Ease-of-care from the physical therapists’ perspective comparing fentanyl iontophoretic transdermal system versus morphine intravenous patient-controlled analgesia in postoperative pain management
This article has been corrected.
VIEW CORRECTIONAbstract
Aim: To compare the ease-of-care (EOC) examining time efficiency, convenience and satisfaction of fentanyl iontophoretic transdermal system ([ITS] IONSYS®) and morphine intravenous patient-controlled analgesia (iv. PCA) in postoperative pain management using a validated physical therapist (PT) EOC questionnaire. Materials & methods: This meta-analysis assessed EOC of fentanyl ITS versus morphine iv. PCA using data from two randomized, active-comparator studies (fentanyl ITS: n = 720 and morphine iv. PCA: n = 739) which used the PT EOC questionnaire (22 items grouped into three subscales; time efficiency, convenience and satisfaction). Each item was scored on a 6-point Likert scale. For time efficiency, PT whose average scores were ≤2 on all items of the time efficiency and convenience subscales or ≥4 on both satisfaction items were considered responders. Results: There were EOC questionnaires from 264 (fentanyl ITS) and 254 (morphine iv. PCA) PTs. There were significantly greater proportions of PTs classified as responders for fentanyl ITS than morphine iv. PCA for overall EOC (81.0 vs 55.7%, respectively), time efficiency (83.1 vs 59.5%, respectively), convenience (87.4 vs 72.0%, respectively) and satisfaction (51.9 vs 30.0%, respectively), all p < 0.0001. Conclusion: In this meta-analysis, fentanyl ITS is associated with a superior EOC profile (overall, time efficiency, convenience and satisfaction) from the PTs’ perspective when compared with morphine iv. PCA.
First draft submitted: 8 June 2016; Accepted for publication: 30 June 2016; Published online: 21 July 2016
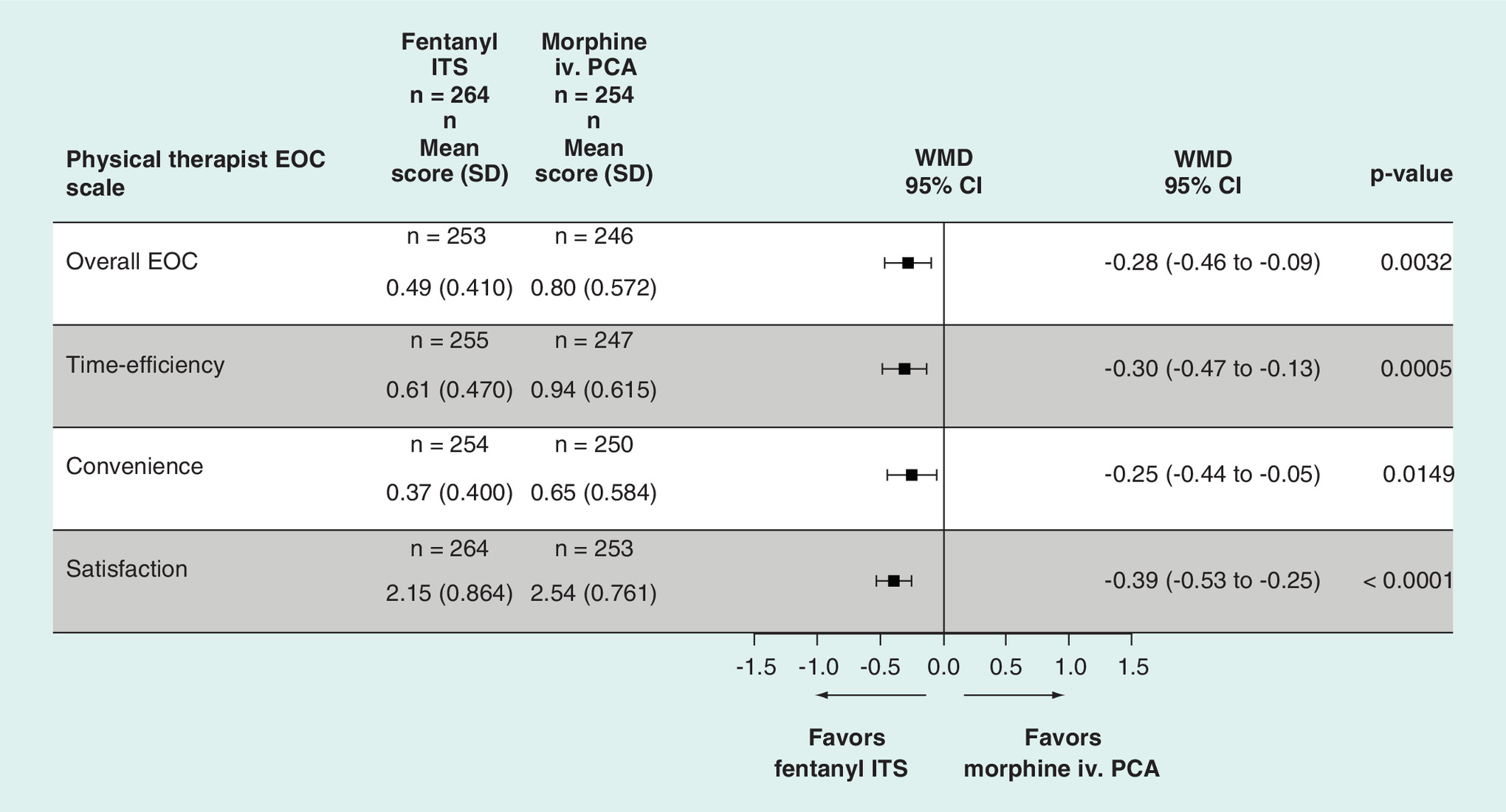
Figure 1. Mean scores for physical therapist ease-of-care.
