Learning effect and diffusion of innovative medical devices: the case of transcatheter aortic valve implantation in Italy
Abstract
Aim: We investigated the diffusion of transcatheter aortic valve implantation (TAVI) since its introduction into the Italian market aimed at identifying the potential drivers of uptake and diffusion at hospital and regional levels. Materials & methods: We estimated the determinants of TAVI diffusion in Italy from 2007 to 2015 with a regression analysis based on registry data. Results: Since 2007, TAVI has shown significant diffusion rates in Italy. The diffusion is positively correlated with implanting centers’ experience and with the presence of key opinion leaders. Regional recommendations on the use of TAVI negatively influence the diffusion. Reimbursement policies do not exert a relevant impact. Conclusion: Learning effect seems to be the major driver of TAVI diffusion in Italy.

Figure 1. Average number of transcatheter aortic valve implantation implants by hospital ownership.
Average number of transcatheter aortic valve implantations per center, grouped by hospital ownership, 2007–2015.
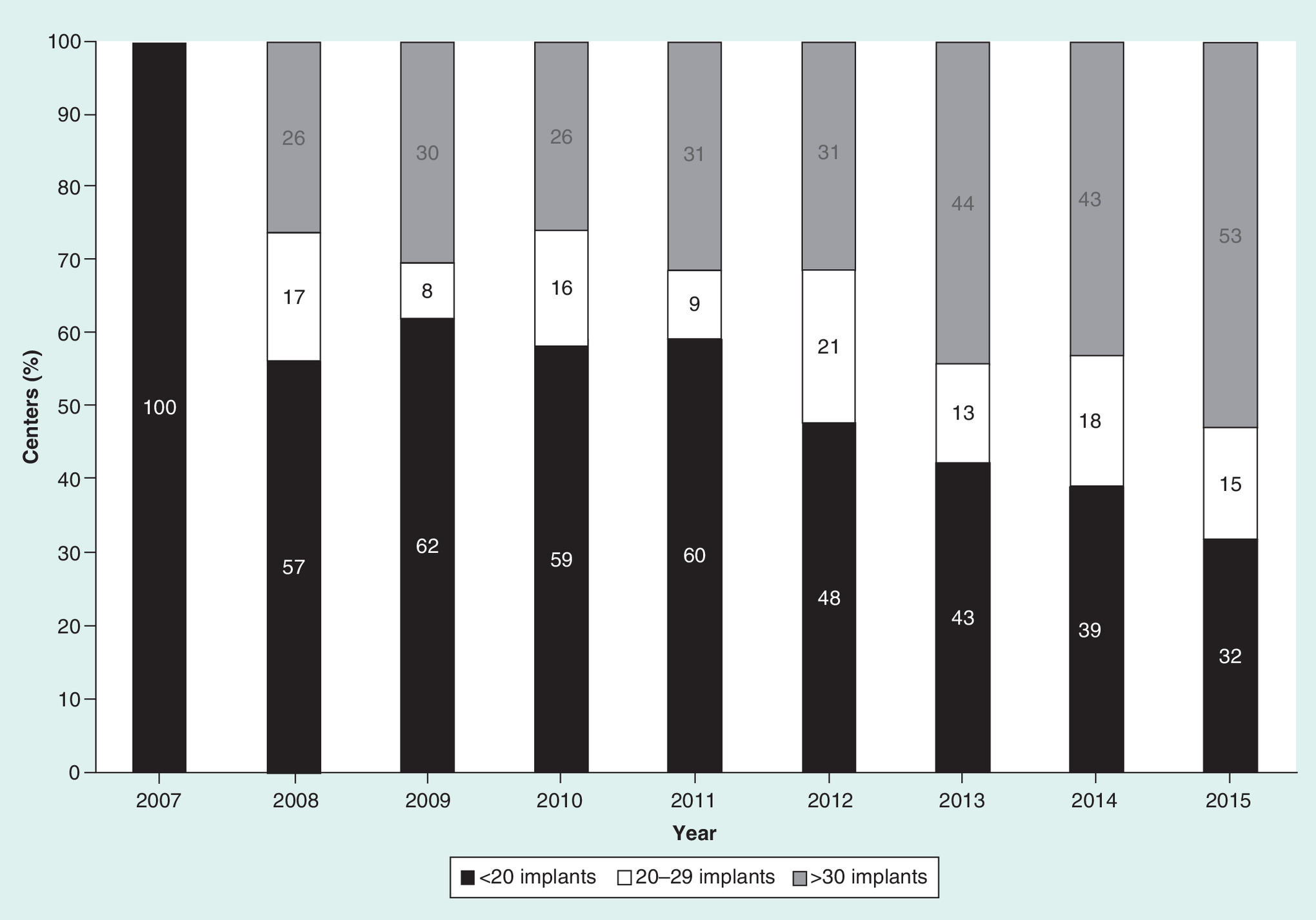
Figure 2. Distribution of transcatheter aortic valve implantation centers by number of annual implants.
Distribution of Italian transcatheter aortic valve implantation centers by average annual number of implants per center, 2007–2015.

Figure 3. Reimbursement system and transcatheter aortic valve implantation adoption across Italian Regions (2015).
Map of the number of transcatheter aortic valve implantations implanted in Italian Regions and regional reimbursement mechanisms, 2015.
†Local health authority-managed hospitals are funded by capitation, all other hospitals by basic diagnosis-related group system.
