surgery.
Addressing pros & cons of treatment or screening
Researchers found that pros of tests or treatments are often more likely to be discussed than cons, and often providers do not ask patients whether they want a test or treatment that may not be necessary. Via a survey of a national sample of adults 40 years or older, Fowler et al. [10] found that for each of ten common tests, medications and procedures, “patients reported more discussion of the pros than of the cons”. Similarly, Hoffman et al. [11] found that “most discussion with providers addressed pros of [breast, colorectal and prostate cancer] screening…but few similarly addressed cons”. We found similar findings elsewhere. For example, via a survey of 412 patients who received an implantable cardioverter defibrillator, Green et al. [12] found that some respondents reported not being told of the option not to get an implantable cardioverter defibrillator, and/or did not remember being asked if they wanted one. Similarly, researchers surveying patients who underwent vascular procedures found that only about half of respondents indicated they were offered a choice [13].
Patient demographics & decision-making processes
Across varied clinical settings, patient demographics such as race and gender also have been shown to have a bearing on decision-making processes and related outcomes. Among women with early stage, nonmetastatic breast cancer considering adjuvant chemotherapy or hormone therapy, Shelton et al. [14] found that black patients had the lowest ratings for communication with their oncologists and involvement in the decision-making process. Similarly, among male veterans receiving outpatient care at a Veterans Affairs Medical Center in Miami, whites expressed more satisfaction with their current role in decision making than did African Americans [15]. Researchers have also demonstrated that gender may be an important factor in SDM processes and outcomes. In their analyses of results from a national survey of adults who made cancer screening decisions, Hoffman et al. [11] found that among adults who made a colorectal cancer screening decision, most men reported that their provider explained the patient could choose whether to have the test and asked if the participant wanted the test, compared with smaller majorities of women. Similarly, most men making a prostate cancer screening decision reported the provider asked if the participant wanted the test versus a smaller majority of women making a breast cancer screening decision. On the other hand, results from a survey of patients with depression and providers treating patients with depression indicated ratings of SDM were more likely to be higher if the survey respondent was female [16].
Patient knowledge of tests & treatments
Adding to the complexity of SDM processes and potential factors affecting them is patient knowledge of tests and treatments. Analyzing results from a sample drawn from a national survey of adults making decisions about ten common cancer screenings and blood pressure or cholesterol medications, Fairfield et al. [17] found overall knowledge scores were low across the study sample (adults 40 years or older); respondents also reported poor decision processes. Via a study of 1041 men deciding whether to undergo prostate-specific antigen testing after viewing a decision aid, researchers found that men with higher knowledge were ‘more likely to lean against’ screening (the US Preventive Services Task Force recommends against routine prostate-specific antigen testing) and ‘less likely to be unsure’ about their decision [18].
Patient perceptions of disease risk & mortality
Patient perceptions of disease risk, disease-related mortality risk and effectiveness of treatments or screenings have also been found to influence exchange of treatment-related information and patient preferences. Hoffman et al. found, via a survey of adults facing cancer screening decisions, that patient perception of being at average/high risk for cancer was a factor highly associated with decision confidence. However, in another study of adults faced with the same decisions, they found most participants greatly overestimated risks of a cancer diagnosis and mortality [19].
Provider knowledge & beliefs
Unsurprisingly, given that providers are the most important and often most trusted source of information for patients making medical decisions (e.g., [13,19,20]), provider knowledge and beliefs about the efficacy of tests and treatments as well as their perceptions of patient preferences also influence the scope of SDM in clinical practice. Volk et al. [21] found that “compared with physicians who ordered prostate cancer screening without discussion, physicians who discussed harms and benefits with patients and then let them decide were more likely to endorse beliefs that scientific evidence does not support screening, that patients should be told about the lack of evidence, and that patients have a right to know the limitations of screening”. The researchers also found that such physicians “were also less likely to endorse the belief that there was no need to educate patients because they wanted to be screened” [21]. Additionally, physician demographics such as specialty (e.g., family physicians vs internists) and physicians’ beliefs about their patients’ aversion to ambiguous scientific information predicted attitudes toward communicating such ambiguity [22]. When physicians felt their patients would respond negatively to ambiguous information, Portnoy et al. [22] found that such physicians ‘were more likely to think that they should decide what is best for their patients’.