There was a statistically significant advantage in favor of fentanyl ITS over morphine iv. PCA in the overall score as well as each of the subscale scores. Scores after the last patient completed the study at a site. Items 1–20, higher scores indicate more difficulty caring for patients using the delivery system (0 = not at all, to 5 = a very great deal). Items 21–22, higher scores indicate less satisfaction with the delivery system (1 = extremely satisfied, to 6 = extremely dissatisfied).
EOC: Ease-of-care; ITS: Iontophoretic transdermal system; iv.: Intravenous; n: Number of physical therapist; PCA: Patient-controlled analgesia; SD: Standard deviation; WMD: Weighted mean difference.
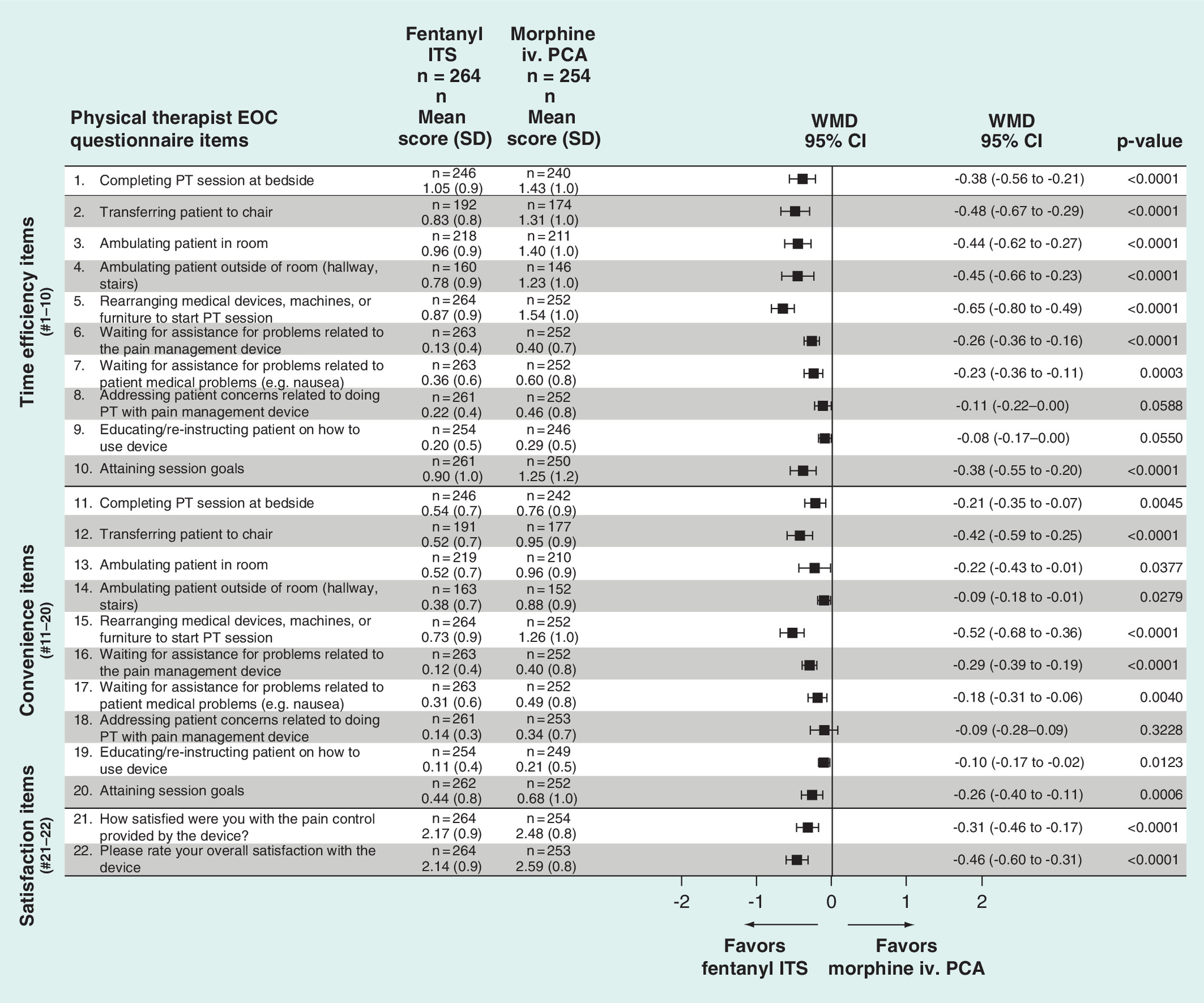
Figure 2. Analysis of ease-of-care from physical therapists by item (mean score).
For the majority of the individual items in the physical EOC (19/22 items) there was a statistically significant advantage for fentanyl ITS over morphine iv. PCA. Scores after the last patient completed the study at a site. Items 1–20, higher scores indicate more difficulty caring for patients using the delivery system (0 = not at all, to 5 = a very great deal). Items 21–22, higher scores indicate less satisfaction with the delivery system (1 = extremely satisfied, to 6 = extremely dissatisfied).
EOC: Ease-of-care; ITS: Iontophoretic transdermal system; iv.: Intravenous; n: Number of physical therapist; PCA: Patient-controlled analgesia; PT: Physical therapist; WMD: Weighted mean difference.