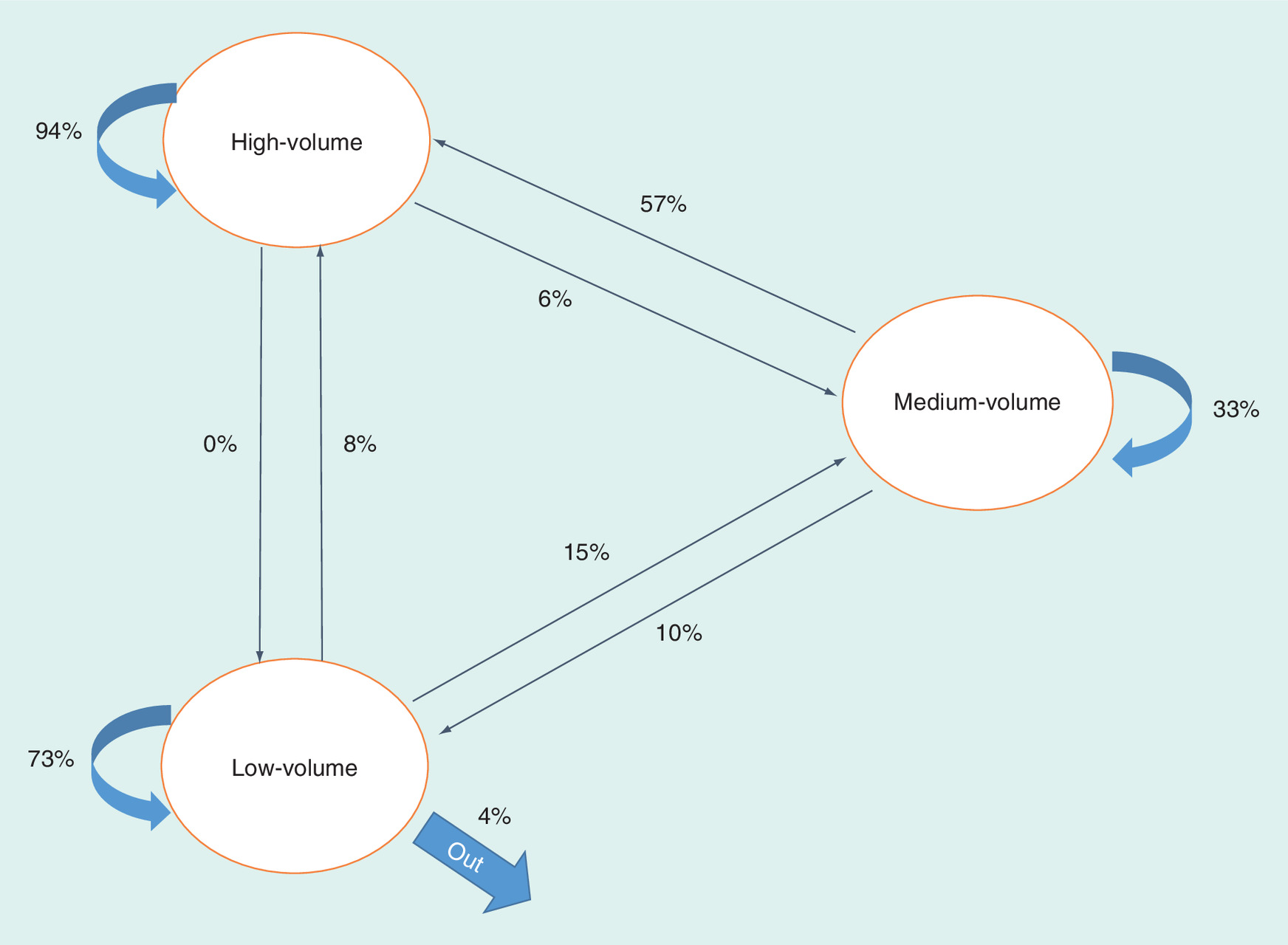
Figure 4. Probability of transition across volume classes.
Map of the probabilities of transition across volume classes.
First draft submitted: 18 November 2016; Accepted for publication: 23 January 2017; Published online: 1 February 2017
Transcatheter aortic valve implantation (TAVI) has emerged as an alternative treatment option for high-risk and inoperable patients with symptomatic severe aortic stenosis (AS) [1–3]. Approximately 190,000 high- or prohibitive-risk elderly patients with symptomatic severe AS, of which 29,600 in Italy, were candidates for TAVI in European countries in 2011, corresponding to a potential target of approximately 18,000 new patients each year [4]. With aging of the population, AS is expected to have an increasingly greater impact in the future. However, the uptake and diffusion of technological innovation in healthcare does not follow a linear trend, and many factors influence its introduction into healthcare systems [5]. The safety, effectiveness and cost–effectiveness of procedures are relevant influencing aspects. Published TAVI results for high-risk and inoperable patients are promising in terms of survival, functional status and quality of life [6]. However, reported 1 year survival rates and the frequency of adverse outcomes vary widely [7]. This variability is partly explained by scarcity of randomized controlled trials, by differences in existing scores used to judge the appropriateness of TAVI, by differences in outcome definitions and by limited numbers of patients per study [8]. The learning curve and operator experience play a major role on procedural efficacy and safety as well [9,10]. It was recently demonstrated that operators’ experience (i.e., >135 procedures) was an independent predictor of 30 days survival [9] and that experience accumulated over 44 transfemoral aortic valve implantations led to significant decreases in procedural times, radiation and contrast volumes [10]. Proficiency increased, with evidence of a plateau, after the first 30 cases [10].
The recent CE mark for intermediate-risk patients obtained in Europe by two TAVI therapies (one of which also obtained FDA approval in the USA), which is likely to increase TAVI economic impact, has relighted the debate on the sustainability of healthcare resource consumption in the future [6]. Thus, the utilization and diffusion of TAVI need to be better investigated, and an understanding of the social, regulatory, economic and political circumstances behind TAVI adoption is vitally important from a public policy perspective. Mylotte et al. [11] described trends in the number of TAVIs implanted from 2007 to 2011 across 11 European countries, underlining substantial variability in TAVI diffusion among countries and in the number of implants per center across nations. The authors also studied the link between TAVI use and reimbursement strategies. Unfortunately, although Italy represents the country with the second largest number of implants in Europe, it was excluded from the analyses due to regional heterogeneity in reimbursement mechanisms.
Our study aimed at investigating the diffusion of TAVI in the Italian market since its introduction in 2007. To this end, we studied the potential drivers of TAVI uptake and diffusion in terms of policy (i.e., reimbursement policies, presence of turnaround plans (TPs), presence of regional guidelines for the appropriate use of TAVI) and management strategies (i.e., ownership, teaching status, implanting centers’ experience with TAVI, mono-specialty activity, presence of opinion leaders clinicians, 24-h services and use of software for medical reporting).
Background
Indications for transcatheter aortic valve implantation
In 2008, the European Society of Cardiology (ESC) and the European Association of Cardio-Thoracic Surgery (EACTS) published a joint position statement in which they indicated that the use of TAVI should be restricted to high-risk patients or those with contraindications for surgery [1]. The selection of patients, and especially the risk assessment, should involve a multidisciplinary consultation. Risk assessment is based both on clinical judgement and on the combination of several quantitative scores (i.e., Logistic EuroScore >20% and STS score >10%). The recommendations were confirmed by the 2012 version of the guidelines, which also pointed out that TAVI should not be performed in patients at intermediate risk for surgery and that trials were required in this population [2]. These indications, valid for all European countries, have been confirmed in Italy by the Italian Federation of Cardiology (FIC) and by the Italian Society for Cardiac Surgery [12]. In addition, given the absence of a perfect quantitative score for the assessment of risk for surgery, several Italian regions published guidelines including clinical criteria for ensuring the appropriate use of TAVI [13–18].
