Cost–effectiveness of different strategies for treatment relapsing-remitting multiple sclerosis
Abstract
Aim: To compare the cost–effectiveness of different disease-modifying therapies’ strategies for treatment of relapsing-remitting multiple sclerosis. Methods: A Markov model was developed to assess the cost–effectiveness and incremental cost–effectiveness ratios for different strategies of using disease-modifying therapies from a US third-party payer perspective. All costs were converted to 2014 US$. Results: Over 20 years, the total costs per patient were estimated at US$161,136.60 for Strategy 1 (symptom management [SM] alone), US$551,650.66 for Strategy 2 (SM and IFN-β-1a), US$703,463.60 for Strategy 3 (SM and natalizumab) and US$670,985.24 for Strategy 4 (SM and alemtuzumab). The accumulated quality-adjusted life years were 10.49, 10.66, 10.69 and 10.71 for each of the four Strategies 1–4, respectively. The resulting incremental cost–effectiveness ratios were 2,297,141.53 comparing Strategy 2 to Strategy 1, and -1,623,918.00 comparing Strategy 4 to Strategy 3. Conclusion: Strategy 1 was the cost-effective strategy for treatment of relapsing-remitting multiple sclerosis when compared with other strategies.

Figure 1. Four treatment strategies for relapsing-remitting multiple sclerosis disease.
SM: Symptom management.
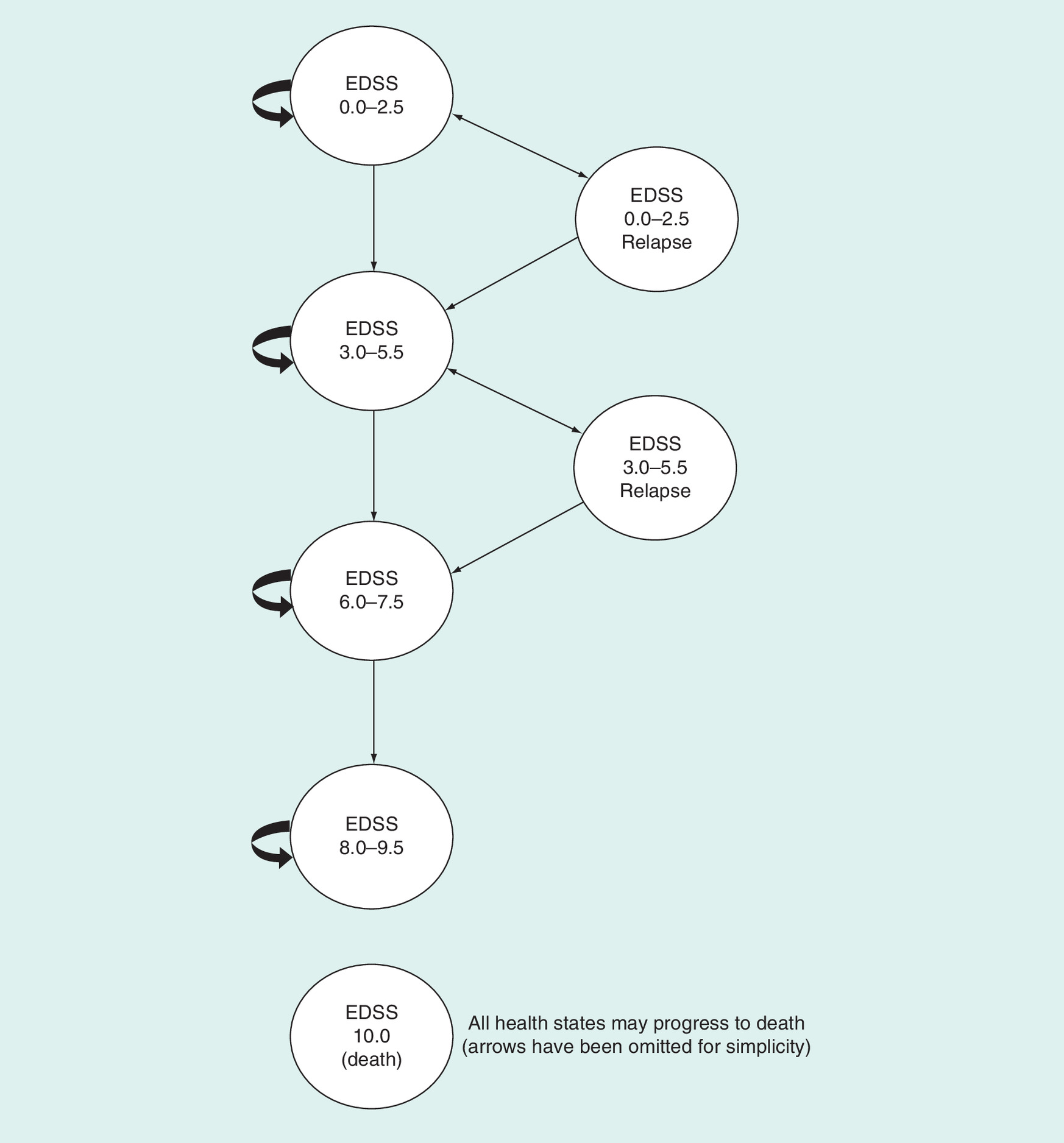
Figure 2. Schematic for the Markov model used in the evaluation.
EDSS: Expanded Disability Status Scale.