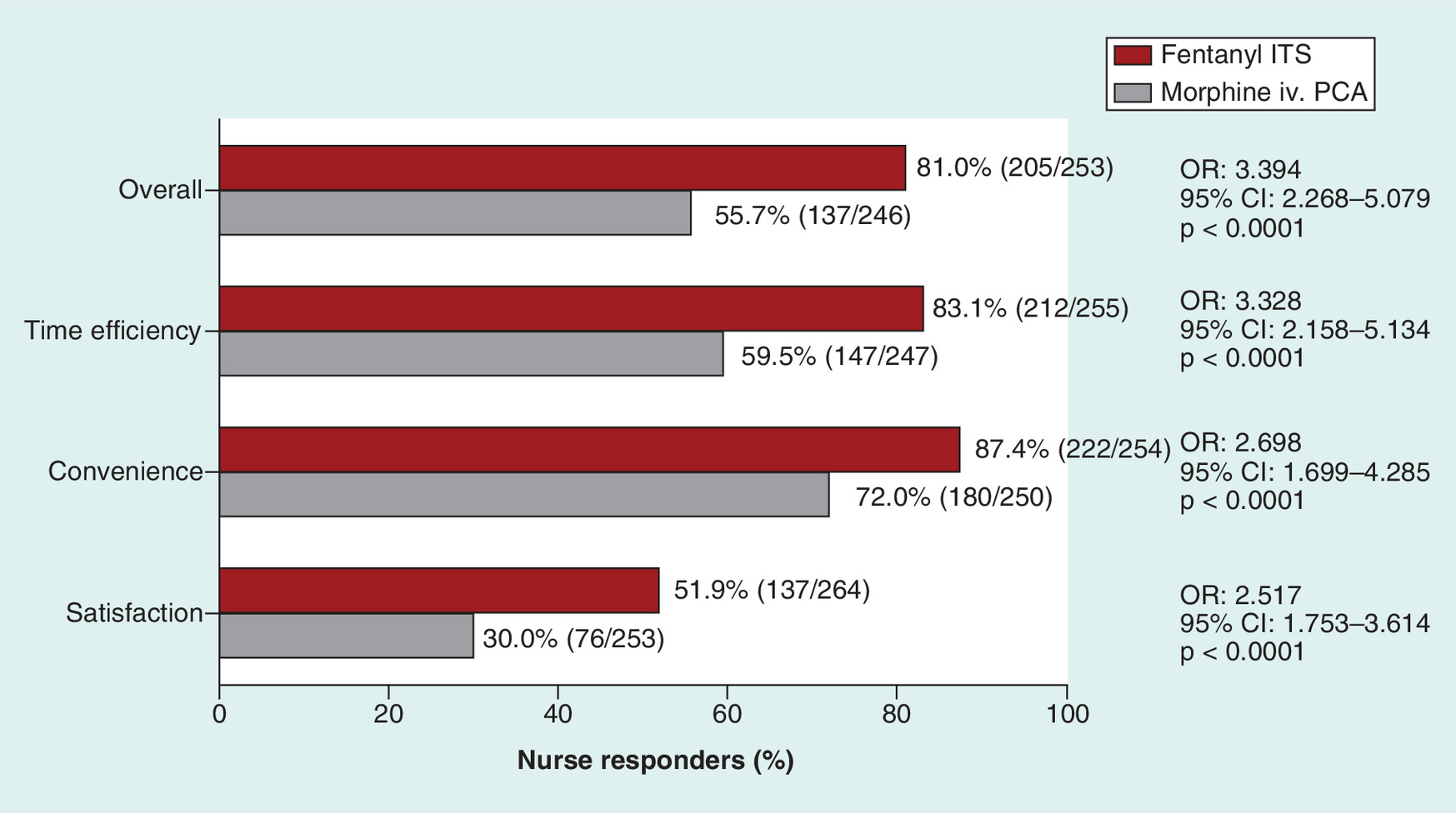
Figure 3. Physical therapist responders for overall, time efficiency, convenience and satisfaction.
Phyisical therapist (PT) responders on the overall score and subscales that measured time efficiency, convenience and satisfaction. A responder for time efficiency and convenience was defined as a PT whose average score was 2 or lower on all items in each respective subscale. A responder on the satisfaction subscale was defined as a PT whose average score was 2 or lower on both subscale items. There were higher percentages of PTs who were responders for the fentanyl ITS system than for the morphine iv. PCA on the overall score and all subscale scores (p < 0.0001).
OR and p-value were based on random effect model for meta-analysis.
ITS: Iontophoretic transdermal system; iv.: Intravenous; OR: Odds ratio; PCA: Patient-controlled analgesia.
