Maximizing the impact of real-world evidence on cancer treatment: what do we need to achieve it?
Publication: Journal of Comparative Effectiveness Research
Abstract
There is an increasing number of studies using real-world data to examine outcomes of drugs in clinical practice. Therefore, it is crucial to carefully evaluate their quality and findings, extract valuable insights, acknowledge their limitations and identify gaps to advance further their use in decision-making. Here we provide an overview of the opportunities offered throughout drug lifecycle, and challenges presented by real-world evidence (RWE) studies. We also highlight the importance of the culture of transparency, along with the development of good practices for reporting RWE studies. In addition, we review common biases and other methodological aspects that can undermine the potential insights a real-world oncology study can provide. We briefly illustrate some questions that RWE studies address that can help us guide clinical decisions. Several possible future directions expected to contribute for RWE improving cancer patients' outcomes emerge, from prospective data collection initiatives to normalization of biomarker data integration or collaborative data sharing platforms.
Plain language summary: Making the most of real-world data in cancer treatment: what is needed to succeed?
What is the context?
The use of real-world data (RWD) to assess drug outcomes in clinical practice is increasing, highlighting the importance of evaluating their quality and findings to derive valuable insights and identify areas for improvement. RWD can be derived from various sources, which can include, but are not limited to, information stored in paper or electronic health records, pharmacy records or billing data, insurance claims, retrospective or prospective disease or product-specific registries, death certificates, patient-reported outcomes and other patient-generated data, like those from mobile or wearable devices/digital health solutions outside of conventional clinical trials.
What is this article about?
This article overviews the opportunities offered throughout drug lifecycle, and challenges presented by studies using RWD, which generate real-world evidence (RWE). It emphasizes the need to account for confounding variables and discusses which might be the most appropriate outcomes for RWE studies in cancer. It also highlights the importance of the culture of transparency to enhance confidence in RWD generating processes, along with the development of good practices for reporting RWE studies. Common biases and other methodological aspects to consider in RWE studies are also presented, as well as few examples illustrating some questions that RWE studies can address to help guide clinical decisions. Finally, we expose several possible future directions expected to contribute to RWE improving cancer patients' outcomes, from prospective data collection initiatives to normalization of biomarker data integration or collaborative data sharing platforms.
Background
Traditionally and continuously, the assessment of drugs' clinical benefit relied on evidence from randomized clinical trials (RCTs). However, the increased number of real-world studies about the effectiveness, safety, and use of medical interventions outside the controlled settings of traditional clinical trials, indicates significant interest in complementary sources of evidence, particularly in oncology [1–4]. The relevance and applicability of real-world evidence (RWE) in substantiating, enhancing or potentially supplanting clinical trials throughout the drug lifecycle have gained increased recognition within the sphere of oncology and drug development [5]. RWE has potential to inform clinical practice, support regulatory reviews, health technology assessments, reimbursement decisions and price negotiations for novel therapies [6].
Real-world data (RWD) can be derived from various sources, which can include, but are not limited to, information stored in paper or electronic health records (EHRs), pharmacy records or billing data, insurance claims, retrospective or prospective disease or product-specific registries, death certificates, patient-reported outcomes (PROs) and other patient-generated data, like those from mobile or wearable devices/digital health solutions outside of conventional clinical trials [5,7,8]. New data sources are likely to emerge in the future [9].
Here we overviewed the opportunities offered throughout drug lifecycle, and challenges presented by RWE studies. Moreover, we went through common biases and other methodological aspects that can undermine the potential insights a real-world oncology study can provide, and we briefly illustrate some questions that RWE studies address that can help guide clinical decisions.
Opportunities & challenges of RWE studies
RWE stands as a vital component in monitoring medicines, complementing and enhancing evidence gathered in RCTs, and allows capturing real clinical practice, adherence, compliance and medication performance in real-life settings [10]. Together with RCTs, RWE can enhance our understanding of disease management and aid in treatment decisions in routine clinical settings. Other opportunities offered by RWE studies are shown in Table 1. However, despite concerted efforts by regulatory bodies such as the US FDA and the EMA to standardize and regulate its application in supporting medicines approval, challenges persist around the use of RWD. These include, among several others (Table 1), mistrust and misunderstanding of RWD captured, EHR systems not built to use in generating RWE, lack of knowledge about full spectrum of RWE studies and inability to distinguish high- and low-quality RWE.
| Opportunities | Refs | Challenges | Refs |
|---|---|---|---|
| Gather comprehensive insights into both common and rare AEs, and those attributed to metabolism differences in diverse racial and genetic groups due to longer follow-ups in larger and more diverse populations | [5,10,11] | Dispersion of databases, often held by different institutions, or when care is provided in multiple sites, poses obstacles to accessing and linking data promptly | [6,13] |
| Identification of predictors of treatment response heterogeneity, prognostic evaluations | [12] | Lack of harmonization in criteria for RWD collection, coding or documentation between organizations or within organizations over time, data access, governance, availability and system interoperability | [6,13] |
| Cost reduction in monitoring long-term outcomes for degenerative and chronic diseases | [10] | Limited availability of clinically relevant structured data elements to be readily extracted from EHRs and compared across systems | [13] |
| Valuable in geriatrics and pediatrics (e.g., historical control arms in pediatric investigation plans) | [10] | Underreporting, especially in case of AEs | [11] |
| Biomarker validation; elaborate on clinicogenomic datasets, rare subpopulations genetically-defined | [10] | Improve the collection and analysis of EHR data, like increased use of PROs as part of routine clinical care and more widespread use of medical device surveillance initiatives | [14] |
| Broader representativeness (higher external validity) and evidence for patient subgroups that are commonly under-represented or excluded from clinical trials | [12] | Full accessibility of many observational datasets in advance of designing specific RWD studies makes preregistration of RWD analysis† challenging | [11] |
| Perform virtual comparative effectiveness studies, use historical (or external) control arms to compare RWD against an uncontrolled treatment arm in a clinical trial, perform studies using synthetic (real-world) control arms to pair with an uncontrolled treatment arm from clinical trial | [11] | Differences in patient populations, care patterns, and data collection in clinical practice impose unique considerations for real-world end point development‡ | [15] |
†
Effective approach to reduce the risk of multiple hypotheses testing and p-hacking.
‡
Overall survival (OS) and other major end points such as hospitalizations can align, but there is significant disconnect for surrogate end points common in oncology, such as objective response rate (ORR) and progression-free survival (PFS) measured by Response Evaluation Criteria in Solid Tumors (RECIST), whose likelihood of being captured in the real-world is low [16].
AE: Adverse event; EHR: Electronic health record; PRO: Patient-reported outcome; RWD: Real-world data.
Types of insights provided by RWD & RWE throughout drug’s lifecycle
Among the oncology products authorized by the EMA in 2018 and 2019 (n = 24), RWD/RWE was found to be present (‘RWE signature’ for any reference to potential use of RWE in the marketing authorization application as presented in the European Public Assessment Report overview) in all stages of drug development: 100.0% in discovery, 37.5% in early development, 58.3% in clinical development, 62.5% in registration decision and 100.0% in post-authorization lifecycle management [3].
The use of RWD to support regulatory decision-making in the post-marketing surveillance setting has increased in recent years, with most activities being legally enforced requests on the marketing authorization holder to further document the product’s safety profile [17]. Comparatively, there is a limited number of examples in which RWD have been used for new approvals and line extensions. A noteworthy illustration encompasses the extension proposal for palbociclib, seeking inclusion for the hormone receptor positive, human epidermal growth factor receptor 2 negative (HR+/HER-) metastatic breast cancer (mBC) indication in men by the FDA, where RWE played a supportive role [18–20]. A summary of the multifaceted insights afforded by RWD and RWE throughout a drug lifecycle [11,21,22,23] can be found in Table 2.
| Preapproval phase | • RWE can elucidate the disease course in the absence of or under current standard of care including treatment requirements to cover unmet medical needs, resource use, adherence. It can also provide information on disease epidemiology, unmet needs and disease burden, help to estimate the number of patients eligible for new treatment/s, gaps in care and differences between observed practice and clinical guidelines. • RWE may be considered to supplement RCTs and support regulatory decision-making: • When used to describe product safety or effectiveness in another country, where the product is already approved. • When approval is sought for a different dose/indication particularly around end points relevant to regulators that are often not captured in RCTs, including overall survival, effectiveness in underrepresented patient populations, and surveillance for rare safety events. • When existing knowledge of the potential class effects for pharmacovigilance is used as an element for the initial authorization. • In case of rare diseases where single-arm clinical trials are sometimes compared against RWE background data. |
| Following approval | • RWE can provide information on head-to-head comparative effectiveness. • RWE contributes to data on cost-effectiveness in the context of competitors. • RWE can inform on patterns of utilization/prescription/switch and adherence. • RWE can support reimbursement decisions and treatment decisions by clinicians and patients. • Using RWD instead of RCT data to inform population-based disease models can better reflect the clinical reality of treatment-eligible patient populations and improve physician engagement and patient experiences. • RWE can also provide data to support clinical guidelines regarding specific subgroups of patients when such analyses are underpowered using RCT data. • RWE has an important role to play in understanding drug effectiveness and AEs based on differences of metabolism in various racial and genetic groups. • Due to size restrictions, clinical trials may not capture rare AEs or drug–drug interactions that could be discovered through RWD analysis. • RWD/RWE can be used to support obligatory active monitoring in the post-approval phase. • RWD can provide evidence about the effectiveness and safety of the drug in off-label use. |
| Mature phase | • RWE on long-term effectiveness and safety. • RWE can be used to demonstrate treatment benefits in broader patient populations, including populations that may be underrepresented in RCTs. • RWE can serve to identify class effects. |
AE: Adverse event; RCT: Randomized clinical trial; RWD: Real-world data; RWE: Real-world evidence.