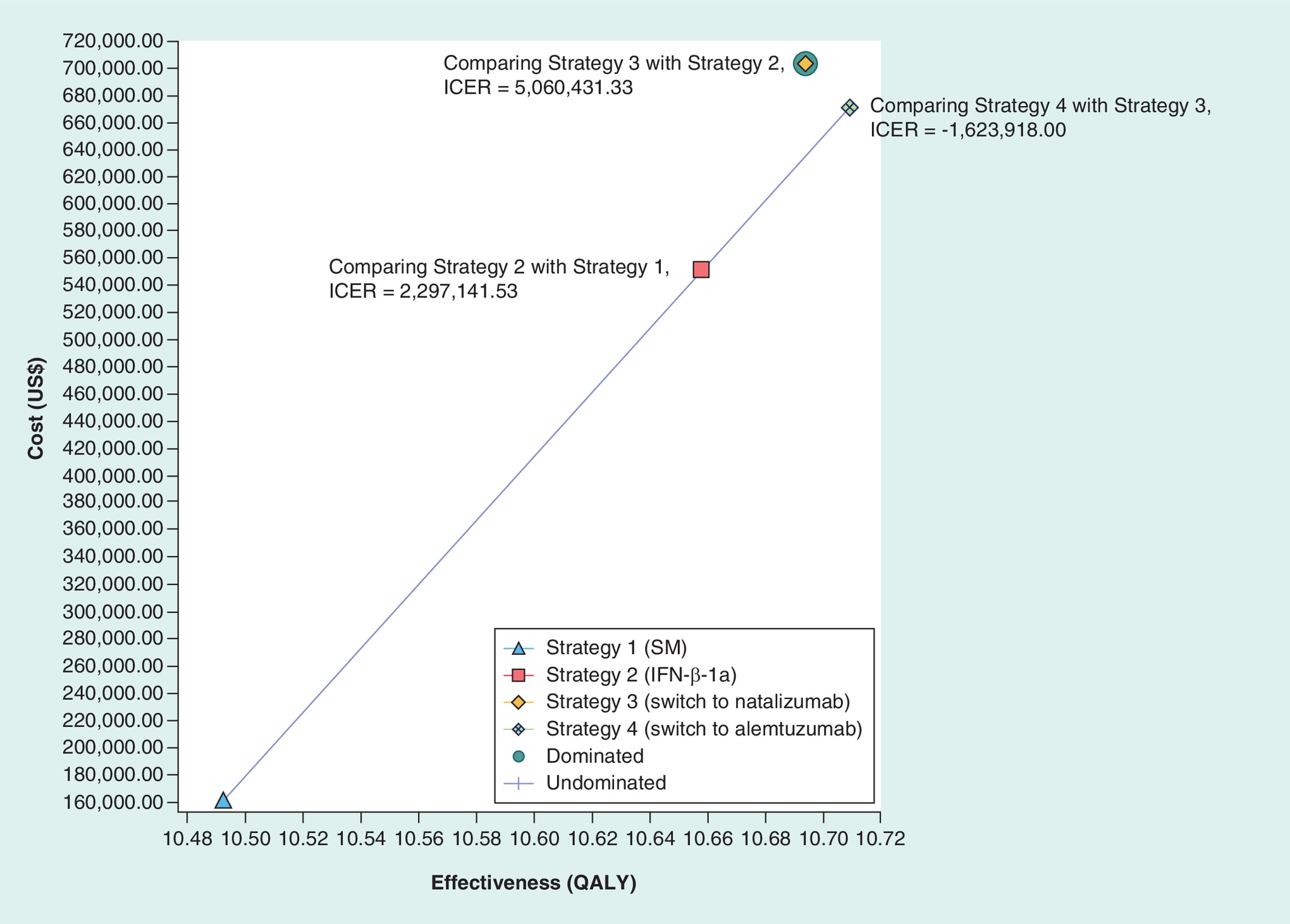
Figure 3. Cost–effectiveness curve.
ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year; SM: Symptom management.

Figure 4. Net monetary benefits of the strategies for treating relapsing-remitting multiple sclerosis.
SM: Symptom management.

Figure 5. Sensitivity analysis (willingness-to-pay = US$50,000).
EDSS: Expanded disability status scale.

Figure 6. Cost–effectiveness acceptability curve.
SM: Symptom management.
First draft submitted: 17 August 2016; Accepted for publication: 10 November 2016; Published online: 25 January 2017
Multiple sclerosis (MS) is a chronic neurodegenerative disease of the CNS [1–3]. This disease affects the transmission of the neurological signals in the body due to demyelination of neurons [1–3]. There are four disease courses or subtypes including relapsing-remitting multiple sclerosis (RRMS), secondary progressive MS, primary progressive MS and progressive-relapsing MS [4].
The most common subtype of MS is RRMS. Around 85% of MS patients are initially diagnosed with RRMS and the remaining are diagnosed with the progressive forms of the disease [5]. RRMS is characterized by worsening of neurological functions unpredictable attacks (also called exacerbations or relapses), which followed by relative recovery periods (also called remissions) [5]. During the periods of remission, there is partially or completely improvement in the symptoms of RRMS with no apparent disease progression. Most of the MS patients who are initially diagnosed with RRMS will finally change to secondary progressive MS (steady MS disease progression with or without acute attacks) [6,7].
There is no cure for MS disease. However, there are disease-modifying therapies (DMTs) used with the aims to modify the MS course and reduce or slow progression of the disease. By 31 December 2014, the USA (the US FDA) had approved 12 DMTs for treatment of relapsing forms of MS [8,9].
A previous study assessed trends in prices of DMTs marketed in the USA and concluded that DMT prices increased faster than the US Consumer Price Index [10]. DMTs are the major component in the management of MS disease, but their prices increased over time, which raised concerns regarding their cost–effectiveness [8–9,11]. Previous studies assessed the costs of MS and compared the cost–effectiveness of MS DMTs [12,13]. However, we did not identify any study in the scientific literature comparing the cost–effectiveness of MS DMTs based on switchable treatments. Also, we did not find any recent studies comparing recent DMTs with symptom management (SM) alone.
