Reshaping the cardiovascular continuum in the management of arterial and venous cardiovascular disease: a narrative review
Publication: Journal of Comparative Effectiveness Research
Abstract
The prevalence of cardiovascular disease (CVaD) is expected to double in the next 25 years, fueled by increasing prevalence of diabetes mellitus, obesity and hypertension. Cardiovascular–kidney–metabolic syndrome is a clinical entity requiring a holistic approach to prevention and management. Another aspect of this syndrome is chronic venous disease (CVeD), which is common in patients with CVaD. This review describes presentations at a symposium by the European Association of Preventive Cardiology (Milan, Italy; April 2025), discussing the interconnectedness of conditions on the CVaD continuum and their relationship with CVeD. Venous and arterial disease share common risk factors and pathogenic pathways, including endothelial dysfunction, increased vascular permeability, oxidative stress and inflammation. Many cardiometabolic and vascular conditions remain underdiagnosed and untreated, and the patients’ level of risk is often underestimated. Examination of the legs is important to identify peripheral arterial disease and/or CVeD. The mainstays of treatment for CVeD are exercise, compression therapy, venoactive drugs and surgery. Failure to achieve and maintain treatment goals is usually the result of therapeutic inertia or poor medication adherence. A coherent approach is needed to identify and manage shared risk factors and comorbidities. Effective disease management and risk reduction require integrated care using multidisciplinary teams; evidence-based treatments, usually with combination therapy; and use of tools to maximize adherence, including digital tools and single-pill combinations to simplify treatment regimens in patients with multiple risk factors or comorbidities.
Plain language summary: a narrative review of the management of arterial & venous cardiovascular disease
What is this article about?
This article describes the common features of cardiovascular disease (CVaD) and chronic venous disease (CVeD) and encourages a holistic approach to their management. This includes actively looking for CVeD in patients with CVaD (and vice versa) and prescribing effective treatments for both conditions. The article also raises awareness of the effect on health outcomes of adherence (patients taking treatment regularly as prescribed) and therapeutic inertia (doctors failing to appropriately escalate treatment to meet patient needs).
Why is this important?
Risk factors for CVaD, such as obesity, diabetes and hypertension (high blood pressure), affect the structure and function of blood vessels (arteries and veins). The resulting damage to arteries has a negative effect on the heart and kidneys, and eventually causes significant health events, such as stroke, heart attack or kidney failure. Damage to veins causes CVeD, which is associated with varicose veins, leg pain, skin problems and leg ulcers. Although CVaD and CVeD are closely related, many doctors do not see them that way.
What methodology/protocol is described?
A symposium on CVaD and CVeD was held at the European Association of Preventive Cardiology annual congress in Milan, Italy on 4 April 2025. This article highlights the presentations at the symposium.
What were the results?
In both CVaD and CVeD, therapeutic inertia can be overcome by actively diagnosing risk factors, managing risk factors and symptoms with evidence-based therapies, monitoring the effect of treatment on the patient, and changing the medication if treatment goals are not being met. Adherence can be maximized by choosing medication that is easy for patients to take (e.g., once daily medications, single-pill combinations), using digital tools to deliver reminders and feedback, and investigating and removing (where possible) other barriers that affect a patient’s medication-taking behavior.
Cardiovascular disease (CVaD) is a significant global health issue, responsible for 30% of global deaths and affecting ∼598 million people in 2025; this prevalence is expected to double in the next 25 years, with increases in every region of the world [1].
The pathogenic process of CVaD is a continuum in which risk factors develop and accumulate, causing vascular and end-organ damage that becomes symptomatic and irreversible [2]. The global increase in CVaD incidence is being fueled by the twin epidemics of ‘diabesity’ (diabetes and obesity) and hypertension [3], key modifiable risk factors for which there are effective treatments.
There are multiple steps along the pathogenic continuum in which patient outcomes can be modified, by identifying risk factors, prescribing appropriate treatments and following up patients regularly to evaluate their ongoing adherence, health and well-being. In addition to the ‘classical’ CVaD risk factors of age, sex, smoking, hyperlipidemia, hypertension, obesity, renal dysfunction and diabetes, there is growing recognition that an unhealthy diet, a sedentary lifestyle, ethnicity and socioeconomic status also contribute to CVaD risk [4]. Risk factors are often shared between cardiovascular, renal and metabolic diseases. The presence of additional conditions, such as obesity in a patient with CVaD or renal disease in a patient with diabetes, accelerates and amplifies the progression of all three [5]. This has led to increasing recognition of cardiovascular–kidney–metabolic syndrome as a clinical entity requiring a holistic approach to patient management [5,6]. There is also growing evidence that disease in an arterial vascular bed is commonly associated with chronic venous disease (CVeD) [7]. Yet, unfortunately, data show that many of the opportunities for effective intervention are being missed [8].
A symposium was held at the meeting of the European Association of Preventive Cardiology in Milan, Italy on 4 April 2025, discussing the interconnectedness of conditions on the CVaD continuum and their relationship with CVeD. The current narrative review describes the content of that symposium, focusing on ways in which the clinical paradigm for CVaD needs to be re-examined and how healthcare professionals (HCPs) can optimize patient management to address the global burden of CVaD and CVeD.
Materials & methods
This review is based on the presentations at the symposium. The speakers at the symposium (and authors of this review) conducted literature searches of PubMed to identify articles relevant to their presentations. Additional ad hoc searches of PubMed were undertaken during the development of the review to support specific statements.
Peripheral & central vascular disease
Peripheral arterial disease (PAD) is a well-established marker of CVaD and a predictor of cardiovascular death, principally because disease in one vascular bed (such as the lower extremity) is often a marker of disease in another (such as the coronary or carotid arteries) [9]. Among patients with intermittent claudication, within 5 years of diagnosis 1.1% will progress to chronic limb-threatening ischemia, but only about 0.2% will require major limb amputation (due to improvements in limb salvage) [10]. However, the 5-year mortality rate is 19–26.7% [10–12], with CVaD the leading cause of death in patients with PAD [10,12]. Unlike the reduction in coronary artery disease (CAD) mortality rates seen in the last 20 years, the PAD mortality rate has not significantly changed, partially because of late diagnosis with higher atheroma burden, but also because of underdiagnosis and undertreatment [9].
Peripheral venous disease & CVaD
Peripheral vascular disease affects not only arterial circulation but venous circulation too; indeed, CVeD is more prevalent than CVaD. CVeD is classified using the clinical, etiological, anatomical, pathophysiological (CEAP) system with the clinical severity graded from C0 (no visible or palpable signs of venous disease) to C6 (active venous ulcer) [13]. Prevalence of some degree of CVeD (CEAP grade C1–C6) was 63.7% when estimated using data from the Vein Consult program involving 23 countries, and the prevalence of chronic venous insufficiency (CVI; CEAP grade C3–C6) was 26.0% [14]. Importantly, preclinical venous disease can be present from a young age: the Bochum study detected reflux in the great saphenous vein in 2.4% of 11- to 12-year-olds and 10.4% of 14- to 16-year-olds [15].
Venous disease tends to progress quickly. About 30% of the young people in the Bochum study with reflux went on to develop truncal varicose veins within 4 years [15]. In the Edinburgh Vein study, the annual rate of progression among patients with CVI or varicose veins was 4.3% [16]. A different study reported 22% of patients with untreated varicose veins (CEAP grade C2) progressing to a venous ulcer (CEAP grade C6) within 6 years [17].
There is accumulating evidence for an association between CVeD and CVaD [18–21]. For example, the Gutenberg Health Study examined the relationship between CVI and CVaD in 12,423 people aged 40–80 years [18]. The majority of patients (91.5%) had some type of CVeD (CEAP grade C1 or higher) and 43.2% had CVI (CEAP grade C3–C6). The prevalence of both cardiovascular risk factors (Figure 1A) and CVaD (Figure 1B) increased with worsening CEAP grade. Patients with more severe CVI (CEAP grades C4–C6) comprised 11.7% of the population. At least 70% of this latter group had hypertension, 40% were obese, almost 20% had diabetes, 10% had CAD and 10% had PAD [18]. Indeed, CVI (CEAP grades C3–C6) was a significant independent predictor of CVaD (p = 0.002), even after adjustment for age, sex and traditional risk factors (hypertension, diabetes, dyslipidemia, family history of CVaD, obesity and smoking) [18]. Patients with more severe CVI had a 10-year CVaD event risk of 23.3%. CVI was also a significant predictor of all-cause death (p < 0.0001), even after adjustment for age, sex and traditional risk factors, and medication use, in the overall population and in the subgroup of patients without prevalent CVaD at baseline (p = 0.006) [18].