Assessing the quality of RWE studies
To achieve benefits to patients, the scientific community, and healthcare authorities it is crucial to address standardization and develop recommendations to improve the quality of RWE [11,12,24].
A multidisciplinary group of experts of the ESMO Real-World Data and Digital Health Working Group developed the first specific guidance for reporting oncology RWE studies in peer-reviewed journals: the ESMO Guidance for Reporting Oncology Real-World Evidence (ESMO-GROW). Although not a quality metrics for RWD studies, ESMO GROW offers a list of 35 recommendations based on current evidence and the authors' collective expert opinion for full manuscript development in different RWE research scenarios applied to oncology [12].
Assessing the quality of a RWD study is not simple, but transparency when presenting study methodology (from data collection to final statistical analysis) is very important to build credibility and evaluate internal validity. The FDA RWE guidance focus on outlining how a data source may be fit-for-use, meeting both principles of relevance and reliability to answer a specific scientific question (Figure 1). To ascertain quality of RWD for regulatory decisions, it is imperative to provide analytic documentation regarding methods for data abstraction, curation, aggregation and transformation (i.e., data provenance), including any deduplication procedures or linkages with external sources [25]. There are a range of validation approaches to check the robustness/accuracy of RWD. These include data quality checks applied to detect logical inconsistencies and erroneous, missing or out-of-range values and the remedial actions that are taken at the level of the data source. One can also perform internal/external reference checks and benchmarking. For example, by addressing quality dimensions from published frameworks, the Flatiron Health EHR-derived RWD were shown to be curated, relevant and reliable using a range of quality processes that optimize for robustness, scalability and feasibility [26].
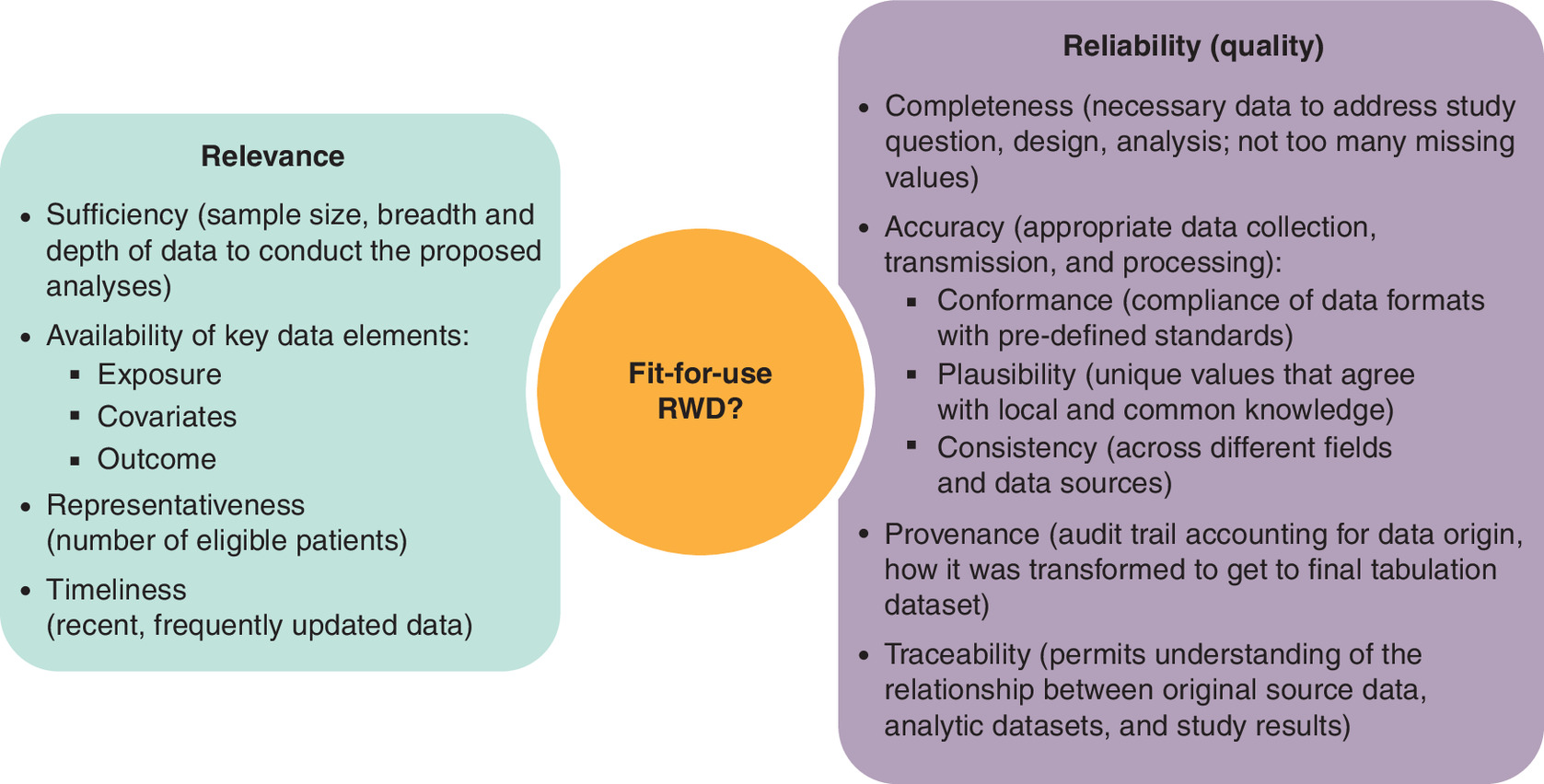
Figure 1. Relevance and reliability in the fit-for-use of real-world data.
RWD: Real-world data.
Variables, bias & methodological aspects in RWE studies in oncology
Variables
Variables that are necessary to conduct real-world comparative analysis in oncology can be categorized into three essential components [6], summarized in Table 3.
| Variables for cohort creation | Variables on baseline demographic and clinical characteristics | Variables on outcomes of interest | |
|---|---|---|---|
| Type of outcome | End point examples | ||
| • Variables to define the disease of interest such as cancer diagnosis codes (ICD-O-3 morphology, topography, behavior code), stage and date of diagnosis • Variables on receipt of treatment, including a drug/regimen identifier, date of treatment and dose administered • Data elements defining treatment indication, line of therapy and/or intent of treatment (curative/palliative) and reason for discontinuation • Appropriate comparator and/or control group populations | Age Sex Neighborhood income quintile Region/rurality Comorbidity Performance status Prior treatment exposures (systemic therapy, radiotherapy and cancer-directed surgery) Concurrent or subsequent treatments (systemic therapy, radiotherapy and cancer-directed surgery) | Clinical effectiveness Safety and toxicity Cost–effectiveness Budget impact Patient-reported outcomes | Overall survival Other time-to-event end points, like time to treatment discontinuation, time to next treatment or time to progression Hospitalizations Emergency department visits Cost data Incremental cost–effectiveness ratio Incremental net-benefit regression Budget over X period Quality of life, late effect end points or survivorship end points |
ICD-O-3: International Classification of Diseases for Oncology-3.
Bias
There are several potential biases that need to be taken into consideration when designing or interpreting real-world studies [5]. These include bias in selection of study participants, bias due to confounding and immortal time, bias due to deviation from intended interventions, bias due to missing data, bias in measurement of outcomes and bias in the selection of the reported result. Definitions, examples and strategies to avoid or mitigate them can be found in ESMO-GROW [12]. Other tools and checklists, to name a few, include Good Research for Comparative Effectiveness (GRACE) checklist, International Society for Pharmacoeconomics and Outcomes Research (ISPOR), Risk Of Bias In Non-randomized Studies – of Interventions (ROBIN-I), Study Type Assessment and Regulatory Tracking (STaRT) and Strengthening the Reporting of OBservational studies in Epidemiology (STROBE). The authors must identify limitations in the data and provide guidance about how they could bias study results.
Sensitivity analysis is a method used to evaluate the robustness of an assessment by investigating how much the results could be influenced by alterations in methods, models, values of unobserved variables or assumptions. This approach is crucial for identifying findings that are highly dependent on potentially questionable or unsupported assumptions, which may compromise the validity of the conclusions [27]. It is important to clearly prespecify the sensitivity analyses before conducting them to ensure that they are designed to address the same research question as the primary analysis. When the results of the primary and sensitivity analyses are consistent, they can strengthen the credibility of the study's findings. However, when the results differ, it is important to consider what this indicates about the assumptions and methodology, rather than simply discarding the conflicting results. A thoughtful interpretation of these discrepancies can lead to meaningful insights and a deeper understanding of the potential limitations and strengths of the study, making the findings more reliable and transparent [28,29].