Given the number and scope of patient and provider factors potentially clouding decision-making processes, it is important to note that our review includes studies indicating that patients and providers utilizing SDM processes have the potential to improve patient knowledge regarding the decisions they make as well as patient satisfaction with confidence in both the decision-making process and decisions made. Bozic et al. [23] found significantly more patients who were assigned to an SDM intervention reached an informed decision compared with a control group, and also ‘reported higher confidence in knowing what to ask their doctor’. Fowler et al. [24] found that patients with more knowledge and those who reported more involvement in decision making more frequently had their decision match their stated goals and concerns. Further, patients whose stated goals were met “reported more confidence in their decisions and feeling more positively about how the treatment turned out” [24].
Discussion
We conducted a systematic review of the peer-reviewed literature to describe current patient and provider perspectives regarding the SDM process. Our primary analysis examined attitudes toward and engagement in SDM, as well as changes in attitudes or engagement as a result of an intervention with a patient decision aid intended to promote SDM. Attitudes toward SDM tended to be positive, whereas actual engagement in SDM tended to be lower. Future research should examine barriers to engagement when attitudes are positive – separately for patients and providers – to better inform the development of interventions or policies to address those barriers. Among studies that examined changes resulting from an intervention, most found improved attitudes and increased engagement. Future research should examine the characteristics of successful interventions.
We also conducted a qualitative analysis of studies that reported on treatment-related patient preferences and information addressed during clinical encounters. In general, pros of tests or treatments were discussed more often than cons, and providers often did not ask patients whether they wanted a potentially unnecessary test or treatment. However, the types of treatment-related information exchanged and whether patient preferences were addressed were influenced by a variety of factors, including patient condition, tests or procedures being considered, patient demographics, patient knowledge and perceptions of treatments and disease-related risk and mortality, and provider knowledge and beliefs about treatment efficacy and patient preferences. Future research should examine these factors to inform the development of interventions to improve provider communication with patients regarding the cons of tests or treatments and more effectively elicit and consider patient preferences and values.
Because we conducted a systematic review that included both quantitative (surveys) and qualitative (interviews and focus groups) studies, we did not conduct a meta-analysis, which would have permitted weighting by study quality. Therefore, a potential limitation of our review is that our results may include lower quality studies, as we did not conduct a systematic assessment of study quality. However, our rigorous screening methodology ensured that all included studies could be coded using our rigorous coding methodology, which likely screened out the lowest quality studies, as those would have been screened out.
Conclusion
The findings from this literature review are promising. They suggest that patients and providers are already positively inclined toward SDM. However, the findings also suggest that actual engagement in SDM behavior is still lagging behind attitudes toward the process. If CER/PCOR is to ensure that clinical decisions at the point of care are evidence based and patient centered, thus promoting healthcare quality and efficiency, the positive attitudes of patients and providers must be translated into behavior. This result could be achieved through interventions that promote SDM and policies that support key SDM processes of sharing evidence, considering patient preferences and values, and discussing the relative advantages of different clinical options.
Future perspective
Over the past 20 years, there has been an increasing emphasis on patient-centered care, including SDM. This trend has been reflected in both research and implementation, and has accelerated in recent years. Funders such as the Patient-Centered Outcomes Research Institute (PCORI) and professional organizations such as the Society for Medical Decision Making (SMDM) have promoted research on SDM, ranging from better understanding of patient and provider decision making to development and evaluation of patient decision aids to assessment of patient preferences. The Agency for Healthcare Research and Quality (AHRQ) has developed a broad range of evidence-based tools, curricula, and other resources to support SDM. Through its Center for Medicare and Medicaid Innovation (CMMI), the Centers for Medicare & Medicaid Services (CMS) has been promoting implementation of SDM through various initiatives – most recently through development of the Beneficiary Engagement and Incentives Models initiative to be launched in early 2018. We anticipate that this accelerating trend will continue over the next 5 years, with a shift in focus as the field matures toward evidence-based refinement and evaluation of interventions and other initiatives that promote SDM.
For comparative effectiveness research/patient-centered outcomes research to be effective, patients and providers must collaborate in shared decision making (SDM) to make evidence-based clinical decisions that also align with patient preferences and values.