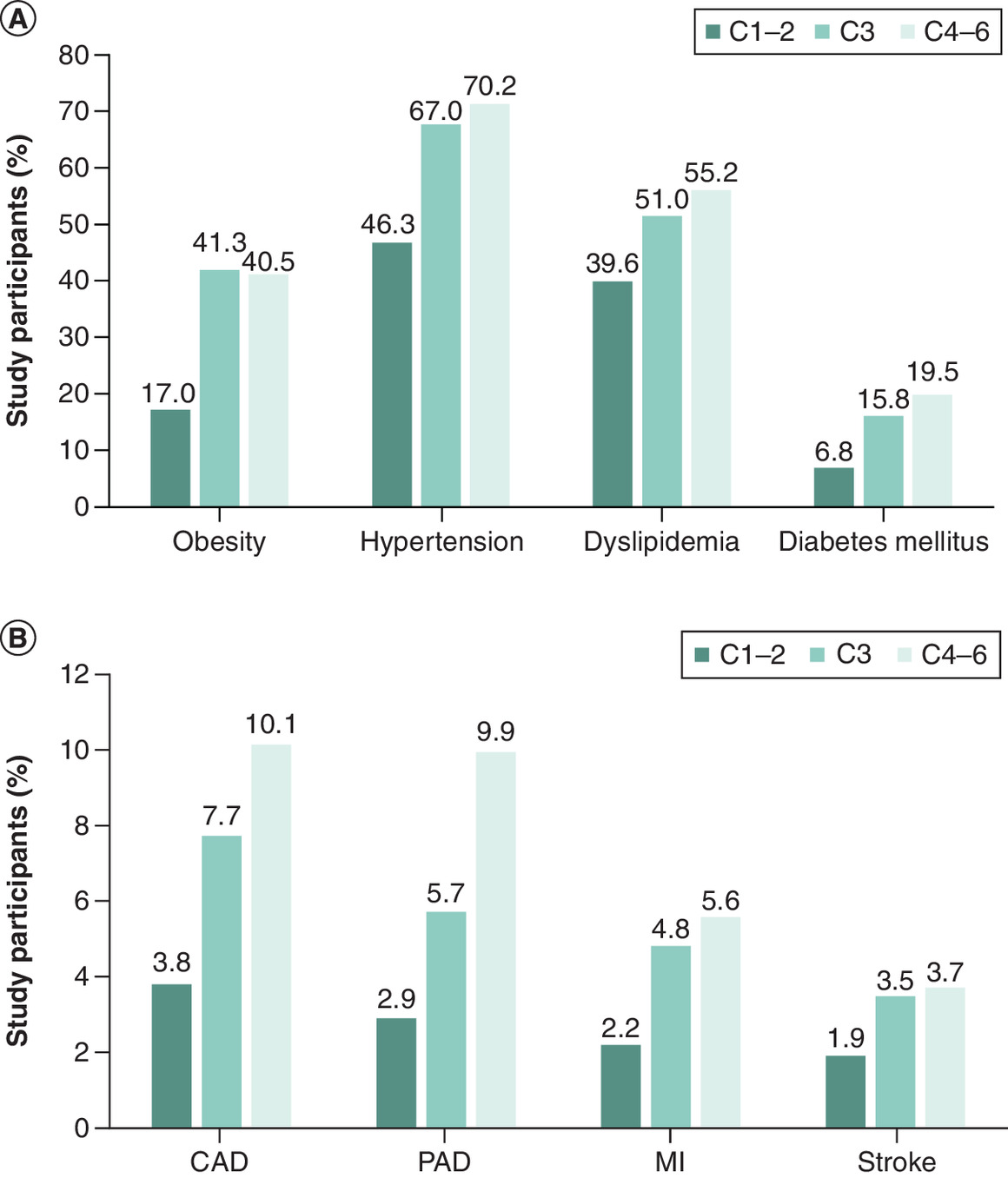
Figure 1. The prevalence of cardiovascular risk factors and cardiovascular disease increases with worsening clinical, etiological, anatomical and pathophysiologica grade in patients with chronic venous disease.
Data are from the Gutenberg Health Study. (A) Cardiovascular risk factor prevalence. (B) Cardiovascular disease prevalence [18].
C1: Telangiectasias or reticular veins; C2: Varicose veins; C3: Oedema; C4: Skin or subcutaneous changes; C5: Healed venous ulcer; C6: Active venous ulcer. CAD: Coronary artery disease; CEAP: clinical, etiological, anatomical, pathophysiological; MI: Myocardial infarction; PAD: Peripheral arterial disease. Obesity was defined as body mass index >30 kg/m2.
Paradigm shift
Venous and arterial disease not only share common risk factors, but they also share common pathogenic pathways (Figure 2), including endothelial dysfunction, increased vascular permeability, oxidative stress, renin–angiotensin–aldosterone system (RAAS) activation and inflammation [7,22,23] (Figure 3). The interconnectedness of these conditions highlights the need for a paradigm shift in the management of CVaD, in which a more coherent approach is taken to the identification and management of shared risk factors and comorbidities. Yet, many cardiometabolic and vascular conditions remain underdiagnosed [24–26] and therefore untreated. Among those who are treated, achievement of guideline-recommended goals is consistently low for most risk factors (in anywhere from 40 to 70% of patients, Figure 3), including low-density lipoprotein (LDL) cholesterol [27–31], blood pressure (BP) [29,32,33] and glycated hemoglobin (HbA1c) [34,35]. Failure to achieve and maintain risk factor targets is usually the result of therapeutic inertia or poor medication adherence [36], which may be prevalent in up to 50% of patients (Figure 3). Not meeting such targets increases the risk of morbidity and mortality [37–45].
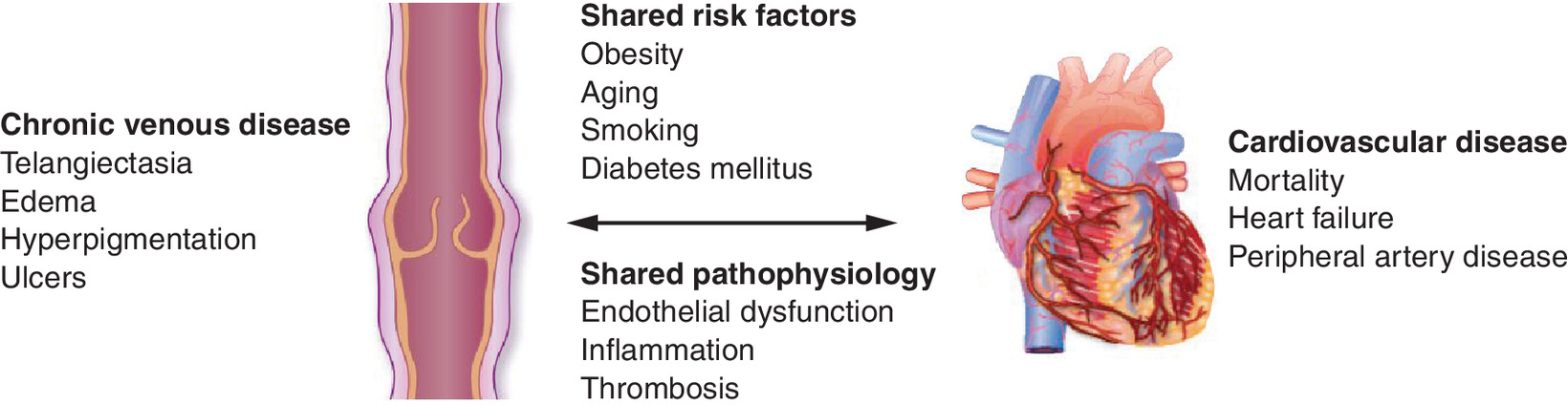
Figure 2. Shared risk factors and pathogenic processes in arterial and venous vascular disease.
Reproduced by permission of Oxford University Press on behalf of the European Society of Cardiology from Hamburg NM [7].