The good results on the new generation of devices [19–21] have supported, in the second half of 2016, CE Mark extension to intermediate-risk patients for two TAVI technologies and US FDA approval for one of them. Indications for intermediate-risk patients have not been published by Scientific Societies yet.
Structural, organizational & clinical competence requirements for TAVI
According to the European and Italian clinical guidelines, the implants should be restricted to centers having both cardiology and cardiac surgery departments [1–2,12]. Patients should be managed by a multidisciplinary heart team, with a predefined composition [1–2,12–18]. ESC/EACTS generically referred to implants performed in a limited number of high-volume centers, but did not define a minimum number of procedures required for competency due to insufficient data [1]. More recently, clinical competence requirements were defined by several Agencies and Scientific Associations: the minimum threshold was defined equal to 20 (in previous year) by the Centers for Medicare and Medicaid Services [22]; two per month by the French Haute Autorité de Santé [23]; 24 by the British Cardiovascular Intervention Society jointly with the Society of Cardiothoracic Surgeons [24]; 30 by the Canadian Institut national d'excellence en santé et en services sociaux [25]; and 50 by the Dutch HTA agency [26].
Regulation as to the identification and accreditation of implanting centers has been heterogeneous in Italy. Only two regions (i.e., Emilia Romagna and Sicilia) explicitly authorized a limited number of hospitals, basing their decisions on clinical competence requirements [13,17]. The other regions did not issue any law and allowed all the hospitals with on-site cardiac surgery to perform implants.
The Italian healthcare system: overview of institutional assets & regional reimbursement mechanisms
The Italian National Health Service is a decentralized, tax-funded healthcare system that provides care to the entire Italian population free of charge. The Italian National Health Service has three tiers: the central government; 21 regional governments (henceforth referred to as regions), with jurisdiction over most healthcare issues, including reimbursement; and providers. Regions allocate funds to providers using two main mechanisms: hospitals directly managed by local health authorities (LHA) are funded on a capitation basis, whereas the other hospitals are prospectively funded according to regional tariffs [27]. Tariff-based reimbursement systems largely vary across regions. Some regions reimburse a standard fee schedule based on the diagnosis-related group (DRG) into which the hospitalization is classified in. In Italy TAVI implantation is generally classified into DRGs of Cardiac valve and other major cardiothoracic procedures, respectively with (DRG 104) and without (DRG 105) cardiac catheterization, with the exception of Lombardia, which classifies the admissions into DRG 518 percutaneous cardiovascular procedures without coronary artery stent or AMI. In a ‘basic’ DRG system, hospitals are reimbursed the standard rate for surgical aortic valve replacement and there is no extra funding for the device's cost. To support TAVI use, Italian regions developed two types of special funding systems [28]. Certain regions (i.e., Lombardia, Basilicata and Sicilia) introduced supplementary payments, paid in addition to the standard DRG rate. We classify this system as ‘add-on’. Other regions (i.e., Emilia Romagna and Campania) use procedure-specific payments instead of DRG-specific, in other words, predetermined fixed sums that include both the cost of hospitalization, procedure and device. This system is defined as ‘lump-sum’.
Materials & methods
Materials
We created an ad hoc dataset by merging data from different sources. The data on the adoption and diffusion of TAVI derive from a public registry of the Italian Society of Interventional Cardiology (GISE), which routinely collects data on the activities of all Italian catheter laboratories [29]. The database also includes information on the region where the cath labs are located, if they use software for medical records and whether they operate 24 h. Our sample consisted of all Italian hospitals that adopted TAVI since its introduction in 2007.
Data on reimbursement policies were retrieved from regional laws and official fee schedules. When official documentation was not entirely clear, key informants were contacted in order to have a better understanding of reimbursement mechanisms concerning TAVI in the specific region. Based on the information retrieved from these sources, we divided hospitals into two groups: tariff and capitation, according to whether they were funded through a tariff-based payment system or through capitation [27]. The first group was further classified into three categories, according to the type of regional reimbursement system: basic (i.e., DRG rate for hospitalization, with no reimbursement for the device), add-on (i.e., additional payments on top of the DRG tariff) and lump-sum (i.e., flat, procedure-specific rates that cover both the cost of hospitalization, procedure and device) [28]. Regional laws were also used as a source of the year of publication of regional recommendations for the use of TAVI [28].
Information on TPs was found on the Ministry of Health website [30]. TPs are agreements between the Italian central government and regions with a persistent deficit [31]. They were introduced in 2007 with the aim of monitoring these regions’ healthcare expenditures and reducing their deficits. The Ministry of Health website also provided information on hospital institutional characteristics. We classified the hospitals according to their ownership (public vs private), teaching status (teaching vs nonteaching), type of activity (cardiologic vs general hospital), location (north, center or south) and presence of TP.
Information on the resident population 2007–2015 and share of people aged 75 years or more was obtained from the Italian Institute of National Statistics website [32], and economic indices and healthcare parameters (i.e., gross domestic product [GDP] per capita, healthcare expenditures as% of GDP) were obtained from the Observatory on Italian Healthcare Providers [33]. Table 1 provides the full list of the variables included in the study and the corresponding sources.
Methods
The following measures were computed: the annual number of implants (total and per million people), the number of implanting centers (total and per million people) and the average number of implants per center.
To assess the adherence of Italian implanting centers to international scientific associations and HTA agencies guidelines [22–26], which require a minimum number of 20 TAVI implants per year, we analyzed the distribution of TAVI implants by implanting centers into three classes: low- (i.e., less than 20 implants per year), medium- (i.e., 20–29) and high-volume (i.e., more than 30). The upper threshold was defined according to recent evidence of increasing proficiency after the first 30 TAVI cases [10]. Last, we followed implanting centers’ classes of implants over time and computed the probability of transition among the different classes.