Therefore, we conducted a systematic review of the peer-reviewed literature to examine patient and provider attitudes toward and engagement in SDM.
Searches in PubMed and PsycINFO identified 1585 articles published between July 2006 and December 2016, of which we screened in 290 for coding and analysis.
We found that patients and providers have generally positive attitudes toward SDM, but actual engagement in SDM behavior is lagging. Among studies that examined changes resulting from an intervention to promote SDM, most found improved attitudes and increased engagement.
During clinical encounters, pros of tests or treatments were discussed more often than cons, and both the types of treatment-related information exchanged and whether treatment-related patient preferences were addressed were influenced by a variety of factors.
Translation of positive attitudes into behavior could be achieved through interventions that promote SDM and policies that support key SDM processes of sharing evidence, considering patient preferences and discussing the relative advantages of different clinical options.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Financial & competing interests disclosure
The research that contributed to the content of this article was conducted by Mathematica Policy Research. The views expressed are those of the authors. The authors take full responsibility for the accuracy of material presented herein. We are grateful to E Rich, director of Mathematica's Center on Health Care Effectiveness (CHCE), for providing CHCE support for the development of the methodology and preparation of an issue brief reporting on the initial analysis (Williams N, Fleming C. Consumer and provider perspectives on shared decision making: a systematic review of the peer-reviewed literature. Issue Brief. Mathematica Policy Research, Center on Health Care Effectiveness, Princeton, NJ [September 2011]), and for analysis of the last batch of articles retrieved. Thanks also to W Rafferty for his assistance with the library searches, and to M and J Cameron for their editing assistance. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the article.
No writing assistance was utilized in the production of this article.
Supplementary Material
File (suppl_appendix.docx)
- Download
- 88.23 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Institute of Medicine. Initial National Priorities For Comparative Effectiveness Research. National Academies Press, DC, USA (2009).
• Mandated by the American Recovery and Reinvestment Act of 2009, this report obtained input from diverse stakeholders (including patients and providers) regarding comparative effectiveness research priorities.
2.
Federal Coordinating Council for Comparative Effectiveness Research. Report to the President and the Congress. US Department of Health and Human Services, DC, USA (2009). https://osp.od.nih.gov/wp-content/uploads/FCCCER-Report-to-the-President-and-Congress-2009.pdf.
• Mandated by the American Recovery and Reinvestment Act of 2009, this report obtained input from diverse stakeholders (including patients and providers) regarding comparative effectiveness research recommendations.
3.
Rich E. Past as prologue: how comparative effectiveness research became patient-centered outcomes research. J. Comp. Eff. Res. 1(6), 475–477 (2012).
• Provides background on the definition of ‘comparative effectiveness research’ and the evolution of the term ‘patient-centered outcomes research’ to highlight the importance of ensuring that clinical decisions are patient centered, following establishment of the Patient-Centered Outcomes Institute by the Affordable Care Act of 2010.
4.
Esposito D, Chen A, Gerteis M, Lake T. Using comparative effectiveness research: information alone won't lead to successful health care reform. Mathematica Policy Research Center on Health Care Effectiveness Issue Brief no. 2 (2010).
• Policy brief highlighting opportunities to ensure that comparative effectiveness research is used at the point of care by addressing challenges in several critical areas, including patient engagement.
5.
Barry M, Edgman-Levitan S. Shared decision making – the pinnacle of patient-centered care. N. Engl. J. Med. 366(9), 780–781 (2012).
•• Highlights the importance of shared decision making (SDM) for ensuring patient-centered healthcare and provides recommendations for promotion of SDM by patients and providers.
6.
Lee EO, Emanuel E. Shared decision making to improve care and reduce costs. N. Engl. J. Med. 368(1), 6–8 (2013).
•• Highlights the importance of SDM for improving healthcare quality and reducing costs and provides recommendations for promotion of SDM by federal health programs and agencies.
7.
Gerteis M, Borck R. Shared decision-making in practice: lessons from implementation efforts. Report Submitted to the Medicare Payment Advisory Commission. Mathematica Policy Research, MA, USA (2009).
•• Summarizes lessons learned regarding facilitators and challenges of implementation of SDM at the point of care.
8.