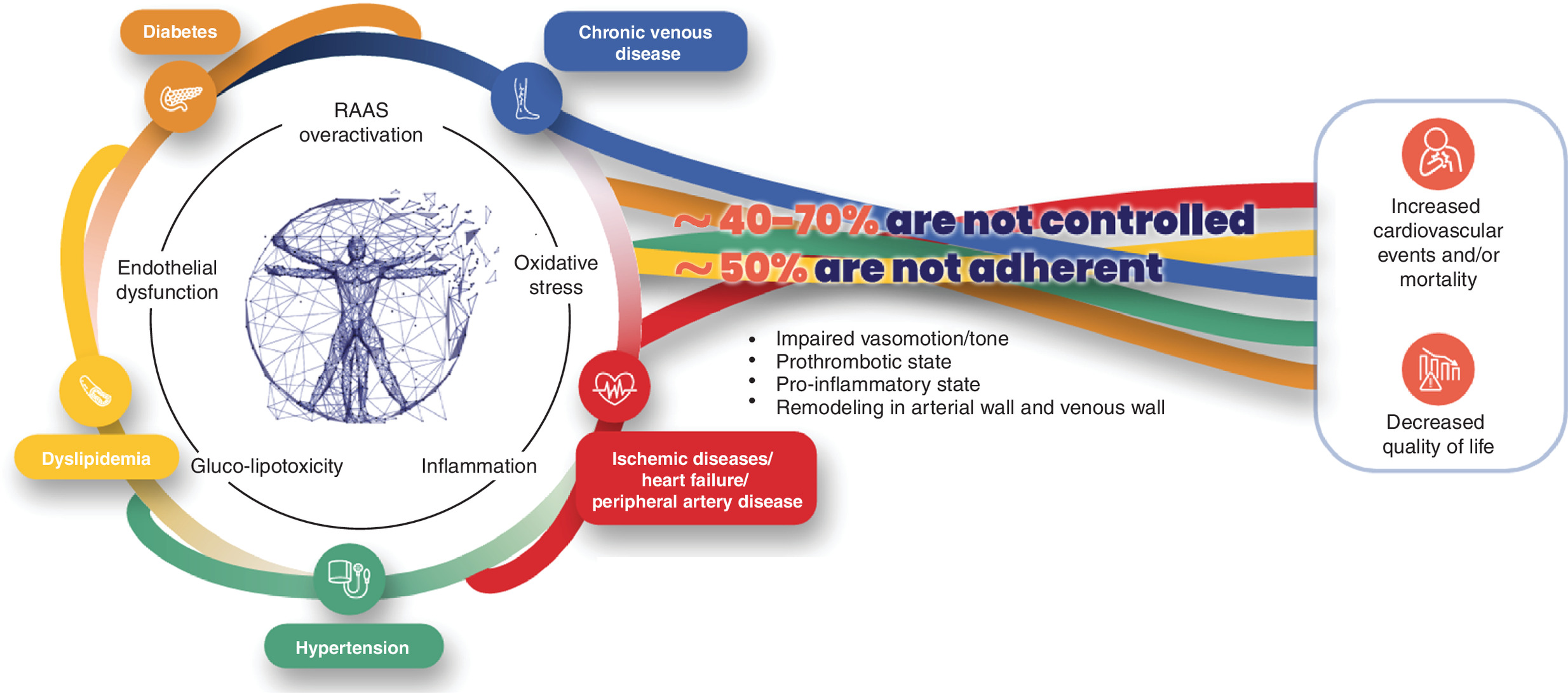
Figure 3. The interconnectedness of arterial and venous disease, and cardiometabolic risk factors, warrants a paradigm shift in which all of these are seen as inter-related elements of the same pathogenic process requiring effective treatment to improve outcomes.
Holistic treatment of CVeD
The key guideline-recommended therapies for CVeD are exercise and lifestyle changes (class IIa recommendation; level of evidence B), compression therapy (class IIa recommendation; level of evidence B), venoactive drugs (class IIa recommendation; level of evidence A) or surgery (class I recommendation; level of evidence B or C) [51]. All of these treatments are aimed at reducing venous hypertension, and they reduce inflammation either directly (as exercise and many venoactive drugs do) or indirectly as a secondary effect of reducing venous pressure [52].
Venoactive drugs target cellular pathophysiological cascades, similarly to medications for arterial hypertension, hypercholesterolemia and diabetes mellitus, and as such, are a highly effective class of therapy for CVeD. Venoactive agents improve the symptoms of venous disease (Table 1) through various mechanisms of action (Table 2) [51–53], mainly improving vascular tone, reducing venous capillary leakage and having an antioxidant effect [52]. More data support the use of micronized purified flavonoid fraction versus other venoactive agents [46]. The question remains as to whether these agents could have similar beneficial effects on arterial endothelium and as such, help reduce cardiovascular risk in patients with venous disease. Studies are urgently required to address this question.
| MPFF | Anthocyanins (red vine leaf extracts) | Rutosides | Ruscus extracts | Horse chestnut extract | Calcium dobesilate |
|---|---|---|---|---|---|
| Pain, heaviness, feeling of swelling, discomfort, cramps, paresthesia, burning, redness, skin changes/trophic disorders, oedema, venous ulcer | Pain, oedema | Pain, heaviness, cramps, swelling, paresthesia, pruritus, oedema | Pain, heaviness, feeling of swelling, fatigue, cramps, paresthesia, pruritus, oedema | Pain, pruritus, oedema | Pain, heaviness, discomfort, fatigue, cramps, swelling, restless legs, paresthesia, pruritus, oedema |
Adapted from De Maeseneer MG et al. [51], licensed under CC BY 4.0 (https://creativecommons.org/licenses/by/4.0/). Changes include minor changes to column titles, selection of drugs represented in table, and data are shown using text rather than tick-mark symbols. Additional effects are shown for some drugs based on information from other sources [52,53].
MPFF: Micronized purified flavonoid fraction.
| Venoactive drugs | Evidence exists for effects on | |||||
|---|---|---|---|---|---|---|
| Venous tone | Venous wall and valve | Capillary leakage | Lymphatic drainage | Hemorheological disorders | Free radical scavenging | |
| Flavonoids (gamma-benzopyrones) | ||||||
| MPFF | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Non-micronized or synthetic diosmins | No data | No data | No data | No data | No data | No data |
| Rutin and rutosides | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Anthocyanins (Vitis vinifera) | ✓ | |||||
| Proanthocyanidins (Vitis vinifera) | ✓ | ✓ | ||||
| Alpha-benzopyrones | ||||||
| Coumarin | ✓ | ✓ | ||||
| Saponins | ||||||
| Horse chestnut seed extract (aescin) | ✓ | ✓ | ||||
| Ruscus extract | ✓ | ✓ | ✓ | ✓ | ||
| Other plant extracts | ||||||
| Gingko extracts | No data | No data | No data | No data | No data | No data |
| Synthetic products | ||||||
| Calcium dobesilate | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Benzarone | No data | No data | No data | No data | No data | No data |
| Naftazone | No data | No data | No data | No data | No data | No data |
MPFF: Micronized purified flavonoid fraction.
Reprinted by permission of Edizioni Minerva Medica [52].
The challenge of multimorbidity
Data from the ongoing, observational BRING-UP Prevention study being conducted at 189 cardiology centers across Italy illustrates the multimorbidity present in the CVaD patient population [54]. Patients are included in the study if they have stable atherothrombotic disease, which includes CAD (history of ACS or revascularization), cerebrovascular disease (history of ischemic stroke or carotid revascularization) or PAD (intermittent claudication with objective evidence of PAD, peripheral revascularization or lower leg amputation as a result of PAD). Figure 4A shows the extent to which these patients have multiple cardiovascular risk factors and Figure 4B the extent of vascular disease and other comorbidities. Among the 4790 patients enrolled during the first phase of this study, 4694 (98.0%) had CAD, 292 (6.1%) had cerebrovascular disease and 329 (6.9%) had PAD, with some patients having involvement in more than one vascular bed [54]. About half of the patients in the BRING-UP Prevention cohort are overweight, with BMI >27 kg/m2 in 42.7% (n = 2044), and one in five patients is obese (BMI ≥30 kg/m2, n = 945 [19.7%]). Although the mean systolic BP (SBP) for the overall cohort was within the target range (120.9 mmHg), 2298 patients (48.0%) had SBP ≥130 mmHg [54]. Around a third of patients (32.6%) had LDL cholesterol levels below the level recommended by the European Society of Cardiology (<55 mg/dl), and 47.2% of patients had LDL cholesterol levels in excess of 70 mg/dl [54]. These data demonstrate that considerable proportions of patients with multimorbidity do not meet therapeutic targets for risk factor control.