Objectives
The objective of this study was to compare the cost–effectiveness of different strategies for the treatment of patients with RRMS. The cost–effectiveness comparisons include four strategies. The strategies were SM alone, SM in combination with one of the following: IFN-β-1a, natalizumab (after switching from IFN-β-1a) and alemtuzumab (after using IFN-β-1a, then switching to natalizumab) (Figure 1). The sequential treatments reflect the clinical practice and are used as the clinically recommended strategy for treatment of RRMS patients. In addition, these strategies represent common treatment alternatives for patients with RRMS and correspond with the indications approved by the FDA for the drugs evaluated. According to the FDA-approved labels, natalizumab is indicated to treat patients with RRMS after treatment failure with a previous DMT; while alemtuzumab is indicated for use in patients with RRMS when two or more DMTs have failed. The DMT failure in this study was defined as increasing in the RRMS disease progression that measured by the expanded disability status scale (EDSS). The DMT switching was at specific EDSS points and it is explained in the method section of this paper.
Data & methods
This cost–effectiveness study was performed from a US third-party payer perspective with a time horizon of 20 years to capture all relevant long-term costs and outcomes of DMTs.
The comparators included in the study were:
IFN-β-1a (Biogen) as a first-line DMT;
Natalizumab as a second-line DMT (previous DMT failed);
Alemtuzumab as a third-line DMT (two former DMTs failed).
Patients were considered to use SM in all treatment strategies (Figure 1). This study compared the incremental cost–effectiveness ratios (ICERs) of the following treatment strategies:
Strategy 1: SM alone (Figure 1A);
Strategy 2: patients use IFN-β-1a. If there was insufficient response to this DMT, they would continue on SM alone (Figure 1B);
Strategy 3: patients use IFN-β-1a, but if there was an insufficient response to this DMT (transition of patients to a higher EDSS health state), they switch to use natalizumab. Then, if there was an inadequate response to natalizumab, they will continue on SM alone (Figure 1C);
Strategy 4: patients use IFN-β-1a, but if there was an insufficient response to this DMT (transition of patients to a higher EDSS health state), they switch to use natalizumab. Then, if there was an insufficient response to natalizumab, they turn to use alemtuzumab. After that, if there was an inadequate response to alemtuzumab, they will continue on SM alone (Figure 1D).
Costs
The wholesale acquisition costs (WACs) were used to calculate the costs of MS DMTs. The WAC is the price for drugs paid by wholesalers to manufacturers. WAC is equal to the average wholesale price (AWP) divided by 1.2. The AWP is the average price where wholesalers sell drugs to pharmacies. AWP per unit for MS DMTs were derived from the RedBook (Truven Health Analytics, Inc.) [14].
Healthcare costs data (ambulatory care, hospital inpatient care, services, tests, adaptations and costs of informal care) were obtained from a study conducted in 2004 by Kobelt et al. assessing the cost of MS disease by stratified EDSS health states [15]. Kobelt et al. were chosen as a reference for healthcare costs data because the reported costs corresponded to each health state in our model [15]. The costs of MS relapses were extracted from a study conducted in 2009 by Oleen-Burkey et al. that reported the impact of MS relapses on economic costs and health-related quality of life for RRMS patients in the USA [16]. Quality-adjusted life years (QALYs) capture the cost of productivity and other indirect costs [17]. Therefore, the costs of productivity losses and other indirect costs were not included in this study.
All costs were inflated to 2014 US$ by using the US Consumer Price Index, US city average, medical care items [15,16]. According to the Panel on cost–effectiveness in health and medicine recommendations, costs were discounted using an annual discount rate of 3% [18]. Cost–effectiveness and the ICERs were estimated.
Health outcomes
Willingness-to-pay
The WHO recommended using three-times the gross domestic product per capita as willingness-to-pay (WTP) threshold per QALY [31,32]. Numerous previous cost–effectiveness studies used US$50,000 as WTP threshold per QALY in the USA [33–35]. However, this threshold is very unlikely consistent with societal preferences in the USA [36]. Therefore, this study considered several WTP thresholds per QALY in the analyses.
Markov model
TreeAge Pro 2015, R2.0 was used to develop a Markov model for simulation of RRMS disease progression in MS patients (Figure 2). Modeling of RRMS disease progression was based on EDSS. The EDSS is a clinician-reported outcome measure, which is most widely used to assess the MS disease progression [37]. The EDSS is measured on an ordinal scale from 0 (means normal neurological functions) to 10 (means death due to MS) [37].
The model is constructed of mutually exclusive and exhaustive health states. The model includes the following health states: EDSS 0.0–2.5 (no or mild disability), EDSS 3.0–5.5 (moderate disability, ambulatory without help), EDSS 6.0–7.5 (walking support required), EDSS 8.0–9.5 (bed restricted), EDSS 10.0 (death due to MS) and two other relapse states (Figure 2). Probabilities of transition from one EDSS health state to another and probabilities of relapses were obtained from previous studies that reported data corresponded to our model (Table 1) [20–24,27,38].
All adult RRMS patients began the model in the EDSS 0.0–2.5 health state (no or mild disability). The duration of each cycle is 1 year. However, we assumed that patients that have a relapse would remain in the relapse health state for 1 month. And the cost and utility of the relapse states were adjusted accordingly. RRMS patients stay in their health state as long as they did not deteriorate (moved to a higher EDSS health state) or died. MS is a progressive disease, so patients could move to more severe health state (higher EDSS state) or a relapse state. Patients who experience relapse could return to the previous health state or deteriorate and move to a higher EDSS state (Figure 2). The probabilities of transition between health states were obtained from the literature [21]. To ensure the internal validity of the model, each author verified the model independently.