To investigate the factors that affect TAVI diffusion, we run several regressions using as dependent variable the number of TAVI implants in Italian hospitals from 2007 to 2015. We used the logarithmic transformation of the variable to allow the interpretation of coefficients as percentage impact. The estimated model is as follows:
where i is for hospital, j for region and t for year. X is a set of observable hospital-specific, time-dependent variables including ownership, teaching status, class of productivity (i.e., low-, medium-, high-) in previous year, mono-specialty cardiologic activity, 24 h activity, use of software for medical records and location in north/center/south Italy. Z is a set of time-variant regional characteristics including reimbursement, presence of regional guidelines for the appropriate use of TAVI, presence of TP, regional GDP per capita, share of regional health expenditure over GDP and share of people aged 75 or more. We tested different models by introducing first control variables (i.e., ownership and teaching status) and yearly dummies (model 1), then adding hospital-level variables (models 2, 4 and 5) and, finally, regional-level variables (models 3, 6 and 7). To have a better understanding of the impact of reimbursement on the uptake and diffusion of TAVI, we run the regressions on two different subsamples of hospitals. We first considered the full sample (i.e., including both hospitals funded through tariffs and capitation) and tested the impact of the type of reimbursement by including a dummy variable for tariff-based payment (models 1–3). Afterward, we focused on tariff-funded hospitals and tested the impact of the level of tariff (models 4 and 6) and of the presence of special funding mechanisms (i.e., add-on payments and lump-sums, models 5 and 7). Last, to assess the goodness of fit, we run predictive models on both the full sample (i.e., 9 years) and on the first 6 years of the data. Statistical analyses were performed using the software package Stata version 14.
Results
Between 2007 and 2015, 15,627 patients underwent TAVI in Italy (Table 2). If we exclude 2007, when TAVI was first introduced in the last months of the year, we observe an increase in the total number of implants diminishing over time, from 154% of increase in 2009 to 34% in 2015. The number of implants per million (M) people shows an increasing trend and reached 57 TAVI/M inhabitants in 2015. The number of implanting centers constantly increased from 23 in 2008 to 87 in 2015, representing an average of 1.4 centers per million people. Overall, in 2015, 39.8 TAVIs per center were performed, with an increase of 29% compared with 2014. If we distinguish hospitals by ownership, private hospitals show on average a higher productivity than public ones until 2014, while in 2015 they were almost overlapping (40.3 TAVIs vs 39.6, Figure 1). If we consider the distribution of centers by number of annual implants, the share of low-volume ones (i.e., centers performing less than 20 TAVIs per year) shows a decreasing trend over time, counterbalanced by an increasing share of high-volume ones (i.e., centers implanting more than 30 TAVIs) (Figure 2). In 2015, 32% of the Italian centers were low-volume centers, high-volume centers being equivalent to 53%.
Figure 3 shows the number of TAVI implants by region and the reimbursement system adopted by Italian Regions in 2015, while Table 3 illustrates the number of TAVIs and implanting centers by region, reimbursement mechanism and level of tariff in 2015.
The results of the regressions are shown in Tables 4 & 5. The explanatory power of the models can be evaluated by considering the between (i.e., interhospital) r-squared. In the analysis on the full sample of hospitals, the model with only control variables and yearly dummies (model 1) explains only 0.4% of the variability in the annual number of TAVI implants. The greatest improvement comes from the inclusion of hospital-level variables (model 2), which increases the value of the between r-squared up to 66.2%. The inclusion of regional variables (model 3) allows the explanatory power to further increases up to 69.8%. We refer our interpretations looking at the full model (i.e., models 3). In the analyses of tariff-based reimbursed hospitals, the explanatory power of the models with only hospital-level variables (models 4 and 5) are, respectively, equal to 68.95 and 67.6%, while of the full models (6 and 7) are 70.24 and 69.8%.
The diffusion of TAVI in Italy has been characterized by a sharp annual increase (+44.8% on average) and appears to be close to the plateau, as testified by the negative coefficient of the variable time squared (Table 4). Anyhow, time variables lose their significance in models 2 and 3, where part of time effect is captured by the volume of implants in previous year. Indeed, hospitals who performed more than 30 implants in previous year (i.e., high-volume hospitals) experience an increase in annual implants equal to 105%. The increase is equal to 77.7% for medium-volume centers. Hospitals with cardiologists or cardiac surgeons who contributed to publish the ESC/EACTS guidelines for the management of valvular heart diseases [1,2], implant 95.4% more TAVIs than other similar hospitals. Hospitals located in regions with TP implant 23.9% less TAVIs, although the impact is only marginally significant. The publication of regional recommendations aimed at identifying patients’ selection criteria and ensuring the appropriate use of TAVI, slows down the diffusion of TAVI in those regions (-15.5% but not significant). The type of reimbursement significantly affects the annual number of implants: hospitals reimbursed through tariffs perform on average 52.6% more implants than those payed through capitation. However, neither the level of tariff nor the presence of special funding mechanisms (i.e., add-on and lump-sum) significantly affect the number of implants (Table 5). The impact of the variables discussed above is confirmed also in the subsample of tariff-based reimbursed hospitals (models 4–7).
The key driver of TAVI diffusion, explaining between 56 and 65% of the models, is implanting centers’ experience with the heart valve. This result is confirmed by the analysis of the probability of transition across classes of centers (Figure 4). Low-volume centers have 73% probability to remain in the same class and to stop implanting of 4%. Once hospitals have increased their experience and reached a medium- or high-volume, they never stop implanting. Medium-volume centers upgrade to high-volume centers in 57% of cases and high-volume centers remain in the same class in 94% of cases.
The predictions obtained using both the full, 9 years sample and the first 6 years of diffusion confirm the goodness of fit of our models. The analyses are available from the authors upon request.
Discussion
Between 2007 and 2011, nearly half of all TAVIs across Europe were performed in Germany (45.9%), with Italy being the next most frequent implanter (14.9%) [11]. The total number of implants in Italy was 1929 in 2011, compared with 7252 in Germany and grew up to 3465 in 2015. Nevertheless, by applying the data on prevalence presented by Osnabrugge [4] to demographic projections over the next decades, we estimate that the potential number of TAVIs will increase to nearly 4300 per year and that more than 62,000 patients will be TAVI candidates in Italy in 2050.
Healthcare innovation has become a major concern for policymakers in all industrialized countries. If it is true that innovation is a main determinant of better health outcomes, it is also true that innovation can only be introduced if economically sustainable. This concept is particularly important in public healthcare systems, in which services are funded by taxpayers and the allocation of public resources must follow the opportunity cost principle. Cost–effectiveness analysis (CEA) is a widespread tool used by policymakers to assess whether incremental benefits outweigh incremental costs. Nevertheless, once CEA is performed and final recommendations are made, the uptake and diffusion of technological innovation is highly dependent on variables other than economic evaluation, such as reimbursement policies, procurement procedures and stakeholders’ influence.