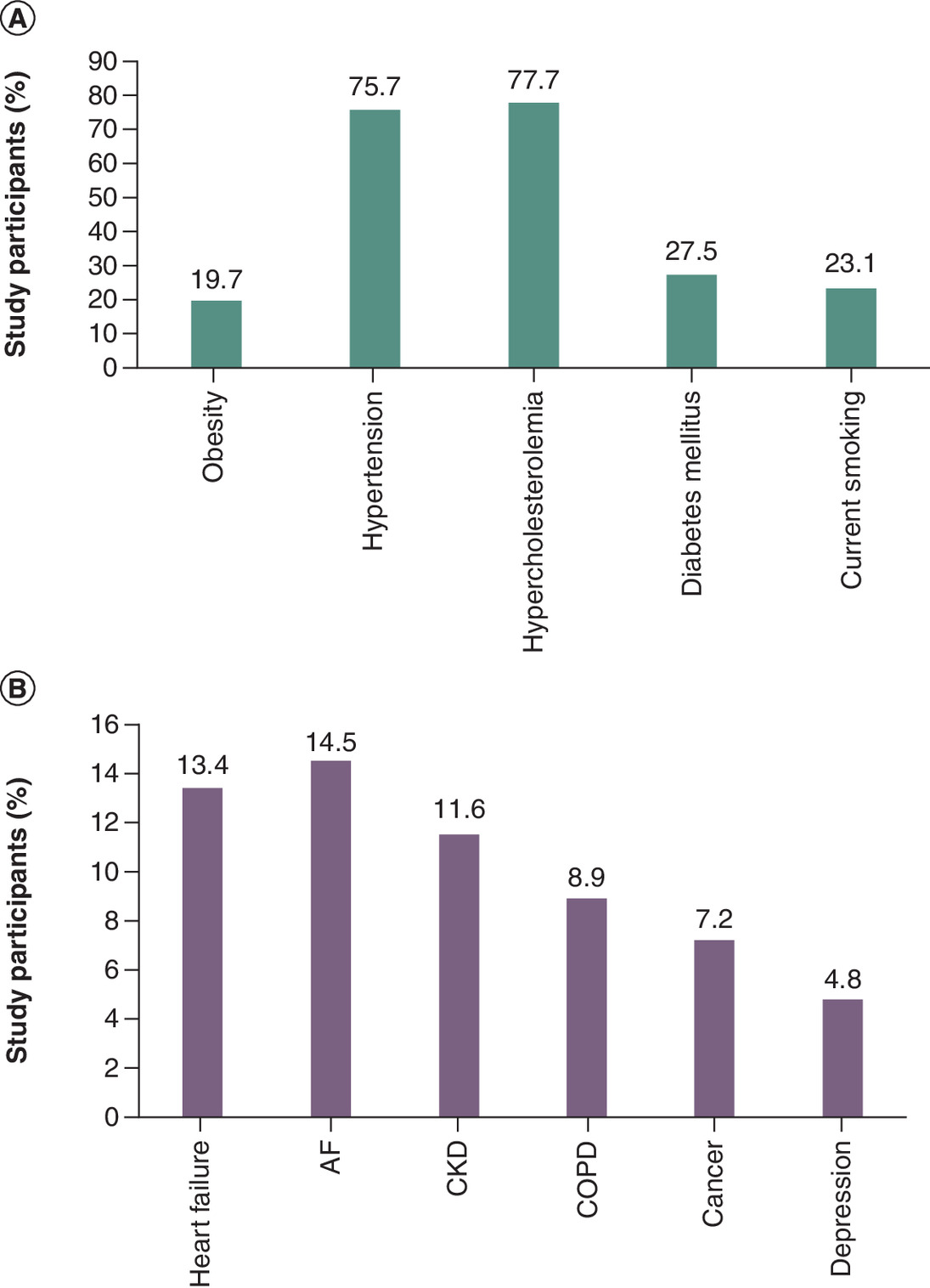
Figure 4. Multimorbidity in 4790 patients with atherothrombotic disease in the BRING-UP Prevention study in Italy.
The prevalence of (A) cardiovascular risk factors and (B) comorbidities [54].
AF: Atrial fibrillation; CKD: Chronic kidney disease; COPD: Chronic obstructive pulmonary disease.
Similar findings have been made in the international SNAPSHOT observational studies in patients with hypertension, which appear to confirm that many patients with one CVaD risk factor have multiple comorbidities (Table 3) [55–57]. Further, the majority of these patients (65–87%) are at very high risk of a CVaD event [55–57]. SNAPSHOT investigators suggested that physicians consistently underestimate patients' risk levels [55,57]. Although the data from the SNAPSHOT studies have not yet been fully published, initial indications suggest that most patients do not have BP, LDL cholesterol or glycemic indices controlled to guideline-recommended levels [55,57].
Missed opportunities
The studies discussed above highlight consistently missed therapeutic opportunities in the management of patients with CVaD and/or CVeD. In our view there are two key reasons: therapeutic inertia and patient treatment adherence.
Therapeutic inertia
The American Heart Association published a Call to Action in 2019, identifying points in the therapeutic continuum where opportunities to improve outcomes are missed, including failure to diagnose and modify risk factors such as hypertension and dyslipidemia, failure to elicit and monitor patient’s goals and needs, failure to use evidence-based interventions, and eventually failure to provide advanced, supportive and palliative care in the final stages of CVaD [8]. One reason for this (as demonstrated in the SNAPSHOT data) is that physicians often underestimate a patient’s CV risk and overestimate the extent to which risk factors such as BP and lipid levels are controlled [60,61]. This underestimation of risk and overestimation of control may lead to therapeutic inertia, whereby treatment is not appropriately escalated to achieve target levels.
The contribution of therapeutic inertia to poor patient outcomes is being addressed internationally by a number of groups [62,63]. Drawing on the available research, these initiatives highlight a number of key determinants of improving therapeutic inertia, including collaborative and team-based care with shared decision-making and personalized management plans [62–64], and increased use of guideline-recommended therapies [62–64].
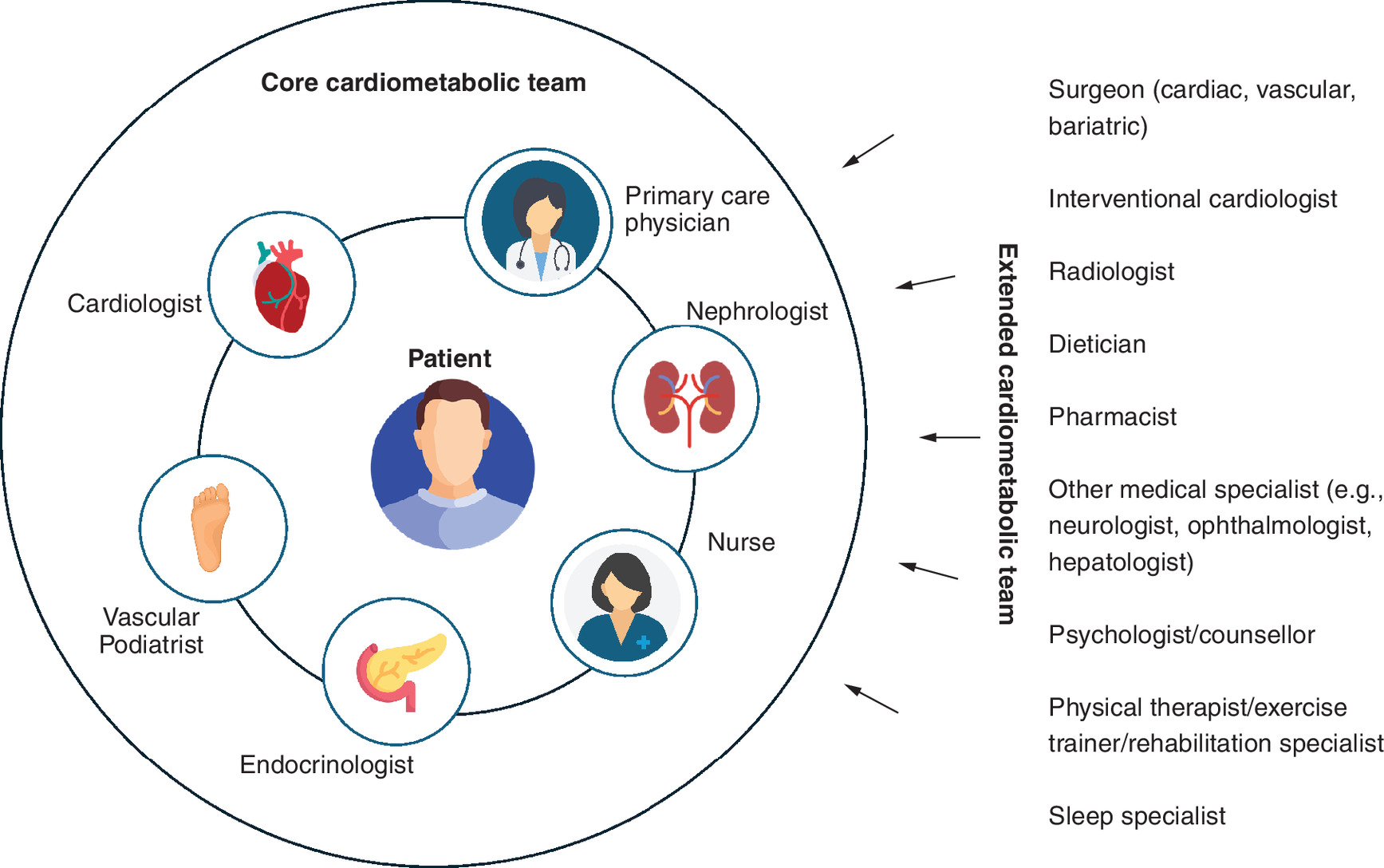
Collaborative care requires the formation of alliances between individual HCPs; in a process the American Diabetes Association has termed “collaborative barrier busting” [63]. The key is to engage a core multidisciplinary team around the patient and co-opt additional HCPs into the patient’s care when the need arises or to address specific comorbidities [65]. An example of what these teams may look like is shown in Figure 5; ideally the core care team will include a cardiologist, vascular podiatrist, endocrinologist, nurse(s), nephrologist as well as their primary care physician, with multiple other specialists involved in the extended cardiometabolic team. In order to do this, systems have to be developed that encourage constructive communication with the patient and between HCPs, which may include the use of information technology to share information [65]. In addition, medical education at both the undergraduate and postgraduate level should be revised to include a more holistic and multidisciplinary approach to cardiometabolic disease prevention and management [6].