Data collection (information) bias
Potential bias in data collection, together with missing data, are the main disadvantages of using administrative data [24]. The use of a nationwide cohort might guarantee a representative, unselected population, but multicenter studies are more susceptible to information bias due to differences in patient monitoring and nonstandardized data collection.
Selection bias
Selection bias can be a concern among studies of metastatic cancers focused solely on individuals referred to a medical oncologist. Indeed, systemic therapy initiation and overall survival from diagnosis among individuals with metastatic cancer were considerably overestimated when restricted to patients who were referred to a medical oncologist [30]. Patients with metastatic cancer who reach an oncologist typically represent a nonrandom subset of the broader population. In many real-world settings, referrals depend on factors such as age, comorbidity burden, performance status, socioeconomic background, geographic access to oncology services and physician practice patterns. Consequently, individuals managed exclusively in primary care or palliative care, or those who are too frail to be referred, are systematically under-represented. This can result in an overestimation of treatment eligibility, uptake and outcomes compared with the general population of patients with metastatic disease. By acknowledging this limitation, we aim to highlight that the observed results may not be fully generalizable to all patients with metastatic cancer.
Confounding by indication
Confounding by indication bias occurs when outcome depends not only on intervention, but also on reasons for the indication (e.g., based on physician- or patient-related aspects, such as perceptions about disease severity, frailty, concomitant diseases/treatments [drug–drug interactions]) [12]. Confounders are of particular concern when strongly prognostic of disease outcome irrespective of the intervention. Unmeasured confounders are very frequent in RWD studies, including Eastern Cooperative Oncology Group (ECOG) performance status and metastatic burden at treatment initiation.
Time-related biases
Guarantee-time bias (immortal time bias) occurs when there is a period of cohort follow-up time during which death (or an outcome that determines end of follow-up) cannot occur. In RWD studies it is common to have index data (start of follow-up and outcome measure) to occur before the exposure of interest happens. For instance, when estimating overall survival ([OS] outcome) in patients with metastatic cancer who have undergone broad genomic testing and precision medicine drugs (exposure), the time from diagnosis of metastatic disease to genomic test is immortal. Many other time-related biases (protopathic [first symptoms of the outcome of interest are the reasons for using the treatment under study], latency, time-window, depletion of susceptible individuals and immeasurable time) can affect the results [31]. Another bias to keep in mind is publication bias, when publishing only studies with positive outcomes and overlooking those with negative results, access to the full of evidence about a particular issue is hampered [32].
Methodological aspects
Many methodological approaches can mitigate biases in real-world studies and the most appropriate depends on the research question being addressed [5]. Propensity scores, a cornerstone for adjusting confounding in observational studies, reflect patients predicted probability of receiving a certain treatment given their characteristics. ECOG, metastatic burden, metastatic sites, comorbidities, concomitant treatments, smoking status, among others, are confounding variables that can impact on oncologic treatment outcomes. If information on potentially confounding factors is unavailable or incomplete in the database, they cannot be statistically controlled, which prevents performing adjusted comparisons and contributes to limitations in the interpretation of the results.
Using propensity score-based methods, researchers can target causal inference in observational studies by measuring the differences in outcomes between treated and reference populations. Propensity score methods include matching, stratification, adjustment as a regressor and weighting [5].
Propensity scores matching (PSM) has an important limitation, as it discards unmatched observations (Figure 2) and requires a very large pool of patients in the control group, making it suboptimal when investigating an uncommon exposure or a rare outcome. In contrast, propensity score weighting allows keeping most observations in the analysis, can facilitate clearer reporting of the balance between the treatment and reference groups and is also far more flexible, with multiple variations allowing the targeting of specific populations. Inverse probability of treatment weighting is a traditional propensity score weighting approach (Figure 2) [5].

Figure 2. Infographic representation of how propensity score matching and inverse probability of treatment weighting work.
PSM pairs individuals from different treatment groups (different colors) who share similar propensity scores (same size), creating a matched study population and excluding unmatched patients. IPTW keeps all individuals (in this representation, 5) but applies weights based on the inverse of their probability of receiving treatment (represented as a change in the size of each individual), generating a weighted pseudopopulation in which treatment groups are balanced on observed characteristics.
IPTW: Inverse probability of treatment weighting; PS: Propensity score; PSM: Propensity score matching; W: Weight.
As mentioned above, the availability of clinically relevant structured data elements to be readily extracted from EHRs and compared across systems is usually limited, and often valuable information regarding the characteristics, treatments, and outcomes of oncologic patients is found in unstructured free text documents that require manual curation and processing to be usable for research purposes. In that sense, application of natural language processing with machine learning (ML) techniques (i.e., ML extraction) to EHR data can contribute to more efficient and scalable generation of RWD. Importantly, ML models should be evaluated and monitored for any potential bias or findings to prevent negative consequences on the integrity of the data. A framework has been proposed covering the fundamentals to evaluate the performance, limitations, and fit-for-purpose use of ML-extracted RWD which can be used for a variety of research purposes in the oncology field [33]. This evaluation framework for research-centric assessment of ML-extracted RWD before its use for research purposes provides a structured approach to documenting the strengths, limitations, and applications of ML-extracted RWD. It includes stratified performance analysis, quantitative error analysis and replication analysis to enable a greater understanding of potential model biases and how the ML-extracted data may perform in research use cases as compared with the corresponding abstracted variables [33].
Benedum et al. [34] assessed the reproducibility of oncology RWE studies using ML-extracted variables compared with the benchmark of the standard approach in retrospective research studies with manual chart review. Using biomarker- and treatment-defined cohorts to perform analyses related to biomarker-associated survival and treatment comparative effectiveness, respectively, they found that the results differed by less than 8% between the data curation methods across all analyses and reached similar conclusions. Thus, evidence generated by analyzing ML-extracted data can lead to the same conclusions as evidence generated with abstracted data when ML models are trained on expert-labeled data and evaluated with a research-centric approach, thus supporting the development of reliable, fit-for-purpose RWD using ML extraction [34].
Which is the most appropriate end point for RWE studies in oncology?
In clinical trials, OS is affected by multiple factors (demographics, baseline characteristics and prior adjuvant/neoadjuvant therapy), but also by post-progression therapy and the total therapy lines. Whereas progression-free survival (PFS) improvement is more often reported than OS improvement, its importance might be understated. For instance, in mBC, PFS in first line is an important predictor of PFS in further lines of therapy and PFS improvement together with maintained health-related quality of life (HRQoL) represents a patient-relevant end point [35,36]. However, the outcome may change if treatment benefit is captured differently in the real-world. For example, response evaluation criteria in solid tumors (RECIST)-based oncology end points, such as PFS and objective response rate, collected in clinical trials may be monitored by individual treating physician’s clinical assessment or interpretation of radiographic or pathologic results [15,16,37,38], and absence of scheduled scans and different timing of tumor assessment can impact. Even if RECIST 1.1 criteria aim to minimize variability in assessing tumor burden, since their introduction (2000) and revision (2009), new therapeutic targets have emerged, clinical trial objectives have changed, and there have been significant advancements in imaging techniques. Consequently, various limitations, problems and clinical-radiological discrepancies have been observed in daily practice, making it crucial to understand the key elements and common mistakes when using the RECIST 1.1 criteria to enhance reporting and address everyday clinical constraints [39]. On the other hand, it was argued that the real-world tumor response is less likely to be over-estimated, and may be confounded by institutional and physician practices [40]. It is also worth mentioning that, in clinical trials, determination of OS itself may face challenges related to data source, integrity and reliability [41], and this can be further expected to occur in the real-world setting.
Relative survival is a particularly suitable end point for real-world studies in oncology, as it estimates cancer-related excess mortality without requiring cause-of-death information. By adjusting for background mortality using population life tables, it better isolates the impact of cancer, especially in older or comorbid populations. Compared with OS, it reduces bias from non-cancer deaths and enhances comparability across populations and time periods. However, it relies on the availability and appropriateness of external mortality tables and may be less intuitive for clinical interpretation than OS.
Alternative end points to PFS such as time to discontinuation (TTD) and time to next treatment (TTNT) are gaining attention in oncology. TTD reflects the patient's experience and tolerability of the treatment, capturing real-world scenarios where treatment is discontinued due to side effects or patient preference serving as an early indicator of treatment failure, potentially before progression being radiographically detectable. However, reasons for discontinuation can vary widely, decisions to discontinue treatment can be subjective and influenced by factors such as patient and physician preferences, fixed duration of certain regimens (such as anthracycline chemotherapy) and the lack of standardized protocol for discontinuation can lead to inconsistencies in data collection and interpretation. On the other hand, TTNT indirectly measures treatment efficacy, as a shorter TTNT may indicate quicker disease progression or intolerance to the treatment. Compared with TTD, TTNT has shown greater consistency of findings across different data sources [42]. According to a systematic review of time to subsequent therapy as a candidate surrogate end point in advanced solid tumors, there was a strong correlation between TTNT and PFS by investigator and by central review, whereas it was medium/poor between TTNT and OS [43]. However, interpreting TTNT can be complex due to the multiple factors that contribute to changing treatments, including nondisease-related reasons. Additionally, there might be delays in starting new treatment due to patient recovery needs, logistical issues or insurance approvals, which can confound the end point. A summary of trial-defined end points versus real-world compatible end points is presented in Table 4.