A comparative analysis of TAVI diffusion trend in European countries concluded that economic and reimbursement variables help explaining the variability in TAVI adoption across nations [11]. More specifically, the authors found that TAVI use increases more in insurance-based systems (e.g., Germany) compared with tax-based systems (e.g., Italy). The authors also inferred that the uneven TAVI distribution across nations raises the uncomfortable issue of equity of patient access. This issue is particularly relevant given the Patients’ Rights in Cross-Border Healthcare Directive (Directive 2011/24/EU) of the EU, which promotes patients’ mobility between EU countries. How would low TAVI penetration-rate nations address their own patients who ask to move to high TAVI penetration-rate countries? If patients’ mobility is to happen, understanding and measuring the impact of coverage policies in EU countries is important to help reduce patients’ uneven access to care.
Although Italy is the second largest market in the EU for TAVIs, it was not included in the study by Mylotte et al. [11] because of the complexity of the Italian funding and reimbursement. Our study filled this gap, and contributed to a better understanding of the main predictors of TAVI diffusion in a tax-based, decentralized EU country such as Italy. We believe that the variety of payment schemes currently in use across the Italian regions and across different hospital types represents an interesting case study for investigating the role of reimbursement mechanisms in the technology's diffusion patterns at the individual hospital level [34].
The main role of prospective payment systems is to orient providers’ behavior. Payers strategically use tariffs to steer providers’ production [35]. According to whether rates are higher or lower than the procedure-specific production costs borne by providers, the providers can be incentivized or discouraged to invest in and deliver certain hospital procedures, whereas capitation-based hospitals have the incentive to keep total production costs as low as possible so as not to exceed the allocated budget. Tariff-based hospitals are therefore expected to invest more than their capitation counterparts in technological innovation do, provided that the specific DRG rate is at least equivalent to the direct procedure costs. Seventy-eight TAVI providers out of 87 are financed through tariffs in Italy (Table 3), and tariff-based hospitals have the highest mean number of implants (41.2 vs 28.1). The difference between the two groups was found to be statistically significant (Table 4), although the level of tariff does not significantly influence providers’ production (Table 5). This may suggest that the payers’ strategy either has not been effective in incentivizing the diffusion of TAVI or that is not considered a key factor by end-users. The first interpretation is consistent with the results of a previous empirical study conducted in Italy on coronary stents [36]. The latter is line with a recent qualitative work, which demonstrated that the diffusion of TAVI in Germany has been influenced by multiple factors (e.g., perceived medical advantages of the new technology, social prestige of implanting centers and of clinicians, opinion leaders heading the departments, cooperation between cardiac surgeons and interventional cardiologists) that go beyond the level of reimbursement [37].
Notably, the marked difference between private and public hospitals, with privates delivering a higher mean number of TAVIs in the first 8 years, dropped in 2015, when the productivity of the two was perfectly in line (Figure 1). We can infer that private hospitals tend to reach earlier the plateau of the learning curve [10], thus profiting from economies of scale and reducing procedural time and complications [8]. Anyhow, it is worth underlining that hospitals’ productivity (i.e., the annual number of implants) shows an increasing trend over time, as testified by the increasing share of high-volume centers (+31% from 2014 to 2015), counterbalanced by a decrease of low- and medium-volume centers (-15 and -13% respectively).
Conclusion
The diffusion of TAVI in Italy is characterized by great variability across regions and different hospital types. The present study is the first that covered the entire population of hospitals implanting TAVIs in Italy and attempted to explain differences across regions and hospitals by a regression analysis. Major drivers of TAVI diffusion are providers’ experience, the presence of key opinion leaders (i.e., clinicians involved in developing the international guidelines for the management of valvular heart disease) and reimbursement schemes (i.e., tariff vs capitation). The latter finding is consistent with what was found by Mylotte et al. [11] and with Cappellaro et al. [36], who found that the amount of the tariff is not however important to explain the diffusion. The strongest predictor of diffusion of TAVI in Italy is implanting centers’ experience: hospitals that performed more than 20 implants in previous year implant a significantly higher number of valves the year after, thus contributing to improving health outcomes.
This study contributes to identify the most important variables that explain the diffusion of new technologies and can help decision-makers governing the introduction of innovations in healthcare.
| Variable | Description | Source |
|---|---|---|
| lnid | Log of yearly number of TAVI implants per center | GISE registry |
| Public | 1 if public hospital, 0 otherwise | MoH |
| Teach | 1 if teaching, 0 otherwise | MoH |
| med_volume | 1 if hospital had medium productivity (i.e., 20–29 implants) in previous year, 0 otherwise | GISE registry |
| high_volume | 1 if hospital had high productivity (i.e., >30 implants) in previous year, 0 otherwise | GISE registry |
| 24 h | 1 if cath lab works 24 h, 0 otherwise | GISE registry |
| sw | 1 if cath lab uses software for medical records, 0 otherwise | GISE registry |
| North | 1 if hospital is located in northern Italian region, 0 otherwise | GISE registry |
| Center | 1 if hospital is located in central Italian region, 0 otherwise | GISE registry |
| South | 1 if hospital is located in southern Italian region, 0 otherwise | GISE registry |
| Cardio | 1 if cardiologic hospital, 0 otherwise | MoH |
| ESC | 1 if hospital's clinicians authored ESC/EACTS guidelines for management of valvular heart disease | ESC/EACTS guidelines |
| Tariff | 1 if hospital funded through tariffs, 0 otherwise | Regional laws/fee schedules |
| tar_level | Level of tariff | Regional laws/fee schedules |
| add_on | 1 for additional payments on top of DRG rate, 0 otherwise | Regional laws/fee schedules |
| lump_sum | 1 for procedure-specific rate, 0 otherwise | Regional laws/fee schedules |
| tp | 1 if TP is active, 0 otherwise | MoH |
| reg_guidelines | 1 if region published guidelines for the appropriate use of TAVI, 0 otherwise | Regional laws |
| gdp_per_cap | Regional GDP per capita | OASI |
| he_%_gdp | Share of regional health expenditures over GDP | OASI |
| %75+ | % of regional population aged 75 years or older | ISTAT |
| t | Year (from 1 to 9) | |
| t2 | Year squared |
EACTS: European Association of Cardio-Thoracic Surgery; ESC: European Society of Cardiology; GDP: Gross domestic product; GISE: Italian Society of Interventional Cardiology; ISTAT: Italian Institute of National Statistics; MoH: Ministry of Health; OASI: Observatory on Italian Healthcare Providers; TAVI: Transcatheter aortic valve implantation; TP: Turnaround plan.