Such systemic changes often take time to implement, but in the meantime, steps can be taken to reduce therapeutic inertia by following international guidelines for early use of combination therapy. European Society of Hypertension (ESH) and European Society of Cardiology (ESC) guidelines now both recommend starting most patients with newly diagnosed hypertension on dual combination therapy with an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, calcium channel blocker or diuretic [66,67]. If this combination is ineffective, the guidelines recommend adding a third agent [66,67]. In patients with overt chronic CAD (angina pectoris), clinical guidelines also recommend the use of combination therapy, tailored to the patient’s clinical profile, hemodynamic status and the presence of vasospasm or microvascular dysfunction [68]. Recommended add-on therapy for chronic CAD includes trimetazidine [68], which (when added to metoprolol) has been shown to significantly reduce the incidence of anginal attacks and improve exercise tolerance in patients with angina, compared with metoprolol monotherapy [69]. The combination of trimetazidine + propranolol was also more effective than isosorbide dinitrate + propranolol for reducing anginal attacks [70].
Adherence
Adherence is difficult to measure but is commonly based on measures of prescription refills, with 80% adherence being the threshold defined as having a clinically relevant effect on outcomes in chronic disease [71]. Using this threshold, data indicate that adherence to cardiovascular preventive therapies is suboptimal, with between 40 and 70% of patients taking their medication as prescribed >80% of the time [50,72–75]. Moreover, about 50% of patients discontinue such therapies within the first 12 months [74]. The low adherence rates among patients with cardiovascular risk factors or CVaD led to the first World Adherence Day on 27 March 2025, drawing attention to the need for patients to take their medication as prescribed to optimize outcomes.
There are multiple factors associated with adherence related to the patient’s circumstances and health, the patient–doctor relationship, the healthcare system and the treatment prescribed (Table 4) [76]. It is important for HCPs to question their patients about adherence and identify potential barriers to adherence that can be addressed. One potential barrier is pill burden.
| Healthcare factors | Treatment-related factors | Patient-related factors | Condition-related factors |
|---|---|---|---|
| • Poor patient–physician relationship/communication • Fragmented care • Lack of follow-up • Short consultation times • Healthcare professional knowledge gap about adherence (generally and specific to the individual patient) | • Complex regimens/pill burden • Need for titration/dose adjustment • Adverse events (actual or perceived) • Lack of feedback • Stigma (e.g., for injectable medications) • Interference with daily life (e.g., medication timing in relation to food and frequent urination caused by diuretics) | • Age • Cognitive impairment/forgetfulness • Physical impairments (e.g., hearing, visual and manual dexterity) • Patient expectations and goals • Psychosocial factors (e.g., stress, depression and anxiety) • Language barriers • Social embarrassment/stigma • Socioeconomic circumstances (e.g., cost of medication and insurance coverage) • Health literacy/educational level • Access to pharmacy • Social support (e.g., spouse, family and friends) | • Chronicity • Lack of symptoms (e.g., for lipid levels and blood pressure) • Long asymptomatic phases (e.g., if condition associated with flares) |
| Data are from Nelson et al. [76]. | |||
Adherence tends to be lower in patients taking more than one type of cardiovascular therapy, i.e., patients taking antihypertensive and lipid-lowering therapy have better adherence for one type of treatment than for both [75,77]. Pill burden may contribute to this phenomenon, since adherence has been shown to decrease as the number of prescription medicines increase [72]. One easy approach to enhancing adherence is to simplify the treatment regimen, by discontinuing unnecessary medications, prescribing agents that are active against more than one cardiovascular risk factor (e.g., treatments for diabetes that cause weight loss, treatments for hypertension that also have renoprotective effects) [23], prescribing once daily medications wherever possible, and considering single-pill combination (SPC) therapies to reduce the pill burden [76].
SPCs have been shown to improve adherence and outcomes across a range of cardiometabolic indications, including hypertension [78], dyslipidemia [79,80] and diabetes [81,82] (Table 5). The use of SPCs is now a class I recommendation in European guidelines for hypertension [66] and chronic CAD [68], to enhance adherence and persistence.
| Cardiometabolic indication | Study | Treatment | Comparator groups (n) | % patients adherent¶ | Patient outcomes | Ref. |
|---|---|---|---|---|---|---|
| Hypertension | Healthcare database study of matched cohorts (Italy) | PER/IND/AML | SPC (n = 12,150) vs FCT (n = 6105) | 59.9 vs 26.9%‡ | Mortality (1000-person/year): 29.9 vs 33.7† Composite death/CV event (1000-person/year): 105.8 vs 139.0‡ | [78] |
| Dyslipidemia | Healthcare database study (Italy) | ROS/EZE | SPC (n = 25,886) vs FCT (n = 7309) | Overall 56.8% vs 44.5%‡ By CV risk level Very high: 65.4 vs 50.4%‡ High: 54.7 vs 42.7%‡ Other: 43.5 vs 35.9%‡ | % pts achieving LDL-C targets# by CV risk level: Very high: 35.4 vs 23.8%‡ High: 46.9 vs 23.1%‡ Other: 71.6 vs 49.5%‡ | [80] |
| Healthcare database study (Italy) | ROS/EZE | SPC (index period) vs FCT (pre-index period) (n = 1219) | 75.2 vs 51.8%‡ | – | [79] | |
| Diabetes | National registry matched cohort study (Sweden) | Metformin + (SGLT2i/DPP4i/TZD) | SPC (n = 13,883) vs FCT (n = 13,883) | 68.6 vs 46.5% | HF rate (per 1000-person years): 8.1 vs 9.2 (HR: 0.88; 95% CI: 0.79–0.99) | [82] |
†
p < 0.05.
‡
p < 0.001.
§
Referred to also as loose-dose combination therapy.
¶
#
LDL-C targets were <55 mg/dL in very high CV risk group, <70 mg/dL in the high-risk group and <116.mg/dL in other risk group [80].
Data are from selected representative studies.
AML: Amlodipine; CI: Confidence interval; CV: Cardiovascular; DPP4i: Dipeptidyl peptidase 4 inhibitor; EZE: Ezetimibe; FCT: Free combination therapy; HF: Heart failure; HR: Hazard ratio; IND: Indapamide; LDL-C: Low-density lipoprotein cholesterol; PDC: Proportion of days covered; PER: Perindopril; ROS: Rosuvastatin; SGLT2i: Sodium-glucose cotransporter 2 inhibitor; SPC: Single-pill combination; TZD: Thiazolidinedione.