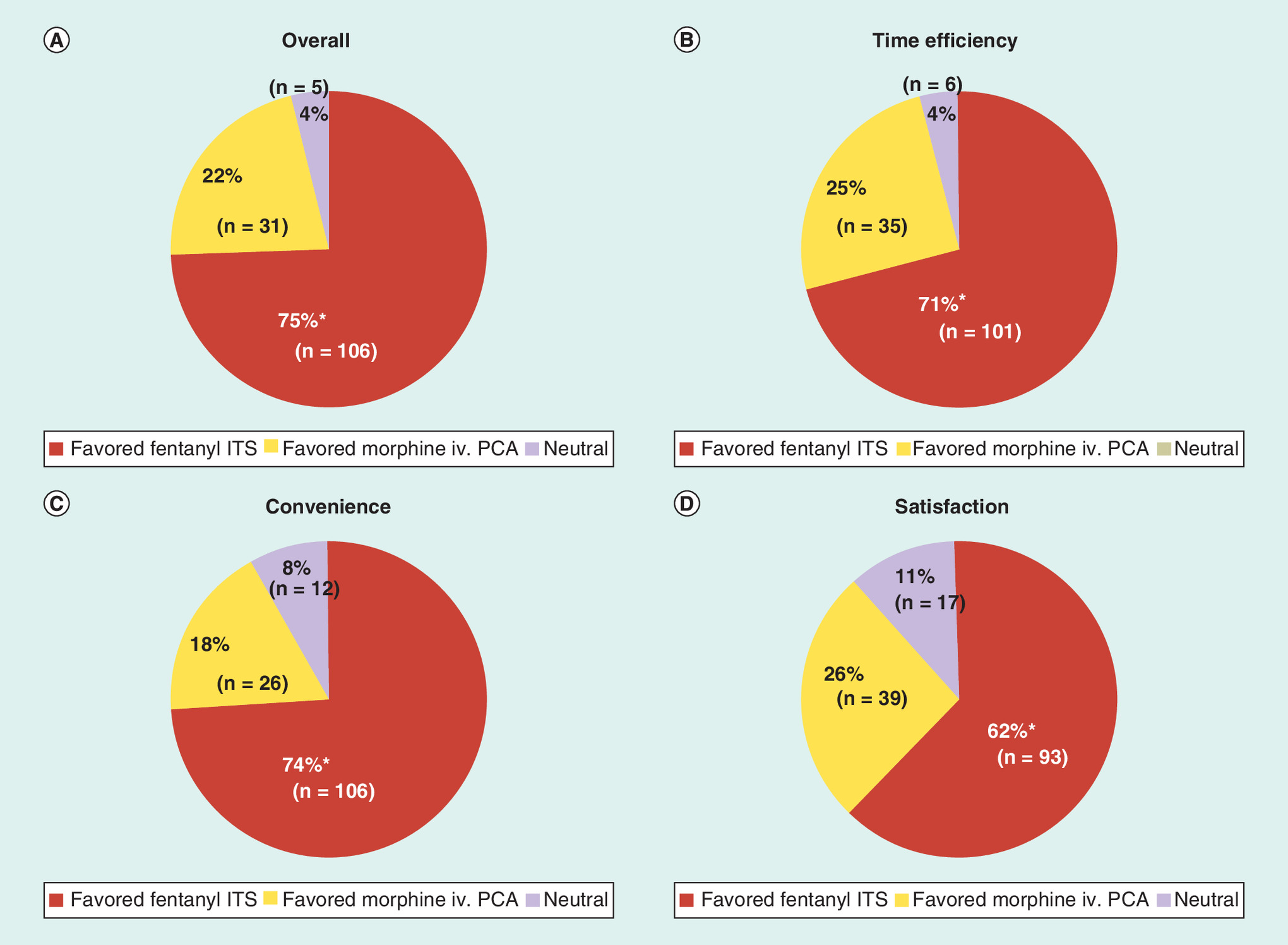
Figure 4. Percentage of physical therapists’ responses that favored each patient-controlled analgesia modality.
(A–D) Percentages of physical therapists’ responses that favored each patient-controlled analgesia modality. Percentages of physical therapists (PTs’) responses that favored each PCA modality (among PTs who treated patients using both modalities). A PT who had a lower mean score on a given subscale for patients who received fentanyl ITS compared with patients who received morphine iv. PCA was considered to have favored fentanyl ITS over morphine iv. PCA on that subscale and vice versa; if a PT had equal mean scores for both treatment groups, he or she was considered to have been neutral toward either modality on that subscale.
*p < 0.0001; p-values were calculated using the sign test.
ITS: Iontophoretic transdermal system; iv.: Intravenous; PCA: Patient-controlled analgesia; PT: Physical therapist.
Patient-controlled analgesia (PCA), frequently administered via an intravenous (iv.) route of administration, is often utilized for pain management in postoperative patients [1–5]. Early mobilization and implementation of inpatient rehabilitation programs are important elements in the postoperative recovery period that can help prevent morbidities associated with surgery and provide an essential foundation for long-term recovery [6–11]. Enhanced recovery after surgery and anesthesia (ERAS) pathways have early mobilization as an integral part of their postoperative protocols [12–18]. However, iv. PCA can often limit mobility due to the incumbrance of iv. lines and thereby affect the implementation of physical therapy.
Fentanyl iontophoretic transdermal system ([ITS] IONSYS®, The Medicines Company, NJ, USA) is a pre-programmed, needle-free PCA approach for the management of moderate-to-severe acute postoperative pain by administering analgesia using iontophoresis which provides transdermal delivery of fentanyl via the application of a low-intensity, nearly imperceptible electrical field [19]. The system is assembled immediately prior to application to the upper outer arm or chest of patient. The patient can administer a dose of fentanyl by pressing the button twice on the system within 3 s. Fentanyl ITS has been evaluated in three placebo-controlled and four active-comparator randomized controlled trials in adult patients with postoperative pain management [20–26]. In the placebo-controlled studies, fentanyl ITS was significantly more efficacious than placebo and in the active-comparator studies, fentanyl ITS was shown to be similarly efficacious and tolerated when compared with morphine iv. PCA.
Ease-of-care (EOC) for physical therapists (PTs) is important to measure with any technology in the postoperative setting. A validated EOC questionnaire from the PTs’ perspective was utilized in two of the adult active-comparator trials [27]. A previously published paper reported the results of one of the two studies [28]. In this current paper, we conducted a meta-analysis of the EOC from the PTs’ perspective comparing fentanyl ITS to morphine iv. PCA using data from the two Phase III trials that utilized this outcome measure.