| Year | TAVI implants | Implanting centers | Average implants per center | ||
|---|---|---|---|---|---|
| n | n per million population | n | n per million population | ||
| 2007 | 72 | 1.2 | 12 | 0.2 | 6.0 |
| 2008 | 450 | 7.5 | 23 | 0.4 | 19.6 |
| 2009 | 1142 | 19.0 | 53 | 0.9 | 21.5 |
| 2010 | 1581 | 26.2 | 70 | 1.2 | 22.6 |
| 2011 | 1929 | 31.8 | 77 | 1.3 | 25.1 |
| 2012 | 2087 | 35.1 | 77 | 1.3 | 27.1 |
| 2013 | 2309 | 38.7 | 75 | 1.3 | 30.8 |
| 2014 | 2592 | 42.6 | 84 | 1.4 | 30.9 |
| 2015 | 3465 | 57.0 | 87 | 1.4 | 39.8 |
TAVI: Transcatheter aortic valve implantation.
| Region | Number of TAVI implants | Number of implanting centers | Level of tariff (min–max); €† | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Capitation | Tariff | Capitation | Tariff | ||||||
| Basic | Add-on | Lump-sum | Basic | Add-on | Lump-sum | ||||
| Piemonte | 214 | 8 | 20,487–24,675 | ||||||
| Lombardia | 988 | 22 | 24,865 | ||||||
| PA Trento | 22 | 1 | |||||||
| Veneto | 189 | 176 | 5 | 2 | 27,476–34,179 | ||||
| Friuli Venezia Giulia | 77 | 2 | 21,551–25,492 | ||||||
| Liguria | 60 | 1 | 15,775–20,160 | ||||||
| Emilia Romagna | 219 | 4 | 30,640 | ||||||
| Toscana | 269 | 6 | 18,237–19,910 | ||||||
| Umbria | 47 | 2 | 20,487–24,675 | ||||||
| Marche | 36 | 1 | 21,102–25,415 | ||||||
| Lazio | 142 | 7 | 20,487–24,675 | ||||||
| Abruzzo | 34 | 1 | |||||||
| Campania | 355 | 10 | 25,000 | ||||||
| Puglia | 2 | 166 | 1 | 6 | 20,487–24,675 | ||||
| Basilicata | 41 | 1 | 28,487–32,675 | ||||||
| Calabria | 85 | 2 | 20,487–24,675 | ||||||
| Sicilia | 301 | 3 | 28,487–32,675 | ||||||
| Sardegna | 6 | 36 | 1 | 1 | 17,043–21,184 | ||||
| Total | 253 | 1308 | 1330 | 574 | 9 | 38 | 26 | 14 | |
†The minimum and maximum level of tariff depend upon the presence of cardiac catheterization, which shifts the hospital admission from diagnosis-related group 105 to 104.
PA: Provincia Autonoma; TAVI: Transcatheter aortic valve implantation.
| Dependent variable | lnTAVI: model 1 | lnTAVI: model 2 | lnTAVI: model 3 |
|---|---|---|---|
| Public | 0.0279 | 0.7219 | 0.168 |
| Teach | 0.426* | 0.205 | 0.206 |
| t | 0.448*** | 0.159 | 0.223 |
| t2 | -0.0222*** | -0.00673 | -0.00979 |
| Tariff | 0.510** | 0.526** | |
| Med_volume | 0.772*** | 0.777*** | |
| High_volume | 1.035*** | 1.050*** | |
| Cardio | 0.0452 | -0.0324 | |
| ESC | 0.937*** | 0.954*** | |
| 24 h | 0.268 | 0.274 | |
| sw | 0.0335 | 0.035 | |
| North | 0.413** | 0.399** | |
| South | 0.478** | 0.125 | |
| tp | -0.239* | ||
| Reg_guidelines | -0.155 | ||
| %75+ | -4.735 | ||
| gdp_per_cap | -0.0000612 | ||
| he_%_gdp | -13.65 | ||
| Constant | 0.637** | 0.359 | 3.528 |
| Observations | 558 | 558 | 558 |
| Number of hospitals | 98 | 98 | 98 |
| R-sq within | 0.3888 | 0.3859 | 0.3860 |
| R-sq between | 0.0042 | 0.6621 | 0.6980 |
| R-sq overall | 0.1151 | 0.5176 | 0.5294 |
*p < 0.1; **p < 0.05; ***p < 0.01.
ESC: European Society of Cardiology; lnTAVI: Natural logarithm of TAVI implants.
| Dependent variable | lnTAVI: model 4 | lnTAVI: model 5 | lnTAVI: model 6 | lnTAVI: model 7 |
|---|---|---|---|---|
| Public | 0.211 | 0.211 | 0.191 | 0.192 |
| Teach | 0.199 | 0.206 | 0.203 | 0.205 |
| t | 0.0463 | 0.0546 | 0.0503 | 0.0761 |
| t2 | 0.00124 | 0.000755 | 0.00127 | 0.00038 |
| Tariff level | 0.000007 | 0.00002 | ||
| Add_on | 0.0201 | -0.0605 | ||
| Lump_sum | -0.108 | -0.122 | ||
| Med_volume | 0.822*** | 0.821*** | 0.820*** | 0.823*** |
| High_volume | 1.068*** | 1.071*** | 1.088*** | 1.098*** |
| Cardio | 0.0574 | 0.0375 | -0.0184 | -0.0345 |
| ESC | 0.965*** | 0.956*** | 1.003*** | 0.981*** |
| 24 h | 0.22 | 0.202 | 0.215 | 0.197 |
| sw | 0.104 | 0.116 | 0.0826 | 0.107 |
| North | 0.322* | 0.344* | 0.294 | 0.381** |
| South | 0.484*** | 0.555*** | 0.235 | 0.28 |
| tp | -0.099 | -0.161 | ||
| Reg_guidelines | -0.267** | -0.193* | ||
| %75+ | 0.528 | -3.352 | ||
| gdp_per_cap | 0.000009 | -0.0000003 | ||
| Health exp%gdp | 9.258 | 6.183 | ||
| Constant | 1.069** | 1.204*** | -0.0797 | 1.236 |
| Observations | 500 | 500 | 500 | 500 |
| Number of hospitals | 86 | 86 | 86 | 86 |
| R-sq within | 0.3762 | 0.3805 | 0.3846 | 0.3857 |
| R-sq between | 0.6895 | 0.6761 | 0.7024 | 0.698 |
| R-sq overall | 0.5393 | 0.5367 | 0.544 | 0.5415 |
*p < 0.1; **p < 0.05; ***p < 0.01.