Sensitivity analyses
Deterministic one-way sensitivity analyses (±25% unless indicated otherwise) were conducted to assess the possible effect of an individual parameter's uncertainty (DMT acquisition costs, EDSS health state costs and time horizon) on the base-case analysis results. The upper and lower limits of the sensitivity analyses range (±25%) were differed markedly from the base-case parameter inputs and comparable to their corresponding confidence intervals (CI = 95%). In the deterministic one-way sensitivity analyses, the upper limits for DMT acquisition costs were 20% more than WAC for DMTs under the assumption that the AWP (WAC is 80% of the AWP) is the maximum price paid for DMTs in the US market. In addition, Tornado diagrams were plotted to show the impact of individual parameter on the expected value (most sensitive parameter at the top of the diagram and least sensitive parameter at the bottom of the diagram).
Probabilistic sensitivity analysis (second-order Monte Carlo simulation. 1000-times) was conducted to assess the possible combined uncertainty of the parameters (healthcare costs for EDSS health states, DMT acquisition costs and utilities) on the overall confidence in the base-case results. The distribution was assumed to be a gamma distribution for healthcare costs of EDSS health states and DMT acquisition costs [39]. The distribution was assumed to be a beta distribution (between 0 and 1) for utilities [39].
Results
Base-case scenario
Over 20 years, the total costs per patient were estimated at US$161,136.60 for Strategy 1 (SM alone), US$551,650.66 for Strategy 2 (SM and IFN-β-1a), US$703,463.60 for Strategy 3 (SM and natalizumab) and US$668,806.50 for Strategy 4 (SM and alemtuzumab). The accumulated QALYs were 10.49, 10.66, 10.69 and 10.71 for each of the four strategies 1–4, respectively.
Strategy 4 had higher effect (10.71 vs 10.69) and lower cost (US$670,985.24 vs US$703,463.60) than Strategy 3, thus Strategy 3 was dominated by Strategy 4. Strategy 2 was extendedly dominated by Strategy 1 and Strategy 4 (Figure 3). Ruling out strategies through dominance or extended dominance; the comparison of Strategy 4 and Strategy 1 results in an ICER of 2,317,493.82. As long as the WTP was greater than US$100,000, the net monetary benefits of Strategies 2–4 would be greater than zero (Figure 4).
Compared with Strategy 1, the ICER was 2,297,141.53 for Strategy 2. In addition, comparing Strategy 4 to Strategy 3 results in ICERs of -1,623,918.00. Therefore, Strategy 1 (SM alone) was the cost-effective strategy for treatment of RRMS when compared with other strategies (Table 2).
Deterministic one-way sensitivity analyses
SM was the optimal strategy, and there was no effect of individual parameters’ uncertainty (DMT acquisition costs and EDSS health state costs) on the base-case analysis results. The results of the base-case analysis were relatively sensitive to changes in the cost of the EDSS 6.0–7.5 health state and the cost for EDSS 0.0–2.5 (Figure 5). The results of the base-case analysis were not sensitive to the extension of the study time horizon. In addition, the base-case analyses results were relatively stable to changes in all other parameters.
Probabilistic sensitivity analyses
Over a range of different WTPs, Strategy 2 was the optimal treatment strategy with 59.7% acceptability (Figure 6). Both Strategy 1 and Strategy 4 had a less than 22% chance of being the optimal strategy treatment for RRMS. However, the probability for Strategy 4 being preferred was constantly higher than that for Strategy 3. Finally, Strategy 3 had a negligible probability of being the optimal treatment strategy.
Discussion
The results of this study indicate that all the ICERs for the different treatment strategies evaluated were above the $100,000 WTP threshold per QALY, and only Strategy 1 (SM) was cost effective. Strategy 3 (SM and natalizumab) was dominated by Strategy 4 (SM and alemtuzumab) as the latter was more effective and less costly. Strategy 2 (SM and IFN-β-1a) was extendedly dominated by Strategy 1 and Strategy 4 (Figure 3). Strategy 4 had an ICER that exceeded US$2.3 million in comparison with Strategy 1, well above the WTP typically considered as cost effective in the USA.
Over 20 years, the total costs per patient for Strategy 4 (US$670,985.24) were lower than that for Strategy 3 ($703,463.60; Table 2). The dose of alemtuzumab (Strategy 4) was intravenous infusion given to RRMS patients on five consecutive days in the first year of alemtuzumab use, followed by intravenous infusion on three consecutive days 1 year later. Then, alemtuzumab was not given to the RRMS patients. Therefore, the total cost of Strategy 4 was lower than that Strategy 3.
Compared with Strategy 1, the ICER was 2,297,141.53 for Strategy 2. In addition, comparing Strategy 3 to Strategy 2 and Strategy 4 to Strategy 3 results in ICERs of 5,060,431.33 and -1,623,918.00, respectively. The negative ICER given by comparing Strategy 4 to Strategy 3 means that Strategy 4 was cost saving compared with Strategy 3 (Strategy 4 has lower cost and higher effect compared with Strategy 3). Strategy 1 (SM alone) was the most cost-effective strategy for treatment of RRMS when compared with other strategies (Table 2).
Previous studies assessed the ICER of individual DMTs (e.g., IFN-β-1a and natalizumab [33–34,40]). However, these studies did not assess the ICER of sequential treatments that reflect the clinical practice and used as the clinically recommended strategy for treatment of RRMS patients. Our study found that the ICERs for the assessed strategies of sequential treatment were significantly higher than the ICER of the individual DMTs described in previous studies.