Other approaches to enhancing adherence include digital tools, such as smart phone apps, wearable devices and text messaging [66,68,76]. These digital tools have proven to significantly improve outcomes in patients with chronic cardiovascular conditions, particularly hypertension [83–85], with data showing that adherence is maximized by initiatives that include more than one type of e-health intervention [72]. As well as providing patients with reminders and feedback, these digital tools can enhance health literacy [86] and help to overcome some of the barriers to risk factor management seen in underserved communities [87].
Conclusions
Addressing the escalating global burden of CVaD necessitates a paradigm shift toward a more integrated, holistic approach to patient management. Recognizing the interconnectedness of arterial and venous vascular conditions, along with shared risk factors such as diabetes, obesity, hypertension and socioeconomic determinants, is crucial for early identification and comprehensive treatment. Clinicians must prioritize timely diagnosis, aggressive risk factor modification and adherence to evidence-based therapies, leveraging multidisciplinary teams and innovative strategies like single-pill combinations and digital health tools to combat therapeutic inertia and improve adherence. Future research should focus on elucidating the role of CVeD in cardiovascular risk, developing targeted interventions, and implementing systemic healthcare reforms that promote proactive, personalized care. Ultimately, such efforts will optimize outcomes, reduce disability and mitigate the devastating impact of CVaD worldwide.
Summary points
•
Cardiovascular disease (CVaD) is a prevalent health condition frequently accompanied by chronic venous disease (CVeD).
•
CVaD risk factors such as obesity, diabetes and hypertension adversely affect the structure and function of arteries and veins.
•
Damage to the veins, known as CVeD, shares common risk factors and pathogenic pathways with CVaD.
•
Mainstays of treatment for CVeD are exercise, compression therapy, venoactive drugs and surgery.
•
Unfortunately, patients with CVaD and/or CVeD or their risk factors are frequently underdiagnosed and untreated.
•
Patients may not achieve guideline-recommended targets for disease control of hypertension, dyslipidemia and diabetes due to therapeutic inertia and/or poor medication adherence.
•
A coherent approach is needed to identify and manage shared risk factors and comorbidities.
•
The authors propose that multidisciplinary teams formulate a clear strategy for patient care, that they utilize treatments for which there is strong evidence of effectiveness, and that tools to maximize adherence be used, particularly in patients with multiple risk factors or comorbidities.
Author contributions
All authors contributed to the conception of this review and drafting of the manuscript. Each author commented on every version of the manuscript, and read and approved the final manuscript.
Financial disclosure
The symposium at the European Association of Preventive Cardiology (Milan, Italy; April 2025) on which this review is based, and the open access publishing fee were sponsored by Servier.
Competing interests disclosure
K Hafidh has received research grants, speaker engagement fees and participated in advisory boards for Novo Nordisk, Lilly, Sanofi, Servier, MSD, Pfizer, Roche Diagnostics, AstraZeneca, Zeullig Pharma, Novartis and Abbot. M Vega de Ceniga has received speaker engagement fees from Servier, Convatec and Urgo. C Borghi has received speaker engagement fees for Servier Pharma, Recordati Pharma, EGIS Pharma, Berlin Chamie and Menarini Pharma. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
The authors thank Catherine Rees and Miriam Robinson who provided medical writing assistance in the preparation of the manuscript on behalf of Springer Health+, and Tracy Harrison of Springer Health+ who provided post-submission editorial assistance. This medical writing assistance was funded by Servier.
Ethical conduct of research
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Data availability
Data sharing is not applicable to this article because the article reviews the existing literature, and no new datasets were generated or analyzed.
Open access
This work is licensed under the Creative Commons Attribution 4.0 License. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Chong B, Jayabaskaran J, Jauhari SM et al. Global burden of cardiovascular diseases: projections from 2025 to 2050. Eur. J. Prev. Cardiol. 32(11), 1001–1015 (2025).
2.
Chrysant SG. A new paradigm in the treatment of the cardiovascular disease continuum: focus on prevention. Hippokratia 15(1), 7–11 (2011).
3.
Vaduganathan M, Mensah GA, Turco JV et al. The global burden of cardiovascular diseases and risk: a compass for future health. J. Am. Coll. Cardiol. 80(25), 2361–2371 (2022).
4.
Bays HE, Taub PR, Epstein E et al. Ten things to know about ten cardiovascular disease risk factors. Am. J. Prev. Cardiol. 5, 100149 (2021).
5.
Ndumele CE, Neeland IJ, Tuttle KR et al. A synopsis of the evidence for the science and clinical management of cardiovascular-kidney-metabolic (CKM) syndrome: a scientific statement from the American Heart Association. Circulation 148(20), 1636–1664 (2023).
6.
International Cardiometabolic Working Group, Krentz A, Jacob S et al. Rising to the challenge of cardio-renal-metabolic disease in the 21st century: translating evidence into best clinical practice to prevent and manage atherosclerosis. Atherosclerosis 396, 118528 (2024).
7.
Hamburg NM. The legs are a pathway to the heart: connections between chronic venous insufficiency and cardiovascular disease. Eur. Heart J. 42(40), 4166–4168 (2021).
• This editorial highlights the interconnectedness of chronic venous insufficiency, cardiovascular disease (CVaD) and mortality, and was published on behalf of the European Society of Cardiology.
8.
McClellan M, Brown N, Califf RM et al. Call to action: urgent challenges in cardiovascular disease: a presidential advisory from the American Heart Association. Circulation 139(9), e44–e54 (2019).
9.
Nordanstig J, Behrendt CA, Baumgartner I et al. European Society for Vascular Surgery (ESVS) 2024 Clinical Practice Guidelines on the Management of Asymptomatic Lower Limb Peripheral Arterial Disease and Intermittent Claudication. Eur. J. Vasc. Endovasc. Surg. 67(1), 9–96 (2024).
• This clinical practice guideline provides valuable insight into how asymptomatic lower limb peripheral arterial disease and intermittent claudication are managed, specifically providing data on underdiagnosis and undertreatment.
10.
Kumakura H, Kanai H, Hojo Y et al. Long-term survival and fate of the leg in de novo intermittent claudication. Eur. Heart J. Qual. Care Clin. Outcomes 3(3), 208–215 (2017).
11.
Kreutzburg T, Peters F, Kuchenbecker J et al. Editor's Choice - The GermanVasc Score: a pragmatic risk score predicts five year amputation free survival in patients with peripheral arterial occlusive disease. Eur. J. Vasc. Endovasc. Surg. 61(2), 248–256 (2021).
12.
Sartipy F, Sigvant B, Lundin F et al. Ten year mortality in different peripheral arterial disease stages: a population based observational study on outcome. Eur. J. Vasc. Endovasc. Surg. 55(4), 529–536 (2018).
13.
Eklöf B, Rutherford RB, Bergan JJ et al. Revision of the CEAP classification for chronic venous disorders: consensus statement. J. Vasc. Surg. 40(6), 1248–1252 (2004).
14.
Vuylsteke ME, Colman R, Thomis S et al. An epidemiological survey of venous disease among general practitioner attendees in different geographical regions on the globe: the final results of the Vein Consult Program. Angiology 69(9), 779–785 (2018).
• Presents the final results of the Vein Consult Program, which was a global survey of venous disease among general practitioners using the clinical, etiological, anatomical, pathophysiological classification.
15.
Schultz-Ehrenburg U, Reich-Schupke S, Robak-Pawelczyk B et al. Propsective epidemiological study on the beginning of varicose veins. Phlebologie 38(1), 17–25 (2009).
16.
Lee AJ, Robertson LA, Boghossian SM et al. Progression of varicose veins and chronic venous insufficiency in the general population in the Edinburgh Vein Study. J. Vasc. Surg. Venous Lymphat. Disord. 3(1), 18–26 (2015).
17.
Salim S, Machin M, Patterson BO et al. Global epidemiology of chronic venous disease: a systematic review with pooled prevalence analysis. Ann. Surg. 274(6), 971–976 (2021).
18.
Prochaska JH, Arnold N, Falcke A et al. Chronic venous insufficiency, cardiovascular disease, and mortality: a population study. Eur. Heart J. 42(40), 4157–4165 (2021).