ESC: European Society of Cardiology; lnTAVI: Natural logarithm of TAVI implants.
The diffusion of new medical technologies is highly dependent on stakeholders’ decisions to adopt innovation, and on the broader environment in which stakeholders are located, including regulatory and financing system, and users’ (i.e., hospitals and physicians) characteristics.
The knowledge of the factors affecting adoption and diffusion of technological innovation is relevant for policymakers because it helps them implementing evidence-based policies aimed at encouraging the desired level of use of new technologies and reducing uneven diffusion across areas and population.
In this paper, we investigated the determinants of diffusion of transcatheter aortic valve implantation (TAVI) in Italy.
TAVI is an alternative treatment option for inoperable and high-risk patients with symptomatic severe aortic stenosis available in the market since 2007.
With aging of the population and the recent CE mark for intermediate-risk patients, TAVI is expected to have an increasing economic impact, thus making the understanding of the factors behind its diffusion vitally important from a public policy perspective.
Our results show that TAVI has diffused in Italy with great variability across regions and different hospital types.
The strongest predictor of diffusion of TAVI in Italy is implanting centers’ experience: medium- and high-volume hospitals in previous year implant a significantly higher number of valves the year after, thus contributing to improving health outcomes.
Major drivers of TAVI diffusion are also the presence of key opinion leaders (i.e., clinicians involved in developing the international guidelines for the management of valvular heart disease) and reimbursement schemes (i.e., tariff vs capitation).
Acknowledgements
The authors would like to acknowledge the contributions of M Corbo and G Beccagutti of Medtronic to developing this project.
Financial & competing interests disclosure
G Callea and MC Cavallo received an unrestricted grant by Regione Lombardia. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Vahanian A, Alfieri O, Al-Attar N et al. Transcatheter valve implantation for patients with aortic stenosis: a position statement from the European Association of Cardio-Thoracic Surgery (EACTS) and the European Society of Cardiology (ESC), in collaboration with the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 29, 1463–1470 (2008).
2.
Vahanian A, Alfieri O, Andreotti F et al. Guidelines on the Management of Valvular Heart Disease (version 2012): the Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 33, 2451–2496 (2012).
• Defines the target patients for transcatheter aortic valve implantation (TAVI), and the implanting centers’ structural and organizational requirements.
3.
Iung B, Cachier A, Baron G et al. Decision-making in elderly patients with severe aortic stenosis: why are so many denied surgery? Eur. Heart J. 26, 2714–2720 (2005).
4.
Osnabrugge RLJ, Mylotte D, Head SJ et al. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modelling study. J. Am. Coll. Cardiol. 62(11), 1002–1012 (2013).
5.
Greenhalgh T, Robert G, Bate P, Kyriakidou O, Macfarlane F. Diffusion of Innovations in Health Service Organisations: A Systematic Literature Review. Blackwell Publishing Ltd, UK (2005).
• Performs a systematic review of the literature on the diffusion of new technologies in healthcare organizations.
6.
Osnabrugge RLJ, Kappeteinen AP, Reynolds MR, Cohen DJ. Cost-effectiveness of transcatheter valvular interventions: economic challenges. EuroIntervention 9, S48–S54 (2013).
7.
Boothroyd LJ, Spaziano M, Guertin JR, Lambert LJ, Rod J, Noiseux N. Transcatheter aortic valve implantation: recommendations for practice based on a multidisciplinary review including cost-effectiveness and ethical and organizational issues. Can. J. Cardiol. 29, 718–726 (2013).
8.
Tarricone R, Drummond M. Challenges in the clinical and economic evaluation of medical devices: the case of transcatheter aortic valve implantation. J. Med. Marketing 3, 221–229 (2011).
9.
Gurvitch R, Tay EL, Wijesinghe N et al. Transcatheter aortic valve implantation: lessons from the learning curve of the first 270 high-risk patients. Cath. Cardiovasc. Interv. 78, 977–984 (2011).
10.
Alli OO, Booker JD, Lennon RJ, Greason KL, Rihal CS, Holmes DR Jr. Transcatheter aortic valve implantation: assessing the learning curve. J. Am. Coll. Cardiol. Intv. 5, 72–79 (2012).
11.
Mylotte D, Osnabrugge RLJ, Windecker S et al. Transcatheter aortic valve replacement in Europe: adoption trends and factors influencing device utilization. J. Am. Coll. Cardiol. 62, 210–219 (2013).
•• Examines TAVI adoption trends in 11 western European countries and quantitatively investigates factors that may influence its heterogeneous use.
12.
Santoro G, Vitali E, Tamburino C et al. Impianto transcatetere di protesi valvolare aortica in pazienti con stenosi valvolare severa sintomatica. Documento di Consenso Federazione Italiana di Cardiologia (FIC)-Società Italiana di Chirurgia Cardiaca (SICCH). G. Ital. Cardiol. 11, 45–53 (2010).
13.
Agenzia Sanitaria e Sociale Regionale, Commissione cardiologica e cardiochirurgia, Regione Emilia Romagna. Documento di indirizzo per l’impianto clinicamente appropriato delle protesi valvolari aortiche per via percutanea e trans apicale (2009). http://assr.regione.emilia-romagna.it/it/servizi/pubblicazioni/rapporti-documenti/documento-di-indirizzo-per-l2019impianto-clinicamente-appropriato-delle-protesi-valvolari-aortiche-per-via-percutanea-e-transapicale.
14.
ARS Liguria, DGR 736/2013, Sistema regionale di gestione dell'Impianto Percutaneo di Protesi Valvolare Aortica – Documento di consenso della rete cardiologica regionale (2013). www.alisa.liguria.it/.
15.
Unità di Valutazione dell'Efficacia del Farmaco, Regione Veneto. Report di HTA Valvola Cardiaca Transcatetere (2010). www.uvef.it/extfiles/10429/attachment/FILE1311340891948-1380.pdf.
16.