The transition points EDSS 3.0, 6.0, 8.0 and 10 are critical in defining the clinical course of MS disease [20,41–43]. The results of the analysis were consistent with previous cost–effectiveness studies comparing different DMTs for treatment RRMS using the same EDSS health states classification and the same path for MS disease progression [33–34,40,44]. Our model better reflects the clinical practice in which patients can switch from IFN-β-1a to natalizumab as a second-line therapy [45,46]
While the EMA registered fingolimod as second-line DMT in RRMS, fingolimod was registered in the USA by the FDA as a first-line DMT in RRMS. So far natalizumab registered in the USA as second-line DMT. Since our study is from the USA perspective, natalizumab was used as second-line DMT in treatment of RRMS. The American Academy of Neurology recommended using natalizumab when a previous DMT failed [45]. A previous study suggested that switching to natalizumab is more effective than switching among first-line therapies in RRMS patients who failed a first-line therapy [47]. Our study includes RRMS treatment strategies in which patients use a DMT and if there was insufficient response to that DMT, they would continue on SM alone (Figure 1). This is reflecting the real life in which some patients get frustrated and stop the DMT when they see no response. Moreover, switching to another DMT could be expensive. Patients may have no access to the alternative DMT (e.g., the alternative DMT may not covered by their healthcare plan or even it covered, the out-of-pocket payments is too high and they cannot afford it). Healthcare plans should consider including the cost-effective treatments in their drug formulary.
Study limitations
This cost–effectiveness study used time horizon of 20 years to capture many relevant long-term costs and outcomes of DMTs. Extrapolating the results from randomized controlled trials over long time horizons requires model assumptions that could affect the final results of the study. Many MS patients would remain alive after the 20-year time horizon, and potential long-term benefits and costs associated with the alternative treatment are not completely captured in the study. However, the sensitivity analysis was done and the results of the base-case analysis were not sensitive to the extension of the study time horizon.
The model uses QALYs for assessing the outcomes in the EDSS health states. However, the negative effects of adverse drug events related to DMTs may not be fully included in the QALY used in the analyses.
The SM is different from RRMS patient to another. However, this study assumed that all RRMS patients used SM in all treatment strategies because the study included cohort RRMS patients. This study excluded several possible RRMS treatment alternatives (e.g., switching between first-line therapies). However, switching to natalizumab is considered more effective than switching among first-line therapies in RRMS patients who failed a first-line therapy [47].
Conclusion
The results of this study indicate that all the ICERs for the different treatment strategies evaluated were above the US$100,000 WTP threshold per QALY, and only Strategy 1 (SM) was cost effective. Use of the most expensive DMTs resulted in ICERs that exceeded the WTP typically considered as cost-effective in the USA. The results of the study were no sensitive to changes in the parameters used in the base-case model. More studies are needed to assess the cost and effectiveness of using DMTs in MS patients. Future studies should include all first-line DMTs available in the US market. Changes in the DMTs safety profiles may result in changes in the utility and hence changes in the available study results. Cost-effectiveness studies should be updated as new DMTs access the US market. Future changes in the prices of DMTs may lead to different results.
| Study parameters | Base case | Range of one-way sensitivity analysis | Study (year) | Ref. |
|---|---|---|---|---|
| Annual probability of disease progression (symptom management): | ||||
| – EDSS 0.0–2.5 to EDSS 3.0–5.5 | 0.066972 | Scalfari et al. (2010) | [20] | |
| – EDSS 3.0–5.5 to EDSS 6.0–7.5 | 0.082993 | Scalfari et al. (2010) | [20] | |
| – EDSS 6.0–7.5 to EDSS 8.0–9.5 | 0.066972 | Scalfari et al. (2010) | [20] | |
| Annual probability of relapse (symptom management) | 0.400 | Hoyert and Xu (2012) | [21] | |
| Annual probability of progressing to death: | ||||
| – EDSS 0.0–2.5 | 0.020022 | Hoyert and Xu (2012) | [21] | |
| – EDSS 3.0–5.5 | 0.027815 | Hoyert and Xu (2012) | [21] | |
| – EDSS 6.0–7.5 | 0.036816 | Hoyert and Xu (2012) | [21] | |
| – EDSS 8.0–9.5 | 0.052192 | Hoyert and Xu (2012) | [21] | |
| Annual percent reduction in probability of relapse: | ||||
| – IFN-β-1a | 27% | Filippini et al. (2003), Khan et al. (2002) | [22,23] | |
| – Natalizumab | 68% | Polman et al. (2006), Kerbrat et al. (2011), Dalton et al. (2004) | [24–26] | |
| – Alemtuzumab | 49% | Hartung et al. (2015), CAMMS223 Trial Investigators et al. (2008), Cohen et al. (2012), Coles et al. (2012) | [27–30] | |
| Annual percent reduction in probability of disease progression: | ||||
| – IFN-β-1a | 30% | Filippini et al. (2003), Khan et al. (2002) | [22,23] | |
| – Natalizumab | 21% | Polman et al. (2006) | [24] | |
| – Alemtuzumab | 21% | Hartung et al. (2015) | [27] | |
| Utilities: | ||||
| – EDSS 0.0–2.5 | 0.899 | 0.674–1 | Prosser et al. (2003) | [19] |
| – EDSS 3.0–5.5 | 0.821 | 0.616–1 | Prosser et al. (2003) | [19] |
| – EDSS 6.0–7.5 | 0.769 | 0.577–0.961 | Prosser et al. (2003) | [19] |
| – EDSS 8.0–9.5 | 0.491 | 0.368–0.614 | Prosser et al. (2003) | [19] |
| Utility decrement associated with relapse | 0.094 | 0.071–0.118 | Kobelt et al. (2006) | [15] |
| Annual costs (2014), US$: | ||||
| – WAC for IFN-β-1a | 62,036 | 46,527.00–74,443.20 | RedBook | [14] |
| – WAC for natalizumab | 60,827 | 45,620.25–72,992.40 | RedBook | [14] |
| – WAC for alemtuzumab | 98,750 (1st year) 59,250 | 74,062.50–118,500.00 | RedBook | [14] |
| Annual healthcare costs (2014), US$: | ||||
| – Cost of EDSS 0.0–2.5 | 7742.27 | 5806.70–9677.84 | Kobelt et al. (2006) | [15] |
| – Cost of EDSS 3.0–5.5 | 16,227.30 | 12,170.48–20,284.13 | Kobelt et al. (2006) | [15] |
| – Cost of EDSS 6.0–7.5 | 40,259.82 | 30,194.87–50,324.78 | Kobelt et al. (2006) | [15] |
| – Cost of EDSS 8.0–9.5 | 80,179.74 | 60,134.80–100,224.67 | Kobelt et al. (2006) | [15] |
| Monthly cost of relapse | 5253.84 | 3940.38–6567.29 | Oleen-Burkey et al. (2012) | [16] |
EDSS: Expanded disability status scale; WAC: Wholesale acquisition cost.