| End point | Clinical trial definition | Real-world definition/proxy | Considerations/differences |
|---|---|---|---|
| OS | Time from randomization to death (all causes) using structured follow-up | Time from index treatment to death using EHR/death registry linkage | OS is generally robust in both settings, but RWD may have variable death data completeness and loss-to-follow-up censoring |
| PFS | Time from randomization to progression (RECIST) or death | rwPFS: time to clinically documented progression or death, often abstracted from notes or non-standard imaging reports | Not RECIST; it depends on documentation quality and visit timing |
| TTP | Time to objective progression (RECIST) ignoring death events | rwTTP abstracted from clinical documentation of progression events (may require adjudication rules) | May be similar in concept to rwPFS but excludes deaths unrelated to progression; definition can vary |
| RFS | Time from surgery (or end of primary curative therapy) to relapse or death | rwRFS possible in adjuvant settings if relapse is reliably captured in records/registries | Depends on consistent reporting of relapse events in routine care |
| TTNT | Not standard in trials (proxy: treatment failure or progression) | Time from start of index therapy to start of next line of therapy | Pragmatic in real-world as progression surrogate; reflects clinical decisions beyond strict progression criteria |
| TTD/rwTTD | Not typical in RCTs | Time from start of index therapy to discontinuation for any reason | Influenced by toxicity, progression, patient choice; thus, reflective of net clinical benefit beyond just disease progression |
| Relative survival | Not typical in RCTs | Ratio of the observed OS of the cancer patients to the expected survival from the comparable cancer-free population | Better isolates the impact of cancer, especially in older or comorbid populations; enhances comparability across populations and time periods, but may be less intuitive for clinical interpretation than OS |
EHR: Electronic health record; OS: Overall survival; PFS: Progression-free survival; RCT: Randomized clinical trial; RECIST: Response evaluation criteria in solid tumors; RFS: Relapse-free/recurrence-free survival; rw: Real-world; RWD: Real-world data; TTD: Time to treatment discontinuation; TTNT: Time to next treatment; TTP: Time to progression.
In conclusion, TTD and TTNT serve as valuable complementary end points to PFS in oncology, providing a broader understanding of treatment impact on patients’ lives and clinical practice. Their integration can lead to more patient-centered cancer care and improved overall treatment strategies.
PROs in RWE generation, are we there yet?
PROs are health data collected to assess symptoms, functional status and quality of life (QoL) directly from patients, not interpreted or modified by anyone else. An expert consensus from the Italian Association of Medical Oncology National Conference highlighted the critical importance of incorporating PROs and QoL measures throughout the cancer care continuum, from screening to survivorship [44]. Impactful HRQoL integration in clinical practice is critical and should be extended to dimensions that are currently rarely addressed [45]. In clinical practice, PROs improve patient-centered care and communication, particularly when oncologists are trained to interpret QoL data [44]. PROs are vital for capturing patients' real-life experiences and for strengthening RWE in patient-centered drug development [46]. Integration of patient-reported outcome measures (PROMs) into cancer care may improve OS and QoL [47]. Moreover, they can offer independent prognostic information for cancer survival. A systematic review (including a total of 69 RCTs comprising 44,030 patients) and meta-analysis (31 RCTs) of studies using the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire found that PROs (global health status, physical functioning and role functioning) were independently associated with improved OS. On the other hand, worsening symptoms (i.e., nausea, vomiting, pain, fatigue, loss of appetite, dyspnea) were associated with worse OS, thus supporting the integration of PRO assessments into clinical decision-making and risk stratification in oncology [48].
Even though RWE generation can be strengthened by incorporating PROs, routine or prospective collection of PROs in everyday clinical settings remains limited as they are rarely collected outside RCTs [46,49], leaving major gaps in understanding everyday treatment impact. Collection of PROs faces operational and methodological challenges, so its use in generating RWE is considered still in a formative stage, with both optimism and uncertainty among stakeholders [49]. Moreover, guidelines on the implementation of PROs are mainly focused on RCTs or clinical practice and guidance specifically to the RWE context is lacking. This is an issue because to capture accurately the patient voice using clinical outcomes assessment in real-world studies, guidance needs to address the particularities outside RCTs. So, there are several barriers and challenges to overcome [46,49–51] to unlock the full potential of patient-reported data and maximize the value of PROs in advancing patient-centered healthcare in clinical practice and through the generation of RWE.
Embracing PROs as a routine part of clinical assessment and engagement of healthcare professionals is vital for promoting patient participation and ensuring consistent data collection. Additionally, effective PROs implementation depends on user-friendly and accessible tools. Instruments should be designed to work across operating systems and devices, with clear layouts that facilitate understanding and completion. Automated reminders can help maintain participant engagement and reduce missing data, thereby improving overall data quality [49]. Importantly, a study reviewing 157 PROMs described frequent problems such as unclear or missing instructions, inconsistent formatting and question designs that may confuse patients. While most PROMs use accessible language and avoid medical terminology, fewer than half include clear, patient-friendly instructions and only a small number meet high comprehensibility standards across all evaluated domains. Insufficient comprehensibility can lead to biased data and exclusion of patients with low literacy, thus highlighting the need to improve clarity, layout, usability and to perform qualitative testing to ensure PROMs effectively support patient-centered care and produce reliable data for clinical practice, but also for RWE generation [52].
Although the primary reason for collecting PROs is to inform routine medical practice at the individual level [49], PROs can be used in oncology toward designing clinical trials, for FDA drug approval and label claims, and for comparative effectiveness research [53]. Capturing patient-subjective experience during treatment and care is essential in prospective clinical comparative effectiveness research to examine real-world outcomes and ensure alignment between outcomes of interest for patients and clinicians [53]. For instance, perceptions between patients with HR+/HER2- mBC and oncologists/oncology nurses regarding the assessment of QoL and the side effects impacting it are divergent. Overall, patients and healthcare professionals differed in the frequency and relevance of discussions around QoL in treatment decisions [54].
Important aspects to keep in mind include the fact that PROMs are usually designed for use and validated in clinical trial settings. Therefore, they may need to be adapted and tested for content validity for use in real-world settings [55,56]. For instance, the ecological validity (the extent to which the assessed symptoms generalize to real world settings and circumstances experienced in everyday life) of the Functional Assessment of Cancer Therapy – Cognitive Function (FACT-Cog) and the Patient-Reported Outcome Measurement Information System Cognitive Function (PROMIS Cog) has been demonstrated, as they effectively capture real-world cognitive symptoms and predict future everyday functioning, including social function and well-being in breast cancer survivors [57]. Additionally, validation of fit-for-purpose PROMs might be needed to unravel physical, psychological, and cognitive symptom burden in oncological patients in real-world settings [58]. Moreover, and in line with the importance of implementing PROs throughout the cancer care continuum and the need to use PROMs adapted to specific contexts, the EORTC Quality of Life Group has developed QLQ-SURV100 to comprehensively assess the HRQoL of disease-free cancer survivors. It includes essential and optional scales and will be validated further in an international Phase IV study [59]. Another issue to consider is that heterogeneity in the questionnaires used might globally complicate the interpretability and comparability of PROs [60], stressing the need to implement an appropriate and standardized set of PROs for routine clinical care and, by extension, to RWE studies.
Thus, there is still a substantial number of challenges to embrace and work to do to achieve a broad, effective and equitable use of PROMs and to accomplish their full potential in real-world oncological care and RWE generation.