Materials & methods
During the clinical development program for fentanyl ITS, there were two Phase IIIB clinical trials that included the PT EOC questionnaire and both are included in this meta-analysis. The two multicenter, active-comparator, randomized studies included in this meta-analysis included adult postoperative patients who had undergone a variety of surgical procedures (Table 1). Methodologies for the two included studies have been previously reported [20,21]. Patients were randomly assigned to receive either fentanyl ITS 40 μg dose over 10 min for up to 6 doses/h for 24 h or a maximum of 80 doses per system, whichever occurred first, after which a new system could be applied if needed, or morphine iv. PCA 1 mg morphine bolus doses for up to 10 doses/h for 24 h (up to a maximum of 240 doses). The meta-analysis was conducted according to the Cochrane methodology [29].
PTs completed a validated PT EOC questionnaire [27] after each therapy session. A minimum percentage of response (>60%) was required for a questionnaire to be included in the analysis. The domains for the PT EOC Questionnaires include time efficiency (measures the time efficiency associated with completing patient-care tasks), convenience (measures the convenience of completing patient-care tasks) and satisfaction. Each item on the EOC questionnaire that contributed to the Overall EOC (time efficiency items #1–10 and convenience items #11–20) was scored on a 6-point Likert scale ranging from ‘not at all’ (0) to ‘a very great deal’ time-consuming or bothersome, respectively (5). Items on the satisfaction subscale include response options on a 6-point Likert scale ranging from ‘extremely dissatisfied’ (1) to ‘extremely satisfied’ (6). However, for purposes of the analyses in this paper we transformed satisfaction scale so that lower scores indicated more favorable results for ease of interpretation (i.e., extremely dissatisfied was originally a 1 but was transformed to a 6 and extremely satisfied was a 6 but was transformed to a 1).
A PT could complete multiple questionnaires in which case the mean score from all questionnaires filled out by an individual PT was used to determine his or her responder status.
Statistical analysis
The meta-analysis was conducted using random effects models [29], with fixed effect models being explored as secondary analyses. The random effects method is usually more conservative, with confidence intervals that are likely to be wider than those from a fixed effects analysis, and has been used previously in Cochrane evaluations of this and other clinical areas [2,29]. The software used in the statistical analysis was SAS version 9.3.
PT EOC evaluation on fentanyl ITS and morphine iv. PCA was compared by meta-analysis. The differences in responses on the PT EOC questionnaire were assessed by use of mean and rate of responders. Mean scores were calculated for each individual item in the questionnaire and for the overall EOC as well as the subscales (time efficiency [items 1–10], convenience [items 11–20] and satisfaction [items 21 and 22]). Lower mean scores indicate better responses from the PTs. In addition to evaluating mean scores, post hoc analyses were completed evaluating responders. On the time efficiency and convenience subscales, a responder was defined as a PT whose average score was 2 or lower on all times in each respective subscale. A responder on the satisfaction subscale was defined as a PT whose average score was 2 or lower on both subscale items. Lower scores indicated a more positive response.
The percentage of PTs who favored each modality was calculated. In order to be included in this analysis the PT had to have conducted sessions with patients from both treatment groups. A PT with a lower mean score on a given subscale for patients who received fentanyl ITS compared with patients who received morphine iv. PCA was considered to have favored fentanyl ITS over morphine iv. PCA on that subscale score or vice versa. If the PT had equal mean scores for both treatment groups they were considered neutral toward either modality on that subscale.
For continuous variables, the weighted mean difference (WMD) between treatments was calculated. For dichotomous variables, odds ratios indicating the probability of the outcome to occur for a patient receiving fentanyl ITS versus morphine iv. PCA were calculated. Statistical tests were performed at the 0.05 significance level, with no multiplicity adjustments. 95% CIs were provided for all parameters.
Results
PT EOC analyses were based on responses to questionnaires from 264 (fentanyl ITS) and 254 (morphine iv. PCA) respondents; PTs provided care for patients from either one or both treatment groups. Patients treated with fentanyl ITS and morphine iv. PCA had similar demographics (Table 1). The mean age of patients in the included studies ranged from 53.0 to 62.8 years of age with the majority being female.
PT ease-of-care
Mean score comparisons
Fentanyl ITS was statistically significantly better compared with morphine iv. PCA in terms of PTs’ Overall EOC (WMD = -0.28; p = 0.0032; Figure 1). Additionally, there was a statistically significant benefit in each of the subscales favoring fentanyl ITS over morphine iv. PCA including time efficiency (WMD = -0.30; p = 0.0005), convenience (WMD = -0.25; p = 0.0149) and satisfaction (WMD = -0.39; p < 0.0001) (Figure 1). For the majority of the individual items in the physical EOC (19/22 items) there was a statistically significant advantage for fentanyl ITS over morphine iv. PCA (Figure 2).
Responder data
There was a statistically significantly larger proportion of PTs who were considered responders for fentanyl ITS compared with morphine iv. PCA on the overall EOC (81.0 vs 55.7%, respectively; p < 0.0001), time efficiency subscale (83.1 vs 59.5%, respectively; p < 0.0001), convenience subscale (87.4 vs 72.0%, respectively; p < 0.0001) and satisfaction subscale (51.9 vs 30.0%, respectively; p < 0.0001) (Figure 3).