| Strategy | Cost (US$) | Incremental cost (US$) | Effect | Incremental effect | ICER |
|---|---|---|---|---|---|
| Strategy 1 (SM alone) | 161,136.60 | – | 10.49 | – | – |
| Strategy 2 (IFN-β-1a) | 551,650.66 | 390,514.06 | 10.66 | 0.17 | 2,297,141.53 |
| Strategy 3 (switch to natalizumab) | 703,463.60 | 151,812.94 | 10.69 | 0.03 | 5,060,431.33 |
| Strategy 4 (switch to alemtuzumab) | 670,985.24 | -32,478.36 | 10.71 | 0.02 | -1,623,918.00 |
In this table, each strategy compared with the strategy mentioned above it (i.e., Strategy 2 compared with Strategy 1, Strategy 3 compared with Strategy 2 and Strategy 4 compared with Strategy 3).
Strategy 1 (SM alone) was the cost-effective strategies for the treatment of relapsing-remitting multiple sclerosis when compared with other strategies at willingness-to-pay = US$50,000/quality-adjusted life year.
ICER: Incremental cost–effectiveness ratio; SM: Symptom management.
Disease-modifying therapies (DMTs) are the major component in the management of multiple sclerosis disease, but their prices increased over time, which raised concerns regarding their cost–effectiveness.
A Markov model was developed to assess the cost–effectiveness and incremental cost–effectiveness ratios (ICERs) for different strategies of using DMTs from a US third-party payer perspective.
The cost–effectiveness comparisons include four strategies. The strategies were symptom management (SM) alone, SM in combination with one of the following: IFN-β-1a, natalizumab (after switching from IFN-β-1a) and alemtuzumab (after using IFN-β-1a, then switching to natalizumab).
Over 20 years, the total costs per patient were estimated at US$161,136.60 for strategy 1 (SM alone), US$551,650.66 for Strategy 2 (SM and IFN-β-1a), US$703,463.60 for Strategy 3 (SM and natalizumab) and US$670,985.24 for Strategy 4 (SM and alemtuzumab).
The accumulated quality-adjusted life years were 10.49, 10.66, 10.69 and 10.71 for each of the four strategies 1–4, respectively. The resulting ICERs were 2,297,141.53 comparing Strategy 2 to Strategy 1 and -1,623,918.00, comparing Strategy 4 to Strategy 3.
All the ICERs for the different treatment strategies evaluated were above the US$100,000 willingness-to-pay threshold per quality-adjusted life year, and only Strategy 1 (SM) was cost-effective.
Previous studies assessed the ICER of IFN-β-1a and natalizumab. However, these studies did not assess the ICER of sequential treatments that reflect the clinical practice and used as the clinically recommended strategy for treatment of relapsing-remitting multiple sclerosis patients. Our study found that the ICERs for the assessed strategies of sequential treatment were significantly higher than the ICER of the individual DMTs described in previous studies.
Acknowledgements
The abstract was presented at the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) 21st Annual International Meeting 2016 (21–25 May 2016 in Washington, DC, USA).
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Noseworthy JH, Lucchinetti C, Rodriguez M, Weinshenker BG. Multiple sclerosis. N. Engl. J. Med. 343(13), 938–952 (2000).
• Provides more information about relapsing-remitting multiple sclerosis (RRMS).
2.
Lutton JD, Winston R, Rodman TC. Multiple sclerosis: etiological mechanisms and future directions. Exp. Biol. Med. (Maywood) 229(1), 12–20 (2004).
• Provides more information about RRMS.
3.
Naci H, Fleurence R, Birt J, Duhig A. Economic burden of multiple sclerosis: a systematic review of the literature. Pharmacoeconomics 28(5), 363–379 (2010).
• Provides more information about RRMS.
4.
Lublin FD, Reingold SC. Defining the clinical course of multiple sclerosis: results of an international survey. National Multiple Sclerosis Society (USA) Advisory Committee on clinical trials of new agents in multiple sclerosis. Neurology 46(4), 907–911 (1996).
•• Explains the importance of disease-modifying therapy (DMT) costs in multiple sclerosis (MS) management and how the costs increase over time.
5.
Lublin FD, Reingold SC, Cohen JA et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology 83(3), 278–286 (2014).
•• Explains the importance of DMT costs in MS management and how the costs increase over time.
6.
Tremlett H, Yinshan Z, Devonshire V. Natural history of secondary-progressive multiple sclerosis. Mult. Scler. 14(3), 314–324 (2008).
•• Explains the importance of DMT costs in MS management and how the costs increase over time.
7.
Koch M, Kingwell E, Rieckmann P, Tremlett H, UBC MS Clinic Neurologists. The natural history of secondary progressive multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 81(9), 1039–1043 (2010).
•• Explains the importance of DMT costs in MS management and how the costs increase over time.
8.
Weiner HL. The challenge of multiple sclerosis: how do we cure a chronic heterogeneous disease? Ann. Neurol. 65(3), 239–248 (2009).