Enhancing confidence in RWD generating processes, with the development of good practices for RWE studies
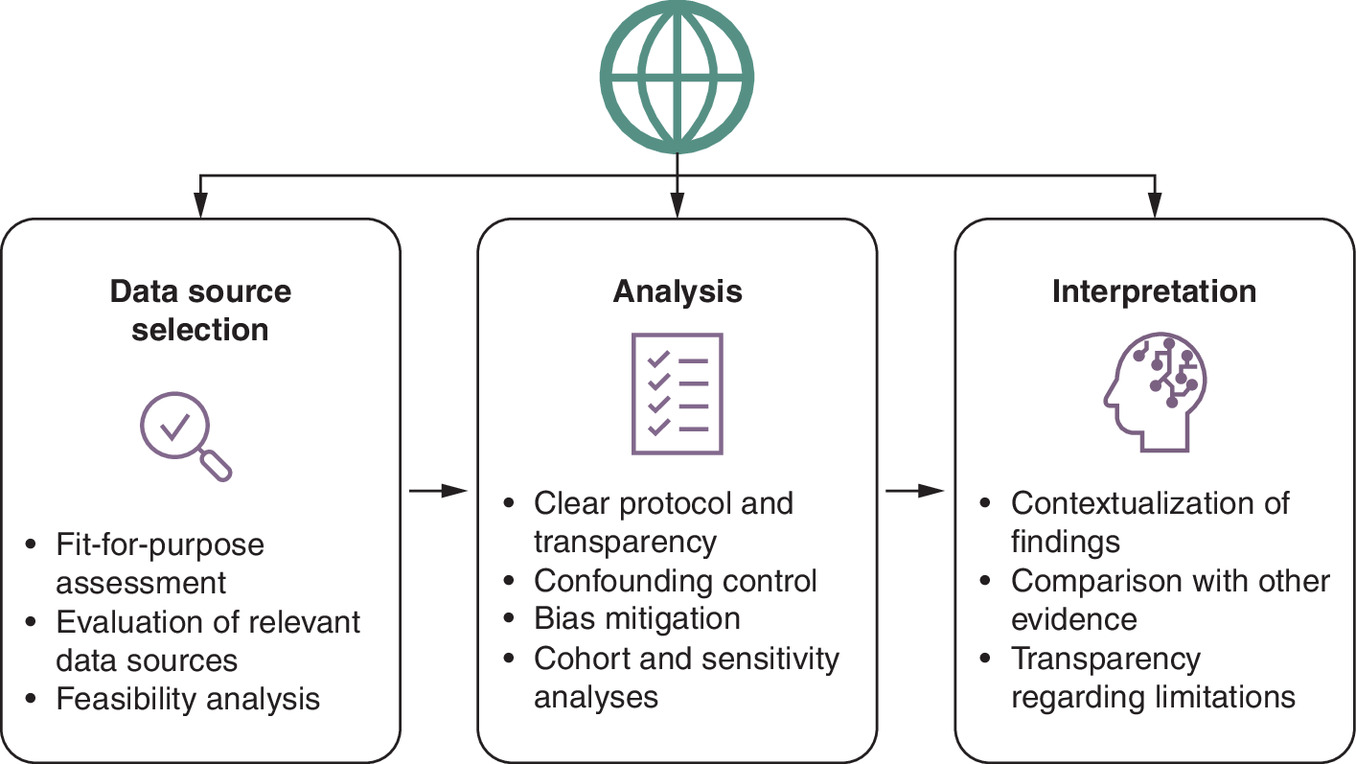
Several recommendations have been put forward aiming to promote trust in RWE by improving the culture of transparency of data, methods, analyses and results in hypothesis evaluating treatment effectiveness RWE studies [32,61]. This fits the UNESCO Recommendation on Open Science, which aims to promote universal access to scientific knowledge, ensuring that research outputs are freely available, transparent, and inclusive, fostering collaboration and equity in global science [62]. The RWE Registry provides researchers with a fit-for-purpose platform to register their study designs in advance, facilitating transparency [63]. Registration at ClinicalTrials.gov or at the Open Science Framework is also an option. On the other hand, the HMA-EMA Catalogues are metadata repositories for RWD sources and studies, that replaced the EU PAS Register® and ENCePP Resource Database. They support regulators, pharmaceutical companies and researchers in using RWD for medicine investigations. The catalogues aid in data source discoverability and suitability assessment, improve study-data source interoperability and increase transparency and opportunities to reproduce the study [64]. Unlike RCTs, RWE studies are often conducted retrospectively, with flexible analytic choices regarding patient selection, exposure definitions, outcome ascertainment and covariate adjustment. These degrees of freedom can increase the risk that study design or analytic modifications are influenced by the observed data. The FDA has highlighted the importance of pre-specification and transparency in RWE study protocols precisely to mitigate this risk [13]. Registration of the study hypotheses, data sources, protocol and statistical analysis plan before study execution is believed to improve study replicability, facilitate evaluation of validity and limit the potential for decisions results-driven [32]. Updates when changes have been introduced and version control are practical strategies to enhance transparency. Nevertheless, transparency does not ensure that a study is of high quality or applicability, as poorly conducted RWE studies can be completely transparent, and there is no statistical method to adjust data that is unfit-for-use or bad study design. Figure 3 provides an integrated overview of the main methodological principles across data source selection, analysis and interpretation of real-world studies.
What questions can RWE studies address that can help us guide clinical decisions?
RWD can be used for treatment effect evaluation, namely of trends in population outcomes, treatment effectiveness and safety, comparative effectiveness research, precision oncology, patient counseling, as well as treatment delivery optimization [65]. In the next lines few examples are provided to illustrate some of them.
Comparative effectiveness
RWD studies offer valuable insights into the effectiveness and safety of treatments in everyday clinical practice, complementing evidence obtained from RCTs. They help understanding treatment patterns and outcomes beyond RCT settings, extending our knowledge of how treatments perform in clinical practice, in broader, more diverse populations. Moreover, in the absence of head-to-head RCTs between treatment options within a therapeutic class, RWE on their comparative effectiveness in clinical practice can complement their efficacy and safety profiles in clinical trials and thus be helpful when choosing the most appropriate option for an individual patient.
RWE can challenge RCTs’ results [38,66–69] and help clarify whether there is, in everyday practice, a clinically relevant in class inter-drug difference in effectiveness, safety or tolerability. Nevertheless, often studies include a low number of patients and/or are limited by the lack of methods for bias mitigation [70–74].
The use of the Flatiron Health EHR-derived deidentified longitudinal database, a US nationwide database containing patient-level structured and unstructured data curated using natural language processing with ML and technology-enabled abstraction can facilitate real-world comparative effectiveness studies when head-to-head trials are not available [69]. Nonetheless, still some limitations must be considered, namely its retrospective nature, with the potential for inaccurate or incomplete data capture of confounders for treatment selection. Also, the differences in sample sizes between the treatment groups due, for instance, to delayed approval dates, can preclude a formal, powered, noninferiority analysis [69]. Thus, it is essential that authors from individual real-world studies acknowledge study limitations.
Sequence of treatment
Real-world studies can inform on current treatment sequencing patterns in clinical practice, could help define the best treatment sequence and can be hypothesis-generating. For instance, the optimal management of patients with HR+/HER2- advanced breast cancer (aBC) after progression on first-line cyclin-dependent kinase 4 and 6 inhibitors (CDK4/6i) therapy remains a key clinical question. Evidence from prospective clinical trials suggests that cross-resistance between CDK4/6i is not absolute, and selected patients may derive continued benefit from CDK4/6i when combined with a new endocrine partner. RWE complements these findings by reflecting treatment outcomes in broader, more heterogeneous populations. Retrospective analyses from large registries (including Flatiron, US Oncology Network and ESME) indicate that approximately 20–40% of patients receive a CDK4/6i re-challenge in clinical practice. Median rwPFS in these cohorts typically ranges from 4 to 6 months, consistent with results from clinical trials. Importantly, RWD help identify subgroups most likely to benefit – such as patients with prior prolonged response (>12 months) to initial CDK4/6i, evidence of endocrine-sensitive disease and absence of RB1 loss or cyclin E1 amplification – while highlighting limited efficacy in those with early resistance or visceral crisis [75–78].
Similarly, no prospective data are available regarding the activity of sequential use of antibody–drug conjugates (ADCs) with similar payloads – such as trastuzumab deruxtecan (T-DXd) and sacituzumab govitecan – among patients with HER2- aBC. Real-world studies have shown shorter rwPFS in patients previously treated with an ADC, suggesting potential cross-resistance between topoisomerase I-based ADCs used sequentially, even when targeting different tumor-associated antigens [79–81]. Thus, considering the approval of multiple ADCs in breast cancer and the lack of clinical trials directly comparing these drugs, RWE will be highly valuable for establishing the value of sequencing these agents.
Evidence in patient profiles not included or underrepresented in RCTs
Obtaining real-world reports on the use of oncologic treatments in patient subgroups usually not well represented in clinical trials such as elderly patients, certain ethnic groups or races or patients with comorbidities can be reassuring if effectiveness results in a larger sample size prove like those in RCTs. Moreover, they help to expand information on drug dosage, safety and adverse events (AEs) management in clinical practice. In relation to the comparative effectiveness studies mentioned above, they can be used to assess whether the outcomes are comparable to a RCT. If both real-world studies and RCTs show the same magnitude of benefit from an intervention, one emulates a RCT with RWD. Then, one can use RWD to ask specific research questions in populations not included or underrepresented in RCTs. It increases the internal validity of the data. The FDA RCT-DUPLICATE project is one example. In this context, ENCORE (Emulation of iNterventional trials in Clinical Oncology with RWE) aims to develop and expand a process to evaluate the ability of RWE to support evidence of effectiveness in oncology, including a systematic evaluation of the fitness of RWD for each study design; demonstrate and examine the systematic process by emulating 12 oncology trials across four cancers and assessing the results of RCT-RWE study pairs. Emphasis is placed on transparency and on conducting extensive sensitivity analyses to assess robustness of findings and trial eligibility criteria (e.g., age, race and comorbidity) [82].
In the context of populations not included or underrepresented in RCTs, it is noteworthy that RWD contributed entirely to evidence that men can benefit from the incorporation of palbociclib to endocrine therapy in HR+/HER2- mBC, with a safety profile consistent with previous observations in women. This RWE supported the extension of palbociclib approval form for male population [19]. According to the sub-analysis of the male population in the POLARIS study, treatment patterns, AEs, PROs and outcomes were generally equivalent to those previously reported among predominantly female HR+/HER2- aBC patients treated with palbociclib [83].
Another example where RWE also supported therapy benefits in a population more representative of clinical practice is the case of idecabtagene vicleucel, an autologous B-cell maturation antigen–directed chimeric antigen receptor T-cell therapy (CART-T), used for relapsed/refractory multiple myeloma as a standard-of-care. Its safety and efficacy in patients with relapsed/refractory multiple myeloma in the standard-of-care setting in a retrospective study at 11 US academic medical centers were comparable with those in the Phase II pivotal trial despite most patients (75%) not meeting trial eligibility criteria for participation because of comorbidities at the time of leukapheresis. This study indicated that idecabtagene vicleucel CAR-T administration in clinical practice is feasible, safe and effective, even among patients with comorbidities who would have been excluded from the pivotal trial [84].