Responses of physical therapists who evaluated both fentanyl ITS & morphine iv. PCA
There was a statistically significantly larger proportion of PTs (of those who had experience with both systems) who favored fentanyl ITS compared with morphine iv. PCA on the overall EOC (75 vs 22%, respectively; p < 0.0001), time efficiency subscale (71 vs 25%, respectively; p < 0.0001), convenience subscale (74 vs 18%, respectively; p < 0.0001) and satisfaction subscale (62 vs 26%, respectively; p < 0.0001) (Figure 4).
Discussion
This is the first meta-analysis conducted utilizing the validated PTs’ EOC comparing fentanyl ITS with morphine iv. PCA. Findings from this meta-analysis indicated that fentanyl ITS is significantly better compared with morphine iv. PCA in terms of EOC from the PTs’ perspective (overall, time efficiency, convenience and satisfaction) using a validated tool [27].
For PTs who were exposed to both fentanyl ITS and morphine iv. PCA there were more who favored fentanyl ITS on each of the three subscales (i.e., time efficiency, convenience and satisfaction) and on the overall in this meta-analysis. The time efficiency and convenience subscales asked the same 10 items but from two perspectives (i.e., time and convenience). These items included such things as completing physical therapy sessions and attaining session goals, transferring and ambulating patients and interference with devices or machines. All of these items are important in the physical therapy that patients receive. Previous reports have also indicated that nurses also favor fentanyl ITS over morphine iv. PCA when they have worked with both systems [30].
ERAS protocols strive to reduce surgical stress, maintain postoperative function and enhance mobilization after surgery [13]. Fentanyl ITS use may allow for early mobilization that is indicated in ERAS protocols [13–18,31–32]. In the current analysis, PTs favored fentanyl ITS over morphine iv. PCA in terms of all of the applicable mobility items (i.e., transferring patient and ambulation) in the PT EOC questionnaire.
The results of this analysis are consistent with the previous paper that evaluated only one of the two Phase IIIB studies conducted that included the PT EOC as an outcome measure [28]. However, this current paper includes a more diverse patient population in terms of different surgical types. The first paper focused on orthopedic surgeries while this paper also includes abdominal, pelvic and general surgeries. It is important to note that the advantage of conducting a meta-analysis is that it should be possible to detect treatment effects with greater power and estimate these effects with greater precision [33].
The EOC questionnaire is a validated instrument [27]. The validation process included correlation of results to the clinical data, adding strength to the instrument validation and these clinical study findings. Additionally, the validation showed that PTs rated most parameters as satisfactory, such that any change is notable. Complementing these Likert scale differences, the overall percent differences in time efficiency, convenience and satisfaction are larger, further supporting the clinical relevance of the physical therapy related study findings. Specifically, what we see from Figure 1 and Figure 4 is that WMD between 0.25 and 0.35 on a 6-point Likert scale with regard to EOC for a PT resulted 15.4–25.3% more responders in patients who were treated by fentanyl ITS compared with those treated by morphine iv. PCV. Hence a WMD between 0.25 and 0.35 is a clinically meaningful improvement in favor of fentanyl ITS.
Respiratory depression is a serious adverse event that may occur with the administration of opioid medications. In the four head-to-head clinical trials, there were four cases of clinically relevant respiratory depression (defined as the simultaneous occurrence of bradypnea [<8 breaths/min] and excessive sedation [patient not easily aroused]) [34]. In all four cases, the patients had been randomized and received morphine iv. PCA. However, as with administration with all opioids, it is important to monitor for signs of respiratory depression during fentanyl ITS administration.
Fentanyl ITS should be applied to intact, nonirritated and nonirradiated skin on the chest or upper outer arm. Topical skin reactions (erythema, sweating, vesicles, papules/pustules) may occur after removal of fentanyl ITS but are typically limited to the application site area. During the clinical development program, most of the skin reactions were classified as mild or moderate in severity. In the study conducted by Grond and colleagues they utilized a separate form specifically for the reporting of application-site reactions, compared with general adverse event form which led to a higher incidence of all application-site reactions [20]. However, it is important to note that even though there were more skin reactions observed with fentanyl ITS, this finding did not translate into greater interruptions in pain control compared with morphine iv. PCA [20]. According to the US prescribing information for fentanyl ITS, if a severe skin reaction is observed, the fentanyl ITS should be removed and further use discontinued.
A limitation of this analysis is that the studies that comprised the meta-analysis were open-label in terms of their design. Both the patient and PT were aware of the treatment that the patient had been receiving. However, this is an advantage in terms of analysis that evaluated which system PTs preferred. If the system was blinded this analysis would not have been possible.
Conclusion
Fentanyl ITS has been shown to be as effective and equally as well tolerated as morphine iv. PCA in acute postoperative pain management in four Phase III randomized clinical trials in a variety of different types of surgery [20–23]. Therefore, the decision for the healthcare provider becomes not so much about the effectiveness of the opioid pain management but rather needs to focus on what are the other benefits or limitations of each system. In this analysis, fentanyl ITS was superior to morphine iv. PCA from the PTs’ perspective in terms of EOC. Patient mobility is central to many ERAS protocols and therefore fentanyl ITS, which is self-contained and does not require an iv. pole or pump, has potential advantages over traditional iv. PCA treatments.