9.
Castro-Borrero W, Graves D, Frohman TC et al. Current and emerging therapies in multiple sclerosis: a systematic review. Ther. Adv. Neurol. Disord. 5(4), 205–220 (2012).
10.
Bin Sawad A, Seoane-Vazquez E, Rodriguez-Monguio R, Turkistani F. Price analysis of multiple sclerosis disease-modifying therapies marketed in the United States. Curr. Med. Res. Opin. 32(11), 1783–1788 (2016).
11.
Schafer JA, Gunderson BW, Gleason PP. Price increases and new drugs drive increased expenditures for multiple sclerosis. J. Manag. Care Pharm. 16(9), 713–717 (2010).
12.
Noyes K, Bajorska A, Chappel A et al. Cost–effectiveness of disease-modifying therapy for multiple sclerosis: a population-based study. Neurology 77(4), 355–363 (2011).
13.
Phillips CJ. The cost of multiple sclerosis and the cost effectiveness of disease-modifying agents in its treatment. CNS Drugs 18(9), 561–574 (2004).
14.
Truven Health Analytics, Inc. Red Book Online [database online]. Greenwood Village, CO, USA. http://micromedex.com/products/product-suites/clinical-knowledge/redbook.
15.
Kobelt G, Berg J, Atherly D, Hadjimichael O. Costs and quality of life in multiple sclerosis: a cross-sectional study in the United States. Neurology 66(11), 1696–1702 (2006).
16.
Oleen-Burkey M, Castelli-Haley J, Lage MJ, Johnson KP. Burden of a multiple sclerosis relapse: the patient's perspective. Patient 5(1), 57–69 (2012).
17.
Weinstein MC, Siegel JE, Gold MR, Kamlet MS, Russell LB. Recommendations of the panel on cost-effectiveness in health and medicine. JAMA 276(15), 1253–1258 (1996).
18.
Siegel JE, Torrance GW, Russell LB, Luce BR, Weinstein MC, Gold MR. Guidelines for pharmacoeconomic studies. Recommendations from the panel on cost effectiveness in health and medicine. Panel on Cost-effectiveness in Health and Medicine. Pharmacoeconomics 11(2), 159–168 (1997).
19.
Prosser LA, Kuntz KM, Bar-Or A, Weinstein MC. Patient and community preferences for treatments and health states in multiple sclerosis. Mult. Scler. 9(3), 311–319 (2003).
20.
Scalfari A, Neuhaus A, Degenhardt A et al. The natural history of multiple sclerosis: a geographically based study 10: relapses and long-term disability. Brain 133(Pt 7), 1914–1929 (2010).
21.
Hoyert DL, Xu J. Deaths: preliminary data for 2011. Natl Vital Stat. Rep. 61(6), 1–51 (2012).
22.
Filippini G, Munari L, Incorvaia B et al. Interferons in relapsing remitting multiple sclerosis: a systematic review. Lancet 361(9357), 545–552 (2003).
23.
Khan O, Zabad R, Caon C, Zvartau-Hind M, Tselis A, Lisak R. Comparative assessment of immunomodulating therapies for relapsing-remitting multiple sclerosis. CNS Drugs 16(8), 563–578 (2002).
24.
Polman CH, O'Connor PW, Havrdova E et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N. Engl. J. Med. 354(9), 899–910 (2006).
25.
Kerbrat A, Le Page E, Leray E et al. Natalizumab and drug holiday in clinical practice: an observational study in very active relapsing remitting multiple sclerosis patients. J. Neurol. Sci. 308(1–2), 98–102 (2011).
26.
Dalton CM, Miszkiel KA, Barker GJ et al. Effect of natalizumab on conversion of gadolinium enhancing lesions to T1 hypointense lesions in relapsing multiple sclerosis. J. Neurol. 251(4), 407–413 (2004).
27.
Hartung HP, Aktas O, Boyko AN. Alemtuzumab: a new therapy for active relapsing-remitting multiple sclerosis. Mult. Scler. 21(1), 22–34 (2015).
28.
CAMMS223 Trial Investigators, Coles AJ, Compston DA et al. Alemtuzumab vs. interferon beta-1a in early multiple sclerosis. N. Engl. J. Med. 359(17), 1786–1801 (2008).
29.
Cohen JA, Coles AJ, Arnold DL et al. Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis: a randomised controlled Phase 3 trial. Lancet 380(9856), 1819–1828 (2012).
30.
Coles AJ, Twyman CL, Arnold DL et al. Alemtuzumab for patients with relapsing multiple sclerosis after disease-modifying therapy: a randomized controlled Phase III trial. Lancet 380(9856), 1829–1839 (2012).
31.
World Health Organization. Cost-effectiveness thresholds. www.who.int/choice/costs/CER_thresholds/en/.
32.
The World Bank. GDP per capita. http://data.worldbank.org/indicator/NY.GDP.PCAP.CD.
33.
Lee S, Baxter DC, Limone B, Roberts MS, Coleman CI. Cost-effectiveness of fingolimod versus interferon beta-1a for relapsing remitting multiple sclerosis in the United States. J. Med. Econ. 15(6), 1088–1096 (2012).
34.
Bell C, Graham J, Earnshaw S, Oleen-Burkey M, Castelli-Haley J, Johnson K. Cost-effectiveness of four immunomodulatory therapies for relapsing-remitting multiple sclerosis: a Markov model based on long-term clinical data. J. Manag. Care Pharm. 13(3), 245–261 (2007).
35.
Hirth RA, Chernew ME, Miller E, Fendrick AM, Weissert WG. Willingness to pay for a quality-adjusted life year: in search of a standard. Med. Decis. Making 20(3), 332–342 (2000).
36.