Future perspective
RWD studies have become a valuable tool to close the gaps in evidence from RCT to clinical practice in oncology, providing insights into the complexities of cancer care and treatment outcomes in real-life settings. They can inform on current treatment sequencing patterns in clinical practice, can be hypothesis-generating and prove to be helpful to guide clinical decision related to topics where evidence from RCT is still scarce and even impossible to obtain. RWE can highlight which patient subgroups respond best, uncover nuances such as biomarkers or resistance mechanisms, and help clinicians make more informed decisions. This will contribute to more personalized and effective care for patients, unnecessary treatments minimization, hopefully improving OS and QoL for patients while ensuring that therapies are used to their fullest potential.
Nevertheless, it is important to keep in mind that the presence of missing data, the difficulty in adjusting for relevant confounders, the lack of consistency in measuring key outcomes, the follow-up (restaging) of patients varying depending on the drug (due to side effects, patient frailty, etc.) can make challenging, even considerably risky, to conduct comparative effectiveness studies. The issues mentioned represent significant bias, so caution is needed when interpreting the results. The use of tools and checklists like GRACE checklist, ISPOR, ROBINS-I, STaRT and STROBE helps to evaluate the quality of RWE studies. In addition, to pursue well-designed RWE studies and transparent reporting, it is also important to recognize the limitations of each study.
Looking ahead, the landscape of RWE in oncology holds exciting possibilities of future directions:
•
Prospective data collection initiatives: collaborative efforts to prospectively collect RWD, including PROMs, such as through pragmatic clinical trials and patient registries, hold promise for generating high-quality evidence in cancer treatment.
•
Advanced analytical methods: continued refinement of analytical methodologies, including ML algorithms and causal inference techniques, might be able to enhance the validity and robustness of RWE analyses, enabling more accurate treatment effect estimation.
•
Integration of biomarker data: incorporating molecular and genomic data into RWE analyses can facilitate the identification of patient subgroups that may derive differential benefits from specific treatments, guiding personalized therapeutic approaches.
•
Real-time data analytics: leveraging real-time data analytics and health informatics technologies enables timely monitoring of treatment patterns, safety signals and outcomes in clinical practice, fostering adaptive decision-making and quality improvement initiatives.
•
Collaborative data sharing platforms: establishing collaborative platforms for data sharing and harmonization promotes transparency, reproducibility and collective learning in RWE research, boosting a culture of collaboration across academic, industry and regulatory stakeholders.
In conclusion, RWE holds immense potential to inform clinical decision-making and enhance patient care in cancer treatment. Despite the inherent challenges, ongoing improvements in data science, technology and collaborative research efforts provide a pathway toward harnessing the full potential of RWE, ultimately improving outcomes for patients facing this challenging disease landscape.
Executive summary
•
Real-world data (RWD) studies offer several opportunities along a drug’s life cycle, but several challenges remain to be addressed to achieve a maximized impact of real-world evidence on cancer treatment.
•
RWD studies are crucial in understanding treatment patterns and outcomes beyond clinical trials' settings, extending our knowledge of how treatments perform in clinical practice, in broader, more diverse populations. Others are hypothesis-generating or may prove helpful to guide clinical decision related to topics where evidence from randomized clinical trials is still scarce.
•
Real-world evidence can play a role in supporting or challenging randomized clinical trials' results and clarify whether there is indeed, in real practice, a clinically relevant in class inter-drug difference in effectiveness, safety or tolerability.
•
Conducting comparative effectiveness studies is challenging, even risky. Significant bias may be present and proper adjustment and control for bias are needed, together with caution when interpreting the results.
Author contributions
All authors contributed equally to the manuscript conceptualization, literature search, manuscript draft and revisions and approved the final version of the manuscript.
Financial disclosure
This work was supported by Pfizer Oncology, Madrid, Spain.
Competing interests disclosure
B Bermejo reports having a consultant or advisory role for Novartis, Pfizer, AstraZeneca, Daichii-Sankyo, Seagen, Gilead and Lilly, a speaker role for Novartis, Astra Zeneca, Daichii Sankyo, Pierre Fabre, Lilly, Pfizer, Gilead and Seagen, as well as receiving research funding (clinical trial participation as PI) from Novartis, Genentech, Seagen and Daiichi-Sankyo, and Gilead. R Dienstmann declares advisory role for AstraZeneca, Foundation Medicine, Pfizer, Roche, received a speaker’s fee from Amgen, AstraZeneca, Bristol Myers Squibb, Foundation Medicine, Gilead, GlaxoSmithKline, Guardant Health, Ipsen, Johnson and Johnson, Libbs, Lilly, Merck Sharp & Dohme, Pfizer, Roche, Sanofi, Servier, Takeda, research grants from AstraZeneca, Daiichi-Sankyo, GlaxoSmithKline, Merck, Novartis, Pfizer, and is investor in Trialing Health, S.L. M Bellet reports advisory board and speaker’s bureau role for Pfizer, Novartis, Lilly, Stemline-Menarini, and Roche, and receiving travel expenses from Pfizer, Novartis, Lilly and Roche. EG-Calvo declares receiving consulting fees (e.g., advisory boards) from Roche, Pfizer, Lilly, Daiichi-Sankyo, Gilead and AstraZeneca. V Obadia: none. A Santaballa reports having received honoraria and providing advisory/consultancy services: MSD, AstraZeneca, GSK, Pharma & Pierre Fabre, Lilly, Novartis, Pfizer; travel/accommodation/expenses: GSK, MSD, Pierre Fabre, Pfizer and participating in a speakers' bureau: MSD, AstraZeneca, GSK, Novartis, Lilly, Pierre Fabre. RR-Medina and M Cuenca are employees of and may own stock in Pfizer Inc. F Moreno declares consulting or advisory role for Novartis, Pfizer, AstraZeneca, MSD, Daiichi Sankyo/Astra Zeneca, Seagen and Pierre Fabre; participating in a speaker’s bureau: Pfizer and Novartis, as well as travel and accommodations expenses from Pfizer, Novartis and Gilead Sciences. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support for this article was provided by Ana Saavedra and Rosa Bugella, Havas Health Spain.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Pellat A, Grinda T, Prelaj A et al. 1689O Comprehensive mapping review of real-world evidence publications focusing on targeted therapies in solid tumors: a collaborative work from ESMO real-world data and digital health working group. Ann. Oncol. 34, S925 (2023).
• Comprehensive review of real-world evidence (RWE) studies on targeted therapies for solid tumors published between 2020 and 2022. The authors highlighted the need for more prospective, international and population-based RWE studies to enhance their impact on oncology practice.
2.
Booth CM, Karim S, Mackillop WJ. Real-world data: towards achieving the achievable in cancer care. Nat. Rev. Clin. Oncol. 16(5), 312–325 (2019).
3.
Eskola SM, Leufkens HGM, Bate A, Louise M, Bruin D, Gardarsdottir H. The role of real-world data and evidence in oncology medicines approved in EU in 2018–2019. J. Cancer Policy 36, 100424 (2023).
4.
Arondekar B, Duh MS, Bhak RH et al. Real-world evidence in support of oncology product registration: a systematic review of new drug application and biologics license application approvals from 2015–2020. Clin. Cancer Res. 28(1), 27–35 (2022).
5.
Azoulay L. Rationale, strengths, and limitations of real-world evidence in oncology: a canadian review and perspective. Oncologist 27, e731–e738 (2022).
• Examines the limitations of randomized clinical trials (RCTs) in oncology, discusses various types of RWE and evaluates how RWE can complement RCT data. The paper also explores the positions of regulatory bodies on RWE and provides an overview of its strengths and limitations in informing oncology practice.
6.
Dai WF, de Oliveira C, Blommaert S et al. Mapping Canadian data assets to generate real-world evidence: lessons learned from Canadian real-world evidence for value of cancer drugs (CanREValue) collaboration's RWE data working group. Curr. Oncol. 29, 2046–2063 (2022).
7.
Khozin S, Blumenthal GM, Pazdur R. Real-world data for clinical evidence generation in oncology. J. Natl Cancer Inst. 109(11), djx187 (2017).
8.
Batra A, Cheung WY. Role of real-world evidence in informing cancer care: lessons from colorectal cancer. Curr. Oncol. 26(Suppl. 1), S53–S56 (2019).
9.
Dagenais S, Russo L, Madsen A, Webster J, Becnel L. Use of real-world evidence to drive drug development strategy and inform clinical trial design. Clin. Pharmacol. Ther. 111(1), 77–89 (2022).
• Explores how biopharmaceutical companies can leverage real-world data (RWD) to inform decisions throughout the drug development process and highlights the role of advanced analytics and artificial intelligence in harnessing large-scale RWD.
10.
European Medicines Agency. Final report on the adaptive pathways pilot. https://www.ema.europa.eu/en/documents/report/final-report-adaptive-pathways-pilot_en.pdf
11.
Beaulieu-Jones BK, Finlayson SG, Yuan W et al. Examining the use of real-world evidence in the regulatory process. Clin. Pharmacol. Ther. 107(4), 843–852 (2020)
12.
Castelo-Branco L, Pellat A, Martins-Branco D et al. ESMO guidance for reporting oncology real-world evidence (GROW). Ann. Oncol. 34(12), 1097–1112 (2023).