| Parameter | Grond [20] | Hartrick [21] | ||
|---|---|---|---|---|
| Fentanyl ITS | Morphine iv. PCA | Fentanyl ITS | Morphine iv. PCA | |
| Location | Europe | USA | ||
| Surgery type | Orthopedic, abdominal, pelvic, general | Hip replacement | ||
| Evaluable population (n) | 322 | 334 | 389 | 397 |
| Sex, n (%): | ||||
| – Female | 184 (57.1) | 190 (56.9) | 204 (52.4) | 202 (50.9) |
| – Male | 138 (42.9) | 144 (43.1) | 185 (47.6) | 195 (49.1) |
| Age (years), mean (SD) | 53.4 (14.5) | 53.0 (14.6) | 62.8 (12.0) | 62.8 (12.4) |
| BMI (kg/m2), mean (SD) | – | – | 29.7 (5.5) | 29.2 (5.5) |
| Race, n (%): | ||||
| – Caucasian | 305 (94.7) | 322 (96.4) | 356 (91.5) | 365 (91.9) |
| – Black | 4 (1.2) | 6 (1.8) | 24 (6.2) | 21 (5.3) |
| – Asian | 2 (0.6) | 2 (0.6) | 3 (0.8) | 0 |
| – Hispanic | 0 | 0 | 5 (1.3) | 6 (1.5) |
| – Other/unknown | 11 (3.4) | 4 (1.2) | 1 (0.3) | 5 (1.3) |
ITS: Iontophoretic transdermal system; iv.: Intravenous; PCA: Patient-controlled analgesia; SD: Standard deviation.
Fentanyl iontophoretic transdermal system (ITS) has been shown to be as effective and equally as well tolerated as morphine intravenous patient-controlled analgesia (iv. PCA) in acute postoperative pain management in clinical trials in a variety of different types of surgery.
Early patient mobility is central to postoperative recovery, including enhanced recovery after surgery and anesthesia protocols, and is critical for patients to have better outcomes.
Fentanyl ITS is a pre-programmed, needle-free patient-controlled analgesia approach for the management of acute postoperative pain that does not require an iv. pole or pump and therefore, may improve patient mobility.
Physical therapists (PTs) favored fentanyl ITS over morphine iv. PCA in terms of all of the applicable mobility items (i.e., transferring patient and ambulation) in the PT ease-of-care questionnaire.
In this analysis, fentanyl ITS was superior to morphine iv. PCA from the PTs’ perspective in terms of overall ease-of-care.
PTs found that fentanyl ITS was superior to morphine iv. PCA in terms of time efficiency.
PTs found that fentanyl ITS was superior to morphine iv. PCA in terms of convenience.
PTs found that fentanyl ITS was superior to morphine iv. PCA in terms of satisfaction.
Acknowledgements
The authors thank Starr Grundy, of SD Scientific, Inc., for medical writing support with this manuscript.
Financial & competing interests disclosure
The analyses and writing of this manuscript were supported financially by The Medicines Company. C Hartrick is on the speakers bureau for The Medicines Company. J Abraham and L Ding are employees of The Medicines Company (Parsippany, NJ, USA). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support was provided by Starr Grundy, of SD Scientific, Inc., and was funded by The Medicines Company.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Creative Commons Attribution-NonCommercial 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Miaskowski C. Patient-controlled modalities for acute postoperative pain management. J. Perianesth. Nurs. 20(4), 255–267 (2005).
2.
Hudcova J, McNicol E, Quah C, Lau J, Carr DB. Patient controlled opioid analgesia versus conventional opioid analgesia for postoperative pain. Cochrane Database Syst. Rev. 4, CD003348 (2006).
3.
Walder B, Schafer M, Henzi I, Tramer MR. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain. A quantitative systematic review. Acta Anaesthesiol. Scand. 45(7), 795–804 (2001).
4.
American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 116(2), 248–273 (2012).
5.
Bainbridge D, Martin JE, Cheng DC. Patient-controlled versus nurse-controlled analgesia after cardiac surgery – a meta-analysis. Can. J. Anaesth. 53(5), 492–499 (2006).
6.
Markey DW, Brown RJ. An interdisciplinary approach to addressing patient activity and mobility in the medical-surgical patient. J. Nurs. Care Qual. 16(4), 1–12 (2002).
7.
Czaplijski T, Marshburn D, Hobbs T, Bankard S, Bennett W. Creating a culture of mobility: an interdisciplinary approach for hospitalized patients. Hosp. Top. 92(3), 74–79 (2014).
8.
Sanguineti VA, Wild JR, Fain MJ. Management of postoperative complications: general approach. Clin. Geriatr. Med. 30(2), 261–270 (2014).
9.
Young AC, Buvanendran A. Pain management for total hip arthroplasty. J. Surg. Orthop. Adv. 23(1), 13–21 (2014).
10.
Freeman R, Maley K. Mobilization of intensive care cardiac surgery patients on mechanical circulatory support. Crit. Care Nurs. Q. 36(1), 73–88 (2013).
11.
Paterno MV, Archdeacon MT, Ford KR, Galvin D, Hewett TE. Early rehabilitation following surgical fixation of a femoral shaft fracture. Phys. Ther. 86(4), 558–572 (2006).
12.
Eras® Society. ERAS Protocol (EP). www.erassociety.org/index.php/eras-care-system/eras-protocol.
13.
Gustafsson UO, Scott MJ, Schwenk W et al. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS[R]) Society recommendations. Clin. Nutr. 31(6), 783–800 (2012).
14.
Gustafsson UO, Scott MJ, Schwenk W et al. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS[R]) Society recommendations. World J. Surg. 37(2), 259–284 (2013).
15.
Lassen K, Coolsen MM, Slim K et al. Guidelines for perioperative care for pancreaticoduodenectomy: Enhanced Recovery After Surgery (ERAS[R]) Society recommendations. World J. Surg. 37(2), 240–258 (2013).