Braithwaite RS, Meltzer DO, King JT Jr, Leslie D, Roberts MS. What does the value of modern medicine say about the $50,000 per quality-adjusted life-year decision rule? Med. Care 46(4), 349–356 (2008).
37.
Kurtzke J. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33(11), 1444–1452 (1983).
38.
Jacobs LD, Cookfair DL, Rudick RA et al. Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis. The Multiple Sclerosis Collaborative Research Group (MSCRG). Ann. Neurol. 39(3), 285–294 (1996).
39.
Briggs A, Schulper MJ, Claxton K. Decision Modeling for Health Economic Evaluation. Oxford University Press, Oxford, UK (2006).
40.
Earnshaw SR, Graham J, Oleen-Burkey M, Castelli-Haley J, Johnson K. Cost effectiveness of glatiramer acetate and natalizumab in relapsing-remitting multiple sclerosis. Appl. Health Econ. Health Policy 7(2), 91–108 (2009).
41.
Weinshenker BG, Bass B, Rice GP et al. The natural history of multiple sclerosis: a geographically based study. 2. Predictive value of the early clinical course. Brain 112(Pt 6), 1419–1428 (1989).
42.
Kremenchutzky M, Rice GP, Baskerville J, Wingerchuk DM, Ebers GC. The natural history of multiple sclerosis: a geographically based study 9: observations on the progressive phase of the disease. Brain 129(Pt 3), 584–594 (2006).
43.
Scalfari A, Neuhaus A, Daumer M, Deluca GC, Muraro PA, Ebers GC. Early relapses, onset of progression, and late outcome in multiple sclerosis. JAMA Neurol. 70(2), 214–222 (2013).
44.
Jankovic SM, Kostic M, Radosavljevic M et al. Cost-effectiveness of four immunomodulatory therapies for relapsing-remitting multiple sclerosis: a Markov model based on data a Balkan country in socioeconomic transition. Vojnosanit. Pregl. 66(7), 556–562 (2009).
45.
Goodin DS, Cohen BA, O'Connor P, Kappos L, Stevens JC, Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Assessment: the use of natalizumab (Tysabri) for the treatment of multiple sclerosis (an evidence-based review): report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 71(10), 766–773 (2008).
46.
Guo S, Pelligra C, Saint-Laurent Thibault C, Hernandez L, Kansal A. Cost-effectiveness analyses in multiple sclerosis: a review of modelling approaches. Pharmacoeconomics 32(6), 559–572 (2014).
47.
Prosperini L, Gianni C, Leonardi L et al. Escalation to natalizumab or switching among immunomodulators in relapsing multiple sclerosis. Mult. Scler. 18(1), 64–71 (2012).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 25 January 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of different strategies for treatment relapsing-remitting multiple sclerosis. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0056
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Martina Holá, Ondřej Gajdoš, Vojtěch Kamenský, Karolína Kubincová, Cost-Effectiveness Analysis of Multiple Sclerosis Treatment Approaches, Advances in Digital Health and Medical Bioengineering, 10.1007/978-3-031-62520-6_9, (69-77), (2024).
- Nasrin Abulhasanbeigi Gallehzan, Majid Khosravi, Khosro Jamebozorgi, Nazanin Mir, Habib Jalilian, Samira Soleimanpour, Saeed Hoseini, Aziz Rezapour, Abbas Eshraghi, Cost-utility and cost-effectiveness analysis of disease-modifying drugs of relapsing–remitting multiple sclerosis: a systematic review, Health Economics Review, 10.1186/s13561-024-00478-7, 14, 1, (2024).
- Y. Seitaridou, M. Dimitrova, T. Chamova, M. Kamusheva, P. Panayotov, Cost-Effectiveness of Multiple Sclerosis Therapies – A Literature Review, Acta Medica Bulgarica, 10.2478/amb-2022-0046, 49, 4, (69-80), (2023).
- Anggie Wiyani, Lohit Badgujar, Vivek Khurana, Nicholas Adlard, How have Economic Evaluations in Relapsing Multiple Sclerosis Evolved Over Time? A Systematic Literature Review, Neurology and Therapy, 10.1007/s40120-021-00264-1, 10, 2, (557-583), (2021).
- Surachat Ngorsuraches, Nabin Poudel, Incorporating patients’ preferences in the value assessment of disease-modifying therapies for multiple sclerosis: a narrative review, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2021.1880321, 21, 2, (183-195), (2021).
- Anna Mokrova, Susanna Sologova, Victoria Ignatyeva, Modelling expenses for multiple sclerosis treatment, Farmacevticheskoe delo i tehnologija lekarstv (Pharmacy and Pharmaceutical Technology), 10.33920/med-13-2003-01, 3, (11-34), (2020).
- Natalie A. Schwehr, Karen M. Kuntz, Eva A. Enns, Nathan D. Shippee, Elaine Kingwell, Helen Tremlett, Adam F. Carpenter, Mary Butler, Informing Medication Discontinuation Decisions among Older Adults with Relapsing-Onset Multiple Sclerosis, Drugs & Aging, 10.1007/s40266-019-00741-1, 37, 3, (225-235), (2020).
- Natalie A Schwehr, Karen M Kuntz, Mary Butler, Eva A Enns, Nathan D Shippee, Elaine Kingwell, Helen Tremlett, Adam F Carpenter, Age-related decreases in relapses among adults with relapsing-onset multiple sclerosis, Multiple Sclerosis Journal, 10.1177/1352458519866613, 26, 12, (1510-1518), (2019).
- Rafael Bolaños-Díaz, César Sanabria-Montañez, Nilton Custodio-Capuñay, Cost-effectiveness of interferon therapy for multiple sclerosis in Peru: impact of treatment adherence, Journal of Pharmaceutical Health Services Research, 10.1111/jphs.12279, 10, 1, (125-132), (2019).