• First oncology-specific guidelines aimed at standardizing the reporting of RWE studies. GROW offers detailed recommendations for authors and reviewers, encompassing aspects such as study design, data sources and outcome reporting.
13.
Food and Drug Administration. Framework for FDA’s real-world evidence program. https://www.fda.gov/media/120060/download
14.
Bartlett VL, Dhruva SS, Shah ND, Ryan P, Ross JS. Feasibility of using real-world data to replicate clinical trial evidence. JAMA Netw. Open 2(10), e1912869. (2019).
15.
Mercon K, Mahendraratnam N, Eckert J et al. A roadmap for developing study endpoints in real-world settings. (2020). Duke. Margolis Institute for Health Policy. https://healthpolicy.duke.edu/publications/roadmap-developing-study-endpoints-real-world-settings
16.
LoCasale RJ, Pashos CL, Gutierrez B et al. Bridging the gap between RCTs and RWE through endpoint selection. Ther. Innov. Regul. Sci. 55(1), 90–96 (2021).
17.
Mofid S, Bolislis WR, Kühler TC. Real-world data in the postapproval setting as applied by the EMA and the US FDA. Clin. Ther. 44(2), 306–322 (2022).
• The authors analyze the utilization of RWD by the EMA and the US FDA in post-approval surveillance of authorized products.
18.
Bolislis WR, Fay M, Kühler TC. Review use of real-world data for new drug applications and line extensions. Clin. Ther. 42(5), 926–938 (2020).
19.
Kraus A, Yu-Kite M, Mardekian J et al. Real-world data of palbociclib in combination with endocrine therapy for the treatment of metastatic breast cancer in men. Clin. Pharmacol. Ther. 111(1), 302–309 (2022).
20.
Wedam S, Fashoyin-aje L, Bloomquist E et al. FDA approval summary: palbociclib for male patients with metastatic breast cancer. Clin. Cancer Res. 26, 1208–1212 (2020).
21.
Cottu P, Ramsey SD, Solà-Morales O, Spears PA, Taylor L. The emerging role of real-world data in advanced breast cancer therapy: recommendations for collaborative decision-making. Breast 61, 118–122 (2022).
22.
Eskola SM, Gerardus H, Leufkens M, Bate A, De Bruin ML, Gardarsdottir H. Use of real-world data and evidence in drug development of medicinal products centrally authorized in Europe in 2018–2019. Clin. Pharmacol. Ther. 111(1), 310–320 (2022).
23.
Gross AM. Using real world data to support regulatory approval of drugs in rare diseases: a review of opportunities, limitations & a case example. Curr. Probl. Cancer 45(4), 100769 (2021).
24.
Ro SK, Zhang W, Jiang Q et al. Statistical considerations on the use of RWD/RWE for oncology drug approvals: overview and lessons learned in oncology drug development. Ther. Innov. Regul. Sci. 57(4), 899–910 (2023).
25.
Lerro CC, Bradley MC, Forshee RA, Rivera DR. The bar is high: evaluating fit-for-use oncology real-world data for regulatory decision making. JCO Clin. Cancer Inf. 8, e2300261 (2024).
26.
Castellanos EH, Wittmershaus BK, Chandwani S. Raising the bar for real-world data in oncology: approaches to quality across multiple dimensions. JCO Clin. Cancer Inform. 8, e2300046 (2024).
• Reviews data quality frameworks from various health agencies and illustrates how these dimensions are applied in curating RWD, emphasizing the need for systematic processes to ensure data reliability and relevance.
27.
Schneeweiss S. Sensitivity analysis and external adjustment for unmeasured confounders in epidemiologic database studies of therapeutics. Pharmacoepidemiol. Drug Saf. 15(5), 291–303 (2006).
28.
Thabane L, Mbuagbaw L, Zhang S et al. A tutorial on sensitivity analyses in clinical trials: the what, why, when and how. BMC Med. Res. Methodol. 13, 92 (2013).
29.
Salciccioli JD, Crutain Y, Komorowski M, Marshall DC. Sensitivity analysis and model validation. 2016 Sep 10. In: MIT Critical Data. Secondary Analysis of Electronic Health Records [Internet]. Springer, Cham (CH) (2016). Chapter 17.
30.
Jarada TN, Sullivan DEO, Brenner DR, Cheung WY, Boyne DJ. Selection bias in real-world data studies used to support health technology assessments: a case study in metastatic cancer. Curr. Oncol. 30(2), 1945–1953 (2023).
31.
Suissa S, Dell'Aniello S. Time-related biases in pharmacoepidemiology. Pharmacoepidemiol. Drug Saf. 29(9), 1101–1110 (2020).
32.
Orsini LS, Berger M, Crown W et al. Improving transparency to build trust in real-world secondary data studies for hypothesis testing-why, what, and how: recommendations and a road map from the real-world evidence transparency initiative. Value Health 23(9), 1128–1136 (2020).
33.
Estevez M, Benedum CM, Jiang C et al. Considerations for the use of machine learning extracted real-world data to support evidence generation: a research-centric evaluation framework. Cancers (Basel) 14, 3063 (2022).
34.
Benedum CM, Sondhi A, Fidyk E et al. Replication of real-world evidence in oncology using electronic health record data extracted by machine learning. Cancers (Basel) 15, 1853 (2023).
35.
Forsythe A, Chandiwana D, Barth J, Baeck J, Tremblay G. Progression-free survival/time to progression as a potential surrogate for overall survival in HR+, HER2– metastatic breast cancer. Breast Cancer - Targets Ther. 10, 69–78 (2018).
36.
Anastasaki E, Harding T, Seddik A, Oddsdottir JSP. Assessment of select HER2-negative mBC agents as a proxy to understand HTA-body uncertainties for HER2-low mBC agents in EU4 and England. Poster presented at: ISPOR EUROPE (2021).
37.
DeMichele A, Cristofanilli M, Brufsky A et al. Comparative effectiveness of first-line palbociclib plus letrozole versus letrozole alone for HR+/HER2- metastatic breast cancer in US real-world clinical practice. Breast Cancer Res. 23(1), 37 (2021).
38.
Rugo HS, Brufsky A, Liu X et al. Real-world study of overall survival with palbociclib plus aromatase inhibitor in HR+/HER2- metastatic breast cancer. NPJ Breast Cancer 8(1), 114 (2022).
• Utilizing the Flatiron Health Analytic Database, the authors analyzed data from 2888 patients who initiated treatment between February 2015 and March 2020. The study found that the combination therapy was associated with significantly improved OS compared to AI monotherapy.
39.
Macho EA, Fernández AM, Parente AS et al. Criterios RECIST 1.1: actualización y análisis. Presented at: 36th meeting of the Spanish Society of Medical Radiology – (SERAM). (2022). https://piper.espacio-seram.com/index.php/seram/article/view/8629/7095
40.
Brufsky A, Liu X, Li B, Mcroy L, Layman RM. Real-world tumor response of palbociclib plus letrozole versus letrozole for metastatic breast cancer in US clinical practice. Target Oncol. 16(5), 601–611 (2021).
41.
Huang H, Tang Y, Yu Y et al. The reliability and integrity of overall survival data based on follow-up records only and potential solutions to the challenges. Lancet Reg. Heal. - West. Pacific. 31, 100624 (2023).
42.
Rivera DR, Henk HJ, Garrett-Mayer E et al. The friends of cancer research real-world data collaboration pilot 2.0: methodological recommendations from oncology case studies. Clin. Pharmacol. Ther. 111(1), 283–292 (2022).
43.
Agapow P, Mulla R, Markuzon N, Ottesen LH, Meulendijks D. Systematic review of time to subsequent therapy as a candidate surrogate endpoint in advanced solid tumors. Future Oncol. 19(23), 1627–1639 (2023).
44.
Puccini A, Viscardi G, Ciani O et al. Patient-reported outcomes (PROs) in clinical trials and in clinical practice: report from the XXI national conference of the Italian Association of Medical Oncology (AIOM). BMJ Oncol. 4(1), e000783 (2025).
45.
Wilczynski O, Boisbouvier A, Radoszycki L, Cotté F-E, Gaudin A-F, Lemasson H. Integrating quality of life in the care pathway of cancer patients undergoing immunotherapy treatment: descriptive, cross-sectional survey of an online patient community's experiences and expectations. J. Med. Internet Res. 24(1), e25792 (2022).
46.
Calvert MJ, O'Connor DJ, Basch EM. Harnessing the patient voice in real-world evidence: the essential role of patient-reported outcomes. Nat. Rev. Drug Discov. 18(10), 731–732 (2019).
47.
Balitsky AK, Rayner D, Britto J et al. Patient-reported outcome measures in cancer care: an updated systematic review and meta-analysis. JAMA Netw. Open 7(8), e2424793 (2024).
48.
Huang RS, Chen D, Benour A et al. Patient-reported outcomes as prognostic indicators for overall survival in cancer: a systematic review and meta-analysis. JAMA Oncol. 11(11), 1303–1312 (2025).
49.
Maruszczyk K, McMullan C, Aiyegbusi OL et al. Paving the way for patient centricity in real-world evidence (RWE): qualitative interviews to identify considerations for wider implementation of patient-reported outcomes in RWE generation. Heliyon 9(9), e20157 (2023).