Pollard S, Bansback N, Bryan S. Physician attitudes toward shared decision making: a systematic review. Patient Educ. Couns. 98, 1046–1057 (2015).
•• Systematic review of provider attitudes toward SDM, focusing on factors associated with variations in attitudes, including provider specialty, specific clinical condition and treatment decision, and patient ability and willingness to participate in SDM.
9.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6(7), e1000097 (2009).
10.
Fowler FJ, Gerstein BS, Barry MJ. How patient centered are medical decisions?: results of a national survey. JAMA Intern. Med. 173(13), 1215–1221 (2013).
•• Study of decision-making processes across multiple common medical conditions, finding that generally pros discussed more frequently than cons, with variation across tests, medications and procedures.
11.
Hoffman RM, Elmore JG, Fairfield KM, Gerstein BS, Levin CA, Pignone MP. Lack of shared decision making in cancer screening discussions: results from a national survey. Am. J. Prev. Med. 47(3), 251–259 (2014).
•• Study finding that generally screening pros discussed more frequently than cons, providers frequently failed to note that screening was optional, and patients feeling well informed associated with confidence in screening decision.
12.
Green AR, Jenkins A, Masoudi FA et al. Decision-making experiences of patients with implantable cardioverter defibrillators. Pacing Clin. Electrophysiol. 39(10), 1061–1069 (2016).
13.
Corriere MA, Avise JA, Peterson LA et al. Exploring patient involvement in decision making for vascular procedures. J. Vasc. Surg. 62(4), 1032–1039 (2015).
14.
Shelton RC, Clarke Hillyer G, Hershman DL et al. Interpersonal influences and attitudes about adjuvant therapy treatment decisions among non-metastatic breast cancer patients: an examination of differences by age and race/ethnicity in the BQUAL Study. Breast Cancer Res. Treat. 137(3), 817–828 (2013).
15.
Rodriguez V, Andrade AD, Garcia-Retamero R et al. Health literacy, numeracy, and graphical literacy among veterans in primary care and their effect on shared decision making and trust in physicians. J. Health Commun. 18(Suppl. 1), 273–289 (2013).
16.
Barr PJ, Forcino RC, Mishra M, Blitzer R, Elwyn G. Competing priorities in treatment decision-making: a US national survey of individuals with depression and clinicians who treat depression. BMJ Open 6, e009585 (2016).
• Study showing relatively low levels of SDM among patients with depression, with somewhat higher levels for psychiatrist providers.
17.
Fairfield KM, Gerstein BS, Levin CA, Stringfellow V, Wierman HR, McNaughton-Collins M. Decisions about medication use and cancer screening across age groups in the United States. Patient Educ. Couns. 98(3), 338–343 (2015).
• Study finding generally poor decision processes and low levels of knowledge among patients making medication or screening decisions.
18.
Barry MJ, Wexler RM, Brackett CD et al. Responses to a decision aid on prostate cancer screening in primary care practices. Am. J. Prev. Med. 49(4), 520–525 (2015).
19.
Hoffman RM, Elmore JG, Pignone MP, Gerstein BS, Levin CA, Fairfield KM. Knowledge and values for cancer screening decisions: results from a national survey. Patient Educ. Couns. 99(4), 624–630 (2016).
• Study finding relatively low levels of knowledge regarding cancer screening and overestimation of lifetime risk of cancer incidence and mortality.
20.
Marrie RA, Salter AR, Tyry T, Fox RJ, Cutter GR. Preferred sources of health information in persons with multiple sclerosis: degree of trust and information sought. J. Med. Internet Res. 15(4), 210–221 (2013).
21.
Volk RJ, Linder SK, Kallen MA et al. Primary care physicians use of an informed decision-making process for prostate cancer screening. Ann. Fam. Med. 11(1), 67–74 (2013).
•• Study showing that primary care provider beliefs about screening are associated with use of SDM with patients.
22.
Portnoy DB, Han PKJ, Ferrer RA, Klein WMP, Clauser SB. Physicians’ attitudes about communicating and managing scientific uncertainty differ by perceived ambiguity aversion of their patients. Health Expect. 16(4), 362–372 (2013).
23.
Bozic KJ, Belkora J, Chan V et al. Shared decision making in patients with osteoarthritis of the hip and knee: results of a randomized controlled trial. J. Bone Joint Surg. Am. 95(18), 1633–1639 (2013).