• Article clearly points out cardiovascular risk factors, particularly highlighting an association between chronic venous disease and CVaD.
19.
Singh TP, Velu RB, Quigley F et al. Association of chronic venous disease with major adverse cardiovascular events. J. Vasc. Surg. Venous Lymphat. Disord. 10(3), 683–688 (2022).
20.
Wu NC, Chen ZC, Feng IJ et al. Severe varicose veins and the risk of mortality: a nationwide population-based cohort study. BMJ Open 10(6), e034245 (2020).
21.
Guo X, Zhang K, Sun Y et al. Causal association of chronic venous insufficiency and cardiovascular diseases: a univariable and multivariable mendelian randomization study. Rev. Cardiovasc. Med. 25(10), 357 (2024).
22.
Marassi M, Fadini GP. The cardio-renal-metabolic connection: a review of the evidence. Cardiovasc. Diabetol. 22(1), 195 (2023).
23.
Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can. J. Cardiol. 34(5), 575–584 (2018).
24.
Argyriou C, Saleptsis V, Koutsias S et al. Peripheral arterial disease is prevalent but underdiagnosed and undertreated in the primary care setting in central Greece. Angiology 64(2), 119–124 (2013).
25.
Falagas ME, Vardakas KZ, Vergidis PI. Under-diagnosis of common chronic diseases: prevalence and impact on human health. Int. J. Clin. Pract. 61(9), 1569–1579 (2007).
26.
Rabe E, Régnier C, Goron F et al. The prevalence, disease characteristics and treatment of chronic venous disease: an international web-based survey. J. Comp. Eff. Res. 9(17), 1205–1218 (2020).
27.
Berteotti M, Profili F, Nreu B et al. LDL-cholesterol target levels achievement in high-risk patients: an (un)expected gender bias. Nutr. Metab. Cardiovasc. Dis. 34(1), 145–152 (2024).
28.
Bruckert E, Parhofer KG, Gonzalez-Juanatey JR et al. Proportion of high-risk/very high-risk patients in Europe with low-density lipoprotein cholesterol at target according to european guidelines: a systematic review. Adv. Ther. 37(5), 1724–1736 (2020).
29.
Elhiny R, O'Keeffe LM, Bodunde EO et al. Goal attainment, medication adherence and guideline adherence in the treatment of hypertension and dyslipidemia in Irish populations: a systematic review and meta-analysis. Int. J. Cardiol. Cardiovasc. Risk Prev. 24, 200364 (2025).
30.
Yun SJ, Jeong IK, Cha JH et al. Current status of low-density lipoprotein cholesterol target achievement in patients with Type 2 diabetes mellitus in Korea compared with recent guidelines. Diabetes Metab. J. 46(3), 464–475 (2021).
31.
Wang X, He Y, Wang T et al. Lipid-lowering therapy and low-density lipoprotein cholesterol (LDL-C) goal achievement in high-cardiovascular-risk patients in Fuzhou, China. J. Cardiovasc. Pharmacol. Ther. 25(4), 307–315 (2020).
32.
Bakris G, Sarafidis P, Agarwal R et al. Review of blood pressure control rates and outcomes. J. Am. Soc. Hypertens. 8(2), 127–141 (2014).
33.
Wang H, Song J, Liu Z et al. Time in target range for blood pressure and adverse health outcomes: a systematic review. Hypertension 82(3), 419–431 (2025).
34.
Bin Rakhis SA Sr, AlDuwayhis NM, Aleid N et al. Glycemic control for Type 2 diabetes mellitus patients: a systematic review. Cureus 14(6), e26180 (2022).
35.
Bitew ZW, Alemu A, Jember DA et al. Prevalence of glycemic control and factors associated with poor glycemic control: a systematic review and meta-analysis. Inquiry 60, 469580231155716 (2023).
36.
Yan X, Mudiganti S, Husby H et al. Medication non-adherence and therapeutic inertia independently contribute to poor disease control for cardiometabolic diseases. Sci. Rep. 12(1), 18936 (2022).
37.
Boussageon R, Bejan-Angoulvant T, Saadatian-Elahi M et al. Effect of intensive glucose lowering treatment on all cause mortality, cardiovascular death, and microvascular events in type 2 diabetes: meta-analysis of randomised controlled trials. BMJ 343, d4169 (2011).
38.
Brunström M, Carlberg B. Association of blood pressure lowering with mortality and cardiovascular disease across blood pressure levels: a systematic review and meta-analysis. JAMA Intern. Med. 178(1), 28–36 (2018).
39.
Deedwania P, Barter P, Carmena R et al. Reduction of low-density lipoprotein cholesterol in patients with coronary heart disease and metabolic syndrome: analysis of the Treating to New Targets study. Lancet 368(9539), 919–928 (2006).
40.
Hansson L, Lloyd A, Anderson P et al. Excess morbidity and cost of failure to achieve targets for blood pressure control in Europe. Blood Press. 11(1), 35–45 (2002).
41.
Orsi E, Bonora E, Solini A et al. Association between on-treatment haemoglobin A1c and all-cause mortality in individuals with Type 2 diabetes: importance of personalized goals and type of anti-hyperglycaemic treatment. J. Clin. Med. 9(1), 246 (2020).
42.
Yang Z, Deng Q, Hao Y et al. Effectiveness of treat-to-target cholesterol-lowering interventions on cardiovascular disease and all-cause mortality risk in the community-dwelling population: a target trial emulation. Nat. Commun. 15(1), 9922 (2024).
43.
Wong ND, Zhao Y, Patel R et al. Cardiovascular risk factor targets and cardiovascular disease event risk in diabetes: a pooling project of the Atherosclerosis Risk in Communities Study, Multi-Ethnic Study of Atherosclerosis, and Jackson Heart Study. Diabetes Care 39(5), 668–676 (2016).
44.
Hyttinen L, Strandberg TE, Strandberg AY et al. Effect of cholesterol on mortality and quality of life up to a 46-year follow-up. Am. J. Cardiol. 108(5), 677–681 (2011).
45.
Testa MA, Simonson DC. Health economic benefits and quality of life during improved glycemic control in patients with Type 2 diabetes mellitus: a randomized, controlled, double-blind trial. JAMA 280(17), 1490–1496 (1998).
46.
Gianesini S, De Luca L, Feodor T et al. Cardiovascular insights for the appropriate management of chronic venous disease: a narrative review of implications for the use of venoactive drugs. Adv. Ther. 40(12), 5137–5154 (2023).
47.
Cosín-Sales J, Campuzano Ruiz R, Díaz Díaz JL et al. Impact of physician's perception about LDL cholesterol control in clinical practice when treating patients in Spain. Atherosclerosis 375, 38–44 (2023).
48.
Prieto-Díaz MA, Pallares-Carratala V, Manuel Micó-Pérez R et al. Clinical characteristics, treatment, and blood pressure control in patients with hypertension seen by primary care physicians in Spain: the IBERICAN study. Front. Cardiovasc. Med. 10, 1295174 (2023).
49.
Rosano GMC, Vitale C, Spoletini I et al. Multidisciplinary approach and combination pharmacotherapy for the management of cardiometabolic patients. J. Cardiovasc. Med. (Hagerstown) 26(6), 297–302 (2025).
50.
Kirkman MS, Rowan-Martin MT, Levin R et al. Determinants of adherence to diabetes medications: findings from a large pharmacy claims database. Diabetes Care 38(4), 604–609 (2015).
51.
De Maeseneer MG, Kakkos SK, Aherne T et al. Editor's Choice - European Society for Vascular Surgery (ESVS) 2022 Clinical Practice Guidelines on the Management of Chronic Venous Disease of the Lower Limbs. Eur. J. Vasc. Endovasc. Surg. 63(2), 184–267 (2022).
52.
Nicolaides A, Kakkos S, Baekgaard N et al. Management of chronic venous disorders of the lower limbs. Guidelines According to Scientific Evidence. Part I. Int. Angiol. 37(3), 181–254 (2018).
53.
Nicolaides A, Kakkos S, Baekgaard N et al. Management of chronic venous disorders of the lower limbs. Guidelines According to Scientific Evidence. Part II. Int. Angiol. 39(3), 175–240 (2020).
54.
Colivicchi F, Fabbri G, Oliva F et al. LDL-cholesterol levels and lipid lowering therapy in secondary prevention. Baseline data from the BRING-UP prospective registry. Int. J. Cardiol. 433, 133290 (2025).