Giani E, Rivoiro C, Romano V. Sostituzione della Valvola Aortica per via Transapicale (TA-TAVI). Short Report A.Re.SS (2011). www2.aress.piemonte.it/cms/short-report.html?download=1188%3Asostituzione-della-valvola-aortica-per-via-transapicale-ta-tavi.
17.
Regione Siciliana, Assessorato della salute, Decreto Assessorile n.2575 del 12/1272011, Impianto transcatetere di protesi valvolare aortica in pazienti con stenosi valvolare severa sintomatica (2011). http://pti.regione.sicilia.it/portal/page/portal/PIR_PORTALE/PIR_LaStrutturaRegionale/PIR_AssessoratoSalute/PIR_Decreti/PIR_Decreti2016/PIR_DecretiAssessoriali2016/D.A.%20n.%202257%20del%2021%20nov.%202016.pdf.
18.
Laziosanità Agenzia di Sanità Pubblica, Regione Lazio. Documento di indirizzo per l'impianto di protesi valvolare aortica trans-catetere (TAVI) (2013). www.asplazio.it/asp_online/doc_indirizzo_TAVI.pdf.
19.
Thyregod HG, Steinbrüchel DA, Ihlemann N et al. Transcatheter versus surgical aortic valve replacement in patients with severe aortic valve stenosis: 1 year results from the All-Comers NOTION Randomized Clinical Trial. J. Am. Coll. Cardiol. 65(20), 2184–2194 (2015).
20.
Søndergaard L, Steinbrüchel DA, Ihlemann N et al. Two-year outcomes in patients with severe aortic valve stenosis randomized to transcatheter versus surgical aortic valve replacement: The All-Comers Nordic Aortic Valve Intervention Randomized Clinical Trial. Circ. Cardiovasc. Interv. 9, e003665 (2016).
21.
Manoharan G, Walton AS, Brecker SJ et al. Treatment of symptomatic severe aortic stenosis with a novel resheathable supra-annular self-expanding transcatheter aortic valve system. JACC Cardiovasc. Interv. 8(10), 1359–1367 (2015).
22.
Centers for Medicare and Medicaid Services. Proposed decision memo for transcatheter aortic valve replacement (TAVR) (CAG-00430N) (2012). www.cms.gov/medicare-coverage-database/details/nca-proposed-decision-memo.aspx?NCAId=257&ver=5&NcaName=Transcatheter±Aortic±Valve±Replacement±(TAVR)&bc=AAAAAAAAIAAA&.
23.
Haute Autorité de Santé, Medical Devices Assessment Department. Transcutaneous aortic valve implantation by the transfemoral or transapical route: reassessment report (2011). www.has-sante.fr/portail/upload/docs/application/pdf/2011--11/assessment_of_tavi_-_summary_vdef.pdf.
24.
British Cardiovascular Intervention Society (BCIS) and the Society of Cardiothoracic Surgeons (SCTS), Transcatheter Aortic Valve Implantation (TAVI). A position statement of the British Cardiovascular Intervention Society (BCIS) and the Society of Cardiothoracic Surgeons (SCTS) (2009). http://bcis.org.uk/wp-content/uploads/2016/12/BCIS-SCTS-position-statement.pdf.
25.
Institut national d'excellence en santé et en services sociaux (INESSS). Implantation valvulaire aortique par cathéter. Évaluation des données probantes et synthèse des considérations organisationnelles. Rédigé par Marco Spaziano, Lucy J. Boothroyd, Jason R. Guertin, Chakor H, Xiao Y, Lambert LJ, Bogaty P. ETMIS 8, 1–84 (2012). www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Cardio/INESSS_resume_TAVI_FR.pdf.
26.
Blekkenhorst B. Transcatheter Aortaklepvervanging. College voor Zorgverzekeringen (2011). www.cvz.nl/binaries/content/documents/zinl-www/documenten/publicaties/rapporten-en-standpunten/2011/1110-transcatheter-aortaklepvervanging/Transcatheter±aortaklepvervanging.pdf.
27.
Fattore G, Torbica A. Inpatient reimbursement system in Italy: how do tariffs relate to costs? Health Care Manage. Sci. 9, 251–258 (2006).
28.
Callea G, Cavallo MC, Tarricone R, Beccagutti G, Busca R, Corbo M. Il governo dell'innovazione tecnologica in sanità. Il caso dell'impianto di valvola aortica transcatetere: stato dell'arte delle indicazioni e della rimborsabilità nelle regioni italiane. Mecosan 95, 137–160 (2015).
•• Draws a detailed picture of the policies devised by Italian regions to govern the introduction of TAVI in Italy.
29.
Società Italiana di Cardiologia Invasiva (GISE). www.gise.it/.
30.
Italian Ministry of Health. http://salute.gov.it/.
31.
Jommi C, Costa E, Michelon A, Pisacane M, Scroccaro G. Multi-tier drugs assessment in a decentralised health care system. The Italian case study. Health Policy 112, 241–247 (2013).
32.
Italian National Institute of Statistics (ISTAT). http://demo.istat.it/.
33.
Observatory on Italian Healthcare Management (OASI). www.cergas.unibocconi.it/wps/wcm/connect/Cdr/Centro_CERGASit/Home/Area+download+Rapporto+OASI+e+Mecosan/.
34.
Ciani O, Tarricone R, Torbica A. Diffusion and use of health technology assessment in policy making: what lessons for decentralised healthcare systems? Health Policy 108, 194–202 (2012).
35.
Tarricone R, Torbica A. Costing and performance in healthcare management. In: Statistical Methods in Healthcare. Faltin FW, Kenett RS, Ruggeri F (Eds). Wiley, UK, 386–404 (2012).
36.
Cappellaro G, Ghislandi S, Anessi-Pessina E. Diffusion of medical technology: the role of financing. Health Policy 100, 51–59 (2011).
37.
Merkel S, Eikermann M, Neugebauer EA, von Bandemer S. The transcatheter aortic valve implementation (TAVI) – a qualitative approach to the implementation and diffusion of a minimally invasive surgical procedure. Impl. Sci. 10, 140–148 (2015).
• Investigates the implementation and diffusion of TAVI in Germany with a qualitative approach.
Information & Authors
Information
Published In
Copyright
© Giuditta Callea.
History
Published online: 1 February 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Learning effect and diffusion of innovative medical devices: the case of transcatheter aortic valve implantation in Italy. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0083
Export citation
Select the citation format you wish to export for this article or chapter.