16.
Lassen K, Coolsen MM, Slim K et al. Guidelines for perioperative care for pancreaticoduodenectomy: Enhanced Recovery After Surgery (ERAS[R]) Society recommendations. Clin. Nutr. 31(6), 817–830 (2012).
17.
Nygren J, Thacker J, Carli F et al. Guidelines for perioperative care in elective rectal/pelvic surgery: Enhanced Recovery After Surgery (ERAS[R]) Society recommendations. Clin. Nutr. 31(6), 801–816 (2012).
18.
Nygren J, Thacker J, Carli F et al. Guidelines for perioperative care in elective rectal/pelvic surgery: Enhanced Recovery After Surgery (ERAS[R]) Society recommendations. World J. Surg. 37(2), 285–305 (2013).
19.
Batheja P, Thakur R, Michniak B. Transdermal iontophoresis. Expert Opin. Drug. Deliv. 3(1), 127–138 (2006).
20.
Grond S, Hall J, Spacek A, Hoppenbrouwers M, Richarz U, Bonnet F. Iontophoretic transdermal system using fentanyl compared with patient-controlled intravenous analgesia using morphine for postoperative pain management. Br. J. Anaesth. 98(6), 806–815 (2007).
•• This reports the methodology for one of the two studies included in this meta-analysis.
21.
Hartrick CT, Bourne MH, Gargiulo K, Damaraju CV, Vallow S, Hewitt DJ. Fentanyl iontophoretic transdermal system for acute-pain management after orthopedic surgery: a comparative study with morphine intravenous patient-controlled analgesia. Reg. Anesth. Pain Med. 31(6), 546–554 (2006).
•• This reports the methodology for one of the two studies included in this meta-analysis.
22.
Minkowitz HS, Rathmell JP, Vallow S, Gargiulo K, Damaraju CV, Hewitt DJ. Efficacy and safety of the fentanyl iontophoretic transdermal system (ITS) and intravenous patient-controlled analgesia (IV PCA) with morphine for pain management following abdominal or pelvic surgery. Pain Med. 8(8), 657–668 (2007).
• This reports one of the four active-comparator trials conducted during the Phase III program.
23.
Viscusi ER, Reynolds L, Chung F, Atkinson LE, Khanna S. Patient-controlled transdermal fentanyl hydrochloride vs intravenous morphine pump for postoperative pain: a randomized controlled trial. JAMA 291(11), 1333–1341 (2004).
• This reports one of the four active-comparator trials conducted during the Phase III program.
24.
Chelly JE, Grass J, Houseman TW, Minkowitz H, Pue A. The safety and efficacy of a fentanyl patient-controlled transdermal system for acute postoperative analgesia: a multicenter, placebo-controlled trial. Anesth. Analg. 98(2), 427–433 (2004).
• This reports one of the three placebo-controlled trials conducted during the Phase III program.
25.
[The Medicines Company, Data on File].
26.
Viscusi ER, Reynolds L, Tait S, Melson T, Atkinson LE. An iontophoretic fentanyl patient-activated analgesic delivery system for postoperative pain: a double-blind, placebo-controlled trial. Anesth. Analg. 102(1), 188–194 (2006).
• This reports one of the three placebo-controlled trials conducted during the Phase III program.
27.
Harding G, Vallow S, Leidy NK et al. Ease of care with patient controlled analgesia systems: questionnaire development and validation. J. Adv. Nurs. 59(5), 530–541 (2007).
• This reports the validation of the physical therapist ease-of-care questionnaire.
28.
Bourne MH, Chelly JE, Damaraju CV, Nelson WW, Schein JR, Hewitt DJ. Physical therapists’ perceptions of ease of care in patients receiving 2 forms of analgesia after total hip arthroplasty. Phys. Ther. 90(5), 707–713 (2010).
•• This reports the physical therapist ease-of-care results from the Hartrick (2006) study.
29.
Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. www.cochrane-handbook.org.
30.
Lindley P, Pestano CR, Gargiulo K. Comparison of postoperative pain management using two patient-controlled analgesia methods: nursing perspective. J. Adv. Nurs. 65(7), 1370–1380 (2009).
31.
Cerantola Y, Valerio M, Persson B et al. Guidelines for perioperative care after radical cystectomy for bladder cancer: Enhanced Recovery After Surgery (ERAS[R]) society recommendations. Clin. Nutr. 32(6), 879–887 (2013).
32.
Mortensen K, Nilsson M, Slim K et al. Consensus guidelines for enhanced recovery after gastrectomy: Enhanced Recovery After Surgery (ERAS[R]) Society recommendations. Br. J. Surg. 101(10), 1209–1229 (2014).
33.
Petrie A, Sabin C. Systematic reviews and meta-analysis. In: Medical Statistics at a Glance, (Eds). Wiley-Blackwell, Oxford, UK (2009).
34.
Viscusi ER, Grond S, Ding L, Danesi H, Jones JB, Sinatra RS. A comparison of opioid-related adverse events with fentanyl iontophoretic transdermal system versus morphine intravenous patient-controlled analgesia in acute postoperative pain. Pain Manag. 6(1), 19–24 (2016).
Information & Authors
Information
Published In
Copyright
© The Medicine Company.
History
Published online: 21 July 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Ease-of-care from the physical therapists’ perspective comparing fentanyl iontophoretic transdermal system versus morphine intravenous patient-controlled analgesia in postoperative pain management. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0038
Export citation
Select the citation format you wish to export for this article or chapter.