• The ongoing, observational BRING-UP Prevention study, provides valuable information on the challenges of multimorbidity at 189 cardiology centers in Italy.
55.
Camafort M, Dzudie A, Ivanovic B et al. Blood pressure control and cardiovascular risk assessment in patients with hypertension: a pooled analysis of 6 countries in Eastern and Southern Europ (SNAPSHOT study). Eur. Heart J. 45(Suppl. 1), ehae666.2549 (2024).
56.
Quintero-Baiz A, Benavides JAC, Correa RCR et al. Cardiovascular risk assessment in hypertensive patients with Type 2 diabetes: a cross-sectional epidemiological study in Colombia (SNAPSHOT study). J. Hypertens. 42(Suppl. 3), e106 (2024).
57.
Quintero-Baiz A, Herazo JJB, Gomez JOI et al. Cardiovascular risk factor control in hypertensive patients with Type 2 diabetes: a cross-sectional epidemiological study in Colombia (SNAPSHOT study). J. Hypertens. 42(Suppl. 3), e98–e99 (2024).
58.
SCORE2 working group, ESC Cardiovascular risk collaboration. SCORE2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 42(25), 2439–2454 (2021).
59.
SCORE2-OP working group, ESC Cardiovascular risk collaboration. SCORE2-OP risk prediction algorithms: estimating incident cardiovascular event risk in older persons in four geographical risk regions. Eur. Heart J. 42(25), 2455–2467 (2021).
60.
Erdine S, Redon J, Bohm M et al. Are physicians underestimating the challenges of hypertension management? Results from the Supporting Hypertension Awareness and Research Europe-wide (SHARE) survey. Eur. J. Prev. Cardiol. 20(5), 786–792 (2013).
61.
Banegas JR, Lundelin K, de la Figuera M et al. Physician perception of blood pressure control and treatment behavior in high-risk hypertensive patients: a cross-sectional study. PLOS One 6(9), e24569 (2011).
62.
Almahmeed W, Alabadla Z, Al Awadi F et al. Improving therapeutic adherence and reducing therapeutic inertia in the management of people with cardiometabolic diseases: a call-to-action from the middle east. Adv. Ther. 42(3), 1340–1359 (2025).
63.
Gabbay RA, Kendall D, Beebe C et al. Addressing therapeutic inertia in 2020 and beyond: a 3-year initiative of the American Diabetes Association. Clin. Diabetes 38(4), 371–381 (2020).
64.
Dixon DL, Sharma G, Sandesara PB et al. Therapeutic inertia in cardiovascular disease prevention: time to move the bar. J. Am. Coll. Cardiol. 74(13), 1728–1731 (2019).
65.
Batchelor WB, Anwaruddin S, Wang DD et al. The multidisciplinary heart team in cardiovascular medicine: current role and future challenges. JACC Adv. 2(1), 100160 (2023).
66.
Mancia G, Kreutz R, Brunström M et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J. Hypertens. 41(12), 1874–2071 (2023).
• This guideline outlines treatment options for hypertension, as well as adherence tools and guidance on management that were developed by a task force of the European Society of Hypertension.
67.
McEvoy JW, McCarthy CP, Bruno RM et al. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. Eur. Heart J. 45(38), 3912–4018 (2024).
• Similar to the European Society of Hypertension guidelines, this guideline outlines the management of hypertension using different combinations of antihypertensives.
68.
Vrints C, Andreotti F, Koskinas KC et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur. Heart J. 45(36), 3415–3537 (2024).
• These European Society of Cardiology guidelines are useful for patients with overt chronic coronary artery disease, and advise on the various steps of management.
69.
Szwed H, Sadowski Z, Elikowski W et al. Combination treatment in stable effort angina using trimetazidine and metoprolol: results of a randomized, double-blind, multicentre study (TRIMPOL II). TRIMetazidine in POLand. Eur. Heart J. 22(24), 2267–2274 (2001).
70.
Michaelides AP, Spiropoulos K, Dimopoulos K et al. Antianginal efficacy of the combination of trimetazidine-propranolol compared with isosorbide dinitrate-propranolol in patients with stable angina. Clin Drug Investig. 13(1), 8–14 (1997).
71.
Karve S, Cleves MA, Helm M et al. Good and poor adherence: optimal cut-point for adherence measures using administrative claims data. Curr. Med. Res. Opin. 25(9), 2303–2310 (2009).
72.
Alfadda AA, Youssef AM, Al-Sofiani ME et al. Medication adherence and treatment satisfaction with lipid-lowering drugs among patients with diabetes and dyslipidemia. Ann. Pharmacother. 59(2), 105–116 (2025).
73.
Choudhry NK, Setoguchi S, Levin R et al. Trends in adherence to secondary prevention medications in elderly post-myocardial infarction patients. Pharmacoepidemiol. Drug Saf. 17(12), 1189–1196 (2008).
74.
de Oliveira Costa J, Lin J, Pearson SA et al. Persistence and adherence to cardiovascular medicines in Australia. J. Am. Heart Assoc. 12(13), e030264 (2023).
75.
Chapman RH, Benner JS, Petrilla AA et al. Predictors of adherence with antihypertensive and lipid-lowering therapy. Arch. Intern. Med. 165(10), 1147–1152 (2005).
76.
Nelson AJ, Pagidipati NJ, Bosworth HB. Improving medication adherence in cardiovascular disease. Nat. Rev. Cardiol. 21(6), 417–429 (2024).
77.
Benner JS, Chapman RH, Petrilla AA et al. Association between prescription burden and medication adherence in patients initiating antihypertensive and lipid-lowering therapy. Am. J. Health Syst. Pharm. 66(16), 1471–1477 (2009).
78.
Snyman JR, Bortolotto LA, Degli Esposti L et al. A real-world analysis of outcomes and healthcare costs of patients on perindopril/indapamide/amlodipine single-pill vs. multiple-pill combination in Italy. J. Hypertens. 42(1), 136–142 (2024).
79.
Perez de Isla L, Liberopoulos E, Dovizio M et al. Differential adherence to free and single-pill combination of rosuvastatin/ezetimibe: findings from a real-world analysis in Italy. Adv. Ther. 41(8), 3407–3418 (2024).
80.
Zambon A, Liberopoulos E, Dovizio M et al. A real-world analysis of adherence, biochemical outcomes, and healthcare costs in patients treated with rosuvastatin/ezetimibe as single-pill combination vs. free combination in Italy. Eur. Heart J. Open 4(5), oeae074 (2024).
81.
Vijayakumar TM, Jayram J, Meghana Cheekireddy V et al. Safety, efficacy, and bioavailability of fixed-dose combinations in Type 2 diabetes mellitus: a systematic updated review. Curr. Ther. Res. Clin. Exp. 84, 4–9 (2017).
82.
Liu Q, Welsh P, Celis-Morales C et al. Fixed-dose vs loose-dose combination antidiabetic therapy and cardiorenal outcomes in Type 2 diabetes: a nationwide comparative effectiveness study. Cardiovasc. Diabetol. 24(1), 365 (2025).
83.
Calderon Martinez E, Zachariah Saji S, Salazar Ore JV et al. Text messages as a tool to improve cardiovascular disease risk factors control: a systematic review and meta-analysis of randomized clinical trials. BMC Public Health 25(1), 1284 (2025).
84.
Agarwal S, Chin WY, Vasudevan L et al. Digital tracking, provider decision support systems, and targeted client communication via mobile devices to improve primary health care. Cochrane Database Syst. Rev. 4(4), CD012925 (2025).
85.
Widmer RJ, Collins NM, Collins CS et al. Digital health interventions for the prevention of cardiovascular disease: a systematic review and meta-analysis. Mayo Clin. Proc. 90(4), 469–480 (2015).
86.
Verweel L, Newman A, Michaelchuk W et al. The effect of digital interventions on related health literacy and skills for individuals living with chronic diseases: a systematic review and meta-analysis. Int. J. Med. Inform. 177, 105114 (2023).
87.
Katz ME, Mszar R, Grimshaw AA et al. Digital health interventions for hypertension management in US populations experiencing health disparities: a systematic review and meta-analysis. JAMA Netw. Open 7(2), e2356070 (2024).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Creative Commons Attribution 4.0 License
History
Received: 7 October 2025
Accepted: 19 December 2025
Published online: 23 January 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Reshaping the cardiovascular continuum in the management of arterial and venous cardiovascular disease: a narrative review. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0162
Export citation
Select the citation format you wish to export for this article or chapter.