• Randomized controlled trial showed that SDM intervention increased likelihood of patient reaching an informed decision during first visit.
24.
Fowler FJ, Gallagher PM, Drake KM, Sepucha KR. Decision dissonance: evaluating an approach to measuring the quality of surgical decision making. Jt Comm. J. Qual. Patient Saf. 39(3), 136–144 (2013).
Information & Authors
Information
Published In
Copyright
© 2017 Future Medicine Ltd.
History
Received: 19 June 2017
Accepted: 1 September 2017
Published online: 17 November 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Patient and provider perspectives on shared decision making: a systematic review of the peer-reviewed literature. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0045
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Paresh C. Giri, Jeanette Merrill‐Henry, Tiffany Rajah, Donald R. Sullivan, Udochukwu Oyoyo, Katrina Barry, Jean M. Elwing, Vijay P. Balasubramanian, Shared Decision‐Making During Pulmonary Arterial Hypertension Therapy Selection: A Patient and Clinician Survey, Pulmonary Circulation, 10.1002/pul2.70364, 16, 3, (2026).
- Michelle Huang, Violeta J. Rodríguez, Koustuv Saha, Tal August, Designing Beyond Language: Sociotechnical Barriers in AI Health Technologies for Limited English Proficiency, Proceedings of the 2026 CHI Conference on Human Factors in Computing Systems, 10.1145/3772318.3791091, (1-18), (2026).
- Preethi Kuryan, Samuel Santhosh, Bernice Theodore, Meghna Jiwanmall, Aparna Williams, Shared Decision-Making in Anesthesia in the Indian Context: A Cross-Sectional Study, Cureus, 10.7759/cureus.96552, (2025).
- David W. Chambers, Parvati Iyer, Introducing Shared Decision-Making to Dentistry, Journal of the California Dental Association, 10.1080/19424396.2025.2460676, 53, 1, (2025).
- Wenze Lu, Janelle Yorke, Yan Li, Winsome-Yuk-Yin Lam, Mengqi Li, Yule Hu, Cindy Sing Bik Ngai, Development and validation of a physician dialogic risk communication instrument scale in Chinese online medical consultations on cancer treatment risks, Humanities and Social Sciences Communications, 10.1057/s41599-025-04758-3, 12, 1, (2025).
- Florian Naye, Yannick Tousignant-Laflamme, Maxime Sasseville, Chloé Cachinho, Thomas Gérard, Karine Toupin-April, Olivia Dubois, Jean-Sébastien Paquette, Annie LeBlanc, Isabelle Gaboury, Marie-Ève Poitras, Linda C. Li, Alison M. Hoens, Marie-Dominique Poirier, France Légaré, Simon Décary, People Living with Chronic Pain Experience a High Prevalence of Decision Regret in Canada: A Pan-Canadian Online Survey, Medical Decision Making, 10.1177/0272989X251326069, 45, 4, (462-479), (2025).
- Şimal Köksal Cevher, Neşe Altınok Ersoy, Ezgi Çoşkun Yenigün, Mehmet Tuncay, Selim Turgay Arınsoy, Erdem Çankaya, Fatih Dede, The impact of “nurse‐led education” vs. “nurse‐led education plus peer support” on patients' decision for peritoneal dialysis treatment in chronic kidney disease patients, Therapeutic Apheresis and Dialysis, 10.1111/1744-9987.14248, (2024).
- Sung-Yeon Park, Daniel M. Cook, Gi Woong Yun, Max J. Coppes, Are Patient-Centered Care, Healthcare Consumerism, and Trust in Physicians Compatible?: Positioning Analysis of the Patient-Provider Relationship, Health Communication, 10.1080/10410236.2024.2408065, 40, 8, (1524-1534), (2024).
- Nancy Junger, Oliver Hirsch, Ethics of Nudging in the COVID-19 Crisis and the Necessary Return to the Principles of Shared Decision Making: A Critical Review, Cureus, 10.7759/cureus.57960, (2024).
- José Verdugo, Lory Laughter, David W. Chambers, Shared decision‐making in scaling and root planing, European Journal of Dental Education, 10.1111/eje.12935, 28, 1, (184-190), (2023).