50.
Hassett MJ, Cronin C. Patient-Reported Outcome Measures Help Patients With Cancer. JAMA Netw. Open 7(8), e2424748 (2024).
51.
Nguyen H, Butow P, Dhillon H, Sundaresan P. A review of the barriers to using patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs) in routine cancer care. J. Med. Radiat. Sci. 68(2), 186–195 (2021).
52.
Tuinenburg A, Determann D, Quik EH et al. Evaluating comprehensibility of 157 patient-reported outcome measures (PROMs) in the Nationwide Dutch Outcome-based healthcare program: more attention for comprehensibility of PROMs is needed. Patient 18(1), 65–76 (2025).
53.
Warsame R, D'Souza A. Patient reported outcomes have arrived: a practical overview for clinicians in using patient reported outcomes in oncology. Mayo Clin. Proc. 94(11), 2291–2301 (2019).
54.
Cardoso F, Rihani J, Harmer V et al. Quality of life and treatment-related side effects in patients with HR+/HER2- advanced breast cancer: findings from a multicountry survey. Oncologist 28(10), 856–865 (2023).
55.
Roborel de Climens A, Findley A, Bury DP, Brady KJS, Reaney M, Gater A. Development and content validation of the patient's qualitative assessment of treatment - real-world (PQAT-RW): an instrument to evaluate benefits and disadvantages of treatments in real-world settings. Patient Relat. Outcome Meas. 15, 255–269 (2024).
56.
Meyer H, Hinz A, Weisgerber C et al. Lower extremity lymphedema in patients with gynecologic cancer: validation of the Gynecologic Cancer Lymphedema Questionnaire (GCLQ) in German language and investigation of lymphedema real-world treatment. Arch. Gynecol. Obstet. 311(4), 1151–1162 (2025).
57.
Henneghan AM, Franco-Rocha OY, Van Dyk KM, Paolillo EW, Haywood D, Moore RC. Establishing the ecological validity of cognitive patient reported outcome measures in breast cancer survivors: a prospective cohort study. Psychooncology 34(11), e70324 (2025).
58.
Wang XS, Srour SA, Whisenant M et al. Patient-reported symptom and functioning status during the first 12 months after chimeric antigen receptor T cell therapy for hematologic malignancies. Transplant Cell Ther. 27(11), 930.e1–930.e10 (2021).
59.
van Leeuwen M, Kieffer JM, Young TE et al. Phase III study of the European organization for research and treatment of cancer quality of life cancer survivorship core questionnaire. J. Cancer Surviv. 17(4), 1111–1130 (2023).
60.
Clarijs ME, Thurell J, Kühn F et al. Measuring quality of life using patient-reported outcomes in real-world metastatic breast cancer patients: the need for a standardized approach. Cancers (Basel) 13(10), 2308 (2021).
61.
Berger ML, Sox H, Willke RJ et al. Good practices for real-world data studies of treatment and/or comparative effectiveness: recommendations from the joint ISPOR-ISPE special task force on real-world evidence in health care decision making. Pharmacoepidemiol. Drug Saf. 26(9), 1033–1039 (2017).
62.
UNESCO. UNESCO recommendation on open science. (2021). https://unesdoc.unesco.org/ark:/48223/pf0000379949
63.
ISPOR. Real-World Evidence Registry (2023). https://www.ispor.org/strategic-initiatives/real-world-evidence/real-world-evidence-registry
64.
European Medicines Agency. HMA-EMA catalogues of real-world data sources and studies. https://catalogues.ema.europa.eu/
65.
van Nassau SCMW, Bol GM, van der Baan FH et al. Harnessing the potential of real - world evidence in the treatment of colorectal cancer: where do we stand? Curr. Treat. Options Oncol. 25(4), 405–426 (2024).
66.
Turner NC, Slamon DJ, Ro J et al. Overall survival with palbociclib and fulvestrant in advanced breast cancer. N. Engl. J. Med. 379(20), 1926–1936 (2018).
67.
Slamon DJ, Diéras V, Rugo HS et al. Overall survival with palbociclib plus letrozole in advanced breast cancer. J. Clin. Oncol. 42(9), 994–1000 (2024).
68.
Brufsky A, Liu X, Li B et al. Real-world effectiveness of palbociclib plus aromatase inhibitors (AI) in metastatic breast cancer patients with cardiovascular diseases. Oncologist 29(12), 1032–1043 (2024).
69.
Rugo HS, Layman RM, Lynce F et al. Comparative overall survival of CDK4/6 inhibitors plus an aromatase inhibitor in HR+/HER2- metastatic breast cancer in the US real-world setting. ESMO Open 10(1), 104103 (2025).
70.
Cejuela M, Gil-Torralvo A, Castilla MÁ et al. Abemaciclib, palbociclib, and ribociclib in real-world data: a direct comparison of first-line treatment for endocrine-receptor-positive metastatic breast cancer. Int. J. Mol. Sci. 24(10), 8488 (2023).
71.
Al-ziftawi NH, Elazzazy S, Bbujassoum S, Izham M, Ibrahim M. The effectiveness and safety of palbociclib and ribociclib in stage IV HR+/HER-2 negative breast cancer: a nationwide real world comparative retrospective cohort study. Front. Oncol. 13, 1203684 (2023).
72.
Tang H, Yeo D, De Souza K et al. Clinical impact of CDK4/6 Inhibitors in de novo or PR- or very elderly post-menopausal ER+/HER2- advanced breast cancers. Cancers (Basel) 15(21), 5164 (2023).
73.
Kahraman S, Erul E, Seyyar M et al. Treatment efficacy of ribociclib or palbociclib plus letrozole in hormone receptor-positive/HER2-negative metastatic breast cancer. Future Oncol. 19(10), 727–736 (2023).
74.
Buller W, Pallan L, Chu T, Khoja L. CDK4/6 inhibitors in metastatic breast cancer, a comparison of toxicity and efficacy across agents in a real-world dataset. J. Oncol. Pharm. Pract. 29(8), 1825–1835 (2023).
75.
Wander SA, Han HS, Zangardi ML et al. Clinical outcomes with abemaciclib after prior CDK4/6 inhibitor progression in breast cancer: a multicenter experience. J. Natl Compr. Canc. Netw. 1–8 doi: (2021) (Epub ahead of print).
76.
Kalinsky K, Accordino MK, Chiuzan C et al. Randomized Phase II trial of endocrine therapy with or without ribociclib after progression on cyclin-dependent kinase 4/6 inhibition in hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer: MAINTAIN trial. J. Clin. Oncol. 41(24), 4004–4013 (2023).
77.
Kalinsky K, Bianchini G, Hamilton E et al. Abemaciclib plus fulvestrant in advanced breast cancer after progression on CDK4/6 inhibition: results from the Phase III postMONARCH trial. J. Clin. Oncol. 43(9), 1101–1112 (2025).
78.
Varnier R, Pérol D, Jacot W et al. Real-world treatment patterns and effectiveness after disease progression on CDK4/6 inhibitors for HR-positive/HER2-negative metastatic breast cancer in the ESME-MBC cohort. ESMO Open 10(10), 105803 (2025).
79.
Tarantino P, Lee D, Foldi J et al. Outcomes with trastuzumab deruxtecan by biomarker status, line of treatment and prior receipt of sacituzumab govitecan in a large real-world database of patients with metastatic breast cancer. ESMO Open 10(7), 105330 (2025).
80.
Occhiogrosso Abelman R, Spring L, Fell G, Davis A, Hensing W, Ryan P. Abstract PS08-03: sequencing antibody-drug conjugate after antibody-drug conjugate in metastatic breast cancer (A3 study): multi-institution experience and biomarker analysis. Cancer Res. 84(Suppl. 9), PS08–03 (2024).
81.
Poumeaud F, Morisseau M, Cabel L et al. Efficacy of administration sequence: sacituzumab govitecan and trastuzumab deruxtecan in HER2-low metastatic breast cancer. Br. J. Cancer 131(4), 702–708 (2024).
82.
RCT-DUPLICATE. https://www.rct-duplicate.org/projects.html
83.
Blum JL, Dicristo C, Gordon D et al. Outcomes of male patients with HR+/HER2– advanced breast cancer receiving palbociclib in the real-world POLARIS study. Breast Cancer Res. Treat. 203(3), 463–475 (2024).
84.
Hansen DK, Sidana S, Peres LC et al. Idecabtagene vicleucel for relapsed/refractory multiple myeloma: real-world experience from the myeloma CAR T consortium. J. Clin. Oncol. 41(11), 2087–2097 (2023).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 November 2025
Accepted: 23 March 2026
Published online: 24 April 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Maximizing the impact of real-world evidence on cancer treatment: what do we need to achieve it?. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0186
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Enrica Antonia Martino, Ernesto Vigna, Antonella Bruzzese, Nicola Amodio, Santino Caserta, Eugenio Lucia, Graziella D'Arrigo, Virginia Olivito, Caterina Labanca, Francesco Mendicino, Maria Eugenia Alvaro, Giovanni Tripepi, Fortunato Morabito, Massimo Gentile, Bridging Randomized Trial Efficacy and Real‐World Effectiveness in Multiple Myeloma: Integrating Clinical Trials and Real‐World Evidence for Individualized Care, European Journal of Haematology, 10.1111/ejh.70263, (2026).